cardiovascular disease prevention in women
TRANSCRIPT

Cardiovascular Disease Prevention in Women
A Paradigm Shift in Risk Assessmentfrom the 2011 Guideline Update
Karen E. Aspry, M.D., M.S., ABCL, FACCAsst. Professor of Medicine—Alpert Medical School
Rhode Island Cardiology Center
>10% Risk of CVD / 10 YrsPregnancy ComplicationsLow Exercise Tolerance Poor DietObesityLupus
Normal BPNormal BMINo Smoking
Normal LipidsDASH-Like Diet
Exercise 150 Min/Week

Sources: CDC/NCHS, AHA Heart Disease and Stroke Statistics, 2011
Cardiovascular Disease Mortality in Women and Men in the U.S.
Recent Progress − 1999 - 2007

Coronary disease mortality rates have increased among middle aged women, and in-hospital mortality during AMI remains higher in women vs. men < 75 years
Stroke prevalence is higher in women, with 55,000 more women experiencing a stroke each year
CV risk factors (obesity, hypertension, hyperlipidemia, physical inactivity) are more prevalent in women
Awareness of CV risk among women remains low, with only 16% identifying CHD as their # 1 health threat
Cardiovascular Disease Morbidity and Mortality in Women
Current and Future Challenges

AHA Guidelines for CV Disease Prevention in Women
Prevention scope is wider
Risk assessment shifts to prediction of global CVD
Low risk category is strictly defined
High and intermediate risk categories expand
Interventions are valued for clinical effectiveness
Diversity and disparities are recognized
Education and adherence are addressed
Cost efficacy is discussed
Key Features of the 2011 Update

Cardiovascular Risk Assessment
and Risk Classification in Women
2011 AHA Guideline Update

Estimated 10 Yr Risk of CHD (via ATP III Risk Score) in a 55 Year Old Female Smoker with Abnormal Blood Lipids and Blood Pressure
www. nhlbi.nih.gov
Cavanaugh-Hussey, MW et al. Preventive
Medicine 2008:47:619.
2011 Guideline Update CHD Risk Scores Underestimate
Global CV Risk in Primary Prevention Women
NATIONAL CHOLESTEROL EDUCATION PROGRAMThird Report of the Expert Panel on
Detection, Evaluation and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III)
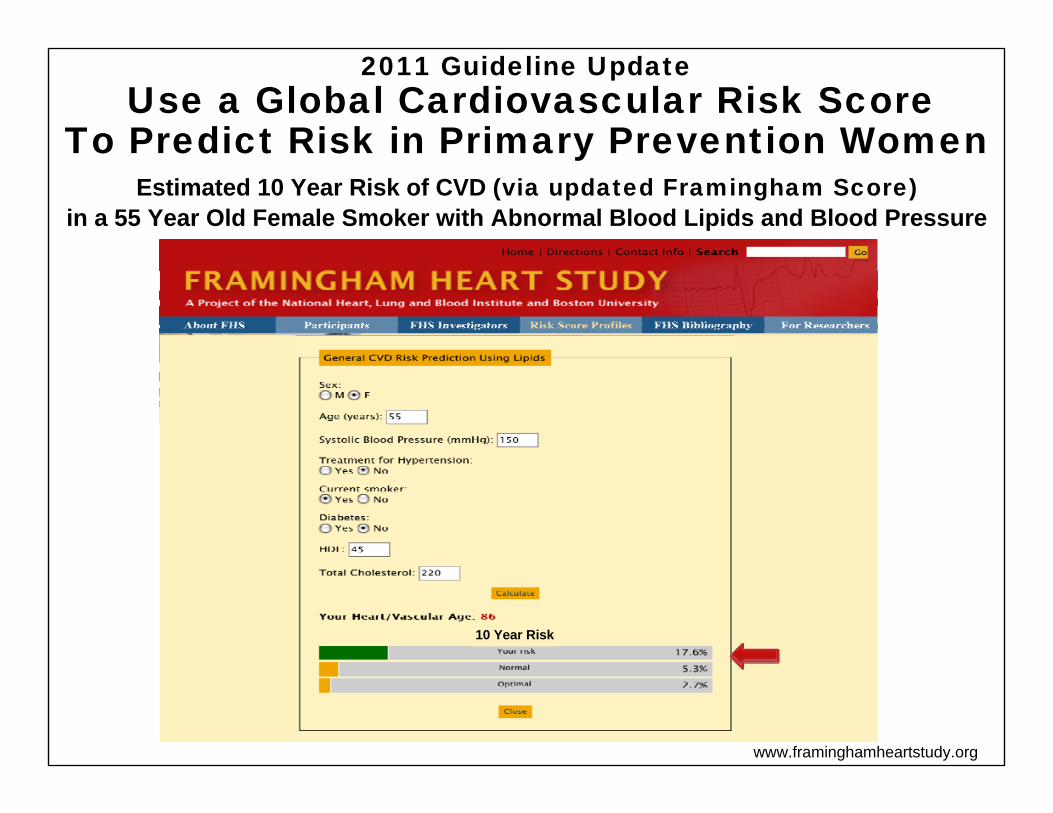
Estimated 10 Year Risk of CVD (via updated Framingham Score) in a 55 Year Old Female Smoker with Abnormal Blood Lipids and Blood Pressure
www.framinghamheartstudy.org
10 Year Risk
2011 Guideline Update Use a Global Cardiovascular Risk Score
To Predict Risk in Primary Prevention Women

