case presentation bueno, kathryn a. 4med san beda college of medicine
TRANSCRIPT
CASE PRESENTATION
BUENO, KATHRYN A.4MED
San Beda College of Medicine

General Data:
M. L. 34y/o G2P1 (1001) Housewife Right-handed Roman Catholic Montalban Rizal

Chief Complaint:
“vaginal bleeding”

History of Present Illness:
3 hours PTC
vaginal bleeding
abdominal pain
frequent uterine contractions
(+) dizzy
(-) fever, vomiting, cough, colds loss of consciousness
no medications

1 hour PTC
vaginal bleeding persisted
abdominal pain increased in frequency
immediately rushed at QMMC-ER on
April 13, 2011

History of Present Pregnancy
LMP: August 12, 2010 AOG: 34 6/7 weeks by LMP EDC: May 19, 2011

Past Medical History
HPN- 20 years old ; no maintenace medication (-) diabetes, renal, lung, heart diseases (-) surgeries, hospitalizations, allergies

Family History
HPN-father (-) diabetes, heart, lung, kidney diseases

Personal and Social History
Housewife Non-smoker Non-alcoholic beverage drinker (-) illicit drugs Diet unrestricted

Menstrual History
13 years old Regular cycle Moderate flow Lasts for 5 days Consumes 3 pads per day (+) dysmenorheal symptoms

Obstetric History
Gravida:2 Parity:1 (1001) 1st child – 2007, full term, NSD, lying in at
Montalban Rizal, (-) complications
Contraceptive History
(-) birth control method

Review of Systems
(-) headache, blurring of vision (-) dyspnea (-) chest pain, palpitations (-) frequency, dysuria
Physical Examination
General Survey:
The patient is conscious, coherent, ambulatory not in cardiorespiratory distress.
Vital signs: BP 120/90 RR-20 HR-72 bpm T-36.5C

Skin: Nails without clubbing, cyanosis.
HEENT: Head is normocephalic, atraumatic and no scar. Hair is evenly distributed. Scalp without lesions. Conjunctiva is pink, sclera is anicteric. Hearing is good, no ear discharge and no pain. No visible masses or ulcerations. Nasal mucosa pink. No sinus tenderness. No masses or polyps. Oral mucosa pink. Dentition good. Tongue midline. No exudates.

Neck: Neck supple. Trachea midline. No lymphadenopathy.
Thorax and lungs: No scars, masses, lessions and tenderness. Thorax is symmetric with equal expansion. Lungs resonant in all fields. Breath sounds is vesicular in all lung fields. Equal fremitus: no bronchophony, egophony or whispered pectoriloquy.

Cardiovascular: No scars, masses, lessions and tenderness Regular rate and rythmn Good S1 and S2. S1 is louder in apex and S2 is louder at the base. No murmurs or extra sounds.

Abdomen: No masses, lessions, or tenderness with a 5cm vertical scar at linea alba. Well coaptated wound with no discharge. Abdomen is flat with normoactive bowel sounds (24/min). It is soft and tymapnitic upon percusssion. Liver span is 6 cm in the right midclavicular line. Spleen and kidneys are non-palpable.

Extremities: Warm without edema.
Muskuloskeletal: Good range of motion in hands, wrists elbows, shoulders, knees, hips, ankles.

Admitting Diagnosis
G2P1 (1001) Intrauterine Fetal Death (IUFD) 34 6/7 weeks AOG by LMP NIL T/C Abruptio Placenta

Course in the Wards
Patient was admitted inserted with IV fluids (D5LR) administered MgS04 4 gram deep IM on each
buttock (then 5 gram IM q6 24 hour post-partum) NSD but had uterine atony after delivery of the
placenta underwent TAHBSO and bilateral hypogastric
artery ligation due to postpartum hemmorhage 3 units of PRBC were transfused

Oral Medications:
FeSo4 1 tab TID
Amlodipine 10 mg tab. BID
Essentiale 1 cap TID
Clonidine 75 mg tab. For BP> 160/100
Mefenamic Acid 500 mg

IV medications: Cefuroxime 750 mg IV q8 Tranexemic Acid 1 gram q8 Furosemide 20 mg q12 Vitamin K 1 ampule q8

