cardiovascular disease assessment in pregnant …
TRANSCRIPT

CARDIOVASCULAR DISEASE IN PREGNANCY AND POSTPARTUM TOOLKIT
NOVEMBER 2017 !
7
CARDIOVASCULAR DISEASE ASSESSMENT IN PREGNANT AND POSTPARTUM WOMEN Afshan'Hameed,'MD'–'University'of'California,'Irvine'Medical'Center'
Elyse'Foster,'MD'–'University'of'California,'San'Francisco'
Elliott'Main,'MD'–'California'Maternal'Quality'Care'Collaborative'
Abha'Khandelwal,'MD,'MS'–'Stanford'University'School'of'Medicine'
Elizabeth'Lawton,'MHS'–'CDPH/MCAH'
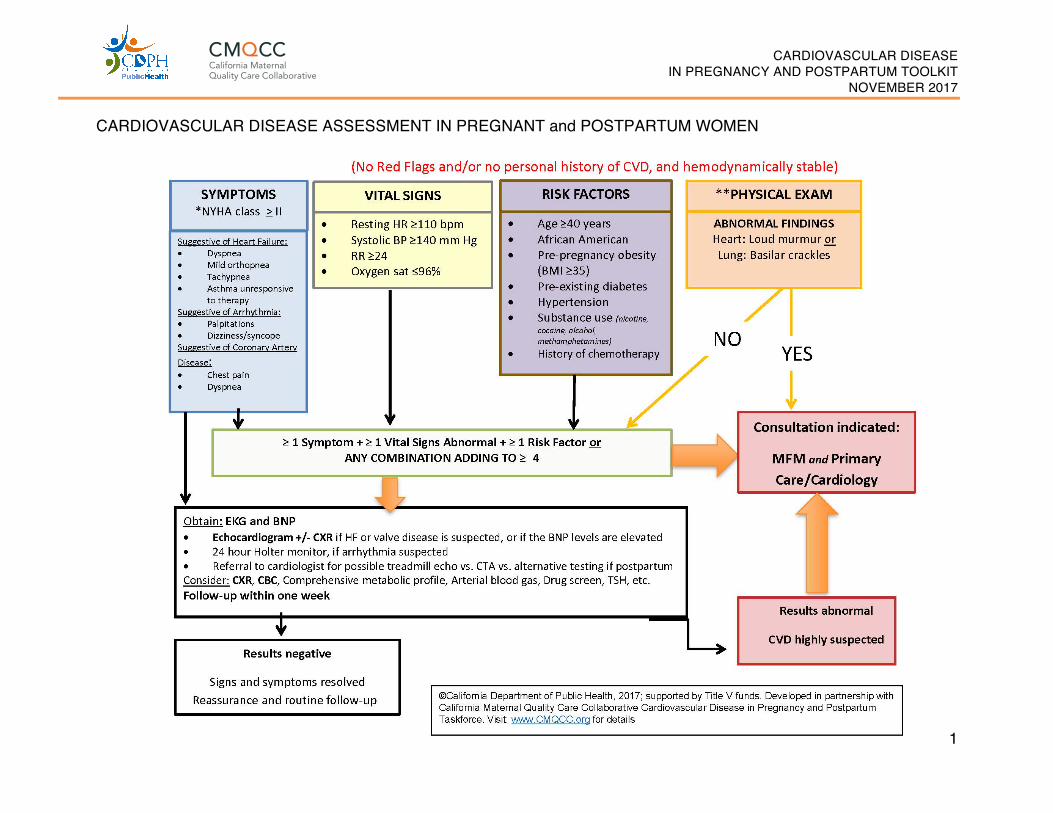
Development of the Algorithm: The CMQCC Cardiovascular Disease in Pregnancy and Postpartum Task Force was charged with developing a toolkit that includes an overview of clinical assessment and management strategies based on risk factors and presenting signs and symptoms. The key components of the Toolkit include an algorithm developed to guide stratification and initial evaluation of symptomatic or high-risk pregnant or postpartum women. The goal of the algorithm is to assist providers in distinguishing between signs and symptoms of cardiac disease and those of normal pregnancy and to guide clinicians in the triage of further cardiac evaluation, appropriate referrals and follow-up of pregnant and postpartum women who may have cardiovascular disease. Drawing from the literature and analysis of cardiovascular deaths reviewed in the California Pregnancy-Associated Mortality Review (CA-PAMR), the authors created this algorithm based on risk factors, symptoms, vital sign abnormalities, and physical examination findings commonly identified in women who die of various types of cardiovascular disease. The most severe symptoms and vital sign abnormalities are labeled as “Red Flags” and include shortness of breath at rest, severe orthopnea necessitating four or more pillows, resting heart rate ≥120 beats per minute, resting systolic blood pressure ≥160 mm Hg, resting respiratory rate of ≥30 breaths per minute and an oxygen saturation ≤94%. The presence of Red Flags or a personal history of cardiovascular disease in pregnant or postpartum women should lead clinicians to conduct a prompt evaluation and seek consultations with specialists in maternal fetal medicine and primary care or cardiology. If other less severe symptoms and vital sign abnormalities are identified, then risk factors and physical examination findings may need to be combined to stratify the women who require further work-up or routine follow-up.

