case study discussions on the nurse’s role in caring for ... and case study ... if there is...
TRANSCRIPT

10/26/2015
1
Case Study Discussions on the Nurse’s Role in Caring
for Patients With Hematologic Malignancies
Welcome and Overview
Lauren Berger, MPHSenior Director, Professional Education and Engagement
The Leukemia & Lymphoma Society
Case Study Discussions on the Nurse’s Role in Caring for Patients With Hematologic Malignancies
www.LLS.org/CE2

10/26/2015
2
Faculty Disclosures
• Emily Bennett, RN, BSN
• Beth Finley, RN, BSNc, OCN
• Lynn Rich, ANP-BC,OCN
Have no affiliations with commercial interests to disclose
3
Acute Promyelocytic Leukemia (APL) Overview and Case Study
Emily Bennett, RN, BSN Nurse Navigator
Winship Cancer InstituteEmory University
Atlanta, GA
Case Study Discussions on the Nurse’s Role in Caring for Patients With Hematologic Malignancies
4

10/26/2015
3
Outline
• Leukemias and outcomes
• History of APL
• Epidemiology
• Treatment and outcomes in large trials
• What happens outside of a trial
• High mortality outside of a trial
• What is involved in our co-management
5
Leukemias and Outcomes
Chronic Leukemias• Chronic myelogenous
leukemia (CML) – Imatinib (Gleevec) ≥90%
survival• Chronic lymphocytic
leukemia (CLL)– Indolent disease in the elderly– Wide array of treatments is
available
Acute Leukemias• Acute lymphoblastic
leukemia (ALL) – Generally pediatric disease
with ≥80% cure rate– Cure rates are approximately
40%–50% in adults• Acute myelogenous
leukemia (AML)– Generally seen in older
patients– M1 to M7: 50% cure rate
across the spectrum• M3 – Acute promyelocytic
leukemia (APL)
6

10/26/2015
4
APL Therapy – History
7
ATO, arsenic trioxide; ATRA, all-trans retinoic acid; CT, chemotherapy; GO, gemtuzumab ozogamicin; RA, retinoic acid.Chen Y, et al. Cancer. 2012;118(23):5811–5818.Nowak D, et al. Blood. 2009;113(16):3655–3665.
First description:Hyperacute fatal illness
associated with hemorrhagic syndrome
First description:Hyperacute fatal illness
associated with hemorrhagic syndrome
Daunorubicin in APL
Daunorubicin in APL
In vivo leukemic cell
differentiation
In vivo leukemic cell
differentiation
Discovery t(15;17) in APL
Discovery t(15;17) in APL
ATRA therapyATRA therapy
Differentiation of APL cells with
RA
Differentiation of APL cells with
RA
ATRA + CTATRA + CT
ATO in relapseATO in relapse
ATO frontline
ATO frontline
ATRA + ATO ± GO
ATRA + ATO ± GO
7
APL Diagnosis – Pathology
• Pancytopenia – low counts
• DIC common
• Bruising – typical complaint
• Bleeding – quite serious
‒ Serious bleeds with normal lab findings
• CNS bleeds – common
‒ Most likely reason for patient deaths due to bleeding
8CNS, central nervous system; DIC, disseminated intravascular coagulation.
Sanz MA, et al. Blood. 2009;113(9):1875–1891.. 8

10/26/2015
5
APL – Epidemiology
• APL is an uncommon disease with approximately 1000 new cases per year in the US
• Rare below 10 years of age
• Most common between the ages of 20 and 60 years
• Historically, this is the first disease for which targeted treatment was developed
• Highly effective and curable treatments
– All-trans retinoic acid (ATRA), arsenic trioxide (ATO), and anthracyclines
9
APL Treatment and Outcomes in Large Trials
Case Study Discussions on the Nurse’s Role in Caring for Patients With Hematologic Malignancies
10

10/26/2015
6
APL Survival in Large Cooperative Group Trials
1111OS, overall survival.
Australasian APML4 (adding ATO to ATRA/chemo)
12CI, confidence interval; DFS, disease-free survival; EFS, event-free survival; HR, hazard ratio; OS, overall survival. 12

10/26/2015
7
ATRA/ATO vs ATRA/Chemotherapy
1313
EFS
prob
abili
tyC
umul
ativ
e in
cide
nce
of re
laps
e
What Happens Outside of a Trial
Case Study Discussions on the Nurse’s Role in Caring for Patients With Hematologic Malignancies
14

10/26/2015
8
Case Study – Real-World Patient
• 56-year-old female; Jehovah’s Witness
• Current diagnosis of flu, normal CBC (early December), treated with Tamiflu; DVT (late December), repeat CBC showing pancytopenia
• Subsequent work-up resulted in a diagnosis of APL
• Refused blood transfusions, so she was supported with cryoprecipitate, Aranesp, Procrit and
G-CSF, which was approved by her congregation
CBC, complete blood count; DVT, deep vein thrombosis; G-CSF, granulocyte colony-stimulating factor. 15
Population-Wide Survival in the US
• Survival of 90% in multicenter trials is not a reflection of the outcome in the general population. Death rate of 5% to 10% is an underestimate
• Recent analysis of US SEER data from 2000–2008 by investigators from MD Anderson showed 71% survival at 1 year and 64% at 5 years
• Current trials that are changing sequence, adding new drugs, and/or withholding maintenance will only have a minimal effect on the survival
• Biggest impact will be made by decreasing early deaths
16Chen Y, et al. Cancer. 2012;118(23):5811–5818. 16

10/26/2015
9
SEER Data (1975–2008)
Chen Y, et al. Cancer. 2012;118(23):5811–5818. 17
Survival Data From SEER Registries
18
0
10
20
30
40
50
60
70
80
90
Sfo SJ LA CA CT HI ATL GA IA KY Lo DTW NJ NM UT Seat
1 yr Survival
2005‐2011 (post atra)
Expected ~95%
18

10/26/2015
10
Early Deaths in APL (Days 1 to 30)
1919
Why Is There High Mortality Outside of a Trial?
Case Study Discussions on the Nurse’s Role in Caring for Patients With Hematologic Malignancies
20

10/26/2015
11
Possible Reasons
• Selection bias: possible reason • Delayed treatment
– Delay in ATRA treatment is commonly cited but not the case
• Decreased supportive care?– Probably the biggest reason
• Prior to ATRA, early deaths in GIMEMA were <10• They have a network of treatment centers that follow
written guidelines• MD Anderson had 5/44 early deaths in their clinical trial
but 9/40 after the trial closed
2121
Can We Do Something Different?
2222Image used with permission from Bearman Cartoons.

