caring for the patient with chronic low back pain: …
TRANSCRIPT

CARING FOR THE PATIENT WITH CHRONIC LOW BACK PAIN:
AN OSTEOPATHIC AND NONOPIOID APPROACH
J’Aimee Lippert, D.O.Department of Osteopathic Manipulative Medicine

OBJECTIVESBy the completion of this educational experience, participants will:
1. Understand the personal, societal, and medical implications of chronic low back pain.
2. Explore the multidisciplinary approaches that can be offered to patients experiencing chronic low back pain.
3. Review and be able to describe the functional anatomy of the lumbar spine, pelvis, and sacrum.
4. Develop a practical approach to physical examination, identification of somatic dysfunction, and documentation of findings specific to this clinical scenario.

OBJECTIVES5. Learn and advance manipulative medicine skills
that are indicated in the care plan for patients experiencing chronic low back pain, specifically focused on myofascial release and muscle energy technique.
6. Formulate a treatment approach incorporating OMM in the medical decision-making process.

Low Back Pain• One of the most common reasons patients see
their primary care physician• 60-80% of adults will have a disabling episode
of low back pain in their lives• ~25% of industrial injuries are due to LBP, but it
accounts for nearly 90% of workman’s compensation costs

Pain Generators in the Low Back• Muscle strain/sprain• Intervertebral disc (e.g., annular tears)• Disc herniations with nerve root impingement• Ligaments• Fascia• Articulations (including joint capsules)• Biomechanical fault

Making the Diagnosis• History and physical exam account for 90% of
what is needed• Ancillary testing: x-rays, CT, MRI, EMG/NCT,
discography, myelograms, labs• 60-70% of cases of low back pain are diagnosed
as idiopathic• 35-45% of asymptomatic people will have
positive imaging studies, including herniations
Red Flags to Consider• Age < 18 yrs or > 50• Weight loss• History of cancer (personal or familial)• Fever, night sweats• Progressive motor weakness• Symptoms of neurologic compromise

Treatment Dilemmas• Most acute back pain is self-limiting• Acute LBP has a high recurrence rate• High risk of developing chronicity• Multifactorial etiology• Psychosocial issues• Narcotic pain medication

Functional Anatomy• Osseous• Ligamentous• Muscular
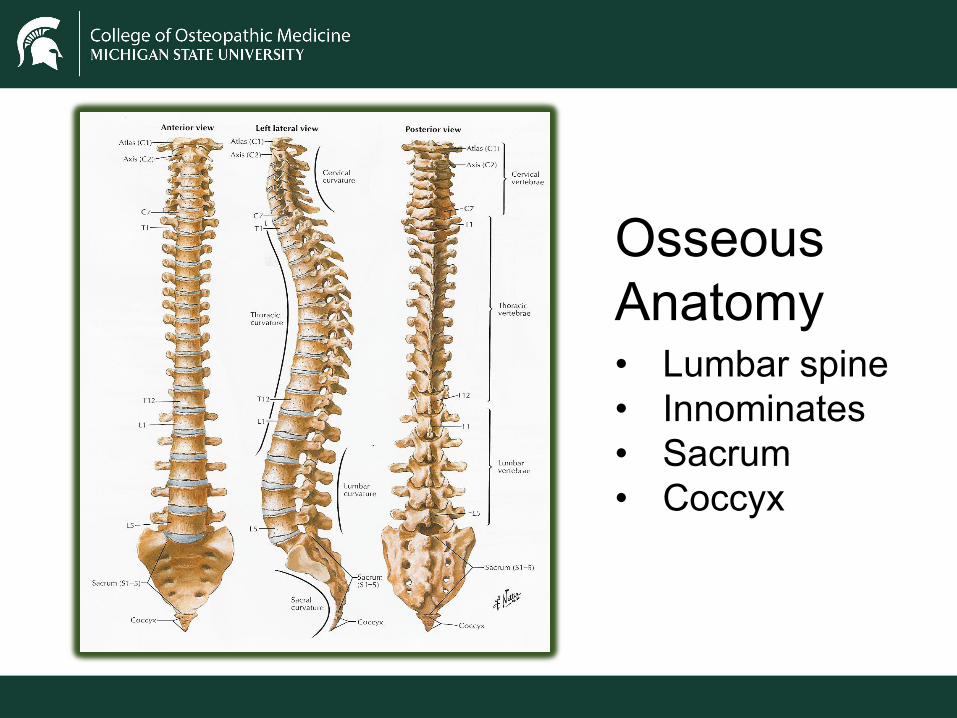
Osseous Anatomy• Lumbar spine• Innominates• Sacrum• Coccyx

