cardiovascular safety in refractory incontinent patients ... · int j clin pract. 2017;71:e12944....
TRANSCRIPT
Drake, M. J., MacDiarmid, S., Chapple, C. R., Esen, A., Athanasiou, S.,Cambronero Santos, J., ... Stoelzel, M. (2017). Cardiovascular safety inrefractory incontinent patients with overactive bladder receiving add-onmirabegron therapy to solifenacin (BESIDE). International Journal ofClinical Practice, 71(5), [e12944]. DOI: 10.1111/ijcp.12944
Publisher's PDF, also known as Version of record
License (if available):CC BY-NC
Link to published version (if available):10.1111/ijcp.12944
Link to publication record in Explore Bristol ResearchPDF-document
This is the final published version of the article (version of record). It first appeared online via Wiley athttp://onlinelibrary.wiley.com/doi/10.1111/ijcp.12944/abstract. Please refer to any applicable terms of use of thepublisher.
University of Bristol - Explore Bristol ResearchGeneral rights
This document is made available in accordance with publisher policies. Please cite only the publishedversion using the reference above. Full terms of use are available:http://www.bristol.ac.uk/pure/about/ebr-terms

Int J Clin Pract. 2017;71:e12944. wileyonlinelibrary.com/journal/ijcp | 1 of 15https://doi.org/10.1111/ijcp.12944
© 2017 The Authors International Journal of Clinical Practice Published by John Wiley & Sons Ltd
Received:20February2017 | Accepted:26February2017DOI: 10.1111/ijcp.12944
O R I G I N A L P A P E R
Cardiovascular safety in refractory incontinent patients with overactive bladder receiving add- on mirabegron therapy to solifenacin (BESIDE)
Marcus J. Drake1 | Scott MacDiarmid2 | Christopher R. Chapple3 | Adil Esen4 | Stavros Athanasiou5 | Javier Cambronero Santos6 | David Mitcheson7 | Sender Herschorn8 | Emad Siddiqui9 | Moses Huang9 | Matthias Stoelzel10
1University of Bristol and Bristol Urological Institute, Bristol, UK2AllianceUrologySpecialists,Greensboro,NC,USA3RoyalHallamshireHospitalandSheffieldHallamUniversity,Sheffield,UK4DokuzEylülUniversitySchoolofMedicine,İzmir,Turkey5UniversityofAthensMedicalSchool,Athens,Greece6InfantaLeonorHospital,Madrid,Spain7StElizabeth’sMedicalCenter,Brighton,MA,USA8SunnybrookHealthSciencesCentre,UniversityofToronto,Toronto,ON,Canada9AstellasPharmaEuropeLtd,Chertsey,Surrey,UK10AstellasPharmaGlobalDevelopment,Leiden,TheNetherlands
CorrespondenceMarcusJ.Drake,UniversityofBristolandBristolUrologicalInstitute,SouthmeadHospital, Bristol, UK.Email: [email protected]
Funding informationAstellasPharmaEuropeLtd;AstellasPharmaGlobalDevelopment
SummaryAims/objectives:IntheBESIDEstudy,combinationtherapy(antimuscarinic[solifena-cin] and β3-adrenoceptor agonist [mirabegron]) improved efficacy over solifenacinmonotherapy without exacerbating anticholinergic side effects in overactive bladder (OAB)patients;however,apotentialsynergisticeffectonthecardiovascular(CV)sys-tem requires investigation.Methods: OABpatientsremaining incontinentdespitedailysolifenacin5mgduring4- week single- blind run- in, were randomised 1:1:1 to double- blind daily combination (solifenacin5mg/mirabegron25mg,increasingto50mgafterweek4),solifenacin5or 10mg for 12weeks. CV safety assessments included frequency of CV-relatedtreatment-emergentadverseevents(TEAEs),changefrombaselineinvitalsigns(sys-tolicbloodpressure[SBP],diastolicbloodpressure[DBP],pulserate)andelectrocar-diogram(ECG)parameters.Results: Thefrequencyofhypertension,tachycardiaandECGQTprolongation,respec-tively,waslowandcomparableacrosscombination(1.1%,0.3%,0.1%),solifenacin5mg(0.7%,0.1%,0.1%),andsolifenacin10mggroups(0.8%,0%,0.1%).Adjustedmean(SE)changefrombaselinetoendoftreatment(EoT)inSBP,DBP,andpulseratewithcom-bination(0.07mmHg[0.38],−0.35mmHg[0.26],0.47bpm[0.28]),solifenacin5mg(−0.93mmHg [0.38], −0.45mmHg [0.26], 0.43bpm [0.28]) and solifenacin 10mg(−1.28mmHg[0.38],−0.48mmHg[0.26],0.27bpm[0.28])wasgenerallycomparable,withtheexceptionofameantreatmentdifferenceof~1mmHginSBPbetweencom-binationandsolifenacinmonotherapy;SBPwasunchangedwithcombinationandde-creasedwith solifenacinmonotherapy.Mean changes frombaseline to EoT in ECGparametersweregenerallysimilaracrosstreatmentgroups,exceptforQTintervalcor-rectedusingFridericia’sformula,whichwashigherwithsolifenacin10mg(3.30msec-onds)vs.combination(0.49mseconds)andsolifenacin5mg(0.77mseconds).Conclusion: Thecomparable frequencyofCV-relatedTEAEs, changes invital signsand ECG parameters indicates no synergistic effect on CV safety outcomeswhen mirabegron and solifenacin are combined.
ThisisanopenaccessarticleunderthetermsoftheCreativeCommonsAttribution-NonCommercialLicense,whichpermitsuse,distributionandreproductioninanymedium, provided the original work is properly cited and is not used for commercial purposes.

2 of 15 | DRAKE Et Al.
1 | INTRODUCTION
Thesymptomcomplexofoveractivebladder(OAB)isdefinedasuri-nary urgency, often accompanied by increased daytime micturition frequency and nocturia in the absence of urinary tract infection or other obvious pathology; urgency incontinence may or may not be present.1,2OABisestimatedtoaffect20%oftheglobalpopulationby2018.3IncreasingageisthemostcommonriskfactorforOAB,withcurrentprevalence ratesof30%-40% inpatientsaged≥65years.4,5 Malesandfemalesareequallyaffected,however,certainsymptomspredominate in males (urgency and nocturia) and females (inconti-nence).6,7 SinceOAB is an age-related condition, significantlymorepatients present with concomitant cardiovascular (CV) comorbidi-ties (eg, hypertension) compared with non-OAB patients,8 which emphasises the importance of evaluating the CV safety of OABpharmacotherapies.
The two available oral pharmacotherapies—antimuscarinicsand the β3-adrenoceptor agonist, mirabegron—mediate relaxationof the bladder by antagonism of themuscarinicM2 andM3 recep-tor subtypes,9 or stimulation of the β3- adrenoceptor subtype, in the urothelium and detrusor muscle.10Muscarinic(M2,M3)receptorsandβ-adrenoceptors(β1, β2 and β3)arealsoexpressedintheCVsystem.TheM2 receptor has a functional role in mediating heart rate11 and theM3 receptor mediates vasodilation,12 and their antagonism could potentially increasebloodpressureorheartrate,prolongtheQTin-terval and induce polymorphic ventricular tachycardia (torsade depointes).11 The β1- adrenoceptor mediates increased heart rate and force of contraction and the β2- adrenoceptor mediates vasodilation in the vascular smooth muscle.13Theroleoftheβ3- adrenoceptor is less clear in human physiology, however, in vitro, the activation of the β3- adrenoceptor induces positive inotropic effects in human atrial tissue and negative inotropic effects in ventricular tissue.14Theantimusca-rinic,solifenacin,isselectivefortheM3 subtype,15 while in-vitro stud-ies show that mirabegron has a 150- fold and 33- fold higher affinity for the β3- vs. β1- and β2- adrenoceptor subtypes.16GiventhelocationoftheM3 receptor and β3adrenoceptorinCVtissues,andthehighden-sity of β1 adrenoceptors in the heart, potential effects on the heart and vasculature cannot be excluded when these drugs are used as mono-therapy or in combination.
MirabegronandsolifenacinsharesimilarefficacyinthetreatmentofOAB,17andareconsideredtohaveanacceptableCVsafetypro-file at therapeutic doses.18,19Aspermirabegron’s labelling, periodicblood pressure monitoring is advocated during treatment, and mi-rabegron is not recommended in patients with severe uncontrolled hypertension (systolicbloodpressure [SBP]≥180mmHgand/ordi-astolicbloodpressure[DBP]≥110mmHg).20Giventhelackofanti-muscarinicandmirabegrondatainolderpatientswithsignificantCVriskfactorsinPhaseIIItrials,itisconsideredgoodclinicalpracticetoperiodicallymonitor blood pressure and heart rate inOABpatientsaged >80 years.18,19
OABpatientsareusuallyinitiatedonanantimuscarinic,however,persistence is often poor because of bothersome anticholinergic side
effects(eg,blurredvision,drymouth)orinadequateimprovementinsymptoms.21,22Switchingtoanalternativeantimuscarinicusuallyhaslittle impact in terms of improved persistence,23 while dose escalation can often exacerbate the anticholinergic burden leading to treatment discontinuation.21,24
Several OAB trials investigating combinations of solifenacin(2.5/5/10mg)andmirabegron(25/50mg)havedemonstratedanad-ditive benefit in efficacy without compromising safety vs. solifenacin monotherapy.25–27IntheBESIDEstudy(NCT01908829),addingmira-begron50mgtosolifenacin5mgfurtherimprovedOABsymptomsandpatient- reported outcomes vs. solifenacin 5 mg or 10 mg, and was well- toleratedinOABpatientsremainingincontinentafterinitialsolifenacin5 mg.25,28Herein,wereportontheCVsafetyoutcomesfromBESIDEincluding subpopulations stratified by hypertensive status and gender (age-relatedCVsafetywillbereportedinasubsequentmanuscript).
2 | METHODS
2.1 | Study design and participants
ThemethodologyforBESIDEhasbeenpreviouslydescribed.25 In sum-mary, adultswithOAB symptoms for≥3months entered a2-weekscreening/wash- out period, followed by a run- in period with single- blind daily solifenacin 5 mg for 4 weeks provided they reported an averageof≥2incontinenceepisodes/24hpriortotherun-inperiod.Patientsremainingincontinentatbaseline(≥1episodeduringthe3-daybladderdiary),whosatisfiedinclusion,anddidnotmeetexclusioncriteria, were randomised 1:1:1- 12 weeks of daily double- blind treat-mentwithcombination(solifenacin5mg/mirabegron25mg,increas-ingto50mgafterweek4),solifenacin5mgor10mgmonotherapy.
