case review bromocriptine-induced cerebrospinal fluid ... · treatment of invasive prolactinoma the...
TRANSCRIPT
rI
Case Review
Essam A Elgamal1
Zain AB Jamjoom2
Hesham Abu Rahma2
IDepartment of NeurosurgeryFrenchay HospitalBristolUnited Kingdom
2Division of NeurosurgeryKing Khalid Univ. HospitalRiyadhSaudi Arabia
Correspondence:Dr. Essam A ElgamalDepartment of NeurosurgeryFrenchay HospitalBristol, BS16 lLEUnited KingdomFax: (44) 117970 1212Email: [email protected]
40
Bromocriptine-induced cerebrospinalfluid rhinorrhea following successfultreatment of invasive prolactinoma
The authors present a case of a 36-year-old man who developed spontaneous cerebrospinal fluid (CSF) rhinorrhea after two years of bromocriptine therapy for an invasive prolactin secreting pituitary adenoma.The patient had never undergone any surgery or radiotherapy in theregion of the tumour. The CSF fistula was best demonstrated by meansof computed tomography cisternography. Magnetic resonance imagingand subsequent surgery confirmed the presence of an empty sella withcomplete regression of the tumour. A review of the pertinent literaturerevealed seven similar cases. The clinical and radiological features of
patients at risk of developing this rare complication are described, andthe treatment options discussed. (P40-45)
Keywords: Invasive prolactinoma, bromocriptine, cerebrospinal fluidrhinorrhea and transsphenoidal surgery.
Introduction
Cerebrospinal fluid (CSF) rhinorrhea is a well-known complicationof the surgical treatment of pituitary adenoma, being encounteredin 1-3.1 % of the operated cases. 15,16,19 In contrast, spontaneous CSFrhinorrhea after bromocriptine therapy is rare and so far only 7 suchcases have been reported in the pertinent lierature.1,3,5,13,20
In this report, the authors describe a new case of CSF rhinorrhea that
developed in the course of bromocriptine therapy for an invasiveprolactin secreting pituitary adenoma. The aim is to draw attention tothis rare complication and outline the clinical and radiological characteristics of patients who are at risk of developing this rare complication.
