care wars: the bpci force awakens
TRANSCRIPT

Care Wars: The BPCI Force AwakensMay 4, 2016
Alexander Strachan, Jr., MD, MBAAsim Usman, MD

Your Presenters
Asim Usman, MD Divisional Executive Vice President
EmCare
Alexander Strachan, Jr., MD, MBADivisional Executive Vice President
EmCare

3
Bundled Payments for Care Improvement(BPCI)
Per CMS: The Bundled Payments for Care
Improvement (BPCI) initiative is comprised of
four broadly defined models of care, which link payments for the multiple
services beneficiaries receive during an episode of care.

4
Shift in Payment Methodology
Chart Courtesy of Remedy Partners – The Episodes of Care CompanyData Source: www.CMS.gov Retrieved January 26, 2015
Category 1 Fee for Service Category 2 Fee for Service Link to Quality
Category 3 Alternative Payment Model Built on FFS
Architecture
Category 4 Population-based Payment
Payments based on volume – no link to
quality
A portion of payments vary by quality or efficiency of care
delivery
Some payment linked to population
management or episode; triggered by delivery of services; shared savings or 2
sided risk
Payment for population management; not linked
to volume; pay care of person for long period
of time (> a year)
•Hospital Value Based Purchasing
•MD Value Modifier•Readmissions Penalties
•Hospital Acquired Conditions
•Bundled Payments•ACOs
•Medical Homes•Comp Primary Care•Medicare Medicaid Financial Alignment
•Eligible Pioneer ACOs years 3-5

5
Bundled Payments for Care Improvement4 Models
Innovation ModelsBPCI Model 1: Retrospective Acute Care Hospital Stay Only
BPCI Model 2: Retrospective Acute & Post Acute Care Episode
BPCI Model 3: Retrospective Post Acute Care Only
BPCI Model 4: Prospective Acute Care Hospital Stay Only

6
What are bundled payments? Single fixed payment amounts designed to pay all the providers involved for coordinating and covering an episode of care• Hospitals• Physicians• Physical therapy• Readmissions
The bundled payment approach is leading to:
• Better coordinated care• Improved efficiencies• Simplification of processes and billing• Savings
Source: The Advisory Board Company. What are bundled payments? Video | September 04, 2013. Retrieved on May 3, 2016 from https://www.advisory.com/research/health-care-advisory-board/multimedia/video/2013/what-are-bundled-payments

7
Gain vs. Risk Bundled payments offer the potential for gain as well as risk for loss.
Betting on:
• Delivering the same (or better) care at less cost
• Cooperation from all stakeholders
• Smooth coordination
Source: The Advisory Board Company. What are bundled payments? Video | September 04, 2013. Retrieved on May 3, 2016 from https://www.advisory.com/research/health-care-advisory-board/multimedia/video/2013/what-are-bundled-payments

8
Types of AwardeesA BPCI participant is a Facilitator Convener if it will not bear risk, but would like to facilitate other organizations (called Designated Awardees and Designated Awardees Conveners) that take risk for redesigning care under an episode payment model.
Applicants
Risk-Bearing
Awardee Awardee Convener
Non-Risk-Bearing
Facilitator Convener

9
Description of Roles in BPCI:Submission
Type
Risk-Bearing
Single Awardee (Episode Initiator)
Awardee Convener
Episode Initiator
Non-Risk-Bearing
Facilitator Convener
Designated Awardee (Episode Initiator) This entity takes risk under the facilitator convener.
Designated Awardee Convener
This entity takes risk under the facilitator
convener.
Episode Initiator

10
BPCI Fast Facts
The Bundled Payments for Care
Improvement (BPCI) Initiative
≈181 DRGs collapsed into 48 Clinical Episodes
Includes Part A & B (Model 2 and 3)
30, 60, or 90 day episodes
Funds Flow: FFS directly to providers
(reconciled retrospectively)
11
BPCI Fast Facts
Base Pricing: Based on provider's average Part A & B payments (7/09 – 6/12) less 2 or
3% discount
Gainsharing Waiver: Organizing entities
("Conveners") share savings with other
providers
Conveners work with Episode Initiators
Very large scale 3+ year demonstration in
50 states

12
Mechanic R. N England J Med 2014;370:692-694.
Medicare Acute and Post-Acute CarePayments for 30-Day Episodes That Began with a Hospitalization, 2008.

