case 1: 75-year-old african-american manmedia.mycme.com/documents/...slides_from_w_26808.pdf ·...
TRANSCRIPT


Case 1: 75-Year-Old African-American Man With AF
Hypertensive and overweight
Lives alone; family members live several miles away
Long history of hypertension (currently 145/85 mm Hg) and elevated LDL-C (most recently measured at 125 mg/dL)
AF = atrial fibrillation; LDL-C = low-density lipoprotein cholesterol.

Case 1: 75-Year-Old African-American Man With AF (cont’d)
BMI: 26 kg/m2
Smoker, with shortness of breath
History of GI bleeding
Neuropathy as a consequence of successful radiation treatment for male breast cancer
BMI = body mass index; GI = gastrointestinal.

Risk Factor Points Congestive heart failure 1
Hypertension 1 Age ≥75 years 1 Diabetes mellitus 1 Stroke or TIA 2 Maximum Score 6
CHADS2 = Congestive heart failure, Hypertension, Age ≥75 years, Diabetes, and prior Stroke/TIA; TIA = transient ischemic attack. Gage BF, et al. JAMA. 2001;285:2864-2870. van Walraven C, et al. Arch Intern Med. 2003;163:936-943. Nieuwlaat R, et al. Eur Heart J. 2006;27:3018-3026. Go AS, et al. JAMA. 2003;290:2685-2692. Gage BF, et al. Circulation. 2004;110:2287-2292.
CHADS2 Stroke (%/y) 0 1.9
1 2.8
2 4.0
3 5.9
4 8.5
5 12.5
6 18.2
3%/y
CHADS2 Risk Score

Risk Factor Points CHF/LV dysfunction 1 Hypertension 1
Age ≥75 years 2
Diabetes mellitus 1
Stroke/TIA/embolism 2
Vascular disease 1 Age 64-74 years 1 Sex category (female) 1
Maximum Score 9
CHA2DS2-VASc = Congestive heart failure, Hypertension, Age ≥75 (doubled), Diabetes, Stroke (doubled), Vascular disease, Age 65-74, and Sex category (female); CHF = congestive heart failure; LV = left ventricular. ESC Guidelines. Eur Heart J. 2010;31:2369-2429.
CHA2DS2-VASc Score Stroke (%/y)
1 0% 2 1.3%
3 2.2%
4 4.0%
5 6.7%
6 9.8% 7 9.6% 8 6.7%
9 15.2%
Redefining Risk: CHA2DS2-VASc

ESC Guidelines. Eur Heart J. 2010;31:2369-2429.
Letter Clinical Characteristic Points
H Hypertension 1
A Abnormal liver or renal function 1 or 2
S Stroke 1
B Bleeding 1
L Labile INR 1
E Elderly (age >65 years) 1
D Drugs or alcohol 1 or 2
Maximum Score 9
Pisters R, et al. Chest. 2010;138:1093-1100.
HAS-BLED = Hypertension, Abnormal renal/liver function, Stroke, Bleeding history or predisposition, Labile INR, Elderly (>65 years), and Drugs/alcohol concomitantly; INR = international normalized ratio.
0 2 4 6 8
10 12 14 16
0 1 2 3 4 5
Redefining Risk: HAS-BLED
HAS-BLED Score Bl
eeds
per
100
Pat
ient
Ye
ars

Case 2: 80-Year-Old Caucasian Man With AF and Cataracts
Accompanied by his caregiver wife Receiving warfarin as stroke prophylaxis due to AF following
mild stroke the previous year Type 2 diabetes
– A1C >8% for past 6 months; BMI: 28 kg/m2
Blood pressure: 155/100 mm Hg Recently underwent total hip replacement surgery Now needs outpatient cataract surgery requiring frequent
clinician visits to adjust INR

Dabigatran
Xa
X IX
IXa VIIIa Va
II
Fibrin Fibrinogen
Adapted from: Weitz JI, Bates SM. J Thromb Haemost. 2005;3:1843-1853.
Rivaroxaban Apixaban Edoxaban*
Novel Oral Anticoagulants (NOACs)
TF/VIIa
IIa
*Approved January 2015.
Case 3: 84-Year-Old Hispanic Woman With AF and Moderate Dementia
Accompanied by her caregiver daughter Receiving warfarin for stroke prophylaxis for
5 years; TIA 2 years ago Family history of cardiovascular disease; father
died of heart failure at age 64 years Mild osteoarthritis, which limits her ability to
take walks
BMI: 27 kg/m2

Case 3: 84-Year-Old Hispanic Woman With AF and Moderate Dementia (cont’d)
Recently experiencing increasing forgetfulness and memory loss; has difficulty with managing medications and activities of daily living; diagnosed with moderate dementia
Requires help from family caregiver and part-time home health aide
Becoming nonadherent to medications

ICH = intracranial hemorrhage; OAB = oral anticoagulant. Friberg L, et al. Circulation. 2012;125:2298-2307.
Net Clinical Benefit of Warfarin All-Cause Mortality, Ischemic Stroke, and ICH
1.0
0.8
0.6
0.4
0.2
0.0
0 1 2 3 4
P<.00001 (n=1,787) Prop
ortio
n Su
rviv
ing
OAC
No OAC
1.0
0.8
0.6
0.4
0.2
0.0
0 1 2 3 4
P<.00001 (n=59,817) Pr
opor
tion
Surv
ivin
g
OAC
No OAC
1.0
0.8
0.6
0.4
0.2
0.0
0 1 2 3 4
P<.00001 (n=43,395) Pr
opor
tion
Surv
ivin
g
OAC
No OAC
1.0
0.8
0.6
0.4
0.2
0.0
0 1 2 3 4
P<.00001 (n=59,817) Pr
opor
tion
Surv
ivin
g
OAC
No OAC
HAS-
BLED
0-2
p
HAS
-BLE
D ≥3
p
Risk
for I
ntra
cran
ial B
leed
ing
CHA2DS2–VASc 0-2 p CHA2DS2–VASc ≥3 p
YEARS YEARS
YEARS YEARS
Risk for Embolic Stroke