CARDIOVASCULAR DISEASE IN PREGNANCY AND POSTPARTUM TOOLKIT
NOVEMBER 2017 !
8
Sample Case Presentation A 25-year-old obese (Body Mass Index (BMI) 38) African-American G2P2 underwent an uncomplicated vaginal delivery 10 days ago. She presents to the urgent care clinic with complaints of fatigue and persistent cough since delivery. She is afebrile with blood pressure of 110/80 mm Hg, heart rate 110 bpm and respiratory rate of 28/minute. Chest X-ray reveals bilateral infiltrates. Oxygen saturation is 94% on room air. The patient is diagnosed with a respiratory infection. Fatigue is attributed to the lack of sleep due to care of the newborn. She is prescribed an antibiotic and sent home. One week later, she presents again with continued symptoms. Antibiotics are switched at this time, and beta agonists are added due to presumptive diagnosis of “new-onset asthma” as evidenced by physical examination findings. Two days later, the patient experiences cardiac arrest at home. Resuscitation attempts are unsuccessful. Autopsy findings were indicative of cardiomyopathy. This case is representative of similar deaths attributed to cardiovascular disease reviewed by CA-PAMR. Maternal mortality due to cardiac disease primarily revolved around the lack of awareness of CVD at both patient and provider levels, coupled with delays in diagnosis. In most cases, diagnosis was made in the perimortem period or at the time of autopsy.
Further testing should include electrocardiogram (EKG) and B-type natriuretic peptide (BNP). Arrhythmia monitor, echocardiogram, chest X-ray, complete blood count, comprehensive metabolic panel, arterial blood gas, assessment of thyroid function, and drug screen may also be considered. BNP is a readily available test that may help identify asymptomatic women with left ventricular dysfunction and assist in triaging pregnant or postpartum women who present with symptoms. BNP is a neurohormone secreted predominantly by the cardiac ventricles in response to volume or pressure overload. A BNP level of <100 pg/mL is considered normal and the half-life is 20 minutes. Its use has been validated in the diagnosis of systolic and diastolic heart failure.1,2 BNP levels in pregnancy remain within normal range despite significant volume overload in pregnancy, and the levels are higher in pathologic conditions. An elevated BNP level should trigger an echocardiogram to evaluate cardiac function. Serial measurements of BNP in pregnant women with dilated cardiomyopathy are shown to be predictive of adverse cardiovascular outcomes.3. BNP is described in detail on page 13 of the Toolkit.
CARDIOVASCULAR DISEASE IN PREGNANCY AND POSTPARTUM TOOLKIT
NOVEMBER 2017 !
