cardiovascular physiology 1
TRANSCRIPT

09/04/2023 2
Cardiovascular system (CVS)
CVS consists of the heart and a
series of blood vessels (arteries,
veins and capillaries).

09/04/2023 3
CVS
Function: Homeostasis through:
– Generate blood pressure.
– Ensuring one way blood flow.
– Regulating blood supply.

09/04/2023 4
Parts of the circulatory system
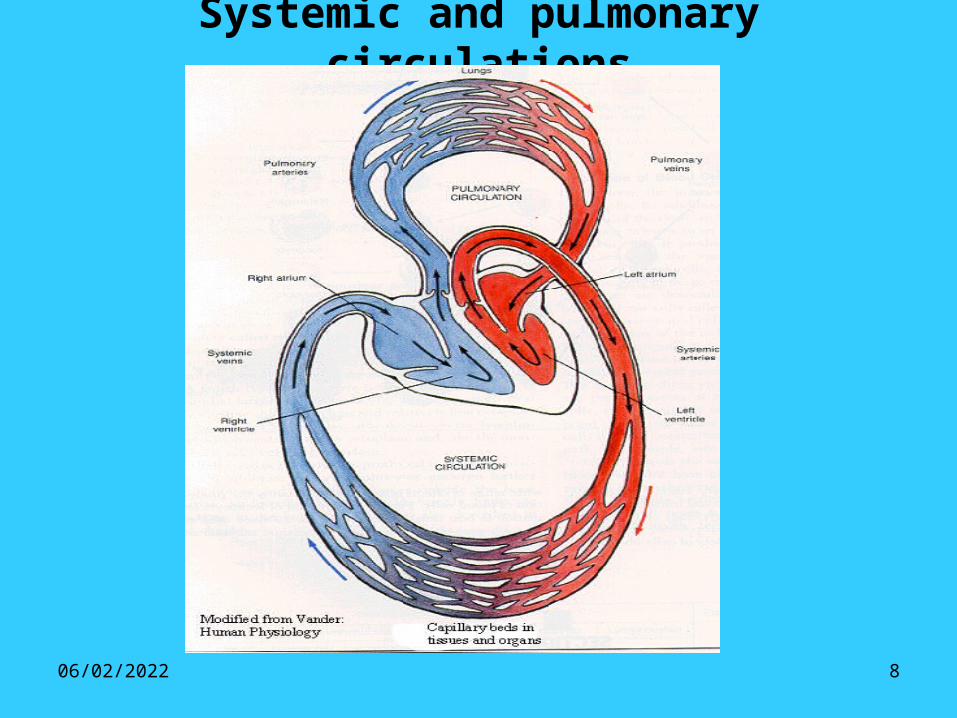
The circulatory system forms two circuits in
series with each other:-
- Systemic circulation (greater circulation)
- Pulmonary circulation (lesser circulation)

09/04/2023 5

09/04/2023 6
The Normal Heart and Regional
CirculationPulmonary Semilunar
ValveSuperior Vena Cava
Aorta
Left Pulmonary Artery
Right Pulmonary Artery
Right Pulmonary Veins
Inferior Vena Cava
Tricuspid Valve
Septum
Lungs
Left Atrium
Left Pulmonary
Veins
Bicuspid or Mitral Valve
Aortic Semilunar Valve

09/04/2023 7
Lungs
Brain
Veins (Flexible Compliant “Pipes”)
Arteries (Stiff Inflexible “Pipes”)
Liver
Stomach
Pancreas
Intestines
Kidneys
Skin
Muscle
Arterioles
Precapillary Sphincters
The Systemic
Circulation
09/04/2023 8
Systemic and pulmonary circulations

09/04/2023 9

09/04/2023 10

09/04/2023 11

09/04/2023 12
LocationHeart is located in thoracic cavity in the mediastinum,
between the lungs.
The heart lies obliquely in the mediastinum with its base directed posteriorly and slightly superiorly and the apex directed anteriorly and slightly inferiorly.
The apex is also directed to the left so that approximately 2/3 of the heart mass lies to the left of midline.
The base of the heart is deep to the sternum and extends to the 2nd intercostal space.
The apex is approximately 9 cm. to the left of the sternum and is deep to the fifth intercostal space.

09/04/2023 13
Pericardium Pericardium: a double layered closed sac that surrounds
the heart: 1- Fibrous pericardium: outer layer, tough, fibrous
connective tissue. Prevents over distension of the heart and anchors it within the mediastinum. Superiorly it is continuous with the connective tissue of the great vessels, and inferiorly attached to the surface of the diaphragm.
2- Serous pericardium: thin transparent inner layer.– Parietal pericardium: part of the serous pericardium
that lines the fibrous pericardium.– Visceral pericardium: part of the serous pericardium
that covers the heart surface.Pericardial cavity: between the parietal and visceral pericardium is filled with a thin layer of serous Pericardial fluid: reduces friction of the beating heart.

09/04/2023 14
Heart Wall
Epicardium: thin serous membrane of the outer surface of the heart. Also called the visceral pericardium
Myocardium: thick middle layer composed of cardiac muscle.
Endocardium: simple squamous epithelium over a layer of connective tissue, continuous with all blood vessels of the body.

09/04/2023 15
Heart Anatomy
• The heart is a strong muscular pump that contracts
and relaxes all life.
• It is the size of the fist of the hand.
• It is formed of 4 chambers:
Two thin walled low pressure reservoirs, the atria and
two thick walled pumping chambers, the ventricles.

09/04/2023 16
Functional anatomy of the heart

09/04/2023 17
Heart beat

09/04/2023 18
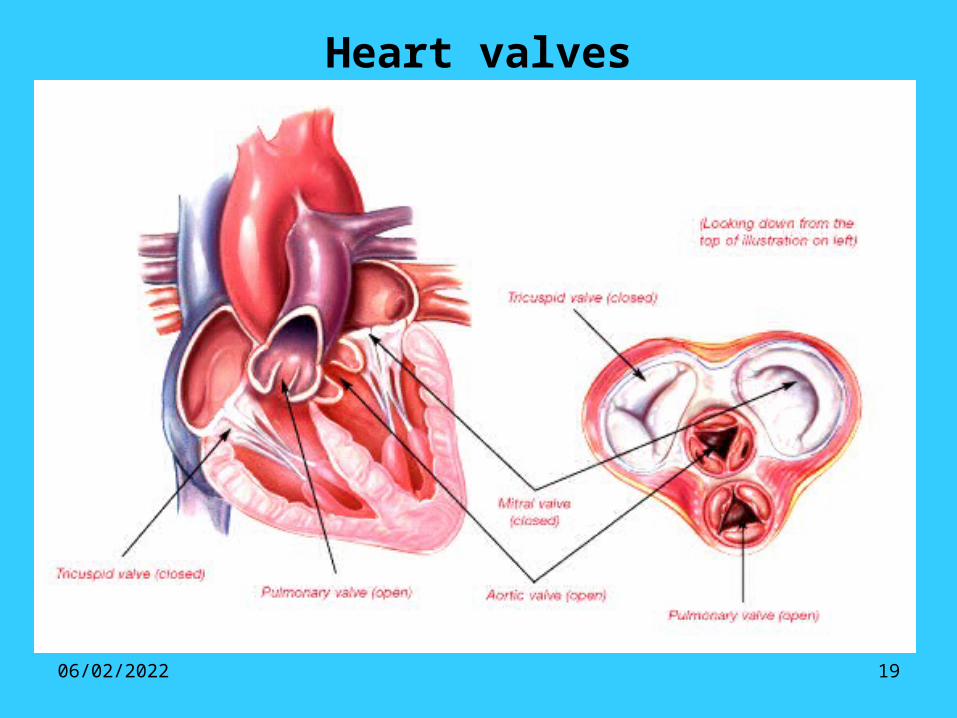
Heart valves • Tricuspid valve: 3 cusps, between the right atrium and
right ventricle. • Bicuspid valve: two cusps, between the left atrium and
left ventricle, also known as the mitral valve. • Semilunar valves: Consists of three pocket like
semilunar cusps, the free inner borders meet in the middle of the artery to block retrograde flow.
Aortic valve: between the left ventricle and the aorta.
Pulmonary valve: between the right ventricle and the pulmonary artery.
09/04/2023 19
Heart valves

09/04/2023 20
���A V and Semilunar Valves

09/04/2023 21
Innervations of heart
autonomic nerve supply:
1- Sympathetic: increase activity of whole heart.
(increase heart rate and contractility)
2- Parasympathetic: comes through vagus nerve and decrease
activity of atria only.
(decrease heart rate)

09/04/2023 22
Autonomic Innervations of the heart

09/04/2023 23
Mammalian Heart

09/04/2023 24

09/04/2023 25
THE CARDIAC MUSCLE• Cardiac muscle is formed of myocardial
muscle fibers which are elongated branched nucleated cells, the ends of which are joined together by intercalated discs, forming a network.
• The intercalated discs contain gap junctions which have low electric resistance and allow free diffusion of ions. Thus, excitation in one area spreads throughout the heart.

09/04/2023 26
• This permits the cardiac muscle to contract as a whole as if it is made of a single muscle cell or as a functional syncytium.
• The heart is composed of 2 functional syncytia: ATRIA AND VENTRICLES.

09/04/2023 27
THE CARDIAC MUSCLE

09/04/2023 28
GAP JUNCTIONS

09/04/2023 29
PROPRTIES OF CARDIAC MUSCLE
• 1- EXCITABILITY
• 2- CONTRACTILITY
• 3- RHYTHMICITY
• 4- CONDUCTIVITY

09/04/2023 30
1- EXCITABILITY• Definition: Excitability is the ability of
the cardiac muscle to respond to a stimulus by generating an action potential followed by a contraction.
• Cardiac muscle resting membrane potential and action potential differ in different parts of the heart.

09/04/2023 31
Cardiac Action Potentials

09/04/2023 32
THE A.P. OF THE VENTRICLES

09/04/2023 33
PHASES OF VENTRICULAR A.P.
- Phase 0: Initial rapid depolarization.
- Phase 1: Brief initial repolarization.
- Phase 2: Prolonged plateau.- Phase 3: Late rapid
repolarization.- Phase 4: Resting membrane
potential (-100 mv)

09/04/2023 34
IONIC BASIS OF VENTRICULAR ACTION POTENTIAL
• Phase 0: Initial rapid depolarization: due to Na+ inflow due to opening of fast Na+ channels.
• Phase 1: Brief initial repolarization: due to opening of transient K+ channels.
• Phase 2: Prolonged plateau: due to opening of slow Ca++ - Na+ channels.( A balance is created between influx of Na+ and Ca+ and outflux of K+)
• Phase 3: Late rapid repolarization: due to delayed opening of K+ channels.
• Phase 4: Resting membrane potential ( -100 mv)

09/04/2023 35

09/04/2023 36
LONG REFRACTORY PERIOD• Cardiac muscle action potential
differs from skeletal muscle action potential.
• Cardiac action potential is characterized by A LONG REFRACTORY PERIOD due to the plateau phase, during which the heart cannot be restimulated.
• The action potential results in a mechanical response: contraction (systole) followed by relaxation (diastole).

09/04/2023 37
Action Potential and Mechanical Response
Cardiac Muscle Skeletal Muscle

09/04/2023 38
NON TETANIZING PROPERTY• The cardiac muscle has a long
refractory period (due to plateau phase), which coincides with the whole period of systole.
• Thus the heart remains non excitable for the entire contraction phase.
• This ensures that the heart cannot go into a sustained state of contraction (tetanus) which could lead to stopping of circulation.