The Innominates• Three fused bones
• Ilium• Ischium• Pubis
• Partially cartilaginous at birth, fuse by age twenty• Innominates articulate with the femur at the
acetabulum, with the sacrum at the SI joints, and with each other through the pubic symphysis

The Sacroiliac Joint: Ilial Aspect


The Sacrum• Composed of five fused vertebrae• Anterior aspect of S1=sacral promontory• Most cephalad part=sacral base• Most caudal=apex (articulates with coccyx)• Space between PSIS and sacral base=sacral
sulci• Inferior lateral aspect=inferior lateral angles

The Sacroiliac Joint: Sacral Aspect






Ligaments of the Pelvis• True pelvic ligaments
• Anterior, posterior, and interosseous sacroiliac ligaments surround and stabilize the SI joint
• Accessory pelvic ligaments• Sacrotuberous ligament• Sacrospinous ligament• Iliolumbar ligaments




Muscular Anatomy• Iliopsoas• Piriformis• Lumbar and sacral paraspinals• Abdominals• Pelvic diaphragm





Posterior Muscle Layers• First Layer
• Latissimus dorsi• Second Layer
• Serratus anterior• Third Layer
• Erector Spinae• spinalis, longissimus, iliocostalis
• Fourth Layer• Multifidus & Rotatores

First and Second Layer Muscles of the Back

Third Layer Muscles of the Back

Fourth Layer Muscles of the Back

Muscles of the diaphragm, posterior abdominal wall, and pelvis

Muscles of the Pelvic Floor• Primary pelvic muscles
• Levator ani• coccygeus
• Secondary pelvic muscles• Iliopsoas• Obturator internus• Piriformis

Primary Pelvic Floor Muscles

Diagnosis and Treatment in the Muscle Energy Model

Greenman’s “Dirty Half Dozen”• Nonneutral lumbar mechanics• Pubic dysfunction• Innominate shear dysfunction• Restricted sacral nutation• Short leg and pelvic tilt syndrome• Muscle imbalance

The Examination• Somatic dysfunction is defined as impaired or
altered function of related components of the body framework system: skeletal, arthrodial, and myofascial structures, and their related vascular, lymphatic, and neural elements.
• Somatic dysfunction is characterized by positional asymmetry, restricted range of motion, tissue texture abnormalities, or tenderness.

A Focused Screening Exam• Establish your dominant eye• Standing landmarks• Lumbar sidebending• Standing flexion test• Stork test• Seated flexion test

Standing Landmarks1. Palpate the iliac crests by pushing soft tissue
out of the way from below and placing proximal phalanges of index fingers on similar portions of right and left hip bones.
2. Palpate and observe the top of the greater trochanter with lateral to medial compression of the soft tissues of the hip.
3. Unleveling of the iliac crest and greater trochanter while standing is first sign of possible short leg pelvic tilt syndrome.
4. Eyes are on the same horizontal plane as palpating fingers.

Lumbar Sidebending1. Observe from the back.2. Patient is asked to sidebend left as far as possible
without bending forward.3. Patient repeats sidebending right.4. Observe symmetry of range reflected by fingertip
distance on lateral leg.5. Observe the induced spinal curve; it should be smooth
with fullness on the side of the convexity. Straightening of the curve and fullness on the side of the concavity suggest vertebral motion dysfunction at that level.
6. Observe symmetry of pelvic shift right or left during sidebending effort and whether loading of lower extremities appears symmetric.

Standing Flexion Test1. Patient stands with feet approximately 4 inches
(10 cm) apart with weight under hip joints.2. With pads of thumbs, palpate the inferior slope
of the posterior superior iliac spine.3. Instruct patient to bend forward as if to touch
the floor. Operator’s thumbs follow the PSIS, observing whether one appears to move more cephalad.
4. Test is positive if one PSIS moves further cephalad than the other.
Standing Flexion Test5. Also observe lower thoracics and lumbars for
signs of segmental restriction.6. This test is very sensitive to dysfunction in the
bony pelvis and fascias of the trunk and lower extremity; lateralizes dysfunction.
7. Repeat the test with arms overhead; this alters the behavior of the pelvis through loads from the fascias of the ribs and upper extremities.
8. Compare the two forward bending findings to gather information regarding whether restrictions are above or below the pelvis.

