caring for the tracheostomised patient- -...
TRANSCRIPT

CARING FOR THE
TRACHEOSTOMISED PATIENT: WHAT TO LOOK OUT FOR
DR MOHD NAZRI ALI
Anaesthesiologist & Intensivist
HRPZ II, Kota Bharu,
Kelantan
asmic 2017
Tracheostomy The Enabling Disability
asmic 2017

Tracheostomy
• Are becoming increasingly common place both within the
acute setting and community
• As a result of this there is an expectation of increased
knowledge and more advanced nursing and
healthcare skills in ward staff caring for this patient.
asmic 2017

• Tracheostomy is commonly performed procedure in ICU
• Estimated 15,000 insertion procedures in the UK annually (NCEPOD UK 2014)
• Local data
( MRIC 2015 )
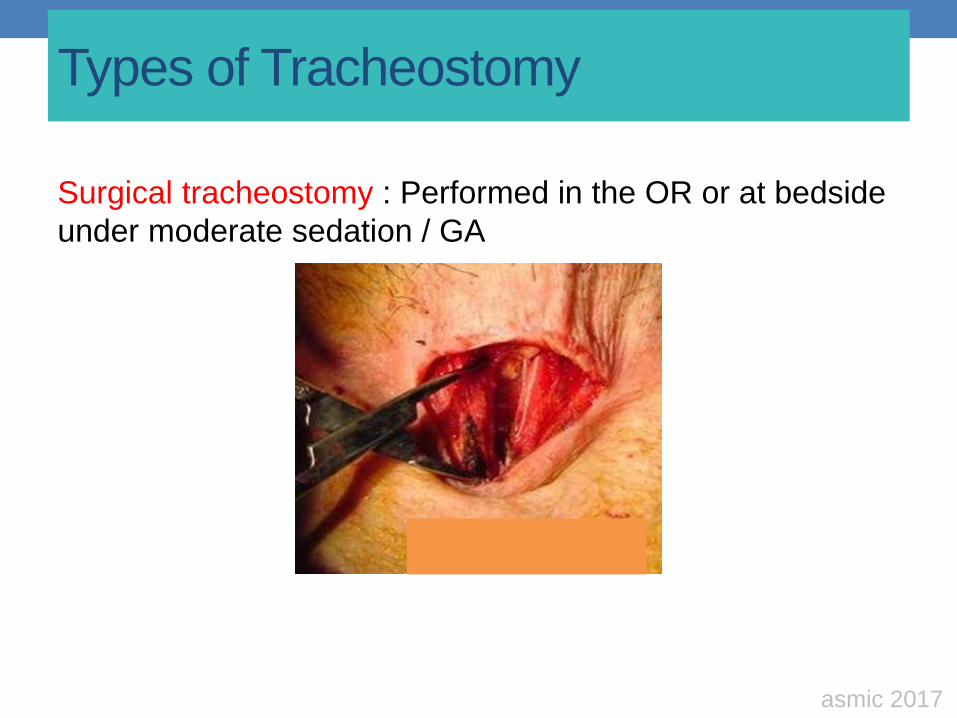
Types of Tracheostomy
Surgical tracheostomy : Performed in the OR or at bedside
under moderate sedation / GA
asmic 2017
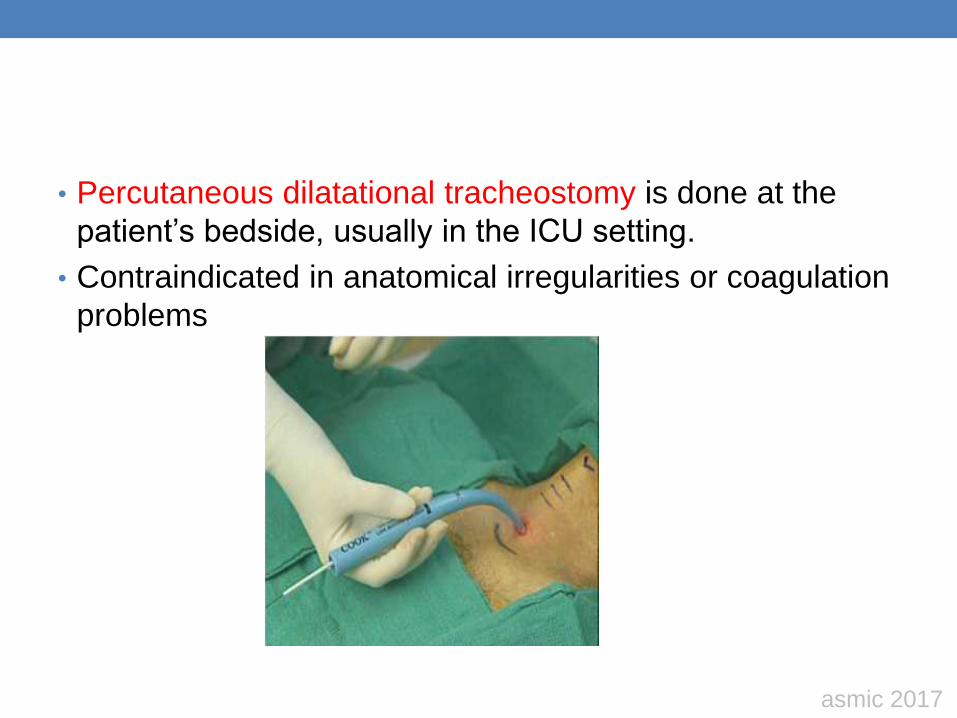
• Percutaneous dilatational tracheostomy is done at the
patient’s bedside, usually in the ICU setting.
• Contraindicated in anatomical irregularities or coagulation
problems
asmic 2017
Why does your patient have a tracheostomy ?
• To maintain a patent airway when the ability to do this is
temporarily or permanently compromised
-Bypass obstructed airway
Tumour
Foreign body obstruction
• Facilitate removal of secretion
• Facilitate weaning of ventilator
• Optimize sedation
• Decreased work of breathing ( severe COAD)
asmic 2017
Is not without
Tracheostomy..
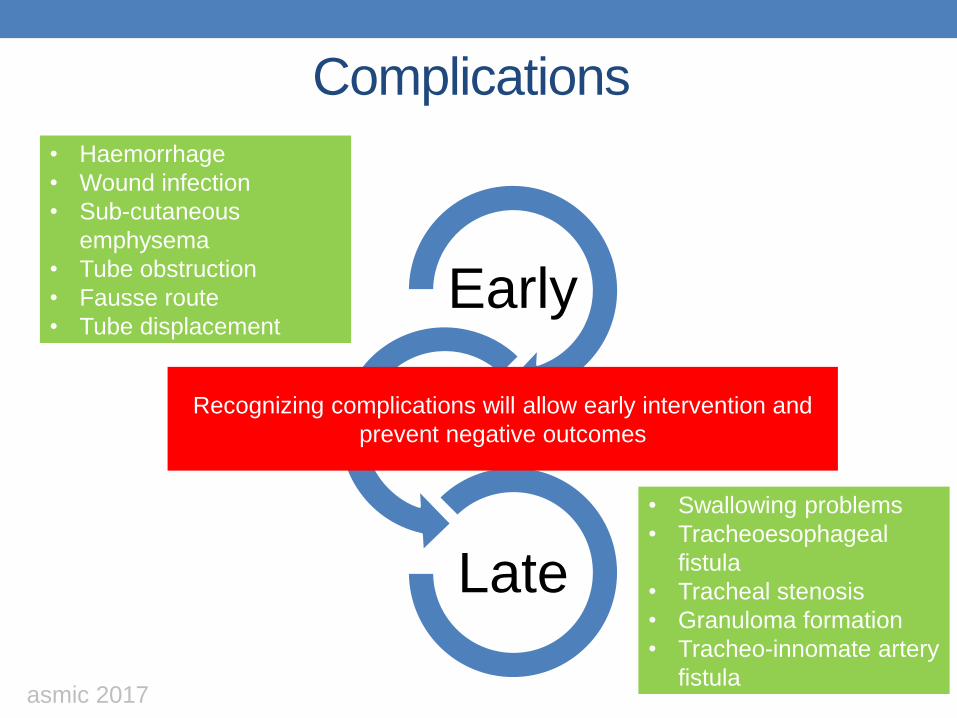
Complications
Early
Late
• Haemorrhage
• Wound infection
• Sub-cutaneous
emphysema
• Tube obstruction
• Fausse route