10/26/2015
12
Strategy (at GRU)
• Developed a simple 1.5-page treatment algorithm
• Quick diagnosis
• Ad hoc meeting and treatment planning
• Rapid initiation of therapy
• Aggressive management of coagulopathy
• Prevention of differentiation syndrome; early recognition and management of ATRA syndrome
• Prophylaxis and aggressive treatment of infections
• Implemented in 2010
2323
Methods Used to Decrease Early Deaths
• Reviewed the literature
• Reviewed all patient charts
• Attended national meetings and talked to experts
• Attended the International APL meeting in Rome
• Obtained an external consultant to review our death charts
• Identified the three main causes of death in the first month: BLEEDING, DIFFERENTIATION SYNDROME AND INFECTION
• Implemented a proactive, simple program to decrease early deaths—at a point when the rest of the country did not recognize this as a problem
2424
10/26/2015
13
What Is Involved in Our Co-Management
25
Case Study Discussions on the Nurse’s Role in Caring for Patients With Hematologic Malignancies
Treatment Outside Our Center
• Co-manage patients
• Text or email has worked very well
• Discuss day-to-day care in case they are more complicated
• Idea is to get them through induction
2626

10/26/2015
14
APL – Workup
• Quick diagnosis
• Rapid initiation of therapy
• Aggressive management of coagulopathy
• Prevention of differentiation syndrome; early recognition and management of ATRA syndrome
• Prophylaxis and aggressive treatment of infections (APL IS A MEDICAL EMERGENCY. TREATMENT WITH ATRA SHOULD BE STARTED ASAP)
• Labs, BMBX, ECHO, PICC (no invasive procedures)
BMBX, bone marrow biopsy; ECHO, echocardiogram; PICC, peripherally inserted central catheter. 27
Supportive Care
• Tumor lysis prophylaxis
• Antibacterial prophylaxis – Levofloxacin 500 mg QD
• Antifungal prophylaxis – Voriconazole 200 mg PO BID or posaconazole 200 mg PO TID
• Antiviral prophylaxis – Acyclovir 400 mg BID
• Keep hemoglobin in the 8 range
• APL IS A MEDICAL EMERGENCY. TREATMENT WITH ATRA SHOULD BE STARTED ASAP
BID, twice daily; PO, orally; QD, daily; TID, three times daily. 28

10/26/2015
15
Treatment of Coagulopathy
• Coagulopathy is a major problem. Procoagulants released by leukemia cells and fibrinolysis
• Intracranial, pulmonary and GI bleeding
• Treatment with ATRA should start ASAP
• Keep platelets above 50,000
• Keep fibrinogen above 150
• If there is clinical evidence of bleeding, give FFP twice a day as you are starting ATRA and chemotherapy until bleeding resolves
• After all clinical and lab coagulopathy resolves, blood product support is like any other leukemia
29FFP, fresh frozen plasma; GI, gastrointestinal. 29
Differentiation Syndrome
• Dyspnea, unexplained fever, weight gain, ARF, CHF, pleuropericardial effusions and interstitial pulmonary infiltrates
• Meticulous monitoring of intake and output. Daily weights
• Keep I/O matched (SHOULD BE METICULOUS)
• Diuretics should be used if there is evidence of fluid retention and weight gain
• Dexamethasone 10 mg BID should be started as soon as symptoms are noted
• In patients with a WBC >10,000, dexamethasone 10 mg BID could be started before initiating ATRA
• Temporary discontinuation of ATRA or ATO is indicated only in case of severe APL differentiation syndrome
30ARF, acute renal failure; BID, twice daily; CHF, congestive heart failure; WBC, white blood count. 30

10/26/2015
16
Treatment: AIDA Regimen Example
• Induction – Low-risk patients
• WBC <10,000 and platelet count >40,000
• GIMEMA protocol. ATRA on day 1 followed by idarubicin 12 mg/m2 on days 2, 4, 6 and 8 (AIDA)
– Intermediate-risk and high-risk patients• WBC >10,000 and platelet count <40,000
• ATRA to be started as soon as diagnosis is suspected
• Idarubicin to be started on the same day and given per the GIMEMA protocol on days 1, 3, 5 and 7. Even if genetic results are unavailable, it is reasonable to give anthracycline
• Older patients (individualized)
31WBC, white blood count.
Older Patients With APL
• Need to individualize
• Maybe begin with single-agent ATRA
• Dose reduction of ATO
• Meticulous supportive care
3232

10/26/2015
17
Nursing Considerations
• Meticulous monitoring of patient during the first 10 days during which 70% of deaths occur
• Primary goal is to decrease early deaths within the first month; three main causes of death in the first month: BLEEDING, DIFFERENTIATION SYNDROME AND INFECTION
• Rapid initiation of therapy • Aggressive management of coagulopathy• “Normal” laboratory values can still cause bleeding• Prevention or early recognition and management of ATRA
syndrome• Prophylaxis and aggressive treatment of infections• Outpatient consolidation, provide calendars, dialogue with
patient and family
33
Consolidation and Maintenance
• Generally depends on induction protocol
• If you pick a regimen, try to stick with the same follow-up treatments
‒ Two to three cycles of anthracycline-based consolidation, given along with ATRA
‒ ATO-based consolidation
• After completion of consolidation, a bone marrow evaluation should be done to demonstrate molecular remission
‒ If molecular remission is achieved, maintenance with 1–2 years of oral ATRA + MTX and 6MP may be beneficial
6MP, 6-mercaptopurine; MTX, methotrexate. 34