Estimated 10 Year Risk of CVD (via the Reynolds Risk Score) in a 55 Year Old Female Smoker with Abnormal Blood Lipids and Blood Pressure
www.reynoldsriskscore.org
2011 Guideline Update Use a Global Cardiovascular Risk Score
To Predict Risk in Primary Prevention Women
Gender O Male Female
Age
Did your Mother or Father have a heart attack before age 60? Yes O No
Systolic Blood Pressure mmHg
HDL or “Good” Cholesterol mg/dL
Do you currently smoke? Yes O No
55
150
Total Cholesterol mg/dL22045
High Sensitivity mg/LC-Reactive Protein (hsCRP) 6
10 Year Risk (age 55) of a heart attackstroke or other heart disease event is 14%
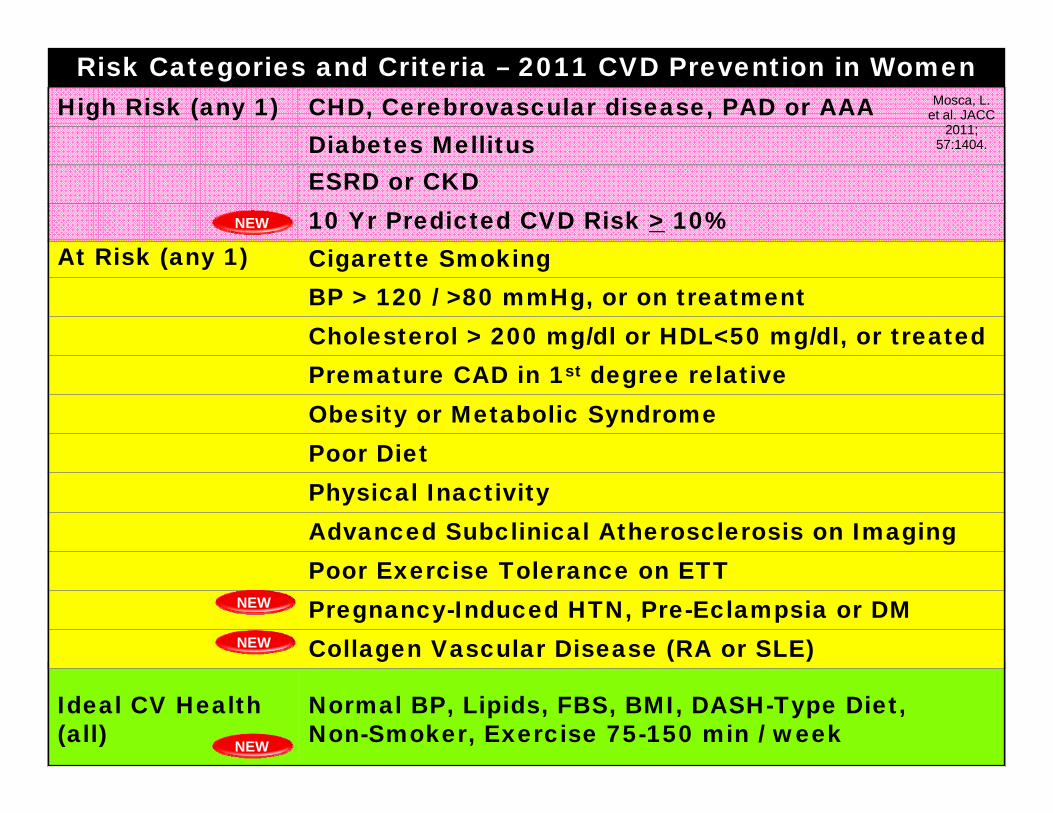
Ideal CV Health (all)
Normal BP, Lipids, FBS, BMI, DASH-Type Diet, Non-Smoker, Exercise 75-150 min / week
Risk Categories and Criteria – 2011 CVD Prevention in Women
NEW
At Risk (any 1) Cigarette SmokingBP > 120 / >80 mmHg, or on treatmentCholesterol > 200 mg/dl or HDL<50 mg/dl, or treatedPremature CAD in 1st degree relativeObesity or Metabolic SyndromePoor DietPhysical InactivityAdvanced Subclinical Atherosclerosis on ImagingPoor Exercise Tolerance on ETTPregnancy-Induced HTN, Pre-Eclampsia or DMCollagen Vascular Disease (RA or SLE)NEW
NEW
High Risk (any 1) CHD, Cerebrovascular disease, PAD or AAADiabetes MellitusESRD or CKD10 Yr Predicted CVD Risk > 10%NEW
Mosca, L. et al. JACC
2011; 57:1404.