• Tube displacement
• Swallowing problems
• Tracheoesophageal
fistula
• Tracheal stenosis
• Granuloma formation
• Tracheo-innomate artery
fistula
Recognizing complications will allow early intervention and
prevent negative outcomes
asmic 2017
The essential principles when caring for
patient with a tracheostomy are based on
• Maintaining patient safety
• Airway patency
• Facilitating communication
• Preventing complication associated with procedures
asmic 2017

Care of the tracheostomy
• Major factors must be considered in the
care of tracheostomy patient Basic nursing care
Cuff pressure
Humidification of inspired air
Airway patency and secretion clearance
Speech
Nutrition
asmic 2017
Basic nursing care
• Some general measures are advocated for immediate
post tracheostomy care :
Tracheostomy cannula is secured in place
Left to heal for 5-7 days
Kept clean and dry
Inner cannula is changed daily or more frequent if necessary
Avoids angulation
asmic 2017
Wound assessment
General
• Offensive odour
• Pain during dressing change
• Allergic reaction to product
Surgical incision
Bleeding
Infection
Wound breakdown
Tracheostomy stoma site
• Increase in size
• Appearances of stoma
edges
• Appearance of peri-stoma
tissue
(maceration,cellulitis)
• Nature &quality of
exudates
• Presence of granuloma
tissue
asmic 2017

Cuff pressure
• Tracheostomy tube cuffs require monitoring to maintain
pressure in a range of 20-25mmHg
• High cuff pressure exceed 25-35 mmHg exceed capillary
perfusion pressure will result compression of mucosal
capillaries
Mucosal ischemia
Tracheal stenosis