10/26/2015
18
Algorithm
35
Work Up CBC, CMP, and DIC Panel to include Fibrinogen, D-Dimers, PT and PTT twice a day until all laboratory and clinical coagulopathy is completely resolved. Echocardiogram. Bone Marrow Examination. Aspirate, Biopsy, Flow cytometry, Cytogenetics, FISH for PML-RAR alpha and PML-RAR alpha by PCR. Tumor banking if available. Baseline Chest X-ray PICC Line. Do NOT attempt to put central lines or perform other surgically invasive procedures such as Bronchoscopy or Spinal Tap. DAY 14 Marrow is not necessary.
Supportive care Tumor Lysis prophylaxis. Antibiotic Prophylaxis with Levofloxacin 500 mg po qd or similar antibiotic. Antifungal prophylaxis with Posaconazole 200 mg po tid, Voriconazole 200 mg po bid or another agent with similar efficacy Anti-viral prophylaxis with Acyclovir 400 po bid or Valacyclovir 1000 mg PO daily Red Cell transfusion is similar to other Leukemia Induction and suggested to transfuse at or below 7gm/dl. APL IS A MEDICAL EMERGENCY. TREATMENT WITH ATRA SHOULD BE STARTED ASAP.
Coagulopathy Intracranial, Pulmonary and GI Hemorrhage. Risk of Bleeding is worse in patients with Active Bleeding, Hypofibrinogenemia, Increased levels of D-Dimers, prolonged PT and PTT, increased WBC, increased Peripheral Blasts, Renal Failure and poor PS
Treatment with ATRA should start ASAP Keep platelets above 50,000 If there is clinical evidence of bleeding at presentation from needle sticks, Bone Marrow Biopsy sites, give 4 units of FFP as you are starting the ATRA and Chemotherapy. Continue FFP support twice a day until
clinical bleeding resolves. Keep fibrinogen above 150. Use cryoprecipitate if needed After all clinical and laboratory coagulopathy has resolved, the guidelines for blood product support are similar to management of other leukemias.
Differentiation
Syndrome Meticulous monitoring of Intake and Output. Daily weights Keep I/O matched (SHOULD BE METICULOUS). Diuretics should be used if clinically there is evidence of fluid retention and weight gain. Dexamethasone at 10 mg BID should be started as soon as symptoms are noted. In patients with a WBC >10,000, Dexamethasone 10 mg bid could be started before initiating ATRA Temporary discontinuation of ATRA or Arsenic Trioxide (ATO) is indicated only in case of severe APL DS. Dexamethasone should be maintained until complete disappearance of symptoms and ATRA or ATO should be restarted. Dexamethasone should be stopped 3 days after all DS symptoms have resolved.
Anthracycline based Induction INDUCTION OF LOW RISK PATEINTS (WBC <10,000/ml and Platelets >40,000/ml) GIMEMA protocol. ATRA on Day 1 followed by idarubicin 12 mg/m2 on Days 2, 4, 6 and 8.INDUCTION OF INTERMEDIATE RISK AND HIGH RISK PATIENTS(WBC> 10,000 and Platelet count <40,000) Idarubicin to be started on the same day and given per the GIMEMA protocol on days 1, 3, 5 and 7. Even if the genetic results are not available, it is reasonable to give the anthracycline. Aggressive management of coagulopathy.
Arsenic trioxide based induction Can be considered in the following patient groupsa) Low and intermediate risk patients (WBC < 10,000/ml)b) Age >70 c) Not candidates for conventional chemotherapy for any reason. Should be restricted to patients with confirmed PML-RAR alpha. ATRA at 45 mg/m2 in divided doses twice a day along with Arsenic at 0.15 mg/kg daily, both continued till complete hematologic remission. Watch for differentiation syndrome. Follow for prolongation of QT interval. Keep Mg above 2.0 and K above 4.0. Follow LFTs and for grade 2 to 4 Liver Dysfunction, HOLD Arsenic.
Hydroxyurea use for Leukocytosis:
NO LEUCOPHERESIS
WBC 5 - 10k – Hydroxyurea 500 mg q day WBC 10 – 15k Hydroxyurea 500mg BID WBC 15 – 20k – Hydroxyurea 500mg TID WBC 20 – 50k – Hydroxyurea 500 mg QID WBC > 50k – Hydroxyurea 1000 mg QID Could also give a dose or two of Idarubicin 12mg/m2 if the Leukocytosis does not resolve or DS does not resolve in spite of using Dexamethasone. 35
Experience in Other Diseases
• STEMI – Shorter door-to-balloon time improves survival
• In stroke patients, administration of TPA within 3 to 4.5 hours of symptom onset improves survival
• THE GOAL IS TO STREAMLINE THE PROCESS
36
STEMI, ST-segment elevation myocardial infarction; TPA, tissue plasminogen activator.McNamara RL, et al. J Am Coll Cardiol. 2006;47(11):2180–2186.Hacke W, et al. N Engl J Med. 2008;359(13):1317–1329. 36
10/26/2015
19
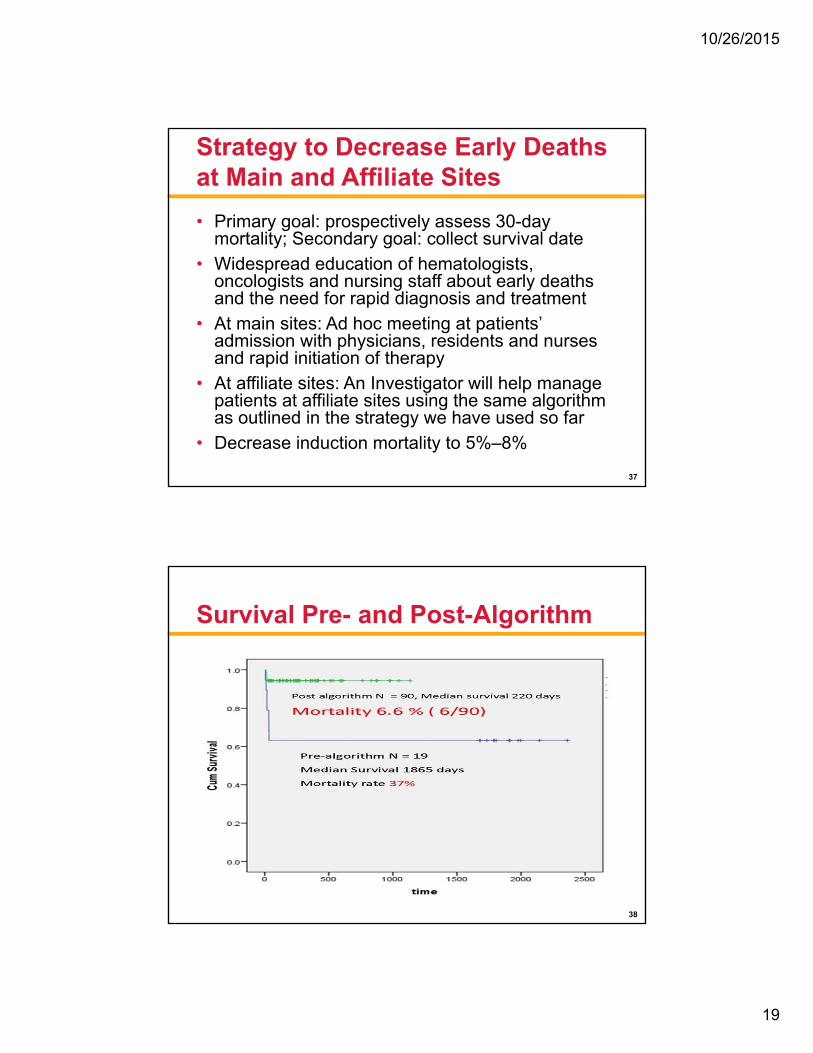
Strategy to Decrease Early Deaths at Main and Affiliate Sites
• Primary goal: prospectively assess 30-day mortality; Secondary goal: collect survival date
• Widespread education of hematologists, oncologists and nursing staff about early deaths and the need for rapid diagnosis and treatment
• At main sites: Ad hoc meeting at patients’ admission with physicians, residents and nurses and rapid initiation of therapy
• At affiliate sites: An Investigator will help manage patients at affiliate sites using the same algorithm as outlined in the strategy we have used so far
• Decrease induction mortality to 5%–8%
3737
Survival Pre- and Post-Algorithm
38

