case study # 1 - 4healtheducation.com4healtheducation.com/pdf/63diabetesmeds.pdf · • employ a...
TRANSCRIPT

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
1
Treatment of Type 2 Diabetes:
CombinationTherapy
1
W. Lane Edwards, Jr., MSN, ARNP, ANP
Affiliate Professor of Nursing
University of Alaska, Anchorage
Internal Medicine Nurse Practitioner
Hospitalist Group of Southwest Florida
Ft . Myers, Florida
Objectives
• Identify the cluster of signs and symptoms that suggest the earliest presence of abnormal glucose disposal
• Discuss the goals for fasting and post meal blood sugars
• Contrast the various classes of medications used to treat diabetes by mode of action
2
y
• Outline combination therapy opportunities for treating diabetes
• Employ a case study to outline the plan of care for a diabetic with abnormal glucose disposal.
Case Study # 1Case Study # 1
3

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
2
Meet Jeff
• CC: Complete physical examination– Additional pertinent information: 47 year-old white male
who presents for a complete physical examination
He has not seen a health care provider for 10 years .
Sleepy after meals, polyuria, blurry vision after larger meal
4
py p y y g
• PHM: Usual childhood diseases– No previous illnesses
• Surgery:– Tonsillectomy - age 5
– Vasectomy – age 35
Jeff
• Family History:– Mother alive – age 77; hypertension and COPD– Father alive – age 79; unknown medical history
• Social History:
5
– Non-smoker– Software engineer working 60 hours per week– No routine exercise program – “active life”– Diet: no particular plan– Alcohol: 1 beer, 2-3 times per week– Drugs: none
Jeff
• Medications:– No daily medications
– Occasional multivitamin
6

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
3
Jeff – Physical Examination
• Weight: 257 lbs• Height: 5’8”• Waist: 47 inches• BMI: 39 1
7
BMI: 39.1• Blood Pressure:
– 3 readings 140/88 mm
• Pulse 95 bpm• Respirations: 18/min• EKG: WNL
Jeff – Laboratory Parameters
• FBS: 93 mg/dL• 2 hr PP Blood Sugar 185 mg/dL• BUN: 18 mg/dL• Creatinine: 0.8 mg/dL• Total Cholesterol: 220 mg/dL
8
• HDL: 34 mg/dL• Triglycerides: 156 mg/dL• LDL: 155 mg/dL• VLDL: 41 mg/dL• AST: 54 mg/dL• ALT: 67 mg/dL• Serum Insulin 46 UU/ml
Conclusions:
• Impaired fasting glucose?– Fasting > 109
• Diabetes, Type 2– Fasting > 126 on two separate occasions
– One time over 200 random
9
One time over 200 random
Does he need medications now?

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
4
Serum Insulin Levels and Insulin Resistance
10www.jewishhospitalcincinnati.com/cholesterol/Research/insulin_resistance.html
Case Study # 2Case Study # 2
11
Meet Allen
• CC: My diabetes is not in control– Additional pertinent information: 43 year-old white male who
employs lifestyle therapy for type 2 diabetes and is reluctant to start oral agents
• PHM: Usual childhood diseases– Diabetic Dyslipidemia
12
y p– Early retinopathy per ophthalmologist– Hypertension – proteinuria 130 micrgrams/L– Obesity (central, abdominal)
• Surgery:– Tonsillectomy - age 5– Vasectomy – age 35

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
5
Allen
• Family History:– Mother died age 64, DM and complications – Father alive – age 73; estranged
Social History:
13
– Non-smoker– Software engineer working 60 hours per week– No routine exercise program – “active life”– Diet: no particular plan– Alcohol: 1 beer, 2-3 times per week– Drugs: none
Allen
• Medications:– None, feels that he gets on meds he will never get off.
14
Allen – Physical Examination
• Weight: 257 lbs• Height: 5’8”• Waist: 47 inches• BMI: 39 1
15
BMI: 39.1• Blood Pressure:
– 3 readings 140/88 mm
• Pulse 92 bpm• Respirations: 18/min• EKG: WNL

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
6
Allen – Laboratory Parameters
• FBS: 146 mg/dL• 2 hr PP Blood Sugar 205 mg/dL• BUN: 18 mg/dL• Creatinine: 0.8 mg/dL• Total Cholesterol: 220 mg/dL
16
• Total Cholesterol: 220 mg/dL• HDL: 34 mg/dL• Triglycerides: 156 mg/dL• LDL: 155 mg/dL• VLDL: 41 mg/dL• AST: 54 mg/dL• ALT: 67 mg/dL• A1C 7.1 %
Obesity and Diabetes: Prevalence Continues to Increase
Obesity From 1994-2005 Diabetes From 1994-2004
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
20042005
17
No Data 10%-14% 15%-19% 20%-24% 25%-29% >30%
No Data <4% 4%-4.9% 5%-5.9% 6+%
*Obesity defined as body mass index (BMI) ≥30, or about 30 lbs overweight for a 5’4” personCenters for Disease Control and Prevention. 2006.
Pathophysiology
18
Pathophysiology