Case ReportThis 36-year-old man had been complaining of frontal headache for five
years and decreased libido for two years. Moreover, he noticed someblurring of vision with drooping of the left eyelid one month prior topresentation to hospital. There was no history of galactorrhea, but thepatient suffered from a bout of meningococcal meningitis 14 yearsearlier.
PAN ARAB JOURNAL OF NEUROSURGERY
BROMOCRIPTINE-INDUCED CSF RHINORRHEA • Elgamal, et al
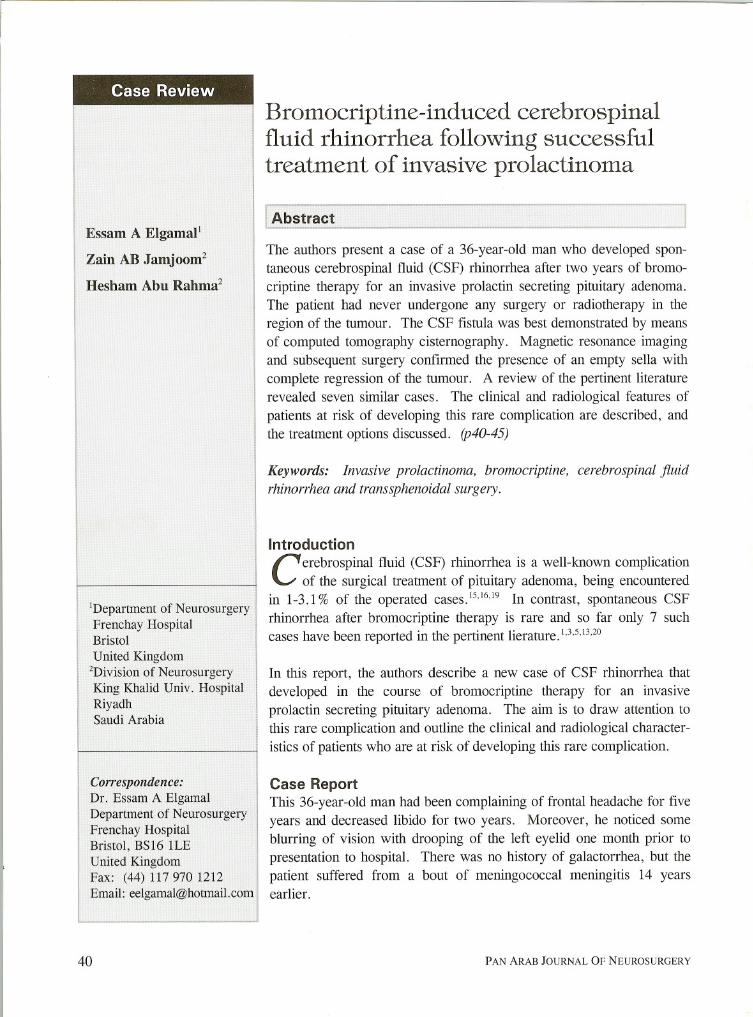
Figure 1 - Sagittal MRI with gadolinium showing a largesellar and suprasellar tumour with enhancing multiple deposits
Neurological examination showed bilateral upper
quadrant anopsia and partial left third nerve palsy.Systemic examination was unremarkable, apartfrom bilateral gynaecomastia.
A random serum prolactin level was 11,350 ng/ml(normal: 35-380), whereas basal levels of otherhormones were within normal limits.
Computed tomography (CT) scan and magneticresonance imaging (MRI) revealed a large intrasellar and suprasellar tumour that invaded bothcavernous sinuses. There was complete destructionof the sellar floor, dorsum sella and the upperclivus, and the tumour filled the sphenoid air sinusand broke through its floor into the epipharynx(Fig. 1).
As the patient was reluctant to undergo surgicalresection of the tumour, he was started on bromo
criptine at a dose of 15 mg/day that was laterincreased to 30 mg/day. Within seven days therewas a dramatic improvement in his visual fieldand eyelid drooping. The serum prolactin level
VOLUME 5. No. 2. OCTOBER 2001
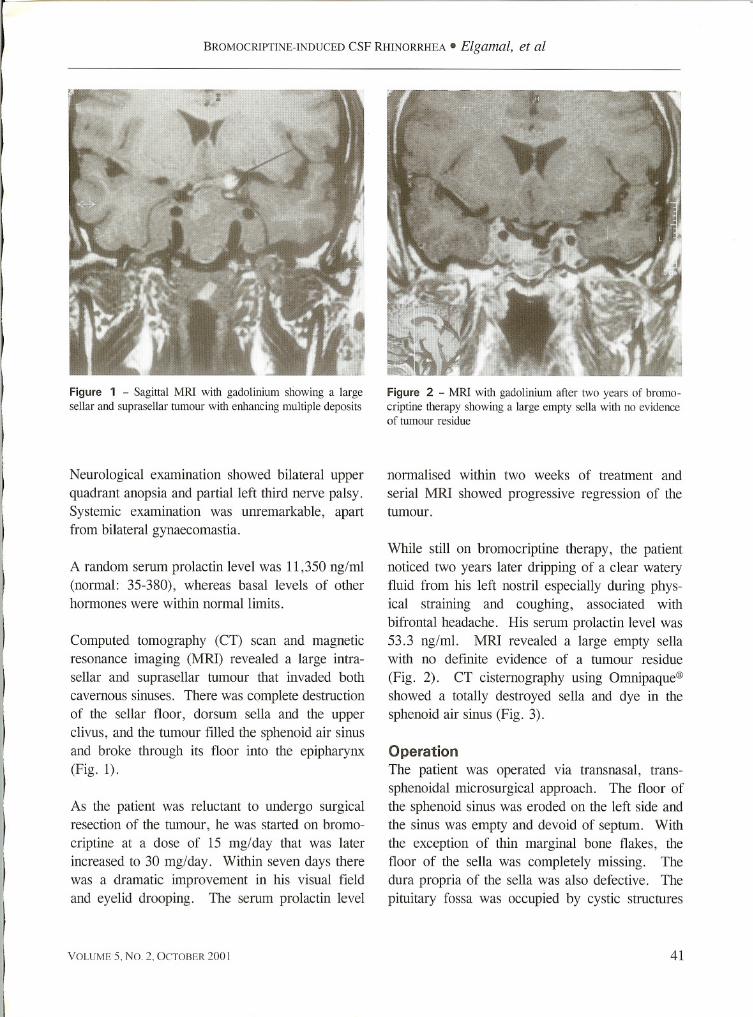
Figure 2 - MRI with gadolinium after two years of bromocriptine therapy showing a large empty sella with no evidenceof tumour residue
normalised within two weeks of treatment and
serial MRI showed progressive regression of thetumour.