What’s known• A combination of antimuscarinic (solifenacin 5mg) and
β3-adrenoceptor agonist (mirabegron 50mg) improvesefficacy without exacerbating anticholinergic side effects vs. solifenacinmonotherapy (5mg, 10mg) in the treat-mentofoveractivebladder(OAB).
• Cardiovascular (CV)comorbiditiesaremoreprevalent inOABpatientscomparedwiththenon-OABpopulation.
• Mirabegron and solifenacin in combinationmay poten-tiallyaffecttheCVsystem;however,monotherapyuseattherapeuticdosesindicatesnoCVsafetyconcerns.
What’s new• Using a combination of mirabegron and solifenacin does nothaveasynergisticeffectontheCVsystemsincethefrequency of CV-related treatment-emergent adverseevents, change in vital signs and ECG parameters arecomparable with solifenacin monotherapy (5mg and10mg).

| 3 of 15DRAKE Et Al.
2.2 | CV safety assessment
The frequency of CV-related treatment-emergent adverse events(TEAEs) was assessed during the study and 2-week follow-up andincludedincreasedbloodpressure,QTprolongation,increasedheartrate, tachycardia, atrial fibrillation, and palpitations. Potentially se-rious CV-related events were adjudicated by the IndependentCardiovascular Adjudication Committee and were summarised bytypeofCVevent (AntiplateletTrialists’Collaboration [APTC]/MajorAdverse Cardiovascular Events [MACE] or non-APTC/MACE) andnon-CVevent.
Forvitalsigns(SBP,DBP,andpulserate),triplicatereadingsweremeasuredon site at screening, randomisation (baseline), andeachfollow- up visit and the average of the last two readings was used toderivetheaverageperanalysisvisit.Thechangefrombaselinetoendoftreatment(EoT)invitalsignsintheoverallpopulation,andac-cording to subpopulations based on hypertension status at screen-ing and β- blocker use during the treatment period were previously presented in the primary analysis of BESIDE,25 and the adjusted changefrombaselinetoEoTvaluesaresummarisedinthisanalysis.Additional sensitivity analyses included a factor for antihyperten-siveuseat screeningoradifferentagegroup factor (<45,≥45 to<65,≥65years)inthemodel.Changeinvitalsignswasalsostrati-fiedbygender.Shiftinvitalsignseverityaccordingtofourcatego-ries of average bloodpressure readings ([i] SBP<140mmHg andDBP<90mmHg;[ii]SBP≥140-159mmHgorDBP≥90-99mmHg;[iii] SBP ≥160-179mmHg or DBP ≥100-109mmHg; [iv] SBP≥180mmHg or DBP ≥110mmHg)was assessed in terms of thepercentage of patients who experienced “no shift”, “categorical in-crease”,or“categoricaldecrease”frombaselinetoEoT.Thepercent-ageofpatientsmeetingchangefrombaselinecriteriaforSBP(≥10,15, 20mmHg), DBP (≥5, 10, 15mmHg), and pulse rate (≥5, 10,15bpm)at threeconsecutivepostbaselinevisitswaspresented inthe overall population and in the subpopulations based on hyperten-sive status at screening or β-blockeruse.Thepercentageofpatientsin the overall population who experienced potentially clinically sig-nificantchangesinvitalsigns(SBP[≥180mmHganda≥20mmHgchangefrombaseline];DBP[≥105mmHgand≥15mmHgchangefrom baseline]; pulse rate [≥120bpm and ≥15bpm change frombaseline])wasalsoreported.
Twelve-lead electrocardiograms (ECGs) were performed atscreening,baseline(week0)andateachfollow-upvisitwiththepa-tient in the supine position, after the patient had been lying down for 15minutes. Triplicate ECGswere recordedwith an interval ofatleast5minutesbetweeneachECG,madeataspeedof25mm/sand all leads including at least 4 complexes. Interpretation of the ECGwasundertakenbytheinvestigator(notreportedinthisanal-ysis) andbyan independentcentral reader.Thepercentageofpa-tients with abnormal/normal readings were reported at each visit. ThemeanvaluesandchangefrombaselineatEoT inthePR inter-val,RR interval,QRS interval,QT interval correctedbyFridericia’sformula (QTcF), and heart rate are reported in the overall popu-lation. The frequency of QTcF extreme values (>450mseconds,
>480msecondsand>500mseconds)andextremesinchangefrombaseline (>30mseconds and >60mseconds)were reported duringdouble- blind treatment in the overall population and stratified by gender.FortheinterpretationoftheECGsbythecentralreader,thepercentage of patients who had “no categorical change”, “abnormal to normal” and “normal to abnormal” during double- blind treatment were presented.
2.3 | Statistical analysis
Samplesizecalculationsrelatedtocategoricalchangesintheprimaryefficacyendpoint(incontinenceepisodes/24h),werebasedonprevi-ous studies with mirabegron alone and in combination with solifena-cin,andaredescribedintheprimaryanalysisofBESIDE.25Thesafetyanalysisset(SAF)consistedofallrandomisedpatientswhoreceived≥1doseofdouble-blindtreatmentandwasusedfortheanalysisofCVsafetyvariables.
CVTEAEsof interest (increasedbloodpressure;QTprolonga-tion; increased heart rate, tachycardia, atrial fibrillation and palpi-tations)wereidentifiedusingstandardisedMedRAqueries(v16.0).Thepercentageofpatientswhoreported≥1AEweresummarisedbySystemOrganClassandPreferredTermbytreatmentwithcorre-sponding95%CI.TachycardiawasreportedasaTEAEaccordingtotheinvestigator’sjudgementindependentofapulserate≥100bpm.Tachycardiawasalsoreportedaccordingtothestandardisedassess-mentofvitalsigndatabasedonameanpulserate≥100bpm.
The average change from baseline to EoT for vital signs wasanalysed using an analysis of covariance (ANCOVA)modelwhichincludedtreatmentgroup,randomisationstratificationfactors(gen-der, agegroup<65and≥65years, geographic region and4-weekincontinenceepisodereductiongroup)asfixedfactorsandbaselinevital sign value as a covariate. Least squares mean estimates and two-sided95%CIsforthemeanchangesfrombaselinewithineachtreatment group, as well as for the difference in change from base-line between combination therapy vs. solifenacin 5 mg and 10 mg, were derivedwith two-sided 95% CIs. The studywas only pow-ered for efficacy endpoints, thus no P- values were calculated for vital signdifferences. Populations forvital sign analyses included:(i)overall (anypatient intheSAF); (ii)pasthistoryofhypertension(medical history of hypertension andno concurrent antihyperten-sivetreatmentatscreening);(iii)hypertensiveatscreening(medicalhistory of hypertension and concurrent antihypertensive treatment atscreening);(iv)nohypertensionatscreening;(v)useofβ- blockers (≥1doseduringtherun-inperiodand≥1doseduringdouble-blindtreatment); (vi) nouseofβ- blockers. For patients meeting change from baseline criteria in vital signs, percentages are based on the total number in each treatment group with non- missing values. Additionalsensitivityanalyseswereperformedincludingantihyper-tensiveuseatscreeningoradifferentagegroupfactor (<45,≥45to<65,≥65years)intheANCOVAmodeltoanalysechangesfrombaseline in vital signs.
Heartrate,PR interval,RR interval,QRS intervalandQTcFweresummarised descriptively for each treatment group at each visit

4 of 15 | DRAKE Et Al.
includingchangesfrombaselinetoeachpostbaselinevisit.Theworstnon-missingvaluewasusedintheanalysisforcategoricalECGvari-ables reported by the central reader.
3 | RESULTS
3.1 | Patient demographics and baseline characteristics
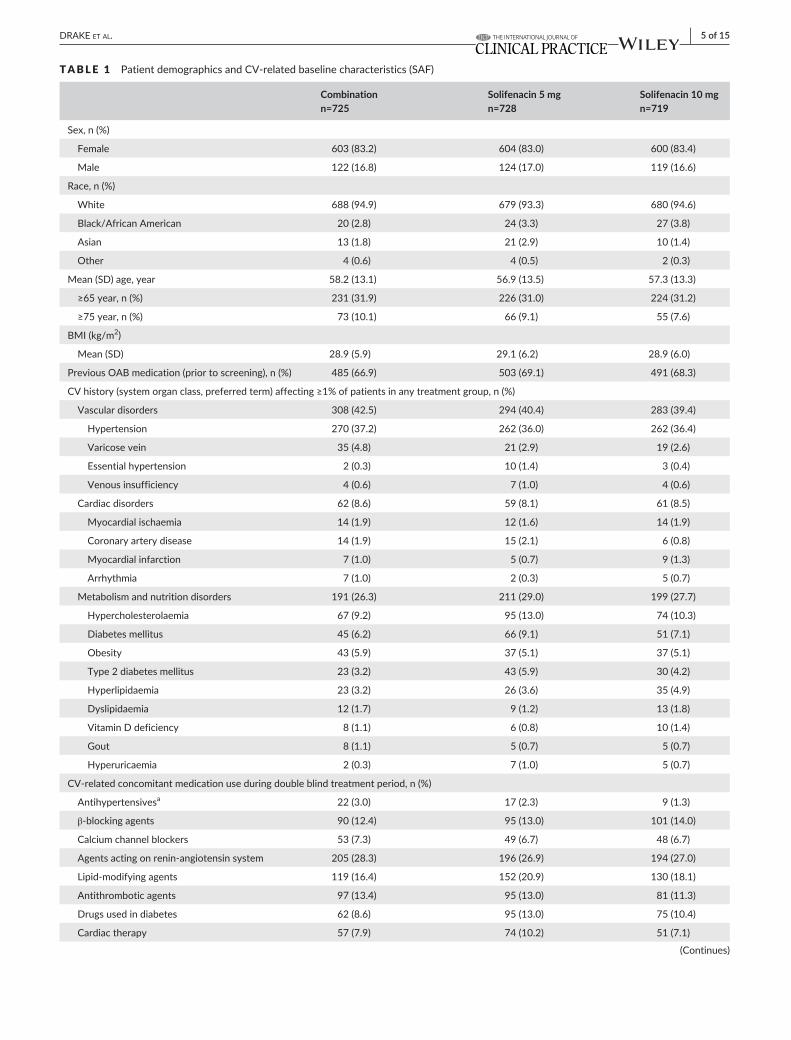
Overall, 2174 patients were randomised into the study, of which 2172 (99.9%) received double-blind study drug and were in-cluded in the safety analysis set (SAF). The discontinuation rate(post-randomisation)was low (6.2%)withno relevantdifferencesamong treatment groups.Theoverallmean age at screeningwas57.5years.Approximately37%ofpatientshadahistoryofhyper-tensionandapproximately7.5%and4.5%, respectively,had type1 and type 2 diabetes mellitus in each treatment group at base-line (Table1).Themost frequently reportedconcomitantmedica-tions during treatment were agents acting on the renin- angiotensin system (~27%);medicationusewascomparableacross treatmentgroups(Table1).