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
7
19
Vascular Biology Working Group, University of FloridaCollege of Medicine, Carl Pepine, MD, Director
Diabetes
• Group of metabolic diseases characterized by hyperglycemia– It results from:
Defects in insulin secretion
Impaired action of insulin
20
Combination of both
Leahy, J.L., Clark, N.G., Cefalu, W.T. Medical Management of DiabetesMellitus: New York, Marcel Dekker, Inc. 2000.
Pre-Diabetes
• Impaired Glucose Tolerance– 2 hour post load plasma glucose > 140 and < 200
• Impaired Fasting Glucose
21
– Fasting glucose > 100 but <126
www.diabetes.org/pre-diabetes/faq.jsp accessed 01/28/07
MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
8
Classifications of Diabetes
• Gestational Diabetes– Glucose intolerance that begins or is detected during
pregnancy
– Increased risk of developing Type 2 diabetes
Current estimates reveal that 50% of women with gestational
22
– Current estimates reveal that 50% of women with gestational diabetes will go on to develop Type 2 diabetes at some point in her lifetime
– Complicates 1% - 12% of all pregnancies or 135,000 pregnancies yearly
Leahy, J.L., Clark, N.G., Cefalu, W.T. Medical Management of DiabetesMellitus:New York, Marcel Dekker, Inc. 2000.
Classifications of Diabetes
• Type 1 Diabetes– Beta Cell Destruction
– Immune Mediated or Idiopathic
– Accounts for 5 – 10% of all individuals with diabetes
• Type 2 Diabetes
23
• Type 2 Diabetes– Insulin resistance with a relative insulin secretory defect to
complete insulin deficiency
– Formerly referred to as adult onset
– Vast majority are obese
Leahy, J.L., Clark, N.G., Cefalu, W.T. Medical Management of DiabetesMellitus:New York, Marcel Dekker, Inc. 2000.
Diabetes – Type 1.5
• Slowly progressing type 1 or latent autoimmune diabetes in adults– Up to 20% of individuals labeled as Type 2 actually have Type
1.5– 50% need insulin within 4 years of being diagnosed
24
• Characterized by presence of antibodies (GAD65) which destroy the pancreas
• Clues: thin, relatively young– Usually no elevated blood pressure, normal triglycerides,
normal HDL
http://www.diabetesnet.com/diabetes_types/diabetes_type_15.php accessed01/28/07