09/04/2023 39

09/04/2023 40
2- CONTRACTILITY• Definition: It is the ability of the cardiac muscle to
contract to pump blood.• The heart is a strong muscular pump that contracts and
relaxes all the time day and night, and its cessation means death.
• There are two types of muscle contraction: a- Isometric contraction: increase muscle tension without shortening (e.g. during early systole) b- Isotonic contraction: Tension is constant but muscle shortens and work is done (e.g. during late systole when blood is ejected)
09/04/2023 41
CONTRACTILITY (cont)• The cardiac contractility obeys two
laws:• ALL OR NONE LAW:
If other conditions are constant, the cardiac muscle either contracts maximally ( if the stimulus is adequate) or does not contract at all
( if the stimulus is inadequate)

09/04/2023 42
CONTRACTILITY (cont)• STARLING’s LAW:
[LENGTH-TENSION RELATIONSHIP]• The ability of the cardiac muscle to generate
force, is dependent on the initial length of the muscle prior to contraction, i.e. end diastolic volume (EDV).
• The greater the initial length of the muscle fibers, the greater the force of contraction (within limits).

09/04/2023 43
Application of STARLING LAW If the amount of blood
returning to the heart increases (i.e.↑venous return) this will stretch the cardiac muscle fibers, i.e. increase its length at end of diastole (↑↑EDV: end diastolic volume )
increase the force of contraction at systole increase stroke volume.
[ Thus, the heart will pump out whatever volume is delivered to it]

09/04/2023 44

09/04/2023 45
3- RHYTHMICITY• Definition: It is the ability of the cardiac
muscle to initiate its own regular impulses (rhythm), independent of any nerve supply.
• Cause: The cardiac muscle has a specialized excitatory conductive system, which have the property of auto rhythmicity.
• Rate of autorhythmicity:• SA Node: 70-80 beats/min• AV Node: 40-60 beats/min• Bundle of His: 30 beats /min• Purkinje fibers: 15 beats/min (incompatible
with life)

09/04/2023 46
Excitatory Conductive system

09/04/2023 47
PACEMAKER OF THE HEART• The area which determines the pace or rhythm of the
heart is called the pacemaker of the heart.• The SA Node is the pacemaker of the heart because:
1- it has the highest rhythm
2- and the whole heart obeys it.• If the SA Node is destroyed, the AV Node will be
pacemaker.• VAGAL TONE: It is the continuous impulses in the
vagus nerve which decrease the inherent high rhythm of the SA Node from 90-100/min to 70-80/min (the normal heart rate)

09/04/2023 48

09/04/2023 49
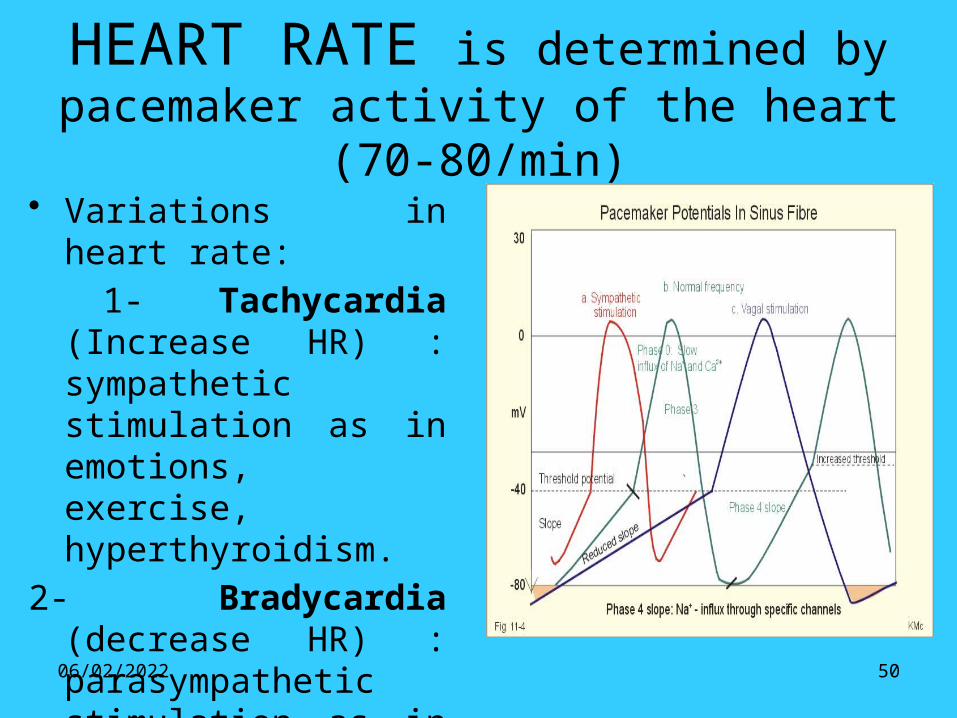
PACEMAKER POTENTIALPacemaker cells have unique electric
properties:• Prepotential: Unstable
membrane potential due to slow continuous leakage of Na+ ions into the myocardium leads to: spontaneous diastolic depolarization.
• After reaching firing level, the next action potential follows automatically.
• No plateau is seen.
09/04/2023 50
HEART RATE is determined by pacemaker activity of the heart (70-80/min)
• Variations in heart rate:
1- Tachycardia (Increase HR) : sympathetic stimulation as in emotions, exercise, hyperthyroidism.
2- Bradycardia (decrease HR) : parasympathetic stimulation as in sleep, hypothyroidism.

09/04/2023 51
4- CONDUCTIVITY• Definition: It is the ability of the cardiac
muscle to conduct or transmit an action potential over the whole heart along specialized conducting system having high conduction velocities.
• Velocity of conduction:• SA Node: 1 m/sec• AV Node: 0.05 m/sec• Bundle of His: 1 m/sec• Purkinje fibers: 4 m/sec

09/04/2023 52

09/04/2023 53
Conduction Velocity in heart
m/sec 1
m/sec 4
m/sec
m/sec 0.05
1

09/04/2023 54
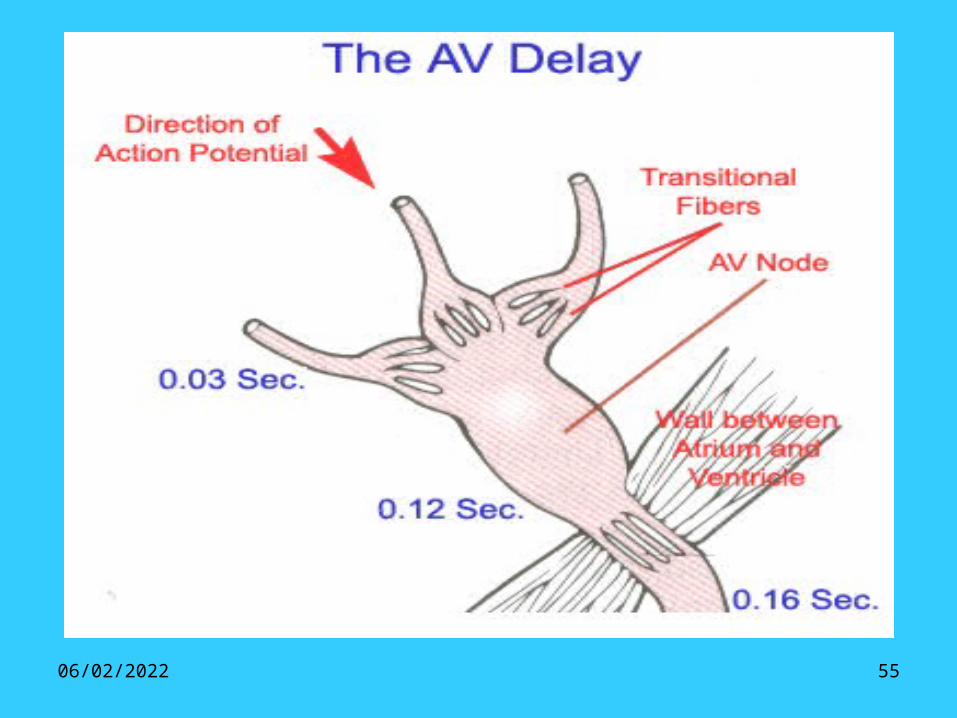
PROPAGATION OF CARDIAC IMPULSE
• Cardiac impulse is initiated by SA Node.• It spreads through atria in internodal tissue at a rapid
rate to reach AV Node.• The conduction velocity slows down in AV Node which
is known as AV Nodal delay. This delay is important as it gives time for proper ventricular filling.
• The wave then travels rapidly down the AV bundle, bundle branches and Purkinje fibers to all parts of the ventricles. The fastest conductivity in Purkinje fibers is important as it excites the whole ventricle as one unit leading to powerful ventricular contraction.
• Block in transmission of impulse is “heart block”
09/04/2023 55

09/04/2023 56
THE CARDIAC CYCLE• Definition: The cyclic events that occur in the
heart chambers during each beat.• As the normal heart rate is 70 beat/min, the
duration of each cardiac cycle is 60/70 = 0.8 sec• Each cardiac cycle includes: Atrial systole
Ventricular systole Diastole of whole heart.• Blood flow in the heart is determined by pressure
difference across the orifices of the heart which leads to opening and closure of valves.
• First and second heart sounds are due to closure of AV and semilunar valves respectively.

09/04/2023 57
STROKE VOLUME
• STROKE VOLUME: is the volume of blood ejected by each ventricle per beat.
= End diastolic volume - End systolic volume
= 120-50= 70 ml

09/04/2023 58
CARDIAC OUTPUT• Cardiac output is the volume of blood
ejected by each ventricle / min
= Stroke volume x Heart rate
= 70 x 70
= 5 liter/min

09/04/2023 59

09/04/2023 60
PHASES OF CARDIAC CYCLEI- SYSTOLE
• Atrial systole: [SA Node depolarization] The atria contract propelling the last 30% of its blood into
ventricles.• Ventricular Systole: [Depolarization of ventricles] 1- Isometric Contraction Phase: - Ventricular pressure>atrial pressureAV valves close. - Now ventricles contract as a closed chamber (all valves
are closed) - No change in volume but pressure increase.2- Ventricular Ejection Phase: - Ventricular pressure> aortic and pulmonary pressure
semilunar valves open. - Now blood gushes out of ventricles into aorta and pulmonary vessels

09/04/2023 61
PHASES OF CARDIAC CYCLEII- DIASTOLE
• Ventricular Diastole: [Repolarization of ventricles]
1- Isometric Relaxation Phase:
- When ventricular pressure < aortic and pulmonary artery pressure Semilunar valves close.
- Now ventricles relax as a closed chamber (with all valves closed)
- No change in volume but pressure decrease.
2- Ventricular Filling Phase:
- Ventricular pressure<atrial pressure AV valves open.
- Now ventricles start to fill with blood from atria.
- First 30% (rapid filling), mid 30% ( reduced filling or diastasis), last 30% (atrial systole)

09/04/2023 62

09/04/2023 63
SYSTOLE

09/04/2023 64
DIASTOLE

09/04/2023 65

09/04/2023 66

09/04/2023 67

09/04/2023 68

09/04/2023 69

09/04/2023 70
ECG

09/04/2023 71
ECG Recording

09/04/2023 72
ECG Intervals and Segments

09/04/2023 73
Normal ECG Record
09/04/2023 74
ECG Leads

09/04/2023 75
ECG LEADS

09/04/2023 76
09/04/2023 77

09/04/2023 78
Normal ECG Recording

09/04/2023 79

09/04/2023 80

09/04/2023 81

09/04/2023 82

09/04/2023 83
ECG Abnormalities

09/04/2023 84


09/04/2023 86
• CARDIAC MUSCLE CELLS• Elongated branching cells with one or two
centrally located nuclei. • Striated • Intercalated discs • Desmosomes • Gap Junctions • Autorhythmicity - cardiac muscle has the
ability to depolarize spontaneously. only 1% of the cells have this ability