Stork Test1. With patient standing, operator places thumb
over most posterior portion of patient’s left PSIS and right thumb over midline of the sacrum at same level.
2. Patient flexes left hip and knee to minimum of 90 degrees of hip flexion.
3. Test is negative if left thumb on PSIS moves caudad in relation to right thumb on the sacrum.
4. Thumb placements are reversed, and right hip is flexed.

Stork Test5. Test is positive if thumb on PSIS moves
cephalad in relation to thumb on sacrum.6. Findings of this test are then correlated with
those of standing flexion test; stork test is more specific for sacroiliac dysfunction.

Seated Flexion Test1. Patient sits on examining stool with knees
apart and feet flat on floor.2. Operator’s thumbs are on inferior slope of
PSIS.3. Patient bends forward with arms between legs
as far as possible.4. Monitor motion of the PSIS’s; the one that
moves furthest cephalad is called positive, indicating restriction on that side.

Seated Flexion Test5. Observe behavior of lower thoracics and
lumbars for suggestions of restriction.6. Compare these findings with the standing
flexion test; this test is not influenced by lower extremities as patient is sitting on ischial tuberosities.
7. Unleveling of iliac crests when seated gives evidence of inequality in size of the right and left hip bones.

Nonneutral Lumbar Mechanics• In the absence of dysfunction and when in an
upright position, the lumbar spine should exhibit type 1 mechanics
• In segmental dysfunction, the lumbar spine loses its neutral coupled motion
• Screening test is standing lumbar sidebending

Extended Lumbar Dysfunction• Lumbar segment is extended, sidebent and
rotated (to the same side) relative to the segment below
• Prefers extension because the zygopophysial joint on the side of rotation is closed and resists opening on flexion


Treatment of ERS (e.g., ERS left at L4)1. Patient lies on left side with neck and head
supported on a pillow; dr. stands facing the pt and flexes pt’s trunk down to L4 while keeping pt’s shoulders perpendicular to the table.
2. Dr. flexes pt’s legs up to L5 while monitoring L4-L5.
3. Dr. introduces right rotation by rotating pt’s right shoulder posteriorly while monitoring at L4-L5.
4. Dr. introduces right sidebending by lifting pt’s feet toward the ceiling until motion is felt at the segment.

Treatment of ERS (e.g., ERS left at L4)5. Dr. resists pt effort to pull feet back toward
the table (left sidebending effort) while monitoring at the segment.
6. Pt performs 3-5 reps of 3-5 seconds each. During relaxation phase, Dr. engages next barrier to flexion, right rotation, right sidebending.
7. Retest.

Flexed Lumbar Dysfunction• Lumbar segment is flexed, sidebent and
rotated relative to the segment below.• Prefers flexion because the zygopophysial joint
on the side opposite rotation is open and resists closing, or extension.
Treatment of FRS (e.g., FRS left at L4)1. Pt is lying on left side with dr. standing in front, facing
the pt.2. Dr. engages extension by translating L4-L5 from
posterior to anterior.3. Dr. fine tunes extension from above by translating the
pt’s shoulder back, and then fine tunes from below by translating the pt’s legs back, all the while monitoring at the segment.
4. Dr. engages right rotation barrier by rotating the pt’s right shoulder back (while monitoring at the segment); pt holds the table to maintain right roation.

Treatment of FRS (e.g., FRS left at L4)5. Dr. lifts pt’s right leg to engage right
sidebending barrier while monitoring at the segment.
6. Pt pulls right knee down toward table for 3-5 reps of 3-5 sec each against Dr.’s effort. After each effort, the dr. engages the next barrier of right sidebending by lifting the pt’s leg, and the next barrier of extension by translating the pt’s leg back.

Treatment of FRS (e.g., FRS left at L4)7. Dr. returns pt’s right knee to the table and
places forearm against pt’s right shoulder to maintain rotation right; dr.s left hand is on pt’s right buttock and engages right sidebending by cephalic translation. A muscle energy effort is performed here, as well.
8. Retest.