3.2 | CV- related TEAEs
Overall, the frequencyofTEAEsof interest related to theCV sys-tem(increasedbloodpressure;QTprolongation;increasedheartrate,tachycardia, atrial fibrillationandpalpitations)was low (<2.0%)andcomparable across treatment groups.Hypertension as a TEAEwasreported in19patients (combinationn=8, [1.1%], solifenacin5mg,n=5 [0.7%], solifenacin 10mg, n=6 [0.8%]) (Table2). One patient(0.1%) in eachgrouphadECGQTprolongation (the threepatientswerefemalewithQTcFreadingsthatrangedfrom447msecondsto476mseconds).TachycardiawasreportedasaTEAEinthreepatients(combination, n=2 [0.3%]; solifenacin 5mg, n=1 [0.1%]); ECG andvital sign results confirmed heart rate was no more than 102 bpm in thesepatients.SevenseriousCV-relatedTEAEswerereported:acutemyocardialinfarction(n=1[0.1%],solifenacin10mg),atrialfibrillation(n=1 [0.1%], solifenacin5mg), atrioventricularblockcomplete (n=1[0.1%],combination)arteriogramcoronarynormal(n=1[0.1%],com-bination),transientischaemicattack(n=1[0.1%],solifenacin10mg),hypertensive crisis (n=1 [0.1%], solifenacin 10mg) and thrombosis(n=1, solifenacin 5mg). The patient in the solifenacin 10mg groupwho experienced hypertensive crisis required hospitalisation for 1dayandtemporarycessationofsolifenacintreatment.Thepatientexperiencing atrioventricular block in the combination group had a cardiac history (ie, previous cardiac surgery, myocardial infarction,andaorticaneurysm)andseconddegreeblockpriortodouble-blindtreatment.Thecaseofthrombosisdevelopedinapreviousfemoralbypass. The coronary arteriogram was requested after an episodeof pneumonia that was considered clinically significant by the study investigator.Noneof thesevenseriousTEAEswereconsideredbythe investigator tobe related to treatment. Tenpotentially seriousCV-relatedTEAEswerereviewedbytheadjudicationcommittee.This
includedfivenon-APTC/MACECVevents(combinationn=1[0.1%],solifenacin5mgn=2 [0.3%]andsolifenacin10mgn=2 [0.3%])andoneAPTC/MACECVevent (non-fatalmyocardial infarction) in thesolifenacin 10 mg group. In addition, there was one event in the solif-enacin 10 mg group for which there was insufficient data to adjudi-cate, and three events in the combination group were adjudicated as non-CVevents.
3.3 | Vital signs
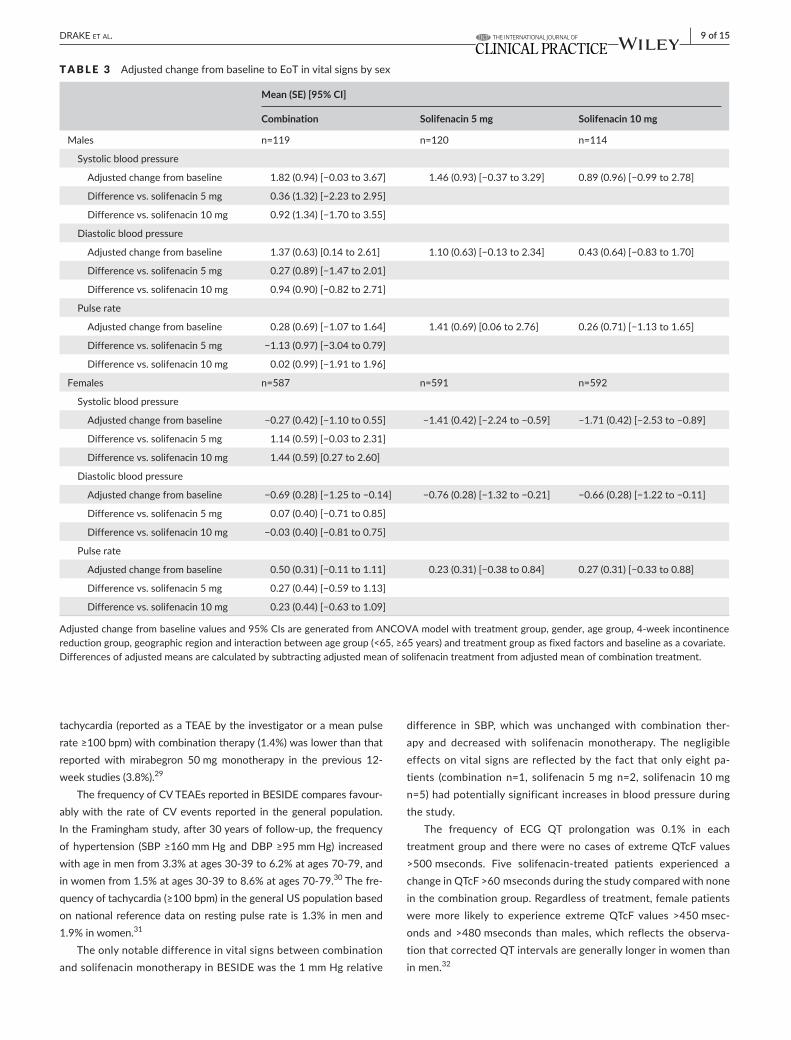
In theoverall SAFpopulation, the adjustedmean (SE) change frombaselinetoEoTinSBPwas0.07(0.38),−0.93(0.38)and−1.28(0.38)for combination, solifenacin 5 mg and solifenacin 10 mg groups, re-spectively; resulting in a mean difference of ~1 mm Hg in the combi-nationgroupvs.solifenacinmonotherapy.Therewerenoappreciabledifferences between combination and solifenacin monotherapy for DBPandpulserate:theadjustedmean(SE)changefrombaselinetoEoT inDBPwas−0.35 (0.26), −0.45 (0.26) and−0.48 (0.26) and inpulseratewas0.47(0.28),0.43(0.28)and0.27(0.28)inthecombi-nation, solifenacin 5 mg and solifenacin 10 mg groups, respectively. Therewerenonotable differences between combination and solif-enacin monotherapies in vital signs in subpopulations stratified by hy-pertensive status and β- blocker use, in the sensitivity analyses using a different age group factor or hypertensive medication use at screen-ing in themodel (Figure1), and betweenmale and female patients(Table3).
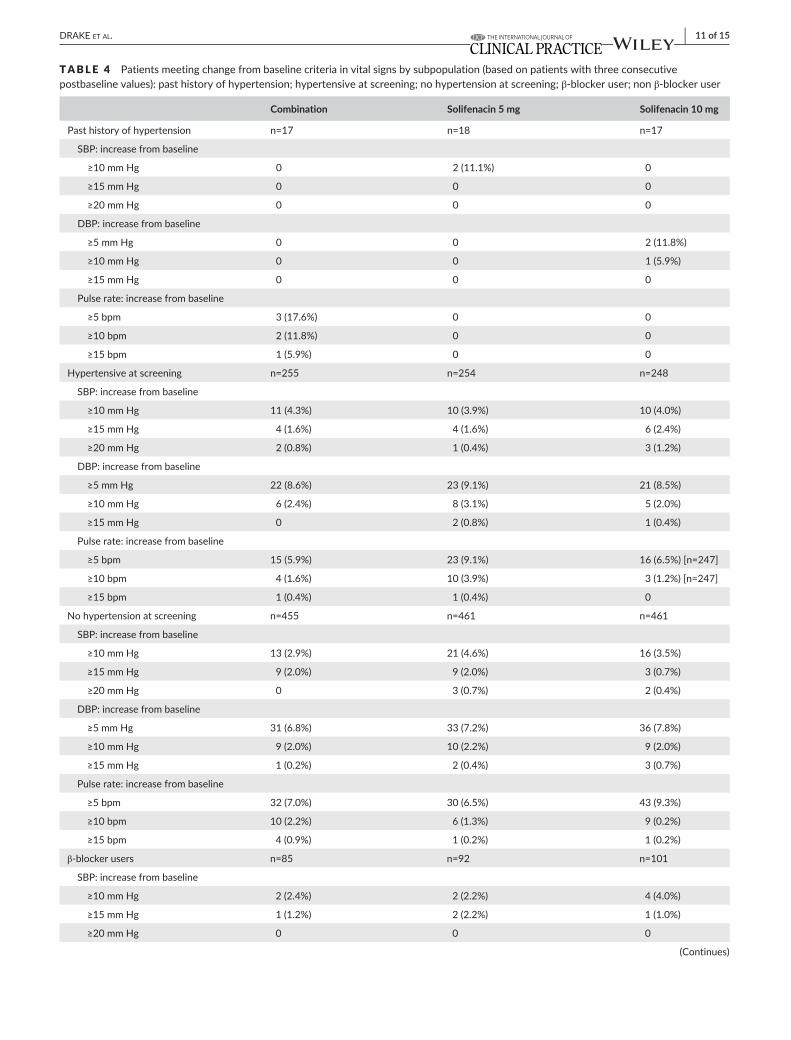
The percentage of patients with increases in vital signs at EoTthat met the change from baseline criteria at three consecutive visits was low and similar across treatment groups in the overall population (Figure2A-C).Similarfindingswereevidentinthesubpopulationsac-cording to hypertension history, hypertensive status at screening and β- blocker use, with the exception of pulse rate in the past history of hypertensioncohort(n=53)inwhichnomorethan3/17(17.6%)pa-tients receiving combination met one of the three criteria for change frombaselinevs.noneinthesolifenacingroups(Table4).