09/04/2023 87
Cardiac muscle

09/04/2023 88
Intercalated discs

09/04/2023 89
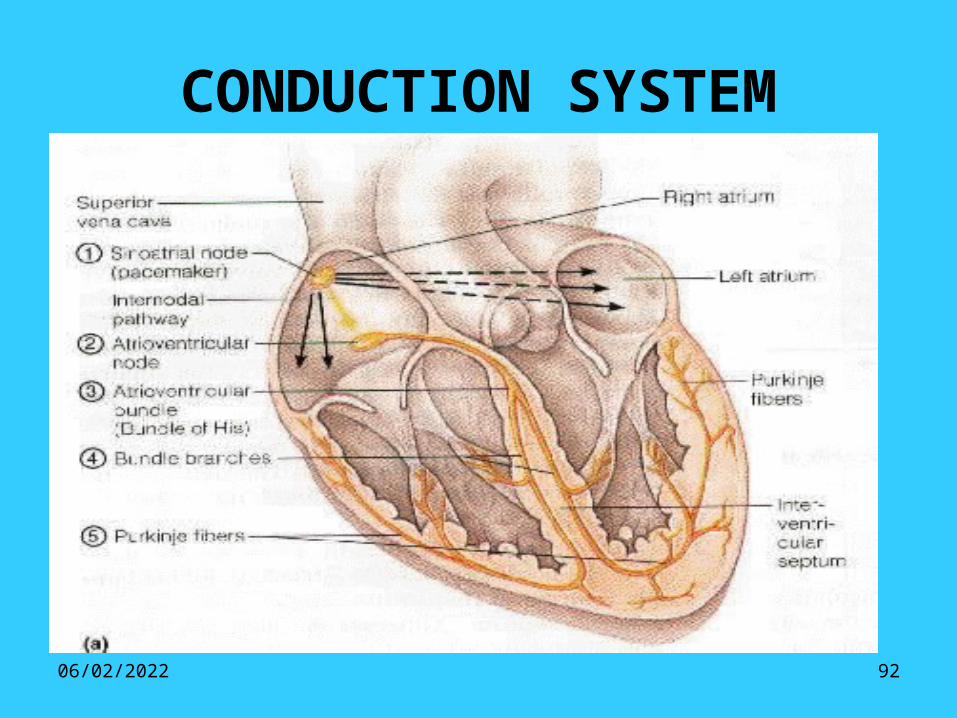
CONDUCTION SYSTEM• Sinoatrial node (SA Node): is medial to the
opening of the superior vena cava. • Action potentials originate here and travel
across the wall of the atrium to the atrioventricular node (AV Node) located medial to the right atrioventricular valve.
• Action potentials pass through the AV node and along the atrioventricular bundle, which extends from the AV node into the interventricular septum.

09/04/2023 90
• The AV bundle divides into right and left bundle branches, the action potential descends to the apex of the heart along the bundle branches.
• Action potentials are carried by Purkinje fibers from the bundle branches up along the ventricular walls.

09/04/2023 91
The cardiac conduction system
09/04/2023 92
CONDUCTION SYSTEM

09/04/2023 93
On the left, the action potential of a contractile cell. On the right is the action potential of an
autorhythmic cell

09/04/2023 94
Ionic changes in autorhythmic cells

09/04/2023 95
Ionic changes in ventricular muscle

09/04/2023 96
09/04/2023 97
Heart sounds

09/04/2023 98
Mitral Area
• located about the apex beat, which is usually in the fifth intercostal space.
• It is also called the apical, or the left ventricular area.
• The systolic murmur of Mitral Regurgitation and the diastolic murmurs of Mitral Stenosis and Increased Valvular Flow.

09/04/2023 99
Tricuspid Area
located at the lower left sternal border (LLSB).
The diastolic murmur of Tricuspid Stenosis.

09/04/2023 100
Pulmonary Area
• located in the second intercostal space at the left sternal border.
• The systolic murmur of Pulmonic Stenosis and the diastolic murmur of Pulmonic Regurgitation.

09/04/2023 101
Aortic Area
• located in the second intercostal space at the right sternal margin.
• The systolic murmurs of Aortic Stenosis and Increased Aortic Valve flow.

09/04/2023 102
Electrocardiography (ECG)• It is a recording of electrical activity of
the cardiac muscle from the surface of the skin of the thoracic cage where the body fluid act as a good conductor from cardiac muscle to electrodes placed on the skin..
• The electrical activity proceed the heart contraction.

09/04/2023 103
Basis of the ECG• When the excitation wave begins to spread in the
heart. • The surface of the cells in the heart depolarized and
becomes negative in relative to the surrounding region.
• Thus there are two areas in the heart one excited and the other is notexcited, and both of them act as two terminals of the battery, one negative and the other is positive.
• This generates an electrical field throughout the body fluid.

09/04/2023 104
Basis of the ECG
• The electrical activity of the heart starts at the SAN then spread to the both atria and then to the both ventricles and the surrounding tissues.
• ECG is used to evaluate some heart problems such as arrhythmias, ischemia, necrosis and hypertrophy of the heart.

09/04/2023 105
• The used apparatus for recording called electrocardiograph which has an electrode placed on the skin and the recording obtained from a specific point called (a lead), the standard ECG has 12 different leads that record the same electric events but from different views.
• The leads are of 3 types:-–Bipolar limb leads.–Unipolar leads.–Augmented unipolar leads.

09/04/2023 106
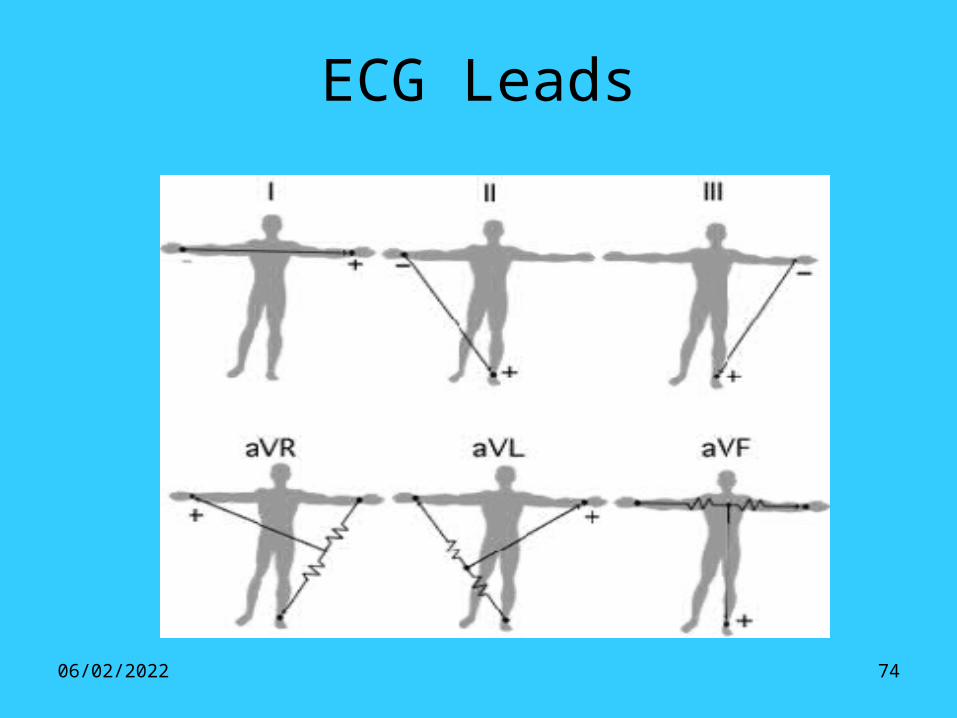
Bipolar limb leads:• These leads measure the potential difference
between 2 limbs by applying active electrodes from ECG apparatus anywhere on the limbs (wrist or ankle).
3 different leads are recorded:- • Lead I: It measures the potential difference between
the left arm (LA) and right arm (RA).• Lead II: It measures the potential difference
between the left (LL) and right arm (RA). • Lead III: It measures the potential difference
between the left leg (LL) and left arm (LA).

09/04/2023 107
Unipolar leads:• These measure the absolute (actual)
potential at a certain point. • This is done by applying one electrode
from electrocardiograph to the desired point while the other electrode is made indifference (-ve), this means that the unipolar leads measures the potential difference between active potential and zero potential.

09/04/2023 108
Unipolar limb leads:
It measures the absolute potential at right arm (VR), left arm (VL) and left leg (VF).
Unipolar (V) leads:
It measures the absolute potential at 6 standard points on the anterior chest wall (V1, V2, V3, V4, V5 andV6).

09/04/2023 109
V1: At right margin of the sternum in the 4th intercostals space.
V2: At left margin of the sternum in the 4th intercostals space.
V3: Midway between V2 and V4.V4: At the left midclavicular line in the 5th
intercostals space.V5: At the left anterior axillary line at the 5th
intercostals space.V6: At the left mid axillary line at the 5th
intercostals space.

09/04/2023 110
Augmented Unipolar limb Leads:
• In this case there is magnification of amplitudes by about 50%.
• The leads called aVR, aVL and aVF, where a= augmented.
• The augmented leads are easier to interpret and recorded by ECG machines.

09/04/2023 111
Normal ECG• Normal ECG consists of 5 main waves called
P Q R S T waves. • These waves are separated by segments. • Each waves start and ends at the isoelectric line.• The QRS waves from a complex called QRS
complex. • This normal ECG can be recorded in aVl, aVF,
V5 and V6 because the exploring electrode faces the left ventricle.

09/04/2023 112
ECG

09/04/2023 113
ECG Components Diagram
09/04/2023 114
The P wave• Represents atrial activation (atrial
depolarization).• Small +ve wave.• Its amplitude 0.1 (up to 0.25) mv.• Its duration 0.08 (up t0 0.11)
seconds.

09/04/2023 115
Abnormalities of P- wave• In left atrial hypertrophy (due to mitral
stenosis), the P wave become broad and notched.
• In right atrial hypertrophy (due to pulmonary hypertension) P wave become tall.
• In AV nodal rhythm: P wave inverted.• In atrial fibrillation: P wave disappear.

09/04/2023 116
The QRS complex• Represents ventricular activation (depolarization).• The QRS duration is the duration of ventricular
activation (0.06-0.1). • Q wave: is –ve wave due to depolarization of
interventricular septum.• R wave: is a large +ve wave, its amplitude is 10
mm (1 mv), caused by depolarization of the apex and ventricular wall, it is + ve wave.
• S wave: is a –ve wave, caused by depolarization of the posterobasal part of the left ventricle and pulmonary conus.

09/04/2023 117
Abnormalities of QRS complex• In ventricular hypertrophy.• Infarction.• Extrasystole.• Bundle branch block.• Electrolyte disturbance.
09/04/2023 118
T wave• It is a +ve large blunt wave.• Represents ventricular activation (ventricular
repolarization).• Its amplitude 0.2 (up to 0.4) mv.• Its duration 0.2 (up to 0.25) second.

09/04/2023 119
Abnormalities of T wave
• Inverted:• Myocardial infraction.• Ventricular hypertrophy.• Extrasystole.• Bundle branch block.• Digitals overdosage.
• Increase amplitude:• Sympathetic overactivity.• Muscular exercise.• Hyperkalmia.

