cardiovascular outcome trials - cardiac safety outcome trials how is benefit-risk appropriately...
TRANSCRIPT

Cardiovascular Outcome TrialsHow is Benefit-Risk Appropriately
Balanced with Respect to
Cardiovascular Outcomes?
Sanjay Kaul, MD, FACC, FAHA
Division of Cardiology
Cedars-Sinai Medical Center
Los Angeles, California, USA

“There is a tendency to make the measurable important,
rather than the important measurable”
Robert S. McNamara
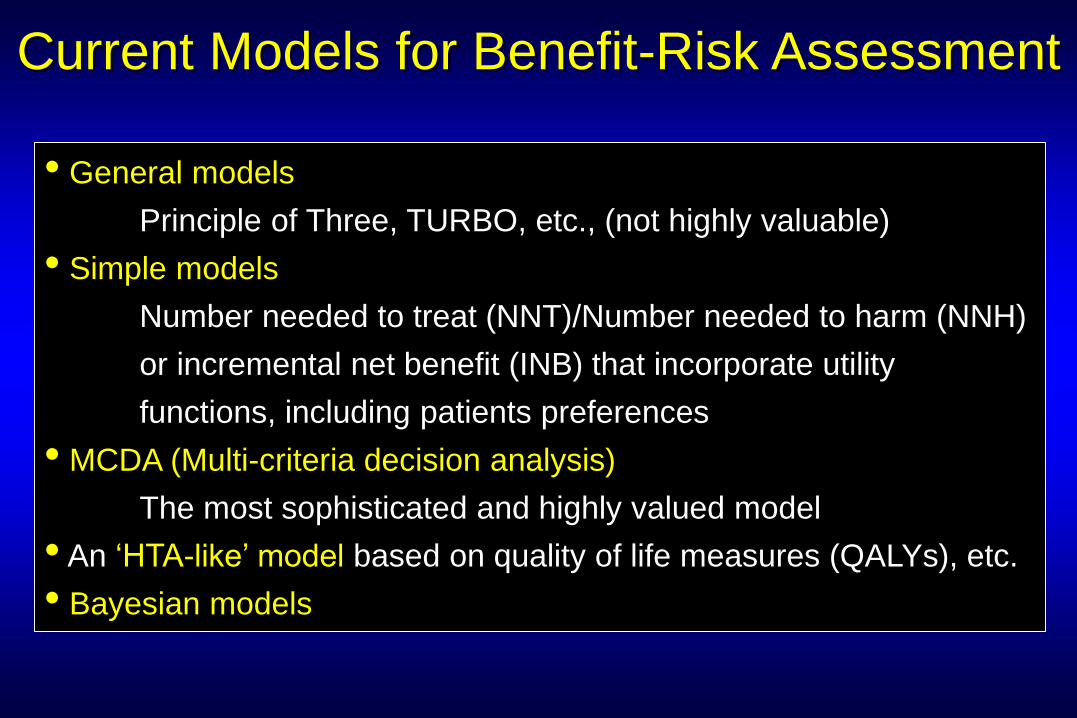
Current Models for Benefit-Risk Assessment
• General models
Principle of Three, TURBO, etc., (not highly valuable)
• Simple models
Number needed to treat (NNT)/Number needed to harm (NNH)
or incremental net benefit (INB) that incorporate utility
functions, including patients preferences
• MCDA (Multi-criteria decision analysis)
The most sophisticated and highly valued model
• An ‘HTA-like’ model based on quality of life measures (QALYs), etc.
• Bayesian models
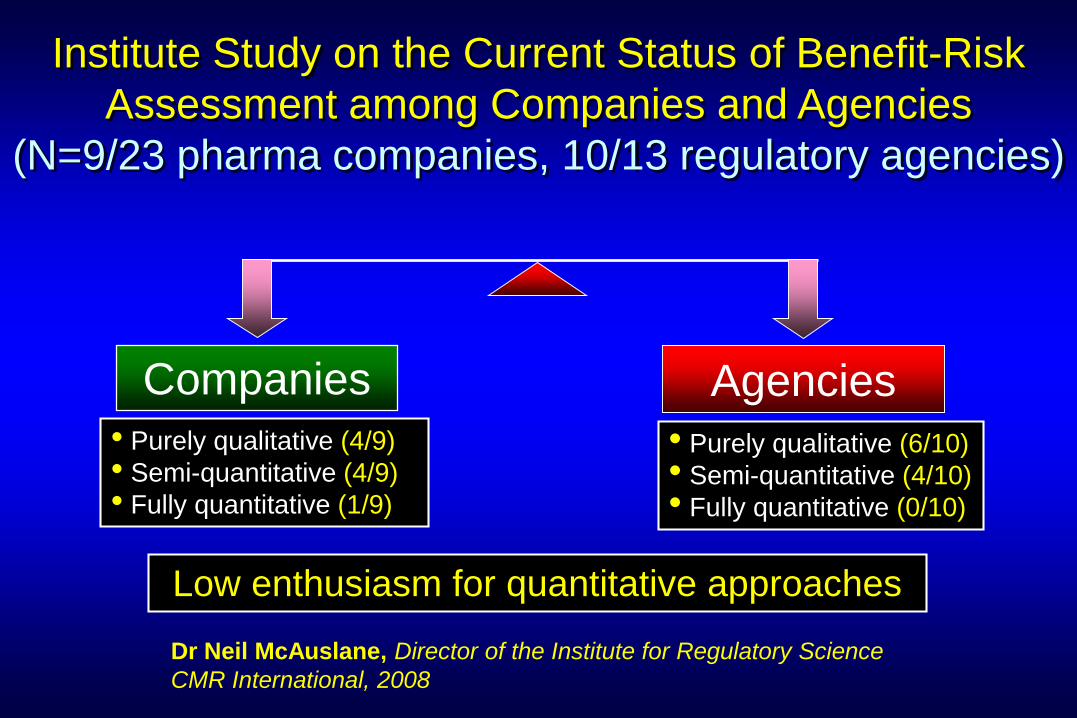
Institute Study on the Current Status of Benefit-Risk
Assessment among Companies and Agencies
(N=9/23 pharma companies, 10/13 regulatory agencies)
Companies
• Purely qualitative (4/9)
• Semi-quantitative (4/9)
• Fully quantitative (1/9)
Agencies
• Purely qualitative (6/10)
• Semi-quantitative (4/10)
• Fully quantitative (0/10)
Dr Neil McAuslane, Director of the Institute for Regulatory Science
CMR International, 2008
Low enthusiasm for quantitative approaches
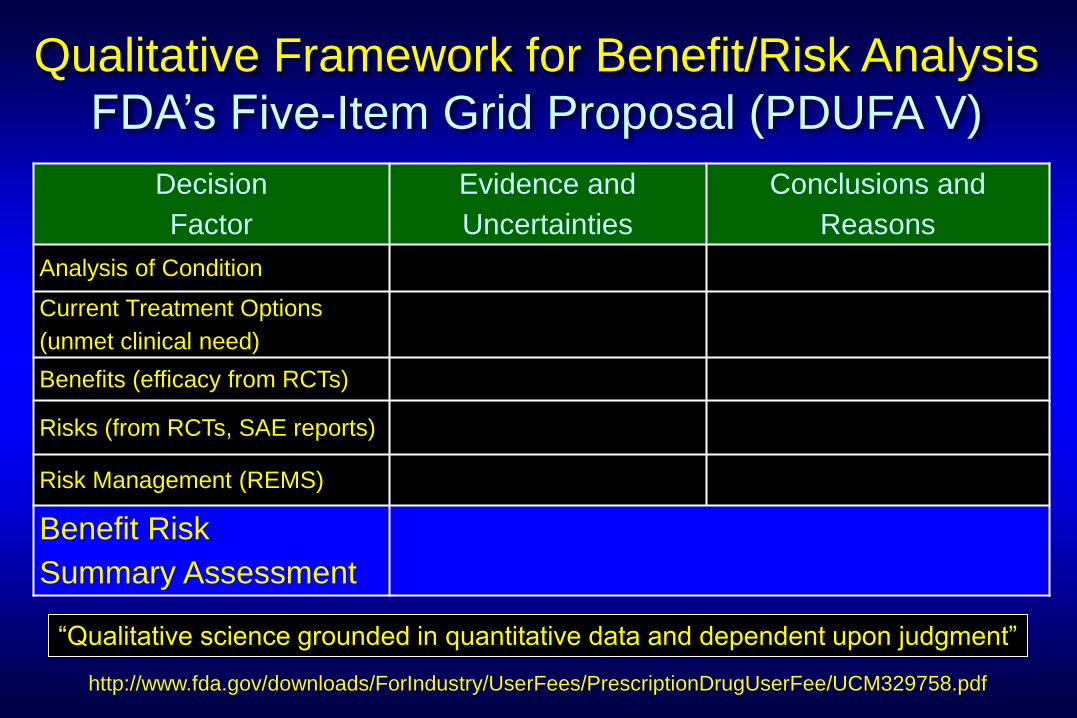
Decision
Factor
Evidence and
Uncertainties
Conclusions and
Reasons
Analysis of Condition
Current Treatment Options
(unmet clinical need)
Benefits (efficacy from RCTs)
Risks (from RCTs, SAE reports)
Risk Management (REMS)
Benefit Risk
Summary Assessment
Qualitative Framework for Benefit/Risk Analysis
FDA’s Five-Item Grid Proposal (PDUFA V)
“Qualitative science grounded in quantitative data and dependent upon judgment”
http://www.fda.gov/downloads/ForIndustry/UserFees/PrescriptionDrugUserFee/UCM329758.pdf