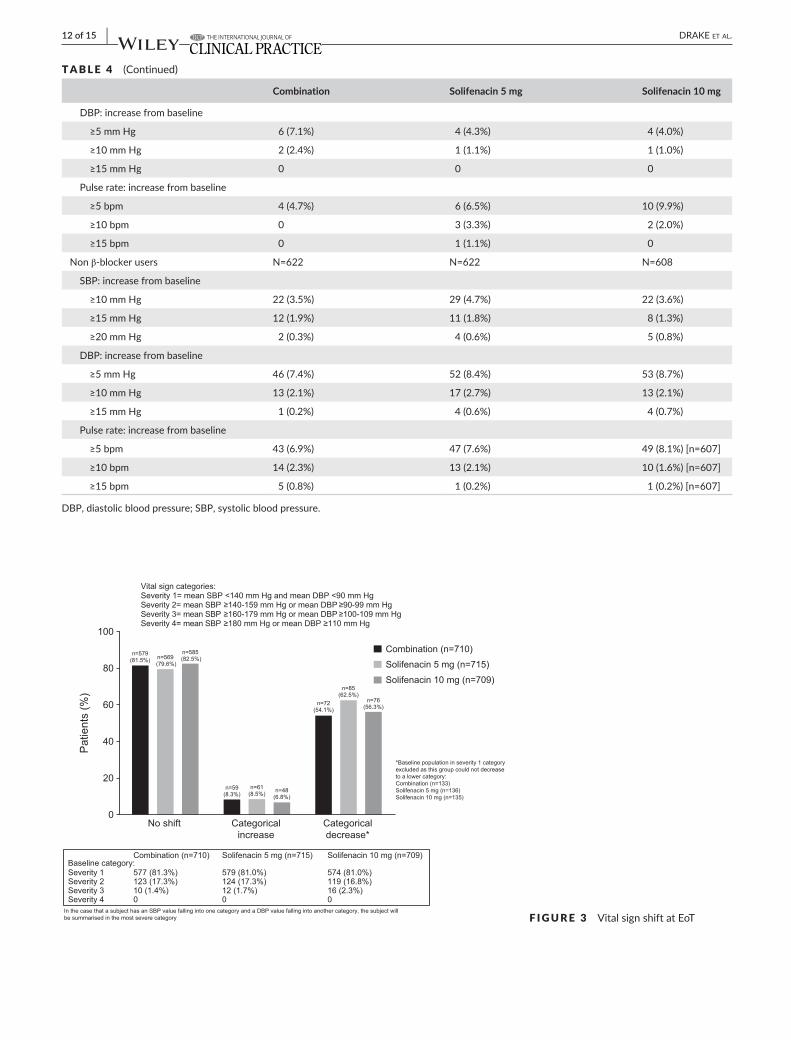
AtEoT,asimilarproportionofpatients(~80%)ineachtreatmentgrouphadnoshiftinvitalsignseverity,whilelessthan10%ofpatientsineachgroupexperiencedacategoricalincrease(Figure3);threepa-tients(n=1combination,n=1solifenacin5mg,n=1solifenacin10mg)shiftedtoseveritycategory4(SBP≥180mmHgandDBP=100mmHg)fromcategory2(SBP≥140-159mmHgandDBP≥90-99mmHg).
During the treatment period, potentially clinically significant valuesinDBP(≥105mmHgand≥15mmHgchangefrombaseline)wereobservedinsixpatients(n=2[solifenacin5mgatweek4],n=3[solifenacin10mgduringthestudy],andn=1[combinationatweek12]),and inSBP (≥180mmHgand≥20mmHgchange frombase-line) in twopatients (solifenacin10mggroupatweek4 [n=1]and8[n=1]).
The frequency of tachycardia, according to the standardisedassessment of vital sign data, and defined as an average pulse rate ≥100bpm,was low and similar across groups during the treatmentperiod (combination n=8, 1.1%; solifenacin 5mg n=12, 1.7% and solifenacin10mgn=10,1.4%).
| 5 of 15DRAKE Et Al.
TABLE 1 PatientdemographicsandCV-relatedbaselinecharacteristics(SAF)
Combination n=725
Solifenacin 5 mg n=728
Solifenacin 10 mg n=719
Sex,n(%)
Female 603(83.2) 604(83.0) 600(83.4)
Male 122(16.8) 124(17.0) 119(16.6)
Race,n(%)
White 688(94.9) 679(93.3) 680(94.6)
Black/AfricanAmerican 20(2.8) 24(3.3) 27(3.8)
Asian 13(1.8) 21(2.9) 10(1.4)
Other 4(0.6) 4(0.5) 2(0.3)
Mean(SD)age,year 58.2(13.1) 56.9(13.5) 57.3(13.3)
≥65year,n(%) 231(31.9) 226(31.0) 224(31.2)
≥75year,n(%) 73(10.1) 66(9.1) 55(7.6)
BMI(kg/m2)
Mean(SD) 28.9(5.9) 29.1(6.2) 28.9(6.0)
PreviousOABmedication(priortoscreening),n(%) 485(66.9) 503(69.1) 491(68.3)
CVhistory(systemorganclass,preferredterm)affecting≥1%ofpatientsinanytreatmentgroup,n(%)
Vasculardisorders 308(42.5) 294(40.4) 283(39.4)
Hypertension 270(37.2) 262(36.0) 262(36.4)
Varicosevein 35(4.8) 21(2.9) 19(2.6)
Essential hypertension 2(0.3) 10(1.4) 3(0.4)
Venousinsufficiency 4(0.6) 7(1.0) 4(0.6)
Cardiac disorders 62(8.6) 59(8.1) 61(8.5)
Myocardialischaemia 14(1.9) 12(1.6) 14(1.9)
Coronary artery disease 14(1.9) 15(2.1) 6(0.8)
Myocardialinfarction 7(1.0) 5(0.7) 9(1.3)
Arrhythmia 7(1.0) 2(0.3) 5(0.7)
Metabolismandnutritiondisorders 191(26.3) 211(29.0) 199(27.7)
Hypercholesterolaemia 67(9.2) 95(13.0) 74(10.3)
Diabetes mellitus 45(6.2) 66(9.1) 51(7.1)
Obesity 43(5.9) 37(5.1) 37(5.1)
Type2diabetesmellitus 23(3.2) 43(5.9) 30(4.2)
Hyperlipidaemia 23(3.2) 26(3.6) 35(4.9)
Dyslipidaemia 12(1.7) 9(1.2) 13(1.8)
VitaminDdeficiency 8(1.1) 6(0.8) 10(1.4)
Gout 8(1.1) 5(0.7) 5(0.7)
Hyperuricaemia 2(0.3) 7(1.0) 5(0.7)
CV-relatedconcomitantmedicationuseduringdoubleblindtreatmentperiod,n(%)
Antihypertensivesa 22(3.0) 17(2.3) 9(1.3)
β- blocking agents 90(12.4) 95(13.0) 101(14.0)
Calcium channel blockers 53(7.3) 49(6.7) 48(6.7)
Agentsactingonrenin-angiotensinsystem 205(28.3) 196(26.9) 194(27.0)
Lipid- modifying agents 119(16.4) 152(20.9) 130(18.1)
Antithromboticagents 97(13.4) 95(13.0) 81(11.3)
Drugs used in diabetes 62(8.6) 95(13.0) 75(10.4)
Cardiac therapy 57(7.9) 74(10.2) 51(7.1)
(Continues)

6 of 15 | DRAKE Et Al.
3.4 | ECG results
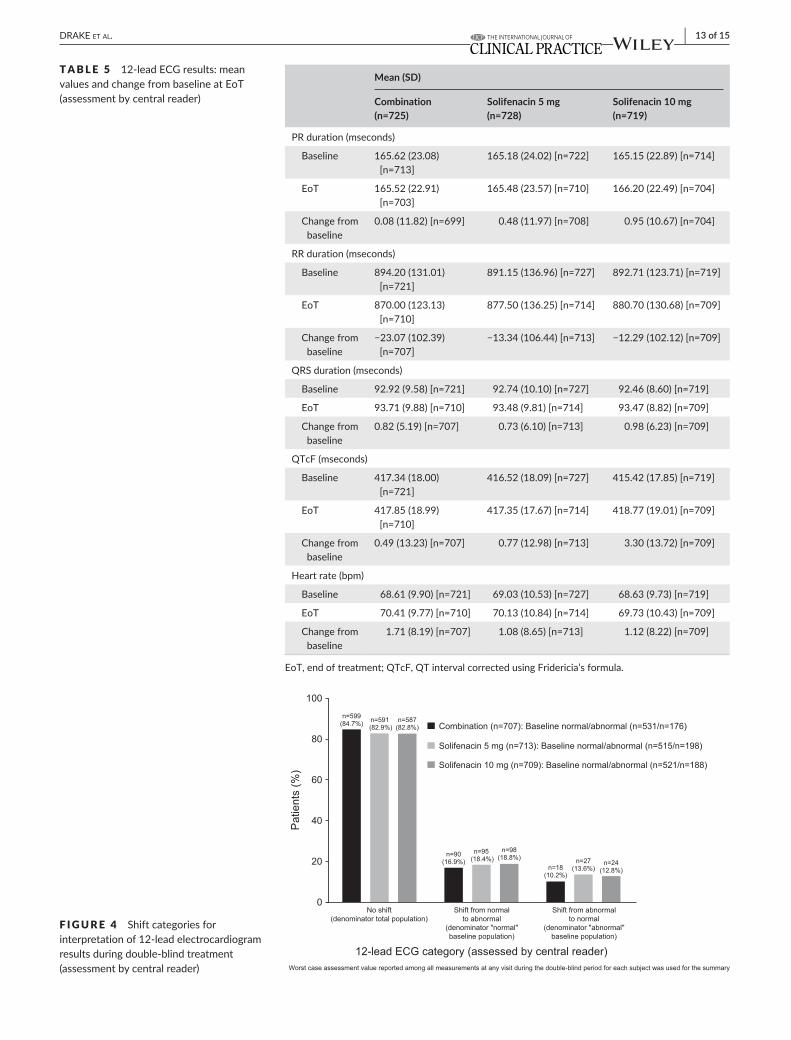
Mean changes from baseline to EoT in ECG parameters (PR, RR,QRS,QTcFandheartrate)weregenerallysimilaracrosstreatmentgroups; the most notable exception being the QTcF, which washigherinthesolifenacin10mg(3.30mseconds)groupvs.combina-tion(0.49mseconds)andsolifenacin5mg(0.77mseconds)(Table5).Thepercentageofpatientswithanormal (~72%-75%)andabnor-mal(~25%-28%)ECGassessmentatbaselineandateachvisitwascomparableacrosseachtreatmentgroup.Thiswasreflectedbytheobservationthat>80%ofpatients ineachgrouphadnochangeinECGinterpretation(Figure4).Duringdouble-blindtreatment,therewerenopatientswithameanQTcFvalue>500mseconds,and11patientshadmeanQTcFvalues>480mseconds (combinationn=4[0.6%]andsolifenacin10mgn=7[1.0%]).Aslightlyhigherpropor-tion of patients in the solifenacin 10 mg group had mean changes from baseline of >30mseconds and >60mseconds in QTcF com-pared with combination and solifenacin 5mg (Figure5A). Therewere no notable treatment differences in QTcF values or changefrom baseline by gender; however, in general, females were more likely to experience a QTcF >450mseconds and >480mseconds,and a change from baseline >60mseconds compared with males(Figure5BandC).
