case study for hospital
DESCRIPTION
study guide and reference to my designTRANSCRIPT

The Practice of Integrated Design:
The Case Study of
Khoo Teck Puat Hospital, Singapore
Tan Shao Yen
31st January 2012
A dissertation submitted in partial fulfillment of the regulations for the Degree of
Masters of Science in Sustainable Building Design in
BCA Academy - University of Nottingham, 2012.


1
Acknowledgements
I would like to thank my supervisor, Dr Peter Rutherford, for the inspiration,
recommendation and continuous personal guidance. The gratitude is also extended to
all the lecturers and tutors from Department of Architecture and Built Environment, for
their dedication despite the geographical, temporal and scheduling challenges between
the United Kingdom and Singapore.
Special thanks go to the BCA Academy and their staff who made the course possible in
the first place. Immense efforts had been put in by them into the logistics and
coordination that had gone into balancing the needs of the academic programme and
the part-time working students, given their diverse background and career demands.
Sincere thanks to the exemplary Khoo Teck Puat Hospital, especially Mr Donald Wai
Wing Tai, for granting visits to and information regarding the Hospital, allowing
invaluable insights into the subject matter discussed in this dissertation.
I am indebted to my company, CPG Consultants Pte Ltd, for the support I have received
from and the inconveniences my colleagues have put up with, in order for me to pursue
the course. Special thanks to Mr Pang Toh Kang, Mr Khew Sin Khoon, Mr Lye Kuan
Loy, Mr Kok King Min for their understanding and support. I would like also to thank
Dr Lee Siew Eang, Mr Glenn Bontigao, Mr Lee Soo Khoong, Mr Lim Lip Chuan, Mr
Jerry Ong, Ms Pauline Tan, Mr Toh Yong Hua, Mr Ng Kim Leong, Mr Soon Chern Yee,
Ms Wong Lee Phing, Mr Yeo Tiong Yeow, Dr Nirmal Kishnani, and Mr Sng Poh Liang
for sharing insights, experience and information regarding the Khoo Teck Puat Hospital
project.
Words cannot express the love, support and sacrifice I have received from my family,
without which it is hard to imagine how I would be able to juggle work, study and
family; a big thank you to you all.

2
Abstract
Contemporary challenges have necessitated the application of sustainable principles and
practices to the building construction industry. In order to do so, integrated design
processes and practices have come to the fore as an important aspect in the delivery of
sustainable buildings. In recent years, sustainable building projects that purport to be
based on integrated design have emerged and appear to be gathering momentum in
different parts of the world, including Singapore. Such an integrated approach is backed
extensively in the literature, and as such numerous questions have been raised with
respect to integrated design in practice. These include what is a sustainable design brief;
how do the various stakeholders play out their roles in the integrated design process;
what are the challenges and mindset changes required by the stakeholders in a building
project to ensure the successful realization of integrated design?
Completed in 2010, the Khoo Teck Puat Hospital in Singapore provided an interesting
case study to study the integrated design process in action. As stated in its design brief, it
aims to be a healthcare building for the future through, first, achieving a “visually
pleasing design that sustain with time” (Alexandra Hospital, 20051); and second, the
“ease and low cost of maintainability resulting from careful overall design and material
selection.” (Ibid.) The outcome of the design necessitated close collaboration between its
many stakeholders through an integrated manner. The aim of this dissertation is
therefore to first, examine how the design of Khoo Teck Puat Hospital has embraced
certain principles of sustainability; second, how elements of the integrated design
process have successfully contributed to such design outcomes, as well as practical
challenges faced in the integrated design process. This dissertation concludes by making
recommendations that aim to overcome the practical challenges, thereby facilitating the
integrated design process, and hence improving the quality of sustainable building
design.
Keywords: Sustainable building design, Integrated design, Sustainable Healthcare Architecture.
1 Tender briefing materials by Alexandra Hospital, the forerunner of Khoo Teck Puat Hospital.

3
Declaration
I understand the nature of plagiarism and I am aware of the University’s policy on this. I
certify that this dissertation reports original work by me and that all the sources I have
used or quoted have been indicated by means of completed references.
31 January 2012
Signature Date

4
Table of Contents
Acknowledgements ..................................................................................................................................... 1
Abstract .......................................................................................................................................................... 2
Declaration .................................................................................................................................................... 3
Table of Contents .......................................................................................................................................... 4
List of Tables ................................................................................................................................................. 9
List of Figures ............................................................................................................................................. 10
Chapter 1.0: Introduction ......................................................................................................................... 13
1.1 Background and Context of Healthcare Architecture ......................................................... 14
1.2 Scope and Objectives ................................................................................................................ 16
1.3 Research Questions ................................................................................................................... 17
1.4 Dissertation Structure............................................................................................................... 17
1.5 The Key Challenges of Healthcare Architecture in Singapore ........................................... 19
1.5.1 Challenges Related to the Provision of Medical Services .................................................... 19
1.5.2 Challenges Related to Healthcare Organization, Structure and Culture ........................... 20
1.6 Sustainable Healthcare Architecture in Singapore’s Context ............................................. 21
1.6.1 Economic Sustainability ........................................................................................................... 22
1.6.2 Social Sustainability .................................................................................................................. 24
1.6.2.1 The Relationship between Human Wellness and Environment ........................................ 24
1.6.2.2 Sustaining Community through Healthy Public Place ....................................................... 26
1.6.3 Environmental Sustainability .................................................................................................. 26
1.6.4 Defining Sustainable Healthcare Architecture ..................................................................... 30
1.7 Discussion: The Need to Integrate Inter-Disciplinary Knowledge .................................... 31
Chapter 2.0: The Integrated Design Approach...................................................................................... 33
2.1 The Definition of Integrated Design Approach .................................................................... 34

5
2.2 Benefits of the Integrated Design Approach in Healthcare Architecture ......................... 35
2.2.1 Increasing Scale & Complexity ............................................................................................... 36
2.2.2 Failure of Traditional Siloed and Linear Design Process .................................................... 36
2.2.3 The Integrated Design Process ................................................................................................ 37
2.2.4 Achieving Sustainable Healthcare Architecture ................................................................... 38
2.2.5 Learning Organization ............................................................................................................. 39
2.3 Essential Elements of the Integrated Design Approach for Healthcare Architecture ..... 39
2.3.1 The Multi-Disciplinary Project Team ..................................................................................... 40
2.3.2 Mind Set Change: The Need for a Whole-System Mental Model ...................................... 42
2.3.3 Integrated Design Process ....................................................................................................... 44
2.3.3.1 Team Formation and Organization ........................................................................................ 46
2.3.3.2 Visioning .................................................................................................................................... 49
2.3.3.3 Objectives Setting ...................................................................................................................... 49
2.3.3.4 Design Iteration ......................................................................................................................... 50
2.3.3.5 Construction & Commissioning ............................................................................................. 53
2.3.3.6 Post Occupancy Feedback Loops ........................................................................................... 54
2.3.3.7 Comparison Between IDP and Linear Design Process ........................................................ 54
2.3.4 Tools and Techniques that Support Integrated Design ....................................................... 55
2.3.4.1 Integrated Design Tools ........................................................................................................... 55
2.3.4.2 Integrated Design Techniques ................................................................................................ 59
2.3.5 Integrated Design Products: Sustainable Healthcare Architecture .................................... 60
2.4 Discussion: The Aspects of Integrated Design Process to be Investigated ....................... 62
Chapter 3.0: Khoo Teck Puat Hospotal: The Case Study ..................................................................... 63
3.1 Background ................................................................................................................................ 64
3.2 KTPH’s Site Context ................................................................................................................. 64
3.3 KTPH Visioning, Objective Setting and Briefing Process ................................................... 68
3.3.1 Methodologies: Focused Group Discussions and References ............................................ 68

6
3.3.2 The Shared Visions ................................................................................................................... 69
3.3.2 Setting the Objectives ............................................................................................................... 71
3.4 KTPH Team Formation and Organization ............................................................................ 75
3.4.1 The role of IDP Facilitator ........................................................................................................ 76
3.4.2 The role of the Architect + IDP Facilitator for Building Design ......................................... 77
3.4.3 The role of the Hospital Planning Team + IDP Facilitator for User Groups ..................... 78
3.4.4 The role of the Prime Consultant Team ................................................................................. 79
3.4.5 The role of the Green Consultant ............................................................................................ 80
3.4.6 The role of User Groups ........................................................................................................... 80
3.4.7 The role of the Contractor ........................................................................................................ 81
3.5 Discussion: KTPH’s Visioning, Objective Setting and Team Formation ........................... 81
Chapter 4.0: KTPH’s Integrated Design Process ................................................................................... 83
4.1 The Process Map ....................................................................................................................... 84
4.1.1 DC: Design Competition (Prelim) .......................................................................................... 85
4.1.2 W1: Visioning Workshop ......................................................................................................... 87
4.1.3 W2: Masterplanning Workshop .............................................................................................. 87
4.1.4 MP: Schematic Design Research/Analysis/Design Process ................................................. 87
4.1.5 SD: Schematic Design ............................................................................................................... 88
4.1.6 VE1: Value Engineering Workshop ........................................................................................ 88
4.1.7 DD1 & DD2: Design Development ......................................................................................... 89
4.1.8 VE2: Value Engineering Workshop ........................................................................................ 90
4.1.9 The Practice of Workshop/Design Charrette ........................................................................ 90
4.1.10 Hospital Planning Committee Meetings that were held monthly ..................................... 91
4.2 The Iterative Process ................................................................................................................. 92
4.2.1 Schematic Design (SD) Stage ................................................................................................... 93
4.2.2 The Design Development (DD1) Stage .................................................................................. 99
4.2.3 The Component Design (DD2) Stage ................................................................................... 107

7
4.2.3.1 Wind Wall at the Naturally Ventilated Subsized Ward Tower ........................................ 108
4.2.3.2 Detailed Deisgn of Spot Cooling at Roof Terraces: New Air ............................................ 110
4.2.3.3 Water Efficient Landscaping Irrigation System .................................................................. 114
4.2.3.4 Resource-Efficient M&E System Design .............................................................................. 115
4.3 Discussion: KTPH’s Integrated Design and Iterative Process .......................................... 116
Chapter 5.0: Conclusion ......................................................................................................................... 118
5.1 KTPH: Sustainable Healthcare Architecture in Singapore................................................ 119
5.1.1 KTPH as a Green Building .................................................................................................... 119
5.1.2 KTPH: Embracing Social Sustainability ............................................................................... 121
5.1.3 KTPH: Embracing Environmental Sustainability ............................................................... 121
5.1.4 KTPH: Mapping the Attributes of Sustainable Healthcare Architecture and Integrated
Design Approach .................................................................................................................... 122
5.2 Lessons Learnt on the Practice of Integrated Design from the KTPH Case Study ........ 124
5.2.1 The KTPH Briefing Process ................................................................................................... 124
5.2.2 Entrenched Practice among Building Professionals .......................................................... 125
5.2.3 Issues Related to Mindset Change ........................................................................................ 126
5.2.4 Lack of Integrated Design Process Toolkit .......................................................................... 126
5.2.5 Fragmentary Design and Documentation Platform ........................................................... 126
5.2.6 Issues Related to Contractor Appointed via Conventional Approach ............................ 127
5.3 Discussion: the Practice of Integrated Design ..................................................................... 127
5.4 Recommendations .................................................................................................................. 129
Appendix I: Roles of Team Members By Design Phases .................................................................... 131
Appendix II: Iterative Process in Integrated Design ........................................................................... 136
Appendix III: Building Information Modelling ................................................................................... 157
Appendix IV: Design Consortium of the KTPH Project ..................................................................... 164
Appendix V: Interview Guide ................................................................................................................ 166

8
Appendix VI: Evidence-Based Design Principles ................................................................................ 173
Appendix VII: Energy-Efficient Active Design Measures .................................................................. 180
Appendix VIII: Water-Efficient Considerations ................................................................................... 183
Appendix IX: Indoor Environmental Quality ...................................................................................... 185
Appendix X: Renewable Energy Systems & Other Innovation Measures ........................................ 188
Appendix XI: Integrated Design during Construction Phase ............................................................ 192
Appendix XII: KTPH’s BCA Green Mark Performance ...................................................................... 195
Appendix XIII: Thermal Comfort Outcome of KTPH’s Bioclimatic and Natural Ventilation
Strategies ................................................................................................................................................... 199
Appendix XIV: Evaluating Human Wellness and Social Sustainability of KTPH .......................... 204
Appendix XV: KTPH’s Environmental Stewardship .......................................................................... 209
Bibliography .............................................................................................................................................. 217
Word Count: 19,023
9
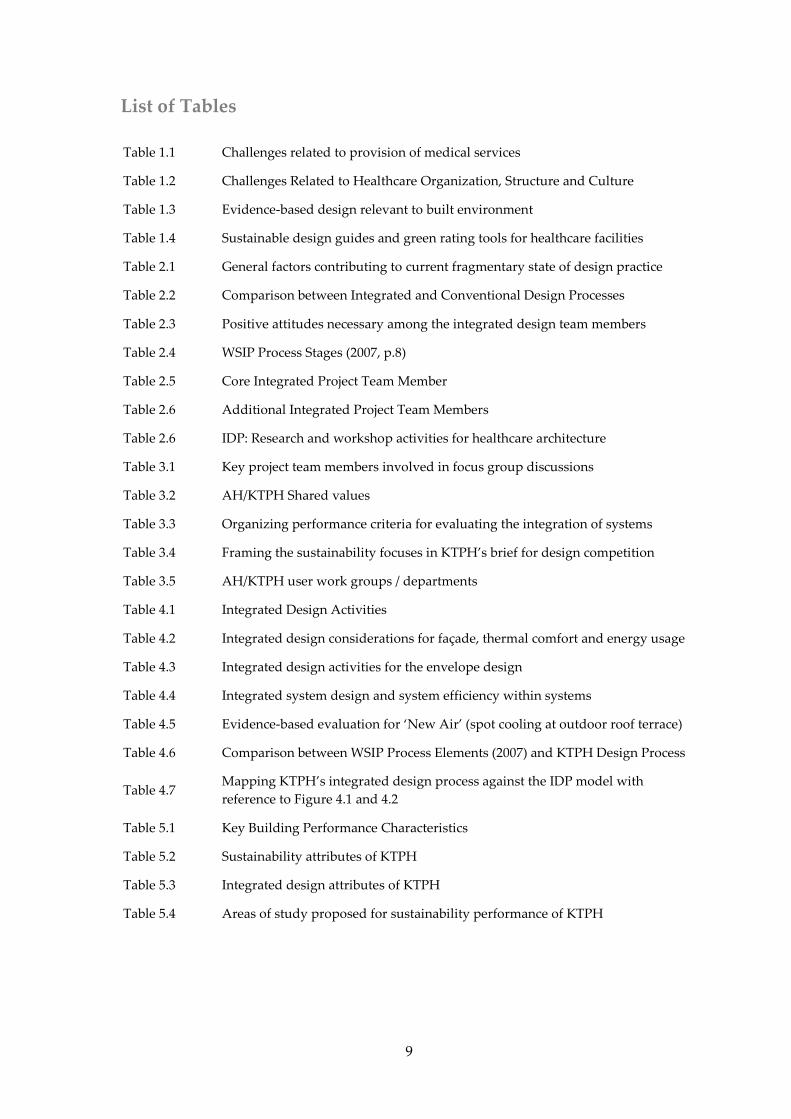
List of Tables
Table 1.1 Challenges related to provision of medical services
Table 1.2 Challenges Related to Healthcare Organization, Structure and Culture
Table 1.3 Evidence-based design relevant to built environment
Table 1.4 Sustainable design guides and green rating tools for healthcare facilities
Table 2.1 General factors contributing to current fragmentary state of design practice
Table 2.2 Comparison between Integrated and Conventional Design Processes
Table 2.3 Positive attitudes necessary among the integrated design team members
Table 2.4 WSIP Process Stages (2007, p.8)
Table 2.5 Core Integrated Project Team Member
Table 2.6 Additional Integrated Project Team Members
Table 2.6 IDP: Research and workshop activities for healthcare architecture
Table 3.1 Key project team members involved in focus group discussions
Table 3.2 AH/KTPH Shared values
Table 3.3 Organizing performance criteria for evaluating the integration of systems
Table 3.4 Framing the sustainability focuses in KTPH’s brief for design competition
Table 3.5 AH/KTPH user work groups / departments
Table 4.1 Integrated Design Activities
Table 4.2 Integrated design considerations for façade, thermal comfort and energy usage
Table 4.3 Integrated design activities for the envelope design
Table 4.4 Integrated system design and system efficiency within systems
Table 4.5 Evidence-based evaluation for ‘New Air’ (spot cooling at outdoor roof terrace)
Table 4.6 Comparison between WSIP Process Elements (2007) and KTPH Design Process
Table 4.7 Mapping KTPH’s integrated design process against the IDP model with
reference to Figure 4.1 and 4.2
Table 5.1 Key Building Performance Characteristics
Table 5.2 Sustainability attributes of KTPH
Table 5.3 Integrated design attributes of KTPH
Table 5.4 Areas of study proposed for sustainability performance of KTPH

10
List of Figures
Figure 1.1 The complex relationships between the hospital functions
Figure 1.2 The typical compartmentalized, episodic model of care
Figure 1.3 Khoo Teck Puat Hospital’s holistic ‘Head-To-Toe Lifelong Anticipatory
Healthcare of Whole Person’ model
Figure 1.4 Comparisons of some green rating systems for sustainable buildings
Figure 1.5 Trajectory of environmentally responsive design
Figure 1.6 Model of sustainable healthcare architecture
Figure 2.1 Multi-disciplinary project team for healthcare project
Figure 2.2 Bryan Lawson’s model of design problems or constraints
Figure 2.3 The new mental model for integrative design
Figure 2.4 Zeisel’s user-needs gap model
Figure 2.5 Conventional design team organization
Figure 2.6 Integrated design Team organization
Figure 2.7 Triple Bottom Line approach goal setting for a project visioning session
Figure 2.8 Integrative design process
Figure 2.9 Iterative process as proposed in ‘Strategies for integrative building design
Figure 2.10 ‘Iteration loops’ as proposed in ‘Strategies for integrative building design
Figure 2.11 Integrative design process versus linear design process
Figure 2.12 The integrated design model
Figure 2.13 The traditional team model and an integrated design team model in information
exchange
Figure 2.14 Achieving sustainable healthcare architecture through integrated design
Figure 3.1 KTPH layout with reference to its site context
Figure 3.2 Garden in a Hospital: Courtyard view of Khoo Teck Puat Hospital with
naturalistic, lush greenery
Figure 3.3 Hospital in a Garden: View of Khoo Teck Puat Hospital across Yishun Pond
Figure 3.4 Integration of healthcare, social, and natural environments
Figure 3.5 KTPH’s integrated design team organization
Figure 4.1 Integrated design process in KTPH

11
List of Figures (Cont’d)
Figure 4.2 The theoretical model of integrative design process
Figure 4.3 Integrated design team organization at the design competition stage
Figure 4.4 KTPH iterative process basing on the model in ‘Strategies for integrative
building design
Figure 4.5 Iterative process model during the schematic design phase
Figure 4.6 Landscape plan showing landscaped courtyard as the heart and lung of design
Figure 4.7 Landscape schematic drawing
Figure 4.8 Sketch design for landscaped roof terrace as social space, while providing good
shading and insulation to interior spaces below
Figure 4.9
Landscaped oof terrace at Level 4 where patients, visitors, staff may enjoy
moments of solitude or share moments of comfort or grieve; it is also a source of
visual relief from the wards
Figure 4.10 Landscaped roof terrace at Level 5 overlooking Level 4
Figure 4.11 Iterative process model during the schematic design phase
Figure 4.12 Bioclimatic response of KTPH: sunpath
Figure 4.13 Bioclimatic response of KTPH: prevalent wind directions
Figure 4.14 Aspect ratio of the various block
Figure 4.15 Critical review based on ‘Environmental Design Guide for Naturally Ventilated
and Daylit Offices’
Figure 4.16 Design study 1 for façade shading of the naturally ventilated ward tower
Figure 4.17 Design study 2 for façade shading of the naturally ventilated ward tower
Figure 4.18 Design study 3 for façade shading of the naturally ventilated ward tower
Figure 4.19 Design developed from Option 3: Fully height louvred façade and light shelf
maximizes natural ventilation and daylight
Figure 4.20
Design developed from Option 3: Effect of rain needs to be considered in the
tropics. These diagrammes indicate integration of monsoon windows providing
ventilation during rain, even when the louvred windows are closed
Figure 4.21
Interior of naturally ventilated ward: Façade system comprising louvred wall,
light shelves, and monsoon window. Natural ventilation is supplemented with
individually controlled fans
Figure 4.22 Iterative process model during the late design development (DD2) phase
Figure 4.23 Sampling points measured in wind tunnel study

12
List of Figures (Cont’d)
Figure 4.24 A sample of the air velocity profile across a typical ward at 1.2m height @ open,
50% open and closed conditions
Figure 4.25 A sample of the pressure coefficients chart across the façade of the subsidised
ward tower obtained as boundary conditions for the CFD study
Figure 4.26 1:20 Wind tunnel model used for the study
Figure 4.27
Subsidized ward tower façade showing solar screen to provide shade and wind
wall to induce air movement. Greenery is also integrated into the façade to
enhance visual relief
Figure 4.28 Design drawing showing location of exhaust nozzle integrated into the façade,
and the direction of throw to cool the landscaped roof terraces
Figure 4.29 CFD Simulation showing approximately 2°C reduction in temperature at the
roof terrace, delivering cooling sensation to users
Figure 4.30 CFD simulation showing the throw of exhaust nozzle, and the wind speed
gradient. A 2m/s wind speed is achieved at the end of the throw
Figure 4.31
Noise level (dBA) at various distances (m) from the nozzle diffuser. The noise
level at landscaped roof terrace at 5m away from nozzle diffuser is 43dBA,
which is equivalent to outdoor ambient sound level
Figure 4.32
Selection of component: Oscillating nozzle diffusers tested to ISO 5135 1997 and
ISO 3741 1999 on sound power level performance to allow for better throw
distribution
Figure 4.33 Conceptual diagramme of irrigation system and built environment as part of
natural systems
Figure 4.34 Schematic of irrigation system, drawing water from Yishun
Figure 5.1 KTPH: Post Occupancy Studies
Figure 5.2 KTPH: Sustainable Attributes mapped onto the Sustainable Healthcare
Architecture Model
Figure 5.3 KTPH Integrated design process: questions framed with the IDP Mental Model