13
Hospitalists and Emergency Physicians Have Increasing Influence in the Value-Focused Healthcare Economy
Concept from Michael Porter, author of Competitive StrategiesRetrieved on April 26, 2016 from http://maaw.info/ArticleSummaries/ArtSumPorter96.htm
Quality &
Access
Cost
Productivity Frontier1. Operational Excellence2. Optimal Care Coordination

14
5%
3%
1%5%
15%
Anchor Admit SNF Readmits OutpatientIRF LTACH HHA Part B
Source: Remedy Partners
Anchor
Admit
33%
SNFReadmits 22% 17%
Spending Distribution within 90-Day Bundles Average Spend per Bundle: $29,991
“Manageable Post-Acute Costs” represent 39% or $11,700 of bundle
Episode Cost Breakdown

15
Pre-discharge Visits Planned Clinician Visits 24/7 Unplanned Care Telephone Support
SNFRehab
LTAC
Home Health
Home
H
Continuum of Care

16
Post Acute Care Settings

17
Post Acute Care Spend Variation
18
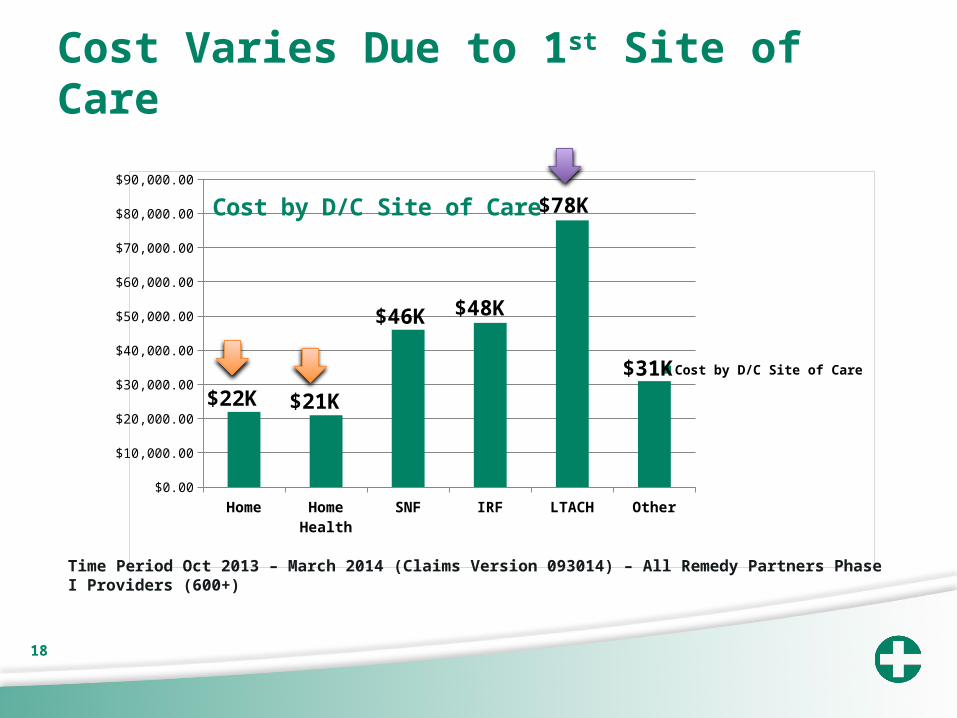
Cost Varies Due to 1st Site of Care
Home Home Health
SNF IRF LTACH Other$0.00
$10,000.00
$20,000.00
$30,000.00
$40,000.00
$50,000.00
$60,000.00
$70,000.00
$80,000.00
$90,000.00
Cost by D/C Site of Care
Cost by D/C Site of Care
Time Period Oct 2013 – March 2014 (Claims Version 093014) – All Remedy Partners Phase I Providers (600+)
$22K $21K
$46K $48K
$78K
$31K
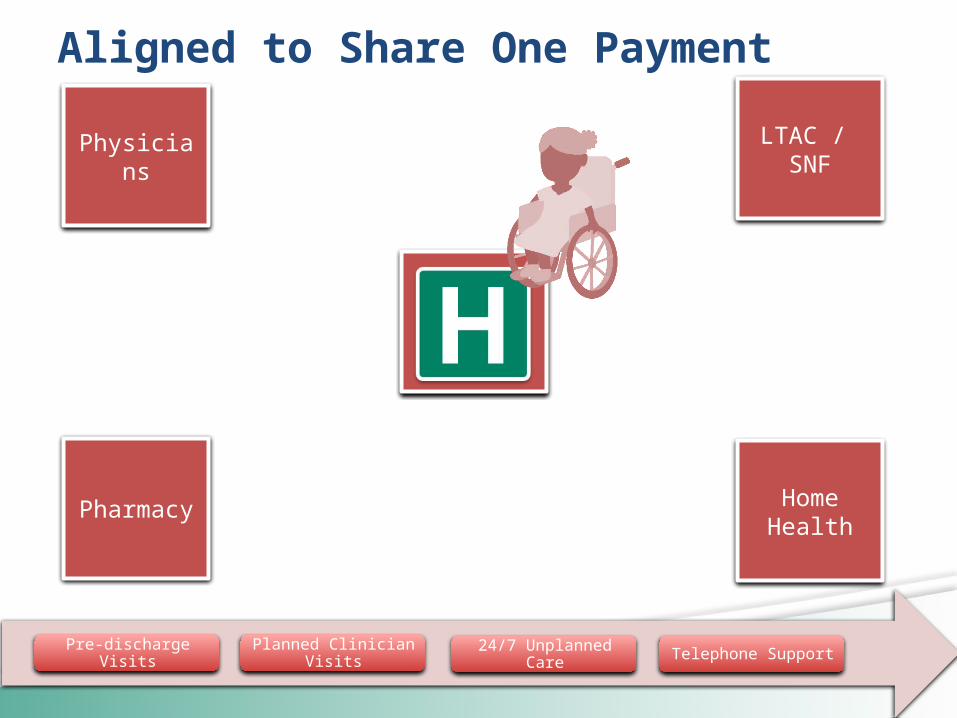
19 Pre-discharge Visits Planned Clinician Visits 24/7 Unplanned Care Telephone Support
Aligned to Share One Payment
Physicians
Pharmacy
LTAC / SNF
Home Health