10/26/2015
20
Planned Coverage on New NCI-ECOG Trial
Cover entire population of ~15 m
Half the population of AL: ~2.5 m
Half the population of FL: ~10 mDr. James Foran
Half the population of MN: ~2.5 m Sub I: Dr. Mark Litzow
Half of NC and TN: ~8 m
Half of IL: ~5 m Dr. Altman
Parts of NY and PA: ~10 mDr. TallmanDr. Luger
States with Investigators:ECOG centers:
39ECOG, Eastern Cooperative Oncology Group; NCI, National Cancer Institute.
Resources
• Difficult obtaining patient assistance for drug• Very expensive • No patient assistance programs for drug cost• The Leukemia & Lymphoma Society’s
Information Resource Center (refer to support and financial assistance programs)
• Limited pharmaceutical assistance program• Social work (prescription plans, financial,
transportation)
40

10/26/2015
21
Conclusions
• Early deaths can and SHOULD be prevented in APL
• This concept was already validated in Latin America—Brazil, Chile,
Uruguay and Mexico. Decreased early deaths from 32% to 15%
• Expedite diagnosis and treatment
• Proactively manage the three main causes of death
• Treating oncologists may be unaware of the problem
• Minimize complications from the presence of thrombocytopenia/
bleeding/infection
• APL is a curable disease amongst the leukemias
Rego EM, et al. Blood. 2013;121(11):1935–1943. 41
Thank You
42
Case Study Discussions on the Nurse’s Role in Caring for Patients With Hematologic Malignancies

10/26/2015
22
Chronic Lymphocytic Leukemia (CLL)Overview and Case Study
Lynn Rich, ANP-BC, OCNNurse Practitioner
JP Wilmot Cancer InstituteUniversity of Rochester
Rochester, NY
Case Study Discussions on the Nurse’s Role in Caring for Patients With Hematologic Malignancies
43
Outline
• Define disease • Describe how CLL/SLL is different from
leukemia: acute vs chronic leukemia• Natural history of disease• Epidemiology• Rai staging • Goal of treatment• Case study
44

10/26/2015
23
What Is CLL?
• Chronic lymphocytic leukemia (CLL) is a cancer of the lymphocytes that normally work as immune cells to protect against infections
CLL Cell
Red Blood Cells
Image courtesy of JP Wilmot Cancer Institute; Chronic Lymphocytic Leukemia (CLL) Booklet. 45
Smudge Cell
CLL
• CLL is caused when a single B lymphocyte becomes abnormal because of damage (mutation) to its DNA
• Once this occurs, the body no longer controls this cell, so it continues to divide and lives longer than it should
• This abnormal cell becomes CLL
46

10/26/2015
24
CLL vs SLL
• Small lymphocytic lymphoma (SLL) is a variant of the disease in which there are not a lot of abnormal lymphocytes in the blood
• World Health Organization (WHO) classification considers the two diseases to be identical—one disease at different stages
47
CLL – Lymphocyte dysfunction is in the bone marrowSLL – There is more lymph node and lymphoid tissue involvement (vs bone marrow) 48