13
Chapter 1.0: Introduction
“Some people prefer to think of health as the
absence of disease, while others insist that
health is a state of physical, mental, and
social well being.”
Ted Schettler
“With twenty-first-century businesses
increasing emphasis on triple-bottom-line
imperatives – not only for competitive
advantage but also for planetary survival –
healthcare’s singular blend of
environmental, economic and social agendas
is a model worthy of replication by other
sectors.”
Robin Guenther and Gail Vittori

14
Chapter 1.0 Introduction
1.1 Background and Context of Healthcare Architecture
Healthcare architecture consists of a wide range of building types, ranging from small
neighbourhood clinics to large hospital complexes; from the general hospitals providing
a comprehensive range of medical services to the specialized hospitals that focus on a
selected field of medical services and/or research. Large-scale hospitals are arguably one
of the most complex building types, having to accommodate a wide range of functions
and services, for example, outpatient facilities, diagnostic and treatment facilities,
accident and emergency facilities, operating theatres, clinical laboratories, radiography
and imaging facilities, administration, food services and housekeeping, etc. The diverse
range of functions and specialized needs require the support of sophisticated and
advanced systems, for example, life support, telecommunication, space comfort and
hygiene, as well as building services that have to be robustly designed (Carr, 2011).
The complex physical functions of large healthcare facilities are to be considered in
relation to the network of stakeholders that are involved with large scale hospitals,
Figure 1.1 The complex relationships between the hospital functions. Source: Carr, R. F. ‘Hospital’ in
Whole Building Design Guide. Internet WWW: http://www.wbdg.org/design/hospital.php

15
including patients, doctors, nursing staff, administration staff, servicing staff, visitors,
social and volunteer workers, maintenance crew, suppliers, etc. Conflicting demands
arising out of the myriad of needs and requirements are only to be expected. Good
healthcare design not only seeks to resolve these conflicts, but provide an integrated
solution that addresses the following (Ibid.):
1. Efficient operation and cost effectiveness
2. Flexibility and expandability
3. Therapeutic environments
4. Cleanliness and sanitation
5. Accessibility
6. Controlled circulation
7. Aesthetic
8. Security and safety
9. Sustainability
Large-scale healthcare facilities also consume significant resources. To begin with, they
are costly to build; hence significant financial resources are committed to building them,
be it funded by the taxpayer, by private means or both, such as via public-private
partnership (PPP) or private finance initiative (PFI). After they are built, not only are
healthcare buildings significant consumers of energy2 and water, they are also producers
of significant quantities of clinical waste, on a round-the-clock, day-to-day basis. The
ultimate goals of healthcare facilities, however, must surely be in meeting social
objectives and human wellness; not only for patients who seek treatment, but also the
community working in the healthcare built environments (Carr, 2011, 2011; Ray, D,
Betterbricks, Mason, 2006). With the rising global demand for both good quality and
affordable healthcare (World Health Report, 2008), a compelling case must surely be put
forth for all healthcare buildings to be designed and operated in a sustainable manner –
economically, environmentally, and socially (Ibid.).
2 The US Commercial Building Energy Consumption Survey conducted in 2003 found that
hospital used an average of 250,000 BTU/ft2 (approximately 788.6kW/m2), second only to food
service buildings (Singer, B. C., 2009).

16
1.2 Scope and Objectives
Through a case study of a hospital project in Singapore that was completed in 2010, this
dissertation examines how the integrated design approach had, in practice, contributed
to social and environmental sustainability in healthcare architecture. This is done by first
studying and understanding the issues related to sustainable healthcare architecture, and
how integrated design can play an important role in realizing sustainable healthcare
architecture, given that it necessitates the involvement of a network of stakeholders with
specialized knowledge. Second, the dissertation shall study the integrated design
approach in theory, so as to identify the key elements relevant for healthcare
architecture. Next, the findings shall be compared with what had taken place in practice
through examining the case study of a recently completed hospital in Singapore, namely
the Khoo Teck Puat Hospital (KTPH). Based on the comparative analysis and lessons
learnt, this dissertation concludes with recommendations on how the practice of
integrated design may be further researched and improved.
The objectives of this dissertation are hence as follows:
1. Explore some recent developments and understanding of sustainable healthcare
architecture, and its relationship with integrated design.
2. Identify, as far as possible, the essential elements that comprise the integrated
design approach in the context of healthcare architecture, by drawing upon and
making comparison from literature references.
3. Through documentation study of the KTPH project and interviews with its
project team members, understand how the visioning and briefing process;
formation and organization of integrated project team; the integrated design
process and the design iterations of KTPH took place, to critically appraise the
integrated design process in practice.
4. Analyze comprehensively the extent of integrated design process played out in
the KTPH project, the lessons learnt by its team members, and how such lessons
could contribute to future application of integrated design process in practice.

17
1.3 Research Questions
Through these objectives, this research will investigate the benefits associated with the
integrated design process in realizing sustainable healthcare architecture. In so doing,
four main research questions are posed, namely:
1. How do we define sustainable healthcare architecture in the Singapore context?
2. What are the salient elements of the integrated design approach and how are they
relevant for sustainable healthcare architecture?
3. How is integrated design carried out in the practice of healthcare architectural
design?
4. What are the lessons learnt in the integrated design process in the practice of
healthcare architecture?
5. How can the lessons learnt benefit future practice of integrated design in
healthcare architecture?
6. The research methodology includes literature review based on publicly accessible
information, access to document archived within the organizations involved in
the KTPH project, and interview with design/project team members involved in
KTPH project. Materials used in this dissertation are limited to information that
had been permitted for publication by the sources of the information.
1.4 Dissertation Structure
To address these aims, objectives and research questions, the dissertation is structured as
six interrelated chapters.
Chapter 1: Introduction
This introductory chapter presents the background and context of healthcare
architecture; the scope and objectives of the thesis, research questions and a brief
description of each chapter. To initiate the discussion, it presents the challenges
associated with the design of healthcare architecture, as well as recent developments and
opportunities in realizing sustainable healthcare architecture.

18
Chapter 2: The Integrated Design Approach
Having established the importance and necessity of sustainable healthcare architecture
in Chapter 1, Chapter 2 focuses on how sustainable architecture may be realized through
the integrated design process. By drawing from various sources, the essential elements of
the integrated design process are discussed, in particular:
1. Who are the key stakeholders and why a multi-disciplinary team is needed;
2. The necessary mindset change required for them to be effective in the integrated
design process;
3. The visioning and objective setting process and the sustainable design brief;
4. The integrated design process including team-based iterative processes.
Chapter 3: Khoo Teck Puat Hospotal - A Case Study
This chapter builds upon the work introduced in previous chapters and as such explores
them within the context of the Khoo Teck Puat Hospital (KTPH), a purported sustainable
healthcare architecture in Singapore (Guenther and Vittori, 2008, p.p. 172-174),
completed in 2010. As such, Chapter 3 will first provide the background of the KTPH
project, followed by examining how through project visioning, objectives setting, team
formation and organization, the KTPH project had aligned team members’ mindsets,
attitude and commitment with a common purpose and shared values. This is done
through a comprehensive study of the literature and project document, as well as
through interviews with the key project team members involved.
Chapter 4: KTPH’s Integrated Design Process
This chapter continues from the previous chapter with the examination of the KTPH
design process by mapping it against a theoretical model of integrated design process. It
is followed by an examination of the team-based iterative processes through the various
design stages, in the process exploring the contribution from different project team
members, including the client representatives, users, various building professionals, etc;
the integrated design techniques such as small group research and all stakeholders’

19
workshops; integrated design tools such as computer building performance simulation
and green rating tools, as well as the challenges encountered in the collaboration process.
Chapter 5: Conclusion
In this chapter, the outcome of the integrated design process, i.e. KTPH as an example of
sustainable healthcare architecture is presented, hence completing the evaluation of the
relationship between integrated design and its outcome. In so doing, it validates the
relevance and importance of the integrated design approach to healthcare architecture. It
is followed by a discussion of the lessons learnt in the practice of integrated design. By
drawing on the lessons learnt, the chapter concludes by providing some
recommendations on further research areas that will contribute towards improving the
theory and practice of integrated design approach.
1.5 The Key Challenges of Healthcare Architecture in Singapore
In 2009, the Laurence Berkley National Laboratory (LBNL) produced a report entitled
High Performance Healthcare Buildings: A Roadmap to Improved Energy Efficiency
(Singer and Tschudi, 2009). This report highlighted many of the challenges confronting
healthcare facilities. Amongst these challenges, several stood out as having an important
role in the design of healthcare architecture, and have prompted the discussion set in the
Singapore context, as presented in section 1.5.1 to 1.5.2.
1.5.1 Challenges Related to the Provision of Medical Services3
Medical services are often required to operate 24 hours a day, every day of the year. This
leads to high overall energy intensity for hospital architecture. Prescribed operational
needs, life-safety concerns and compliance with codes and standards often demand
building services and equipment to be robust, reliable and with backup. Some of the
issues relevant to Singapore healthcare facilities are summarized in Table 1.1.
3 Singer, B. C., Tschudi, W. F., (2009). High Performance Healthcare Buildings: A Roadmap to
Improved Energy Efficiency. Lawrence Berkeley National Laboratory. pp 4.

20
1.5.2 Challenges Related to Healthcare Organization, Structure and
Culture4
The complex functions in large scale healthcare facilities (Section 1.1) have to be
managed, and its organization and operational structure can likewise be very complex.
The organizational structure and culture of the healthcare organization and/or operator
has a large influence on the design of healthcare architecture. Some of the issues relevant
to Singapore healthcare facilities are summarized in Table 1.2.
4 Singer, B. C., Tschudi, W. F., (2009). High Performance Healthcare Buildings: A Roadmap to
Improved Energy Efficiency, Lawrence Berkeley National Laboratory, p. 8.
Table 1.1 Challenges related to provision of medical services in Singapore
Challenges
1. High Receptacle Loads: To provide good quality medical services, modern medical equipment and
processes are required. Inevitably, energy is required for their operation, resulting in high receptacle
and cooling loads (Singer and Tschudi, 2009). As a reference, BCA-NUS Building Information and
Research Centre rated Singapore office building with total building energy efficiency of
147kWh/year/m2 as ‘excellent’, and 348.35kWh/year/m2 or more as ‘poor’. Using KTPH as a reference,
if it is designed based on code requirement, its annual consumption is estimated to be
532.11kWh/year/m2 (Toh, Y. H., project mechanical engineer for KTPH, file archive), which is 1.5time
more than the office buildings rated as ‘poor’ in energy performance.
2. Space Cooling for Tropical Climate: Due to the warm, humid tropical climate in Singapore, and due
to the long operating hours, space cooling becomes one of the main contributing factors for high
energy consumption in healthcare facilities in Singapore. If thermal comfort can be achieved by low-
energy means, significant savings in terms energy consumption and operating expenses can be
achieved. (Lai-Chuah, 2008)
3. Needs for Infection Control: The need for infection control in hospitals, and hence high ventilation
rate, leads to the need for large mechanical systems and high energy demand. Natural ventilation
reduces energy consumption, but poses a question on thermal comfort and whether infection control is
effective. (Infection control association, Singapore)
4. High Energy Costs: As Singapore imports all her energy needs, any measure to reduce energy
consumption – be it through conservation, equipment efficiency or process innovation, contributes to
national competitiveness, lowered costs, and better environment by mitigating carbon emission and
combating climate change. The introduction of a national green rating system, the BCA Green Mark
Scheme in January 2005, followed by mandatory compliance in 2007, illustrates Singapore’s resolve in
bringing energy consumption in check. (National Energy Agency, Singapore; Building Control
Authority, Singapore)
5. Policy and Cost Control Considerations: For government-funded public hospitals, patients in
different wards either pay medical expenses in full (ward A class), or subsidized between 20%
(maxmimum subsidy in ward B1 class) and 80% (maximum subsidy in ward C class), depending on
their financial means. As all Singaporeans are accessible to enjoy the subsidies, it is therefore essential
that healthcare facilities are designed and operated to provide good quality medical services while
minimizing public expenditure. In this regards, two immediate benefits that sustainable healthcare
architecture may bring is reduced resource consumption and improved wellness for patient and staff.
(Lai-Chuah, 2008; Lim, 2003)

21
1.6 Sustainable Healthcare Architecture in Singapore’s Context
Since the introduction of the concept of the ‘triple-bottom-line’ by John Elkington5, the
concept has been widely understood and accepted as essentially “an assessment of social
value and eco-efficiency in addition to the conventional economic/financial balance”
(Szokolay, 2008, p. 322)6. The issues of sustainable healthcare architecture in Singapore’s
context may hence be framed along the economic, social and environmental dimensions,
and this three-dimensional framing is adopted for this dissertation. They are briefly
discussed in Section 1.6.1 to 1.6.3, so as to provide the background as well as to highlight
the opportunities for sustainable healthcare architecture Singapore.
5 The concept of ‘triple bottom line’ was first coined in 1998 by John Elkington in the book
‘Cannibals with Forks: the Triple Bottom Line of 21st Century Business’. 6 Guenther and Vittori (2008) has put forth the business case for sustainable healthcare the needs
to balance multiple priorities and perspectives, represented by triple-bottom-line viewpoints of:
Strategist (represented by the CFO, who is concern with capital cost, revenue streams,
operational efficiency, etc), Seeker (represented by the CEO, who is concern with market growth,
business opportunities, leadership, etc), and the Citizen (represented by the COO, who is concern
with community health and participation, staff relations/retention/recruitment, civic value, etc)
(p. 107).
Table 1.2 Challenges Related to Healthcare Organization, Structure and Culture
Challenges
1. Regulatory and Operational Requirements: As health care is a life-and-death business, some of the
high-energy applications are needed to meet the requirements of medical care, and will not be
compromised. Its operational procedures are also subjected to strict regulatory requirements (Singer
and Tschudi, 2009).
2. Environmental Stewardship: Singapore healthcare sector has a long history of playing the role of
environmental stewardship. For example, Changi General Hospital has a successful programme of
cultivating gardens and vegetables on its roof garden (Verderber, 2010, pp. 162); Alexandra Hospital
(AH) has embraced the notion of ‘healing gardens’ by cultivating lush landscaping within the hospital
premise to provide respite for patients, staff and public (FuturArc, 2011 ). As the KTPH management
team comprises largely from the AH team, the values to uphold environmental stewardship was
brought over. Despite the high-energy nature of healthcare operation, the KTPH management team
was resolute in setting high environmental performance target for the new KTPH (Guenther and
Vittori, 2008, p.p. 172-174).
3. Organizational Culture: The budget and decision structures of the usually complex healthcare
organization, as well as its culture, will influence the value-decision such as the willingness (or lack of)
to incur higher capital expenditure to achieve efficient or high-performance building. In addition, the
nature of the healthcare industry may create a risk-averse and conservative culture, and a complex
healthcare organizational structure may be besieged by bureaucracy or partisan-interests, resulting in a
lack of consensus in decision-making. It takes strong courage and management will for healthcare
management and administration to deviate from established practices and approaches to seek
innovative solution to conflicting demands. It also requires from them the ability to mobilize and
organize resources to put in place a project committee and sub-committees, empowered to take actions
and make decisions (Singer and Tschudi, 2009).

22
1.6.1 Economic Sustainability
Singapore’s healthcare system is ranked by World Health Organization as the best in
Asia and six globally7. She has one of the lowest infant mortality rates but at the same
time also amongst the lowest in total health care expenditure when compared to
advanced economies in Asia (Gauld et al, 2006, pp. 331), if not the World (Lim, 2003,
p.84). This is achieved by a combination of government funding, healthcare insurance
and varying degrees of co-payment by individuals, as a result balancing good quality
healthcare with restraint and responsible expenditure. Within such a healthcare
economic system, the government is heavily involved in governance and administration,
with public hospitals providing 80% of the hospital care. The reverse is true for primary
care, with 80% of the services provided by private clinics (Gauld et al, 2006, p. 331).
In addition, the Singapore government places “a strong emphasis on fitness and health,
evident in workplace-based fitness programmes, and anti-smoking and healthy food
campaigns.” (Ibid., p. 332). Such a wellness philosophy is seen echoed in KTPH’s holistic
model of care, in which emphasis on ‘pre-hospitalization’ and ‘post-hospitalization’
(promoting wellness) stages is supplemented by an efficient and effective
‘hospitalization’ stage (treating illness) (Liat, 2009; See Figure 1.2 and 1.3).
To achieve competitive pricing and affordable healthcare costs for patients, hospital
management and administration have to focus on efficiency and cost control measures,
such as lean and efficient operation and staffing, without compromising on the quality of
medical care and services; this is very much embraced at KTPH.8
7 WHO’s World Health Report in 2000 on health systems. 8 In chapter 6 ‘Efficiency’ of the book Evidence-based Design for Healthcare Facilities, Pille, E. and
Richter, P. wrote about how process improvement e.g. Six Sigma was increasingly employed in
the improvement and planning of healthcare facilities. In the case of KTPH, this is very much the
case, with Six Sigma and the process philosophy of the Toyota Production System harnessed for
process improvement (Design Business Case Study: Alexandra Hospital, 2009).

23
With the assurance of an equitable and sustainable healthcare economic system (Lim,
2003), and no doubt one that will continually to be improved upon to better serve the
evolving society and communities of Singapore9, the next inter-related questions and the
focus of this dissertation, i.e. sustainable healthcare architecture in the Singapore context,
are essentially along the social and environmental dimensions.
9 Corporatization of government hospitals in Singapore to aim at efficient and price-competitive
operation commenced in the mid-80s, and had largely been completed in the 90s. The re-
structuring and clustering of healthcare organizations continued, with the latest restructuring
exercise having taken place in 2008 with the formation of two clusters - the National Healthcare
Group (NHG) and the Singapore Health Services (SingHealth) to provide vertically integrated
health care, aimed at “making public healthcare more accessible to its patients”(MOH Holdings,
2009)
Figure 1.2 “The typical compartmentalized, episodic model of care.”
Source: Liat, T. L. (2009), Planning for a Hassle Free Hospital.
Figure 1.3” Khoo Teck Puat Hospital’s holistic ‘Head-To-Toe Lifelong Anticipatory Healthcare of
Whole Person’ model”. Source: Liat, T. L. (2009), Planning for a Hassle Free Hospital.