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
9
Stages of Type 2 Diabetes
100
75
Beta Cell Death Patient loses first phase insulin secretion; this isthe first defense against postprandial
hyperglycemiaTime of diagnosis for most individuals
50% beta cell death
25
IGT Post-PrandialHypergly-cemia
Type2 Diabetes
Phase I Type 2 DiabetesPhase II Type 2
DiabetesPhase III
50
25
0-12 -10 -6 -2 0 2 6 10 14
Adapted from Leahy, J.L., Clark, N.G., Cefalu, W.T. Medical Management of DiabetesMellitus:New York, Marcel Dekker, Inc. 2000.
2 X
3 X
26
27
www.byetta.com assessed 9-3-07
MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
10
When and Howdo we measure
28
do we measureblood sugars
Measuring and Treating Impact of Diabetes
•Fasting Blood Sugar?
•2 hrs after the beginning of a meal?
•A1C quarterly?
29
•CGMS
– Continuous glucose monitoring system ( Medtronic)
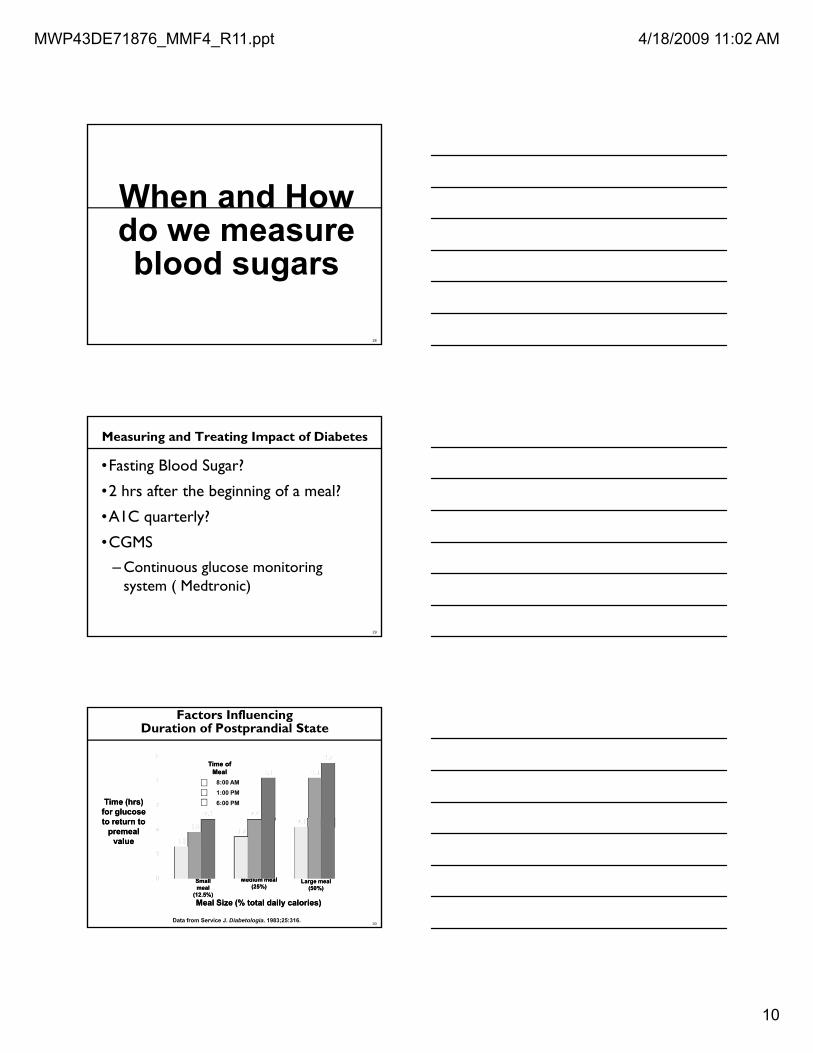
Time (hrs) Time (hrs) for glucose for glucose
Time of Time of MealMeal
Factors Influencing Duration of Postprandial State
8:00 AM1:00 PM6:00 PM
30Data from Service J. Diabetologia. 1983;25:316.
to return to to return to premeal premeal
valuevalue
Meal Size (% total daily calories)Meal Size (% total daily calories)
Small Small mealmeal
(12.5%)(12.5%)
Medium mealMedium meal(25%)(25%)
Large mealLarge meal(50%)(50%)

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
11
Postprandial Glucose Postprandial Glucose Infl enced bInfl enced b
Fasting Glucose Fasting Glucose
HbAHbA1c1c ==
Glucose Contributions to HbA1c
31
++Influenced by:Influenced by:
•• PreprandialPreprandial glucoseglucose•• Insulin secretionInsulin secretion•• Glucose load from mealGlucose load from meal•• Insulin sensitivity in Insulin sensitivity in
peripheral tissuesperipheral tissues
Influenced by:Influenced by:•• Hepatic glucose Hepatic glucose
productionproduction•• Hepatic sensitivity to Hepatic sensitivity to
insulininsulin
..
UKPDS_HDS – Lancet 1998, 352:837-853. Presented at AHA 2000.
Changes in A1c Standardization
• A1c = chronic glycemic control
• Blood Glucose = measure of acute control
• These are different and unrelated units
• How can we better look at acute vs chronic control without difficult conversion equations that may not be
32
without difficult conversion equations that may not be accurate
• So – ADAGE Research group started a new correlation study
Poor Correlation between A1C & BS
33Nathan DM et al Diabetes Care 2008;31:1-6.

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
12
ADAG Study OutcomesNew Correlation A1c & BS
34Nathan DM et al Diabetes Care 2008;31:1-6.
New Acute number on lab slipsA1c Derived Average Glucose
35Nathan DM et al Diabetes Care 2008;31:1-6.
36