09/04/2023 120
ECG Intervals and Segments

09/04/2023 121
P-R interval• - From the start of P-wave to the start of R wave.- Its range from 0.12 to 0.21 second.- It means conduction of cardiac impulse through
A-V node.Abnormalities of P-R interval:• 1- Prolonged:• - First degree of heart block.• - Increased vagal tone.• 2 - Shortened:• - A- V nodal rhythm.• - Sympathetic overactivity.• - Wolff- Parkinson- white syndrome.

09/04/2023 122
Q-T intervalStart from the onset of Q wave to the end of T wave.• Its duration 0.36- 0.24 second.• It is called electrical systole of the heart.T- Q interval:• Start from the end of the T wave to the onset of the
next Q wave.• It is called electrical diastole. • Its duration is about 0-4 second.Abnormalities of T-Q interval: • It is shortened before atrial and ventricular
extrasystole.• It is prolonged after ventricular extrasystole.

09/04/2023 123
S-T segment- Start from the end of S wave to start of T
wave.• Its duration is about 0.12.
Abnormalities of S-T segment:• Its deviation upward or downward indicates
myocardial damage.

09/04/2023 124
ECG changes in myocardial infraction

09/04/2023 125
Intima
Adventitia
Media
The Normal Heart - Coronary Artery Anatomy
Left Main CA
Circumflex
Left Anterior Descending CA
Right CA
Marginal Branch
Layers of the Arterial Wall
Intima composed of endothelial cells

09/04/2023 126
End Diastolic Volume (EDV)Volume at the end of diastole(end of ventricular filling)
End Systolic Volume (ESV)Volume at the end of systole(end of ventricular contraction)
Stroke Volume (SV) = EDV - ESV
Ejection Fraction (EF) = SV EDV
Left Ventricular Volumes - Definitions
Left ventricular norm for EF: 62%
Ejection Fraction is the best indicator of heart performance and disease prognosis

09/04/2023 127
Changes in Ventricular Volumes with Exercise
Rest Peak Exercise
600 - 750300
LVEDV
LVESV
10
20
30
40
80
70
60
50
100
90
120
110
SV
Kg meters / min
Left Ventricular Volume (ml)
LVEDV - LVESV = SV

09/04/2023 128
• Cardiac Output: (Q) = HR X SV
• Cardiac Index = Q / body surface area
• Preload: (EDV) volume of the left ventricle at the end of diastole (dependent on venous return & stretch of the cardiac muscle
cells)
• Afterload: resistance to ventricular emptying during systole (the amount of pressure the left ventricle must generate to
squeeze blood into the aorta)
• Frank Starling Law of the Heart: the heart will contract with greater force when preload (EDV) is increased
• Myocardial Contractility: the squeezing contractile force that the heart can develop at a given preload• regulated by:• sympathetic nerve activity (most influential)• catecholamines (epinephrine norepinephrine)• amount of contractile mass • drugs
Definitions

09/04/2023 129
Starlings Law of the Heart and Contractility
SV
(left ventricular performance)
Preload
(venous return)
u contractility
normal contractility
d contractility(heart failure)

09/04/2023 130
u Contractility related to :b sympathetic adrenergic nervescatecholamines: - epinephrine
- norepinephrine
drugs: - digitalis- sympathomimetics
d Contractility related to:- loss of contractile mass (may be due to heart attack)
- myocardial muscle disease (cardiomyopathy)
- drugs (anesthetics, barbiturates)
Influences on Myocardial Contractility

09/04/2023 131
• Arteriovenous Oxygen Difference (AVO2D) the difference in oxygen content between arterial and venous blood • measured in ml% - ml O2 / 100 ml blood
• Oxygen Consumption (VO2) - the rate at which oxygen can be used in energy production and metabolism
• “absolute” measures: L O2 / min , ml O2 / min• “relative” measures: ml O2 / kg body wt. / min• Fick equation: VO2 = Q X AVO2D
• Maximum Oxygen Consumption (VO2max) maximum rate at which a person can take in and utilize oxygen to create usable energy• defined as plateau of consumption rate increase• often estimated with VO2peak
• Myocardial Oxygen Consumption VO2 of the heart muscle (myocardium)• "estimated" by RPP: HR X SBP
• Functional Aerobic Impairment:
predicted VO2max - attained VO2max
predicted VO2max
mild 27% - 40%moderate 41% - 54%marked 55% - 68%severe > 69%
Definitions

09/04/2023 132
• Systolic Blood Pressure (SBP) pressure measured in brachial artery during systole (ventricular emptying and ventricular contraction period)
• Diastolic Blood Pressure (DBP) pressure measured in brachial artery during diastole (ventricular filling and ventricular
relaxation)
• Mean Arterial Pressure (MAP) "average" pressure throughout the cardiac cycle against the walls of the proximal systemic
arteries (aorta)• estimated as: .33(SBP - DBP) + DBP
• Total Peripheral Resistance (TPR) - the sum of all forces that oppose blood flow• length of vasculature (L)
• blood viscosity (V)
• vessel radius (r)
Definitions
TPR = ( 8 ) ( V ) ( L )
( p ) ( r 4 )

09/04/2023 133
Cardiovascular Hemodynamic Basics
Flow (Q) Pressure (MAP) P aorta – P vena cava
= = Resistance (TPR) (8) (V) (L)
() (r 4)
Flow (Q) = () (Pa – Pv) (r 4)
(8) (V) (L)
V = viscosity of fluid (blood) flowing through the pipe L = length of pipe (blood vessel) r = radius of the pipe (blood vessel) Pa = aortic pressure Pv = venous pressure
Normally Resting Q is about 5 - 6 liters / minute

09/04/2023 134
• Minute Ventilation (VE) - amount of air passing through the lungs in one minute
• Dyspnea - breathing difficulty
• Respiratory Exchange Ratio - amount of CO2 expired by the lungs divided by the amount of O2 extracted from the air in the lungs (VCO2 / VO2 ).
RER = .7 r 100% fat 0% carbRER = .85 r 50% fat 50% carbRER = 1.0 r 0% fat 100% carb
Respiratory Physiology - Definitions

09/04/2023 135
Neurophysiology - Definitions & ConceptsAfferent - sensory nerves - going toward spinal column
Efferent - effector nerves - going away from spinal column
Adrenergic Receptor Types
a1 stimulation r constriction of:
blood vessels visceral sphinctersbronchioles bladder
a2 stimulation:vasodilatation bronchiole constriction
b1 stimulation:u HR and contractility u renin secretion
b2 stimulation:vasodilatation bronchiole dilationurinary tract relaxationrelaxation of visceral smooth muscle

09/04/2023 136
Smooth Muscle Arteriole
Anastomosis (Shunt)
Precaillary Sphincter
True Capillary With Single
Layer of Endothelium
Metarteriole
Venule
Microcirculatory Anatomy – a Capillary Bed

09/04/2023 137
Development of the Driving Pressure in the Human Cardiovascular System
Arterial Pressure(mm Hg)
Central Venous Pressure(mm Hg)
Cardiac Output (Q)(Liters / min)
1 5
0
7
77
26
102100
7 6 2
0
Mean CirculatoryFilling Pressure
Normal RestingCardiac Output
Normal Resting Pressure Driving the Blood from Left Ventricle to Vena Cava:102 - 2 = 100 mmHg

09/04/2023 138
RA
RV
LUNGS LA
LV
AORTA
ARTERIOLES
SYSTEMIC ARTERIES
VEINS (CAPACITANCE VESSELS)
(100)
(92)
(40)
low compliance
13% of blood volume
high compliance
64% of blood volume
PO2 = 40 PCO2 = 46
(0)
(2)
PO2 = 100 PCO2 = 40
PO2 = 160 PCO2 = .3
CAPILLARYBEDS
7% of blood volume
9% of blood volume
(7)
(13) (3)
Ohms Law: Flow (Q) = upstream pressure – downstream pressure resistance
Systemic Circulation = 100 mmHg – 0 mmHg = 100 ml / sec = 6 liters / min Flow (Q) 1 mmHg sec / ml
The “Closed” Cardiovascular Hemodynamic System
Mean arterial pressures in red
(20)

09/04/2023 139
Sites of Cardiorespiratory
Control

09/04/2023 140
• Heart Rate – CNS (medulla) and neurohormone regulation
• Parasympathetic vagus control (Neurotransmitter: acetlycholine)
• Vagal control dominant at rest – withdrawn during exercise
• Sympathetic cardio–acceleration (Neurotransmitter: E and NE)
• Baroreceptor influences
• Sympathetic discharge indirectly proportional to firing rate
• Parasympathetics are directly proportional to firing rate
• d pressure r d receptor firing r u sympathetics r u HR
• u pressure r u receptor firing r u parasympath. r d HR
• Chemoreceptor influences
• Main function: protect brain from poor perfusion
• u O2 or d CO2 r u parasympathetic discharge r d HR
• d O2 or u CO2 r d pH r pressor area stimulation r u HR
Cardiorespiratory Control

09/04/2023 141
Stroke Volume – regulated by Frank Starling mechanism
• u venous return r u EDV r u stroke volume
Cardiac Output (Q) – main determinant: body O2 needs • Autoregulated by intrinsic changes in preload, & SV
• u afterload r initial d in Q r u EDV r u SV back to normal
• u venous return r u preload r u SV
• Autoregulated by extrinsic hormonal influences
• Norepinephrine release r u HR and SV
Cardiorespiratory Control
09/04/2023 142
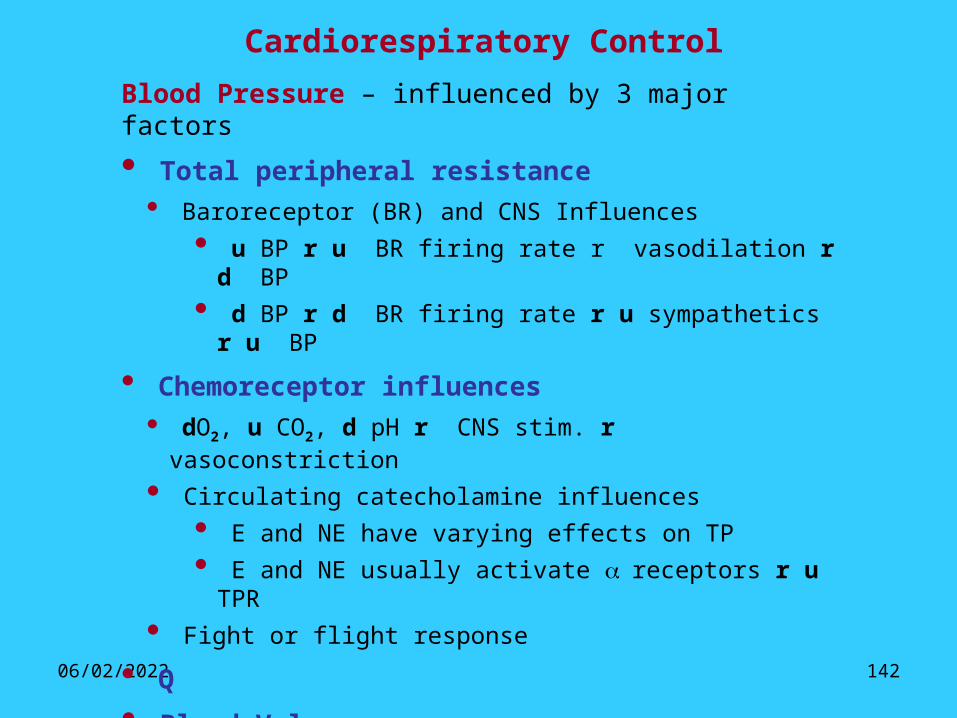
Cardiorespiratory Control
Blood Pressure – influenced by 3 major factors
• Total peripheral resistance
• Baroreceptor (BR) and CNS Influences
• u BP r u BR firing rate r vasodilation r d BP
• d BP r d BR firing rate r u sympathetics r u BP
• Chemoreceptor influences
• dO2, u CO2, d pH r CNS stim. r vasoconstriction
• Circulating catecholamine influences
• E and NE have varying effects on TP
• E and NE usually activate a receptors r u TPR
• Fight or flight response
• Q
• Blood Volume• Renin – Angiotensin system