While still on bromocriptine therapy, the patientnoticed two years later dripping of a clear wateryfluid from his left nostril especially during physical straining and coughing, associated with
bifrontal headache. His serum prolactin level was53.3 ng/ml. MRI revealed a large empty sellawith no definite evidence of a tumour residue
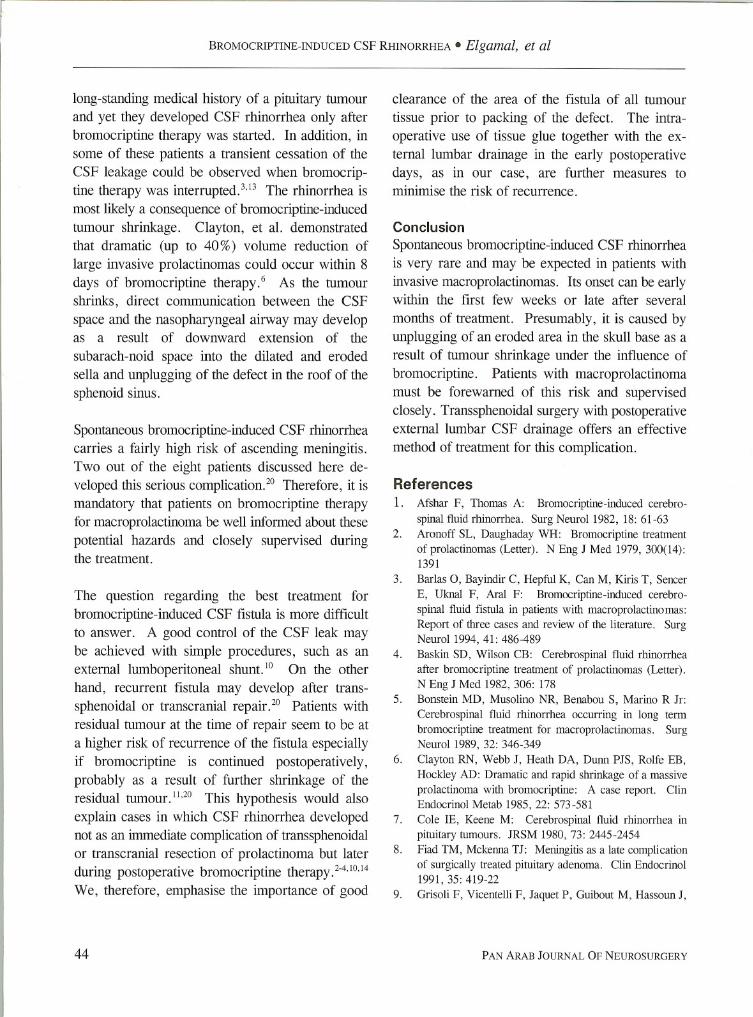
(Fig. 2). CT cisternography using Omnipaque®showed a totally destroyed sella and dye in thesphenoid air sinus (Fig. 3).