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
13
Limitations of HbA1c
• Masks high and low fluctuations….does not reveal glycemic variability.
• Normal to low HbA1c values can be achieved with frequent hypoglycemic episodes.
• Anemia can alter accuracy of A1C
37
Medications: May Increase Glucose
• Atypical antipsychotics
• Centrally acting alpha blockers
• Beta blockers
• Corticosteroids
• Estrogens
• Lithium
• Niacin
• Phenytoin
• Protease inhibitors
38
• Minoxidil
• Diuretics
• Cyclosporine
• Rifampin
• Thyroid preparations
Edelman, S.V., Henry, R.R. Diagnosis and Management of Type 2 Diabetes;6th ed. West Islip, NY; Professional Communications, Inc. 2005.
How do I target my treatment of DM?
• Postprandial hyperglycemia is a significant contributor to A1C levels, particularly at the lower end of A1C’s– For instance:
A1C of 7.3% to 9.2%: postprandial glucose accounts for 50% of this number
39
A1C < 7.3%: postprandial glucose accounts for 70% of this number
Take away message – Allen with an A1C of 8.6% -need work on basal and post meal excursions
Monnier L, Lapinski, H, Colette C. Contributions of fasting and postprandial plasma glucose increments to the overall diurnal hyperglycemia of type 2 diabetic patients: Variations with increasing levels of HbA(1c).
Diabetes Care. 2003;26:881-885.

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
14
Assessing the Damage of Diabetes by A1C
• For every 1% rise in A1c above 6%:– 14% increase in fatal and non fatal MI
– 12% increase in strokes
40
– 43% increase in peripheral vascular disease
– 16% rise in congestive heart failure
UKPDS_HDS – Lancet 1998, 352:837-853. Presented at AHA 2000.
Glycemic Control Reduces Risk of Type 2 Diabetes Complications
19%16%12%14%
0
15
Risk reduction with 1% decline in updated A1c
P<0.0001 P=0.035 P=0.021 P<0.0001
41
43%37%
15
30
45 Micro-vasculardisease
PVD* MI Stroke Heartfailure
Cataractextraction
Source: Stratton IM, et.al (UKPDS). BMJ 2000;321:405-412.
Tight Control…?? !!
• ADVANCE – more mortality
• ACCORD – no change in mortality
• UKPDS – 10 years later
42
y– Intensive glucose lowering, not tight BP control decreased
MI and all cause mortality
– Early and aggressive glycemic control showed protective effects on macrovascular damage
European Assessment for the Study of Diabetes 2008: Holman RR., et al.N Engl J Med, Sept 2008, reviewed online before publication.

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
15
Case StudyCase Study
43
Assessing the Damage of Diabetes
Allan = 7.1%– 28% increase in fatal and non fatal MI
24 2 % i i t k
44
– 24.2 % increase in strokes
– 86% increase in peripheral vascular disease
– 36% rise in congestive heart failure
UKPDS_HDS – Lancet 1998, 352:837-853. Presented at AHA 2000.
Insulin resistance
Glucagon(alpha cell)
Insulin
Islet-cell dysfunction
Major Pathophysiologic Defectsin Type 2 Diabetes
PancreasPancreas
45
Hepatic glucoseoutput
resistance
Glucose uptake in muscle and fat
(beta cell)
Hyperglycemia
Adapted with permission from Kahn CR, Saltiel AR. Joslin’s Diabetes Mellitus. 14th ed. Lippincott Williams & Wilkins; 2005:145–168.Del Prato S, Marchetti P. Horm Metab Res. 2004;36:775–781.Porte D Jr, Kahn SE. Clin Invest Med. 1995;18:247–254.
LiverLiver Adipose Adipose tissuetissue
LiverLiver
MuscleMuscle

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
16
Allen – Initial Intervention
• Life Style Changes– Discussion on Diabetes
– Discussion on Target Organ Damage
– Carb Counting
– Glycemic Index
46
Glycemic Index
– Blood Glucose Testing
– ExerciseAfter stress testing??
Then what if the post meal numbers are high?
BetaBeta--cellcelldysfunctiondysfunction
Major Targeted Sites of Oral Drug Classes Pancreas
Muscle and fatLiver
Sulfonylureas
MeglitinidesDPP-4 inhibitorsIncretin Memetics
47
Glucose Glucose absorptionabsorption
Hepatic glucoseHepatic glucoseoverproductionoverproduction
InsulinInsulinresistanceresistance
DPP-4=dipeptidyl peptidase-4; TZDs=thiazolidinediones.DeFronzo RA. Ann Intern Med. 1999;131:281–303. Buse JB et al. In: Williams Textbook of Endocrinology. 10th ed. Philadelphia: WB Saunders; 2003:1427–1483.
↓Glucose level
Biguanides
TZDs BiguanidesTZDs
Alpha-glucosidase inhibitors
Gut
DPP-4 inhibitors
Biguanides
Incretin Memetics
DPP-4 inhibitorsIncretin Memetics
Major Classes of Medications
1. Drugs that sensitize the body to insulin and/or control hepatic glucose production
ThiazolidinedionesBiguanides
48
2. Drugs that stimulate the pancreas to make more insulin
3. Drugs that slow theabsorption of starches
SulfonylureasMeglitinides
Alpha-glucosidase inhibitors