20
ALOS in Days by Age Group Trends from 1970-2010
Source: Data from: http://www.cdc.gov/nchs/data/series/sr_13/sr13_165.pdf , http://www.cdc.gov/nchs/data/series/sr_13/sr13_168.pdfhttp://www.cdc.gov/nchs/data/nhds/2average/2007ave2_ratesexage.pdf, http://www.cdc.gov/nchs/data/nhds/2average/2008ave2_ratesexage.pdfhttp://www.cdc.gov/nchs/data/nhds/2average/2009ave2_ratesexage.pdf, http://www.cdc.gov/nchs/data/nhds/2average/2010ave2_ratesexage.pdf Hall MJ, DeFrances CJ, Williams SN, Golosinskiy A, Schwartzman A. National Hospital Discharge Survey: 2007 summary. National health statistics reports; no 29. Hyattsville, MD: National Center for Health Statistics. 2010. Retrieved April 26, 2016 from http://www.cdc.gov/nchs/data/nhsr/nhsr029.pdf
1970 1980 1985 1990 1995 2000 2005 2006 2007 2008 2009 20100
2
4
6
8
10
12
14
All Ages Under 15 15-44 45-64 65 and over
Patients Discharged Earlier (Sicker)

21
Timeline for Change is Short
“HHS reaches goal of tying 30 percent of Medicare payments to quality ahead of schedule…”
Retrieved April 21, 2016 from http://www.hhs.gov/about/news/2016/03/03/hhs-reaches-goal-tying-30-percent-medicare-payments-quality-ahead-schedule.html# and http://www.hhs.gov/about/news/2015/01/26/better-smarter-healthier-in-historic-announcement-hhs-sets-clear-goals-and-timeline-for-shifting-medicare-reimbursements-from-volume-to-value.html
85%
All Medicare FFS (Categories 1-4) FFS Linked to quality (Categories 2-4)
Alternative payment models (Categories 3-4)
2016 2018
30%
85%
50%
90%