Pubic Dysfunction• Unleveling at the pubic symphysis and
tenderness to palpation in this region are physical exam findings of dysfunction
• Pubic dysfunction alters gait through impaired motion of the innominates during the walking cycle
• Muscle imbalance can be found between the thigh adductors below and the abdominals above

Pubic Dysfunction• Superior pubic shear
• Etiology: trauma or tight rectus abdominus• Static findings:
• ASIS and PSIS landmarks are level• Pubic bone is superior ipsi
• Dynamic findings:• + standing flexion test ipsi• ASIS compression restricted ipsi

MET for Left Superior Pubic• Pt is supine• Drop pt’s left leg off the table and abduct
until resistance is felt• Instruct pt to bring left knee to right ASIS
against your counterforce for 3-5 seconds• During relaxation, take up the slack• Repeat 3-5 times and recheck

Pubic Dysfunction• Inferior pubic shear
• Etiology: trauma or tight adductors• Static findings:
• ASIS and PSIS landmarks are level• Pubic bone inferior ipsi
• Dynamic findings:• + standing flexion test ipsi• ASIS compression restricted ipsi

MET for Right Inferior Pubic Shear• Pt is supine• Flex and abduct pt’s right hip until
resistance is felt• Instruct pt to push right knee to left foot
against your counterforce for 3-5 seconds
• After relaxation, take up the slack• Repeat 3-5 times and recheck

Innominate Dysfunction• Superior innominate shear
• Etiology: fall on ipsilateral buttock or misstep• Static findings:
• ASIS and PSIS superior ipsi• Iliac crest superior ipsi• Pubic ramus superior ipsi• Ischial tuberosity superior ipsi• Slack sacrotuberous ligament ipsi
• Dynamic findings:• + standing flexion test ipsi• ASIS compression restricted ipsi

Innominate Shear• Opposing surfaces of the sacroiliac joints lose
normal sacral concavity and bevel change at S2 in 10-15% of the population
• Under right circumstances, ligamentous support may be lost due to sudden trauma, resulting in a shear
• Classic presentation: lumbosacral pain radiating into sacroiliac and glut areas and frequent radiation to posterolateral thigh and lateral knee
• Simulates radiculopathy


MET for Left Superior Innominate Shear• Pt is supine• Stand at foot of table with left thigh blocking pt’s right foot• Grasp pt’s left leg just proximal to the ankle• Abduct the left leg to 10-15 degrees to loose pack the SI
joint• Internally rotate the extended, abducted leg to close pack
the hip joint• Put long-axis traction on the leg while pt inhales and
exhales several times• During last exhalation, pt coughs while operator
simultaneously tugs on leg in caudal direction

Sacral Mechanics• Form and Force Closure: creates stability• Dynamic motion
• Occurs during ambulation; sacrum engages two oblique axes
• Weight bearing on the left leg causes a left sacral axis to be engaged

Restricted Sacral Nutation• Sacral mechanics include nutation and
counternutation with every step and every breath
• Assessment easiest with pt prone and then in prone prop (asymmetry worsens in prop)
• Frequently found with a nonneutral dysfunction at L5

Unilateral Sacral Extension• In the prone position, the sacral base is
posterior, and the ILA is posterior/inferior on the opposite side.
• Standing and seated flexion tests are positive on the side of the posterior sacral base.
• Findings worsen on prone prop.

MET for Unilateral Sacral Extension
1. Pt is prone on table with dr. standing on side of posterior sacral base.
2. Dr. monitors SI joint as pt’s ispilateral leg is abducted to ~15 degrees (loose-packing the jt).
3. Dr. externally rotates the pt’s abducted leg to gap the anterior aspect of the SI jt.
4. Pt’s trunk is extended by prone prop while dr’s pisiform contacts the posterior sacral base, maintaining a ventral and caudad force.

MET for Unilateral Sacral Extension (cont.)5. Dr’s free hand on the pt’s ipsilateral ASIS
provides a counterforce against the compression.
6. Pt performs series of forced exhalations while dr. maintains ventral force
7. At end of each exhalation effort, the pt pulls the ipsilateral ASIS down toward the table.
8. 3-5 reps later, dr. maintains ventral/caudad force while pt returns to neutral.
9. Retest.

Posterior Sacral Torsion• In the prone prop position, the sacral base and
the ILA are posterior on the same side.• Standing and seated flexion tests are positive
on the same side at the posterior sacral base.• Findings worsen on prone prop.

MET for Posterior Sacral Torsion• R-on-L example
1. Pt lies on left side with dr. standing facing in front and monitoring at lumbosacral junction.
2. Dr pulls pt’s left arm anterior and caudad, introducing left sidebending and right rotation until L5 first rotates to the right.
3. Dr. introduces extension of both legs until base first moves anteriorly.
4. Dr. drops pt’s right leg in front of pt’s left knee and places left hand against pt’s distal right femur.