Strength
of evidence
Assessing Drug SafetyKey Elements in Decision Making
Seriousness
& magnitude
of adverse
event
Safer
alternatives
& patient
preference

9Critical
(death, Q-MI, disabling stroke,
major bleeding)
8
7
6 Important, but not critical(recurrent ischemia, recurrent
hospitalization, restenosis / TVR,
silent /biomarker MI, groin hematoma)
5
4
3Informative, but not important
(surrogate markers: LDL, BS/A1C, BP,
CRP, PVCs, creatinine)
2
1
Grading Importance of Outcomes
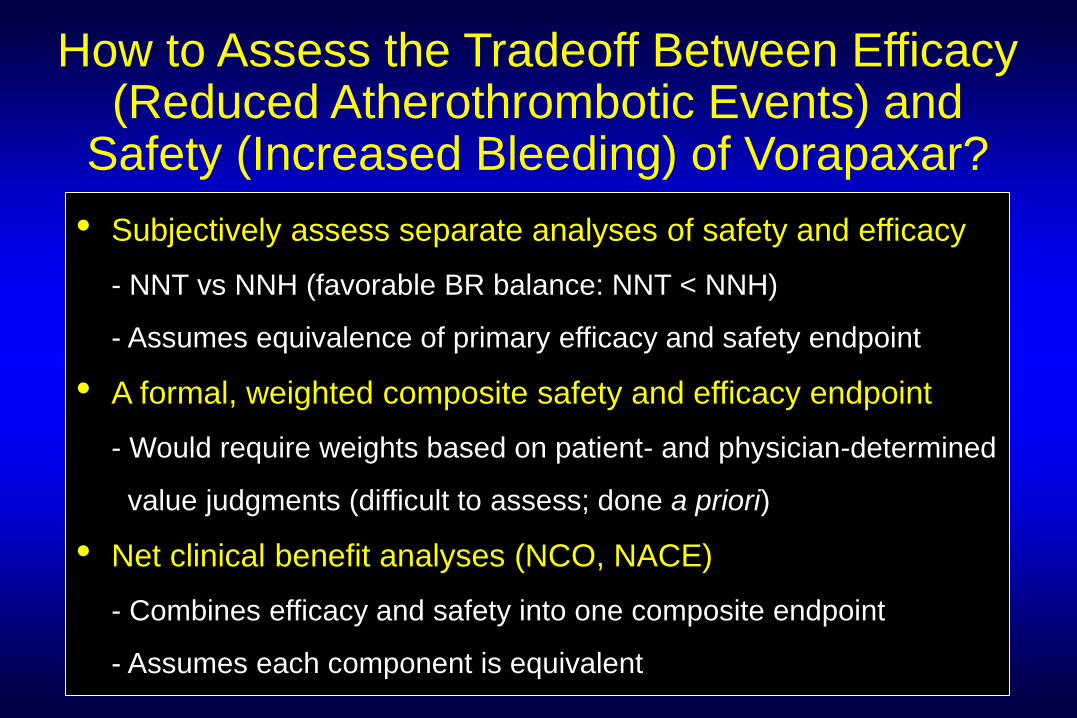
How to Assess the Tradeoff Between Efficacy (Reduced Atherothrombotic Events) and
Safety (Increased Bleeding) of Vorapaxar?
• Subjectively assess separate analyses of safety and efficacy
- NNT vs NNH (favorable BR balance: NNT < NNH)
- Assumes equivalence of primary efficacy and safety endpoint
• A formal, weighted composite safety and efficacy endpoint
- Would require weights based on patient- and physician-determined
value judgments (difficult to assess; done a priori)
• Net clinical benefit analyses (NCO, NACE)
- Combines efficacy and safety into one composite endpoint
- Assumes each component is equivalent
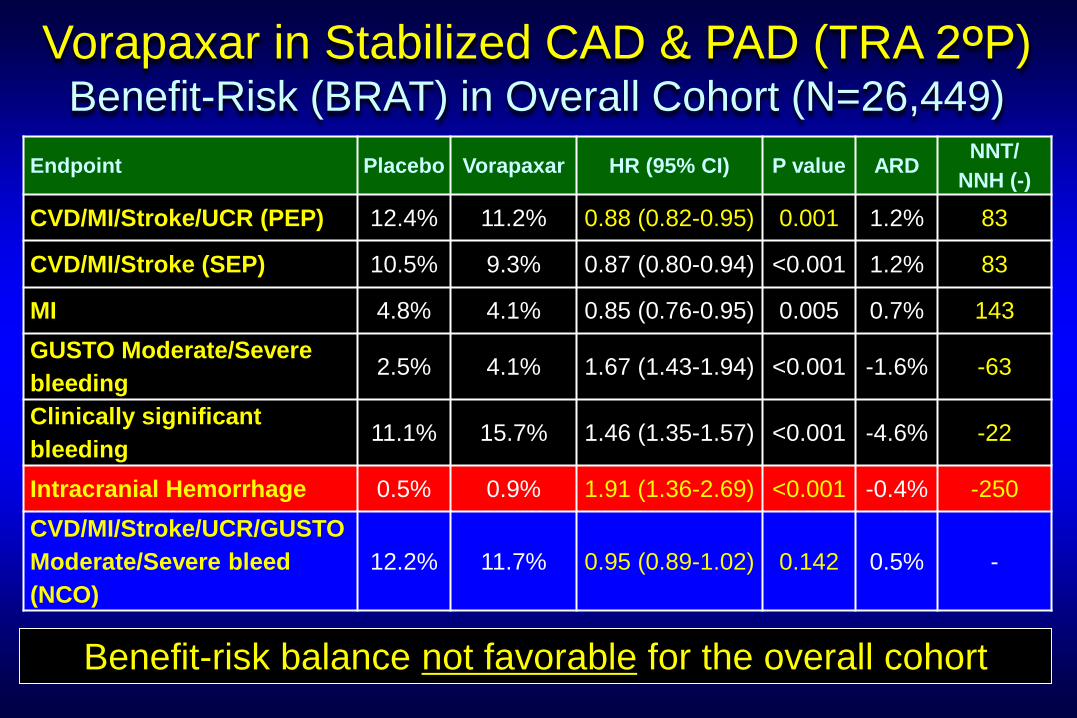
Endpoint Placebo Vorapaxar HR (95% CI) P value ARDNNT/
NNH (-)
CVD/MI/Stroke/UCR (PEP) 12.4% 11.2% 0.88 (0.82-0.95) 0.001 1.2% 83
CVD/MI/Stroke (SEP) 10.5% 9.3% 0.87 (0.80-0.94) <0.001 1.2% 83
MI 4.8% 4.1% 0.85 (0.76-0.95) 0.005 0.7% 143
GUSTO Moderate/Severe
bleeding 2.5% 4.1% 1.67 (1.43-1.94) <0.001 -1.6% -63
Clinically significant
bleeding11.1% 15.7% 1.46 (1.35-1.57) <0.001 -4.6% -22
Intracranial Hemorrhage 0.5% 0.9% 1.91 (1.36-2.69) <0.001 -0.4% -250
CVD/MI/Stroke/UCR/GUSTO
Moderate/Severe bleed
(NCO)
12.2% 11.7% 0.95 (0.89-1.02) 0.142 0.5% -
Vorapaxar in Stabilized CAD & PAD (TRA 2OP) Benefit-Risk (BRAT) in Overall Cohort (N=26,449)
Benefit-risk balance not favorable for the overall cohort