24
1.6.2 Social Sustainability
Opportunities in enhancing social sustainability in healthcare architecture rest in the
following areas:
1. Enhancing the wellness of patients, clinicians and hospital staffs through a stress-
reducing environment, as supported by evidence-based research.
2. A healthcare built environment serving as a sustainable public place for the
community.
1.6.2.1 The Relationship between Human Wellness and Environment
Not only are healthcare facilities merely the premise for the practice of medical science
and technology that provide patient safety and quality patient care, it should also be
designed to “embrace the patient, family, and caregivers in a psycho-socially supportive
therapeutic environment” (Smith and Watkins, 2010). The Therapeutic Environment
theory stems from the “fields of environmental psychology (the psycho-social effects of
environment), psychoneuroimmunology (the effects of environment on the immune
system), and neuroscience (how the brain perceives architecture)” (Ibid.), and researches
have shown that provision of therapeutic environment can measurably improve well-
being of patient, healthcare workers, and care givers, including:
1. Supporting clinical excellence in the treatment of the physical body (Ibid);
2. Supports the psycho-social and spiritual needs of the patient, family, and staff
(Ibid);
3. Produces measurable positive effects on patients' clinical outcomes and staff
effectiveness (Ibid).
Such evidence-based research have contributed to the rise of evidence-based design
(EBD), a relatively new field of multi-disciplinary study that places importance in using
25
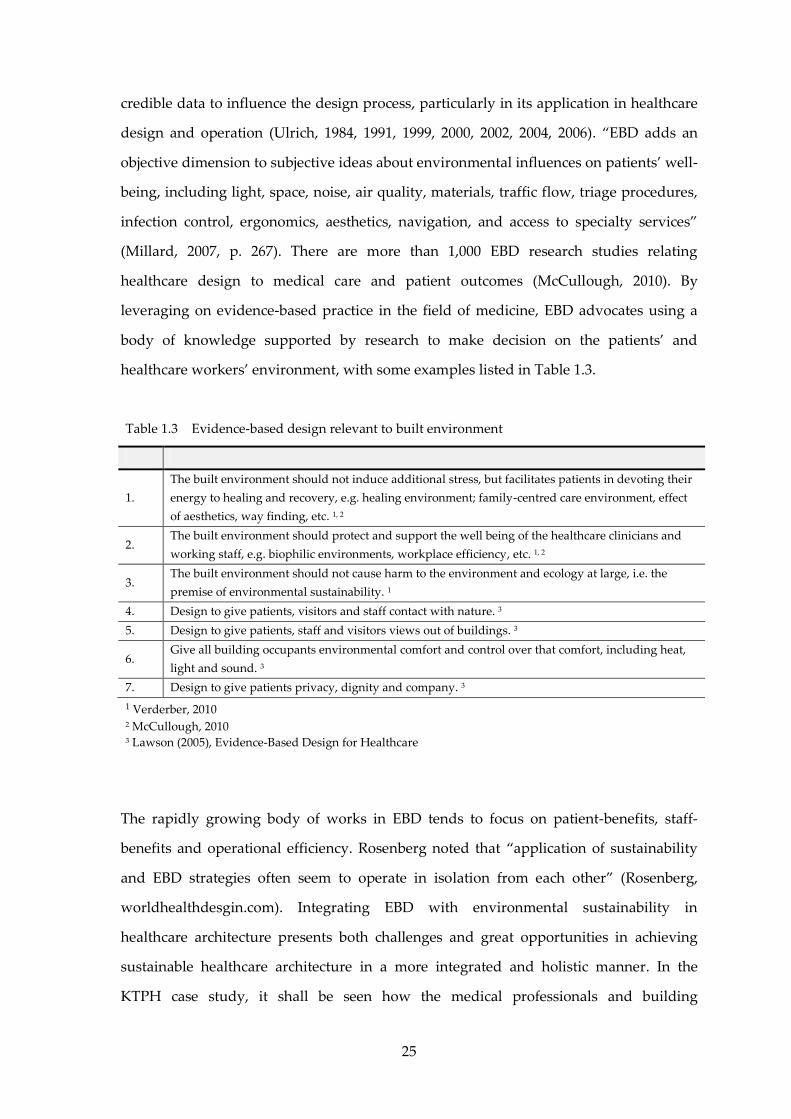
credible data to influence the design process, particularly in its application in healthcare
design and operation (Ulrich, 1984, 1991, 1999, 2000, 2002, 2004, 2006). “EBD adds an
objective dimension to subjective ideas about environmental influences on patients’ well-
being, including light, space, noise, air quality, materials, traffic flow, triage procedures,
infection control, ergonomics, aesthetics, navigation, and access to specialty services”
(Millard, 2007, p. 267). There are more than 1,000 EBD research studies relating
healthcare design to medical care and patient outcomes (McCullough, 2010). By
leveraging on evidence-based practice in the field of medicine, EBD advocates using a
body of knowledge supported by research to make decision on the patients’ and
healthcare workers’ environment, with some examples listed in Table 1.3.
The rapidly growing body of works in EBD tends to focus on patient-benefits, staff-
benefits and operational efficiency. Rosenberg noted that “application of sustainability
and EBD strategies often seem to operate in isolation from each other” (Rosenberg,
worldhealthdesgin.com). Integrating EBD with environmental sustainability in
healthcare architecture presents both challenges and great opportunities in achieving
sustainable healthcare architecture in a more integrated and holistic manner. In the
KTPH case study, it shall be seen how the medical professionals and building
Table 1.3 Evidence-based design relevant to built environment
1.
The built environment should not induce additional stress, but facilitates patients in devoting their
energy to healing and recovery, e.g. healing environment; family-centred care environment, effect
of aesthetics, way finding, etc. 1, 2
2. The built environment should protect and support the well being of the healthcare clinicians and
working staff, e.g. biophilic environments, workplace efficiency, etc. 1, 2
3. The built environment should not cause harm to the environment and ecology at large, i.e. the
premise of environmental sustainability. 1
4. Design to give patients, visitors and staff contact with nature. 3
5. Design to give patients, staff and visitors views out of buildings. 3
6. Give all building occupants environmental comfort and control over that comfort, including heat,
light and sound. 3
7. Design to give patients privacy, dignity and company. 3
1 Verderber, 2010 2 McCullough, 2010 3 Lawson (2005), Evidence-Based Design for Healthcare

26
professionals had contributed their respective knowledge domains e.g. the notion of
healing garden by the medical professionals, as informed by their practice of the same in
their previous premise, Alexandra Hospital (AH), and the notion of bioclimatic,
resource-efficient green building by the building professionals; and through the
integrated design process, contributed to the eventual design outcomes in KTPH.
1.6.2.2 Sustaining Community through Healthy Public Place
‘Healthy hospitals’ (Walsh; in Guenther and Vittori, 2008, p. 390), i.e. hospitals not
merely to treat illness but support and sustain human wellness, may possibly open up its
premise to connect, engage and be enjoyed by its neighbourboods and communities.10
For the case of KTPH, this relates to the surrounding public housing estates, community
club, Yishun Town Centre and the Yishun Pond and public parks near its vicinity. Over
time, a well-used public place is expected to build up a strong civic identity (Verderber,
2010, p. 45). An environmentally friendly and socially engaging hospital encourages
community participation in environmental, social and healthcare programmes e.g.
healthy living, community gardening, medical social works, etc, promoting community
wellness while fostering environmental awareness. In this regards, KTPH again is used
as a case study of a public hospital taking up such community and environmental
stewardships (see Appendix XIV and XV).
1.6.3 Environmental Sustainability
In response to challenges posed by climate change, environmental degradation and
depletion of resources, many green rating tools have been developed to guide the design
of environmentally sustainable architecture. As best practices evolve, the green rating
systems are updated. The UK-developed BREEAM, one of the earliest green rating tools
10 Tzonis, A.(2006) holds the view that while substantial knowledge advancement had been made
“in designing sustainable ecological environments”, in terms of “sustainable social quality”,
“(the) field to explore is enormous and the task of inquiry is just beginning”. He proposed to
“explore and discover how decisions about the spatial structure of the environment as a
communicator enable interactions”. The evidence-based design as informed by healthcare
architecture and research such as space syntax by Bill Hillier (Hillier, 1999) appear to point
towards this direction.

27
initiated (in 1990; see Figure 1.4), introduced the BREEAM Healthcare in 2008 to cater for
the design of healthcare architecture. The US-developed LEED Healthcare has also been
newly introduced in 2011. It was developed in close collaboration with Green Guide for
Healthcare (GGHC), introduced in 2007, providing guidelines on both design and
healthcare operation. Some other design guides or green rating tools for healthcare
facilities are shown in Table 1.4. The list is not exhaustive. In addition, these tools are
constantly being improved and new tools emerging.
Figure 1.4 Comparisons of some green rating systems for sustainable buildings
Source: Bauer, M., Mösle, P., Schwarz, M. (2010)

28
Situated in the tropics, Singapore needed its own green rating system in order to address
the specific requirements in responding to the climatic, natural, economic, social, cultural
political and national security constraints that Singapore faces (BCA)11. A national green
rating system, namely the BCA Green Mark Scheme, was introduced in January 2005 to
guide the design and operation of green buildings in Singapore. It is a matrix and point
system, with four levels of achievement:
Green Mark Platinum (Highest)
Green Mark Gold Plus
Green Mark Gold
Green Mark certified (Lowest)
As a relatively new green rating system, there is no healthcare-specific Green Mark
system. Green Mark Version 3.0 was adopted for KTPH’s design, with Green Mark
Platinum set as the target to achieve. A key question is: is that considered as
environmentally sustainable?
In ‘Trajectory of Environmentally Responsive Design’ (2006) by Integrative Design
Collaborative & Regenesis, ‘[environmentally] sustainable’ is defined as being at a
11 BCA Green Mark Scheme website [online] Available at: <http://www.bca.gov.sg/greenmark/
green_mark_buildings.html>
Table 1.4 Sustainable design guides and green rating tools for healthcare facilities
1. BRE’s BREEAM New Construction: Healthcare is an environmental assessment method and
certification scheme for healthcare buildings in the UK (http://www.breeam.org/).
2. Green Guide for Health Care which provides resources for voluntary, self-certifying metric toolkit
of health-based best practices (http://www.gghc.org/).
3. USGBC’s LEED for healthcare customized the popular LEED green building rating system to
support healthcare building’s unique challenges.
4.
The Strategic Energy Management Planning (SEMP) tools and resources by BetterBricks provide
resources for hospital management and facility directors, healthcare designers, and energy service
providers (http://www.betterbricks.com/ healthcare).
5.
The public review draft of the proposed ASHRAE/ASHE Standard 189.2P for the design,
construction and operation of sustainable high-performance health care facilities was launched in
March, 2011 (http://www.ashe.org/advocacy/advisories/)

29
neutral, “inflection point from degenerating to regenerating health” (Ibid., p. 1; Figure
1.5). Anything less than that, even though it may be ‘Green’ or ‘High Performance’,
simply means that it is better than conventional practice but still causes degeneration to
the environment, albeit to a lesser degree. A ‘restorative’ design or system is one that is
able to “restore the capability of local natural systems to a healthy state of self
organization” (Ibid., p. 2), and ‘Regenerative’ design or system are “an integral part of
the process of life in that place” (Ibid., p. 2). In a regenerative system, people, built-form
and natural systems enter a healthy state of co-evolution. In this sense, not only is
sustainable architecture one that seeks to restore human wellness in the social
dimension, but as part of the natural systems, one that seeks to restore and regenerate
natural health in the environmental dimension.
Figure 1.5 Trajectory of environmentally responsive design
Source: Integrative Design Collaborative and Regenesis (2006)

30
Some have therefore promoted the notion of ‘restorative environmental design’ (Kellert,
2004; Birkeland, 2002), by ‘extending the concept of ecological health to include humans
in the ecological equation’ (Kellert, 2004, p. 3). Architecturally, this includes embracing
nature in the built environment, which complements the inter-related notion of biophilic
architecture (Ibid., Wilson, 1984; Kellert et al, 1993). The notion of ‘biophilia’ premised on
human’s innate affinity with nature and living things, promoting human wellness and
social sustainability in the process. In this regards, environmental and social
sustainability may be seen as symbiotic. To relate to the healthcare context, natural
systems may be embraced to achieve human wellness outcomes, in the process
regenerating the natural systems. Set out to embrace nature for its therapeutic properties,
KTPH again provides a case study demonstrating attempts in fostering natural systems.
1.6.4 Defining Sustainable Healthcare Architecture
By taking into account the various sustainability dimensions in the Singapore healthcare
context (Section 1.6.1 on economic dimension, Section 1.6.2 on social dimension, Section
1.6.3 on environmental dimension), sustainable healthcare architecture may be defined
as an integrated solution that addresses all three dimensions in a holistic manner (Figure
Figure 1.6 Model of sustainable healthcare architecture
Eco-DesignBiophilic Built Environment
Built environment that integrates with natural and ecological systems
Green BuildingHigh-performanceResource-efficient
Maximize passive strategies, e.g. NV
Evidence-Based WellnessCommunity-Stewardship
Built environment that supports integrated healthcare and social systems
EnvironmentalSustainability
EconomicSustainability
SocialSustainability

31
1.6). As proposed, KTPH that was built in 2010 provides a case study for the examination
and discussion of these sustainability dimensions (from Chapter 3 onwards). The
immediate question is: what are the process challenges to be overcome before one is able
to arrive at the outcomes of sustainable healthcare architecture? This is discussed in the
next section.
1.7 Discussion: The Need to Integrate Inter-Disciplinary Knowledge
Section 1.5 of this dissertation presents the key challenges confronted in healthcare
architecture, especially in large scale hospitals. These challenges are rooted in the
complex functions and stringent operational requirements affecting human well-beings.
It is followed by Section 1.6, which presents the opportunities in the Singapore context
for healthcare architecture to advance the economic, social and environmental
sustainability dimensions. Given such opportunities, the main challenges being
confronted by the building professionals (including designers and project team
members) in undertaking the design are as follows:
1. The knowledge domains required to address the economic, social, and
environmental sustainability dimensions reside in different professional
disciplines e.g. evidence-based studies on patient outcomes from the medical
profession, space planning, building safety requirements and high-performance;
green building design from the building professions; and natural systems from
landscape designers and ecologists, etc.
2. The various disciplines need to propose and agree on the specific objectives and
requirements to be achieved in the sustainable healthcare architecture. In so
doing, they must resolve any conflict between these objectives and requirements,
by asking the following questions: Are there trade-offs between these objectives?
Are they mutually supportive? Are there inter-dependencies?
3. After the design objectives and requirements have been determined, a design
process is needed to generate solutions. As the solutions generation is likely to

32
require knowledge input from different professional disciplines, a team-based,
collaborative approach is not only advocated, but necessary. More pertinently,
the solutions generated need to be integrated into a holistic, overall solution.
This team-based, collaborative approach is generally known as the integrated design
approach, and some sources have advocated that it is particularly useful for the design
of healthcare facilities (Guenther and Vittori, 2008, LEED 2009 for Healthcare, Green
Guide for Health Care v2.2). The relevance of integrated design for healthcare
architecture is examined in the next chapter. It starts by defining the integrated design
approach, followed by presenting its relevance to healthcare architecture, before moving
on to presenting the essential elements in an integrated design approach.

33
Chapter 2.0: The Integrated
Design Approach
“An integrated design process creates
opportunities for the design team to link the
many parts of social, technical and earth
systems into a coherently and mutually
supportive whole systems.”
Bill Reed
“(Integrated design process) provides the
means to apply the design strategies and
move society towards sustainability, one
project at a time.”
Alex Zimmerman

34
Chapter 2.0 The Integrated Design Approach
Chapter 1 presents the challenges in the design of sustainable healthcare architecture, in
which knowledge inputs from the different disciplines need to be integrated in a holistic
solution, through a collaborative, team-based process. Such is the premise of the
integrated design approach. In this chapter, by drawing from literature, the following are
presented:
1. The definition of the integrated design approach (Section 2.1);
2. The benefits of integrated design approach to healthcare architecture (Section
2.2);
3. The essential elements of integrated design approach (Section 2.3).
4. Discussion (Section 2.4).
2.1 The Definition of Integrated Design Approach
The ‘Roadmap for the Integrated Design Process’ (2007) defines the integrated design
approach as providing “a means to explore and implement sustainable design principles
effectively on a project while staying within budgetary and scheduling constraints.” (p. i)
Using the term “integrative design”, 7group and Bill defines it as one that “optimizes the
interrelationships between all the elements and entities associated with building projects
in the service of efficient and effective use of resources” (7group)12. Known also as the
“whole building design process”, Whole Building Design Guide website defines
‘integrated design’ as one that “includes the active and continuing participation of users,
code officials, building technologists, cost consultants, civil engineers, mechanical and
electrical engineers, structural engineers, specifications specialists, and consultants from
many specialized fields.”13 This dissertation takes the position that the above definitions
refer to the same subject matter by taking slightly different perspectives; but their intent
and purpose are the same. Hence, for simplicity, the term ‘integrated design’,
12 7group website (2011), Integrative Design. Internet WWW at: <http://www.sevengroup.
com/integrative-design/#fragment-1> (Accessed 10.01.2012). 13 Engage the Integrated Design Process, WWW at: The Whole Building Design Guide. Internet
WWW webpage at: <http://www.wbdg.org/index.php> (Accessed 24.06.2011. Revised 30.10.2010).

35
‘integrative design’ and ‘whole-system design’ as defined by various literature sources
are referred to in this dissertation by the term ‘integrated design’. Summarizing from
these sources, the definitions of the integrated design approach for the purpose of this
dissertation are as follows:
1. A team-based, collaborative design process which includes the active and
continuing participation of users, building professionals, specialists, and
stakeholders from other diverse but relevant disciplines;
2. To explore and implement design outcomes based on sustainable design
principles, including economic, social and environmental sustainability
considerations;
3. So as to achieve sustainable architecture as an end product that meets the
sustainability objectives.
2.2 Benefits of the Integrated Design Approach in Healthcare
Architecture
In chapter 6 Design Process of the book Sustainable Healthcare Architecture, Guenther and
Vittori (2008) give a comprehensive account relating the benefits of the integrated design
approach in delivering values to sustainable healthcare architecture. With
supplementary support from other literature sources, the views are briefly explained in
sections 2.2.1 to 2.2.5:
1. Increasing scale and complexity of healthcare facilities (Section 2.2.1);
2. Failure of traditional siloed and linear design process (Section 2.2.2);
3. The integrated design process allows a broad range of expertise to be integrated
into a holistic solution through a collaborative process (Section 2.2.3);
4. The first outcome is the realization of the healthcare built environment as
sustainable architecture (Section 2.2.4);
5. The second outcome is the building up of an ongoing learning culture within the
healthcare organizations, with integrated design approach both providing
supports and benefiting from such a culture (Section 2.2.5).
36
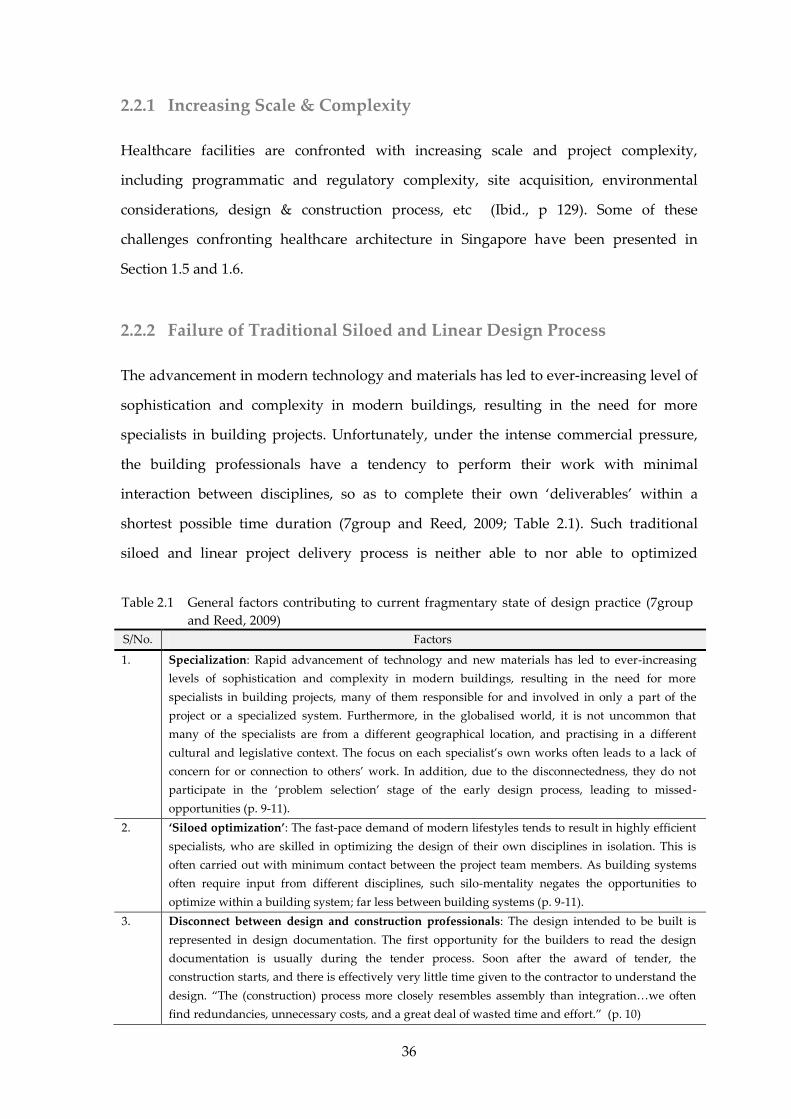
2.2.1 Increasing Scale & Complexity
Healthcare facilities are confronted with increasing scale and project complexity,
including programmatic and regulatory complexity, site acquisition, environmental
considerations, design & construction process, etc (Ibid., p 129). Some of these
challenges confronting healthcare architecture in Singapore have been presented in
Section 1.5 and 1.6.
2.2.2 Failure of Traditional Siloed and Linear Design Process
The advancement in modern technology and materials has led to ever-increasing level of
sophistication and complexity in modern buildings, resulting in the need for more
specialists in building projects. Unfortunately, under the intense commercial pressure,
the building professionals have a tendency to perform their work with minimal
interaction between disciplines, so as to complete their own ‘deliverables’ within a
shortest possible time duration (7group and Reed, 2009; Table 2.1). Such traditional
siloed and linear project delivery process is neither able to nor able to optimized
Table 2.1 General factors contributing to current fragmentary state of design practice (7group
and Reed, 2009)
S/No. Factors
1. Specialization: Rapid advancement of technology and new materials has led to ever-increasing
levels of sophistication and complexity in modern buildings, resulting in the need for more
specialists in building projects, many of them responsible for and involved in only a part of the
project or a specialized system. Furthermore, in the globalised world, it is not uncommon that
many of the specialists are from a different geographical location, and practising in a different
cultural and legislative context. The focus on each specialist’s own works often leads to a lack of
concern for or connection to others’ work. In addition, due to the disconnectedness, they do not
participate in the ‘problem selection’ stage of the early design process, leading to missed-
opportunities (p. 9-11).
2. ‘Siloed optimization’: The fast-pace demand of modern lifestyles tends to result in highly efficient
specialists, who are skilled in optimizing the design of their own disciplines in isolation. This is
often carried out with minimum contact between the project team members. As building systems
often require input from different disciplines, such silo-mentality negates the opportunities to
optimize within a building system; far less between building systems (p. 9-11).
3. Disconnect between design and construction professionals: The design intended to be built is
represented in design documentation. The first opportunity for the builders to read the design
documentation is usually during the tender process. Soon after the award of tender, the
construction starts, and there is effectively very little time given to the contractor to understand the
design. “The (construction) process more closely resembles assembly than integration…we often
find redundancies, unnecessary costs, and a great deal of wasted time and effort.” (p. 10)

37
building performance, nor keep pace with rapid innovation in medical sciences and
technologies (Guenther and Vittori, 2008, p. 129), as they do not invest time in learning.
This is further exacerbate by the increasingly litigatious environments; in response many
professionals have resorted to design by basing on conservative (often rule-of-thumb)
code-compliant norms (7group and Reed, 2009, p. 9 – 11; see also Table 2.1).
2.2.3 The Integrated Design Process
The alternative design process, i.e. the purported integrated design process is one that
seeks to:
1. Harness contributions from a multi-disciplinary team (Guenther and Vittori,
2008, p. 130; Yudelson, 2009, p. 53; LEED for Healthcare 2009, p. 89, Green Guide
for Health Care v2.2, p. 5-3);
2. Establish new, inclusive and collaborative mindset (Guenther and Vittori, 2008,
p. 131; 7group and Bill, 2009, p. 52);
3. Set bold vision and objectives (Guenther and Vittori, 2008, pp. 130; Yudelson,
2009, p. 46);
4. Employ iterative design process through group workshops and design charettes
(Guenther and Vittori, 2008, pp. 130; 7group and Bill, 2009, pp. 68);
5. After delivering the project, continue to learn from it through post-occupancy
feedback loops so as to inform future design (7group and Bill, 2009, p. 312-313).
A comparison between the integrated design process and the conventional design
process, as collated and summarized from various literature sources is shown in Table
2.2.