09/04/2023 143
HypotensionHypovolemia
renal perfusion
ECF volum e
aldosterone
angiotensin I
renin
angiotensin II
H O reabsorbed2
ADH (vasopressin)sym pathetic tone
NaCl delivery to m acula densa cells
afferent arteriolarstretch in JG cells
renin
GFR
BLOOD PRESSURE(vasoconstriction)
thirst (thirst is m ore strongly regulated by osm otic
receptors in hypothalam us)
Na reabsorption(and K excretion)
+
+
neg feedback
neg feedback
m essangial cell contraction
Renin - Angiotensin System of Body Fluid Balance and other Body Fluid Regulation Mechanisms
stretch receptor activation in atria, aorta, and carotid sinuses

09/04/2023 144
Dehydration
• Dehydration: the loss of body water and associated electrolytes
• Causes: • Gastroenteritis (viral / bacterial infection r vomiting & diarrhea) most common
• Diseases: yellow fever, cholera,
• Excessive alcohol consumption
• Most liquors have Congeners which are toxins….they must be removed
• The clearer & better quality your liquor (vodka & gin) the less congeners
• more distillation cycles r better quality
• This removal is done by the liver (liver glucose is broken down r lethargy)
• The excess fluid is flushed out by the kidneys (u water usage r dehydration)
• Prolonged exercise without fluid replacement (heat exhaustion & heat stroke risk)
• Diabetes: hyperglycemia r u glucose excretion r u water loss r dehydration
• Shock: blood loss due to some hypotensive state
• Gastrointestinal blood loss: bleeding from ulcers or colorectal cancer
09/04/2023 145
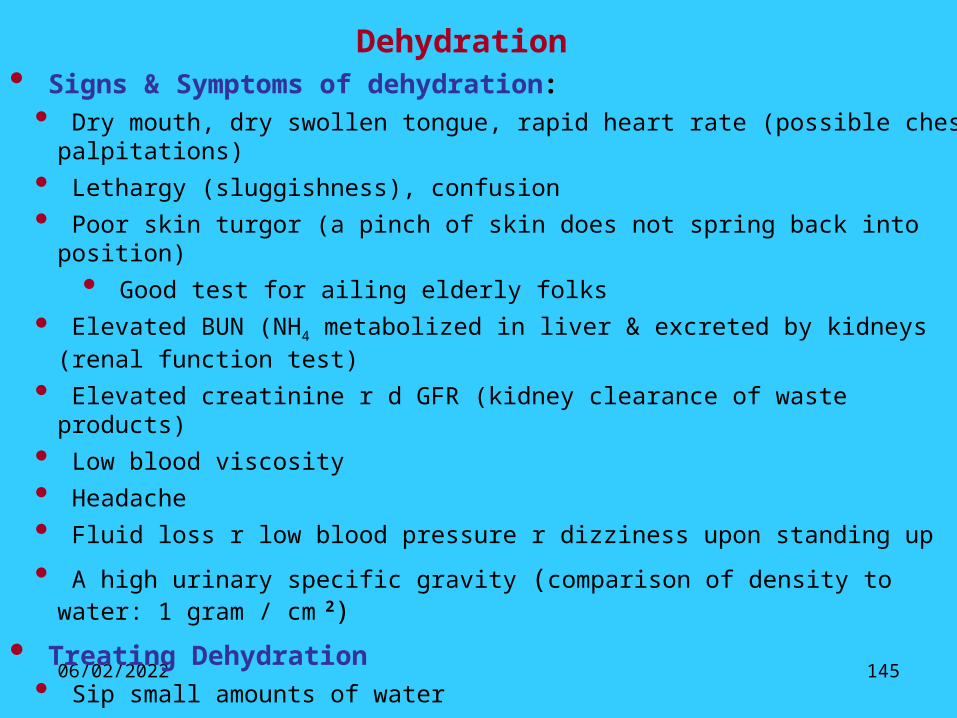
Dehydration• Signs & Symptoms of dehydration: • Dry mouth, dry swollen tongue, rapid heart rate (possible chest palpitations)
• Lethargy (sluggishness), confusion
• Poor skin turgor (a pinch of skin does not spring back into position)
• Good test for ailing elderly folks
• Elevated BUN (NH4 metabolized in liver & excreted by kidneys (renal function test)
• Elevated creatinine r d GFR (kidney clearance of waste products)
• Low blood viscosity
• Headache
• Fluid loss r low blood pressure r dizziness upon standing up
• A high urinary specific gravity (comparison of density to water: 1 gram / cm 2)
• Treating Dehydration• Sip small amounts of water
• Drink carbohydrate / electrolyte solutions: Gatorade, Pedialyte.etc
• If core body temperature > 104 0 + d BP or u HR r consider IV fluid replacement
09/04/2023 146
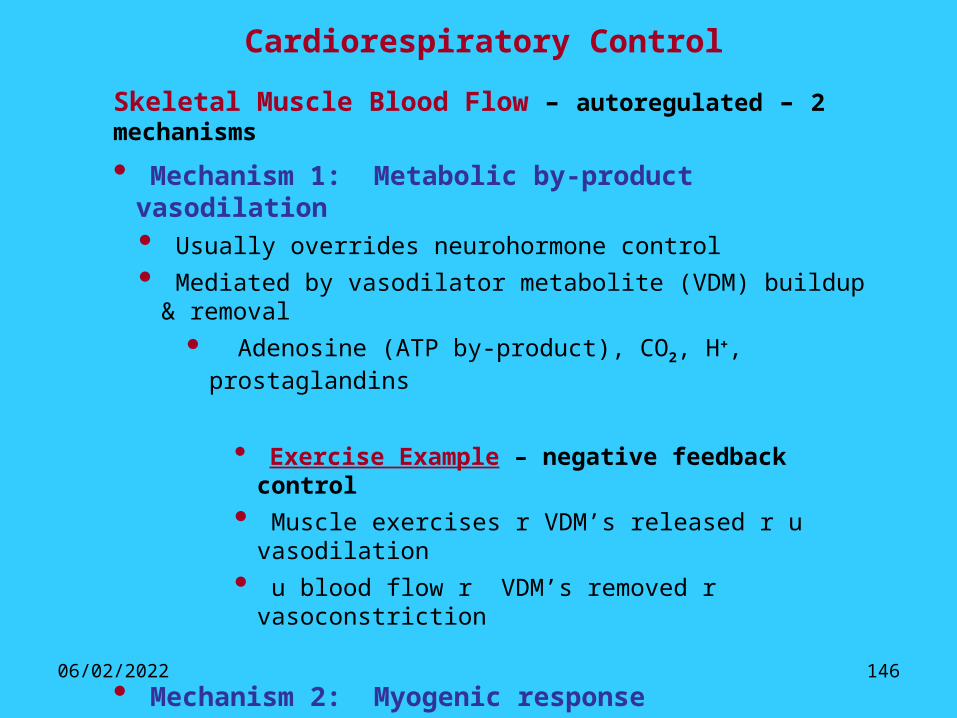
Skeletal Muscle Blood Flow – autoregulated – 2 mechanisms
• Mechanism 1: Metabolic by-product vasodilation• Usually overrides neurohormone control
• Mediated by vasodilator metabolite (VDM) buildup & removal
• Adenosine (ATP by-product), CO2, H+, prostaglandins
• Exercise Example – negative feedback control
• Muscle exercises r VDM’s released r u vasodilation
• u blood flow r VDM’s removed r vasoconstriction
• Mechanism 2: Myogenic response• Involves stretch activated Ca++ channels
• u blood flow r vessel stretch r channel activation
• u [Ca++ ] in smooth muscle r vasoconstriction r d flow
Cardiorespiratory Control

09/04/2023 147
Cardiorespiratory Control
Exercise Systemic Blood Flow: Autonomic influences• Sympathetic outflow & circulating catecholamines• a activation r vasoconstriction in non - exercising tissue
• Redistribution of blood flow during maximal exercise - NC in brain blood flow - 500 ml/min u to heart
- 11,300 ml/min u to muscle - 400 ml/min u to skin
- 500 ml/min d to kidneys - 800 ml/min d to viscera
- 200 ml/min d to various other parts of the body

09/04/2023 148
Respiration: VE = Tidal Volume X Respiratory Rate
• Controlled via the medulla respiratory center
• Peripheral chemoreceptors – not a big influence• u blood CO2 content r receptor activation r u VE
• d blood O2 content r receptor activation r u VE
• Central chemoreceptors – dominant influence• u blood CO2 & lactate r receptor activation r u VE
• PaCO2 r u HCO3¯ + H+ r H+ activates receptor r u VE
• Respiratory control during exercise – no consensus• u venous return r mechanoreceptor activation r u VE
• proprioceptor activation r u VE
• intrapulmonary receptor activation r u VE
• Minute ventilation control during exercise• Low exercise intensity: VE u by both u TV and u RR
• High exercise intensity: VE u by u RR only
Cardiorespiratory Control

09/04/2023 149
Acute Responses to Aerobic Exercise• Oxygen Consumption (VO2)
• u VO2 in direct proportion to u workload (power requirement of exercise)
• Expressed in both relative and absolute terms
• Relative: ml O2/kg/min Absolute: ml/min or L/min
• average VO2max for 40 year old male 37 ml/kg/min
• Oxygen consumption linked to caloric expenditure (1 liter of O2 consumed = 5 kcal)
• Heart Rate• u up to 3 times resting value at peak exercise (d time spent in diastole)
180
160
140
100
HeartRate
1.0 2.0 3.0Oxygen Uptake (L / min)
50 150 250
Workloads (Watts)
HR – VO2
relationship is
linear until about
90% VO2max

09/04/2023 150
• Stroke Volume• u up to 1.5 resting value at peak exercise
• increase levels off at 40% - 50% VO2 max• u in venous return r u EDV (Starling mechanism)• d ESV eluding to an u in myocardial contractility• u ejection fraction rest: 58% max exercise: 83%
• Cardiac Output (Q)• u up to 4 times resting value at peak exercise (u is rapid at onset, then levels off)• u Q r u venous return
• Venous return mediated by and related to:• sympathetic venoconstriction• muscle pump• u inspiration r d thoracic pressure
• blood flows to an area of reduced pressure• u inspiration r u abdominal pressure
• contraction of abdominal muscles • squeezing of abdominal veins
StrokeVolume(ml/beat)
120
110
70
25% 50% 75%Percentage of VO2 max
Acute Responses to Aerobic Exercise

09/04/2023 151
• Arteriovenous oxygen difference• Difference in [O2] between arterial and mixed venous blood• Illustrated by the oxyhemoglobin desaturation curve• u approximately 3 fold from rest to max exercise• at rest, about 25% of arterial O2 is extracted
• at peak exercise 85% of arterial O2 is extracted
• Blood Pressures and Resistance to Flow• SBP: u - failure to u signifies heart failure• DBP: slight u or slight d or NC• MAP: slight u • TPR: d - mainly due to vasodilation in exercising muscle
• Coronary (Myocardial) Blood Flow• 4.5% of Q goes to myocardium at rest and at peak exercise
• this increase is due to u MAP and CA vasodilation
• Blood Flow to the Skin• u as exercise duration u to allow for heat dissipation• d at max exercise to meet exercising muscle demands
• u during exercise recovery, again for heat dissipation
Acute Responses to Aerobic Exercise