OperationThe patient was operated via transnasal, trans
sphenoidal microsurgical approach. The floor ofthe sphenoid sinus was eroded on the left side and
the sinus was empty and devoid of septum. Withthe exception of thin marginal bone flakes, thefloor of the sella was completely missing. Thedura propria of the sella was also defective. Thepituitary fossa was occupied by cystic structures
41

BROMOCRIPTINE-INDUCED CSF RHINORRHEA • Elgamal, et al
Figure 3 - CT cisternography showing a destroyed sella anddye leaked to the sphenoid air sinus
and thin, grayish, fibro-gelatinous membranes, butno tumour tissue could be seen. The pituitary glandwas identified as a small yellow mass on the rightside of the fossa. The pituitary fossa and sphenoidsinus were packed respectively with fat and musclepieces obtained from the right thigh. The marginsof the muscle plug were finally sealed up by usinga tissue glue (Tisse1(R». An external lumbar CSFdrain was inserted immediately postoperatively toeliminate the risk of early CSF leakage that mayinterfere with good healing of the reconstruction.The postoperative course was uneventful and CSFrhinorrhea ceased completely. The lumbar draincould be removed 5 days later and bromocriptinetherapy was discontinued gradually. At last follow
up examination one year after surgery, the patientwas neurologically intact and free of recurrence ofeither tumour or CSF rhinorrhea. His basal hor
mone levels, including prolactin, were within normal limits.
Discussion
Invasive prolactinoma has always posed a therapeutic challenge to neurosurgeons, endocrinologists
42
and radiotherapists. 12 With tumour extensions intocomplex neighbouring anatomical structures, suchas the cavernous sinus and skull base, a cure of
these lesions by surgery alone could be expectedin only an exceptional case of localised invasion,which can be exposed and resected radically.14Consequently, a combination of different therapeuticmodalities is necessary for the treatment of thevast majority of these lesions. In recent years,bromocriptine has emerged as the treatment of
first choice for most prolactin secreting pituitaryadenomas, including large and invasive lesions. 17
It has been shown that 80 % of macroprolactinomasshrink under the influence of this dopamine agonist,often associated with a significant decline in serumprolactin level and improvement of pre-existingvisual disturbances.18 Although adverse reactionsduring bromocriptine therapy are not uncommon,they are usually transient and limited to dizzinessand gastrointestinal discomfort.14,18 The manifestation of CSF rhinorrhea during the treatment withbromocriptine, as in our case, is in contrast rare,and has so far been described in 20 other patientsin the literature.I-6,8,1O,11,13,14,20However, 13 out of
these 20 patients had at some stage, before orduring bromocriptine therapy, undergone trans
nasal/transsphenoidal surgery or craniotomy, sometimes combined with postoperative radiotherapy. 24,6,8,10,11,14Truly spontaneous CSF rhinorrhea duringbromocriptine therapy had probably occurred inonly 8 cases, including this case (Table 1). Theonset of CSF rhinorrhea was early (within the first6 weeks of treatment) in one half, but late (between 9-24 months of treatment) in the other half
of patients. All 8 patients shared the common feature of harbouring a large invasive prolactinomathat had widely eroded the sellar floor and oftenextended into the sphenoid sinus.
Although CSF rhinorrhea may be directly causedby tumours invading the skull base, the causativerole of bromocriptine in the development of CSFrhinorrhea in patients with invasive prolactinomasis highly probableY Most of these patients had a
PAN ARAB JOURNAL OF NEUROSURGERY

- -
<orc$tT1
Ch
zo5"
o()--Jot:O
tT1
?=Noo
.p..w
Table 1 - A summary of reported cases of spontaneous CSF rhinorrhea during bromocriptine therapy for invasive macroprolactinoma
Duration of
ProlactinBromocrip-Interval to Repair of
No.