• Low cuff pressure below 18 mmHg may caused the cuff to
develop longitudinal folds
Micro aspiration
VAP
asmic 2017

Cuff pressure should be monitored
with calibrated devices
asmic 2017
Humidification
• The importance of humidification can’t be over-
emphasized
• Nasopharynx :
provide natural humidification mechanism for the airway
Keep airway moist
• Bypass by the tracheostomy
asmic 2017
Strategies
Properly hydrated with oral, IV fluids ( mucosal surface
to remain moist and to ensure the viscid secretions
remain atop the cilia)
Instillation sterile saline directly into tracheostomy
during suctioning
(not too much)
Conserved patient’s own moisture ( HME)
Saline nebuliser – moist the airway
asmic 2017
Airway patency and secretion clearances
• Many of the nursing skills employed are aimed at the
mobilization of pulmonary secretions
• Strategies
• Frequent turning
• Encouragement of deep breathing and ambulation
• Chest physiotherapy and postural drainage
• Saline nebulizer
• Suctioning
asmic 2017
1.Suctioning a patient never be considered routine
• Suction when :
Clinically in distress
Increase airway pressures
Increase patient apprehension
Auscultation – ronchi
Other-request by the patient
asmic 2017

Suctioning should be done
PRN, after chest
physiotherapy,nebulisation
Use the lowest pressure
needed ( usually < 120 mmHg,
definitely not beyond 200
mmHg
Suctioning performed less
than 10 seconds
Insert the catheter : length of
trachy + ¼ inch
Size of suction
catheter
Less than half of
internal diameter
tracheostomy
Divide the
internal diameter
of trachy by two
AND multiply the
answer by three
French gauge