2011 Guideline Update Lowering the Threshold for ‘High Risk’*
Reflects the High Lifetime Incidence of CVD in Middle Age Women With Risk Factors
Lloyd-Jones D M et al. Prediction of Lifetime Risk of CVD by Risk Factor Burden
at Age 50. Circulation2006;113:791-798.
0.7
0.6
0.5
0.4
0.3
0.2
0.1
Attained Age, Years
50 60 70 80 90
50%
39%
27%
8%
Cumulative Incidence of CVD by Risk Factor (RF) Burden at Age 50 In Women in the Framingham Study (N=4,362)
BP >160/100, TC>240, Smoking, or DM BP 140/90-160/100, TC 200-240, non-smoker, no DMBP <140/90, TC<200 non-smoker, no DMBP <120/80, TC< 180, non-smoker, no DM
*to >10% / 10 Yrs= >30% / 30 Yrs
Except for those with DM, all
would have a <20% 10 Yr Risk of CVD at age 50

2011 Guideline Update Classification of Pre-Eclampsia as
a Risk Factor is Supported by Observational Studies Showing Increased CHD Rates
From:
Bellamy L et al. BMJ 2007;
335:974.
Systematic Review of Pre-Eclampsia and Relative Risk of CHDin 8 Cohort Studies (n=121,487 cases) with Mean FU 11.7 YrsStudy Total # Cases /
Women with Pre-Eclampsia
Total # Cases / Women With No Pre-Eclampsia
Hannaford, 1997 69 / 2371 216 / 14,831
Irgens, 2001 27 / 24,155 325 / 602,117
Smith, 2001 12 / 22,781 31 / 106,509
Wilson, 2003 26 / 1,043 10 / 796
Kestenbaum, 2003 35/20,552 64/92,902
Funai, 2005 41 / 1,070 269 / 35,991
Ray, 2005 228 / 36,982 1,262 / 950,885
Wirkstrom, 2005 176 / 12,533 2,306 / 383,081
Total (95% CI)Heterogeneity Test
Test for Overall Effect
614 / 121,487X2=9.6, P 0.21
Z=10.00, P 0.001
4,483 / 2,187,112