4 | DISCUSSION
CVsafetyconcernsareparticularlyrelevantinchronicmedicalcon-ditionssuchasOAB, inwhichpatientshavea significantlyhigherrateofpre-existingCVcomorbiditiesthanpatientswithoutOAB.8 Of the two oral pharmacotherapies investigated inBESIDE, solif-enacin selectively inhibits the M3 receptor subtype in the para-sympathetic system, and mirabegron selectively stimulates the β3 adrenoceptor in the sympathetic system, hence the potential for
additional systemic effects beyond the bladder, including the heart and vasculature. OAB studies investigating mirabegron mono-therapy (25mg/d or 50mg/d) for 12weeks and 12months, orsolifenacin (5mg/d or 10mg/d)monotherapy for 12weeks havenot demonstrated an increased CV risk, with no clinically rele-vant changes in cardiac function or blood pressure reported.18,19 However, the concomitant exposure to these agents with distinct mechanisms of action raises the potential for a synergistic effect on theCVsystem.
ThisassessmentfromtheBESIDEstudyisthefirsttoinvestigateCVsafetyinOABpatientstreatedwithacombinationofmirabegronandsolifenacin.TheOABpopulationrepresentsareal-lifeclinicalset-ting characterised by refractory, treatment- experienced patients with amoderatelevelofCVrisk(ie,hypertension,diabetes)andpolyphar-macy; almost one- third of the population were controlled hyperten-sivepatients.InthisanalysisofCVsafety,thefrequencyofCVTEAEs,andchangeinvitalsignsandECGresults,werecomparablebetweencombination therapy and solifenacin monotherapy (5mg or 10mg)confirmingnosynergisticeffectontheCVsystemregardlessofpre-existingCV risk factors (eg,hypertensionhistoryorhypertensiveatscreening).
ThefrequencyofCVTEAEsandthemagnitudeofchangeinvitalsignsandECGparameterswithcombinationtherapyisconsistentwithmirabegron and solifenacin monotherapy,18,19 and with other studies that have investigated a combination of mirabegron and solifena-cin in a JapaneseOABpopulation26 and in a Phase II dose-rangingstudy.27Thefrequencyofhypertension(<2%)acrosstreatmentgroupsinBESIDEisconsiderablylowerthanthatreportedwithplaceboandmirabegronmonotherapyinprevious12-weekPhaseIIIstudies(pla-cebon=7.6%,mirabegron50mgn=7.5%).29 However, hypertension was defined using three prespecified criteria in the previous PhaseIIImonotherapytrials,whereas inBESIDEtherewerenopredefinedcriteriaandhypertensionwas reportedasanAE, if consideredclin-ically relevantby the investigator.Similarly, theoverall frequencyof
Combination n=725
Solifenacin 5 mg n=728
Solifenacin 10 mg n=719
Vitalsigns,mean(SD) n=724 n=728 n=719
SBPmmHg 126.73(13.83) 125.63(14.24) 125.88(14.64)
DBPmmHg 76.43(8.31) 76.15(8.63) 75.70(8.41)
Pulseratebpm 71.35(9.62) 71.33(9.47) 71.17(9.20)[n=718]
ECGparameters(Centralreader)n(%) n=721 n=727 n=719
QTcF>450mseconds 31(4.3) 24(3.3) 17(2.4)
QTcF>480mseconds 1(0.1) 1(0.1) 0
QTcF>500mseconds 0 0 0
BMI,bodymassindex;CV,cardiovascular;DBP,diastolicbloodpressure;ECG,electrocardiogram;OAB,overactivebladder;QTcF,QTintervalcorrectedusingFridericia’sformula;SBP,systolicbloodpressure;SE,standarderror.aAlphaadrenoceptorantagonists,imidazolinereceptoragonists,tadalafil,magnesiumsulphate,pyrimidinederivatives,hydrazinophthalazinederivatives,methyldopa, rauwolfia alkaloids.
TABLE 1 (Continued)

| 7 of 15DRAKE Et Al.
TABLE 2 Treatment-emergentadverseevents(TEAEs)(MedRAv16.0)ofinterestrelatedtotheCVsystem,seriousCV-relatedTEAEsandfrequencyofadjudicatedCV-relatedTEAEs(SAF)
TEAEs of interest SOC and PT
Patients, n (%) [95% CI]
Combination (n=725)
Solifenacin 5 mg (n=728)
Solifenacin 10 mg (n=719)
Increased blood pressure
Overall 12(1.7)[0.7to2.6] 6(0.8)[0.2to1.5] 13(1.8)[0.8to2.8]
Vasculardisorders 8(1.1)[0.3to1.9] 5(0.7)[0.1to1.3] 7(1.0)[0.3to1.7]
Hypertension 8(1.1)[0.3to1.9] 5(0.7)[0.1to1.3] 6(0.8)[0.2to1.5]
Hypertensive crisis 0 0 1(0.1)[0.0to0.4]
Investigations 4(0.6)[0.0to1.1] 1(0.1)[0.0to0.4] 6(0.8)[0.2to1.5]
Blood pressure increased 4(0.6)[0.0to1.1] 1(0.1)[0.0to0.4] 6(0.8)[0.2to1.5]
QTprolongation
Overall 1(0.1)[0.0to0.4] 1(0.1)[0.0to0.4] 2(0.3)[0.0to0.7]
Investigations 1(0.1)[0.0to0.4] 1(0.1)[0.0to0.4] 1(0.1)[0.0to0.4]
ECGQTprolonged 1(0.1)[0.0to0.4] 1(0.1)[0.0to0.4] 1(0.1)[0.0to0.4]
Nervous system disorders 0 0 1(0.1)[0.0to0.4]
Syncope 0 0 1(0.1)[0.0to0.4]
Increased heart rate, tachycardia, atrial fibrillation and palpitations
Overall 7(1.0)[0.3to1.7] 5(0.7)[0.1to1.3] 4(0.6)[0.0to1.1]
Cardiac disorders 7a(1.0)[0.3to1.7] 5(0.7)[0.1to1.3] 3(0.4)[0.0to0.9]
Palpitations 6(0.8)[0.2to1.5] 2(0.3)[0.0to0.7] 2(0.3)[0.0to0.7]
Tachycardia 2(0.3)[0.0to0.7] 1(0.1)[0.0to0.4] 0
Atrialfibrillation 0 1(0.1)[0.0to0.4] 0
Supraventricularextrasystoles 0 0 1(0.1)[0.0to0.4]
Ventricularextrasystoles 0 1(0.1)[0.0to0.4] 0
Nervous system disorders 0 0 1(0.1)[0.0to0.4]
Syncope 0 0 1(0.1)[0.0to0.4]
SeriousCV-relatedTEAEs(PTonly)
Arteriogramcoronarynormal 1(0.1) 0 0
Acutemyocardialinfarction 0 0 1(0.1)
Atrialfibrillation 0 1(0.1) 0
Atrioventricularblockcomplete 1(0.1) 0 0
Transientischaemicattack 0 0 1(0.1)
Hypertensive crisis 0 0 1(0.1)
Thrombosis 0 1(0.1) 0
AdjudicatedseriousCV-relatedTEAEs
Overall 4(0.6) 2(0.3) 4(0.6)
APTC/MACECVevents 0 0 1(0.1)
Non- fatal myocardial infarction 0 0 1(0.1)
Non- fatal stroke 0 0 0
CVdeath 0 0 0
Non-APTC/MACECVevents 1(0.1) 2(0.3) 2(0.3)
Unstable angina 0 0 0
Coronary revascularization 0 0 0
Transientischaemicattack 0 0 1(0.1)
Venousandperipheralarterialvascularthromboticevent
0 1(0.1) 0
(Continues)

8 of 15 | DRAKE Et Al.
TEAEs of interest SOC and PT
Patients, n (%) [95% CI]
Combination (n=725)
Solifenacin 5 mg (n=728)
Solifenacin 10 mg (n=719)
Congestive heart failure 0 0 0
Arrhythmia,noevidenceofischaemia 1(0.1) 1(0.1) 0
Otherseriousnon-MACECVevent 0 0 1(0.1)
Other 3(0.4) 0 1(0.1)
Insufficient data 0 0 1(0.1)
Non-CVevent 3(0.4) 0 0
APTC,antiplatelettrialistscollaboration;CV,cardiovascular;ECG,electrocardiogram;MACE,majoradversecardiovascularevent;PT,preferredterm;SOC,systemorganclass;TEAEs,treatment-emergentadverseevents.TEAEreferstoanAEwhichstartedorworsenedintheperiodfromfirstdouble-blindmedicationintakeuntil30daysafterthelastdouble-blindmedicationintake.aOne patient experienced both tachycardia and palpitations; the patient is counted once under each of palpitations and tachycardia, but only once under theSOCcardiacdisorders.