RE-LY (Dabigatran)
ROCKET-AF (Rivaroxaban)
ARISTOTLE (Apixaban)
ENGAGE AF (Edoxaban)
# randomized 18,113 14,264 18,201 21,105 Age, years 72 ± 9 73 [65-78] 70 [63-76] 72 [64-78] Female, % 37 40 35 38 Paroxysmal AF 32 18 15 25
VKA naive 50 38 43 41 Aspirin use 40 36 31 29
Baseline Characteristics
32 35
33 13
87 47 53 34
36
30 CHADS2
2
3-6
0-1
Ruff CT, et al. Lancet. 2014;383:955-962. VKA = vitamin K antagonist.

All-Cause Mortality
Myocardial Infarction
Hemorrhagic Stroke
Ischemic Stroke
0.90 (0.85-0.95)
0.97 (0.78-1.20)
0.49 (0.38-0.64)
0.92 (0.83-1.02)
Risk Ratio (95% CI)
P = 0.0003
P = 0.77
P < 0.0001
P = 0.10
Favors NOAC Favors Warfarin
0.2 0.5 1 2
Secondary Efficacy Outcomes
Heterogeneity P = NS for all outcomes.
Ruff CT, et al. Lancet. 2014;383:955-962.
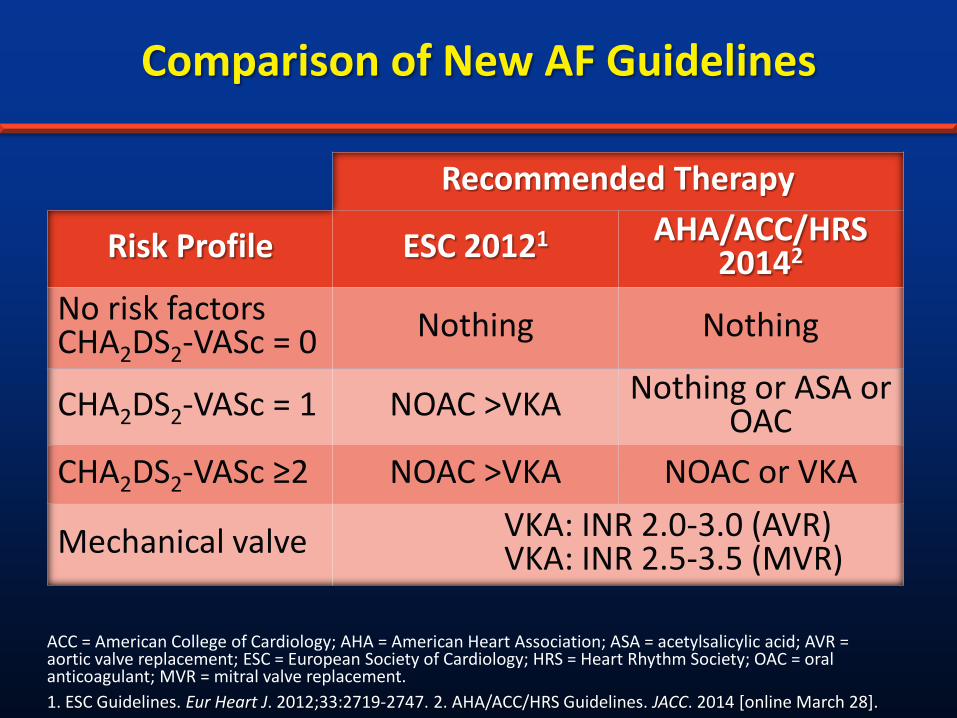
Comparison of New AF Guidelines
Recommended Therapy
Risk Profile ESC 20121 AHA/ACC/HRS 20142
No risk factors CHA2DS2-VASc = 0 Nothing Nothing
CHA2DS2-VASc = 1 NOAC >VKA Nothing or ASA or OAC
CHA2DS2-VASc ≥2 NOAC >VKA NOAC or VKA
Mechanical valve VKA: INR 2.0-3.0 (AVR) VKA: INR 2.5-3.5 (MVR)
ACC = American College of Cardiology; AHA = American Heart Association; ASA = acetylsalicylic acid; AVR = aortic valve replacement; ESC = European Society of Cardiology; HRS = Heart Rhythm Society; OAC = oral anticoagulant; MVR = mitral valve replacement. 1. ESC Guidelines. Eur Heart J. 2012;33:2719-2747. 2. AHA/ACC/HRS Guidelines. JACC. 2014 [online March 28].

Shared Decision Making: Principles
Clinicians and patients share the best available evidence when making decisions, and clinicians support patients to consider options to achieve informed preferences1,2
– Rather than clinicians making decisions on behalf of patients1
Based on premise that individual self-determination is a desirable goal and that clinicians need to support patients to achieve this goal1
Highlights the importance of probing for/explaining the diagnosis and then explaining how various treatments may work
1. Elwyn G, et al. J Gen Intern Med. 2012;27:1361-1367. 2. Elwyn G, et al. BMJ. 2010;341:c5146.