09/04/2023 152
• Minute Ventilation• resting average: 6 Liters/min• peak exercise average: 175 Liters/min• respiratory rate: resting 12-18 peak exercise: 45-60• tidal volume: resting .5 liters peak exercise: 2.25 Liters
• Plasma Volume• blood plasma u in the interstitum of exercising muscle• fluid shift results in a 5% u in the hemoconcentration• blood viscosity increases
Acute Responses to Aerobic Exercise

09/04/2023 153
Untrained or people with certain cardiorespiratory diseases will have larger DEBTS and DEFICITS
Oxygen DEBT & Oxygen DEFICIT
Oxygen Debt(EPEOC)
Oxygen Deficit“Steady State”VO2
VO2
Rest
Onset TerminationEXERCISE TIMEAT CONSTANT WORKLOAD
Oxygen Debt and Deficit
Oxygen Deficit due to:• delay in time for aerobic ATP production to supply energy
Oxygen Debt due to:• resynthesis of high energy pohosphates (CP, ATP)• replace oxygen stores• lactate conversion to glucose (gluconeogenesis)• u HR, respiration, catecholamines, body temperature

09/04/2023 154
V O 2
VCO 2VO 2
V E
HCO 3
-
pH
m ax
P CO P COA 2 a 2&
P Oa 2
P OA 2
Increasing workload
OBLA Respiratory Compensation(hyperventilation)
No Change inVE
VCO2
Ventilatory and Metabolic Changes During
Exercise

09/04/2023 155
• RestingNC NC
VO2 = HR x SV x AVO2diff
due to: due to: u time in diastole u preload
d afterloadu ventricle sizeu blood volume
• Submax Workload (measured at same pre-training workload)
NC NC VO2 = HR x SV x AVO2diff
note: a d in afterload (mentioned above) accompanied by a d in HR response translates into
a d myocardial VO2 at rest or at any workload
• Max Workload (measured at peak exercise) NC
VO2 = HR x SV x AVO2diff
some studies show a slight decrease
Effects of Exercise Training on the Components of the Fick Relationship

09/04/2023 156
• Mean Arterial Pressure• NC at rest or during exercise
• Systolic and Diastolic Blood Pressure• usually NC at rest or during exercise• possible d at submaximal workload• may d at rest in borderline hypertensives
• some studies report a mean d of about 9 mmHg
• Total Peripheral Resistance and Afterload• u capillarization (more parallel circuits) r d TPR• d TPR r d Afterload (slight – not of major significance)• Respiratory Variables• Respiratory Rate
• Rest: NC• Submax exercise: d• Max exercise: slight u
• Tidal Volume• Rest: NC• Submax exercise: NC or slight u • Max exercise: slight u
• Anaerobic Threshold
• Occurs at a higher percentage of VO2 max
• Pre-training: 50% VO2max Post-training: 80% VO2max
Training Adaptations

09/04/2023 157
• Mitochondria• u number, size and membrane surface area
• Aerobic Enzymes in Exercising Muscle• u Krebs cycle enzymes (succinate dehydrogenase)• u b oxidation enzymes (carnitine acyltransferase)• u electron transport enzymes (cytochrome oxydase)
• Fatty Acid & Glycogen Utilization• u utilization of b oxidative pathways to produce ATP• Called the “glycogen sparring” effect• d RER for any given submaximal workload• u muscle glycogen stores (with high carbohydrate diet)
• No Appreciable Change in Resting Metabolic Rate Exception: training induced u in lean muscle mass
• d Platelet Aggregation• u Fibrinolytic Activity• d Circulating Catecholamines
• u vagal tone r d risk of arrhythmia• Resistance to Pathological Events• smaller infarct size and quicker recovery• Less of a d in ventricular function during ischemia
Training Adaptations

09/04/2023 158
75
185
60
185
0
50
100
150
200
sedentary-rest sedentary-max trained-rest trained-max
"Average" Values for Sedentary and Trained Individuals
Heart Rate( beats / minute )

09/04/2023 159
Stroke Volume( ml / beat )
"Average" Values for Sedentary and Trained Individuals
60
120
80
160
0
50
100
150
sedentary-rest sedentary-max trained-rest trained-max

09/04/2023 160
Cardiac Output( liters / minute)
"Average" Values for Sedentary and Trained Individuals
5
22
5
30
05
10152025303540
sedentary-rest sedentary-max trained-rest trained-max

09/04/2023 161
A-V O2 Difference( ml%)
"Average" Values for Sedentary and Trained Individuals
6
14
6
16
0
5
10
15
20
sedentary-rest sedentary-max trained-rest trained-max
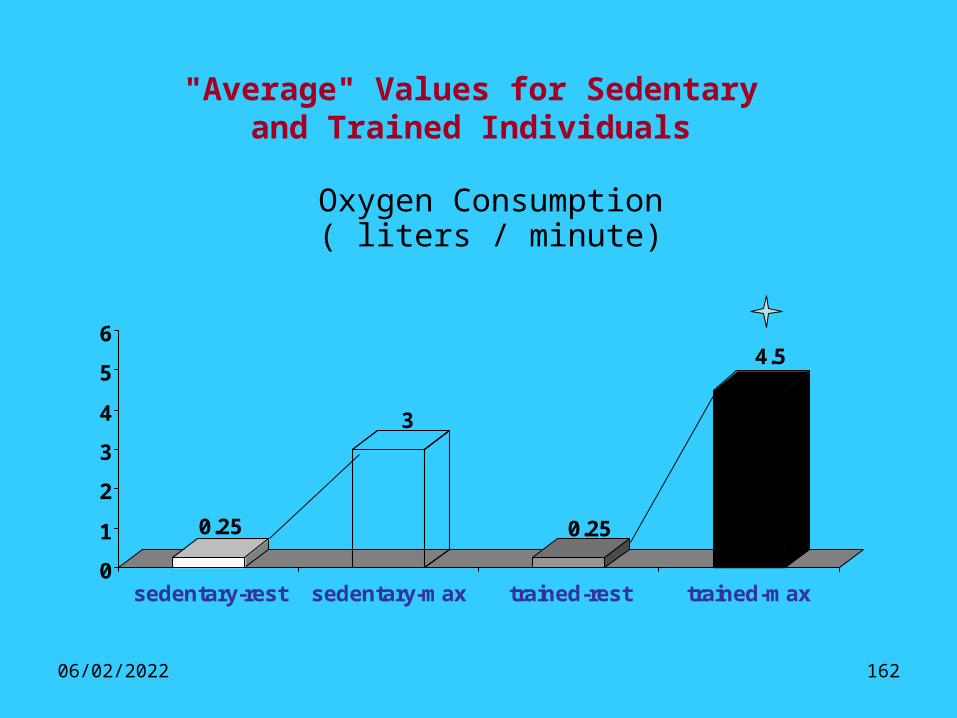
09/04/2023 162
Oxygen Consumption( liters / minute)
"Average" Values for Sedentary and Trained Individuals
0.25
3
0.25
4.5
0
1
2
3
4
5
6
sedentary-rest sedentary-max trained-rest trained-max

09/04/2023 163
"Average" Values for Sedentary and Trained Individuals
3.5
38
3.5
55
0
10
20
30
40
50
60
sedentary-rest sedentary-max trained-rest trained-max
Oxygen Consumption( ml / kg / minute)
09/04/2023 164
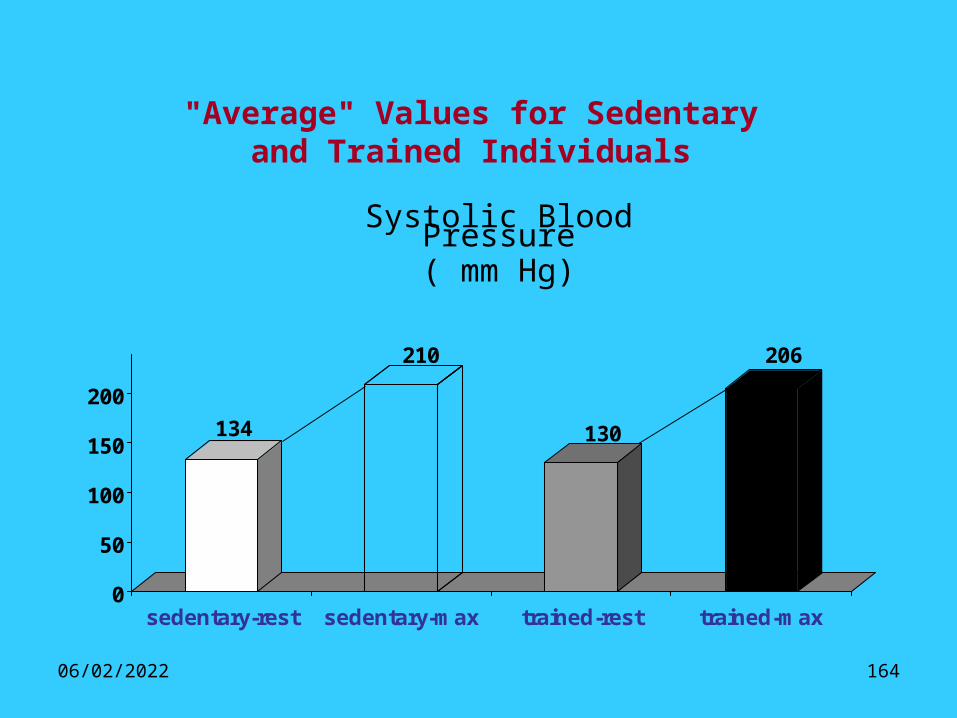
"Average" Values for Sedentary and Trained Individuals
134
210
130
206
0
50
100
150
200
sedentary-rest sedentary-max trained-rest trained-max
Systolic Blood Pressure( mm Hg)

09/04/2023 165
"Average" Values for Sedentary and Trained Individuals
8284
80
82
747678808284868890
sedentary-rest sedentary-max trained-rest trained-max
Diastolic Blood Pressure( mm Hg)

09/04/2023 166
HEART ANATOMY (EXTERNAL VIEW)
• The heart is a complex muscular pump that maintains oxygen and blood circulation through the lungs and the rest of the body.
• The heart pumps about 7200 liters/day.

09/04/2023 167
HEART ANATOMY (CROSSECTION VIEW)
The heart has four chambers.
Two atria act as collecting reservoirs.
Two ventricles act as pumps.
The heart has four valves for: Pumping action of the
heart. Maintaining
unidirectional blood flow.

09/04/2023 168
HEART (PHYSIOLOGY)
Deoxygenated blood returns to the heart via the superior and inferior vena cava, enters the right atrium, passes into the right ventricle, and from here it is ejected to the pulmonary artery.
Oxygenated blood returning from the lungs enters the left atrium via the pulmonary veins, passes into the left ventricle, and is then ejected to the aorta.

09/04/2023 169
VASCULAR FLUID MECHANICS
Velocity and pressure are inversely related to the cross sectional area of blood vessels.
These parameters drop in the capillaries where the cross-sectional area is more.