10/26/2015
25
CLL vs Acute Leukemia
• Chronic leukemias usually progress slowly, and there are a greater number of mature cells that can generally carry out normal function
• Acute leukemias are diseases that progress rapidly and affect cells that are not fully developed
49
Image courtesy of JP Wilmot Cancer Institute; Chronic Lymphocytic Leukemia (CLL) Booklet. 50

10/26/2015
26
How Is CLL Diagnosed?
• Often found on random complete blood count (CBC) by primary
• Notice an elevated white blood count (WBC), specifically elevated lymphocytes
51
Case Study: Maria S.
• 76-year-old widowed female in reasonably good heath; no other comorbidities
• Retired bus driver • Lived in upstate NY • March 2011: went to primary
– Fatigue; “just did not seem right”
• Noted to have elevated WBC: 30 (normal 4–10)• Was sent to local community oncologist
52

10/26/2015
27
Normal CBC
• WBC – normal 4–10• Differential:
– Neutrophils: 1.8–5.4 K/uL (ANC)– Lymphocytes: 1.3–3.6 K/uL (ALC)– Monocytes: 0.3–3.6 K/uL– Eosinophils: 0–0.5 K/uLALC >5.0 – criteria to meet CLL (lymphocytosis)
must show clonality on peripheral blood
• 2008 update of the National Cancer Institute guidelines
ALC, absolute lymphocyte count; ANC, absolute neutrophil count. 53
Natural History of CLL
• Considered indolent (slow-growing) in nature
• Can watch for 5–10 years without intervening
• Life expectancy could be 10–20 years• However, some patients need treatment
quickly and aggressively• How can we tell?
54
10/26/2015
28
Further Staging: FISH(fluorescent in situ hybridization)
• 13 q = favorable (17-year median OS)• Trisomy 12 and 11 q = less favorable
(9–11 years)• 17p – associated with mutated TP53
– Poor response rate– Short duration of response with standard
treatment– Most unfavorable prognosis (7-year median OS)
Example: Combined 11q + 17p = more unfavorable
OS, overall survival.
Wormsley SB, et al. Blood. 1990;76(1):123–130. 55
Case Study: CBC at Presentation
• WBC: 30• ALC: 6.0• What else is needed when initially diagnosed?• Obtain CT staging scans
• Assess for organomegaly, extent of lymphadenopathy• Patient did not have
• Obtain bone marrow biopsy• Assess for evidence of disease; if so, how much?• Patient had 85% CLL in bone marrow
ALC, absolute lymphocyte count; CT, computed tomography. 56
10/26/2015
29
Epidemiology
• In 2013, an estimated 119,386 people in the United States were living with CLL
• 15,720 people were expected to be diagnosed with CLL in 2014
The Leukemia & Lymphoma Society. Chronic Lymphocytic Leukemia. 2014.
Total CLL
CLL 2014
Total CLL expected in 2014: 120,000New CLL cases in 2014: 15,720
57
Epidemiology (cont’d)
• The most common type of leukemia in Western countries
• Considered disease of the elderly
• Median age at diagnosis is 70 years
• However, not unusual to make this diagnosis in younger individuals from 30–39 years of age
58

10/26/2015
30
Risk Stage Description
Low 0 Lymphocytosis in blood or bone marrow
Intermediate
I Lymphocytosis + enlarged lymph nodes
II Lymphocytosis + enlarged liver or spleen with/without lymphadenopathy
High
III Lymphocytosis + anemia (Hgb <11), with/without enlarged liver, spleen or lymph nodes
IV Lymphocytosis + thrombocytopenia (<100) with/without anemia, enlarged liver, spleen or lymph nodes
Hgb, hemoglobin.International Workshop on CLL. Ann Intern Med. 1989;110(3):236–238.
Modified Rai Clinical Staging for CLL
59
Case Study: Patient
• March 2011: Presented with intermediate Rai stage • August 2011: Rituximab• October 2011: Bendamustine/Rituximab• January 2012: Increasing WBC, enlarging organomegaly• Responded poorly: ALC from 30 to 100
• Referral made to CLL specialist at University of Rochester: clinical trial options
ALC, absolute lymphocyte count. 60

10/26/2015
31
61
Ibrutinib: BTK
• 140-mg oral tablet:– CLL dose is 480 mg daily
– FDA approved in 2014
62

10/26/2015
32
Case Study: Treatment Course
0
50
100
150
200
250
300
Lenalidomiderituximab
IdelalisibGS-9973
Ibrutinib
• Significant lymphocytosis: WBC spikes within first month of treatment• Usually takes 2–3 months for WBC to return to normal
63
Other Nursing Considerations
• Reasonably well tolerated – Not known to cause nausea
• Important side effect profile• Bleeding and bruising
– Should be considered “blood-thinning agent”– Hold 5–7 days prior to invasive procedure; restart
7 days after
• Known to cause some diarrhea– Typically can treat through; expect 1–2 bouts per day
for first week. Patients usually recover quickly
64

10/26/2015
33
Duration of Response
• Patients attain a complete remission
• How long will this last?
• Patients have been in remission for up to 3 years to date
65
Survivorship Issues
• Social workers and nursing: necessary to offer extensive emotional support
• During remission: often feel satisfied with response, but fearful of time because they wonder how long remission will last
• Secondly, ibrutinib is an expensive drug – Often need social work support to assist with financial
assistance– Often turn to The Leukemia & Lymphoma Society for
assistance with information gathering, as well as financial support
66
10/26/2015
34
67
Audience Discussion QuestionMany oncologists consider any patient diagnosed with cancer a survivor, what makes a CLL survivor
different? What special considerations are required in this population?
Case Study Discussions on the Nurse’s Role in Caring for Patients With Hematologic Malignancies
Multiple Myeloma Overview and Case Study
Beth Finley-Oliver, RN, BSNc, OCNPrimary Nurse
Moffitt Cancer Center
Tampa, FL
Case Study Discussions on the Nurse’s Role in Caring for Patients With Hematologic Malignancies
68This presentation was recorded in the studio following the ONS symposium