TABLE 2 (Continued)
F IGURE 1 AdjustedchangefrombaselinetoEoTforvitalsignsintheoverallpopulationandbysensitivityanalyses:A,systolicbloodpressure:combinationvs.solifenacin5mgand10mg;B,diastolicbloodpressure:combinationvs.solifenacin5mgand10mg;C,Pulserate:combination vs. solifenacin 5 mg and 10 mg
Systolic blood pressure (mm Hg): combination vs solifenacin 5 mg
1.01 (95% CI: –0.06, 2.07)
–0.67 (95% CI: –7.89, 6.55)
1.74 (95% CI: –0.27, 3.75)
0.64 (95% CI: –0.58, 1.85)
1.68 (95% CI: –1.94, 5.30)
0.85 (95% CI: –0.26, 1.95)
0.88 (95% CI: –0.18, 1.94)
1.05 (95% CI: –0.01, 2.11)
Systolic blood pressure (mm Hg): combination vs solifenacin 10 mg
1.35 (95% CI: 0.29, 2.42)
0.99 (95% CI: –6.26, 8.24)
2.42 (95% CI: 0.40, 4.44)
0.70 (95% CI: –0.51, 1.91)
1.58 (95% CI: –1.96, 5.11)
1.27 (95% CI: 0.16, 2.38)
1.30 (95% CI: 0.24, 2.36)
1.36 (95% CI: 0.30, 2.42)
Overall safety analysis set
Patients with past history of hypertension
Patients hypertensive at screening
Patients with no hypertension at screening
β-blocker users
Non β-blocker users
With age group (<45, ≥45 to <65, ≥65 years)
With antihypertensive use at screening
Overall safety analysis set
Patients with past history of hypertension
Patients hypertensive at screening
Patients with no hypertension at screening
β-blocker users
Non β-blocker users
With age group (<45, ≥45 to <65, ≥65 years)
With antihypertensive use at screening
Adjusted change from baseline to EoT Adjusted change from baseline to EoT–10–10 –5–5 00 5 5 1010
Diastolic blood pressure (mm Hg): combination vs solifenacin 5 mg
0.10 (95% CI: –0.61, 0.82)
1.05 (95% CI: –4.20, 6.30)
0.27 (95% CI: –0.99, 1.52)
0 (95% CI: –0.87, 0.87)
0.85 (95% CI: –1.34, 3.03)
–0.04 (95% CI: –0.80, 0.72)
0.05 (95% CI: –0.67, 0.76)
0.11 (95% CI: –0.60, 0.83)
Diastolic blood pressure (mm Hg): combination vs solifenacin 10 mg
0.13 (95% CI: –0.59, 0.85)
–1.25 (95% CI: –6.60, 4.11)
0.67 (95% CI: –0.59, 1.94)
–0.13 (95% CI: –1.0, 0.74)
0.23 (95% CI: –1.89, 2.36)
0.09 (95% CI: –0.67, 0.86)
0.11 (95% CI: –0.61, 0.82)
0.13 (95% CI: –0.59, 0.85)
Overall safety analysis set
Patients with past history of hypertension
Patients hypertensive at screening
Patients with no hypertension at screening
β-blocker users
Non β-blocker users
With age group (<45, ≥45 to <65, ≥65 years)
With antihypertensive use at screening
Overall safety analysis set
Patients with past history of hypertension
Patients hypertensive at screening
Patients with no hypertension at screening
β-blocker users
Non β-blocker users
With age group (<45, ≥45 to <65, ≥65 years)
With antihypertensive use at screening
Adjusted change from baseline to EoT Adjusted change from baseline to EoT
–10–5 –50 5 0 510
Pulse rate (bpm): combination vs solifenacin 5 mg
Adjusted change from baseline to EoT
0.04 (95% CI: –0.75, 0.82)
–0.64 (95% CI: –6.26, 4.98)
–0.07 (95% CI: –1.42, 1.28)
0.04 (95% CI: –0.93, 1.01)
–0.92 (95% CI: –3.13, 1.28)
0.2 (95% CI: –0.64,1.05)
0.07 (95% CI: –0.72, 0.85)
0.03 (95% CI: –0.75, 0.82)
Pulse rate (bpm): combination vs solifenacin 10 mg
Adjusted change from baseline to EoT
Overall safety analysis set
Patients with past history of hypertension
Patients hypertensive at screening
Patients with no hypertension at screening
β-blocker users
Non β-blocker users
With age group (<45, ≥45 to <65, ≥65 years)
With antihypertensive use at screening
Overall safety analysis set
Patients with past history of hypertension
Patients hypertensive at screening
Patients with no hypertension at screening
β-blocker users
Non β-blocker users
With age group (<45, ≥45 to <65, ≥65 years)
With antihypertensive use at screening
0.19 (95% CI: –0.59, 0.99)
1.12 (95% CI: –4.62, 6.86)
0.07 (95% CI: –1.29, 1.43)
0.21 (95% CI: –0.76, 1.18)
–0.26 (95% CI: –2.42, 1.90)
0.24 (95% CI: –0.60, 1.09)
0.21 (95% CI: –0.58, 0.99)
0.19 (95% CI: –0.59, 0.98)
–5–5–10 00 5 0 5 10
(A)
(B)
(C)
| 9 of 15DRAKE Et Al.
tachycardia(reportedasaTEAEbytheinvestigatororameanpulserate≥100bpm)withcombinationtherapy(1.4%)waslowerthanthatreported with mirabegron 50 mg monotherapy in the previous 12- weekstudies(3.8%).29
ThefrequencyofCVTEAEsreportedinBESIDEcomparesfavour-ablywith the rateofCVevents reported in thegeneralpopulation.In the Framingham study, after 30 years of follow- up, the frequency of hypertension (SBP≥160mmHg andDBP≥95mmHg) increasedwithageinmenfrom3.3%atages30-39to6.2%atages70-79,andinwomenfrom1.5%atages30-39to8.6%atages70-79.30Thefre-quencyoftachycardia(≥100bpm)inthegeneralUSpopulationbasedonnational referencedataonrestingpulserate is1.3% inmenand1.9%inwomen.31
TheonlynotabledifferenceinvitalsignsbetweencombinationandsolifenacinmonotherapyinBESIDEwasthe1mmHgrelative
difference in SBP,whichwas unchangedwith combination ther-apy and decreasedwith solifenacin monotherapy. The negligibleeffects on vital signs are reflected by the fact that only eight pa-tients (combination n=1, solifenacin 5mgn=2, solifenacin 10mgn=5)hadpotentiallysignificantincreasesinbloodpressureduringthe study.
The frequency of ECG QT prolongation was 0.1% in eachtreatmentgroupandtherewerenocasesofextremeQTcFvalues>500 mseconds. Five solifenacin- treated patients experienced a changeinQTcF>60msecondsduringthestudycomparedwithnonein the combination group. Regardless of treatment, female patients weremore likely to experience extremeQTcF values >450msec-onds and >480 mseconds than males, which reflects the observa-tionthatcorrectedQTintervalsaregenerallylongerinwomenthanin men.32
TABLE 3 AdjustedchangefrombaselinetoEoTinvitalsignsbysex
Mean (SE) [95% CI]
Combination Solifenacin 5 mg Solifenacin 10 mg
Males n=119 n=120 n=114
Systolicbloodpressure
Adjustedchangefrombaseline 1.82(0.94)[−0.03to3.67] 1.46(0.93)[−0.37to3.29] 0.89(0.96)[−0.99to2.78]
Difference vs. solifenacin 5 mg 0.36(1.32)[−2.23to2.95]
Difference vs. solifenacin 10 mg 0.92(1.34)[−1.70to3.55]
Diastolic blood pressure
Adjustedchangefrombaseline 1.37(0.63)[0.14to2.61] 1.10(0.63)[−0.13to2.34] 0.43(0.64)[−0.83to1.70]
Difference vs. solifenacin 5 mg 0.27(0.89)[−1.47to2.01]
Difference vs. solifenacin 10 mg 0.94(0.90)[−0.82to2.71]
Pulserate
Adjustedchangefrombaseline 0.28(0.69)[−1.07to1.64] 1.41(0.69)[0.06to2.76] 0.26(0.71)[−1.13to1.65]
Difference vs. solifenacin 5 mg −1.13(0.97)[−3.04to0.79]
Difference vs. solifenacin 10 mg 0.02(0.99)[−1.91to1.96]
Females n=587 n=591 n=592
Systolicbloodpressure
Adjustedchangefrombaseline −0.27(0.42)[−1.10to0.55] −1.41(0.42)[−2.24to−0.59] −1.71(0.42)[−2.53to−0.89]
Difference vs. solifenacin 5 mg 1.14(0.59)[−0.03to2.31]
Difference vs. solifenacin 10 mg 1.44(0.59)[0.27to2.60]
Diastolic blood pressure
Adjustedchangefrombaseline −0.69(0.28)[−1.25to−0.14] −0.76(0.28)[−1.32to−0.21] −0.66(0.28)[−1.22to−0.11]
Difference vs. solifenacin 5 mg 0.07(0.40)[−0.71to0.85]
Difference vs. solifenacin 10 mg −0.03(0.40)[−0.81to0.75]
Pulserate
Adjustedchangefrombaseline 0.50(0.31)[−0.11to1.11] 0.23(0.31)[−0.38to0.84] 0.27(0.31)[−0.33to0.88]
Difference vs. solifenacin 5 mg 0.27(0.44)[−0.59to1.13]
Difference vs. solifenacin 10 mg 0.23(0.44)[−0.63to1.09]
Adjustedchangefrombaselinevaluesand95%CIsaregeneratedfromANCOVAmodelwithtreatmentgroup,gender,agegroup,4-weekincontinencereductiongroup,geographicregionandinteractionbetweenagegroup(<65,≥65years)andtreatmentgroupasfixedfactorsandbaselineasacovariate.Differences of adjusted means are calculated by subtracting adjusted mean of solifenacin treatment from adjusted mean of combination treatment.

10 of 15 | DRAKE Et Al.
A substantial proportion of the BESIDE populationwas takingmedication to control hypertension, which may have concealed po-tential increases in blood pressure; however, this would apply across all treatment arms. Furthermore, the study lacked a placebo arm, whichwouldhaveallowedamorerobustcomparisonofCVsafetybetween active treatment and a control cohort in this refractory in-continentpopulation. In thispaper,CVsafetywasnot reported inpatients stratifiedbyolderage (≥65yearsand≥75years)—theco-hortmostlikelytohavepre-existingCVmorbiditiesandatriskofde-velopingCV-relatedAEs—resultsforthesepatientswillbepresentedinasubsequentanalysisinolderpatientsfromtheBESIDEstudy.
InadditiontothesafetyanalysisinolderpatientsinBESIDE,fu-ture subanalyses using integrated clinical trial data could investigate combinationtherapyvs.placeboinotherhighriskCVpopulations(eg,
diabetes,hypertension,andBMI>30),andcompareoffice-basedvs.ambulatory blood pressure monitoring.
5 | CONCLUSION
InOABpatientstreatedwithacombinationofmirabegronandsolif-enacin,thefrequencyofCV-relatedAEsandchangesfrombaselineinvitalsignsandECGparameterswerecomparablewiththerecom-mended doses of solifenacin monotherapy (5mg and 10mg), indi-catinga lackofasynergisticeffectonCVsafetywithcombination.However, good clinical practice advocates regular blood pressure monitoring in older patientswhere CV riskmay be cumulative be-cause of comorbidities or co- medication.
F IGURE 2 A-C,Patientsmeetingchangefrombaselinecriteriaforsystolicbloodpressure(A),diastolicbloodpressure(B)andpulserate(C)
0
1
2
3
4
5 Combination (n=710)
Solifenacin 5 mg (n=715)
Solifenacin 10 mg (n=709)
Patients meeting change from baselinecriteria for systolic blood pressure
≥10 mm Hg ≥15 mm Hg ≥20 mm Hg
n=24(3.4%)
n=13(1.8%)
n=2(0.3%)
n=31(4.3%)
n=13(1.8%)
n=4(0.6%)
n=26(3.7%)
n=9(1.3%)
n=5 (0.7%)
SBP criteria on three consecutive post-baseline visits
Pat
ient
s (%
)
Pat
ient
s (%
)
0
2
4
6
8
10 Combination (n=710)
Solifenacin 5 mg (n=715)
Solifenacin 10 mg (n=708)
Patients meeting change frombaseline criteria for pulse rate
≥5 bpm ≥10 bpm ≥15 bpm
n=47(6.6%)
n=14(2.0%)
n=5(0.7%)
n=53(7.4%)
n=16(2.2%)
n=2(0.3%)
n=59(8.3%)
n=12(1.7%)
n=1(0.1%)
Pulse rate criteria on three consecutivepost-baseline visits
0
2
4
6
8
10Combination (n=710)
Solifenacin 5 mg (n=715)
Solifenacin 10 mg (n=709)
Patients meeting change from baselinecriteria for diastolic blood pressure
n=53(7.5%)
n=15(2.1%)
n=1(0.1%)
n=56(7.8%)
n=18(2.5%)
n=4(0.6%)
n=57(8.0%)
n=14(2.0%)
n=4(0.6%)
DBP criteria on three consecutive post-baseline visits
Pat
ient
s (%
)
≥5 mm Hg ≥10 mm Hg ≥15 mm Hg
(A) (B)
(C)
| 11 of 15DRAKE Et Al.