Vorapaxar in TRA 2OPBenefit-Risk in Proposed Label Population* (N=16,856)
Endpoint Placebo Vorapaxar HR (95% CI) P value ARDNNT/
NNH (-)
CVD/MI/Stroke/UCR (PEP) 11.4% 9.8% 0.82 (0.74-0.90) <0.001 1.6% 63
CVD/MI/Stroke (SEP) 9.0% 7.4% 0.78 (0.70-0.88) <0.001 1.6% 63
MI 5.3% 4.4% 0.83 (0.72-0.95) 0.005 0.9% 111
GUSTO Moderate/Severe
bleeding2.0% 3.0% 1.54 (1.24-1.90) <0.001 -1.0% -100
Clinically significant
bleeding10.2% 14.8% 1.48 (1.35-1.63) <0.001 -4.6% -22
Intracranial Hemorrhage 0.4% 0.5% 1.44 (0.87-2.40) 0.160 -0.1% -
CVD/MI/Stroke/UCR/GUSTO
Moderate/Severe bleed
(NCO)
11.5% 10.3% 0.89 (0.82-0.98) 0.017 1.2% 83
Benefit-risk balance favorable for proposed label population
*History of MI and without prior stroke or transient ischemic attack (post hoc subset)

Vorapaxar in TRA 2OPTreatment Effect According to Eligibility Criterion
• Benefit driven by treatment effect in CAD stratum
• No heterogeneity of treatment effect in CAD and PAD strata
PopulationEnrollment
Criterion
Proposed
Label
Approved
Label
CAD stratum
(>2-52 wks post-MI)0.83 (0.76-0.92) 0.82 (0.74-0.90) 0.82 (0.74-0.90)
CVD stratum 1.02 (0.84-1.23) No No
PAD stratum 0.95 (0.79-1.14) No 0.87 (0.71-1.06)
Overall 0.88 (0.82-0.95) 0.82 (0.74-0.90) 0.83 (0.76-0.90)
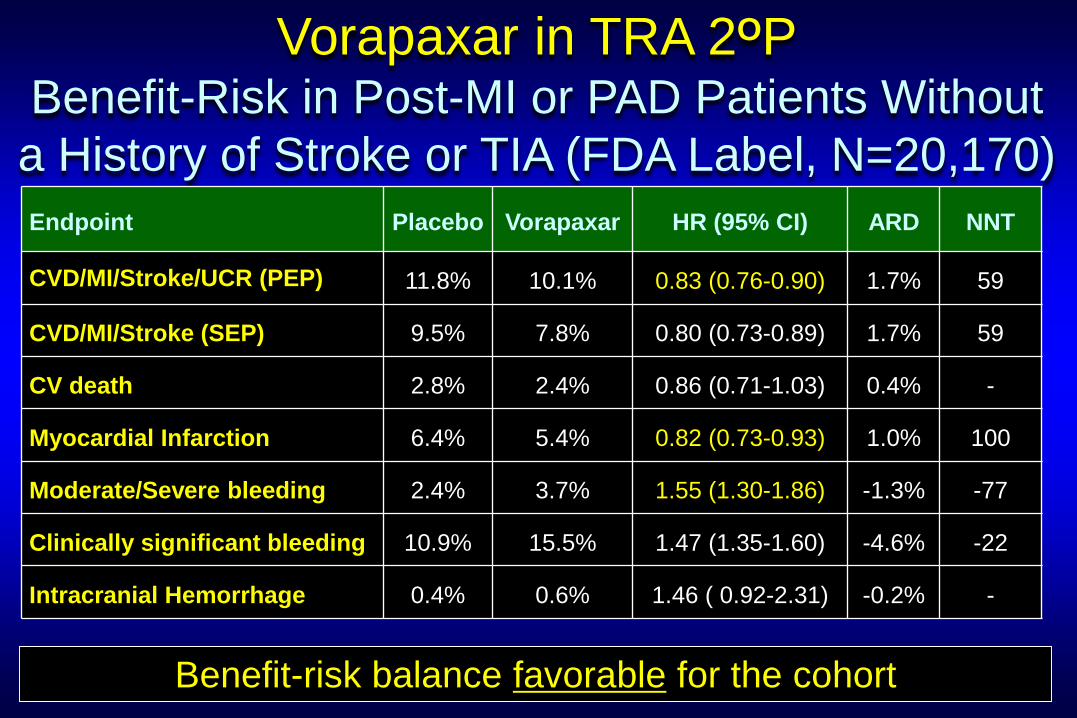
Vorapaxar in TRA 2OPBenefit-Risk in Post-MI or PAD Patients Without
a History of Stroke or TIA (FDA Label, N=20,170)
Benefit-risk balance favorable for the cohort
Endpoint Placebo Vorapaxar HR (95% CI) ARD NNT
CVD/MI/Stroke/UCR (PEP) 11.8% 10.1% 0.83 (0.76-0.90) 1.7% 59
CVD/MI/Stroke (SEP) 9.5% 7.8% 0.80 (0.73-0.89) 1.7% 59
CV death 2.8% 2.4% 0.86 (0.71-1.03) 0.4% -
Myocardial Infarction 6.4% 5.4% 0.82 (0.73-0.93) 1.0% 100
Moderate/Severe bleeding 2.4% 3.7% 1.55 (1.30-1.86) -1.3% -77
Clinically significant bleeding 10.9% 15.5% 1.47 (1.35-1.60) -4.6% -22
Intracranial Hemorrhage 0.4% 0.6% 1.46 ( 0.92-2.31) -0.2% -