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
17
Thiazolidinediones
• Thiazolidinediones decrease insulin resistance by making muscle and adipose cells more sensitive to insulin. They also suppress hepatic glucose production.
• Efficacy– Decrease fasting plasma glucose ~35-40 mg/dl (1.9-2.2
49
g p g g (mmol/L)
– Reduce A1C ~0.5-1.0%– 6 – 12 weeks for maximum effect
Thiazolidinediones
• Other Effects– Weight gain, edema – Hypoglycemia (if taken with insulin or agents that stimulate
insulin release)Contraindicated in patients with abnormal liver function or
50
– Contraindicated in patients with abnormal liver function or CHF
– Improves HDL cholesterol and plasma triglycerides; usually LDL neutral
• Medications in this Class: pioglitazone (Actos), rosiglitazone (Avandia), [troglitazone (Rezulin) - taken off market due to liver toxicity]
– WATCH DOSE WITH INSULIN!!
FDA and Avandia (rosiglitazone)
• Nov 14th release
• FDA adds boxed warning for Heart-related risks to Anti-Diabetes Drug Avandia
• “At this time FDA has concluded that there isn’t enough
51
At this time, FDA has concluded that there isn t enough evidence to indicate that the risks of heart attacks or death are different between Avandia and some other oral type 2 diabetes treatments. “
• FDA has requested that GSK conduct a new long-term study to evaluate the potential cardiovascular risk of Avandia.

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
18
Biguanides
• Biguanides decrease hepatic glucose production and increase insulin-mediated peripheral glucose uptake.
• Efficacy– Decrease fasting plasma glucose 60-70 mg/dl (3.3-3.9 mmol/L)– Reduce A1C 1.0-2.0%
• Other Effects
52
– Diarrhea and abdominal discomfort– Lactic acidosis– Cause small decrease in LDL cholesterol level and triglycerides– No specific effect on blood pressure– No weight gain, with possible modest weight loss– Contraindicated in patients with impaired renal function (Serum Cr > 1.4
mg/dL for women, or 1.5 mg/dL for men)
• Medications in this Class: metformin (Glucophage), metformin hydrochloride extended release (Glucophage XR)
Sulfonylureas
• Sulfonylureas increase endogenous insulin secretion• Efficacy
– Decrease fasting plasma glucose 60-70 mg/dl (3.3-3.9 mmol/L)– Reduce A1C by 1.0-2.0%
• Other EffectsH l i
53
– Hypoglycemia– Weight gain – No specific effect on plasma lipids or blood pressure– Generally the least expensive class of medication
• Medications in this Class:– Second generation sulfonylureas: glyburide (Micronase, Glynase,
and DiaBeta), glimepiride (Amaryl), glipizide (Glucotrol, Glucotrol XL)
Meglitinides• Meglitinides stimulate insulin secretion (rapidly and for a
short duration) in the presence of glucose.• Efficacy
– Decreases peak postprandial glucose– Decreases plasma glucose 60-70 mg/dl (3.3-3.9 mmol/L)– Reduce A1C 1.0-2.0%
54
• Other Effects– Hypoglycemia (although may be less than with sulfonylureas if patient has a
variable eating schedule)– Weight gain – No significant effect on plasma lipid levels– Safe at higher levels of serum Cr than sulfonylureas
• Medications in this Class: repaglinide (Prandin), nateglinide (Starlix)

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
19
Alpha-glucosidase Inhibitors
• Alpha-glucosidase inhibitors block the enzymes that digest starches in the small intestine
• Efficacy– Decrease peak postprandial glucose 40-50 mg/dl (2.2-2.8 mmol/L)– Decrease fasting plasma glucose 20-30 mg/dl (1.4-1.7 mmol/L)– Decrease A1C 0.5-1.0%
• Other Effects
55
• Other Effects– Flatulence or abdominal discomfort – No specific effect on lipids or blood pressure– No weight gain– Contraindicated in patients with inflammatory bowel disease or
cirrhosis
• Medications in this Class: acarbose (Precose), miglitol (Glyset)
Efficacy of Monotherapy with Oral Diabetes Agents
Drug Fasting PlasmaGlucose Reduction
(mg/dl)
A1CReduction
(%)Thiazolidinedione 35-40 0.5-1.0
S lf l 60 70 1 0 2 0
56
Sulfonylurea 60-70 1.0-2.0
Biguanide 60-70 1.0-2.0
Meglitinide 60-70 1.0-2.0
Alpha-glucosidaseinhibitor
20-30 0.5-1.0
DeFronzo Annals of Internal Medicine 1999;131:281-303
Nathan N Engl J Med 2002; 347:1342-1349
Sulfonylurea + Biguanide Glyburide + Metformin = Glucovance Glipizide + Metformin = Metaglip
Sulfonylurea + ThiazolidinedioneGlimepiride + Rosiglitazone = AvandarylGli i id + Pi li D (4/30)
Fixed dose combinations for diabetes
57
Glimepiride + Pioglitazone = Duetact (4/30)
Thiazolidinedione + BiguanideRosiglitazone + Metformin = Avandamet Pioglitazone + Metformin = ActoPlus Met
Gliptins + BiguanideSitagliptin + Metformin = Janumet
(50/500;50/1000)