09/04/2023 170
JUST BEFORE I LEAVE……
One of the Keys to
Happiness is having a
good health and a bad memory…

09/04/2023 171
• Is a muscle about the size of your fist• Weighs approximately one pound• Is located behind and slightly to the left of the breastbone• Pumps about 5 quarts (4.7 liters) of blood every minute

09/04/2023 172

09/04/2023 173
The function of the heart is to circulate blood throughout the body by:
• Pumping blood through the lungs removes carbon dioxide and refreshes the blood with oxygen
• The oxygenated blood is pumped to the body to provide oxygen and nutrients and to remove waste products.
• The coronary arteries are the blood vessels that supply blood and oxygen to the heart muscle.

09/04/2023 174
2 coronary arteries branch from the main aorta just above the aortic valve. “No larger than drinking straws, they divide and encircle the heart to cover its surface with a lacy network that reminded physicians of a slightly crooked crown (coronary comes from the Latin coronarius, belonging to a crown or wreath). They carry out about 130 gallons of blood through the heart muscle daily.” (Clark, 119)
Blood Supply To The Heart

09/04/2023 175
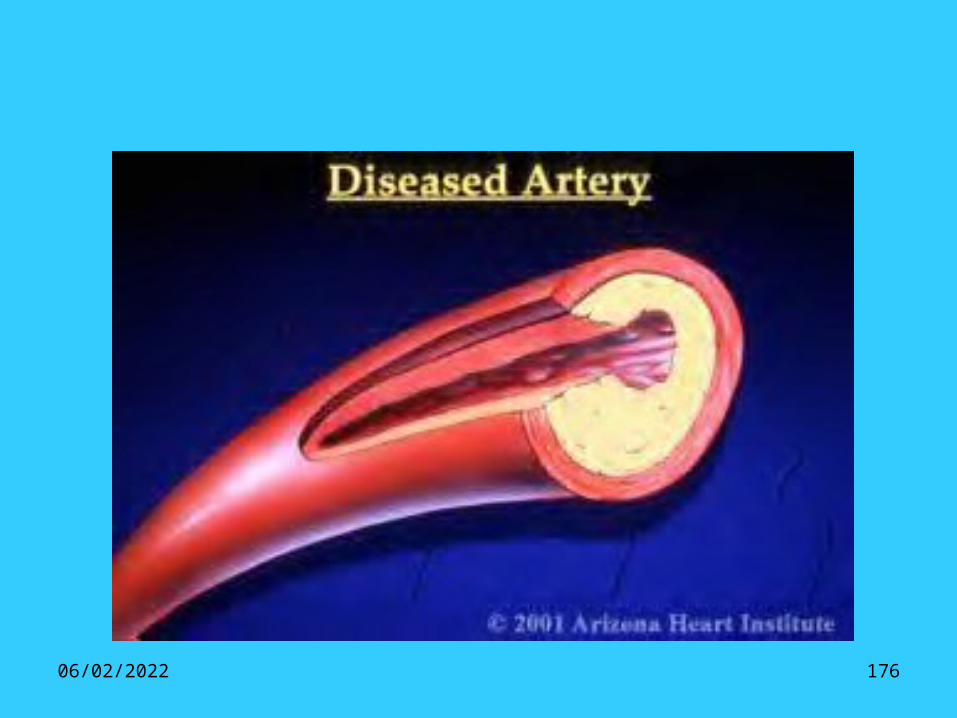
Coronary Artery Disease• Coronary artery disease is one of the most common
and serious effects of aging. Fatty deposits build up in blood vessel walls and narrow the passageway for the movement of blood. The resulting condition, called atherosclerosis often leads to eventual blockage of the coronary arteries and a “heart attack”.
09/04/2023 176

09/04/2023 177

09/04/2023 178
Signs and Symptoms• None: This is referred to as silent
ischemia. Blood to your heart may be restricted due to CAD, but you don’t feel any effects.
• Chest pain: If your coronary arteries can’t supply enough blood to meet the oxygen demands of your heart, the result may be chest pain called angina.
• Shortness of breath: Some people may not be aware they have CAD until they develop symptoms of congestive heart failure- extreme fatigue with exertion, shortness of breath and swelling in their feet and ankles.
• Heart attack: Results when an artery to your heart muscle becomes completely blocked and the party of your heart muscles fed by that artery dies.
Signs & Symptoms
NoneChestPain
ShortnessOf Breath
HeartAttack

09/04/2023 179
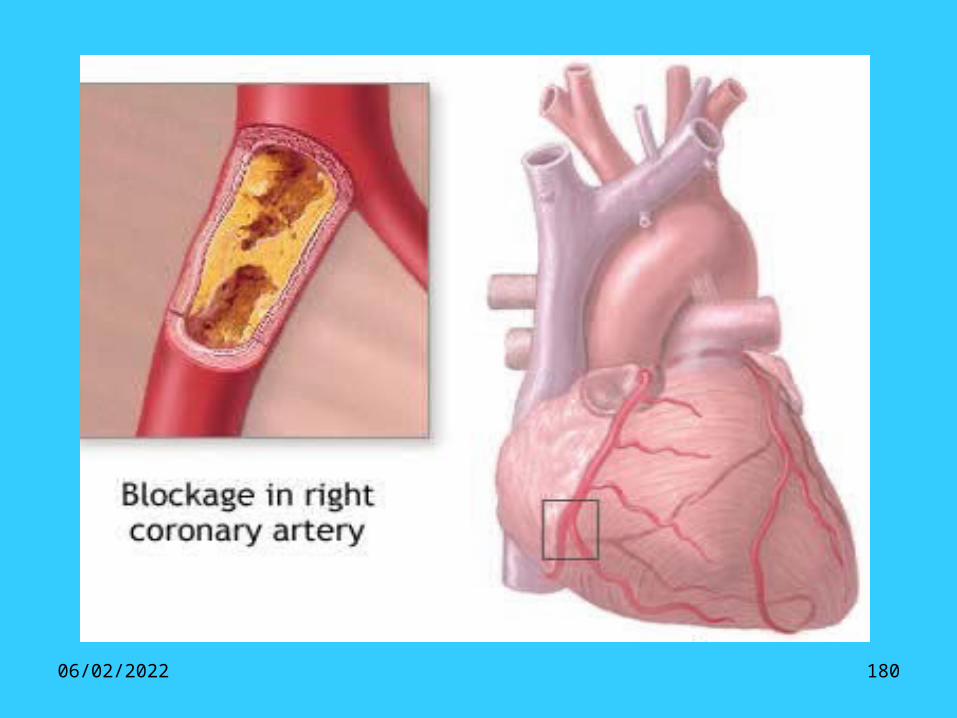
can, and does, occur in almost any artery in the body. But in the heart it’s effects can be crucial. “The body depends on a strong pumping heart to circulate life-giving blood, and this includes to the heart muscle itself. If the coronary arteries become blocked, the cardiac muscle begins to fail, and so the blood circulation decreases, which includes the circulation to the heart muscle itself.” (Thibodeau, 494)
09/04/2023 180

09/04/2023 181
• High blood cholesterol• High blood pressure• Smoking• Obesity• Lack of physical activity

09/04/2023 182
Risk Factors
UncontrollableUncontrollable
• Sex
• Hereditary
• Race
• Age
ControllableControllable
• High blood pressure
• High blood cholesterol
• Smoking
• Physical activity
• Obesity
• Diabetes
• Stress and anger

09/04/2023 183
Screening and Diagnosis
StressTest
measures
bloo
d
supply
to h
eart
CoronaryAngiography
spec
ific
shows
coro
nar
ies
Narrowing in
Sites of
Electro-cardiogram
measures
elec
tric
al
impulses

09/04/2023 184
• Blood tests: used to evaluate kidney and thyroid function as well as to check cholesterol levels and the presence of anemia.
• Chest X-ray: shows the size of your heart and whether there is fluid build up around the heart and lungs.
• Echocardiogram: shows a graphic outline of the heart’s movement
• Ejection fraction (EF): determines how well your heart pumps with each beat.

09/04/2023 185
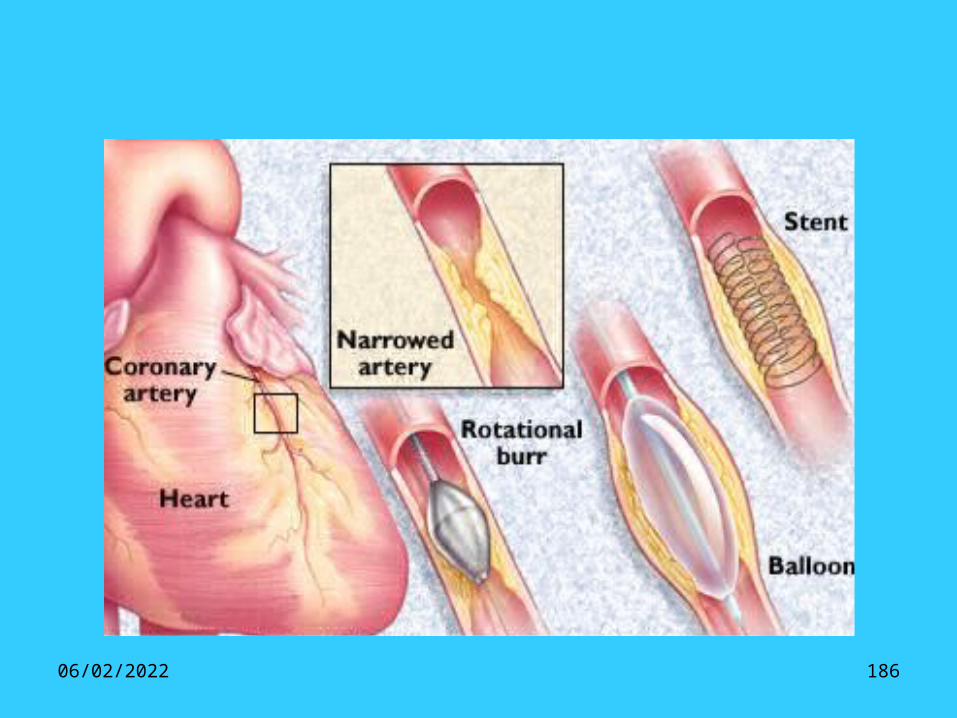
• Many people are able to manage coronary artery disease with lifestyle changes and medications.
• Other people with severe coronary artery disease may need angioplasty or surgery.
09/04/2023 186

09/04/2023 187
Arterial Blood PressureIt is the lateral pressure exerted by
blood on the walls of aorta and arteries.
• Ejection of blood into the aorta by the left ventricle results in a characteristic aortic pressure pulse.
• The peak of the aortic pressure pulse is termed the systolic pressure (Psystolic).
• The lowest pressure in the aorta is termed the diastolic pressure (Pdiastolic).
• The difference between the systolic and diastolic pressures is the aortic pulse pressure.
• The mean aortic pressure (MAP) is the average pressure (geometric mean) during the aortic pulse cycle

09/04/2023 188
As the aortic pressure pulse travels down the aorta and into distributing arteries, there are characteristic changes in the systolic and diastolic pressures, as well as in the mean pressure.
As the pressure pulse moves away from the heart, the systolic pressure rises and the diastolic pressure fall.
There is also a small decline in mean arterial pressure as the pressure pulse travels down distributing arteries due to the resistance of the arteries.

09/04/2023 189
• Therefore, when arterial pressure is measured using a sphygmomanometer (i.e., blood pressure cuff) on the upper arm, the pressure measurements represent the pressure within the brachial artery, which will be slightly different than the pressure measured in the aorta or the pressure measure in other distributing arteries.