Endpoint Placebo Vorapaxar HR (95% CI) P value ARDNNT/
NNH (-)
CVD/MI/Stroke/UCR (PEP) 19.9% 18.5% 0.92 (0.85-1.01) 0.072 1.4% -
CVD/MI/Stroke (SEP) 16.4% 14.7% 0.89 (0.81-0.98) 0.018 1.7% 58
MI 10.3% 9.2% 0.88 (0.78-0.99) 0.033 1.4% 71
GUSTO Moderate/Severe
bleeding 5.8% 7.6% 1.36 (1.18-1.57) <0.001 -1.9% -56
Clinically significant
bleeding14.6% 19.5% 1.41 (1.29-1.54) <0.001 -4.9% -21
Intracranial Hemorrhage 0.4% 1.1% 2.52 (1.48-4.29) <0.001 -0.7% -143
Vorapaxar in ACS (TRACER Trial) Benefit-Risk in Overall Cohort (N=12,944)
Benefit-risk balance not favorable for the overall cohort

Benefit-Risk Balance in TRA 2OP (Approved Label)1000 Patients Treated with Vorapaxar Instead of Placebo
Vorapaxar vs placebo
Benefit
• 17 ischemic endpoints prevented
- 10 MIs
Risk
• 13 excess GUSTO Mod/Severe bleedsor
• 46 excess clinically significant bleeds- 12 GI bleeds
Does the evidence favor Class I (benefit >>> risk)
recommendation for vorapaxar in stabilized ACS/PAD?
Clinical importance of MIs? Fatal vs nonfatal
? Q-wave vs non-Q wave MI
? Heart failure/LVSD, arrhythmia, SCD
Clinical importance of Bleeds? Hospitalizations
? Resource utilization

How is Bleeding Different from a MI?Variable Weights Based on Perception of “Utility”
CAD
MI risk Bleeding risk • MIs are part of the disease,
incompletely prevented by
therapy
• Can’t count the MIs that
are prevented
• All MIs are not created equal
(clinical importance varies)
• Spontaneous major bleeding
is unusual, bleeding
unequivocally caused by Rx
• Events are easy to count
• Bleeding causes panic
• Increased LOS and cost
Asymmetry in assessment of benefit-harm (bleeding > MI)
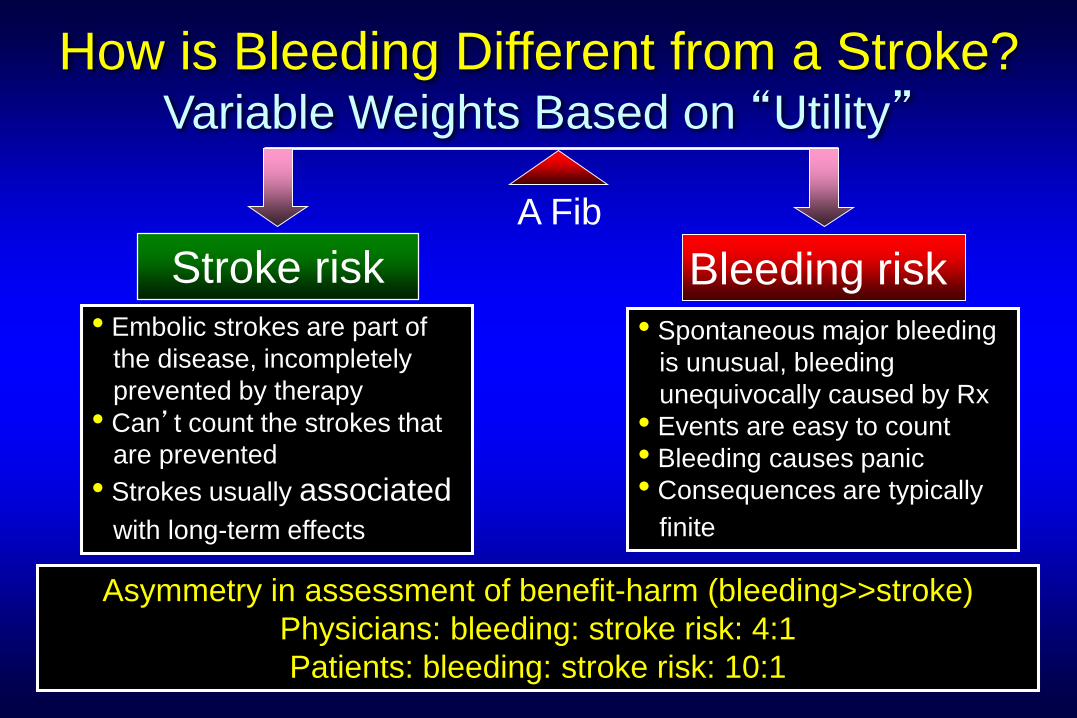
How is Bleeding Different from a Stroke?Variable Weights Based on “Utility”
A Fib
Stroke risk Bleeding risk • Embolic strokes are part of
the disease, incompletely
prevented by therapy
• Can’t count the strokes that
are prevented
• Strokes usually associated
with long-term effects
• Spontaneous major bleeding
is unusual, bleeding
unequivocally caused by Rx
• Events are easy to count
• Bleeding causes panic
• Consequences are typically
finite
Asymmetry in assessment of benefit-harm (bleeding>>stroke)
Physicians: bleeding: stroke risk: 4:1
Patients: bleeding: stroke risk: 10:1
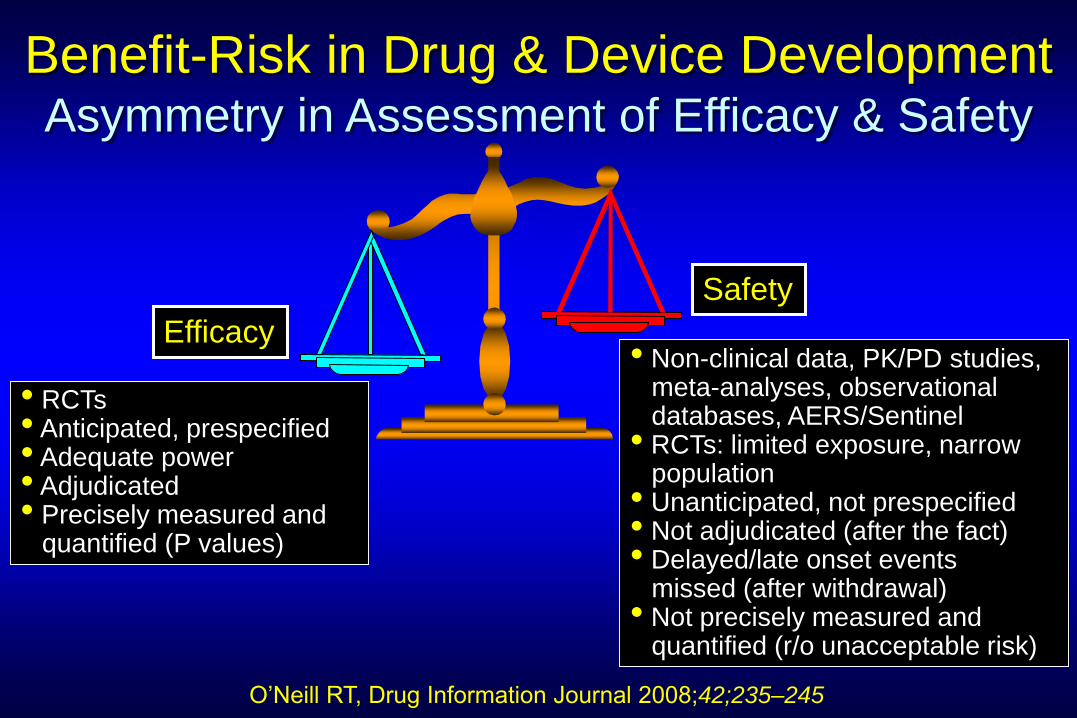
Benefit-Risk in Drug & Device DevelopmentAsymmetry in Assessment of Efficacy & Safety
• RCTs• Anticipated, prespecified• Adequate power• Adjudicated• Precisely measured and
quantified (P values)
Efficacy• Non-clinical data, PK/PD studies,
meta-analyses, observational databases, AERS/Sentinel
• RCTs: limited exposure, narrow population
• Unanticipated, not prespecified • Not adjudicated (after the fact)• Delayed/late onset events
missed (after withdrawal)• Not precisely measured and
quantified (r/o unacceptable risk)
Safety
O’Neill RT, Drug Information Journal 2008;42;235–245