38
2.2.4 Achieving Sustainable Healthcare Architecture
To Guenther and Vittori (2008), the main intended outcome of the integrated design
approach is sustainable healthcare architecture; one that optimizes building site
planning, envelope design, systems design and material selection in a holistic manner,
“reducing initial cost and delivering sustained, improved performance.” (Ibid., p. 129;
Bokalders and Block, 2010), providing positive outcomes to the community and human
wellness, as well as ecologically restorative and/or regenerative. Briefly defined in
Section 1.6.4, the notion of sustainable healthcare architecture in the Singapore context is
worthy to be revisited in Section 2.3.5, after the integrated design approach has been
presented.
Table 2.2 Comparison between Integrated and Conventional Design Processes
Integrated Design Process Conventional Design Process
Establish clear and shared goals and values 3 Lack clear and shared goals and values 4
Front-loaded – time and energy invested early1;
Intensive design process begins early at the concept
stage with charettes, workshops, etc.3
Involves team members only when essential 1;
Activities become more intense towards
documentation stage with design coordination,
resolve conflicts 1
Engages in individual research as well as group
iteration process, e.g. charettes, workshops, etc.1, 2
Linear or siloed process 1, 2, 4; limited group
contribution in design formulation.
Emphasis on ongoing learning and research 1 Preordained sequence of events
Adopt ‘whole system thinking’ 1 or ‘whole-building
approach’; allow for full optimization.1
Focuses on efficient design of individual systems in
isolation; limited to constrained optimization 1
Seeks synergies 1 Diminish opportunity for synergies 1; poor
communications 4
Life cycle costing 1; consider budget as a whole,
allowing higher cost but better design in one system
(e.g. façade) to be offset by savings from a system
(e.g. space cooling or heating).
Considers budget as isolated, independent systems.
Innovate by applying existing technologies in new
ways, or incorporate group- sanctioned new
technologies to solve problems identified.
Avoid new and unproven technologies to avoid risk
of failure or blame by others.
Preparation of two, three or more options in concept
design alternatives, supported by energy
simulations.
Concept design was formulated based on functions
or image; without thorough considerations for
environmental and social sustainability issues.
Decisions involve all the key stakeholders 1 Decisions are made by a few decision makers 1
Process continues through post-occupancy 1 Typically finished when construction is complete 1
References:
1 Busby Perkins+Will and Stantec Consulting, (2007). Roadmap for the Integrated Design Process. p. 8. 2 7Group, Reed, B., (2009). The Integrative Design Guide to Green Building: Redefining the Practice of Sustainability. p. 9. 3 Yudelson, J., (2009). Green Building through Integrated Design. p. 46. 4 ANSI MTS 1.0 WSIP Guide, (2007). Whole System Integrated Process Guide. p. 3-4.

39
2.2.5 Learning Organization
Guenther and Vittori (2008) further suggested that healthcare organizations should
indeed strive to be learning organizations, imbue with a culture that values continual
learning and improvement, and engages all its members in doing so. By engaging the
integrated design process, the healthcare organization may endeavour to embody it’s
project vision and goals into the architectural design (ibid., p. 130), achieving synergy
and integration between built environment and operations.
Having established the benefits of the integrated design approach to achieving
sustainable healthcare architecture, the next section discusses the essential elements of
the integrated design approach.
2.3 Essential Elements of the Integrated Design Approach for
Healthcare Architecture
This section expands on the integrated design approach for healthcare architecture by
examining the following:
1. The multi-disciplinary project team and the expertise they need to bring to bear
on the project (Section 2.3.1);
2. Mindset change that is required among the project team members in order to be
effective in achieving integrated design (Section 2.3.2);
3. The integrated design process: What the project team members need to do right
(Section 2.3.3);
4. Tools and techniques: What are the tools and techniques that support integrated
design? (Section 2.3.4);
5. The integrated design product: What are the expected outcomes of integrated
design? (Section 2.3.5).

40
2.3.1 The Multi-Disciplinary Project Team
The integrated design approach advocates at bringing together, at an early stage, all key
stakeholders, e.g. owner, management, building designers (e.g. architects, civil &
structural engineers, mechanical and electrical engineers, landscape designers, etc)
consultants (e.g. cost, lighting, acoustic, façade, green design, etc), builders, users,
operators, and perhaps even community representatives, to identify common goals and
objectives of the hospital project (Guenther and Vittori, 2008). This is because no one
party has all the knowledge of the design problems, especially for a large, complex
hospital. Without a proper brief formulation process at an early stage, the opportunity
for deriving a holistic, integrated solution will quickly diminish as project time is
expended (Ibid., Section 1.7).
A suggested list of members for an integrated project team is given in LEED 2009 for
Healthcare (Figure 2.1). The organization of the team is discussed in Section 2.3.3.1.
To balance sustainability priorities, it is often necessary to include non-building experts
in the team. For the case of sustainable healthcare facilities, it is essential to include in the
project team the representatives from the medical professionals, e.g. clinicians, nursing
Figure 2.1 Multi-disciplinary project team for healthcare project
Source: LEED 2009 for Healthcare (New Construction & Major Renovations)

41
leaders and operational managers. Not only are they expected to share knowledge and
experience, as a result providing insights on how work in the healthcare facilities is done
today, they are expected to think through how work can be done better, hence providing
foresight for the next 10 to 15 years (Pille and Richter, in McCullough, 2010, p. 16, 119).
After the myriad of clinical and operational requirements had been identified, they need
to be put together spatially and systemically, and resolved with other building
requirements.
Multi-disciplinary problems that require spatial and whole-system solution
Amongst the established building professionals, architects as “three-dimensional
problem solvers” (Williams, 2007, p. 14), are the most suited in leading the team of
building professionals to “devise an integrated solution to a whole cluster of
requirements.” (Lawson, 2005, p. 59) In his book ‘How Designers Think: The Design
Process Demystified’, Bryan Lawson proposes a three-dimensional model of design
problems to represent the range of design problems, issues or constraints that building
designers need to grapple with (Figure 2.2). They include design problems generated
from the designers’ own knowledge, as well as those from building regulations
(legislator), clients and users.14
These problems may be internal, e.g. designer’s own set of values; or external, e.g. fire
safety measures stipulated in building authorities’ planning requirements. In addition,
further requirements are imposed from: Purpose of the building project (radical);
practical issues such as ease of construction, cost, and availability of technology
(practical); visual organization e.g. massing, proportion, texture, colour, etc; and the
expressive qualities and perceptive interpretation of the design (symbolic).
14 In the case of KTPH, clients are represented by the hospital management (Alexandra Health)
and the government (Ministry of Health), which is the policy maker and funding agency. The
users include the clinicians, nursing leaders, laboratory leaders, office administrators, operational
managers, etc.

42
The whole cluster of design problems requires holistic solution finding with design
iteration involving different experts, balancing one requirement versus another, in the
process seeking to find synergies between these requirements. This is the premise of
integrated design process, presented in Sub-section 2.2.3.15
2.3.2 Mind Set Change: The Need for a Whole-System Mental Model
Before moving on to the presentation of the integrated design process and tools, it is
important to emphasize on the need for mindset change among the integrated design
team members (Reed, Todd and Malin, 2005; Reed in Guenther and Vittori, 2008, pp.
132). At this juncture, it is useful to refer to the model developed by Bill Reed and Barbra
15 Lawson has also put it that, “(design) inevitably involves subjective value judgement” (2005, p.
124), and as “three-dimensional problem solvers” in control of the ‘primary (design) generator’
(ibid), the architect plays a highly influential role in perpetuating the values in the design
solution, but it also comes with heavy responsibilities in the success of the integrated design
process, e.g. to adopt an open mind and listen to views (and values) offered by other team
members; “it demands that architects fundamentally alter their role. But giving up control goes
against everything architects are taught” (Deutsch, 2011, p. 136). This may impose hurdles in the
practice of integrated design, so a critical self-examination in architectural education and practice
is warranted.
Figure 2.2 Bryan Lawson’s model of design problems or constraints
Source: Lawson, B. (2005). How Designers Think: The Design Process Demystified, p 106.

43
Batshalom (Reed, Todd and Malin, 2005; Guenther and Vittori, 2008, pp. 131-135) as
shown in Figure 2.3. It clarifies the relationship between mental model (mindset, attitude
and will), process (design, iterative analysis, workshop, charrette), tools (green rating
tools, design guides, benchmarks, modeling programs), and products/technologies
(building components, technologies, techniques, and the built environment as end
product).
The siloed and linear traditional mode of thinking and design approach needs to be
replaced by a mental model centred on whole-system thinking (Reed, Todd and Malin,
2005). It is premised on seeing not only the parts, but the whole; and not only what the
system does, but what is the purpose of the system, or how does the system contributes
to larger whole (Ibid).
Attitude of the project team members
Even with the multi-disciplinary project team in place, without the right team attitude,
gaps in communication and sharing of knowledge and information are likely to be
encountered (Figure 2.4). Many integrated design guides hence advocate the needs to
cultivate positive, inclusive, collaborative and trusting attitudes among integrated
design team members. These attitude attributes tend to foster a group dynamics that
allows the design team to generate design outcomes “beyond the abilities of the
Figure 2.3 The new mental model for integrative design
Source: Barbra Batshalom and Bill Reed (Reed, Todd and Malin, 2005, p. 17).

44
collective individual talents” (Lawson, 2005, p. 242). A summary of these attributes from
various sources is shown in Table 2.3.
2.3.3 Integrated Design Process
The right mindset needs to be supported by the right process. The Whole Systems
Integrated Process (WSIP, 2007) as recommended in LEED 2009 for Healthcare (p. 93) is
used in this dissertation as the IDP reference, supported and complimented by other
literature references as and when necessary. The WSIP (2007) is “intended as a standard
Figure 2.4 Zeisel’s user-needs gap model Source: Lawson, B. (2005). How Designers Think: The Design Process Demystified. p 86.
Table 2.3 Positive attitudes necessary among the integrated design team members
S/No. Factors
1. Clear leadership 2;
2. Inclusion and collaboration 1; everyone buys in and participate 3
3. Outcome oriented 1; set stretch goals 3; commit to zero-cost increase 3
4. Trust and transparency 1; social team-building 2
5. Open-mindedness and creativity 1;
6. Rigour and attention to details 1;
7. Continuous learning and improvement 1; team building through teaching and learning 2
References:
1 Busby Perkins+Will and Stantec Consulting, (2007). Roadmap for the Integrated Design Process. p. 9.
2 7Group and Reed, (2009). The Integrative Design Guide to Green Building: Redefining the Practice of Sustainability. p. 30-
31.
3 Yudelson, J., (2009). Green Building through Integrated Design. p. 46.

45
guideline to support the building industry in the practice of integrative design” (p. 1)16,
and its purpose is to provide a common reference for “all practitioners (architects,
builders, designers, engineers, landscape architects, ecologists, clients, manufacturers,
and so on) in support of process changes needed to effectively realize cost savings,
deeper understanding of human and environmental interrelationships, and an improved
environment for all living systems – human, other biological, and earth systems.” (Ibid.,
p. 1) Based on WSIP (2007, p. 8), the process stages in IDP may be categorized into six
stages (see Table 2.4), presented in Section 2.2.3.1 to 2.2.3.6.
16 Whole System Integration Process (WSIP, 2007), The Institute for Market Transformation to
Sustainability, Washington.
Table 2.4 WSIP Process Stages (2007, p.8)
Stage Elements
1. Team Formation “Fully engage Client in the design decision process.”
“Assemble the right team.”
Key attributes in team formation is ‘teachable attitude’; members come on board
not as experts but co-learners.
2. Visioning “Align team around basic Aspirations, a Core Purpose, and Core Values.”
3. Objectives Setting “Identify key systems to be addressed that will most benefit the environment
and project”
“Commit to specific measurable goals for key systems”
Compile into a Sustainable design brief
Key attributes in objective setting is to involve all participants, including the
main financial decision maker, not unempowered representative. Also, identify
champions for the objectives and issues.
4. Design Iteration “Optimization of the design of systems”
Key attributes in objective setting is to “understand and make best use of key
systems in relationship to each other, to the goals, and to the core purpose”, and
“Iterate ideas and systems relationships among team with all participants,
including the main financial decision maker.”
5. Construction &
Commissioning
“Follow through during the Construction Process.”
“Commission the project.”
6. Post-occupancy
Feedback Loops
“Maintain the system.”
“Measure performance and respond to feedback - adjust key aspects of the
system accordingly.”

46
2.3.3.1 Team Formation and Organization
The need for multi-disciplinary team formation has been covered in Section 2.3.1.
However, the team structure and organization and how effective each team members
play out their role is very important in driving the process forward. The ‘Road Map for
the Integrated Design Process’ (IDP Road Map; Busby Perkins+Will and Stantec
Consulting, 2007) proposes that the integrated design team (IDT) be formed as early as
practicable. In principle, a typical IDT comprises the following (p. 15):
1. Client: The client takes an active role throughout the design process.
2. Expertise/Stakeholders: A broad range of expertise and stakeholder perspectives
is present.
3. Team Leader: A team leader (champion) is responsible for motivating the team
and coordinating the project from pre-design through to occupancy.
4. Facilitator: An experienced facilitator is engaged to help guide the process.
5. Core Project Team: The core group of team members remains intact for the
duration of the project.
6. Collaborative: Team members collaborate well.
The multi-disciplinary core project team is responsible to collaborate and drive the
project forward, as well as to identify and bring in additional team members with
relevant expertise that support the project (Ibid. p. 15-17). Table 2.5 provides a basic
summary of the recommended core project team members, additional members and
description of their expected roles. A more detailed role of the various members
throughout the project stages as provide in IDP Roadmap is shown in Appendix I.
To facilitate the collaborative spirit among the team members, the IDP Roadmap
recommends two additional roles not usually found in traditional team organization:
1. Facilitator: The IDP Facilitator manages the integrated design process. He/she
may be one of the project core team members, e.g. project manager or architect, or
it may comprise a team, but the most important attribute skill sets they bring to

47
bear are in facilitation and group dynamics, and they must have a good
knowledge of the ‘integrated design process’ (IDP) (IDP Roadmap 2007, p. 17).
2. Champion: The Champion is aligned with the vision of the project and is
someone who is able to empower the team, understand the political and
organizational barriers and is able to overcome them. The Champion may also be
the Facilitator (IDP Roadmap 2007, p. 17).
A comparison between the conventional team organization and the IDP team
organization is shown in Figures 2.5 and 2.6 (IDP Road Map, 2007, p. 18).
Table 2.5 Core Integrated Project Team Members (IDP Road Map, 2007, p.15-17, Appendix B)
Core Team Member Role and Expertise
1. Client or owner’s
representative
With expertise in operations management
With expertise in facilities management
2. Project manager Manages project schedule, team communication and control of budget
3. Architect
Site planning and response to climate, natural and physical context
Space planning to meet programmatic and authority requirements
Form, envelope design, visual and aesthetics design to meet client/user
aspirations
4. IDP facilitator Facilitates workshops. May be one of the team member with the
necessary facilitation skills.
5. Champion (optional) Align with the project vision and empowers the team
6. Structural engineer Structural system and choices that impact form and massing
Understands the inter-relationship between structural, architectural and
spatial programmes, and mechanical and electrical systems
7. Mechanical engineer With expertise in simulation: energy modeling, thermal comfort analysis,
and/ or CFD simulations.
With expertise in energy analysis: an energy engineer and/or bioclimatic
engineer may be required in order to cover the necessary areas of
expertise, such as: passive solar design, renewable energy technologies,
and hybrid–tech strategies.
8. Electrical engineer Provide input on energy systems, lighting/daylight design, etc.
9. Green design specialist Provides input on energy-efficient and energy generation options.
Provides support on green design processes and tools.
10. Civil engineer With expertise in: stormwater, groundwater, rainwater, and/or
wastewater systems.
11. Facilities manager/
Building operator
Lessons learnt on operating other buildings
Participate in workshops, review design and documentation
12. Green design specialist Knowledge and advise on green design strategies and resources
13. Cost consultant With experience in life-cycle costing
14. Landscape architect Provide input on landscape design, habitat preservation or restoration
15. General contractor or
construction manager.
Provide input on construction methods, materials, etc. Support the green
design strategies during construction execution.

48
Table 2.6 Additional Integrated Project Team Members (IDP Road Map, 2007, p.15-17,
Appendix B)
Additional Member
1. Ecologist 9. Commissioning agent
2. Occupants’ or users’ representatives 10. Marketing expert
3. Building program representative 11. Surveyor
4. Planning/regulatory/code approvals agencies
reps
12. Valuation/appraisal professional
5. Interior designer/ materials consultant 13. Controls specialist
6. Lighting or daylighting specialist 14. Other experts as required (e.g., natural
ventilation, thermal storage, acoustic)
7. Building program representative 15. Academics and/or students with knowledge of
a relevant subject
8. Soils or geotechnical engineer 16. Members of the community who are affected
by the project.
Figure 2.5 Conventional design team organization Source: Roadmap for the Integrated Design Process. p. 18
Figure 2.6 Integrated design team organization
Source: Roadmap for the Integrated Design Process. p. 18

49
2.3.3.2 Visioning
The visioning exercise provides the opportunity to align team members’ mindsets,
attitude (as discussed in Section 2.3.2) and will or commitment to a common purpose
and shared values. For healthcare organizations, this also provides the opportunity to
align its long-term health vision and mission to serve as the navigation beacons to guide
the integrated project team’s design (Guenther and Vittori, 2008).
2.3.3.3 Objectives Setting
Visions need to be supported by specific design objectives establish early in the project.
To achieve balanced objectives, one recommendation is to guide the objective and goal
formulation by taking the triple bottom line approach to sustainable development
(Figure 2.7; Yudelson, 2009).
For healthcare project, this may include setting objectives such as:
Figure 2.7 Triple Bottom Line approach goal setting for a project visioning session
Source: Yudelson (2009). Green Building through Integrated Design. p. 147.

50
1. Economic sustainability: Setting high-performance goals that raise the bar or
challenge the status quo, by specifying measurable targets such as ‘reduce energy
consumption by 50% as compared to the baseline’ (Yudelson, 2009).
2. Social sustainability: Basing on evidence-based studies to improve environmental
supportive qualities, clinical, service, and operational efficiencies; as a result
enhancing social sustainability (McCullough, 2010)
3. Environmental Sustainability: Through integrating natural systems with built
environment, (Kellert, 2004; Wilson, 1984; Kellert et al, 1993)
The vision and objectives shall not, however, become prescriptive, or worse, describe the
solution, in so doing giving little room for designers to seek creative solution (Lawson
2004; Yudelson, 2009).
2.3.3.4 Design Iteration
Design iteration is a key feature in any IDP methodologies. WSIP (2007) emphasized the
need to alternate between individual or small group research activities by participating
parties (represented by the coloured bars in Figure 2.8) and team charrettes or workshop
sessions participated by key stakeholders (represented by the blue dots in Figure 2.8).
These are denoted as R1 to R4 and W1 to W7, and their iterative activities are
summarized in Table 2.7.
Figure 2.8 Integrative design process. Adapted from WSIP (2007).
R2R1 R3 R4
W1 W2 W3 W4 W5 W6 W7

51
Table 2.7 IDP: Research and workshop activities for healthcare architecture
Stage Elements
R1: Research/
Analysis #1
Preliminary research, e.g. “identify base condition, context of project,” and
sustainability opportunities; project programming; preliminary climatic
studies, etc.
W1: Workshop/
Charrette #1
Visioning exercise involving all key stakeholders
“Goal Setting and alignment of purpose/objectives among all participants.”
R2: Research/
Analysis #2
Continue research, e.g. establish comparative benchmarks, envelope and
shading study, energy modeling, water management studies, clinical and
operational workflow studies, space planning, circulation analysis,
investigation of structural system, life cycle cost studies, etc.
Test initial concept for feasibility
W2: Workshop/
Charrette #2
Generate or iterate concept design or early schematic design through
charrettes.
“Review integrative cost bundling studies.”
Confirm with client the alignment of project with vision and objectives.
R3: Research/
Analysis #3
Schematic design: “Alignment of research and integration of design.”
Iterate design at more detailed levels, optimize system designs.
“Review integrative cost bundling studies.”
Use metric, benchmark and green rating tools to test design.
Perform simulation studies.
W3: Workshop/
Charrette #3
Mid schematic design: “Fine-tuned refinement of the design and definitive
inclusion of sustainability objectives with supporting data.”
“Confirm the alignment of Client, Design, and Construction (or Cost
Estimating) team around the objectives and aspirations.”
“Continue refining the integration of systems.”
“Refine the Design and/or schedule the refining meeting and research process
to get there,” e.g. confirm detailed layout plan with users.
R4: Research/
Analysis #4
“Continue to refine modeling and design.”
“Continue to test design concepts against the Core Purpose, Design
Drivers, and Metrics and Benchmarks.”
“Review any Integrative Cost Bundling Studies in process continuous Value
Engineering.”
“Begin documentation process for rating system.”
“Build performance measurement and feedback loops into project.”
W4: Workshop #4
W5: Workshop #5
“Late Schematic Design / Early Design Development.”
Sign-off workshop; tie-up loose ends.
W6: Workshop #6/
Construction
Documentation
“Detailed review of Drawings and Specifications”
“Address non-building related sustainability issues.”
Refine documentation; continue value engineering; green rating
documentation.
W7: Workshop #7/
Bidding &
Negotiations
“Pre-bid & Post Award Conferences to explain unique aspects of project
Detailed review of Drawings and Specifications”
“Address non-building related sustainability issues.”
Refine documentation; continue value engineering; green rating
documentation.
Adapted from Whole Systems Integrated Process Guide (2007)

52
In ‘Strategies for integrative building design’, van der Aa, Heiselberg and Perino (2011)
proposed a more detailed iterative process during the schematic design (SD) phase and
design development (DD) phase. They proposed that design iteration shall progress
from ‘concept design’ phase to ‘system design’ phase, and eventually to ‘component
design’ phase (Figure 2.9). In the concept design phase, broad strategies are considered,
including response to local climate (Ibid.). For sustainable healthcare architecture, other
considerations at this phase may include programmatic requirements, regulatory
requirements, and opportunities for ecological integration with the surrounding. In the
system design phase, specific architectural and technical solutions are proposed,
supported by design calculations and simulations. In the process, the design team
members should seek opportunity for design integration of systems (Ibid.). The
component design phase takes place in WSIP 2007’s design development (DD) stage,
which seeks to confirm the system design, before proceeding to the design and selection
of actual building components.
van der Aa, Heiselberg and Perino (2011) highlight that the integrated design process is
characterized by the iteration loops (Figure 2.10), providing “problem-oriented analyses
of design alternatives and optimization…and taking into consideration input from other
Figure 2.9 Iterative processes as proposed in ‘Strategies for integrative building design (van der
Aa, Heiselberg and Perino, 2011). Text in red added for referencing with WSIP (2007).
SDD
D
Research/Analysis Workshops/Decisions

53
specialists, influences from context and society that provide possibilities and/or
limitations to design solutions as well as evaluates the solutions according to the design
goals and criteria” (ibid., p. 8). There are many alternative theories regarding the
iteration loops or process, which are presented in Appendix II. The position taken in this
dissertation is that it is not advisable to be overly prescriptive; as expounded by Lawson
(2005), “there is no infallibly good way of designing. In design the solution is not just the
logical outcome of the problem, and there is therefore no sequence of operations which
will guarantee a result” (p.p. 123-124).
Both the Integrated design process (WSIP, 2007; Figure 2.8) and the Iterative process (van
der Aa, Heiselberg and Perino, 2011; Figure 2.9) are used as models to examine the
KTPH integrated design process.
2.3.3.5 Construction & Commissioning
Depending on the type of contract procurement method, the contractor may join the
project team earlier or only at this stage. Again, an alignment between client, design
team, stakeholders and contractor is required. Construction through to commissioning
takes place at this stage.
Figure 2.10 ‘Iteration loops’ as proposed in ‘Strategies for integrative building design’ (van der
Aa, Heiselberg and Perino, 2011). [This author is of the view that ‘Coal’ in the diagramme is a
typological error and show read as ‘Goal’ instead].