22
Gaps in Care
Based on Medicare claims data from 2003–2004N Engl J Med 2009;360:1418-28. Retrieved April 20, 2016 from http://www.compassionandsupport.org/pdfs/about/Jencks_-rehospitalization_among_pts_in_the_medicare_fee_for_service_program_-_2009.pdf
0
20
40
60
80
100
120
Lack of follow-up with PCP leads to readmissions
“Almost one fifth (19.6%) of the 11,855,702 Medicare beneficiaries who had been discharged from a hospital were rehospitalized within 30 days”
“In the case of 50.2% of the patients who were rehospitalized within 30 days after a medical discharge to the community, there was no bill for a visit to a physician’s office between the time of discharge and rehospitalization.”
{ }30-day readmissions50% No PCP follow-up
The New England Journal of Medicine - Special ArticleRehospitalizations among Patients in the Medicare Fee-for-Service ProgramStephen F. Jencks, M.D., M.P.H., Mark V. Williams, M.D., and Eric A. Coleman, M.D., M.P.H.

23
BPCI – Likely to Grow in SizeUS healthcare spend through bundled payments
Share of relevant market
in long-term
Source: CMS, Kaiser Family Foundation, industry participants, lit search, AHA, AIS

24
Cost Variation Across & Within Episodes
DME
Part B
OP
Readmits
HHA
SNF
IRF
LTCH
Anchor

25
Spending Shifts
MedPac - Spending in PAC has more than
doubled from 2001-2013 ($27 billion to $59 billion)
IOM - CMS spent $28 billion on skilled-nursing
care in 2013, up from $13.6 million in 2001
Source: National Health Policy Forum 2012 Report - http://www.nhpf.org/library/issue-briefs/IB847_PostAcutePayment_12-07-12.pdf

26
BPCI Opportunity
Home, Home, HomeThe biggest area of waste SNF utilization
•20-25% of episode costs, with significant variation
The biggest adverse outcome Readmissions•12% of all episode costs
Sample 90-Day Medicare Spending Breakdown
Anchor Admission; 35.30%
Long-term Care; 1.60%
Inpatient Rehab; 3.20%
Skilled Nursing Facility, 24.50%
Home Health; 4.40%
Readmission; 11.90%
Outpatient; 5.00%
Part B; 13.00%
Durable Medical Equipment; 1.10%

The light at the end of the tunnelmay be an oncoming train.

28
ALOS for Hip Replacement
Includes only four listed procedures in this analysis.
SOURCE: CDC/NCHS, National Hospital Discharge Survey, 2000–2010.
Average length of stay among inpatients aged 45 and over with total hip replacement: United States, 2000–2010
CDC Report - Retrieved from http://www.cdc.gov/nchs/products/databriefs/db186.htm

29
Making Bundling Mandatory
Because CJR is the continuation of a trend towards value-based care that has accelerated over time and CMS has very publicly committed to pushing it forward.CMS has been leading the charge (followed by commercial payers) in shifting risk to providers and making payments based on quality and outcomes as opposed to volume.
We all should have seen this coming.
CJR — Why you should have seen it coming and where is this all going? Written by Paul Jawin, JD, | December 07, 2015. Retrieved April 28, 2016 from http://www.beckershospitalreview.com/hospital-physician-relationships/cjr-why-you-should-have-seen-it-coming-and-where-is-this-all-going.html
30
Making Bundling Mandatory
• Payed a fixed amount (hospital wins or loses)
DRG system shifted some risk to the hospital
New in bundled payment - includes a period of post-acute care
CJR — Why you should have seen it coming and where is this all going? Written by Paul Jawin, JD, | December 07, 2015. Retrieved April 28, 2016 from http://www.beckershospitalreview.com/hospital-physician-relationships/cjr-why-you-should-have-seen-it-coming-and-where-is-this-all-going.html