Assessing Drug Safety Post-Approval Lessons from Vioxx, Avandia and Meridia
CharacteristicRofecoxib
(Vioxx)
Rosiglitazone
(Avandia)
Sibutramine
(Meridia)
Date of approval 5/20/1999 5/25/1999 11/22/1997
Approval outcome Pain control Glycemic control Weight loss
Indication- Osteoarthritis
- Acute pain in adults
- Dysmenorrhea
- Type 2 DM in
conjunction with
diet and exercise
- Obesity
BMI>30kg/m2
BMI>27kg/m2 + CRF
Warnings, precautionsGI side effects,
renal diseaseClass III/IV CHF
Uncontrolled HTN,
CVD, CHF, arrhythmia
Post-marketing safety trialVIGOR
(N=8,076; 9m)
RECORD
(N=4,447)
SCOUT
(N=10,000; 3.8y)
Safety signal Excess CV risk ? CV risk Excess CV risk
Post-approval
regulatory actionWithdrawn
9/29/2004
Restricted access
10/8/2010
Withdrawn
10/8/2010
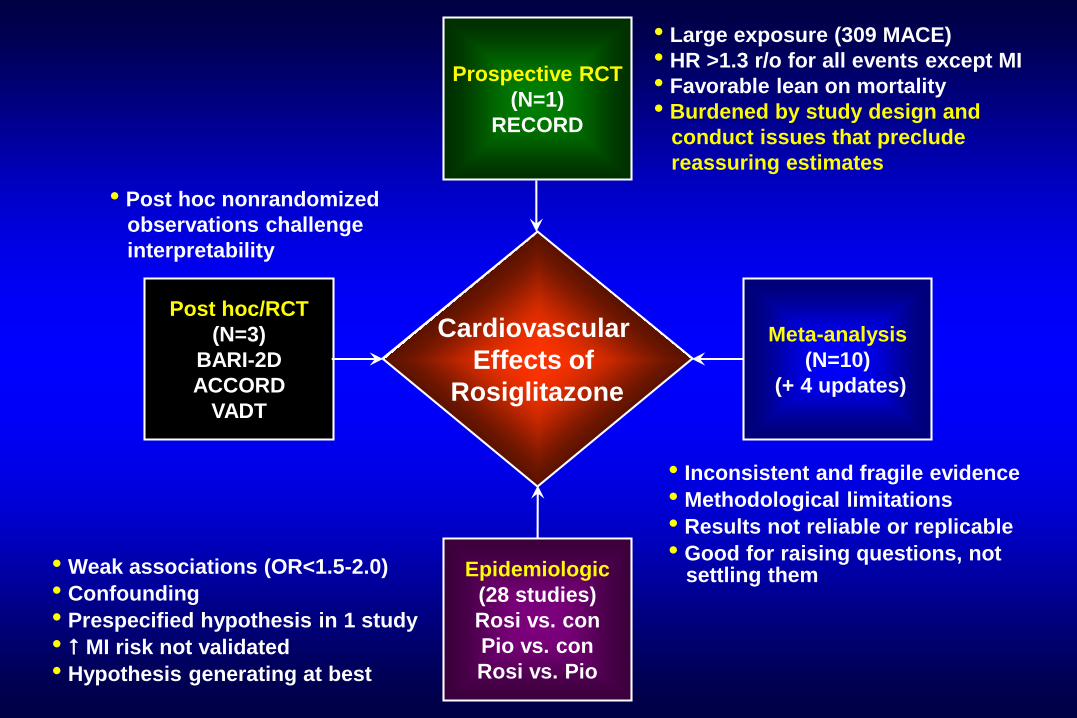
Meta-analysis
(N=10)
(+ 4 updates)
Prospective RCT
(N=1)
RECORD
Epidemiologic
(28 studies)
Rosi vs. con
Pio vs. con
Rosi vs. Pio
Post hoc/RCT
(N=3)
BARI-2D
ACCORD
VADT
Cardiovascular
Effects of
Rosiglitazone
• Large exposure (309 MACE)
• HR >1.3 r/o for all events except MI
• Favorable lean on mortality
• Burdened by study design and
conduct issues that preclude
reassuring estimates
• Inconsistent and fragile evidence
• Methodological limitations
• Results not reliable or replicable
• Good for raising questions, not settling them • Weak associations (OR<1.5-2.0)
• Confounding
• Prespecified hypothesis in 1 study
• MI risk not validated
• Hypothesis generating at best
• Post hoc nonrandomized
observations challenge
interpretability