54
2.3.3.6 Post Occupancy Feedback Loops
After proper handing over of building and facilities, the operations and maintenance of
the facilities are carried out by trained personnel, based on sustainable principles.
Building monitoring systems begin to measure and trend building performance, and
post-occupancy evaluations are conducted to compare design assumptions and actual
usage. The owner, design team continue to receive feedback on the systems’ data
(building, energy, water, landscape, habitat, etc), so that the information gained can be
studied, analyzed and form evidence-based studies to inform future design. This
attribute of a continuous learning culture in the integrated design process augurs well
with healthcare organizations that strive to be learning organizations, as presented
earlier in Section 2.2 and 2.2.5, particularly in studies relating environment to human
wellness.
2.3.3.7 Comparison between IDP and Linear Design Process
Before moving on to discuss about the IDP tools and techniques, a comparison between
the IDP and linear design process (LDP) will provide clarity on the difference between
IDP and LDP. With reference to Figure 2.11, the IDP is contrasted against LDP as follows
(Figure 2.11):
1. Activities are front loaded for IDP, and the reverse for LDP.
2. Longer time duration in schematic design (SD) when compared to design
development (DD) and construction documentation (CD) for IDP; short SD, long
DD and CD for LDP.
3. For IDP, intense team collaboration, workshops and individual/small group
research are held from the start, gradually tapering off near DD; for LDP,
activities start slow but begins to peak at DD, and probably continues through
CD stage. Meetings are held focusing on individual disciplines.
4. Continuous value engineering (VE) for IDP, sporadic and intense during bid and
negotiation for LDP.

55
5. VE for IDP focuses on system synergy, VE for LDP focuses on eliminating
features to reduce cost.
2.3.4 Tools and Techniques that Support Integrated Design
The integrated design process needs to be facilitated by design tools to inform team-
based design decisions, as well as design techniques to facilitate team-based
collaboration. These are briefly presented in the sub-sections 2.2.4.1 and 2.2.4.2.
2.3.4.1 Integrated Design Tools
During the integrated design process, various tools may be utilized to permit informed
decision-making. Many of such tools are becoming widely available (Reed, Todd and
Malin, 2005). Some of the tools relevant for healthcare architecture include:
1. Green rating tools, e.g. BREEAM Healthcare, LEED for Healthcare, Green Mark,
etc.
2. Green design guides, e.g. Green Guide for Health (GGHC), Practice Greenhealth,
etc.
Figure 2.11 Integrative design process versus linear design process. Source: WSIP (2007)

56
3. Scale modeling tools, e.g. wind tunnel test;
4. Computer modeling tools, e.g. energy modeling, climatic simulation,
computational fluid dynamics (CFD) simulations, etc;
5. Life cycle costing and Life cycle assessment tools, e.g. Building for Environmental
and Economic Sustainability (BEES), etc.
6. Digital design collaboration tools, e.g. building information modeling (BIM).
Green rating tools (GRT) had been briefly discussed in 1.6.3. Those tailored for
healthcare facilities are usually jointly developed and endorsed by both building and
healthcare industries and/or authorities (e.g. BREEAM Healthcare, LEED Healthcare).
GRT or metrics are primarily used as building performance metric to set design
objectives for the project (WSIP, 2007), but may also be used as systematic frameworks to
guide and align the project team members (IDP Roadmap, 2007). GRT provide a
commonly accepted standard for assessing green buildings in their respective home
markets (Yudelson, 2009), and widespread industry participation in a prevalent green
rating system also allows building design parameters and best practices to be captured
in a central database (Ibid., 2009). Over time this is a form of learning loops to allow the
building industry to progressively improve upon the sustainable performance of its
building design. Other forms of tools such as Green design guides e.g. GGHC are
typically self-assessment metric toolkits to provide objective criteria based on best
practices in which “designers, owners, and operators can use to guide and evaluate their
progress towards high performance healing environments” (GGHC version 2.2, p. 1-1).
Scale and computer modeling tools allow the building performance of different design
iteration to be ‘predicted’ through simulation, so that informed design decisions can be
made (IDP Roadmap, p. 15). Currently, the common modeling tools used in the design
process includes climatic, sun path and shading analysis software (Autodesk Ecotect;
Integrated Environmental Solutions, etc); wind tunnel and CFD software that simulates
air buoyancy and air movement which is useful when strategies involving natural
ventilation are considered (Phoenix; Fluent; Integrated Environmental Solutions, etc);
and energy modeling software which is playing an increasingly important role in

57
integrated design process, as it allows the different contributing factors that affect energy
performance of the building to be simulated to obtain a combined outcome, in the
process enhancing the project teams’ understanding of project opportunities and
constraints (Hatten, Betterbricks). The utilization of computer modeling tools is gaining
momentum in Singapore in recent years, as encouraged by BCA Green Mark scheme
which credit points to aptly applied energy modeling and other forms of simulations
(BCA).17
Life cycle cost (LCC) provides consideration of cost based on whole-life principle, which
includes considerations for initial capital expenditure as well as costs associated to
maintenance, operation and disposal (Riggs, 1982). The use of LCC tools facilitate the
IDP project team by allowing decisions to be made based on the long-term cost impact of
each iteration option. The parameters of LCC need to be defined, e.g. whether it
considers only building operation, or also takes into account human productivity (Fuller,
2010). Life cycle assessment (LCA) tools such as ISO 14040 (2006) assesses environmental
impact of the entire life cycle of a development, including considerations materials
processing, manufacture, distribution, use, repair, maintenance, disposal and/or
recycling (Ibid.).
Building information modeling (BIM) is slated to replace computed aided-design (CAD)
as a design and documentation tool. Instead of representing buildings as lines and
shapes, BIM allows a building design to be represented by virtual components with
parametric properties that may be manipulated in the design process (Krygiel and Nies,
2008). What is perhaps more important is that BIM allows a central, shared virtual model
to be accessible by all the integrated design team members. Each team member is able to
contribute by adding ‘layers’ of information to the model, and their effects on other team
members’ layers of information becomes apparent in the virtual model (Ibid.; Figure
2.12). Immediately, this facilitates the elimination of conflicts between information
provided by different disciplines, a common occurrence in the fragmentary practice of
17 BCA Green Mark Assessment Criteria. Available at: <http://bca.gov.sg/GreenMark/
green_mark_criteria.html> [Accessed 21.01.2011].

58
having separate CAD files. A more profound impact it brings to the building industry is
that the new paradigm of BIM workflow mirrors the integrated design paradigm (Fig
2.13), facilitating sharing and real-time collaborative working (A more detailed
presentation of BIM and its benefits are presented in Appendix III). Due to its benefits
and huge potentials in reinventing the construction industry, BIM is actively promoted
by the Singapore government through BCA (Cheng, 2011).
BIM adoption in Singapore gathers speed only after 2008, and unfortunately KTPH did
not utilize BIM as a design and documentation platform.
Figure 2.12 The integrated design model. Source: Krygiel and Nies, 2008, p. 37
Figure 2.13 The traditional team model and an integrated design team model in information
exchange. Source: Krygiel and Nies, 2008, p. 61

59
2.3.4.2 Integrated Design Techniques
Employing social techniques in the integrated design process facilitate behavioural
change, such as (7Group et al, 2009; Busby Perkins+Will, 2007; WSIP, 2007; Roadmap,
2007)18:
1. Team-based meetings/charrettes/discussions to facilitate an integrated,
synergistic, co-designer approach.
2. Group sessions are facilitated or guided by members with good leadership
quality.
3. Good communication/dialogue/conversation/narration/negotiation.
4. Shared responsibilities among team members.
5. Shared values developed among team members.
6. Trust-building among team members.
The integrated design approach explicitly promotes the often overlooked aspect of
design as a social, collective process, ‘’in which the rapport between group members can
be as significant as their ideas’’ (Lawson, 2005, p. 240). Since large scale and complex
healthcare projects often require a sizable building design team with support from
specialists and non-design professionals e.g. clinicians, nursing leaders and operation
managers, social skills and group dynamics among the team members are as crucial as
their professional skills and knowledge in ensuring project success. The adoption of new
mindset (Section 2.3.2) needs to be supported by appropriate social, team-based design
techniques and methodologies.
In addition, some have suggested that in the creative process, group dynamics has a
distinct advantage over the individual. In How Designers Think: The Design Process
Demystified, Lawson (2005) described in the design of St Mary Hospital, how Tim Burton
assembled a group comprising representatives from three client bodies and consultants,
and over a three-day intensive design process, led the group to agree on the ‘’main
18 Some IDP literature provides very specific guides on techniques, e.g. ‘effective facilitation’
(Roadmap, 2007, p.p. 21-22). Effectiveness of these techniques may be subjected to cultural
influences, and is not the focus of this dissertation.

60
heading of the brief, identified three basic design strategies and selected one for further
development including rough costings’’ (Ibid., p. 241). The selected scheme became the
basis for the final design.
In postulating the future roles of the designers (not limited to building designers, but
particularly relevant to them) in the post-industrial society or knowledge-based society,
Lawson stated that one plausible outcome is ‘’designers remain professionally qualified
specialists but try to involve the users of their designs in the process’’ (Ibid., p. 30) In
such a world, in which designers no longer have a monopoly of design knowledge, the
participatory approach allows designers to stay relevant and engaged with the
stakeholders (who may hire design and building professionals to represent them), by
offering specialist skills to ‘‘identify the crucial aspects of the problem, make them
explicit, and suggest alternative courses of action for comment by the non-designer
participants’’ (Ibid., p. 30). The evolution of such a role for designers will be coupled
with the development of new processes, e.g. IDP and new tools, e.g. building
information modeling, building performance simulation, etc, as discussed in Section
2.3.3 and 2.3.4.
2.3.5 Integrated Design Products: Sustainable Healthcare Architecture
In Section 1.6.4, sustainable healthcare architecture is defined as a holistic, integrated
solution that addresses the three dimensions (economic, social, environmental) in a
holistic manner (Figure 1.5). In Section 2.2.4, it is further put forward that the integrated
design approach is a means to realizing sustainable healthcare architecture, by
integrating whole-building system design that optimizes building site layout, envelope
design, system design and material selection in a holistic manner, “reducing initial cost
and delivering sustained, improved performance.” (Ibid., p. 129; Bokalders and Block,
2010), community and human wellness considerations supported by evidence-based
studies, as well as ecologically regenerative considerations.

61
Summarizing from the discussion so far, in the Singapore context, the relationship
between sustainability opportunities and challenges, integrated design approach and
sustainable healthcare architecture as an outcome may be represented by Figure 2.14.
Figure 2.14 Achieving sustainable healthcare architecture through integrated design
EnvironmentalSustainability
EconomicSustainability
SocialSustainability
1. Disparate operational and sustainability Issues and requirements
Eco-DesignBiophilic Built Environment
Built environment that integrates with natural and ecological systems
Green BuildingHigh-performance
Built environment as holistic, bioclimatic system of systems
Evidence-Based WellnessCommunity-Stewardship
Built environment that supports integrated healthcare and social systems
Environmental Sustainability
Economic SustainabilitySocial Sustainability
EnvironmentalSustainability
EconomicSustainability
SocialSustainability
3. Sustainable Healthcare Architecture as a holistic, integrated design outcome/solution
2. Integrated Design Approach
Team Formation and OrganizationMindset ChangeIntegrated Design Process
Project VisioningObjective SettingDesign IterationConstruction & CommissioningPost Occupancy Feedback Loops
Tools & Techniques
Design Problems
Design Process
Design Solution

62
2.4 Discussion: The Aspects of Integrated Design Process to be
Investigated
In Section 2.1 of this chapter, by drawing from literature, the definition of integrated
design approach has been defined. It is then followed by Section 2.2, in which its
relevance and benefits to the design of healthcare architecture is presented. Section 2.3
presents the essential elements of the integrated design approach (Figure 2.3). Following
that, Section 2.3.3 focuses on the integrated design process, which contains the following
important stages, with stage 1 to 4 being the focused study areas of this dissertation:
1. The formation and organization of the multi-disciplinary team;
2. The visioning process;
3. The objective setting process;
4. The design iteration process;
5. Construction and commissioning process;
6. Post occupancy feedback loops.
In summary, this chapter presents a model of the integrated design approach in theory.
Most of the IDP literature acknowledged that the IDP model needs to be tailored to real-
world constraints faced in practice (WSIP, 2007; IDP Roadmap, 2007). KTPH, purported
to be an example of sustainable healthcare architecture in the Singapore context, provide
a case to examine integrated design in practiced, to be compared to the theoretical
model. The comparison will be carried out in the next two chapters, starting with
Chapter 3: Briefing introduction of the KTPH project, followed by its visioning, objective
setting and briefing process.
63
Chapter 3.0: Khoo Teck Puat Hospotal:
The Case Study
“I posed the challenge to the AH rebuilding team: build
a hospital…designed with patients unambiguously at
the centre of the focus, with technology fully exploited
for the benefit and convenience of patients…. It will be
a hospital which is well linked… and to which the
patients can be transferred seamlessly… It will be a
hassle-free hospital.”
Khaw Boon Wan,
then Minister of Health, Singapore
“Exterior landscaped spaces on the ground of
healthcare facilities have become widely referred to as
healing gardens…These spaces afford respite, and
hiatus, however brief, from the day-to-day stresses of
the hospital.”
Stephen Verderber

64
Chapter 3.0 Khoo Teck Puat Hospotal: The Case Study
Section 2.3.3 provides a theoretical model of the integrated design process. This chapter
compares the visioning and objective setting process between theory and in practice by
using KTPH as a reference. It begins by providing the basic background of the KTPH
project, followed by an examination of the KTPH visioning and objective-setting
exercises. This is done through a comprehensive study of the literature and project
document, as well as through interviews with the key project team members involved.
This chapter then discusses the findings.
3.1 Background
As of 2011, there are eight public hospitals in Singapore, with Khoo Teck Puat Khoo Teck
Puat Hospital (KTPH) being the latest addition. The KTPH is a 550 bed acute care public
hospital offering a comprehensive range of medical and health services, situated in the
North to serve more than 700,000 residents in the region. (KTPH Website).
The KTPH design was developed from the winning entry selected from an international
design competition. The winning design was an outcome of collaboration by a design
consortium led by CPG Consultants Pte Ltd (CPG) from Singapore with many multi-
disciplinary team members (Appendix IV). CPG is the firm where this dissertation
author is currently working in. The author had no involvement in the KTPH project, but
by way of access to personnel involved in the project and unpublished document, it
facilitated the investigation of KTPH’s design process, which may be difficult for
someone from outside the organization. Expressed consent was given by CPG as well as
personnel interviewed in this project for the information published in this document.
3.2 KTPH’s Site Context
Situated in the northern Yishun town, the KTPH site is within walking distances to the
town amenities: Yishun Town Centre, Yishun MRT Station, Yishun Bus Interchange,
Yishun Town Park. It is adjacent to the existing Yishun Polyclinic, Yishun Pond, and a
planned site for a future community hospital (Figure 3.1). Across the Yishun Central
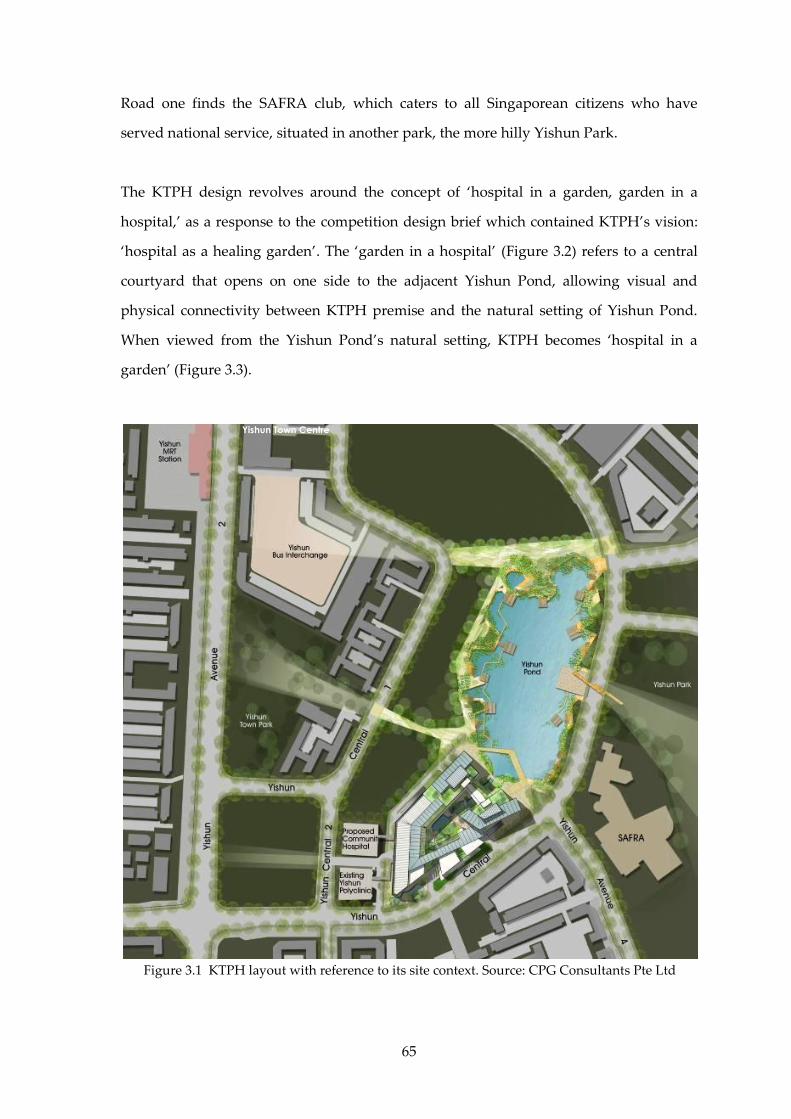
65
Road one finds the SAFRA club, which caters to all Singaporean citizens who have
served national service, situated in another park, the more hilly Yishun Park.
The KTPH design revolves around the concept of ‘hospital in a garden, garden in a
hospital,’ as a response to the competition design brief which contained KTPH’s vision:
‘hospital as a healing garden’. The ‘garden in a hospital’ (Figure 3.2) refers to a central
courtyard that opens on one side to the adjacent Yishun Pond, allowing visual and
physical connectivity between KTPH premise and the natural setting of Yishun Pond.
When viewed from the Yishun Pond’s natural setting, KTPH becomes ‘hospital in a
garden’ (Figure 3.3).
Figure 3.1 KTPH layout with reference to its site context. Source: CPG Consultants Pte Ltd
Yishun Town Centre
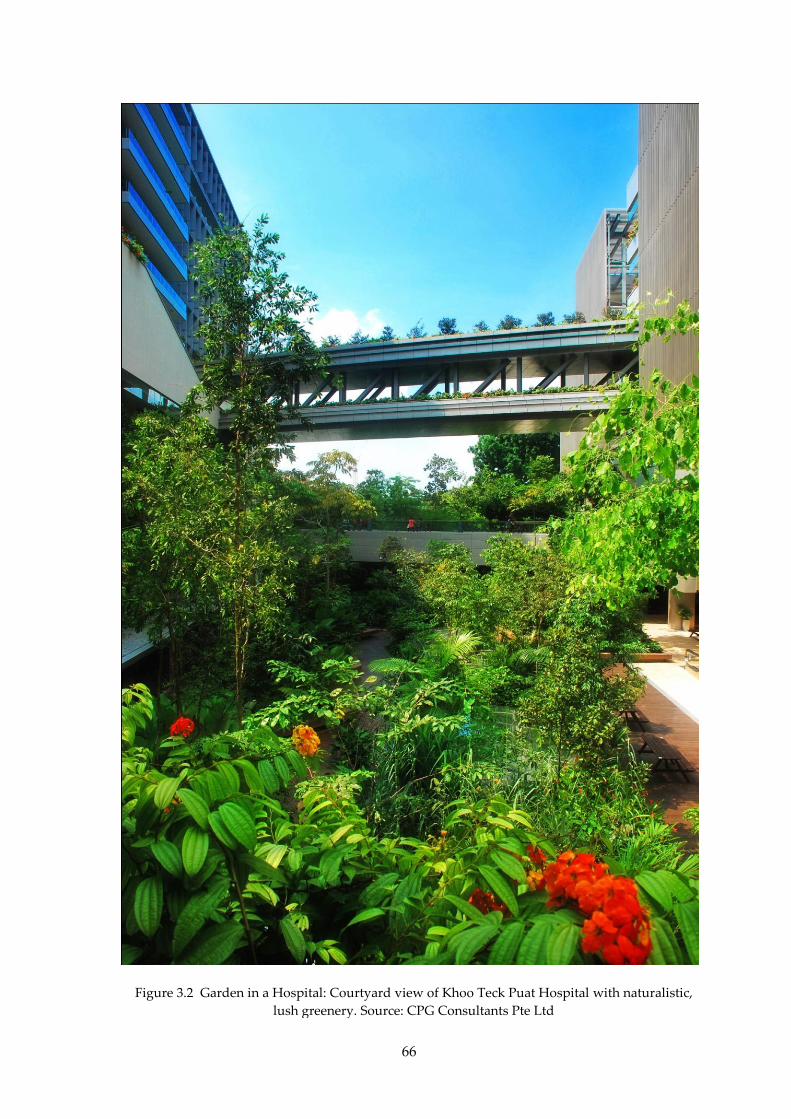
66
Figure 3.2 Garden in a Hospital: Courtyard view of Khoo Teck Puat Hospital with naturalistic,
lush greenery. Source: CPG Consultants Pte Ltd