MET for Posterior Sacral Torsion (cont.)
5. Dr’s right forearm maintains L5 rotation to right while left hand resists pt’s effort to raise right knee toward ceiling.
6. Pt performs 3-5 contractions of 3-5 seconds each while dr. engages new barrier after relaxation by further extending the pt’s bottom leg and dropping the pt’s right leg more toward the floor.
7. Retest.

Documentation and Coding Tips

HISTORY• Chief Complaint• HPI
• Elements: location, duration, timing, quality, severity, context, modifying factors, associated signs and symptoms

HISTORY• Past Family, Social, Medical History• Review of Systems
• Elements: constitutional, respiratory, skin, eyes, ENT, GI, GU, neurologic, psychiatric, endocrine, musculoskeletal, cardiovascular, heme/lymph, allergy/immunology

PHYSICAL EXAMINATION• Vitals• General • HEENT• Cardiovascular• Neurologic• Musculoskeletal• Skin

Assessment• Primary diagnoses• Somatic dyfunction
• Regional codes• Cranial• Cervical• Thoracic• Ribs• Lumbar
• Pelvis• Sacrum• Abdomen• Upper extremities• Lower extremities

Plan• Assessment:
• Chronic low back pain• Lumbar degenerative disc disease• Lumbar spondylolisthesis• Somatic dysfunction lumbar spine, pelvis, sacrum
• Plan:• Exercise • Nutrition goal• Stress management• Pharmaceuticals• Nutraceuticals• Osteopathic manipulative medicine

Plan• Osteopathic manipulative medicine
• Be mindful of local somatic dysfunction• Assess and balance the autonomic nervous
system if appropriate• Release lymphatic transition zones and
augment flow• Consider indications and contraindications

Procedure note• Pre-service work documented below in "ART
was noted." Technique was chosen after ART defined and OMT techniques were explained to the patient and/or guardian(s) in detail prior to its application. Patient and/or guardian(s) verbally consented to treatment.

Procedure note• Structural Examination:
• Cranial Region• ART was noted:• Technique(s) used:

Procedure note• Consent Statement:
• OMT was explained to the patient and/or guardian(s) in detail before its application. The patient and/or guardian(s) verbally consented to treatment. OMT was applied as indicated to the regions documented above.

Procedure note• OMT performed: in areas that are noted
above• Post-service work: The patient tolerated
today’s manipulation well with desired results and without complication. The patient and/or guardian(s) was/were advised of possible side-effects, stiffness, and proper post-treatment care.
• See plan.

Procedure note• Abbreviation Key: ART= Asymmetry, Range
of motion restriction, and Tissue texture abnormality; MET=muscle energy technique; MFR=myofascial release; HVLA=high-velocity, low-amplitude thrust; BLT=balanced ligamentous tension; BMT=balanced membranous tension; StT=Still technique; st=soft tissue; LAS=ligamentous articular strain; CS=counterstrain; FI=functional indirect technique; Art=articulatory technique
Procedure note• Somatic Dysfunction Key:• FRS right - Flexed, Rotated and sidebent right;
FRS left - Flexed, Rotated and sidebent left• ERS right - Extended, Rotated
and sidebent right; ERS left - Extended, Rotated and sidebent left
• NSlRr - Neutral, Sidebent left, rotated right; NSrRl - Neutral, Sidebent right, rotated left

Procedure note• Billing and coding reference:https://osteopathic.org/practicing-medicine/business-of-medicine/osteopathic-billing-coding/#:~:text=Report%20the%20appropriate%20CPT%20E,code%20(98925%2D98929)

Somatic Dyfunction Codes• M99.0 Cranium SD• M99.01 Cervical
Spine SD• M99.02 Thoracic
Spine SD• M99.03 Lumbar
Spine SD• M99.04 Sacral SD
• M99.05 Pelvis SD• M99.06 Lower
Extremity SD• M99.07 Upper
Extremity SD• M99.08 Rib SD• M99.09 Abdomen SD

CPT Codes• 98925 = 1-2 areas• 98926 = 3-4 areas• 98927 = 5-6 areas• 98928 = 7-8 areas• 98929 = 9-10 areas

The 25 Modifier• A significant, separately identifiable Evaluation and
Management (E/M) service by the same physician or other qualified health care professional on the same day of the procedure or other service.