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
20
New Agents
58
New Agents
The Role of Incretins in Type 2 Diabetes
Incretin Effect
In 1964, it was demonstrated that the insulin secretory response was greater when glucose was administered orally
59
response was greater when glucose was administered orallythrough the gastrointestinal tract than when glucose was
delivered via IV infusion
The incretin effect implies that nutrient ingestion causes the gut to release substances that enhance insulin secretion
beyond the release caused by the rise in glucose secondary to absorption of digested nutrients..
New Medications
• Exenatide (Byetta) –– Incretin mimetic
• Exenatide - synthetic version of exendin-4– A naturally-occurring hormone first isolated from the saliva of a
Gila monster (lizard).
60
• Exenatide lowers blood glucose by increasing insulin secretion, suppresses glucagon secretion and slows gastric emptying– Because it only has this effect in the presence of elevated blood
glucose levels, it does not tend to increase the risk of hypoglycemia on its own
Product insert, 2006

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
21
Exenatide
• Indications– Adjunct to metformin, sulfonylureas or combination– For individuals who have not achieved glycemic control with the
above products• Dosage
– Exenatide is injected with morning and evening meals (bid)
61
j g g ( )– 5 mcg bid x 30 days then 10 mcg bid if able to tolerate injected
subcutaneously– Inject in arm, thigh or abdomen 60 minutes before meals– Prefilled pens
Product insert, 2006
AMIGO trials: GLP-1 analog in type 2 diabetes
Active treatmentChange from baseline
Exenatide 5 µg bid
Exenatide 10 µg bid
Placebo
Sulfonylurea1 A1C (%) –0.46 –0.86 +0.12
(N = 377) Weight (lb) 2 0 3 6 1 3
AC 2993: Diabetes Management for Improving Glucose Outcomes; 30-week, placebo-controlled trials of exenatide sc added to oral
hypoglycemic therapy
62
(N = 377) Weight (lb) –2.0 –3.6 –1.3
Metformin2 A1C (%) –0.40 –0.78 +0.08
(N = 336) Weight (lb) –3.6 –6.2 –0.7
Metformin + sulfonylurea3 A1C (%) –0.55 –0.77 +0.23
(N = 733) Weight (lb) –3.6 –3.6 –2.0
1Buse JB et al. Diabetes Care. 2004;27:2628-35.2DeFronzo RA et al. Diabetes Care. 2005;28:1092-100.
3Kendall DM et al. Diabetes Care. 2005;28:1083-91.
Exenatide• Biggest side effect: nausea
– Up to 40% of individuals
• Dosing information:– Consider reducing sulfonylurea dosage when initiating
• Benefits:
63
– Modest weight loss sustained through 82 weeks
– Improved glycemic control
– ? Beta cell preservation

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
22
Incretins Play an Important Role in Glucose Homeostasis
Insulin from beta cells(GLP-1 and GIP)
Release of gut hormones—Incretins1,2
Pancreas2,3
Glucose DependentGlucose DependentGlucose DependentGlucose Dependent
↓ Blood ↓ Blood GI tractGI tract
Food ingestionFood ingestion
↑↑Glucose Glucose uptake by uptake by peripheral peripheral tissuetissue2,42,4
Beta cellsBeta cellsAl h llAl h ll
64
1. Kieffer TJ, Habener JF. Endocr Rev. 1999;20:876–913. 2. Ahrén B. Curr Diab Rep. 2003;2:365–372.3. Drucker DJ. Diabetes Care. 2003;26:2929–2940. 4. Holst JJ. Diabetes Metab Res Rev. 2002;18:430–441.
Glucagon fromalpha cells
(GLP-1)
Glucose DependentGlucose DependentGlucose DependentGlucose Dependent
ActiveGLP-1 & GIP
DPP-4 enzyme
InactiveGIP
InactiveGLP-1
glucoseglucoseGI tractGI tract
↓↓Glucose Glucose production production
by liverby liver
Alpha cellsAlpha cells
Sitagliptin:Indications and Usage
• Monotherapy– JANUVIA is indicated as an adjunct to diet and exercise to improve
glycemic control in patients with type 2 diabetes mellitus.
• Combination therapy
– JANUVIA is indicated in patients with type 2 diabetes mellitus to improve glycemic control in combination with metformin or a PPARγ
i ( hi lidi di ) h h i l l i h di
65
agonist (eg, thiazolidinediones) when the single agent alone, with diet and exercise, does not provide adequate glycemic control.
• Important limitations of use
– JANUVIA should not be used in patients with type 1 diabetes or for the treatment of diabetic ketoacidosis, as it would not be effective in these settings.
PPARγ=peroxisome proliferator-activated receptor gamma.
Caution
• Caution:– Gastroparesis
– Medications that require rapid GI absorptionContraceptives
66
p
Antibiotics
Product insert, 2006