2011 Guideline Update Classification of RA and SLE as Risk Factors
is Supported by Observational Studies Showing Increased Relative Risk of MI*
Adjusted* Relative Risk of First MI Among Women with Confirmed RA In the Nurses’ Health Study (N=114,342)
Solomon, DH et al. Circulation 2003; 107:1303-07.
Myocardial Infarctions No RA RA P
Incidence/100,000 person-years 96 272
Adjusted RR 1.0 (ref) 2.0 0.0025
**Adjusted for Age, DM, Hyperlipidemia, Hypertension, Parental history of MI, Smoking, Physical activity, BMI, use of ASA, steroids, and NSAIDS, and intakes of vitamin E, folate and Omega-3-FAs

Interventions for Preventionof CV Disease in Women
2011 AHA Guideline Update

Class I
Benefit >>> Risk
Procedure/ Treatment SHOULD be performed/ administered
Class IIa
Benefit >> RiskAdditional studies with focused objectives needed
IT IS REASONABLE to perform procedure/administer treatment
Class IIb
Benefit ≥ RiskAdditional studies with broad objectives needed; Additional registry data would be helpful
Procedure/Treatment MAY BE CONSIDERED
Class III
Risk ≥ BenefitNo additional studies needed
Procedure/Treatment should NOT be performed/administeredSINCE IT IS NOT HELPFUL AND MAY BE HARMFUL
Level A: Multiple randomized clinical trials or meta-analyses provide dataMultiple populations evaluated
Level B: Single randomized trial or nonrandomized studies provide data Limited populations evaluated
Level C: Consensus of opinion, case studies, or standard of care provide data Very limited populations evaluated
Recommendation Classification and Level of Evidence
Level of Evidence (LOE):

Interventions Level of Evidence
Menopausal TherapyHormone Replacement Therapy or SERMs
III A
Anti-Oxidant SupplementsVitamin E, Vitamin C, Beta-Carotene
III A
Folic Acid III A
Aspirin in At Risk Women Age < 65 III B
Class III RecommendationsTreatment Not Useful and May Be HarmfulClass III RecommendationsTreatment Not Useful and May Be Harmful
JACC 2011; 57:1404-23

Diet and Lifestyle Interventions Class, LOE
Smoking Cessation Counsel and provide nicotine replacement and pharmacotherapy I, BPhysical Activity Advise 150 min/week of moderate or 75min/week of vigorous exercise, and muscle strengthening 2 days/week
I, B
Diet and Supplements Advise a diet rich in fruits, vegetables, whole grains, high fiber foods, and oily fish; low in saturated fat, cholesterol, alcohol, sodium, and sugar; and free of trans-fatsConsider Omega-3-Fatty Acid supplementation
I, B
II b, BWeight MaintenanceAdvise weight loss through exercise, calorie reduction, or behavioral programs to maintain BMI < 25 and waist <35” I, BCardiac Rehabilitation Advise formal on-site or in-home exercise training after a CHD event or CVA, or with symptomatic PAD or chronic angina
I, AJACC 2011; 57:1404-23
Class I and II RecommendationsTreatment Should Be Provided (Class I)
or Is Reasonable (Class IIa) or Can Be Considered (IIb)
Class I and II RecommendationsTreatment Should Be Provided (Class I)
or Is Reasonable (Class IIa) or Can Be Considered (IIb)

