care coordination home telehealth pamela canter, rn james h quillen va medical center
TRANSCRIPT

CARE COORDINATIONCARE COORDINATIONHome TelehealthHome Telehealth
Pamela Canter, RNPamela Canter, RN
James H Quillen VA Medical James H Quillen VA Medical CenterCenter

Definition of Care CoordinationDefinition of Care Coordination
The wider application of care and case The wider application of care and case management principles to the delivery of management principles to the delivery of healthcare services using health informatics, healthcare services using health informatics, disease management and telehealth to disease management and telehealth to facilitate access to care and to improve the facilitate access to care and to improve the health of designated individuals and health of designated individuals and populations with the specific intent of populations with the specific intent of providing the right care in the right place at providing the right care in the right place at the right time.the right time.
GOALS OF CCHTGOALS OF CCHT
Integration of healthcare environment Integration of healthcare environment to best meet the patient’s needsto best meet the patient’s needs
Proactive delivery of evidence-based Proactive delivery of evidence-based care & Establish continuous healing care & Establish continuous healing relationshipsrelationships
Follow-upFollow-up

EXPECTED OUTCOMESEXPECTED OUTCOMES
Increased access and patient satisfactionIncreased access and patient satisfaction Enhanced functional status and quality of lifeEnhanced functional status and quality of life Increased Provider and CCHT staff satisfactionIncreased Provider and CCHT staff satisfaction Reduced admissions and bed days of careReduced admissions and bed days of care Reduced clinic and ER visitsReduced clinic and ER visits Reduced nursing home admission ratesReduced nursing home admission rates Reduced overall costs for patients with history of Reduced overall costs for patients with history of
frequent admissions and clinic visits.frequent admissions and clinic visits.
CCHT HISTORYCCHT HISTORYEstablished:2004 National roll-out began for CCHT. 1st enrollment for VISN 9 was February 2005.Mission: To coordinate the right care, in the right place, at the right time.Vision: The place of residence is the preferred place of care to provide the “just in time” approach for both the patient and caregiver.Goal – Core Values:
Maximize access to VHA systemPatient Centric ProgrammingIntegrityEvidenced Based PracticeTeamwork/CollaborationFlexibility/Sensibility
Support for Congestive Heart Failure and Diabetes
ELIGIBILITY FOR CCHTELIGIBILITY FOR CCHT Have at least one of the following chronic conditions: Have at least one of the following chronic conditions:
congestive heart failure (CHF), diabetes mellitus (DM), congestive heart failure (CHF), diabetes mellitus (DM), hypertension (HTN) or chronic obstructive pulmonary hypertension (HTN) or chronic obstructive pulmonary disease (COPD) and may have conditions such that disease (COPD) and may have conditions such that technology and care coordination could improve technology and care coordination could improve resource utilization and clinical outcomes. resource utilization and clinical outcomes.
o Requires more than one home-health visit per week due Requires more than one home-health visit per week due to severity of illness and need for monitoring, to severity of illness and need for monitoring, management or education.management or education.
o Patients will have had two (2) or more hospital Patients will have had two (2) or more hospital admissions or emergency room visits in the preceding admissions or emergency room visits in the preceding fiscal year.fiscal year.
o Will be enrolled in a Primary Care Clinic with greater Will be enrolled in a Primary Care Clinic with greater than eight (8) outpatient visits in the preceding fiscal than eight (8) outpatient visits in the preceding fiscal year.year.