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
23
Pramlintide
• Pramlintide (Symlin) - synthetic form of the hormone amylin, produced by the beta cells in the pancreas.
• Amylin, insulin and glucagon work together to maintain normal blood glucose levels.
• Pramlintide injections are taken with meals
67
• Pramlintide injections are taken with meals– No hypoglycemia (alone) or weight gain– May even promote modest weight loss– Biggest side effect: nausea - which tends to improve over time – Pramlintide cannot be combined in the same vial or syringe with
insulin
Product insert, 2006
Case StudyCase Study
68
Allen – Physical Examination
• Weight: 257 lbs• Height: 5’8”• Waist: 47 inches• BMI: 39 1
69
BMI: 39.1• Blood Pressure:
– 3 readings 140/88 mm
• Pulse 92 bpm• Respirations: 18/min• EKG: WNL

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
24
Allen – Laboratory Parameters
• FBS: 146 mg/dL• 2 hr PP Blood Sugar 205 mg/dL• BUN: 18 mg/dL• Creatinine: 0.8 mg/dL• Total Cholesterol: 220 mg/dL
70
• Total Cholesterol: 220 mg/dL• HDL: 34 mg/dL• Triglycerides: 156 mg/dL• LDL: 155 mg/dL• VLDL: 41 mg/dL• AST: 54 mg/dL• ALT: 67 mg/dL• A1C 7.1 %
Allen
• Medications:– None at this time
71
So, what to do• Sensitizers
– TZD
– Metformin “ bring the body back to baseline”
• Incretins– Oral – Januvia / Janumet
72
• SU– Lets burn out the pancreas and get to insulin sooner?
• Inhaled Insulin– now off the market due to $$$
• Insulin sub q– Lispro + basal
• Insulin Pump

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
25
Guideline Recommendations Are Becoming More Aggressive
• 2007 ADA standards1
– “The A1C goal for patients in general is an A1C goalof <7%.”
– “The A1C goal for the individual patient is an A1C as close to normal (<6%) as possible without significant hypoglycemia.”
73
yp g y
ADA=American Diabetes Association; EASD=European Association for the Study of Diabetes.1. American Diabetes Association. Diabetes Care. 2007;30(suppl 1):S4–S41. 2. Nathan DM et al. Diabetes Care. 2006;29:1963–1972.
• ADA/EASD consensus statement2
– “If lifestyle intervention and maximal tolerated dose of metformin fail to achieve or sustain glycemic goals, another medication should be added within 2–3 months of the initiation of therapy or at any time when A1C goal is not achieved.”
How do I target my treatment of DM?
• Postprandial hyperglycemia is a significant contributor to A1C levels, particularly at the lower end of A1C’s– For instance:
A1C of 7.3% to 9.2%: postprandial glucose accounts for 50% of this number
74
A1C < 7.3%: postprandial glucose accounts for 70% of this number
Take away message – Jeff with an A1C of 7.2% - look very closely at reducing postprandial glucose
Monnier L, Lapinski, H, Colette C. Contributions of fasting and postprandial plasma glucose increments to the overall diurnal hyperglycemia of type 2 diabetic patients: Variations with increasing levels of HbA(1c).
Diabetes Care. 2003;26:881-885.
Insulin Therapywhere
Food becomes a
75
Food becomes a medicine to maintain
Blood sugars!Must have fixed carbohydrate intake
For fixed AC insulin dose – (bad)

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
26
Starting Insulin
• Prepare for the WORST ( MDI)– Needle phobia
– Hypoglycemia
– Increased intravascular volume
– Bad insulin and weird values
76
Bad insulin and weird values
– Ketoacidosis
– Weight gain
– Sick days
Back to the Basics
• Significant patient education now--- face time
• Start with description of what goals are– AC 100 mg/dL; 2 hour post meal < 135 mg/dL
• Revisit carbohydrate counting
77
• Revisit carbohydrate counting
• Revisit glycemic index
• Revisit hypoglycemic protocol
• Revisit lactic acidosis (DKA)
• Introduce strict regimen of blood sugar testing and multiple dosing of insulin ( about 4 day)
Label ReadingLabel Reading
What is the serving size?What is the serving size?
78
How many grams of Carbohydrates?
How many grams of Carbohydrates?
How many grams of Fat?
How many grams of Fat?

