case scenarios atrial switch univentricular repair dr.yasser salem
TRANSCRIPT
Case scenariosAtrial switch
Univentricular repair
Dr.Yasser Salem

The case of Dr. Marwa Khyry

Atrial switch ??
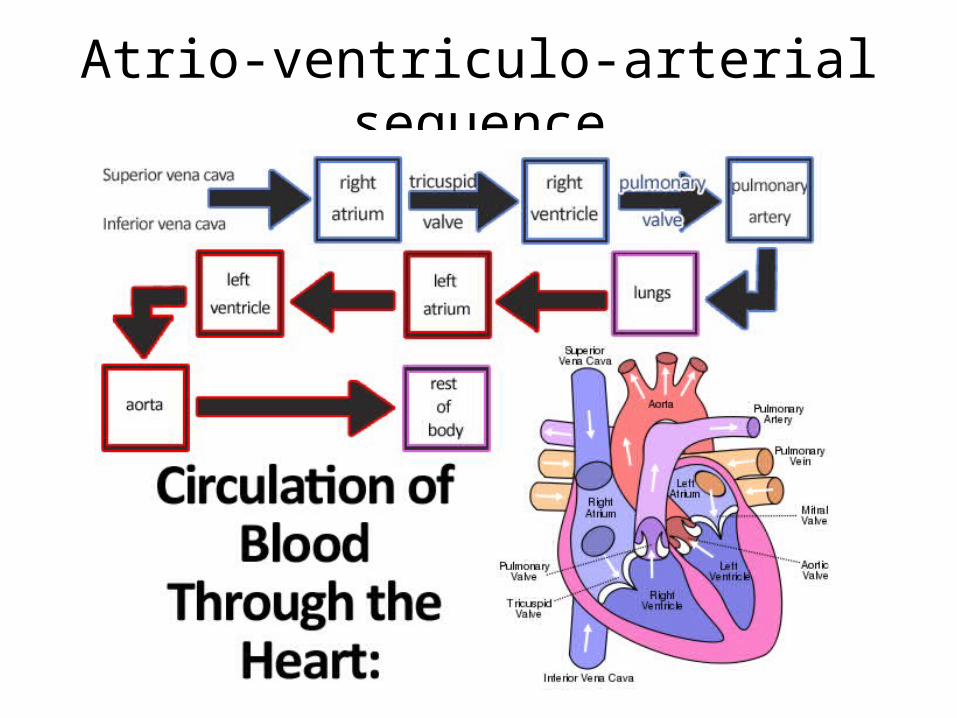
Atrio-ventriculo-arterial sequence

Atrio-ventriculo-arterial sequence
• Concordance
Normal sequence AV & VA
• Discordance
Reversed sequence AV & VA
Corrected TGA = AV discordance + VA discordance

Atrial switch
Corrected TGA = AV discordance + VA discordance

Corrected TGA = AV discordance + VA discordance
Atrial switch
Senning operationMustard operation
Anatomic consideration:

• RV facing systemic pressure
• Pulmonary hypertension may be present
• Baffle may leak or obstruct flow
• Suture line near the SA node
Atrial switchFunctional consideration:

Mysterious RV

Mysterious RV
CO
AFTERLOAD (MEAN PRESSURE)
RV LV
Positive inotropes
45 mmHg 150 mmHg


Mysterious RV

Ventricular interdependence
PVA
SVA

PVA
SVA
Atrial interdependence
Ventricular interdependence

• RV facing systemic pressure
• Pulmonary hypertension may be present
• Baffle may leak or obstruct flow
• Suture line near the SA node
Atrial switch
Functional consideration:
• Evaluation of RV function
• Evaluation of pulmonary pressure
• Evaluation of baffle status
• Evaluation of arrhythmias and pacemaker
Preoperative assesment:


Single ventricle physiology


Mixing lesions
• Defects with mixing of oxygenated and deoxygenated blood
• Partial desaturation lead to compensatory in red cell mass and increase 2,3 DPG with increase in blood viscosity.

Single ventricle physiology

• The driving force for Qp is SVC pressure
• Qp must pass through two separate and highly regulated vascular beds: cerebral and pulmonary vasculature
• Removes the left-to-right shunt and thus the volume load from the single ventricle
Single ventricle physiology

Single ventricle physiology

SVC Pressure
• Acute rise in SVC pressure
• Selection of patients with low PVR minimizes the risk from elevated SVC pressure
• Failure to maintain low SVC pressure lead to problems maintaining adequate SaO2
• Small veno-venous collateral vessel contribute to arterial desaturation

Single ventricle physiology
PSVC = PPA – PPV x
QPA : QSA
QPB : QSB
+ PLA


Single ventricle physiology
PSVC = PPA – PPV x
QPA : QSA
QPB : QSB
+ PLA
PSVC PLA- = PPA – PPV
xQPA : QSA
QPB : QSB
PSVC PLA-
=PPA – PPV
QPA : QSA
QPB : QSB
Minimize SVC Pressure
• Minimize use of positive pressure, including PEEP, following surgery
• Allow the end-expiratory lung volume to approximate FRC
• Minimal mean airway pressure and early extubation in patient with healthy lungs– Negative-pressure ventilation associated with increased Qp
• Higher airway pressure to maintain FRC in pneumonia or ARDS
• Aprotinin and modified ultrafiltration: transpulmonary pressure gradient, less pleural drainage, improved SaO2

Vascular Resistance
• Qp largely dependent on resistance of 2 highly but differentially regulated vascular beds
• Cerebral and pulmonary vasculatures– Opposite responses to changes in CO2, acid-base status,
and O2
– Qp dependent on venous return through SVC (largely cerebral blood flow)
– Hyperventilation following bidirectional cavopulmonary anastomosis impair cerebral blood flow and decrease SaO2
– Inhaled NO may be the best treatment for high PVR and low SaO2 after bidirectional cavopulmonary anastomosis
Volume Unloading
• The right-to-left shunt is eliminated and all Qp is effective pulmonary flow
• An acute increase in wall thickness and decrease in cavity dimension has been associated with improved tricuspid valve function
• Preload and afterload are both decreased• Change in ventricular geometry may increase
risk for systemic outflow obstruction in some
Single ventricle physiology
• Backward effect– Systemic venous congestion– Need for higher SVC pressure to drive flow in
the shunt
• Forward effect– Non pulsatile pulmonary flow– Left atrial filling totally dependant on pulmonary
flow– Systemic hypotension

Single ventricle physiology
• Pitfalls– Saturation is not sytemic pressure dependent
– Saturation is pulmonary pressure dependent
– All circulatory and ventilatory support should bedirected to:
• Lower PVR• Higher SVR• Higher Rt filling pressure(within limits)

Single ventricle physiology
• Pitfalls
(within limits)
↓PVR↑SVR↑CVP