Major Risk Factor Interventions Class, LOE
Blood Pressure Control to <120/80mmHgAdvise DASH-diet and lifestyle interventions in allAdvise drugs if BP >140/90 (>130/80 with DM or CKD)
I, BI, A
Lipid Control to LDL<100, TG <150, HDL >50 and Non-HDL to <130mg/dlAdvise diet and lifestyle interventions in allDrugs useful to achieve LDL <100 with CHD Drugs useful to achieve LDL <100 with DM, PVD or Risk >20% Niacin/fibrates useful if HDL<50 or non-HDL>130 in high risk Drugs useful if LDL >130 and Risk is 10-20%Drugs useful if LDL >160 even if Risk is <10%Drugs useful if LDL >190 regardless of risk levelDrugs can be considered if age >60, LDL<130 and hsCRP>2
I, BI, A I, B
IIb, B I, BI, BI, B
IIb, BBlood Glucose Control in Diabetics Advise diet with or without drugs to achieve HgbA1C<7% IIa, B
Class I and II RecommendationsTreatment Should Be Provided (Class I)
or Is Reasonable (Class IIa) or Can Be Considered (IIb)
Class I and II RecommendationsTreatment Should Be Provided (Class I)
or Is Reasonable (Class IIa) or Can Be Considered (IIb)
High Risk
At Risk
?

Preventive Drug Interventions Class, LOE
AspirinShould be used in all women with CHD, unless contraindicatedIs reasonable in women with DM, unless contraindicatedCan be useful in women > 65 years, if BP is controlled May be reasonable for women <65 years for CVA preventionShould be used in women with AF unable to take anti-coagulants
I, AIIa, BIIa, BIIb, BI, A
Anti-Coagulant Therapy for Atrial Fibrillation Should be used in women with AF, stroke risk and low bleeding risk I, ABeta BlockersShould be used for up to 3 years post ACS with normal LVEFShould be used indefinitely with LV failureMay be considered in other women with CHD or vascular disease
I, BI, A
IIb, C ACE Inhibitors or ARBSShould be used if MI, CHF, LVEF<40%, or DM, unless contraindicated I, AAldosterone AntagonistsShould be used post MI with heart failure, unless contraindicated 1, B
Class I and II RecommendationsTreatment Should Be Provided (Class I)
or Is Reasonable (Class IIa) or Can Be Considered (IIb)
Class I and II RecommendationsTreatment Should Be Provided (Class I)
or Is Reasonable (Class IIa) or Can Be Considered (IIb)