suction catheter
asmic 2017
2. Inner cannula
• Inner cannula is one of the most important parts of
tracheostomy
• Keep clear of secretion build-up since can be removed
and cleaned
• Care always requires strict aseptic technique
• Every 2-3 hours for first 48 H
• Every 4 hours thereafter
asmic 2017
Weaning tracheostomy
Increase period of cuff deflated
Fenestrated tube
Speaking valve
Down sizing the tube
Capping off tracheostomy tube
Decannulation
asmic 2017
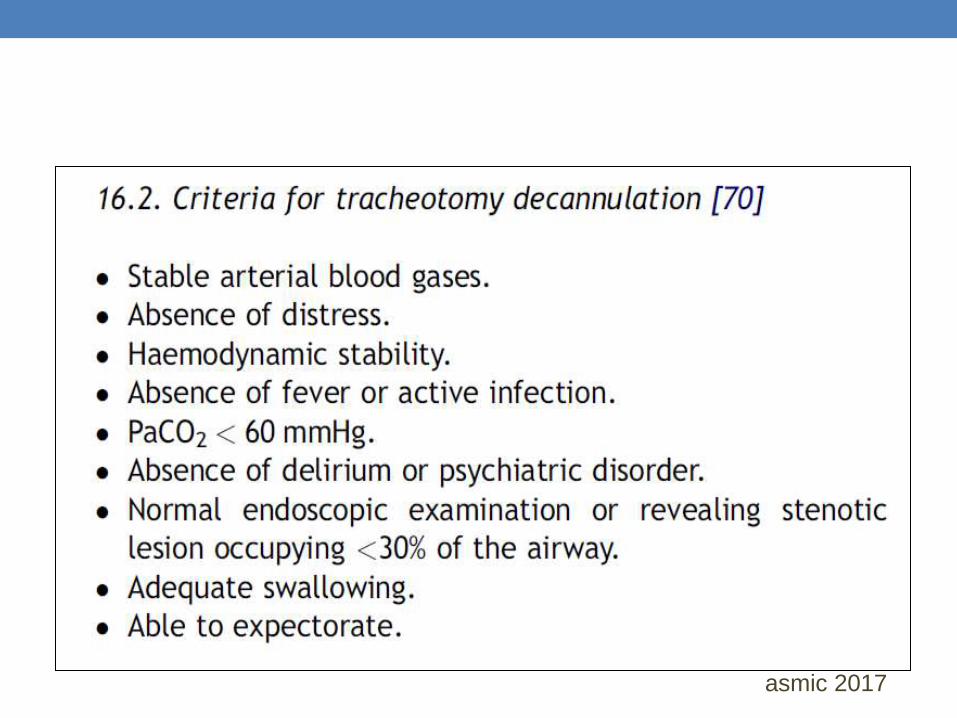
Decannulation
• When the patient is being weaned from mechanical
ventilation or from tracheostomy tube
• The use of fenestrated tracheostomy tube may facilitate
the decannulation procedure
• Design of the tube
Allows the patient to gradually become used to handling secretions
and breathing on his/her own
Protection of the cuff if patient should required supportive
ventilation
asmic 2017
• When it is desired to have the patient breath through
his/her upper airway
Removed inner cannula
Cuff deflated
Occlude the outer cannula with de-cannulation cap
( monitor for features of airway obstruction / distress )
asmic 2017
asmic 2017
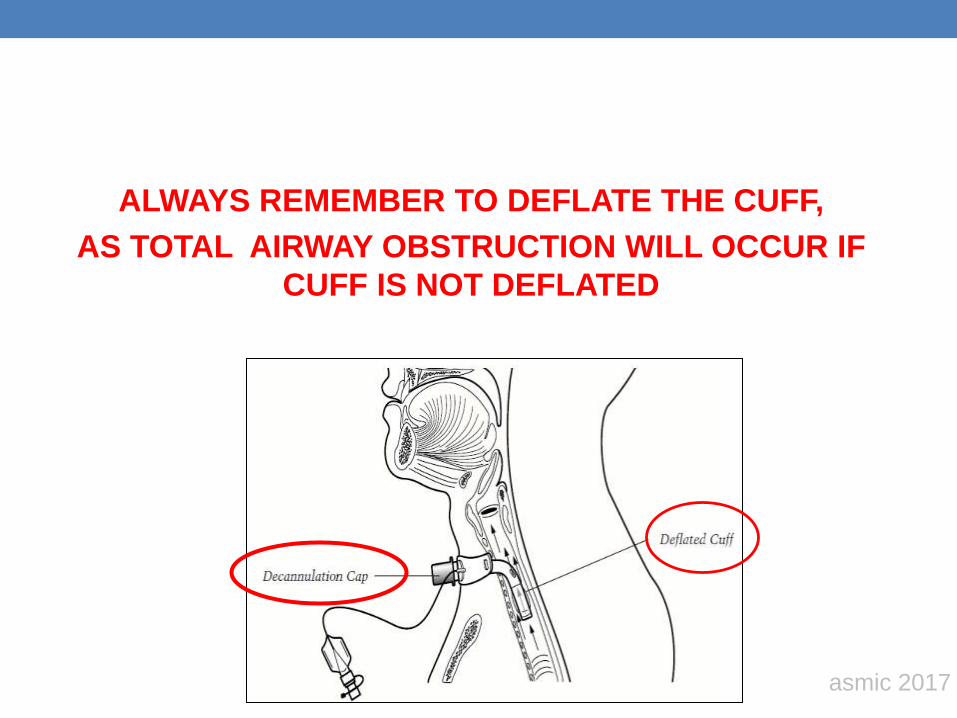
ALWAYS REMEMBER TO DEFLATE THE CUFF,
AS TOTAL AIRWAY OBSTRUCTION WILL OCCUR IF
CUFF IS NOT DEFLATED
asmic 2017

Speech
Ventilator-dependant patient
• Whispered speech
• Partially deflation of
tracheostomy tube cuff
• Provided good swallowing
• Minimal secretion above
the cuff
Non-ventilator dependant
• Remove inner cannula
• Occlude external end of
tracheostomy ( cap, one
way valve)
-Deflated the tube cuff**
-Non-cuff tracheostomy