AuthorYearAgeSexsymptoms
leveltine doseonset ofMeningitisCSFRemarks
(ng/ml)
(mglday)rhinorrhea rhinorrhea
1
Afshar &1982
28F 12y 1855 polwNTSp1Fibronecrotic tissue, no
Thomas (4)
residual tumour
Partial excision of tumour,2
Wilson,1983
32F 8y 2007.5 po5wNTCR2rhinorrhea recurred after
et al. (5)
2 weeks. Transsphenoidal
repaIr .Rhinorrhea recurred after6 weeks. Transcranial3
55M lOy 4547.5 po6wNTSRrepair + removal ofresidual tumour.Postoperative radiotherapyRhinorrhea ceased whenKok,
bromocriptine was dis-
4et al. (6)
198547M 4y 1350015 po9mNTSPcontinued and recurred
when resumed. Necrotictissue removed.
5
Bronstein,1989
52F 20y 11105 po16 mNTSPSmall amount fibrotic
et al. (7)
tumour removed
6
33M 3y 170010 po17mYTSPResidual tumour
Rhinorrhea ceased when7
Barlas,1994
46F 16y 3105 po15 dyTSPbromocriptine was dis-
et al (8)
continued and recurred
when resumed
8
Elgamal,2001
36M 2y 1135015 po2yNTSPFibrogelatinous tissue, no
et al.
residual tumour
to:;0os::::o():;0
::a>-3
Zt;n
Zt:Ic::(')tI1t:Inen'Tj
~~zo:;0:;0~tI1>-•~~~~J'-~"""
~-.
__ ·,. __ ._U~" ~ ~_
BROMOCRIPTINE-INDUCED CSF RHINORRHEA • Elgamal, et al
long-standing medical history of a pituitary tumourand yet they developed CSF rhinorrhea only afterbromocriptine therapy was started. In addition, in
some of these patients a transient cessation of the
CSF leakage could be observed when bromocriptine therapy was interrupted. 3, 13 The rhinorrhea is
most likely a consequence of bromocriptine-inducedtumour shrinkage. Clayton, et al. demonstratedthat dramatic (up to 40%) volume reduction oflarge invasive prolactinomas could occur within 8
days of bromocriptine therapy. 6 As the tumourshrinks, direct communication between the CSF
space and the nasopharyngeal airway may developas a result of downward extension of the
subarach-noid space into the dilated and erodedsella and unplugging of the defect in the roof of thesphenoid sinus.
Spontaneous bromocriptine-induced CSF rhinorrhea
carries a fairly high risk of ascending meningitis.Two out of the eight patients discussed here developed this serious complication.2o Therefore, it ismandatory that patients on bromocriptine therapyfor macroprolactinoma be well informed about these
potential hazards and closely supervised duringthe treatment.
The question regarding the best treatment forbromocriptine-induced CSF fistula is more difficultto answer. A good control of the CSF leak may
be achieved with simple procedures, such as anexternal lumboperitoneal shunt. 10 On the otherhand, recurrent fistula may develop after transsphenoidal or transcranial repair. 20 Patients withresidual tumour at the time of repair seem to be ata higher risk of recurrence of the fistula especially
if bromocriptine is continued postoperatively,probably as a result of further shrinkage of the
residual tumour.l1,20 This hypothesis would alsoexplain cases in which CSF rhinorrhea developednot as an immediate complication of transsphenoidalor transcranial resection of prolactinoma but laterduring postoperative bromocriptine therapy. 2-4.10,14
We, therefore, emphasise the importance of good
44
clearance of the area of the fistula of all tumour
tissue prior to packing of the defect. The intra
operative use of tissue glue together with the external lumbar drainage in the early postoperativedays, as in our case, are further measures tominimise the risk of recurrence.
Conclusion
Spontaneous bromocriptine-induced CSF rhinorrheais very rare and may be expected in patients withinvasive macroprolactinomas. Its onset can be earlywithin the first few weeks or late after several
months of treatment. Presumably, it is caused byunplugging of an eroded area in the skull base as aresult of tumour shrinkage under the influence of
bromocriptine. Patients with macroprolactinomamust be forewarned of this risk and supervisedclosely. Transsphenoidal surgery with postoperativeexternal lumbar CSF drainage offers an effective
method of treatment for this complication.