Yes
Recent CV Event?
Refer to Cardiac Rehab
Implement Class I Risk Factor and Drug
RecommendationsASA
Beta BlockerACEI or ARB
LDL control to <100
Algorithm for CVD Prevention In Women per
the 2011 Guideline Update
Modified from: JACC 2011; 57:1404-23.
Risk AssessmentCV Symptoms and Depression ScreeningMedical, Pregnancy and Family History
PE including BMI and Waist SizeLabs including FBS and Lipids
CVD Risk Scoring if no CHD, PAD or DM
History of Arial Fibrillation ?
Implement ASA or Anti-Coagulant Therapy
Yes
Implement Diet and Lifestyle Interventions (Class I) For AllSmoking Cessation DASH-type Diet Physical Activity Weight Control
High Risk ?CHD, CVA, PAD or AAA
DM or CKD>10% Predicted Risk of CVD in 10 Yrs
Yes
Yes
Yes
Consider Class II Recommendations
LDL control to <70Drugs to target non-HDL + HDL
Omega-3 fatty acids
At Risk ?Any 1 Risk Factor From Table
Implement Class I Risk Factor
RecommendationsBP control
LDL control to goal
Consider Class II Recommendations
ASATherapy for non-HDL + HDL
(in selected women)
No
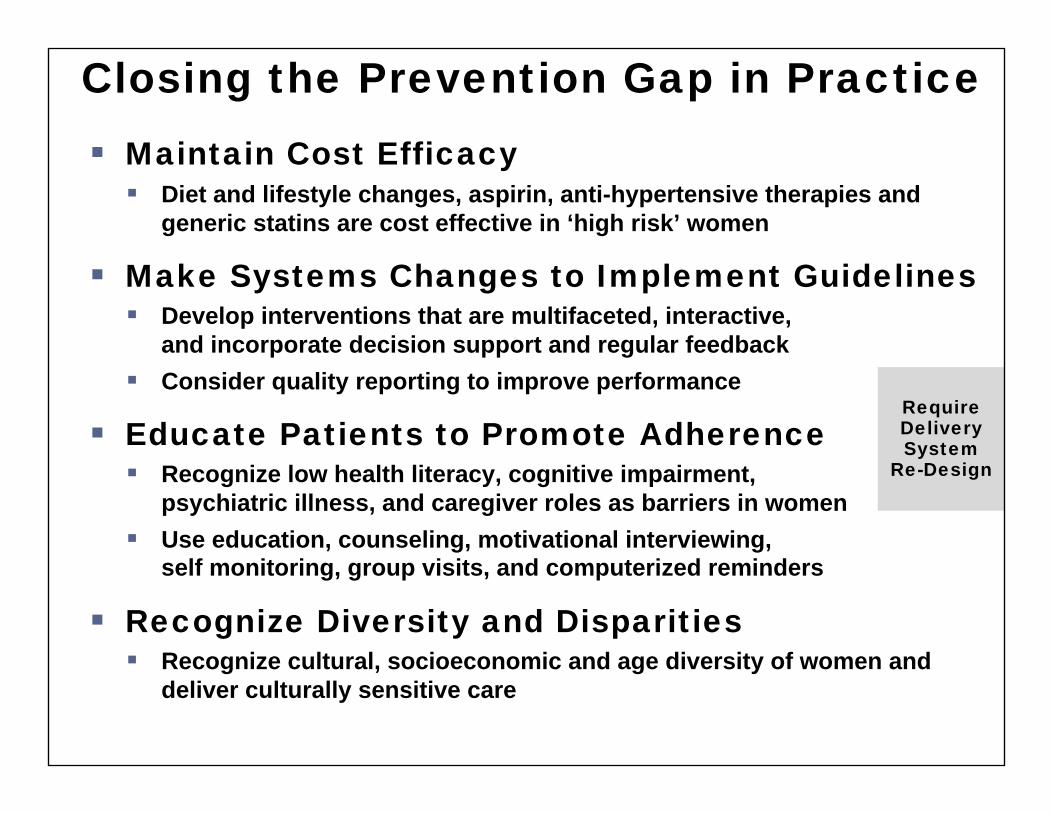
Closing the Prevention Gap in Practice Maintain Cost Efficacy Diet and lifestyle changes, aspirin, anti-hypertensive therapies and
generic statins are cost effective in ‘high risk’ women
Make Systems Changes to Implement Guidelines Develop interventions that are multifaceted, interactive,
and incorporate decision support and regular feedback Consider quality reporting to improve performance
Educate Patients to Promote Adherence Recognize low health literacy, cognitive impairment,
psychiatric illness, and caregiver roles as barriers in women Use education, counseling, motivational interviewing,
self monitoring, group visits, and computerized reminders
Recognize Diversity and Disparities Recognize cultural, socioeconomic and age diversity of women and
deliver culturally sensitive care
RequireDelivery System
Re-Design

Summary CV disease mortality in women has decreased in the
last decade but challenges remain
Higher mortality during acute CHD events, higher stroke rates, a higher burden of CV risk factors, and lower awareness of CV risk mandate more aggressive prevention efforts in women
The 2011 update shifts to global CV risk assessment, redefines optimal risk, lowers the threshold for high risk, and adds ‘gender specific’ risk factors
Prevention efforts are likely to be more successful if they incorporate elements of the Chronic Care Model, including team approaches, decision support, patient education, and regular feedback; recognize and respect patient diversity, and maintain cost efficacy