31
Making Bundling Mandatory
Two bundled payment programs leading up to CJR
• Cardiovascular and orthopedic episodes
Acute Care Episode (ACE) – 2009
• Voluntary national program
CMS launched BPCI – 2013
CJR — Why you should have seen it coming and where is this all going? Written by Paul Jawin, JD, | December 07, 2015. Retrieved April 28, 2016 from http://www.beckershospitalreview.com/hospital-physician-relationships/cjr-why-you-should-have-seen-it-coming-and-where-is-this-all-going.html
32
Making Bundling Mandatory
Choose from 48 episodes of care
Choose between a 30 and 90 day post-acute period
Permitted to take the economic risk on the episode of care
CJR — Why you should have seen it coming and where is this all going? Written by Paul Jawin, JD, | December 07, 2015. Retrieved April 28, 2016 from http://www.beckershospitalreview.com/hospital-physician-relationships/cjr-why-you-should-have-seen-it-coming-and-where-is-this-all-going.html

33
CJR is Mandatory
• Based on BPCI Model 2 • Limited to the Total Joint Replacement
episode of care• Mandatory• Hospital put at risk by CMS
CJR is a direct offshoot of these prior programs
CJR — Why you should have seen it coming and where is this all going? Written by Paul Jawin, JD, | December 07, 2015. Retrieved April 28, 2016 from http://www.beckershospitalreview.com/hospital-physician-relationships/cjr-why-you-should-have-seen-it-coming-and-where-is-this-all-going.html

34
Mandatory for Hospitals – Not Patients
Maybe I will.Maybe I won’t.

35
Where is all this going?
CMS announced 1/16/15: By 2016, 30% of
payments through ACOs and Bundles
Up to 50% of all payments by 2018
The Health Care Transformation Task Force • Shift 75% of their business to
contracts with incentives for quality and lower-cost by 2020
36
A Glimpse of the Future
CMS goals makes risk shifting programs mandatory
Will not stop at the 50%
It is critical to: • Understand your costs• Collect and analyze
your claims data• Redesign and
coordinate care across all providers
• Design incentives for alignment

37
What Does it Take to Succeed?

38
What Does it Take to Succeed?

39
New Business Imperative: Care Process Redesign
In order to achieve
success, we have to
“redesign care”
This includes clinical and non-clinical
care process
We decided to take a
process-oriented “project
management” approach
We decided to involve and engage all
stakeholders

40
What Do Our Hospitalists Have to Do?
Documentation excellence:
DRG distribution and
impact
Think more carefully about discharge level
of care and discharge
destination: CARL tool, etc.
Care Coordination:
TCC RNs, APPs
Readmission reduction:
partner with home health,
PCP and SNFists:
narrow network
Consider palliative care
when appropriate

41
Envision Healthcare
Focus: improving the value of post-
acute care by optimizing post-
acute spending—driven mostly by SNF costs—and
minimizing avoidable
readmissions.
Stakeholders must work together:
Control costs.Maximize patient
outcomes.
Must engage the patient in self-
management post-discharge.
Effective health coaching.
Participate in monitoring and
managing health-related social
factors.

42
Additional ResourcesKaiser: Payment and Delivery System Reform in Medicare A PRIMER ON MEDICAL HOMES, ACCOUNTABLE CARE ORGANIZATIONS, AND BUNDLED PAYMENTS http://files.kff.org/attachment/report-payment-and-delivery-system-reform-in-medicare-a-primer-on-medical-homes-accountable-care-organizations-and-bundled-payments
Health Care Costs: A Primer http://kff.org/report-section/health-care-costs-a-primer-2012-report/
AHA: Moving Towards Bundled Payment http://www.aha.org/content/13/13jan-bundlingissbrief.pdf
CMS: Better Care, Smarter Spending, Healthier People: Improving Our Health Care Delivery System https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2015-Fact-sheets-items/2015-01-26.html
H&HN: Bundled Payments http://www.hhnmag.com/articles/5694-bundled-payment
Becker’s Hospital Review: CJR — Why you should have seen it coming and where is this all going? http://www.beckershospitalreview.com/hospital-physician-relationships/cjr-why-you-should-have-seen-it-coming-and-where-is-this-all-going.html
The Advisory Board Company: 'Bring it on': Why one hospital says it's fired up for mandatory bundles https://www.advisory.com/daily-briefing/2015/09/28/fired-up-for-mandatory-bundles