9
The TSH screen is essential for the high risk pregnancy by history or with cardiovascular (CV) symptoms; however, because of the cardiovascular risk with subclinical hypothyroidism and hyperthyroidism and the fact that even high-normal thyroid function may cause cardiovascular problems – all pregnant women with CV problems should get full thyroid function testing.4 When deciding to conduct thyroid screening (TSH) on all pregnant women and advancing to potentially full diagnostic testing (T3 and T4), one is especially looking for subclinical disease that might need treatment.4 Validation of the Algorithm: Pregnant and postpartum women who die from cardiovascular disease represent the most extreme consequence of missed or delayed recognition of cardiovascular disease. Accordingly, any triage algorithm should be able to detect the most serious cases and not return a ‘false negative’ assessment of cardiovascular disease. To assess how well the triage algorithm would have identified pregnant and postpartum women with the most need of further work-up, we compared the 64 cardiovascular disease deaths identified by CA-PAMR for 2002-2006, using the seven critical risks and abnormalities, including heart rate, systolic blood pressure, respiration rate, oxygen saturation, tachypnea, cough and wheezing. We found that the use of algorithm would have identified 56 out of 64 (88%) cases of CVD. The proportion of women identified increased to 93% when we restricted comparison to the 60 cases of women who were symptomatic or had sufficient documentation with which to compare to the algorithm.5 REFERENCES 1. Wei T, Zeng C, Chen L, et al. Systolic and diastolic heart failure are associated
with different plasma levels of B-type natriuretic peptide. Int J Clin Pract. 2005;59(8):891-894.
2. Grewal J, McKelvie R, Lonn E, et al. BNP and NT-proBNP predict echocardiographic severity of diastolic dysfunction. Eur J Heart Fail. 2008;10(3):252-259.
3. Blatt A, Svirski R, Morawsky G, et al. Short and long-term outcome of pregnant women with preexisting dilated cardiomypathy: an NTproBNP and echocardiography-guided study. Isr Med Assoc J. 2010;12(10):613-616.
4. Ertek S, Cicero AF. Hyperthyroidism and cardiovascular complications: a narrative review on the basis of pathophysiology. Arch Med Sci. 2013;9(5):944-952.
5. Hameed A, Main EK, Lawton E, Morton CH, CA-PAMR Committee. Validation Study of Cardiovascular Disease Assessment Algorithm for Pregnant and Postpartum Women among Pregnancy-Related Cardiovascular Deaths in California, 2002-2006. In: University CMQCCaS, ed. Palo Alto, CA2015.

CARDIOVASCULAR DISEASE IN PREGNANCY AND POSTPARTUM TOOLKIT
NOVEMBER 2017
10
CVD ASSESSMENT ALGORITHM FOR PREGNANT and POSTPARTUM WOMEN
CARDIOVASCULAR DISEASE IN PREGNANCY AND POSTPARTUM TOOLKIT
NOVEMBER 2017
11
CARDIOVASCULAR DISEASE ASSESSMENT IN PREGNANT and POSTPARTUM WOMEN

CARDIOVASCULAR DISEASE IN PREGNANCY AND POSTPARTUM TOOLKIT
NOVEMBER 2017
12
*New York Hospital Association Functional Classification (shown on algorithm) Class
Descriptors
I Asymptomatic, no limitation of physical activity II Asymptomatic at rest, symptoms with exertion and heavy physical activity III Asymptomatic at rest, symptoms with normal physical activity IV Symptomatic at rest, limitation to physical activity
Reference: Used with permission from American Heart Association, Inc. NYHA Functional Classification, American Heart Association, Inc. http://www.heart.org/HEARTORG/Conditions/HeartFailure/AboutHeartFailure/Classes-of-Heart-Failure_UCM_306328_Article.jsp Accessed May 1, 2015
**Physical Examination (shown on algorithm)
Lungs (presence of) Heart (presence of) •! Adventitious breath sounds,
particularly crackles •! Diastolic murmur
•! Jugular vein distention •! Loud systolic murmur (III/IV intensity or higher)
o! Functional murmurs generally are of lesser intensity
•! Cyanosis (peripheral) •! Clubbing of extremities
Reference: Easterling TR and Stout K. Heart disease in pregnancy, Chapter 37 in Obstetrics: Normal and Problem Pregnancies, 7th Ed. Eds: Gabbe SG, Niebyl JR, Simpson JL et al. 2017. Elsevier: Philadelphia.