67
Figure 3.3 Hospital in a Garden: View of Khoo Teck Puat Hospital across Yishun Pond
Source: CPG Consultants Pte Ltd
Figure 3.4 Integration of healthcare, social, and natural environments.
Source: Design document, CPG Consultants Pte Ltd
YISHUN TOWNCENTRE, TOWN PARK, MRT STATION, BUS
INTERCHANGE
SAFRA/YISHUN
PARK
‘Garden in a
Hospital’ as
Community Space
HDB ESTATES
Public and
shuttle arrival/
drop-off
Physical
integration of
green and
social
environments
View towards
Yishun Pond and
Yishun Park to
engage nature
68
KTPH’s landscaped environment not only provides the setting of ‘healing gardens’ for
the well-beings of its patients and staff, it also lends itself to the Yishun community,
enhancing the opportunities for social and community interaction through the spatial
integration of the hospital and external landscaped environments (Figure 3.4).
In Section 3.3, KTPH’s visioning, objective setting and briefing process is be presented
and compared to the visioning and objective setting in the integrated design approach
presented in chapter 2.
3.3 KTPH Visioning, Objective Setting and Briefing Process
In the integrated design process, it is essential that the project establish clear vision to
align team members’ mindsets, attitude (as discussed in Section 2.3.2 and 2.3.3) and
commitment to align with the common purpose and shared values. This section
examines the rigour and commitment by KTPH in its visioning and bar-raising objective-
setting exercises; and how these have served as the navigation beacons to guide the
integrated project team’s design outcome.
3.3.1 Methodologies: Focused Group Discussions and References
Focused group discussions were conducted with the KTPH project team members who
were involved in the project, either individually or in groups, over one or more sessions.
The discussions were made with reference to the IDP model (see Appendix IV on
discussion guide), and the project document made available to this dissertation author.
The use of the reference to IDP model is to ensure that the definition and mutual
understanding of the ‘integrated design approach’ is as close as possible to that defined
in this dissertation. The objective of the discussions and reference to the project
document is to identify similarities and deviations between KTPH’s design and work
processes in contrast to the IDP model. The project team members involved in the
focused group discussions are shown in Table 3.1

69
3.3.2 The Shared Visions
Back in 2004, when the decision to build the KTPH was made, the vision was first set by
Minister of Health Khaw Boon Wan (Liak, 2009):
I posed the challenge to the AH rebuilding team19: build a hospital… designed
with patients unambiguously at the centre of the focus, with technology fully
exploited for the benefit and convenience of patients…. It will be a hospital which
is well linked… and to which the patients can be transferred seamlessly… It will
be a hassle-free hospital.
In short, it was to be patient-centric. The challenge was taken up by the KTPH
management and staff, led by the visionary and determined CEO Liak Teng Lit, who
“had a tremendous impact in shaping the planning and operations of KTPH as well as
the organizational culture (Wu, 2011, p. 106). Under his leadership, and through working
together as a team in Alexandra Hospital since 2000, KTPH’s hospital planning
committee (HPC), comprising eight key members representing the hospital management,
19 KTPH was taken over by the management and staff from the Alexandra Hospital, while the
original Alexandra Hospital premise was transferred to JurongHealth in 2010. See History of
Alexandra Hospital. Available at <http://www.alexhosp.com.sg/index.php/about_us/our_history>.
Table 3.1 Key project team members involved in focus group discussions
(See also Appendix II)
Role Name Company
AH/KTPH Hospital Planning Team Donald Wai Alexandra Health/
Khoo Teck Puat Hosiptal
Project Director/Architect Lee Soo Khoong CPG Consultants Pte Ltd
Architect Lim Lip Chuan CPG Consultants Pte Ltd
Architect Jerry Ong CPG Consultants Pte Ltd
Architect Pauline Tan CPG Consultants Pte Ltd
Civl & Structural Engineer Soon Chern Yee CPG Consultants Pte Ltd
Mechanical Engineer Toh Yong Hua CPG Consultants Pte Ltd
Electrical Engineer Wong Lee Phing CPG Consultants Pte Ltd
Green Building Consultant Dr Lee Siew Eang Total Building Performance Team
Green Building Consultant Dr Nirmal Kishnani CPG Consultants Pte Ltd
Landscape Consultant Glenn Bontigao Peridian Asia Pte Ltd
Quantity Surveyor Yeo Tiong Yeow CPG Consultants Pte Ltd

70
a representative from Ministry of Health, as well as sixteen staff-in-attendance (HPC
Minutes of meeting dated 13.01. 2010), had developed a set of shared values as presented
in Table 3.2.
The above findings validated the emphasis in the integrated design approach to have
clear project vision from the start. In the case of KTPH, the CEO appeared to have played
the role of a sustainability ‘champion’ (IDP Roadmap, 2007; Section 2.3.3.1) in the early
stages, aligning the values and mindsets of the HPC and staff members.
Table 3.2 AH/KTPH Shared values
S/No. Name
1.
CEO Liak’s personal philosophy viewing “sustainability as an integral way of life,”
and his vision in promoting “sustainability as a lifestyle to his staff and the
community” (Liak, 2009, p. 107).
2. CEO Liak’s belief that in “a food resource-constrained world… his hospital needed to
do their part through urban agriculture” (Ibid, p. 107). As an outcome, KTPH
management teamed up with retired farmers in the community to volunteer and take
ownership of the roof top farm (Ibid, p. 107; Section 3.5.1)
3. Managers keep abreast with latest trends in healthcare and management issues (Ibid,
p. 106-107).
4. Patient-centric focus had become a shared vision among KTPH management and staff
(Ibid, p. 107). This was carried out through a series of pilot projects even while
operating at the Alexandra Hospital premise (DSC Case Study, 2009) . The initiatives
include “shorter waiting time, access to better information, and savings on medical
bills.” (Ibid., p. 2) The management tools and philosophies adopted include “the
Toyota Production System (TPS) and Six Sigma to help improve the hospital’s
workflow and efficiency” (Ibid., p. 6). “AH also learned from leading organizations in
various industries including hospitality, airlines, finance, and manufacturing” (Ibid.,
p. 6).
5. Emphasis of energy efficiency and the use of natural ventilation to reduce energy
consumption (Wu, 2011, p. 109).
6. Enthusiastic staff e.g. Rosalin Tan that believes in increasing “the indigenous wild life
biodiversity by introducing native species of plants in the hospital’s landscaping.”
(Ibid, p. 109)
7. A believe in hospital as a healing environment in accordance with Erik Asmussen’s
seven principles: unity of form and function, polarity, metamorphosis, harmony, with
nature and site, living wall, color luminosity and color perspective and dynamic
equilibrium of spatial experience (Ibid, p. 110-111).
8. Ulrich’s theory of supportive design (Ibid, p. 111), which is the domain of the
evidence-based design, presented in Section 1.6.2.

71
3.3.2 Setting the Objectives
Visions need to be translated into specific project objectives for targeted actions. In an
interview with Dr Lee Siew Eang 20 , who assisted KTPH in developing the project
objectives, he stated that the total building performance (TBP) approach was adopted to
develop the project objectives. The TBP approach was developed by Public Works
Canada between 1981 and 1985, and promoted by Hartkopf and Loftness as a framework
to measure building performance (Hartkopf and Loftness, 1999; Harkopf et al, 1986). It
focuses on integrating six key qualities of a building, namely spatial quality, thermal
comfort, acoustic quality, indoor air quality, visual quality, and building Integrity, with
reference to not only economic and building performance, but human physiological,
sociological, and psychological needs (Ng, 2005; Table 3.3). It is interesting that in TBP
approach, considerations which contribute to social sustainability are given under the
‘Spatial quality’ criteria, with qualitative attributes such as ‘beauty’, ‘calm’, ‘excitement’,
‘view’, etc. Set up in 2000, the Centre for Total Building Performance (CTBP), a joint
research centre by NUS and the Building and Construction Authority (BCA), adapted
the TBP approach21 to the Singapore context, with an aim to develop it into a design
guide that is “first, an objective and comprehensive matrix, second, is user-oriented by
incorporating building performance mandate agreed with users, based on building
performance benchmarks obtained from existing buildings. It therefore encapsulates
both a measurable, life-cycle performance indicators that is also user-driven and
performance-based,” said Dr Lee in the same interview, “and after the KTPH TBP matrix
had been developed, the Green Mark Platinum requirements were then slotted into the
TBP matrix”(Interview in January 2012).
20 Interview session was held in January 2012. Dr Lee Siew Eang is Director, Centre for Total
Building Performance (CTBP). CTBP is a Joint BCA-NUS Centre for Tropical Building Research,
School of Design and Environment. Dr Lee is also an Associate Professor in Department of
Building, School of Design and Environment, National University of Singapore, with research
interest in building performance and acoustics. 21 Other projects in Singapore developed under the TBP approach include The Urban
Redevelopment Authority Centre of Singapore and the National Library Building (NLB) of
Singapore.

72
By basing on the TBP approach, the KTPH HPC organized the visions into a set of thirty-
one objectives, grouped under nine categories (AH tender brief for design competition,
2005). This became the design requirements for the design competition. In order to make
a comparison between the TBP approach and the triple bottom line approach, these
objectives are mapped against the three sustainability dimensions of economic, social
and environmental/ecological, as shown in Table 3.4. While the design competition brief
was not explicit, the mapping revealed that all three sustainability dimensions of
economic, social and environmental were considered.
Table 3.3 Organizing performance criteria for evaluating the integration of systems (Hartkoft
and Loftness, 1999)
Specific
Performance
Criteria
Physiological Needs Psychological Needs Sociological Needs Economical
Needs
1 Spataial
Ergonomic Comfort,
handicapped access,
functional servicing
Habitability, calm,
excitement, view
Wayfinding,
functional adjacencies
Space
Conservation
2 Thermal
No numbness,
frostbite; no
drowsiness, heat
stroke
Healthy plants, sense
of warmth, individual
control
Flexibility to dress
with the custom
Energy
Conservation
3 Air Quality
Air purity; no lung
problems, no rashes,
cancer
Healthy plants, not
closed in, stuffy; no
synthetics
No irritation from
neighbours, smoke,
smell
Energy
Conservation
4 Acoustical
No hearing damage,
music enjoyment,
speech clarity
Quiet, soothing;
activity excitement
‘alive’
Privacy,
communication
5 Visual
No glare, good task
illumination,
wayfinding, no
fatigue
Orientation,
cheerfulness, calm,
intimate, spacious,
alive
Status of widnow,
daylit office, ‘sens of
territory’
Energy
Conservation
6 Building
Integrity
Fire safety; structural
strength and stability;
weather tightness, no
outgassing
Durability, sense of
stability, image
Status, appearance,
quality of
construction,
‘craftsmanship’
Material/
Labour
Conservation
General
Performance
Criteria
Physical Comfort
Health
Safety
Functional
Psychological
Comfort
Mental Health
Psychological Safety
Esthetics
Privacy,
Security,
Community,
Images/Status
Material,
Time,
Energy,
Investment
73
At this stage, the alignment of values was confined to mainly the medical professionals,
with the assistance of Dr Lee and his team. The value alignment with the building
professionals has not yet been carried, because they are yet to be appointed. As a public
commission funded by government, it was necessary for KTPH’s project consultancy to
be procured through public tender. In an interview with Donald Wai, a key member of
the KTPH HPT, he said that it was decided very early on that an integrated design team
was needed for the KTPH project. This decision was in part informed by their previous
hospital planning experience in an attempt to relocate the Alexandra Hospital operation
to another site in Jurong, and in part to meet the very tight project schedule to complete
KTPH. The requirements for the formation of an integrated design team and the
provision of the integrated design proposal were hence specified in the design
competition. A 2-stage design competition was held, based on the quality-fee method
(QFM; BCA22), in which shortlisted design consortium after Stage 1 proceed to submit
design and fee proposals in Stage 2. In the Stage 2 award evaluation, both the quality of
the design proposal and the total consultancy fee were taken into account, based on a
predetermined weightage between quality and fee.
After the conclusion of the design completion, KTPH selected the winning design
submitted by the CPG-led consortium, and appointment the design consortium in May
2006. A visioning session was soon organized, to align the shared visions and to set the
objectives for the whole project team. The KTPH visioning and objective setting process
thus validated the IDP’s emphasis on aligning values and mindset. At this stage, the
KTPH visioning and objective setting process as advocated in the IDP had been carried
out in manner that suited Singapore and AH/KTPH.
The formation and organization of the multi-disciplinary building consultant team, and
its working relationship with the KTPH HPC and user group is presented in the next
section.
22 “QFM Framework”, BCA Website. Available at: <www.bca.gov.sg/PanelsConsultants/others/
QFM_Framework.pdf>

74
Table 3.4 Framing the sustainability focuses in KTPH’s brief for design competition (AH,
2005), with sustainability attributes added by author.
S/No. KTPH’s brief for design competition Eco Soc Env
1. A hassle free hospital:
a. Patients shall be at the centre of the focus, with technology fully exploited for
the benefit and convenience of the patients.
b. It will be well-linked, and patient transfer will be seamless.
2. Adopt a ‘Tricycle Model’: The three thrusts of patient care, teaching &
sharing, and learning & research will mutually support one another.
3. A hospital for the future:
a. It is to be visually pleasing that sustains with time.
b. Ensures ease and low cost of maintainability.
4. Design scalability:
a. Designed for flexibility and adaptability.
b. ‘Breathability’ in master planning.
c. Modular design for ease of conversion.
d. Ability for lock-down of the hospital by zone during emergencies.
5. Patient centric:
a. Hassle-free processes designed for patients’ convenience.
b. Engaging patients and their families as partners.
c. Safety of patients is of paramount importance.
d. Intuitive, ease of moment for patients and visitors.
e. Minimal movement required for patients.
f. Clustering of services and facilities.
6. Technology as an Enabler: Better, faster, cheaper and safer healthcare
through digitisation, wireless technology, automation and robotics.
7. Energy Efficient:
a. 50% More energy efficient than existing hospitals.
b. Designed to with the tropical climate in mind.
c. Harness natural ventilation.
d. Allow for ample overhangs.
e. Designed for high ceilings.
f. Make use of solar and wind power.
g. To achieve Green Mark Platinum Award.
8. High Touch:
a. To have a warm, ‘cuddling’ feel.
b. Environment to be calming and cheerful.
c. Sensitive to the different age group of patient population, catering both to
the vibrant young and the mature aged.
9. Healing Environment:
a. Hospital within a garden, garden within a hospital.
b. Environment to have tranquil, restful, and healing qualities.
c. Users are in touch with the sight, scent and sound of nature.
d. Surrounding patients with nature, e.g. through roof garden, hanging gardens
at verandahs.
e. Replacement ratio of 0.7 or more for greenery.
Eco = Economic Sustainability
Soc = Social/Human Wellness Sustainability
Env = Environmental/Ecological Sustainability

75
3.4 KTPH Team Formation and Organization
Based on the individual and focused group discussions conducted with the project team
members, the organization chart of the original KTPH team organization was reflected in
a hierarchical manner similar to Figure 2.5. This is due to the fact that in the building
industry that is the commonly accepted way organizational charts are drawn. When
presented with alternative diagramme of integrated design team organization (Figure
2.6), all project team members interviewed agreed that Figure 2.6 indeed better reflects
the KTPH team organization. Based on the findings of the focused group discussions, a
KTPH integrated design team organization chart (Figure 3.5) is prepared to reflect the
manner in which KTPH project team was organized. In Figure 3.5, building professionals
are shown in green, and communication among them was facilitated by the CPG
architects. The medical professionals are shown in blue, and communication among
them was facilitated by the HPT. The Core Project Team (CPT) comprises Architect,
prime consultant team, KTPH HPT, project manager and often includes landscape
architect and green consultant.23
23 Document from CPG file archive and information from interview sessions with Ong, Lim, Toh,
and Bontigao between Dec 2011 and Jan 2012.
Figure 3.5 KTPH’s integrated design team organization. By author, adapted from IDP Roadmap (2007).
ArchitectCPG
Cost Consultant/Quantity Surveyor
CPG
Interior DesignerBent Severin
Main ContractorHyundai
Green Mark Authority
BCA
Regulatory Authorities
Other government
agencies, planners, etc
Hospital PlannerRMJM Hillier
Façade Consultant
Aurecon
Landscape ArchitectPeridian
Green Consultant
TBPT
IDP Facilitator?
OperatorKTPH HPT
Project ManagerPMLink
Prime Consultant Team: Mechanical, Electrical,
Structural, Civil Engineers
CPG
User Work Groups/Departments
KTPH User Reps
ClientMinistry of Health
Representative
KTPH ManagementKTPH HPC
Wayfinding/Signage
Space Syntax/Design objectives
Core Project Team

76
Through the focused group discussions, it was revealed that while the project team
members intended to undertake design and the project in an integrated manner, they
were not aware and hence did not make use of any specific integrated design process
methodologies, such as those identified in Chapter 2.0. They were therefore very much
self-reliant, basing on past experience, as well as constantly making adjustment to the
group dynamics that was evolving and developing through working on the KTPH
project. The group dynamics began to mature as the project develops, and was stabilize
after about six months since the formal appointment of the consultants in May 2006. As
the appointment of the consultants did not make IDP a prescribed requirement, the fee
structure is similar to the traditional design approach. In other words, the fee structure
did not anticipate the rigour of the IDP. Hence throughout the project, the project team
had to adapt to the IDP practice while operating under the financial pressure of a
conventional fee structure similar to typical large scale projects in Singapore.24
The roles of the key members of the KTPH Integrated design team are discussed in 3.4.1
to 3.4.6.
3.4.1 The role of IDP Facilitator
One key difference between the KTPH integrated design team and Roadmap (2007) is
the lack of a formerly appointed champion or facilitator. While KTPH’s CEO Mr Liak
Teng Lit was the defacto leader in championing sustainability issues as outlined in
Section 3.3.2, and availed himself in many of the workshops or small group meetings, he
could not be considered as an IDP champion. Understandably so, as first, a specific IDP
methodology was not consciously adopted; second, it was never a practice in Singapore
for such a role. The prevailing practice was for the architect to act as the lead consultant
to co-ordinate the efforts of the consultant team, or for the large and complex project, for
a project manager to be appointed to act on behalf of the client to oversee the project
matters. For KTPH, the project team members recounted that the integrated design
24 Document from CPG file archive and information from interview sessions with Ong, Lim, Toh,
and Bontigao between Dec 2011 and Jan 2012.

77
efforts do require facilitation, and through group consent that the facilitation
responsibilities were taken up and shared among the CPG architectural team, the KTPH
HPT, and the PM Link project management team. The architectural team members
focused on facilitation among the building professionals. The HPT focused on liasison
and coordination with the many user work groups and hospital departments. The
project manager team focused on work programming, people management and
scheduling which is typical of what project managers do in Singapore. The roles of the
project team members that played key roles to the integrated design process are
presented below.25
3.4.2 The role of the Architect + IDP Facilitator for Building Design
For KTPH, a 10-member architectural team was deployed by CPG, including the project
director Mr Lee Soo Khoong, architects Lim Lip Chuan, Jerry Ong and Pauline Tan who
were interviewed in focused group discussions for this dissertation. They worked in
collaboration with healthcare architectural consultant RMJM Hillier, and are supported
by medical planner Medical Planning Research International and other architectural
support staffs. Hence, team-based design was an important attribute in the architectural
design process.26
As the lead consultant, the CPG architectural team leads the building professionals in
engaging the HPT and the user representatives, as well as the building authorities. They
put in lot of efforts to facilitate inputs and requirements from different parties to be
tabled early, so as to seek opportunity for more holistic solutions. They also have to be
open to new ideas, possess good listening skills, and the willingness to learn and
develop an understanding of healthcare operation, needs and requirements of healthcare
staff, as well as the needs and requirements of patients, families and public visitors.
25 See Appendix IV for list of personnel. 26 Ibid.