10/26/2015
35
Outline
• Understanding the Disease– Staging systems– Response criteria
• Case Study• Treatment Strategy
– Transplant vs non-transplant candidate• Treatment Options
– Newly diagnosed• Nursing Considerations for Myeloma Patients
– Bone health– Kidney health– Anemia– Preventing complications
• Multidisciplinary Team– Social worker– Physical and occupational therapist
• Financial assistance69
What Is Myeloma?
Cancer of plasma cells• An uncontrolled growth of plasma cells
Myeloma begins in the bone marrow• Spongy tissue found in the center of bones
Bone marrow
Marrow cells from apatient with myeloma
70

10/26/2015
36
“M-spike”– Monoclonal Paraproteins
Myeloma Cell- Produce Antibodies
Antibody- Heavy and light chain
components
Intact Ig Myeloma~80% MM
Eg, IgG kappa
Light Chain Myeloma
~15%–20% MMEg, kappa
Non-Secretory/Oligosecretory
~0.5%–5% MMEg, kappa
Heavy Chain- IgG >IgA >>IgD &
IgE >> IgM
Light Chain- Kappa (κ) > lambda (λ)
Ig, immunoglobulin; MM, multiple myeloma.71
Diagnosing Myeloma
72

10/26/2015
37
Diagnosis: “CRAB” Criteria
Presentation:• Hypercalcemia (C)• Renal Failure (R)• Anemia (A)
– Fatigue
• Fractures (B)– Bone pain
• Infections (I)
Durie BG, et al. Leukemia. 2006;20(9):1467–1473.73
Ca++
Lytic Lesions
74

10/26/2015
38
Durie-Salmon Staging System
Ig, immunoglobulin.
Durie BG, et al. Cancer. 1975;36(3):842–854.
Stage I
All of the following:Hemoglobin >10 g/dLSerum calcium normal (<12 mg/dL)Bone X-ray normal or solitary bone plasmacytoma onlyLow M-protein production (IgG <5 g/dL; IgA <3 g/dL)Bence-Jones protein <4 g/24 hours
One or more of the following:Hemoglobin <8.5 g/dLSerum calcium >12 mg/dLAdvanced lytic bone lesionsHigh M-protein production rates (IgG >7 g/dL; IgA >5 g/dL; Bence-Jones protein >12 g/24 hours)
Stage III
Fitting neither stage I nor IIIStage II
75
Durie-Salmon sub classifications (either A or B)A: Relatively normal renal function (serum creatinine value <2.0 mg/dL)B: Abnormal renal function (serum creatinine value =2.0 mg/dL)
Stage II
Factors: Beta-2 microglobulin <3.5 mg/LAlbumin <3.5 g/dL or
Beta-2 microglobulin ≥3.5–<5.5 mg/L
Stage III
Factors: Beta-2 microglobulin ≥5.5 mg/L
Better Response to Therapy
Stage I
Factors: Beta-2 microglobulin <3.5 mg/LAlbumin ≥3.5 g/dL
Lesser Response to Therapy
LessFavorable Prognosis
MostFavorable Prognosis
International Staging System (ISS)
Greipp PR, et al. J Clin Oncol. 2005;23(15):3412–3420. 76

10/26/2015
39
MM Risk Stratification
High Risk (25%) Standard or Good Risk (75%)
t(4;14) by FISH
t(14;16) or t(14;20) by FISH
Deletion 17q13 by FISH
Deletion 13 by metaphase analysis
Aneuploidy by metaphase analysis
Plasma cell labeling index >3.0
Beta-2 microglobulin >5.5
High-risk MyPRS™
Hyperdiploidy
t(11;14) by FISH
t(6;14) by FISH
Βeta-2 microglobulin <5.5
Labeling index <2.0
FISH, fluorescence in situ hybridization; MM, multiple myeloma; MyPRS, Myeloma Prognostic Risk Signature.77
TreatmentTreatment Plan
Patient
Preference Cytogenetics
Overall Health Status
AgeMyeloma
Stage
Factors Influencing Treatment Choice
78The Leukemia & Lymphoma Society. Myeloma: A Guide for Patients and their Families. March 2005.

10/26/2015
40
Response Criteria
Response Type M ProteinPlasma Cells in Bone Marrow Other
Stringent complete response (sCR) None (blood/urine) No abnormal
plasma cellsNo free light chains
Complete response (CR) None (blood/urine) <5% Disappearance of soft tissue plasmacytoma
Very good partial response (VGPR) >90% reduction (blood) NA NA
Partial response (PR)>50% reduction in serum and >90% reduction in urine
NA>50% reduction in the size of soft tissue plasmacytoma
Minimal response (MR)25%–49% reduction in blood and reduction of 50%–89% in urine
NA25%–49% reduction in the size of soft tissue plasmacytoma
Stable disease (SD) Does not meet criteria for response or progressive disease
Progressive disease (PD) >25% increase (blood or urine) >10%
New bone lesions, soft tissue plasmacytoma, high calcium levels
Durie BG, et al. Leukemia. 2006;20(9):1467–1473.79
Case Study
• 61-year-old male
• Presentation– SPEP: 3.6
– IgG: 6791
– Serum free light chain -Lambda: 89.56
– Beta-2 microglobulin: 2.3
– Albumin: 3.2 g/dL
– Calcium: 8.2 mg/dL
– Creatinine: 0.8 mg/dL
– Hemoglobin: 9.3 g/dL
– UPEP: 156 mg/24 hours
• BMBX 70%–80% plasma cells
• Survey + lytic lesions– Skull
– 8th rib fracture
– FISH results• Hyperdiploidy
• 13q deletion
• t(11;14)
– ISS II
– Durie-Salmon Stage 2A
BMBX, bone marrow biopsy; FISH, fluorescence in situ hybridization; Ig, immunoglobulin; SPEP, serum protein electrophoresis; UPEP, urine protein electrophoresis.
80