TABLE 4 Patientsmeetingchangefrombaselinecriteriainvitalsignsbysubpopulation(basedonpatientswiththreeconsecutivepostbaselinevalues):pasthistoryofhypertension;hypertensiveatscreening;nohypertensionatscreening;β- blocker user; non β- blocker user
Combination Solifenacin 5 mg Solifenacin 10 mg
Pasthistoryofhypertension n=17 n=18 n=17
SBP:increasefrombaseline
≥10mmHg 0 2(11.1%) 0
≥15mmHg 0 0 0
≥20mmHg 0 0 0
DBP:increasefrombaseline
≥5mmHg 0 0 2(11.8%)
≥10mmHg 0 0 1(5.9%)
≥15mmHg 0 0 0
Pulserate:increasefrombaseline
≥5bpm 3(17.6%) 0 0
≥10bpm 2(11.8%) 0 0
≥15bpm 1(5.9%) 0 0
Hypertensive at screening n=255 n=254 n=248
SBP:increasefrombaseline
≥10mmHg 11(4.3%) 10(3.9%) 10(4.0%)
≥15mmHg 4(1.6%) 4(1.6%) 6(2.4%)
≥20mmHg 2(0.8%) 1(0.4%) 3(1.2%)
DBP:increasefrombaseline
≥5mmHg 22(8.6%) 23(9.1%) 21(8.5%)
≥10mmHg 6(2.4%) 8(3.1%) 5(2.0%)
≥15mmHg 0 2(0.8%) 1(0.4%)
Pulserate:increasefrombaseline
≥5bpm 15(5.9%) 23(9.1%) 16(6.5%)[n=247]
≥10bpm 4(1.6%) 10(3.9%) 3(1.2%)[n=247]
≥15bpm 1(0.4%) 1(0.4%) 0
No hypertension at screening n=455 n=461 n=461
SBP:increasefrombaseline
≥10mmHg 13(2.9%) 21(4.6%) 16(3.5%)
≥15mmHg 9(2.0%) 9(2.0%) 3(0.7%)
≥20mmHg 0 3(0.7%) 2(0.4%)
DBP:increasefrombaseline
≥5mmHg 31(6.8%) 33(7.2%) 36(7.8%)
≥10mmHg 9(2.0%) 10(2.2%) 9(2.0%)
≥15mmHg 1(0.2%) 2(0.4%) 3(0.7%)
Pulserate:increasefrombaseline
≥5bpm 32(7.0%) 30(6.5%) 43(9.3%)
≥10bpm 10(2.2%) 6(1.3%) 9(0.2%)
≥15bpm 4(0.9%) 1(0.2%) 1(0.2%)
β- blocker users n=85 n=92 n=101
SBP:increasefrombaseline
≥10mmHg 2(2.4%) 2(2.2%) 4(4.0%)
≥15mmHg 1(1.2%) 2(2.2%) 1(1.0%)
≥20mmHg 0 0 0
(Continues)
12 of 15 | DRAKE Et Al.
F IGURE 3 VitalsignshiftatEoT
0
20
40
60
80
100
Combination (n=710)Solifenacin 5 mg (n=715)Solifenacin 10 mg (n=709)
No shift Categoricalincrease
Categoricaldecrease*
n=579(81.5%)
n=59(8.3%)
n=72(54.1%)
n=569 (79.6%)
n=61(8.5%)
n=85(62.5%)
n=585 (82.5%)
n=48(6.8%)
n=76(56.3%)
Combination (n=710) Solifenacin 5 mg (n=715) Solifenacin 10 mg (n=709)Baseline category:
574 (81.0%)119 (16.8%)16 (2.3%)0
579 (81.0%)124 (17.3%)12 (1.7%)0
577 (81.3%)123 (17.3%)10 (1.4%)0
Severity 1Severity 2Severity 3Severity 4
*Baseline population in severity 1 categoryexcluded as this group could not decreaseto a lower category:Combination (n=133)Solifenacin 5 mg (n=136)Solifenacin 10 mg (n=135)
In the case that a subject has an SBP value falling into one category and a DBP value falling into another category, the subject willbe summarised in the most severe category
Vital sign categories:Severity 1= mean SBP <140 mm Hg and mean DBP <90 mm HgSeverity 2= mean SBP ≥140-159 mm Hg or mean DBP ≥90-99 mm HgSeverity 3= mean SBP ≥160-179 mm Hg or mean DBP ≥100-109 mm HgSeverity 4= mean SBP ≥180 mm Hg or mean DBP ≥110 mm Hg
Pat
ient
s (%
)Combination Solifenacin 5 mg Solifenacin 10 mg
DBP:increasefrombaseline
≥5mmHg 6(7.1%) 4(4.3%) 4(4.0%)
≥10mmHg 2(2.4%) 1(1.1%) 1(1.0%)
≥15mmHg 0 0 0
Pulserate:increasefrombaseline
≥5bpm 4(4.7%) 6(6.5%) 10(9.9%)
≥10bpm 0 3(3.3%) 2(2.0%)
≥15bpm 0 1(1.1%) 0
Non β- blocker users N=622 N=622 N=608
SBP:increasefrombaseline
≥10mmHg 22(3.5%) 29(4.7%) 22(3.6%)
≥15mmHg 12(1.9%) 11(1.8%) 8(1.3%)
≥20mmHg 2(0.3%) 4(0.6%) 5(0.8%)
DBP:increasefrombaseline
≥5mmHg 46(7.4%) 52(8.4%) 53(8.7%)
≥10mmHg 13(2.1%) 17(2.7%) 13(2.1%)
≥15mmHg 1(0.2%) 4(0.6%) 4(0.7%)
Pulserate:increasefrombaseline
≥5bpm 43(6.9%) 47(7.6%) 49(8.1%)[n=607]
≥10bpm 14(2.3%) 13(2.1%) 10(1.6%)[n=607]
≥15bpm 5(0.8%) 1(0.2%) 1(0.2%)[n=607]
DBP,diastolicbloodpressure;SBP,systolicbloodpressure.
TABLE 4 (Continued)
| 13 of 15DRAKE Et Al.
Mean (SD)
Combination (n=725)
Solifenacin 5 mg (n=728)
Solifenacin 10 mg (n=719)
PRduration(mseconds)
Baseline 165.62(23.08)[n=713]
165.18(24.02)[n=722] 165.15(22.89)[n=714]
EoT 165.52(22.91)[n=703]
165.48(23.57)[n=710] 166.20(22.49)[n=704]
Change from baseline
0.08(11.82)[n=699] 0.48(11.97)[n=708] 0.95(10.67)[n=704]
RRduration(mseconds)
Baseline 894.20(131.01)[n=721]
891.15(136.96)[n=727] 892.71(123.71)[n=719]
EoT 870.00(123.13)[n=710]
877.50(136.25)[n=714] 880.70(130.68)[n=709]
Change from baseline
−23.07(102.39)[n=707]
−13.34(106.44)[n=713] −12.29(102.12)[n=709]
QRSduration(mseconds)
Baseline 92.92(9.58)[n=721] 92.74(10.10)[n=727] 92.46(8.60)[n=719]
EoT 93.71(9.88)[n=710] 93.48(9.81)[n=714] 93.47(8.82)[n=709]
Change from baseline
0.82(5.19)[n=707] 0.73(6.10)[n=713] 0.98(6.23)[n=709]
QTcF(mseconds)
Baseline 417.34(18.00)[n=721]
416.52(18.09)[n=727] 415.42(17.85)[n=719]
EoT 417.85(18.99)[n=710]
417.35(17.67)[n=714] 418.77(19.01)[n=709]
Change from baseline
0.49(13.23)[n=707] 0.77(12.98)[n=713] 3.30(13.72)[n=709]
Heartrate(bpm)
Baseline 68.61(9.90)[n=721] 69.03(10.53)[n=727] 68.63(9.73)[n=719]
EoT 70.41(9.77)[n=710] 70.13(10.84)[n=714] 69.73(10.43)[n=709]
Change from baseline
1.71(8.19)[n=707] 1.08(8.65)[n=713] 1.12(8.22)[n=709]
EoT,endoftreatment;QTcF,QTintervalcorrectedusingFridericia’sformula.
TABLE 5 12-leadECGresults:meanvaluesandchangefrombaselineatEoT(assessmentbycentralreader)
F IGURE 4 Shiftcategoriesforinterpretation of 12-lead electrocardiogram results during double- blind treatment (assessmentbycentralreader) Worst case assessment value reported among all measurements at any visit during the double-blind period for each subject was used for the summary
0
20
40
60
80
100
Combination (n=707): Baseline normal/abnormal (n=531/n=176)
Solifenacin 5 mg (n=713): Baseline normal/abnormal (n=515/n=198)
Solifenacin 10 mg (n=709): Baseline normal/abnormal (n=521/n=188)
No shift(denominator total population)
Shift from normalto abnormal
(denominator "normal"baseline population)
n=599(84.7%)
n=90(16.9%)
n=18(10.2%)
n=591 (82.9%)
n=95 (18.4%) n=27
(13.6%)
n=587(82.8%)
n=98(18.8%)
n=24(12.8%)
12-lead ECG category (assessed by central reader)
Shift from abnormalto normal
(denominator "abnormal"baseline population)
Pat
ient
s (%
)

14 of 15 | DRAKE Et Al.
ACKNOWLEDGEMENTS
Thestudywas fundedbyAstellasPharmaEuropeLtd,whichhadarole in the design and conduct of the study; management, analysis and interpretation of the data; and preparation, review and approval of themanuscript.Medicalwritingsupport(preparationoftheinitialandfinaldraftsofthemanuscript incollaborationwiththeauthors)wasprovidedbyStuartMurray,MSc(EnvisionScientificSolutions),fundedbyAstellasPharmaGlobalDevelopment.