09/04/2023 190
Measurements of Blood Pressure
1- Direct Method• The most accurate means for measuring blood
pressure is directly within an artery (intra-arterial) using a catheter.
• But because this method is invasive, it is neither practical nor appropriate for repeated measurements in non-hospital settings, or for large-scale public health screenings.
2- The mercury-filled sphygmomanometer• The usual method of measurement, therefore, is a
noninvasive means that uses a sphygmomanometer, which includes either a column of mercury or pressure-registering gauge.

09/04/2023 191
Physiological factors affecting Arterial Blood pressureAge: • New born: 80/40 mmHg• 4 years: 100/65 mmHg.• Adults: 120/80 mmHg• After that: Gradually increase due to increase elasticity of arteries.Sex:• Children: have equal Blood pressure.• Adults before 45 years: male more than female.• Adults after 45 years: the diastolic B.P. is more in female than males.
Race: ABP in oriental is less than in European and American.
Gravity: B.P. in upper parts of the body is more than the lower parts especially during standing.
Meals: Digestion increases the arterial blood pressure.
Emotions and exercise: increase the arterial blood pressure.
Sleep: Deep quiet sleep decrease A.B.P., while sleep with dreams increase A.B.P.

09/04/2023 192
Factors that Affect Blood Pressure
• Blood pressure is affected by several factors:
• 1- Cardiac output.• 2- Peripheral resistance • 3- Vessel elasticity • 4- Blood volume

09/04/2023 193
1- Cardiac OutputIt is the amount of blood pumped by the left
ventricle per minute. It keeps the arteries full of blood.An increase in cardiac output results in
increased blood pressure.Anything that decreases cardiac output also
decreases blood pressure, because there is less pressure on the vessel walls.
Cardiac Output = Heart Rate X Stroke VolumeAnything that affects heart rate or stroke volume
affects cardiac output and thus blood pressure.
09/04/2023 194
Regulation of Cardiac Output
• The cardiac output is regulated by two forces:
• Intrinsic (Frank-starling mechanism).
•Extrinsic (autonomic nervous system).

09/04/2023 195
Intrinsic control• Increased end-diastolic volume = increased
strength of cardiac contraction and increased stroke volume
• This increase in strength of contraction due to an increase in end-diastolic volume (the volume of blood in the heart just before the ventricles begin to contract) is called the Frank-Starling law of the heart:
• Increased end-diastolic volume = increased stretching of cardiac muscle = increased strength of contraction = increased stroke volume

09/04/2023 196

09/04/2023 197
Extrinsic control• Increased sympathetic stimulation,
increased strength of contraction of cardiac muscle
Mechanism • sympathetic stimulation cause release
of norepinephrine which increase permeability of muscle cell membranes to calcium and calcium diffuses through more cross-bridges and causes stronge contraction

09/04/2023 198
Extrinsic control

09/04/2023 199
2- Peripheral ResistanceOne of the main factors that affect blood
pressure is peripheral resistance.
• Blood cells and plasma encounter resistance when they contact blood vessel walls.
• If resistance increases, then more pressure is needed to keep blood moving.
Three main sources of peripheral resistance:• a. Blood vessel diameter • b. Blood viscosity • c. Total vessel length

09/04/2023 200
2 a)- Vessel Diameter• Vessel diameter affects peripheral
resistance.• As a diameter of a tube gets smaller, a
greater proportion of the fluid is in contact with the wall of the tube. Therefore resistance to flow is increased and pressure rises.
• Larger diameter, same volume, less pressure.
Smaller diameter, same volume, more pressure.

09/04/2023 201
Vasomotor Fibers• Constriction of blood vessels raises blood
pressure.• Vessel diameter is actively regulated by
vasomotor fibers, sympathetic nerve fibers that innervate the vessel's smooth muscle layer.
• Vasomotor fibers release norepinephrine, a powerful vasoconstrictor.
• A vasoconstrictor is a substance that causes blood vessels to constrict.
Vasoconstrictors• Blood vessel diameter is also regulated by
blood-borne vasoconstrictors.• (Epinephrine, Angiotensin II, Vasopressin)

09/04/2023 202
2 b)- Viscosity of bloodBlood viscosity affects peripheral resistance.• Viscosity is related to the thickness of a fluid.The greater the viscosity, the less easily molecules slide
past one another and the more difficult it is to get the fluid moving and keep it moving.
• Because of this greater resistance to flow, a greater pressure is required to pump the same volume of viscous fluid.
• The hematocrit is the percentage of red blood cells in the total blood volume.
• The hematocrit affects blood viscosity and therefore resistance to flow.
• The more viscous the blood, the greater resistance it encounters and the higher the blood pressure.
• The hematocrit can increase when there are more red blood cells or less plasma in the blood.
• The hematocrit can decrease when there are fewer red blood cells or more plasma.

09/04/2023 203
2 c)- Vessel Length
• Total vessel length affects peripheral resistance.
• Increased fatty tissue requires more blood vessels to service it and adds to the total vessel length in the body.
• The longer the total vessel length, the greater the resistance encountered, and the greater the blood pressure.

09/04/2023 204
3 - Vessel Elasticity• Besides peripheral resistance, blood vessel
elasticity also affects blood pressure.
• A healthy elastic artery expands, absorbing the shock of systolic pressure.
• The elastic recoil of the vessel then maintains the continued flow of blood during diastole.
• When an individual has arteriosclerosis, arteries become calcified and rigid, so they can't expand when the pulse wave of systolic pressure passes through them

09/04/2023 205
4 - Blood VolumeBlood volume affects blood pressure.• When there is a greater volume of fluid, more fluid
presses against the walls of the arteries resulting in a greater pressure.
• When there is less volume there is less pressure.• Reduced blood volume (for example due to excessive
sweating) reduces blood pressure short term. Long term homeostatic mechanisms compensate, bringing blood volume and blood pressure back up to normal levels.
• Increased blood volume (for example due to water retention from excessive salt intake) increases blood pressure short term. Long term homeostatic mechanisms compensate, bringing blood volume and blood pressure back up to normal levels.

09/04/2023 206
Regulation of arterial blood pressure
Blood pressure is maintained at a constant level within a narrow limit to ensure an adequate flow of blood to the tissue especially the vital organs e.g. heart, brain and kidney.

09/04/2023 207
Regulation of arterial blood pressure 2• Blood pressure=cardiac output X peripheral resistance
Thus the regulation of arterial blood pressure depend upon the previous two factors through two mechanisms:-
1- Nervous
2- Hormonal

09/04/2023 208
Regulatory mechanisms
• 1- immediately acting mechanisms.
• 2- intermediately acting mechanisms.
• 3- Long term acting mechanisms.

09/04/2023 209
Immediately acting mechanisms• Starts: within seconds.• Lasts: hours.• Type: Nervous.• Mechanism:
– Stimulation of baroreceptors in the aortic arch or carotid sinus by changes of blood pressure between 60mmHg and 200mmHg blood pressur.
– Stimulation of chemoreceptors in the aortic body or carotid body by changes of blood pressure between 40mmHg and 60mmHg blood pressure.

09/04/2023 210
1- immediately acting mechanisms
09/04/2023 211
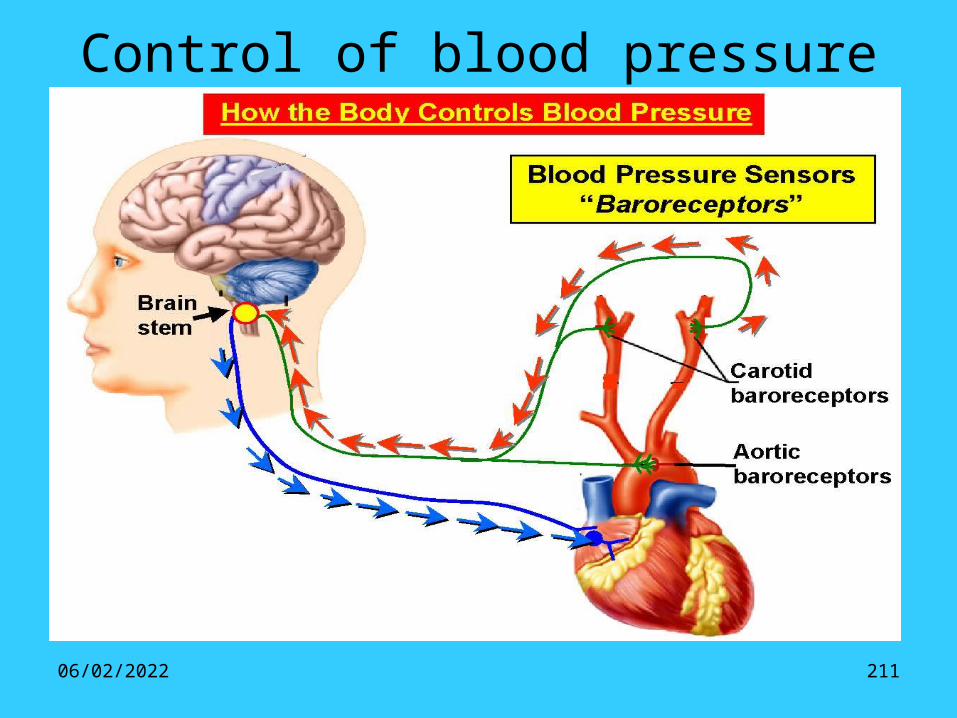
Control of blood pressure

09/04/2023 212
2- intermediately acting mechanisms.
• Starts: within half an hour.• Lasts: hours to 3-4 days.• Type:• Mechanism:
– Fluid shift mechanism.– Stress relaxation mechanism.
09/04/2023 213
3- Long term acting mechanisms
• Starts: within half an hour.• Lasts: days, months, or even years.• Type: hormonal.• Mechanisms:
– 1- Renin mechanism.– 2- Aldosterone mechanism.– 3- Antidiuretic hormone mechanism.

09/04/2023 214

09/04/2023 215
SHORT-TERM CONTROL OF ARTERIAL BLOOD PRESSURETHE SENSORY ARM
Arterial blood pressure is controlled by a negative feedback process
Carotid sinus and aortic arch baroreceptors respond to changes of blood pressure.
Ext carotid
Int carotid
Carotidsinus baro-
receptor
Aortic arch baroreceptor
sinus nerveto CN IX
vagus nerveCN X
Afferent nerve firing reflects both the rate of change of blood pressure during the pulse and the mean level
Inte
grat
ed n
erve
act
ivit
y%
max
imum
0
100
110 20060arterial pressure, mm Hg
vagusnerve
sinusnerve

09/04/2023 216
Medullary cardiovascular
centres
sympathetic parasympathetic
Receptorafferents
SHORT-TERM CONTROL OF ARTERIAL BLOOD PRESSURETHE EFFERENT ARM
Medullary cardiovascular centres regulate the efferent arm via the autonomic nervous system.
When activated:Sympathetic fibres innervate• arterioles - vasoconstriction• the s.a. node - tachycardia• myocardium - positive inotropy
Parasympathetic (vagal) fibres innervate • the s.a. node - bradycardia
Vagal tone to the s.a node predominates

09/04/2023 217
On standing up venous return falls
Cardiac output diminishes
Arterial blood pressure is reduced
Baroreceptor afferent firing reduced
Medullary centres inhibition reduced
THE BARORECEPTOR REFLEX - AN EXAMPLECORRECTION OF POSTURAL HYPOTENSION
Effect of gravity on venous returnPreload diminished - Starling’s LawSubject possibly feels faint as cerebral flow is reducedDue to reduced arterial B.P.
Vasoconstriction
Tachycardia
Raised stroke work
Tend to restore arterial blood pressure
Increased sympathetic tone to arteriolesReduced vagal tone to s.a. nodeIncreased myocardial sympathetic tone

THANK YOU …………………………………..
09/04/2023 218