10/26/2015
41
Treatment Options for Transplant-Eligible Patient
• Transplant• Avoid melphalan
– RVD• Lenalidomide 25 mg,
days 1–14
• Bortezomib 1.3 mg/m2, days 1, 4, 8, and 11
• Dexamethasone 20 mg PO, days 1, 2, 4, 5, 8, 9, 11, and 12
– VDC• Bortezomib 1.3 mg/m2,
days 1, 4, 8, and 11
• Cyclophosphamide 500 mg PO, days 1, 8, and 15
• Dexamethasone 20 mg PO, days 1, 2, 4, 5, 8, 9, 11, and 12
Bisphosphonate Monthly
RVD, lenalidomide, bortezomib, and dexamethasone; VDC, bortezomib, dexamethasone, and cyclophosphamide.81
Response: VGPR
0
0.51
1.5
2
2.53
3.5
4
12/11
/201
2
01/11
/201
3
02/04
/201
3
02/22
/201
3
03/15
/201
3
04/05
/201
3
04/26
/201
3
Date
0
10002000
3000
4000
50006000
7000
8000
M protein
IgG
BMT evaluation:
PR, 2 more cycles
BMT, bone marrow transplant; Ig, immunoglobulin.82

10/26/2015
42
Disease Course
0
0.51
1.5
2
2.53
3.5
4
12/11
/201
2
01/11
/201
3
02/04
/201
3
02/22
/201
3
03/15
/201
3
04/05
/201
3
04/26
/201
3
05/13
/201
3
09/09
/201
3
02/20
/201
4
07/01
/201
4
01/06
/201
5
03/03
/201
5
Date
M s
pik
e (g
/dL
)
0
10002000
3000
4000
50006000
7000
8000
IgG
(m
g/d
L)
M protein
IgG
High-dose melphalan and autologous
transplant 6/5/2013
PD
Ig, immunoglobulin.83
Nursing Considerations
84
Case Study Discussions on the Nurse’s Role in Caring for Patients With Hematologic Malignancies

10/26/2015
43
Managing Side Effects
85
Case Study Discussions on the Nurse’s Role in Caring for Patients With Hematologic Malignancies
Immunomodulatory Drugs (IMiDs)
Thalidomide Lenalidomide Pomalidomide
Myelosuppression Minimal Yes Yes
VTE Yes Yes Yes
GI Constipation Diarrhea Diarrhea
Rash Yes Yes Yes
Sedation Yes No No
Neuropathy Yes No No
Teratogens!
GI, gastrointestinal; VTE, venous thromboembolism.86

10/26/2015
44
Proteasome Inhibitors
Bortezomib Carfilzomib
Schedule Days 1, 4, 8, and 11 every 21 days
Days 1, 2, 8, 9, 15, and 16 every 28 days
Modes of administration IV/SC IV
Myelosuppression/ thrombocytopenia
Yes Yes
Neuropathy Yes No
Zoster Yes Yes
Dyspnea No Yes
Fatigue Yes Yes
GI Yes No
Cardiac/pulmonary (RARE) No Yes
GI, gastrointestinal; IV, intravenous; SC, subcutaneous. 87
Steroids (Dexamethasone/Prednisone)
• Mood Swings
• Insomnia
• Irritability
• Hyperactivity
• Edema
• Flushing
• Fatigue
• Blurry vision
• Cataracts
• Dyspepsia– PPI
• Muscle atrophy
• Hyperglycemia
• Acne
• Muscle cramping
• Taste changes
• Ulcer
• Weight gain
• Hair loss
PPI, proton pump inhibitor.
Faiman B, et al. Clin J Oncol Nurs. 2008;12(3):53–62.88

10/26/2015
45
Nurse’s Role
• Education and support– Oral adherence to complex regimens
• Improving quality of life by helping to manage side effects
• Navigating patients and their caregivers throughout the disease process
89
Bone Health
• Bisphosphonates– Avoid invasive dental procedures
– Prevent pathological fractures• Orthopedist
• Neurosurgeon
• Pain control– Avoid NSAIDs
– Narcotic education
NSAID, non-steroidal anti-inflammatory drugs.
Miceli TS, et al. Clin J Oncol Nurs. 2011;15(4):9–23.90

10/26/2015
46
Renal Health
• Cast nephropathy (myeloma kidney)• Hypercalcemia
– Aggressive hydration and treatment• Dehydration
– IV fluids• NSAIDS• IV contrast• Aminoglycoside antibiotics
– Gentamycin, tobramycin, etc.• Bisphosphonates
IV, intravenous; NSAID, non-steroidal anti-inflammatory drugs.
Faiman B, et al. Clin J Oncol Nurs. 2011;15(4):66–76.91
Anemia
• Due to disease or treatment
• Supportive care
– Erythropoietin-stimulating agents
• Epoetin alfa
• Darbepoetin alfa
– PRBC transfusions
– Fatigue • Treatment
• Disease
• Physical therapyPRBC, packed red blood cell.
92

10/26/2015
47
Safety and Mobility
• Exercise– Physical/Occupational therapy
• Nutrition and hydration– Consult from nutritionist
• Psychosocial well-being– Support system– Fatigue– Sleep disturbances– Anxiety– Depression
Rome SI, et al. Clin J Oncol Nurs. 2011;15(suppl):41–52.93
Multidisciplinary Team Approach
• Social workers– Financial assistance programs
• Non-profit organizations– The Leukemia & Lymphoma Society– Chronic Disease Fund– Patient Network Access
• Pharmaceutical companies• Physical and occupational therapists• Dietician• Pharmacist• Dentist
94