• ODE/CDER/FDA
• ACCF/AHA
• US FDA restricts marketing
No risk risk
• OSE/CDER/FDA
• ADA/EASD
• EMA suspends marketing
Rosiglitazone and Cardiovascular EventsDivergence of Opinion
Insufficient evidence to either incriminate or exonerate rosiglitazone
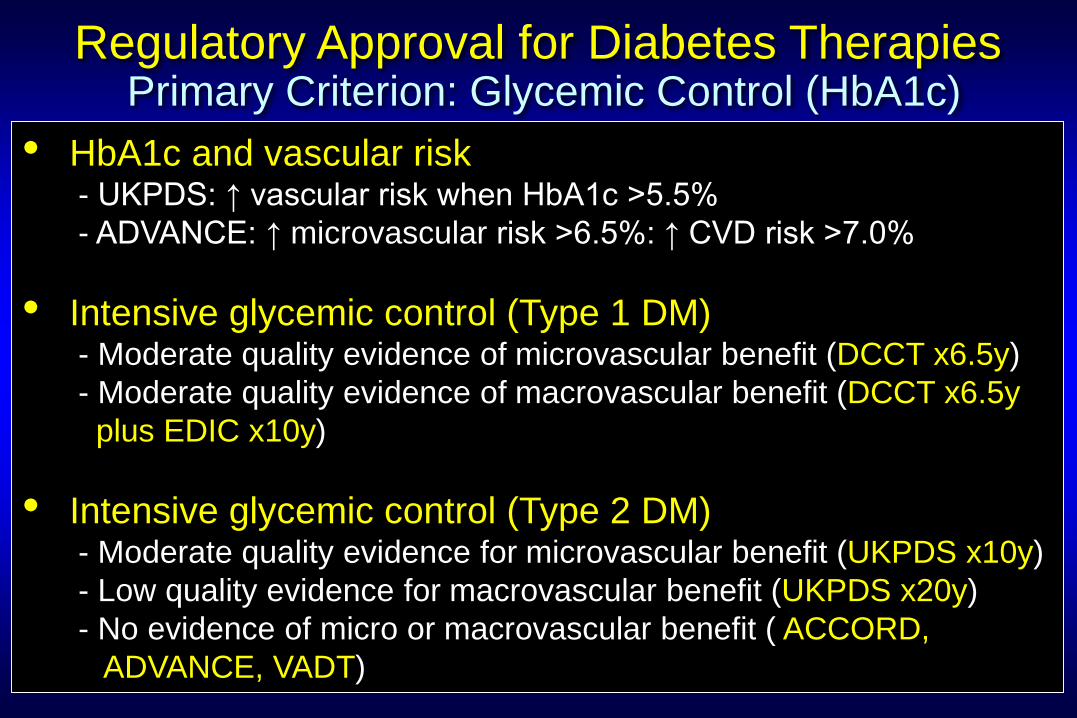
Regulatory Approval for Diabetes TherapiesPrimary Criterion: Glycemic Control (HbA1c)
• HbA1c and vascular risk- UKPDS: ↑ vascular risk when HbA1c >5.5%
- ADVANCE: ↑ microvascular risk >6.5%: ↑ CVD risk >7.0%
• Intensive glycemic control (Type 1 DM)- Moderate quality evidence of microvascular benefit (DCCT x6.5y)
- Moderate quality evidence of macrovascular benefit (DCCT x6.5y
plus EDIC x10y)
• Intensive glycemic control (Type 2 DM) - Moderate quality evidence for microvascular benefit (UKPDS x10y)
- Low quality evidence for macrovascular benefit (UKPDS x20y)
- No evidence of micro or macrovascular benefit ( ACCORD,
ADVANCE, VADT)

Treatment HbA1c Lipids Weight BS CHF CV event
Sulfonylureas ~1% +/- +/-
Metformin* ~1% LDL (10mg%) +/- +/- +/- ? (obese)
Acarbose ~0.5% +/- +/- ? +/- ?
Rosiglitazone** ~1% LDL, HDL TG +/- 2-fold ?
Pioglitazone** ~1% LDL, HDL,
TG +/- 1.5-fold ?
Nateglinide ~0.5% +/- +/- ? ?? ??
Repaglinide ~1% +/- +/- ?? ??
DPP-4 inhibitors ~1% ? +/- +/- ? No
GLP-1 agonists ~1% LDL, TG, HDL +/- ?? ??
SGLT2 inhibitor ~0.7% LDL, HDL,TG +/- ?? ?
Comparison of Oral Antidiabetic Therapies
Bolen et al, Systematic Review. Ann Int Med 2007;147:386-99; Ann Int Med 2011
*Lactic acidosis, GI side effects; ** fractures, macular edema (case reports), ? bladder cancer
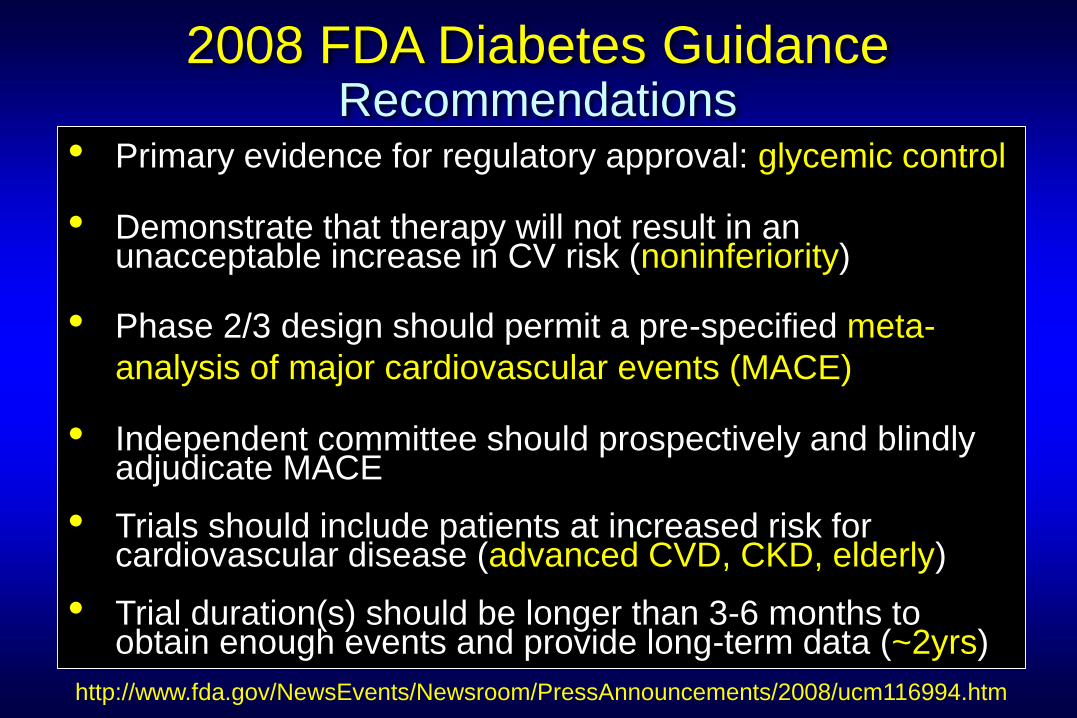
2008 FDA Diabetes GuidanceRecommendations
• Primary evidence for regulatory approval: glycemic control
• Demonstrate that therapy will not result in an unacceptable increase in CV risk (noninferiority)
• Phase 2/3 design should permit a pre-specified meta-
analysis of major cardiovascular events (MACE)
• Independent committee should prospectively and blindly adjudicate MACE
• Trials should include patients at increased risk for cardiovascular disease (advanced CVD, CKD, elderly)
• Trial duration(s) should be longer than 3-6 months to obtain enough events and provide long-term data (~2yrs)
http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2008/ucm116994.htm