Laboratory exam results: CBC (April 20, 2011)
Result Normal Value
RBC 3.39 (L) 3.8-5.1
Hemoglobin 9 (L) 11-16 g/dl
Hematocrit 0.30 (L) 0.36-0.47
MCV 91.2 78-98 fL
MCH 30.4 27-35 pg
MCHC 33.3 31-37%
Platelet Adequate 150,000-400,000
WBC 17.2 (H) 3.8-11
Neutrophils 0.60 50-81%
Lymphocytes 0.40 14-44%

Clinical chemistry results (April 16, 2011)
Result Normal Vaue
Creatinine 56.83 53-115
BUN 5.13 2.5-6.40
Na 138 136-145
K 3 3.5-5.1
Cl 105 97-107

Abruptio Placenta
The separation of the placenta from its site of implantation after the 20th week of pregnancy and before the delivery of the fetus.

Classification
As to extent: Total Partial
As to onset: Acute abruption Chronic abruption

As to type: External Concealed Marginal sinus rupture


Risk factors Increased age and parity Preeclampsia Chronic hypertension Preterm ruptured membranes Cigarette smoking Thrombophilias Cocaine use Prior abruption Uterine leiomyoma Trauma

Pathophysiology
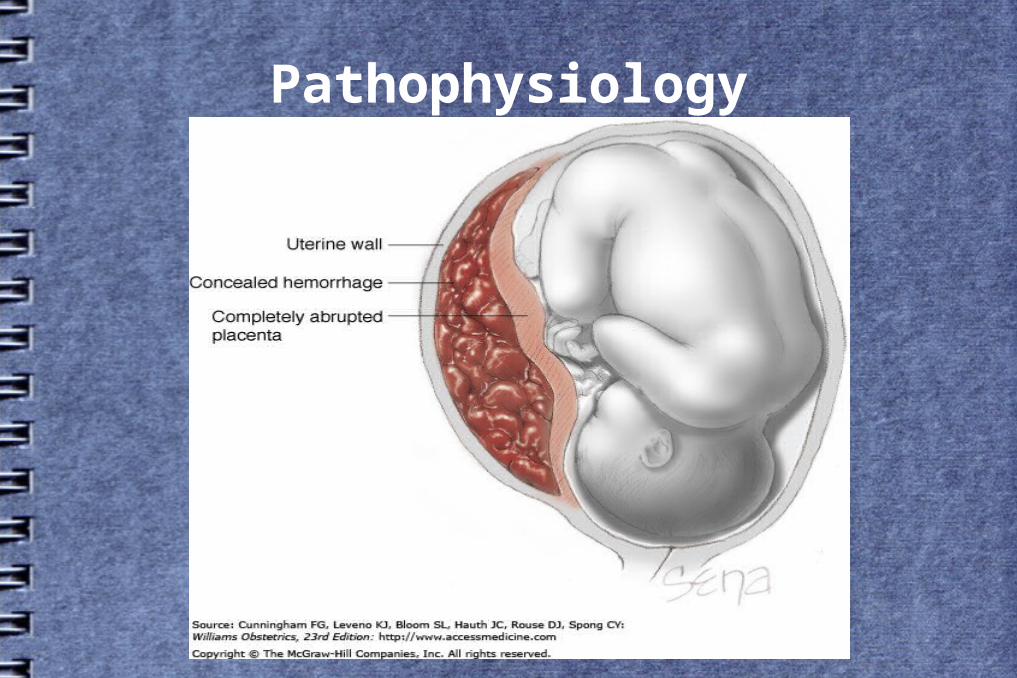
Pathophysiology


Signs and symptoms
Vaginal bleeding Uterine tenderness or back pain Fetal distress High frequency contractions Hypertonus Idiopathic preterm labor Dead fetus

Diagnosis
Clot formation retroplacentally Ultrasonography and doppler imaging MRI Non-specific markers

Management
Institute crystalloid fluid resuscitation for the patient (D5LR or D5W).
Monitor BP, FH, pulse rate, respiratory rate, fluid intake and urinary output.
Type and crossmatch blood. Request for CBC, including platelet count, plasma fibrinogen,
fibrin degradation products and partial thromboplastin time. If plasma level is critical – administer fibrinogen using
cryoprecipitate If platelet count is less than 50,000 ml, 6-8 platelet packs are
transfused.

Delivery
Vaginal Cesearian

Complications
Couvelaire uterus Acute Renal Failure Consumptive Coagulopathy

Thank You!!!