• Allowing expiratory airflow
through the larynx
asmic 2017
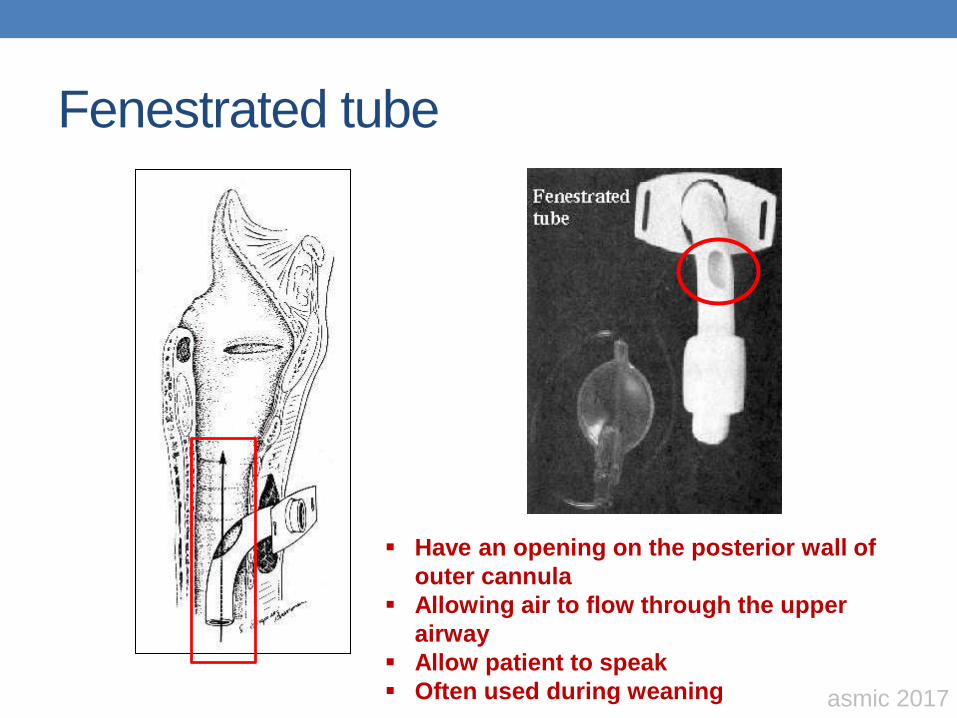
Fenestrated tube
Have an opening on the posterior wall of
outer cannula
Allowing air to flow through the upper
airway
Allow patient to speak
Often used during weaning asmic 2017
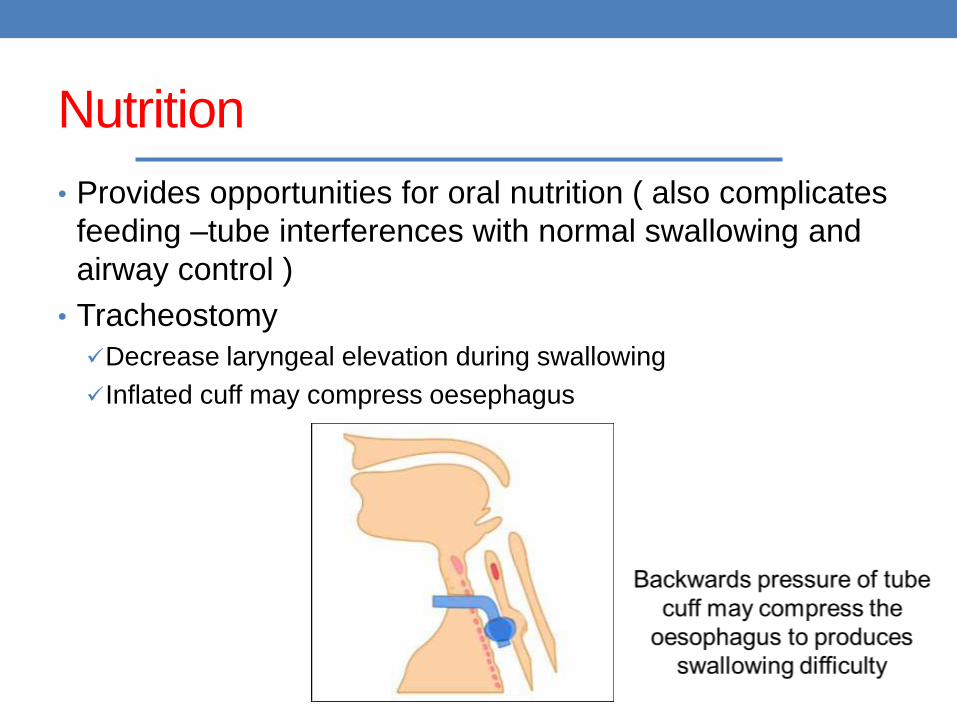
Nutrition
• Provides opportunities for oral nutrition ( also complicates
feeding –tube interferences with normal swallowing and
airway control )
• Tracheostomy
Decrease laryngeal elevation during swallowing
Inflated cuff may compress oesephagus
• Risk factors for swallowing problems in patients with
tracheostomy
Neurological injury eg. Bulbar palsy
Disuse atrophy
Head and neck surgery
Evidence of aspiration of enteral feed or oral secretion on tracheal
suctioning
Increase secretion load
Coughing and desaturation following oral intake
Patient anxiety or distress during oral intake
High FiO2
Risk factors for swallowing problems in patient with
tracheostomy
asmic 2017
• Reduce risk of aspiration by:
Confirm that patient can tolerate cuff deflation
Sit patient up with head slightly flexed,
placed a suction catheter just at the end of tracheostomy
deflate the cuff while suctioning.This is to prevent secretion falling into the airway
Start with sip of clear fluid then soft diet
Observe for respiratory distress, coughing,desaturation,tachypneic
For problematic cases consider referral to speech and language therapy for swallowing test / endoscopic or radiological assessment
Reduce risk of aspiration by
asmic 2017
RED FLAGS
Airway
• A suction catheter not passing easily into the trachea