References
1. Afshar F, Thomas A: Bromocriptine-induced cerebro
spinal fluid rhinorrhea. Surg Neuro11982, 18: 61-63
2. Aronoff SL, Daughaday WH: Bromocriptine treatment
of prolactinomas (Letter). N Eng J Med 1979, 300(14):1391
3. Barlas 0, Bayindir C, Hepful K, Can M, Kiris T, Sencer
E, Uknal F, Aral F: Bromocriptine-induced cerebro
spinal fluid fistula in patients with macroprolactinomas:Report of three cases and review of the literature. SurgNeuro11994, 41: 486-489
4. Baskin SD, Wilson CB: Cerebrospinal fluid rhinorrhea
after bromocriptine treatment of prolactinomas (Letter).N Eng J Med 1982, 306: 178
5. Bonstein MD, Musolino NR, Benabou S, Marino R Jr:
Cerebrospinal fluid rhinorrhea occurring in long term
bromocriptine treatment for macroprolactinomas. SurgNeurol 1989, 32: 346-349
6. Clayton RN, Webb J, Heath DA, Dunn PJS, Rolfe EB,
Hockley AD: Dramatic and rapid shrinkage of a massive
prolactinoma with bromocriptine: A case report. ClinEndocrinol Metab 1985, 22: 573-581
7. Cole lE, Keene M: Cerebrospinal fluid rhinorrhea inpituitary tumours. JRSM 1980, 73: 2445-2454
8. Fiad TM, Mckenna TJ: Meningitis as a late complication
of surgically treated pituitary adenoma. Clin Endocrinol1991,35: 419-22
9. Grisoli F, Vicentelli F, Jaquet P, Guibout M, Hassoun J,
PAN ARAB JOURNAL OF NEUROSURGERY

BROMOCRIPTINE-INDUCED CSF RHINORRHEA • Elgamal, et al
Farnarier P: Prolactin secreting adenoma in 22 men. SurgNeuro11980, 13: 241-247
10. Hildebrandt G, Zierski J, Christophis P, Laun A, Schatz
H, Lancranjan I, Klug N: Rhinorrhea following dopamineagonist therapy of invasive macroprolactinomas. Acta
Neurochir (Wien) 1989, 96: 107-11311. Holness RO, Shlossberg AH, Heffeman LRPM: Cerebro
spinal fluid rhinorrhea caused by bromocriptine therapyofprolactinoma. Neurol1984, 34: 111-113
12. Jamjoom ZAB, Malabarey T, Jamjoom AH, Sulimani R,
Naim-U-Rahman, Sadiq S: Problems in the managementof large prolactin-secreting pituitary adenomas. SaudiMed J 1995, 15(2): 119-125
13. Kok JG, Bartelink AKM, Schlte BPM, Smals A, Pieters
G, Meyer E, Merx H: Cerebrospinal fluid rhinorrheaduring treatment with bromocriptine for prolactinoma.Neuro11985, 35: 1193-1195
14. Landolt AM: Cerebrospinal fluid rhinorrhea: A com
plication of therapy for invasive prolactinomas. Neurosurg1982, 11: 395-401
15. Laws ER, Kern EB: Complications of transsphenoidal
surgery. Clin Neurosurg 1976, 23: 401-41616. Nicola G: Trans-sphenoidal surgery for pituitary
adenomas with extrasellar extension. Prog. Neurol Surg1975, 6: 142-199
17. Scherrer H, Turpin G, De-Gennes JL, Schaison CM,
Heshmati HM, Thibierge M, Metzger J: Results of
bromocriptine treatment of giant or invasive prolactin
adenomas. Aprops of 20 cases. Ann Med Interne Paris1985, 136(6): 459-466
18. Vance ML, Evans WS, Thorner MO: Bromocriptine.Ann Intern Med 1984, 100: 78-91
19. Wilson CB, Dempsly LC: Transsphenoidal microsurgicalremoval of 250 pituitary adenomas. J Neurosurg 1978,48: 13-22
20. Wilson JD, Newcomb RLG, Long FL: Cerebrospinal
fluid rhinorrhea during treatment of pituitary tumourswith bromocriptine. Acta Endocrinol (Copenh) 1983, 103:457-460