2008 FDA CVOT GuidanceRuling Out Excess CV Risk: Two-Step Approach
Trial
phase
“Reassuring”
Point Estimate
0 1 2
Hazard ratio
No. of
Events
Patient
Exposure
Screening
(Premarketing, Stage 1)<1.262122 2500 x 2y
1.81.3
<0.91
<0.53
Premarketing 122 2500 x 2y
Pre- + post-
marketing*122 2500 x 2y
*Using O’Brien-Fleming adjustment
Goal is to rule out 6 excess events/1000 PY from a baseline of 20 events/1000 PY
Confirmatory
(Postmarketing, Stage 2) <1.11611 6000 x 5y
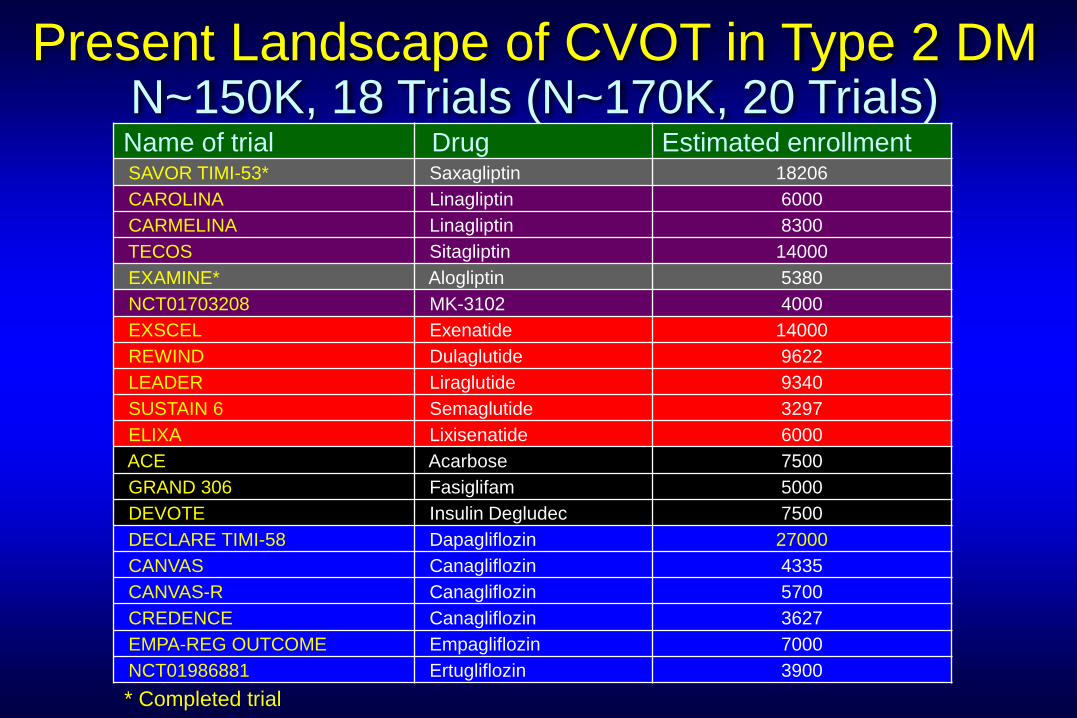
Present Landscape of CVOT in Type 2 DM N~150K, 18 Trials (N~170K, 20 Trials)Name of trial Drug Estimated enrollmentSAVOR TIMI-53* Saxagliptin 18206
CAROLINA Linagliptin 6000
CARMELINA Linagliptin 8300
TECOS Sitagliptin 14000
EXAMINE* Alogliptin 5380
NCT01703208 MK-3102 4000
EXSCEL Exenatide 14000
REWIND Dulaglutide 9622
LEADER Liraglutide 9340
SUSTAIN 6 Semaglutide 3297
ELIXA Lixisenatide 6000
ACE Acarbose 7500
GRAND 306 Fasiglifam 5000
DEVOTE Insulin Degludec 7500
DECLARE TIMI-58 Dapagliflozin 27000
CANVAS Canagliflozin 4335
CANVAS-R Canagliflozin 5700
CREDENCE Canagliflozin 3627
EMPA-REG OUTCOME Empagliflozin 7000
NCT01986881 Ertugliflozin 3900
* Completed trial

Alogliptin vs placebo
Benefit
• HbA1C (-0.36%)- HR 0.96 (-0.88% = HR 0.911)
• Weight loss (+0.06kg)
• BP lowering (neutral) 2
• Lipid profile (neutral) 3
Risk
• CHF signal (RR 1.19)4
1Diabetologia 2009, 2BMJ 2009, 3CTT Meta-analysis, Lancet 2010, 4NEJM 2013
Potential CV Effects of DPP-4 Inhibitors Modeling Projection Based on Intermediate Outcomes
Expected MACE benefit: 0.96 x 1.00 x 1.00 = 0.96
(4% risk reduction in MACE4 vs 19% risk increase in CHF4 )

Saxagliptin vs placebo
Benefit
• HbA1C (-0.20%)- HR 0.98 (-0.88% = HR 0.911)
• Weight loss (-0.50kg)- ? Impact on CV outcomes
• BP lowering (neutral) 2
• Lipid profile (neutral) 3
Risk
• CHF signal (RR 1.27)4
1Diabetologia 2009, 2BMJ 2009, 3CTT Meta-analysis, Lancet 2010, 4NEJM 2013
Potential CV Effects of DPP-4 Inhibitors Modeling Projection Based on Intermediate Outcomes
Expected MACE benefit: 0.98 x 1.00 x 1.00 = 0.98
(0% risk reduction in MACE4 vs 27% risk increase in CHF4 )