• A changing,inadequate or absent capnograph trace
• Patient with a cuff tracheostomy tube suddenly being able to talk or noise or bubble coming from the upper airway
• Frequent requirement for (excessive) inflation of the cuff to prevent air leak
• Pain at the tracheostomy
site
• Visibly displaced
tracheostomy tube
• Bleeding from the tube /
stoma
asmic 2017

Breathing
• Increasing ventilator
support / O2 requirement
• Respiratory distress
• Subcutaneous
emphysema
• Patient complaining that
they cannot breath /
difficulty in breathing
• Suspicious of aspiration
Circulation
• An airway emergency
may lead to CVS collapse
• Anxiety, restlessness,
agitation and confusion
may also due to airway
problem
asmic 2017
In a nutshell….
• Tapes : keep the tracheostomy tube secure
• Resus / emergency care : know the resuscitation
procedure
• Airway clear : use the correct suction technique
• Care of the stoma and neck
• Humidity : essential to keep the tube clear
• Emergency equipment : have the box present
Tube changes planned
TRACHE bundle
asmic 2017
Elizabeth Taylor's Tracheostomy
Taylor went to Europe, awaiting production of Cleopatra. In spring of 1961, she developed a case of pneumonia, which led to an emergency tracheotomy and worldwide talk of her impending death. The swelling of sympathy was widely thought to have influenced Academy voters, who awarded Taylor her first Best Actress Oscar —Elizabeth later commented, I knew it was a sympathy award, but I was still proud to get it." Meanwhile, Taylor's competitor Shirley MacLaine memorably quipped, "I lost to a tracheotomy!"