10/26/2015
48
Summary
• Multiple myeloma is most often a chronic and complex disease
• Treatment decisions are individualized to the patient
• Managing side effects helps patients maintain quality of life
• A multidisciplinary team approach helps support patients and caregivers
95
Thank You
96
Case Study Discussions on the Nurse’s Role in Caring for Patients With Hematologic Malignancies

10/26/2015
49
Follicular Lymphoma Overview and Case Study
Lynn Rich, ANP-BC, OCNNurse Practitioner
JP Wilmot Cancer InstituteUniversity of Rochester
Rochester, NY
Case Study Discussions on the Nurse’s Role in Caring for Patients With Hematologic Malignancies
97This presentation was recorded in the studio following the ONS symposium
Outline
• Define disease• Epidemiology• Natural history of disease
– Indolent vs curable• Approved treatment options
– Rituxan maintenance vs observation• Use of idelalisib • Communication strategies: support of social
workers• Resources: survivorship challenges
98

10/26/2015
50
Lymphoma
General name given to a group of cancers that affect the lymphatic system• Includes:
– Lymph nodes – Plasma cells– Spleen– Lymphatic vessels– Bone marrow – Immunoglobulins
• Immune system helps protect against disease and infection
The Leukemia & Lymphoma Society. Non-Hodgkin Lymphoma. 2013.
Spleen
Lymphnodes
Bone Marrow
99
Lymphoma
Two distinct types: • Non-Hodgkin lymphoma (NHL)
– Approx. 50 different subtypes• Hodgkin lymphoma (HL)
– Approx. 5 different subtypes
100

10/26/2015
51
Follicular Lymphoma (FL)
• B-cell NHL (vs T/NK-cell NHL)
• Damage to DNA of one of the parent B cells causes a malignant transformation resulting in uncontrolled and exaggerated growth of the lymphocyte
101Image courtesy of JP Wilmot Cancer Institute; Chronic Lymphocytic Leukemia (CLL) Booklet.
Follicular Lymphoma (FL)
• 2nd most common subtype of NHL• Average age at diagnosis is 60 years• Indolent: slow-growing disease• Treatable, but not curable
– Impact of deciding treatment
The Leukemia & Lymphoma Society. Non-Hodgkin Lymphoma. 2013. 102

10/26/2015
52
NHL: Epidemiology
DLBCL
FL
T cell
Other B cell
Approximately 70,800 new cases of NHL in 2014
DLBCL, diffuse large B-cell lymphoma.The Leukemia & Lymphoma Society. Non-Hodgkin Lymphoma. 2013.
103
Case Study: MB
• 57-year-old married female– 3rd-grade elementary teacher – Symptom profile
• Abdominal fullness• Sweats• Fatigue• Lymphadenopathy
– Next step, stage?
104

10/26/2015
53
Ann Arbor Staging System
The Leukemia & Lymphoma Society. Non-Hodgkin Lymphoma. 2013.105
Case Study: MB
• Stage III– Bilateral axillary – small
– Abdominal – 10-cm mass
– Small inguinal node (groin node)
– Bone marrow negative (would have been stage IV)
106

10/26/2015
54
Treatment
• Watch and wait?
• Grade 1, 2, or 3?
107
Ready to Treat
• Criteria includes: – >3 sites of disease, 3 cm or
more
– 1 node measuring 7 cm
– Cytopenias – refractory thrombocytopenia disease
– Effusions
– Symptoms of disease, or B symptoms
– Threatened organ involvement
– Elevated LDH
LDH, lactate dehydrogenase.108

10/26/2015
55
Case Study: MB
• Treated with R-CHOP – completed 2007– Attained complete remission
• Consider maintenance with rituximab vs observation– Upfront vs consolidation– Things to consider:
• Expected response• Impact on overall survival• Quality of life• Financial impact
R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.109
Case Study: MB
• No maintenance rituximab
• Relapsed in 5/2008– Concerning?
• What we did: – Salvage RICE×2, then autologous
stem cell transplant
– Complete remission 9/2008
RICE, rituximab, ifosfamide, carboplatin, and etoposide.110

10/26/2015
56
Case Study: MB
• Relapsed 12/2014 – Essentially asymptomatic – mild abdominal
fullness
– However, CT of abdomen showed increased disease
• Is she ready for treatment?– What are the treatment options?
CT, computed tomography.111
Idelalisib – What Is It?
• PI3K inhibitor– Phosphoinositide 3-kinase delta
112

10/26/2015
57
Idelalisib
• Oral agent
• FDA approved in 2014
• Used for CLL/SLL or FL
• In relapsed setting
CLL/SLL, chronic lymphocytic leukemia/small lymphocytic lymphoma.113
Side Effect Profile
• Concern for pneumonitis or colitis– What to look for– When concerned– How to follow
• Concern for evolution of liver function abnormalities – What to look for – When concerned– How to follow
114

10/26/2015
58
Things to Consider
• Is this patient a good candidate?– Why wouldn’t she be?– Why would she be?
• Bring in social worker– Help to assess medical literacy (implications)– Help with financial assistance
• What are potential sources of assistance?
115
Communication Strategies
• Create a calendar with details– When to take pills, get blood drawn, etc.
• Dialogue with patient – Check in by phone
• At least weekly initially
• Consider MyChart®
• Eventually evolve to monthly visits, if tolerated
116

10/26/2015
59
What Happened to MB?
• Began idelalisib 150 mg BID
• Well tolerated
• Held after 2 months for elevated LFTs
• Update to date…
BID, twice daily; LFTs, liver function tests.117
Resources – Survivorship Issues
• The Leukemia & Lymphoma Society– www.LLS.org– Explore local chapter
support groups • YMCA – Exercise program
– Explain cancer survivor – Describe health and fitness
programs • Look for specific related survivor support groups
– www.LLS.org/survivorship
118

10/26/2015
60
Thank You
Case Study Discussions on the Nurse’s Role in Caring for Patients With Hematologic Malignancies
119