Cont. ELIGIBILITY CCHTCont. ELIGIBILITY CCHTo Have greater than ten (10) active medication Have greater than ten (10) active medication
prescriptions.prescriptions. The home environment is such that daily care and The home environment is such that daily care and
medical problems can be managed in the home. Access medical problems can be managed in the home. Access to utilities and safety concerns are addressed for to utilities and safety concerns are addressed for appropriate installation of equipment.appropriate installation of equipment.
The patient and caregiver accept the technology in the The patient and caregiver accept the technology in the home.home.
The patient and caregiver demonstrate competency in The patient and caregiver demonstrate competency in using and maintaining telehealth equipment.using and maintaining telehealth equipment.
Other circumstances that may improve quality of life and Other circumstances that may improve quality of life and improve clinical outcomes.improve clinical outcomes.
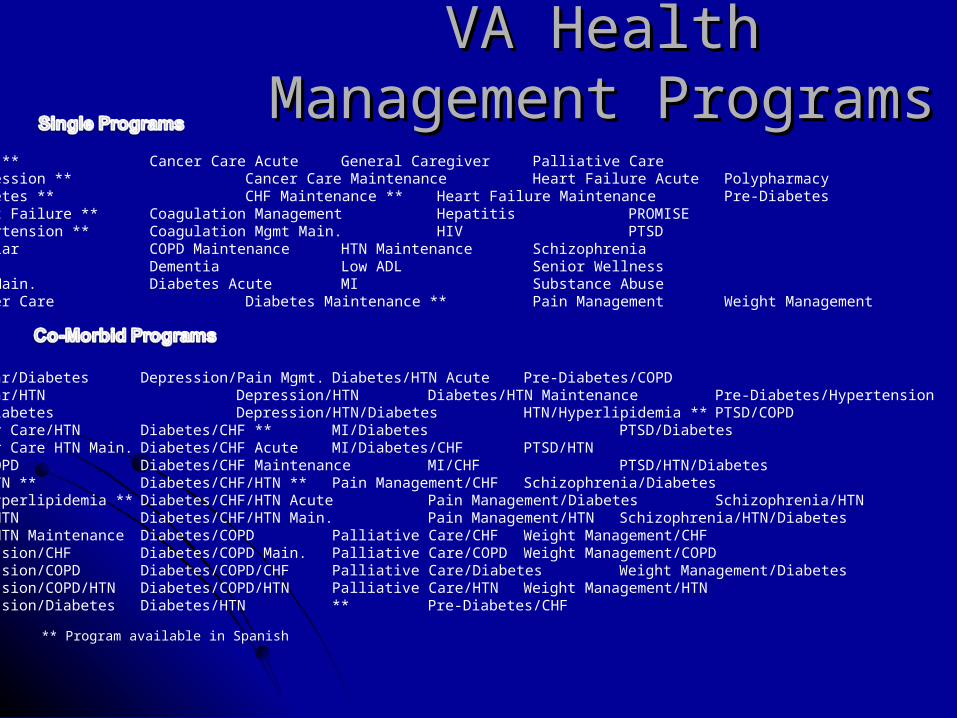
VA Health VA Health Management ProgramsManagement Programs
** Program available in Spanish
COPD ** Cancer Care Acute General Caregiver Palliative CareDepression ** Cancer Care MaintenanceHeart Failure Acute Polypharmacy Diabetes ** CHF Maintenance ** Heart Failure Maintenance Pre-DiabetesHeart Failure ** Coagulation Management Hepatitis PROMISEHypertension ** Coagulation Mgmt Main. HIV PTSDBipolar COPD Maintenance HTN Maintenance SchizophreniaCAD Dementia Low ADL Senior WellnessCAD Main. Diabetes Acute MI Substance AbuseCancer Care Diabetes Maintenance ** Pain Management Weight Management
Bipolar/Diabetes Depression/Pain Mgmt. Diabetes/HTN Acute Pre-Diabetes/COPDBipolar/HTN Depression/HTN Diabetes/HTN Maintenance Pre-Diabetes/HypertensionCAD/Diabetes Depression/HTN/Diabetes HTN/Hyperlipidemia ** PTSD/COPDCancer Care/HTN Diabetes/CHF ** MI/Diabetes PTSD/DiabetesCancer Care HTN Main. Diabetes/CHF Acute MI/Diabetes/CHF PTSD/HTNCHF/COPD Diabetes/CHF Maintenance MI/CHF PTSD/HTN/DiabetesCHF/HTN ** Diabetes/CHF/HTN ** Pain Management/CHF Schizophrenia/DiabetesCHF/Hyperlipidemia ** Diabetes/CHF/HTN Acute Pain Management/Diabetes Schizophrenia/HTNCOPD/HTN Diabetes/CHF/HTN Main. Pain Management/HTN Schizophrenia/HTN/DiabetesCOPD/HTN Maintenance Diabetes/COPD Palliative Care/CHF Weight Management/CHFDepression/CHF Diabetes/COPD Main. Palliative Care/COPD Weight Management/COPDDepression/COPD Diabetes/COPD/CHF Palliative Care/Diabetes Weight Management/DiabetesDepression/COPD/HTN Diabetes/COPD/HTN Palliative Care/HTN Weight Management/HTNDepression/Diabetes Diabetes/HTN ** Pre-Diabetes/CHF