78
Some of the difficulties encountered by CPG architects were the initial communication
problems with non-building professionals, e.g. even when both parties were reading the
same drawings, the interpretation and spatial understanding of clinicians and the
architect may be different. As a result:
1. Extra time spent and additional efforts were hence needed in order to ensure that
a common understanding was attained.
2. Non-building professionals did not have a full understanding of the constraints
and complexities in building design and contract implementation. Certain design
ideas that they had preferred may be constraint by other requirements, and
usually alternative, work-around solutions proposed by the building
professionals are required. Intense and pro-longed user group meetings
involving co-learning were hence necessary. On the other hand, the intense
meetings had also built trust and understanding among building and medical
professionals.
3.4.3 The role of the Hospital Planning Team + IDP Facilitator for User
Groups
The 9-member hospital planning team (HPT)27 is the bridge that straddles between the
building design/project team and the hospital management represented by the Hospital
Planning Committee (HPC) and user committees. Led by the Chief Operating Officer
Chew Kwee Tiang 28 and deputized by Donald Wai, the HPT comprises clinicians,
managers and administrators (AH org chart dated 09.01.2009) who would liaise with
various departments and work groups.
27 The HPT initially comprises Director, Hospital Planning Chew K. T., Deputy Director Donald
Wai who oversee day-to-day hospital planning issues with focus on contract administration and
facilities management, Koh Kim Luan, Sim Siew Ngoh and Esther Yap in the early stages. Cynthia
Ong, Lye Siew Lin, Poh Puay Yong joined the project and HPT in later stages. All were involved
in specific departments based on their background. They help to bridge between the users and
consultants, were involved in NSC tenders (ID, fitment, loose furniture tenders etc) and site
coordination (Based on interview with CPG Architect Jerry Ong in Jan 2012 and AH org chart
dated 09.01.2009). 28 The role was performed by Grace Chiang up to the masterplanning stage, but later taken over
by Chew after that and through to completion and building operation.
79
The HPT organized a few types of meetings/workshops:
1. The monthly HPC meetings, in which inter-departmental issues, policy issues
and management issues were raised for decision making. Annotated agenda for
each HPC meeting was submitted to the participants, and key decisions were
made timely to facilitate the design process. In addition, the latest trends in
medical process, procedures and (operation) were also presented in the meetings,
and hard decisions were made decisively to incorporate some proposals into the
final design and facilities.
2. A one-week workshop was conducted once every month (User group design
workshop) during the schematic and design development stages. Altogether,
approximately fifteen such design workshops were conducted.
3. Working sessions were conducted in between the workshops involving specific
user representatives from different departments and building professionals to
follow up on issues identified in the workshops. In these working sessions,
architect, the prime consultant team (civil & structural engineer, mechanical
engineer, electrical engineer) were always represented, and selected specialist
consultant e.g. green consultant, landscape consultant, interior designer and
signage consultant were frequently present, particularly when their inputs were
required.
3.4.4 The role of the Prime Consultant Team
The Civil & Structural Engineers, Mechanical Engineers, Electrical Engineers were from
the same company as the architect, i.e. CPG Consultants Pte Ltd. This helped to reduce
potential hurdles that may impede close collaboration between the disciplines that are
from different companies, e.g. sharing of information. By being co-located in the same
building, the physical proximity between the various disciplines had also facilitated the
face-to-face interaction and design collaboration. Despite that, the focused group
discussions had also revealed that the habits developed from the entrenched linear and
fragmentary industry practices was hurdles that require persistent efforts to overcome.

80
3.4.5 The role of the Green Consultant
The CPG team was supported by its in-house green studio, CPGreen, headed by Dr
Nirmal Krishnani29 at that time during the early research stage of the design competition.
The Green Consultant role was taken up by Total Building Performance Team (TBPT)
during the design competition. They are familiar with the then new Green Mark
requirements, and provided the design team with support on climate analysis, energy
modeling, life cycle cost estimation, computational fluid dynamic (CFD) simulation, and
wind tunnel test. By utilizing these tools, TBPT worked with CPG architect and engineer
in achieving energy efficiency through integrating:
1. The bioclimatic responds of the building envelope, reducing the cooling load,
taking in considerations of view, day light and aesthetics;
2. Optimized air-conditioning and mechanical ventilation (ACMV) system, e.g. heat
recovery system, CO2 sensor, and other energy-efficient systems e.g. lighting,
transportation, etc.
Dr Lee Siew Eang who headed the TBPT recounted30 that initially, the engineers were not
comfortable providing design information to the TBPT. The trust gradually built up after
a few months, with TBPT making it a point to always return to the engineers to discuss
their findings, before they would jointly present the outcomes or proposals to the
HPT/user groups.
3.4.6 The role of User Groups
Prior and throughout the project, some twenty-plus user groups were formed e.g.
clinicians from various departments, hospital support, administration and facilities
management groups (Table 3.5). Generally, these user groups would first conduct their
own work flow studies, benchmarking practices from the best-in-class, propose system
29 Interview session with Dr Nirmal Krishnani held in December 2011. Dr Nirmal is currently
Senior Lecturer at National University of Singapore, as well as Chief Editor of Future Arc journal. 30 Interview session held in January 2012.

81
improvements, and translate these into design and spatial requirements for discussion
with the architect and the prime consultant team. These working sessions are facilitated
by the HPT and the PM Link project managers.
3.4.7 The role of the Contractor
The main contract was procured using the conventional design-bid-build method, and
hence the main contractor M/s Hyundai Engineering & Construction Co Ltd were on
board only after the award of the main tender, and was not able to participate in the
integrated design process. The project team experienced some coordination issues
during construction stage, which affirms the view that there is a disconnect between
design and construction professionals (7group and Reed, 2009, p. 10; Section 2.1).
3.5 Discussion: KTPH’s Visioning, Objective Setting and Team
Formation
Even without relying on any structured integrated design methodology or guide,
through document review and focused group discussion, it was found that the KTPH
project had by and large put in place the following essential elements of the integrated
design process:
Table 3.5 AH/KTPH user work groups / departments (AH org chart dated 09.01.2009)
Call Centres MOT Project Development
CD HPVF Offices Construction Progress & Site Mgt
Childcare Centre OSMH Technical
Day Surgery Pharmacy Infrastructure & IT
DEM PSC/IPC Archt & Struct. Design Review
Delivery Suites & NICU Radiotherapy Community & Grassroot Relation
DI Renal Unit AH Facilities & Migration Plan
Endoscopy SOCs Liason with authorities & MOH
ICUs (Surgery & Medical) Staff Facilities Fire Command Centre
Laboratories Toilets Yishun Pond
Lobby & Retail Wards (Private, subsidized, iso)

82
1. Formation of multi-disciplinary, integrated project team that comprises not only
building professionals, project manager, green design consultant, and other
building specialists, but also medical professionals, organized as user groups;
2. Robust visioning and objective setting processes were carried out, through the
application of total building performance framework, which was customized to
suit Singapore’s context.
With the integrated design team, the visions and objectives in place, it remains to be seen
how the integrated design process and iterations were played out. This is examined in
the next chapter.

83
Chapter 4.0: KTPH’s Integrated
Design Process
“This requires rethinking principles and
procedures at a higher level of generality. It
would mean changing routines and old ways
of doing things. It would require a
willingness to accept the risks that
accompany change.”
David Orr
“Part of the charrette process lies in knowing
that a good idea can come from anyplace.
You have to be willing to accept it. It dosen’t
matter where the idea comes from.”
Dan Heinfeld

84
Chapter 4.0 KTPH’s Integrated Design Process
This chapter examines KTPH’s design process. The objective is to compare and contrast
the integrated design process in theory and in practice. Three aspects are focused on:
1. The alternation between research/analysis and workshop;
2. The iteration process in each stage, namely ‘prelim’ (PD), ‘schematic design’ (SD),
and ‘design development’ (DD);
3. Some examples of the multi-disciplinary collaboration in the iteration process, the
role that the different professionals or experts played, and the contributions they
made.
The methodology includes, first, by mapping out the KTPH’s design process, focusing
on the alternating patterns of research/analysis and workshops. It is then compared with
the IDP theoretical model, followed by a discussion. Next, examination of the iteration
processes are conducted through the various stages: design competition stage, schematic
design stage and design development stage. During the examination, the tools and
techniques employed to support integrated design decisions are highlighted. Particular
focus is drawn on the two salient features of KTPH: the biophilic site layout and massing
design that was developed in the early design stages, and the bioclimatic and naturally
ventilated subsidized ward design that was developed in the later design stages. The
examination is done through a comprehensive study of the literature and project
document available, as well as through focus group discussions with the key project
team members involved (Table 3.1).
4.1 The Process Map
Based on the focused group discussions, the integrated design process of KTPH is
mapped out in Figure 4.1. For ease of comparison, the IDP theoretical model in Figure
2.8 is reproduced in Figure 4.2. The alternating patterns of workshops and
research/analysis activities are quite similar between the KTPH process and the IDP
theoretical model, but the two starts to deviate during the schematic design stage. The

85
main activities that took place during the various stages in the process map are
summarized in Table 4.1.
4.1.1 DC: Design Competition (Prelim)
The initial research/analysis stage ‘R1’ in the theoretical IDP model (Figure 4.2) is
undertaken as the design competition stage ‘DC’ in the KTPH (Figure 4.1). The design
proposal put forward by the design team (See Figure 4.3) is indeed an attempt to address
the design requirements and objectives (problems/constraints) through solution finding
(Lawson, 2005). As the design competition was conducted in two stages, feedback given
to the design team after the first presentations was given due considerations and an
improved design was put forth in the final submission. At this stage, the design concept
revolving around the notion of ‘hospital in a garden, garden in a hospital’ that
Figure 4.1 Integrated design process in KTPH. Adapted from WSIP (2007).
Figure 4.2 The Theoretical model of integrative design process. Adapted from WSIP (2007).
Decision Workshops
WorkshopsKTPH Integrated Design Process
CDDC MP SD DD1
Prelim Masterplan SD DD CD T&A
DD2
W2W1
S1 VE1 VE2 S2
R2R1 R3 R4
W1 W2 W3 W4 W5 W6 W7

86
responded to the competition design brief was established. The design integrated inputs
and basic considerations from various consultants, including (CPG’s file archive):
1. Architectural and medical planning
2. Interior design
3. Wayfinding
4. Mechanical and electrical engineering design
5. Civil and structural engineering design
6. Transportation and traffic studies
7. Costing and budget
8. Total building design and green design
9. Landscape design
10. Security design
11. Acoustic design
The design led to the successful award of the design competition and the formal
appointment of the consultant team. KTPH HPT’s Wai recalled that one of the reasons
was the support of the design concept by objective data and analysis. For example,
during a design competition briefing, TBPT demonstrated by way of meteorological data
and computer simulation that by opening the courtyard towards the Yishun Pond, wind
is funneled through the courtyard to improve thermal comfort (Figure 4.12).
Figure 4.3 Integrated design team organization at the design competition stage. Adapted from
IDP Roadmap (2007).
Interior DesignerBent Severin
Landscape ArchitectPeridian
Green ConsultantTBPT/CPG
Prime Consultant Team: Mechanical, Electrical,
Civil, Structural Engineers, Quantity Surveyor
CPG
ArchitectCPG
Hospital PlannerRMJM Hillier
WayfindingSpace Syntax

87
4.1.2 W1: Visioning Workshop
In Section 3.2.2, it was presented that a visioning workshop was conducted soon after the
formal appointment of consultants. This is represented as ‘W1’ in Figure 4.1. During the
1-day visioning workshop, the KTPH key representatives and the building professionals
participated in a project chartering process, in which the project visions and objectives
were thought through, debated, and chartered with all participants committing to it by
signing off the charter. Architect Ong recalled, “It was emphasized to us that we are
KTPH’s ‘partners’ in realizing the hospital’s vision.”31
At this point, the project team had expanded to include both building professionals and
healthcare professionals in the Core Project Team, with other supporting building and
healthcare experts, as presented in Figure 3.5.
4.1.3 W2: Masterplanning Workshop
The visioning workshop (W1) was closely followed by a masterplanning workshop
conducted over four days, in which the programmatic requirements, the site planning,
the massing iterations were conducted through the use of sketches, simplified digital
massing studies, powerpoint slide presentations and verbal discussions. Drastic changes
were made to the programmatic arrangement, so as to better accpmmodate KTPH’s
‘integrated care’ operation philosophy.32
4.1.4 MP: Schematic Design Research/Analysis/Design Process
After the masterplanning workshop, the building professionals proceeded with the
design revision and iteration process. At this stage, preliminary design studies were
conducted to validate that the objectives set out in the visioning workshop were
achievable. This stage may be considered as part of the schematic design (R2) of the
theoretical IDP model. The stage was completed with the signing off of the revised
31 Interview session held in Dec 2011. 32 Document from CPG file archive and information from interview sessions with Ong, Lim, Toh,
and Bontigao between Dec 2011 and Jan 2012.

88
masterplan (S1), which took place after a presentation to HPC was made and
endorsement by HPC was obtained. The signing off was more for the purpose of
recognizing work done and billing for the building professionals. In terms of design
activities, the transition from masterplan to schematic design was an on-going process,
fuzzy process.33
4.1.5 SD: Schematic Design
Issues that required a more detailed level of resolution was brought into the schematic
design (SD) stage. During this stage, the block massing, spatial organization of
departments in relation to each other, was decided. More user groups (See Section 3.4.6)
were brought in to interact with the Core Project Team (CPT; See Section 3.4). The CPT
was usually represented by the HPT, architect, mechanical engineer, electrical engineer,
with other professionals e.g. landscape and interior designers joining in as and when
required. The user groups were coordinated and facilitated by the HPT and project
manager team. The user group meetings were typically a process of co-learning, where
the users would take the building professional through their specific operational
requirements, while the building professionals would explore design options while
explaining the constraints and considerations related to building design and
construction. As recounted by Architect Ong34, during this process, KTPH’s CEO Liak
Teng Lit would often attends the user group meetings for key decisions to be made,
especially pertaining to landscape and environmental sustainability issues, which are
very much his personal interests.35
4.1.6 VE1: Value Engineering Workshop
A VE workshop ‘VE1’ was conducted at the end of the schematic design (SD) stage. An
external facilitator was brought in by KTPH to facilitate the VE process. The different
33 Document from CPG file archive and information from interview sessions with Ong, Lim, Toh,
and Bontigao between Dec 2011 and Jan 2012. 34 Interview session held in Jan 2012. 35 Document from CPG file archive and information from interview sessions with Ong, Lim, Toh,
and Bontigao between Dec 2011 and Jan 2012.

89
options of the main building elements, e.g. link bridges, M&E design strategies, medical
service strategies, etc were presented, their pros and cons discussed, and at the end of
the VE workshop, decisions were made regarding which major design options were to
be selected.36
4.1.7 DD1 & DD2: Design Development
During the design development (DD) stage, there were two sub-stages. In DD1, internal
layouts of the individual departments were developed with the users. It was followed by
DD2, where the detailed room requirements were agreed, e.g. provision and locations of
equipment and services. Throughout the DD, the building professionals were essentially
developing the design into more specific systems and components, supported with
design tools such as calculations, simulations and metrics. Throughout this process, the
HPT and project manager would conduct interim reviews to check that the design
objectives were being met. In fact, as the design was being developed, many of the
objectives were also refined or updated. For example, as recounted by mechanical
engineer Toh Yong Hwa37, one of the KTPH’s objectives was ‘50% more energy efficient
than existing hospitals’. This was initially based on an assumption that 70% of the floor
areas were to be naturally ventilated, and the remaining 30% to be air-conditioned. As
the design developed, it was realized that even after optimization, 54% of the floor areas
were needed to be air-conditioned to meet operational requirements, and as a result the
energy saving target was agreed to be revised to 35%.38 The design development was
signed off (‘S2’ in Figure 4.1) for the preparation of the tender bid documentation. Again,
this was more meaningful for the recognition of work done and billing; the actual design
refinement continued well into the documentation phase.39
36 Document from CPG file archive and information from interview sessions with Ong, Lim, Toh,
and Bontigao between Dec 2011 and Jan 2012. 37 Interview session held in January 2012. 38 This was nonetheless a higher target than the minimum energy saving criteria of 30% for Green
Mark Platinum. 39 Document from CPG file archive and information from interview sessions with Ong, Lim, Toh,
and Bontigao between Dec 2011 and Jan 2012.
90
4.1.8 VE2: Value Engineering Workshop
A second VE workshop (VE2) was conducted in between DD1 and DD2, primarily to
decide on the façade screen design options generated. Again, an external facilitator was
appointed to facilitate the VE process. The different façade screening options were
presented and evaluated, and at the end of the VE workshop, decision regarding which
option to adopt was made. This is presented in Section 4.2.2.40
4.1.9 The Practice of Workshop/Design Charrette
From the above process map, it is observed that workshops were held frequently
throughout the project duration. CPG Architect Lim41 commented that hospital planner
RMJM-Hillier were familiar with the group design technique of ‘design charrettes’42
(Todd, 2009), which they frequently employed in their projects. For KTPH, workshops
were practice in part to overcome the constraints of working with RMJM-Hillier as a
foreign consultant, as the physical distance of their home office in the United States
means that it is impractical to hold weekly or bi-weekly meetings, a common practice in
Singapore. Instead, a focused one-week workshop where all key stakeholders are present
to be held on a monthly basis was more effective, and it had become an established
practice with the Singapore-based project team as well, even after RMJM-Hillier had
completed their main scope of works by DD1 stage and stopped participating on a
regular basis. KTPH’s Wai recounted that in between the main workshops involving key
stakeholders, many user group meetings to resolve design issues were needed. As many
of the users are clinicians and managers who had to perform duties during official hours,
it was necessary to conduct user group meetings with building professionals through
intensive mini-workshops, very often between 5pm and 10pm after working hours. Such
intense sessions were prevalent in the masterplanning and schematic design stages, but
40 Ibid. 41 Interview session held in January 2012. 42 Todd (2009) defined design charrettes in Whole Building Design Guide website as “a charrette
is defined as an intensive workshop in which various stakeholders and experts are brought
together to address a particular design issue, from a single building to an entire campus,
installation, or park.”

91
the intensity began to reduce in design development stage, as the design was
progressively resolved.43
4.1.10 Hospital Planning Committee Meetings that were held monthly
Not shown in the process map are the monthly HPC meetings, where the CEO, COO,
departmental heads, clinicians, nursing leaders and operation managers were
represented, as well as representative from Ministry of Health, which finances the
project. The interim solutions agreed between the user groups and the building
professionals in the workshops were presented in HPC meetings for endorsement. Issues
that could not be resolved at the workshops (e.g. inter-departmental conflicts, etc) or
opportunities for inter-departmental synergies (e.g. sharing of common resources, etc)
are identified in annotated agenda to be iterated in the HPC meetings for decision. On
the other hand, issues surfaced during the HPC meetings were also assigned to specific
user group working sessions for detailed study and/or resolution. While VE exercises
were not conducted as an on-going process as advocated in the theoretical model of IDP,
budget review was constantly conducted in the HPC meeting agenda.
While KTPH’s design process map somewhat deviated from the theoretical model of the
IDP, it has so far validated such recommendations (WSIP, 2007, see Table 2.4) as:
1. Fully engage client in the design decision process (WSIP, 2007).
2. Assemble the right team (WSIP, 2007), in the case of KTPH, this includes both
building professionals and medical professionals.
3. Key attributes in team formation is ‘teachable attitude’; members come on board
not as experts but co-learners (WSIP, 2007).
4. Align team around basic aspirations, a core purpose (a hassle-free hospital), and
core values (WSIP, 2007).
43 Document from CPG file archive and information from interview sessions with Ong, Lim, Toh,
and Bontigao between Dec 2011 and Jan 2012.
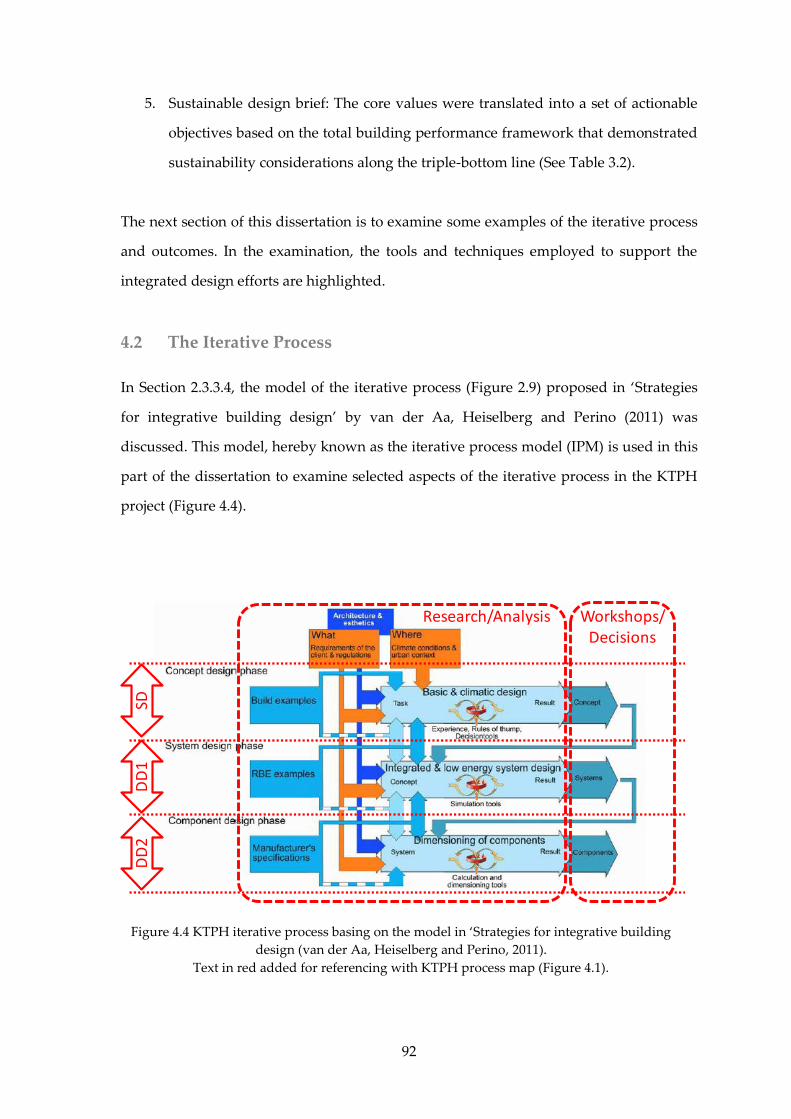
92
5. Sustainable design brief: The core values were translated into a set of actionable
objectives based on the total building performance framework that demonstrated
sustainability considerations along the triple-bottom line (See Table 3.2).
The next section of this dissertation is to examine some examples of the iterative process
and outcomes. In the examination, the tools and techniques employed to support the
integrated design efforts are highlighted.
4.2 The Iterative Process
In Section 2.3.3.4, the model of the iterative process (Figure 2.9) proposed in ‘Strategies
for integrative building design’ by van der Aa, Heiselberg and Perino (2011) was
discussed. This model, hereby known as the iterative process model (IPM) is used in this
part of the dissertation to examine selected aspects of the iterative process in the KTPH
project (Figure 4.4).
Figure 4.4 KTPH iterative process basing on the model in ‘Strategies for integrative building
design (van der Aa, Heiselberg and Perino, 2011).
Text in red added for referencing with KTPH process map (Figure 4.1).
SDD
D1
DD
2
Research/Analysis Workshops/Decisions