SGLT2 inhibitors
Benefit
• Effective glycemic control
(-0.66% HbA1c c/w placebo)
• hypoglycemia (-SU, insulin)
• Weight loss (-1.8Kg)
• BP lowering (-4.5 mmHg)
Risk
• Mycotic genital infection (OR 5.0)
• UTI (OR 1.4)
• Polyuria, nocturia, dysuria
• Volume depletion, thirst, ↑ Hct
• Dyslipidemia (↑ LDL, non-HDL)
SGLT2 Inhibitors for Treatment of Diabetes
Balancing Benefits and Risks
Uncertainty about CV & renal effects, bone health, malignancy
Adapted from Vasilakou et al, Ann Intern Med 2013;159;262-274
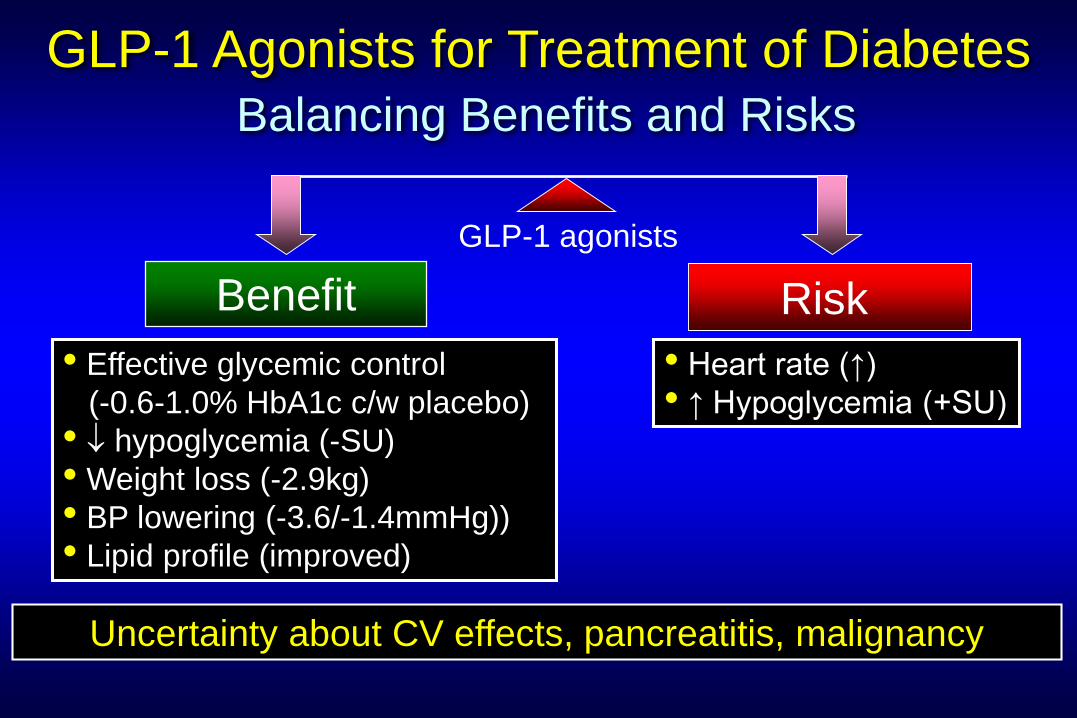
GLP-1 agonists
Benefit
• Effective glycemic control
(-0.6-1.0% HbA1c c/w placebo)
• hypoglycemia (-SU)
• Weight loss (-2.9kg)
• BP lowering (-3.6/-1.4mmHg))
• Lipid profile (improved)
Risk
• Heart rate (↑)
• ↑ Hypoglycemia (+SU)
GLP-1 Agonists for Treatment of Diabetes
Balancing Benefits and Risks
Uncertainty about CV effects, pancreatitis, malignancy
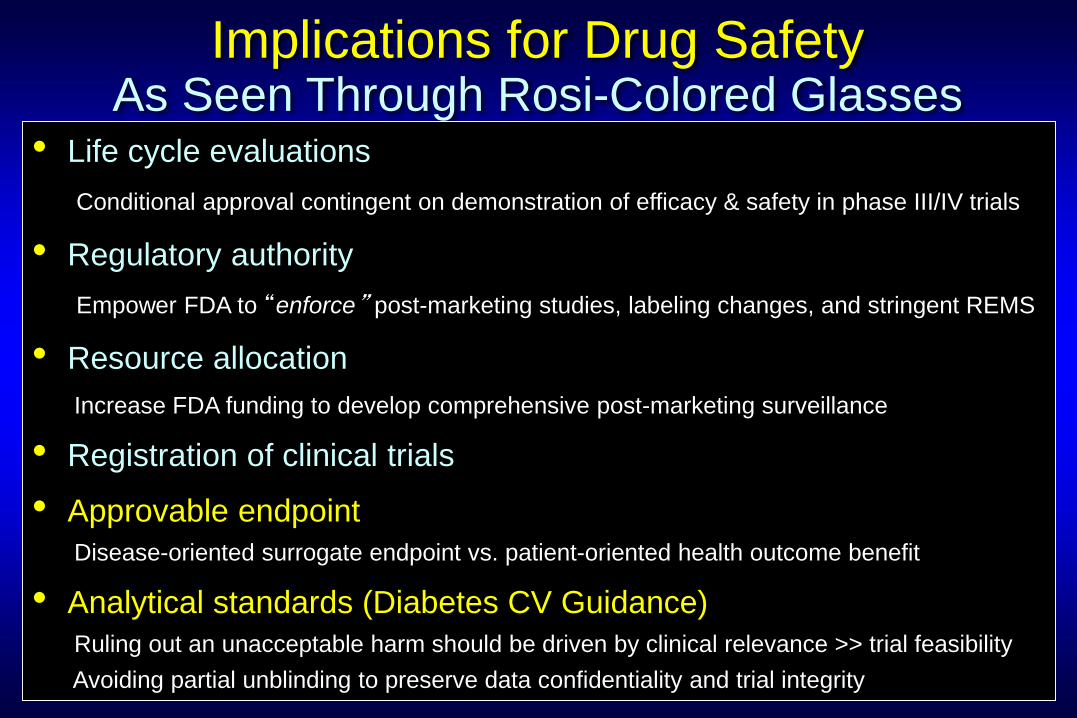
Implications for Drug SafetyAs Seen Through Rosi-Colored Glasses
• Life cycle evaluations
Conditional approval contingent on demonstration of efficacy & safety in phase III/IV trials
• Regulatory authority
Empower FDA to “enforce” post-marketing studies, labeling changes, and stringent REMS
• Resource allocation
Increase FDA funding to develop comprehensive post-marketing surveillance
• Registration of clinical trials
• Approvable endpoint
Disease-oriented surrogate endpoint vs. patient-oriented health outcome benefit
• Analytical standards (Diabetes CV Guidance)
Ruling out an unacceptable harm should be driven by clinical relevance >> trial feasibility
Avoiding partial unblinding to preserve data confidentiality and trial integrity

• Determine efficacy validly
• Detect risks prudently
• Do both in a timely and efficient way
Drug Approval ProcessKey Attributes
Is the drug development and approval
process meeting these goals?