Health Buddy 3 a Look Health Buddy 3 a Look Inside the BoxInside the Box

Health Buddy 3Health Buddy 3
HB 3 must have ROM Build number 49714 or greater to use Ethernet connection
•110V power outlet
•Standard single-line telephone
Dial tone only (not pulse or VOIP)
Analog line (not digital)
No cellular connection
One digit outside line access code
•DSL Filter - The Health Buddy appliance has a modem inside of the appliance that can interfere with telephone lines that also share a DSL connection. If a patient has a DSL line ask them to contact their DSL provider to install a filter. This picture is an example of a filter.
What does the patient need
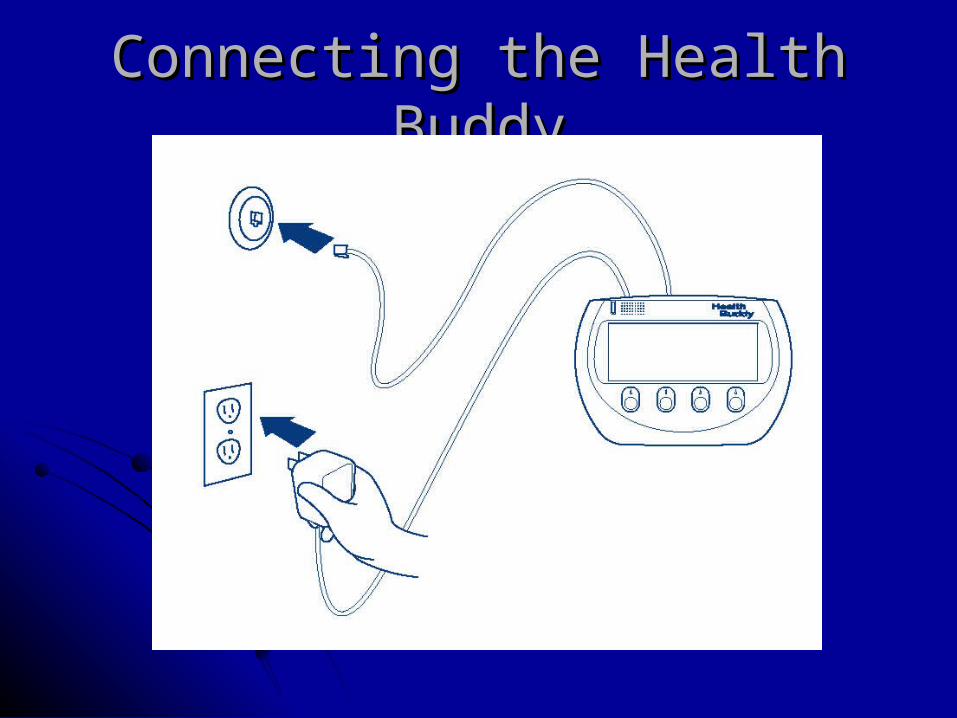
Connecting the Health Connecting the Health BuddyBuddy
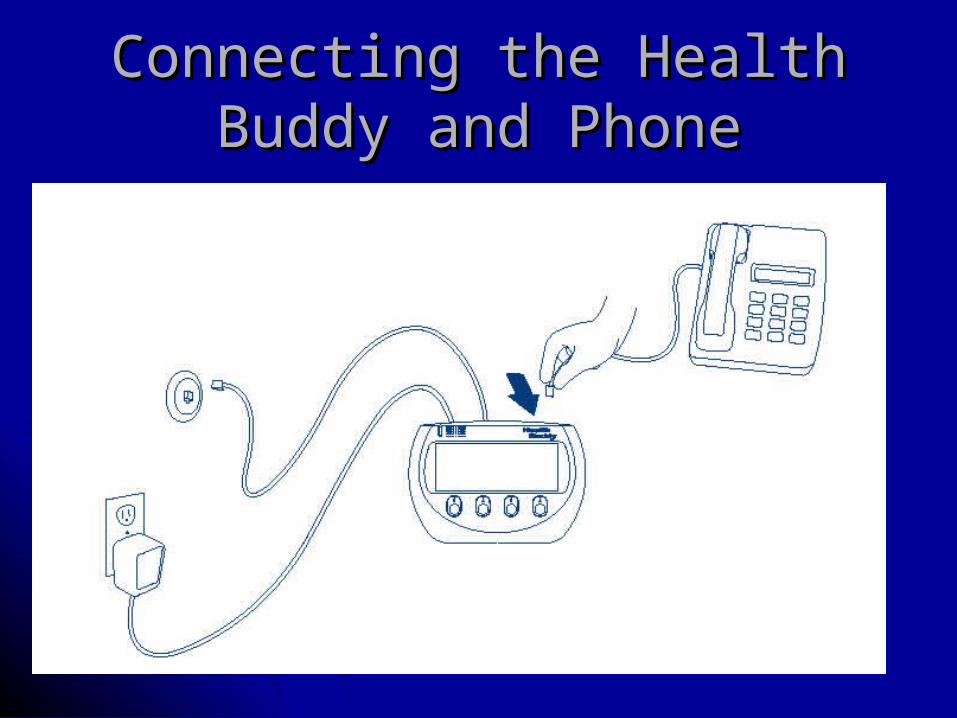
Connecting the Health Connecting the Health Buddy and PhoneBuddy and Phone

Medical Devices Medical Devices Visit
www.healthbuddy.com for a complete list of Medical Devices that
can connect via a cable, Blue Tooth or InfraRed to the Health Buddy 2 and or Health Buddy 3

The Patient’s First The Patient’s First ExperienceExperience
Once the patient has successfully set up the Health Buddy and the green light is on, they press start to begin.
The patient will be presented with a tutorial that guides them through how to use the 4 blue buttons to answer questions.