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
27
Preparing the patient for insulin
• Carbohydrate Counting
• 1 piece of white bread
• 12 cherries
• Glycemic Index
• 72
• 22
79
• 2” apple
• ½ cup strawberries
• ½ cup watermelon
• M&M Choc Peanut– Individual serving
• 38
• 32
• 72
• 33
• Peanut Butter
HypoglycemicProtocol
80
Hypoglycemic Protocol
• Feel low ( or check low)
• Check blood sugar if can
• 15 grams of glucose– Not something that has to be converted to glucose
• Wait 15 minutes
81
• Wait 15 minutes
• Take Blood Sugar
• 15 grams of glucose
• If blood sugar is now acceptable, have a low glycemic snack to maintain blood sugar
• Evaluate why hypoglycemia occurred.

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
28
Insulin Choices
82
83
Insulin Choices
• Rapid Acting Insulin
• Short Acting Insulin
• Intermediate Acting Insulin
• Mixes
L A ti I li
84
• Long Acting Insulin
• Combination Insulin
• rapid acting only (The Pump)

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
29
Rapid Acting Insulin
Examples Onset Peak Duration Advantages Disadvantages
Glulisine(Apidra)
10-15 min
40-70 3-5 hr Rapid absorption (even in obesepatients)Short half life
High cost vs regular
Lispro(Humilog)
15 min 40-70 3-5 hr Short half life High cost vs regular
85
Aspart(NovoLog)
15 min 40-50 3-6 hr Short half life High cost vs regular
Slightly longer duration of action than other rapid acting insulins
Product inserts accessed 2-1-08
300
350
250
NovoLog®Humalog®
(pm
ol/L
)
Rapid Acting Insulins
86
200
150
100
50
0
Free
Insu
lin (
Hedman, Diabetes Care 2001; 24(6):1120-21
0 60 120 180 360 480
Time in Minutes
Product inserts
Short Acting Insulin
Examples Onset Peak Duration Advantages Disadvantages
Regular Insulin
Regular Iletin,Humulin R, Novolin R,Velosulin BR
30 –60 min
50 –120 min
3-8 hrs Low cost Long duration of action may lead to :
Nocturnal hypoclycemias
87
Velosulin BR
Product inserts accessed 2-1-08

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
30
Intermediate Acting Insulin
Example Onset Peak Duration
Advantages Disadvantages
NPH
NHP Iletin IIHumulin NNovolin N
1-3 hrs 8 hrs 20 hrs Low cost Peak at 6-8 may lead to hypoglycemia
L t 1 2 5 7 15 18 24 L t U di t bl k
88
Lente
Lente Iletin IIHumulin L
1-2.5 hrs
7-15 hrs
18- 24 hrs
Low cost Unpredictable peaks may lead to hypoglycemia
Product inserts accessed 2-1-08
Intermediate & short/rapid acting mixes
Examples Onest Peak Duration
Advantages Disadvantages
50/5070/3075/25
NPH withRegular
Depends Depends Depends Convenient administration
Not possible to customize delivery of short and rapid acting insulin to patients
89
RegularLisproProtamineAspart
Product inserts accessed 2-1-08
Long Acting – Basal Insulin
Examples Onset Peak Duration Advantages Disadvantages
Detemir(Levemir)
1- 2 hrs
None 12-24 hrs Continuous doselevels prevents hypoglycemia
Shorter duration than insulin glargine
May be better bidAlbumin binding –Dose level may change in hypoalbuminemic pts
90
hypoalbuminemic pts
Glargine(Lantus)
1 hr None 24 hrs Continuous doselevel prevents hypoglycemia; can be administered once daily
High cost;Not effective for postprandial glucose elevations; can not be mixed with short acting insulin
Product inserts accessed 2-1-08

MWP43DE71876_MMF4_R11.ppt 4/18/2009 11:02 AM
31
usio
n ra
te/m
in)
Basal InsulinsGlargine, Detemir
91
Glu
cose
infu
(mg/
kg/
Time (h) after s.c. injection
Just wanted
To say it
92
To say it
FORMALLY!For
Listening
93
239-810-1859 [email protected]