DISCLOSURES
MJD has received research grants and consultancy/speaker feesfromAstellas, Allergan and Ferring. SMhas received speaker andconsultancy fees fromAstellas,Allergan,Medtronic andCogentix.CRC has received grants, speaker and consultancy fees from
Astellas, speaker and consultancy fees fromAllergan andBoston,and consultancy fees from Medtronic, Pfizer and Recordati. AEhasnofinancialdisclosurestodeclare.SAhasreceivedgrantsandspeakerfeesfromAstellas,andconsultancyfeesfromAllergan.JCShasreceivedpersonal feesasstudy investigator fromAstellasandGSK. SH has received grants and consultancy fees from Astellas,Allergan and Ipsen, and consultancy fees from Pfizer,Merus andFerring.DMhas received speaker fees fromAstellas.ES,MHandMSareemployeesofAstellas.
AUTHOR CONTRIBUTIONS
MJD,SM,CRC,AE,SA,JCS,DM,SH,ES,MH,MS:concept/design.MJD,SM,CRC,AE,SA,JCS,DM,SH,ES,MH,MS:dataanalysis/inter-pretation.MJD,SM,CRC,AE,SA,JCS,DM,SH,ES,MH,MS:drafting
F IGURE 5 FrequencyofQTintervalcorrectedusingFridericia’sformulaextremevaluesandextremesinchangefrombaselineatanyvisitintheoverallpopulation(A),male(B)andfemalepatients(C);resultsarebasedontheworstpostbaselinemeanvalueduringthedouble-blindtreatment period
0
2
4
6
8
10Combination (n=710/707*)
Solifenacin 5 mg (n=714/713*)
Solifenacin 10 mg (n=709)
QTcF extreme values and extremes inchange from baseline at any visit
QTcF value (ms)
>450 >480 >500
n=55(7.7%)
n=4(0.6%)
n=0
n=17(2.4%)
n=0 n=0n=0
n=53(7.4%)
n=62(8.7%)
n=7(1.0%)
n=0
n=21(2.9%)
n=35(4.9%)
n=2(0.3%)
n=3(0.4%)
Change frombaseline
>30*
Change frombaseline
>60*
Pat
ient
s (%
)
Change frombaseline
>60
0
2
4
6Combination (n=121)
Solifenacin 5 mg (n=121)
Solifenacin 10 mg (n=116)
n=5(4.1%)
n=6(5.0%)
n=6(5.2%)
n=0 n=0 n=0 n=0n=0 n=0
>450
QTcF value (ms)
>480 >500 Change frombaseline
>30
n=0 n=0 n=0
n=3(2.5%)
n=3(2.5%)
n=5(4.3%)
Mal
e pa
tient
s (%
)
Change frombaseline
>60*
0
2
4
6
8
10 Combination (n=589/586*)
Solifenacin 5 mg (n=593/592*)
Solifenacin 10 mg (n=593)
n=50(8.5%)
n=47(7.9%)
n=56(9.4%)
n=4(0.7%)
n=0
n=7(1.2%)
n=0 n=0 n=0
>450
QTcF value (ms)
>480 >500 Change frombaseline
>30*
n=14(2.4%)
n=18(3.0%)
n=30(5.1%)
n=0
n=2(0.3%)
n=3(0.5%)
Fem
ale
patie
nts
(%)
(A)
(C)
(B)

| 15 of 15DRAKE Et Al.
article/critical revision/approval of article.MS: statistics.MJD, SM,CRC,AE,SA,JCS,DM,SH:datacollection.
REFERENCES
1. AbramsP,CardozoL,FallM,etal.Thestandardisationofterminologyoflowerurinarytractfunction:reportfromtheStandardisationSub-committeeoftheInternationalContinenceSociety.Neurourol Urodyn. 2002;21:167-178.
2. DrakeMJ.Doweneed a newdefinition of the overactive bladdersyndrome?ICI-RS2013.Neurourol Urodyn.2014;33:622-624.
3. IrwinDE,KoppZS,AgatepB,MilsomI,AbramsP.Worldwideprev-alence estimates of lower urinary tract symptoms, overactive blad-der, urinary incontinence and bladder outlet obstruction. BJU Int. 2011;108:1132-1138.
4. MilsomI,StewartW,ThuroffJ.Theprevalenceofoveractivebladder.Am J Manag Care.2000;6:S565-S573.
5. Stewart WF, Van Rooyen JB, Cundiff GW, et al. Prevalence andburden of overactive bladder in the United States. World J Urol. 2003;20:327-336.
6. AgarwalA,EryuzluLN,CartwrightR,etal.Whatisthemostbother-some lower urinary tract symptom? Individual- and population- level perspectives for both men and women. Eur Urol.2014;65:1211-1217.
7. SextonCC,CoyneKS,KoppZS,etal.Theoverlapofstorage,voidingand postmicturition symptoms and implications for treatment seek-ing intheUSA,UKandSweden:EpiLUTS..BJU Int.2009;103(suppl3):12-23.
8. Andersson KE, Sarawate C, Kahler KH, Stanley EL, Kulkarni AS.Cardiovascular morbidity, heart rates and use of antimuscarinics in patients with overactive bladder. BJU Int.2010;106:268-274.
9. AnderssonKE,YoshidaM.Antimuscarinicsandtheoveractivedetru-sor – which is the main mechanism of action? Eur Urol. 2003;43:1-5.
10. WuestM,EichhornB,GrimmMO,etal.Catecholaminesrelaxdetru-sor through beta 2- adrenoceptors in mouse and beta 3- adrenoceptors in man. J Pharmacol Exp Ther. 2009;328:213-222.
11. AnderssonKE,CampeauL,OlshanskyB.Cardiaceffectsofmuscarinicreceptor antagonists used for voiding dysfunction. Br J Clin Pharmacol. 2011;72:186-196.
12. WalchL,BrinkC,NorelX.Themuscarinicreceptorsubtypesinhumanblood vessels. Thérapie.2001;56:223-226.
13. BroddeOE,MichelMC.Adrenergicandmuscarinicreceptorsinthehuman heart. Pharmacol Rev.1999;51:651-690.
14. SkeberdisVA,GendvilieneV,ZablockaiteD,etal.Beta3-adrenergicre-ceptor activation increases human atrial tissue contractility and stim-ulates the L- type Ca2+ current. J Clin Invest. 2008;118:3219-3227.
15. VESICARE® (solifenacin succinate) product label. FDA.gov,Revised 2010. http://www.accessdata.fda.gov/drugsatfda_docs/la-bel/2010/021518s008lbl.pdf.AccessedOctober14,2016.
16. Committee for Medicinal Products for Human Use (CHMP).Assessment report:Betmiga.EuropeanMedicinesAgencywebsite.http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/002388/WC500137308.pdf.AccessedNovember10,2016
17. MamanK,AballeaS,NazirJ,etal.Comparativeefficacyandsafetyofmedical treatments for the management of overactive bladder: a sys-tematic literature review and mixed treatment comparison. Eur Urol. 2014;65:755-765.
18. Rosa GM, Bauckneht M, Scala C, et al. Cardiovascular effects ofantimuscarinic agents in overactive bladder. Expert Opin Drug Saf. 2013;12:815-827.
19. Rosa GM, Ferrero S, Nitti V, et al. Cardiovascular safety of β3- adrenoceptor agonists for the treatment of patients with overactive bladder syndrome. Eur Urol.2016;69:311-323.
20. AstellasPharma,Inc.PrescribinginformationforMYRBETRIQ®(mirabe-gron)extendedreleasetablets,fororaluse.Revised2015.http://www.us.astellas.com/docs/Myrbetriq_WPI.pdf.AccessedSeptember1,2015.
21. SextonCC,NotteSM,MaroulisC,etal.Persistenceandadherencein the treatment of overactive bladder syndrome with anticholin-ergic therapy: a systematic review of the literature. Int J Clin Pract. 2011;65:567-585.
22. ChappleCR,KhullarV,GabrielZ,etal.Theeffectsofantimuscarinictreatments in overactive bladder: an update of a systematic review and meta- analysis. Eur Urol.2008;54:543-562.
23. Chancellor MB, Migliaccio-Walle K, Bramley TJ, et al. Long-termpatterns of use and treatment failure with anticholinergic agents for overactive bladder. Clin Ther. 2013;35:1744-1751.
24. Benner JS, Nichol MB, Rovner ES, et al. Patient-reported rea-sons for discontinuing overactive bladder medication. BJU Int. 2010;105:1276-1282.
25. DrakeMJ,ChappleC,EsenAA,etal.Efficacyandsafetyofmirabe-gron add- on therapy to solifenacin in incontinent overactive bladder patients with an inadequate response to initial 4- week solifenacin monotherapy: a randomised double- blind multicentre phase 3B study (BESIDE).Eur Urol.2016;70:136-145.
26. YamaguchiO,KakizakiH,HommaY,etal.Safetyandefficacyofmira-begronas‘add-on’therapyinpatientswithoveractivebladdertreatedwithsolifenacin:apost-marketing,open-labelstudyinJapan(MILAIstudy).BJU Int.2015;116:612-622.
27. AbramsP,KelleherC,StaskinD,etal.Combinationtreatmentwithmi-rabegron and solifenacin in patients with overactive bladder: efficacy and safety results from a randomised, double- blind, dose- ranging, phase2study(Symphony).Eur Urol.2015;67:577-588.
28. MacDiarmid S, Al-Shukri S, Barkin J, et al. Mirabegron as add-ontreatment to solifenacin in patients with incontinent overactive blad-der and an inadequate response to solifenacin monotherapy. J Urol. 2016;196:809-818.
29. NittiV,KhullarV,vanKerrebroeckP,etal.Mirabegronforthetreat-ment of overactive bladder: a prespecified pooled efficacy analysis and pooled safety analysis of three randomised, double- blind, placebo- controlled, phase III studies. Int J Clin Pract.2013;67:619-632.
30. DannenbergAL,GarrisonRJ,KannelWB.IncidenceofhypertensionintheFraminghamStudy.Am J Public Health.1988;78:676-679.
31. OstchegaY,PorterKS,HughesJ,DillonCF,NwankwoT.Restingpulseratereferencedataforchildren,adolescentsandadults:UnitedStates1999- 2008. Natl Health Stat Report.2011;41:1-16.
32. Wolbrette D, Naccarelli G, Curtis A, et al. Gender differences in arrhythmias. Clin Cardiol.2002;25:49-56.
How to cite this article:DrakeMJ,MacDiarmidS,ChappleCR, et al. Cardiovascular safety in refractory incontinent patients with overactive bladder receiving add- on mirabegron therapytosolifenacin(BESIDE).Int J Clin Pract. 2017;71:e12944. https://doi.org/10.1111/ijcp.12944