Health Buddy Results are sent to a VA Secure Data Center where the Care Coordinator can access Health Buddy Patient Results on their computer.
Health Buddy® System


FY2009 – 1FY2009 – 1stst quarter Bed Days quarter Bed Days of Care Cost Avoidance of Care Cost Avoidance
PreCCHT PostCCHT Summary of Avoidance
Pt’s Disch’s Cost Pt’s Disch’s Cost
site Pt’s Disch’s Cost
117 201 $1,829,129.56 74 137 $1,231,291.81 43 64 $597,837.75
123 231 $2,158,300.45 60 126 $1,129,843.09 63 105 $1,028,457.36
144 237 $2,360,505.46 84 140 $2,143,888.55 60 97 $216,616.91
41 70 $1,160,888.25 25 36 $460,871.60 16 34 $700,016.65
63 106 $1,095,371.14 46 80 $1,257,976.90 17 26 -$162,605.76
152 257 $3,171,639.81 89 161 $1,735,614.38 63 96 $1,436,025.43
640 1102 $11,775,834.67 378 680 $7,959,486.33
TOTALS 262 422 $3,816,348.34

FY2009 – 6 months follow up FY2009 – 6 months follow up Cost AvoidanceCost Avoidance
Eligible for FY09 Outcomes
Eligible for FY09 Outcomes
Eligible for FY09 Outcomes
Eligible for FY09 Outcomes
Eligible for FY09 Outcomes
Eligible for FY09 Outcomes
Eligible for FY09 Outcomes
PatientsPatients with Outcomes
BDOC Baseline
BDOC Followup
BDOC % Change
Admission Baseline
Admission Followup
40 40 61 52 -14.8% 14.5 11
50 50 54.5 38 -30.3% 16 13
32 31 81 29 -64.2% 15 10
73 71 259 73 -71.8% 21.5 18
45 45 144.5 63 -56.4% 13 13
39 38 89 37 -58.4% 16.5 11
279 275 689 292 -57.6% 96.5 76
Calc BDOC Diff Cost per BDOC
9 2483 $22,347.00
16.5 1626 $26,829.00
52 2106 $109,512.00
186 1689 $314,154.00
81.5 1584 $129,096.00
52 1452 $75,504.00
$677,442.00

Emergency Room/Primary Care Emergency Room/Primary Care VisitsVisits
PreCCHT PostCCHT Summary of Avoidance
Pt’s Encounter Cost Pt’s Encounter Cost
site Pt’s Encounter Cost
490 3226 $585,240.52 457 2862 $568,203.02 33 364 $17,037.50511 2463 $564,165.76 421 1766 $424,957.25 90 697 $139,208.51358 2022 $472,575.80 319 1639 $398,000.99 39 383 $74,574.81289 1247 $254,048.26 245 942 $198,541.26 44 305 $55,507.00440 2002 $415,600.78 404 1671 $362,590.02 36 331 $53,010.76756 3071 $633,266.81 611 2362 $468,994.46 145 709 $164,272.35
2844 14031$2,924,897.93 2457 11242 $2,421,287.00
TOTALS 387 2789 $503,610.93
DISCHARGE FROM CCHTDISCHARGE FROM CCHT
Care Coordination/Home Telehealth may be Care Coordination/Home Telehealth may be terminated when:terminated when:
1)1) The patient is admitted to a nursing home The patient is admitted to a nursing home setting as a long-term or permanent placement.setting as a long-term or permanent placement.
2)2) The patient/caregiver no longer wish to The patient/caregiver no longer wish to participate in the project.participate in the project.
3)3) The patient has permanently relocated The patient has permanently relocated outside of treatment area.outside of treatment area.
4)4) The patient has achieved clinical goals.The patient has achieved clinical goals.

Remote Education- FindingsRemote Education- FindingsCHF/DIABETESCHF/DIABETES
Enrolled patients had similar:Enrolled patients had similar: Achievement of behavior change goalsAchievement of behavior change goals Decreased unscheduled PC visitsDecreased unscheduled PC visits Improvement in HbA1cImprovement in HbA1c Improvements in quality of lifeImprovements in quality of life
High patient satisfactionHigh patient satisfaction
ConclusionsConclusions
Telehealth is:Telehealth is:FeasibleFeasibleAcceptable to patients & providersAcceptable to patients & providersCan improve care Can improve care