93
4.2.1 Schematic Design (SD) Stage
During the schematic design stage (known as concept design phase in IPM), broad
strategies were considered, including local climate (Ibid.), programmatic zoning,
circulation strategy, green design strategy, site response, etc. A diagramme represented
this part of the iterative process is shown in Figure 4.5 (Ibid., p. 9). In the case of KTPH,
this took place in the masterplan and schematic design stages (‘MP’ and ‘SD’ in Figure
4.1), soon after the masterplanning workshop.
Based on Architect Lim’s reflection44, he learnt from the masterplan workshop that the
main reasons for KTPH’s selection of the CPG-Hillier scheme as winning entry for
further development were:
1. The scheme revolving around a garden as the ‘heart’ of the scheme. This opens
up opportunities for the development of the notion of ‘healing garden’, a practice
that the KTPH management team had established since year 2000 in their
previous premise, Alexandra Hospital. The KTPH HPC’s firm belief and
recurring emphasis of integrating natural environment into the healthcare
44 Interview session held in January 2012.
Figure 4.5 Iterative process model during the schematic design phase. Adapted from van der
Aa, Heiselberg and Perino (2011). Red annotation added for referencing with KTPH process
map (Figure 4.1).
SD VE1
Schematic Design
(Concept Design)

94
environment to harness its therapeutic properties, not only for patients, but also
for patients’ families, visitors, and hospital staff had since the masterplanning
workshop became ingrained into the building professionals’ mindset. This belief
is supported by the biophilia hypothesis (Wilson, 1984; Kellert et al, 1993) and
evidence-based studies (Ulrich, 2001; Dellinger, 2010; McCullough, 2010;
Whitehouse et al., 2001), as presented in Appendix VI.
2. The courtyard was recognized as a good orientation device to enhance way
finding, as a result contributing to KTPH’s vision of ‘a hassle-free hospital’. This
is also supported by evidence-based studies (Ulrich et al, 2004), also presented in
Appendix VI. In addition, to translate the notion of ‘patient-centric’ into
actionable performance criteria, KTPH’s CEO Liak specifically set such challenge
for the design team: Walking distance for patient from arrival point to the
accident and emergency department shall be no more than 20m; to the clinics, no
more than 50m; to the wards, no more than 100m.
3. The layout demonstrated that good potentials for natural ventilation, which
supports one of KTPH’s main objectives of ‘high energy efficiency’, ‘tropical
design’ and ‘harness natural ventilation’ (See Table 3.2).
The said shared values were taken up by the integrated design team. In response, design
iterations through masterplanning and schematic design, supported by evidence-based
and performance-simulated studies were focused on refining and improving the site
planning and massing layout design as shown in Table 4.1.
The design tools utilized during this stage to support the iterative process includes
climatic simulation performed by TBPT, way finding simulation performed by space
syntax45 (Figure 4.5), traffic simulation performed by CPG Transport, ETTV calculation
performed by CPG Mechanical Engineer, etc.
45 Space Syntax claimed to “developed evidence-based methods for analysing spatial layout,
observing patterns of space use within the hospital environment and designing ward layouts and

95
The landscape drawings by Peridian Asia (Figure 4.6 to 4.10) demonstrated the design
outcome at this stage, where biophilic design took centre-stage; one in which building
and constructed landscape “foster a positive connection between people and nature in
places of cultural and ecological significance and security” (Guenther and Vittori, 2008,
p. 88). The biophilic approach set the stage for further and deeper collaboration between
the KTPH hospital planning team and building professionals. For example:
hospital circulation which optimise space use, wayfinding and interaction. These techniques work
by measuring the properties of spatial layouts that users perceive: lines of sight along streets and
corridors, visual fields from reception areas and nurse stations and degrees of openness and
privacy.” (‘Healthcare’ at Space Syntax website). Based on Hillier’s space syntax theory (Hillier,
1999), it is being promoted as a evidence-based approach (Sailer et al, 2010).
Table 4.1 Integrated Design Activities
Professional Built Form Courtyard Space Site Response
Architect
(CPG)
Adjust and provide the
revised massing layout and
site planning; provide
typical floor plans according
to programmatic
requirements
Examine the relationship of
the built form and the
courtyard space
Examine the relationship of
the built form, the courtyard
space and the Yishun Pond
Healthcare Planner
(RMJM-Hillier)
Provide options on internal
layout
Consider the view out to
courtyard for ward and staff
area
Consider the view out to
Yishun Pond for ward and
staff area
Mechanical Engineer
(CPG)
Provide the design team
ETTV estimate; advising on
envelope performance
Proposed the use of raw water from Yishun Pond for
irrigation of landscape and outdoor washing
Landscape Architect
(Peridian)
Consider design of green
roof, green terraces and
vertical planting; adopt
naturalistic approach
Investigate the effect of
daylight/shading in the
courtyard space, affecting
plant types
Investigate opportunities in
integration of landscape
design with Yushun Pond
Green Consultant
(TBPT)
Advise on effect of
bioclimatic response of the
built form; performed
simulation to support the
advices.
Advise on effect of climate
on the courtyard as shaped
by built form
Consider effect of wind
movement from across
Yishun Pond
Civil & Structural
Engineer (CPG)
Advise design team on
structural system
Electrical Engineer
(CPG)
Advise on preliminary
energy consumption
Wayfinding Consultant
(Space Syntax) Analyze wayfinding using software simulation
CPG Transport
Engineer
Conducted traffic sim-
ulation at drop off area
Hospital Planning Team
(KTPH)
Educate design team on
operational requirements;
review design with
consultants
Review design with
consultants
Review design with
consultants
KTPH Landscape
Workgroup
Examine issue of urban
farming at KTPH roof top
Share with design team
experience from AH and
preference of plant types

96
1. To engage in ‘place-making’, a term used by the KTPH hospital planning team in
looking out for opportunities to create landscaped corners, seating areas, terraces
(Figure 4.8 to 4.11), for patients, families, staff, and breakout spaces where
clinicians and patient/families may communicate in humane manners. This is
also presented in Section 4.2.4.
2. To enhance the thermal comfort of roof terraces (Figure 4.9 to 4.11), spot cooling
was introduced by directing the HEPA-filtered exhaust air from air-conditioned
spaces into these landscaped roof terrace areas. Mechanical Engineer Toh said
that, “it effectively lowered the ambient temperature by about 2°C,”46 which
contributed towards achieving a cooling sensation for users of these spaces.
Architect Ong added that to complete the integrated design, it was necessary for
the architect and landscape architect to consider the integration of the exhaust
with the façade and landscape design. As a result, ‘waste’ from one system
(exhaust cooled air from air-conditioning) is hereby used as a resource to
enhance another system (outdoor landscaped social and therapeutic space).
46 Interview session held in January 2012.
Figure 4.6 Landscape plan showing landscaped courtyard as the heart and lung of design.
Source: Peridian Asia; CPG file archive

97
Figure 4.8 Sketch design for landscaped roof terrace as social space, while providing good
shading, insulation to interior spaces below, and integrated with spot cooling by recovering
‘cooled’ temperature from exhaust air. Source: Peridian Asia; CPG file archive
Figure 4.7 Landscape schematic drawing. It
shows landscaped courtyard as the heart,
addressing main entrance as arrival/foyer,
opens to basement 1 for light and ventilation,
and surrounded by landscaped terraces. The
replacement rate for the greenery is 70%.
Source: CPG Consultants Pte Ltd

98
Figure 4.9 Landscaped oof terrace at Level 4 where patients, visitors, staff may enjoy moments
of solitude or share moments of comfort or grieve; it is also a source of visual relief from the
wards. Source: Peridian Asia; CPG file archive
Figure 4.10 Landscaped roof terrace at Level 5 overlooking Level 4.
Source: Peridian Asia; CPG file archive

99
4.2.2 The Design Development (DD1) Stage
As the design process enters the design development stage (DD1; known as system
design phase in IPM; Figure 4.11), van der Aa, Heiselberg and Perino proposed that
integration of system design be carried out. For KTPH at this stage, block layout and
floor plans reflecting each department’s operational work flow were progressively being
iterated and agreed. Specific architectural and technical solutions were proposed,
supported by design calculations and simulations. During this phase, the design team
members were also seeking opportunity for integration of system design.
The bioclimatic response of the KTPH site planning is shown in Figures 4.12 (sun path)
and 4.13 (prevalent wind directions). The orientation of the blocks, as constraint by the
site boundary and the primary objective of orientating the courtyard towards the Yishun
Pond, is less than ideal as the private wards tower (P) is directly exposed to east and
west sun, while the subsidized ward (S) and the specialist outpatient clinics blocks (SOC)
are exposed to east and west sun at an angle, and the project team noted that careful
envelope design was required to address that. On the other hand, as stated in Section
4.1.1, the site orientation does facilitate air movement from the prevalent wind directions
through the courtyard. One other consideration is to place the naturally ventilated
subsidized ward tower furthest away from the main road as it is most vulnerable to
traffic noise pollution.
Figure 4.11 Iterative process model during the schematic design phase.
Adapted from van der Aa, Heiselberg and Perino (2011)
DD1 VE2
Design Development
(System Design)

100
Figure 4.12 Bioclimatic response of KTPH: sunpath
Sunpath generated using Autodesk Ecotect with weather data from EnergyPlus website.
Overall Massing Outline
NV Ward Outline
N15°
30°
45°
60°
75°
90°
105°
120°
135°
150°
165°180°
195°
210°
225°
240°
255°
270°
285°
300°
315°
330°
345°
10°
20°
30°
40°
50°
60°
70°
80°
8
910
111213141516
17
18
191st Jan
1st Feb
1st Mar
1st Apr
1st May
1st Jun1st Jul
1st Aug
1st Sep
1st Oct
1st Nov
1st Dec
Stereographic DiagramLocation: SINGAPORE, SGP
P
SOC
SOC
SOC
S
Figure 4.13 Bioclimatic response of KTPH: prevalent wind directions
Sunpath generated using Autodesk Ecotect with weather data from EnergyPlus website.
NORTH15°
30°
45°
60°
75°
EAST
105°
120°
135°
150°
165°SOUTH
195°
210°
225°
240°
255°
WEST
285°
300°
315°
330°
345°
10 km/ h
20 km/ h
30 km/ h
40 km/ h
50 km/ h hrs
381+
342
304
266
228
190
152
114
76
<38
Prevailing WindsWind Frequency (Hrs)
Location: SINGAPORE, SGP (1.4°, 104.0°)
Date: 1st January - 31st December
Time: 00:00 - 24:00
© Weather Tool
Overall Massing Outline
NV Ward Outline
P
SOC
SOC
SOC
S

101
In addition, the breeze across the open pond park land area would also be more
beneficial to the naturally ventilated wards than the air-conditioned private wards.
In the design, the project team had also taken into account the aspect ratio of the block
massing in response to the ventilation mode (Figure 4.14). To facilitate natural
ventilation, shallow plans were adopted for the naturally ventilated subsidized ward
tower. The air-conditioned private ward tower and the specialist outpatient clinics block
were designed with deeper plans to reduce the envelope-to-space ratio, so as to conserve
energy by minimizing heat gain through thermal exchange of the envelope. A critical
review based on BRE’s environmental design guidelines (Rennie and Parand, 1998)
revealed that the naturally ventilated ward design have satisfied the environmental
design guidelines (Figure 4.15). For example, the room depth to height ratio of 2.5 or less
was achieved for natural ventilation. This does mean that the day light penetration of
room depth to height ratio of 2.0 was marginally sub-standard; hence the integrated
design again came into play. Architect Ong recounted that when light shelf was
considered, daylight simulation was performed by TBPT to validate the improvement in
daylight distribution. After that, to meet the lighting performance criteria of 550lux,
M&E engineer Toh Yong Hua designed artificial lighting linked to photo-sensors. The
artificial lighting will only be turned on when the photo-sensors detect that the daylight
Figure 4.14 Aspect ratio of the various block. Source of base drawing: CPG Consultants Pte Ltd.
40m
75m20m
70m 30m
75m
40+3m35m
Naturally Ventilated Subsidized Wards

102
level has fallen below 550lux. As a result, energy is consumed only when it is absolutely
necessary to meet the performance required. For air-conditioned areas, this also resulted
in a reduction of heat load attributable to artificial lighting.
Toh added that for the air-conditioned single-room private wards, local control is
provided to the patients. For patients who prefer natural ventilation, the windows are
openable. When the windows are opened, the micro-switch at the window would
immediately deactivate the air-conditioning system, hence reducing chill water usage,
conserving both energy and water usages. The air-conditioning system design must
therefore incorporate control systems that dynamically monitor the demand. To match
demand with supply as closely as possible, variable flow chilled water system is used.
The demonstration of integrated design effort at this stage is most clearly seen in the
integrated envelope design solution to balance the considerations for view, day lighting
and thermal comfort by examining influencing factors holistically as shown in Table 4.2.
Figure 4.15 Critical review based on ‘Environmental Design Guide for Naturally Ventilated and
Daylit Offices’ (Rennie and Parand, 1998). Source of base drawing: CPG Consultants Pte Ltd.
4.2m 2.7m
0.6m
0.8m 0.7m
H = 3.3m2.5H = 8.25m
H = 3.3m2H = 7.6m
0.4m
External shading
Light Shelf
Wind wall

103
The role and activities played by the various team members are summarized in Table 4.3.
Each design iteration of the façade system (by architect; Figure 4.16 to 4.21) were
analyzed in terms of its ETTV performance (by mechanical engineer), daylight
performance and natural ventilation performance (by green consultant), construction
cost estimate (by quantity surveyor), and estimation of life-cycle electrical consumption
as an outcome to the resultant cooling load (by electrical engineer). These factors of
considerations were deliberated at the second value engineering workshop (VE2),
allowing an informed decision to be made, balancing the considerations for view,
daylight, natural ventilation, shading coefficient, aesthetic, capital expenditure, and life-
cycle cost, etc. In a nutshell, the building envelope, daylighting/artificial lighting,
ventilation strategy, view, rain protection, and aesthetics were performing as a system
and an integrated whole (Ong, interview sessions in Jan 2012).
Table 4.2 Integrated design considerations for façade, thermal comfort and energy usage
Naturally ventilated areas Air-conditioned areas
View View
Daylight level Daylight level
Daylight distribution Daylight distribution
Shading from direct solar penetration Shading from direct solar penetration
Tint on glazing to achieve glare reduction Shading coefficient of glazing materials
Minimizing heat gain through external envelope,
i.e. ETTV (a composite value measure in W/m2 that
takes into account conduction and radiation)
Minimizing heat gain through external envelope,
i.e. ETTV (a composite value measure in W/m2 that
takes into account conduction and radiation)
Thermal comfort based on the adaptive model Thermal comfort based on the adaptive model
Air movement through CFD and wind tunnel
study; introduce ‘Wind Wall’. -
Rain protection -
Table 4.3 Integrated design activities for the envelope design
Professional Built Form
Architect (CPG) +
Façade Consultant (Aurecon)
Considered various design iterations of shading device, including
aesthetics.
Make design adjustment based on consultants’ input.
Mechanical Engineer (CPG)
Provide the design team ETTV estimate for each iteration of shading
device design option.
Provide advice on the envelope performance to be targeted.
Green Consultant (TBPT)
Provide advice passive and active design strategy.
Performed simulation iterations to support the advices.
Performed daylight simulations.
Performed CFD simulations and wind tunnel tests.
Propose design improvement to enhance the performance of the
building envelope.
Electrical Engineer (CPG) Provide advice on estimation of energy consumption
Provide life cycle cost estimation, based on energy consumption.
Civil & Structural Engineer (CPG) Provide advice on support system for shading devices.
Quantity Surveyor (CPG) Provide cost estimate for each design iteation.

104
Figure 4.16 Design study 1 for façade shading of the naturally ventilated ward tower.
Source of drawing: CPG Consultants Pte Ltd.
Figure 4.17 Design study 2 for façade shading of the naturally ventilated ward tower.
Source of drawing: CPG Consultants Pte Ltd.

105
Figure 4.18 Design study 3 for façade shading of the naturally ventilated ward tower. This
design was selected to maximize NV and lighting. Source of drawing: CPG Consultants Pte Ltd.
Figure 4.19 Design developed from Option 3: Fully height louvred façade and light shelf
maximizes natural ventilation and daylight. Source of drawing: CPG Consultants Pte Ltd.

106
Figure 4.20 Design developed from Option 3: Effect of rain needs to be considered in the tropics.
These diagrammes indicate integration of monsoon windows providing ventilation during rain,
even when the louvred windows are closed. Source of drawing: CPG Consultants Pte Ltd.
Figure 4.21 Interior of naturally ventilated ward: Façade system comprising louvred wall, light
shelves, and monsoon window. Natural ventilation is supplemented with individually
controlled fans. Source of image: CPG Consultants Pte Ltd.
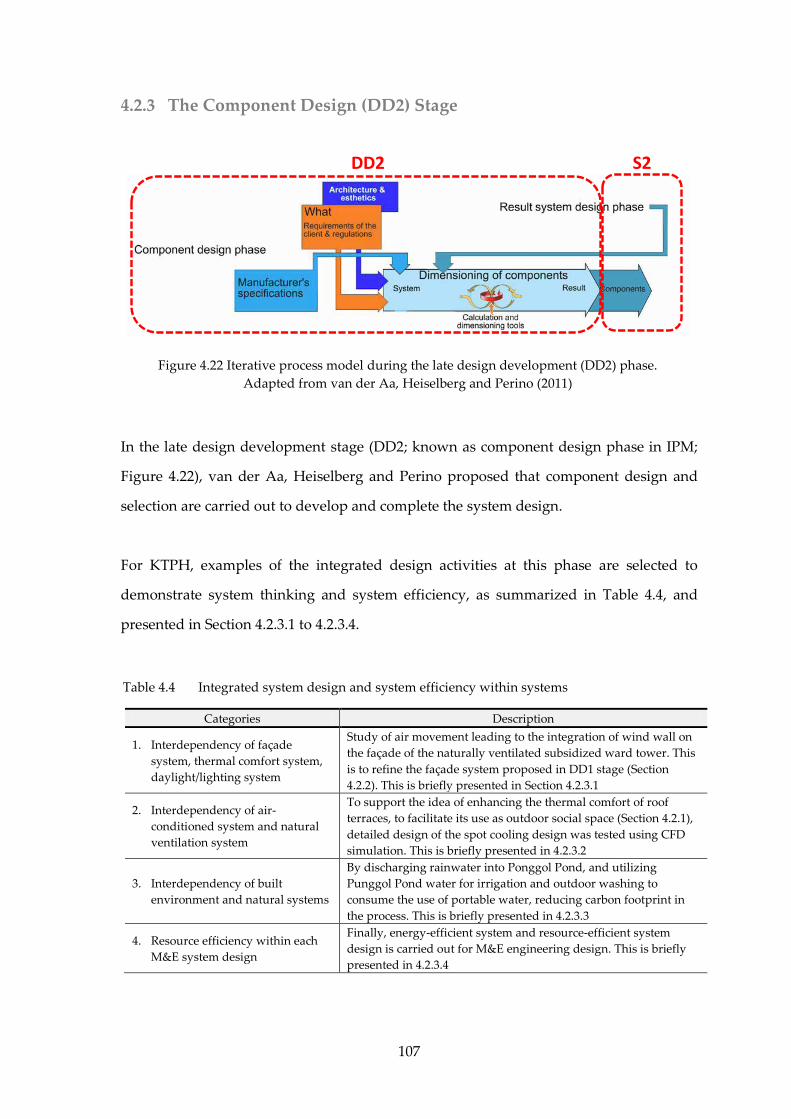
107
4.2.3 The Component Design (DD2) Stage
In the late design development stage (DD2; known as component design phase in IPM;
Figure 4.22), van der Aa, Heiselberg and Perino proposed that component design and
selection are carried out to develop and complete the system design.
For KTPH, examples of the integrated design activities at this phase are selected to
demonstrate system thinking and system efficiency, as summarized in Table 4.4, and
presented in Section 4.2.3.1 to 4.2.3.4.
Figure 4.22 Iterative process model during the late design development (DD2) phase.
Adapted from van der Aa, Heiselberg and Perino (2011)
DD2 S2
Table 4.4 Integrated system design and system efficiency within systems
Categories Description
1. Interdependency of façade
system, thermal comfort system,
daylight/lighting system
Study of air movement leading to the integration of wind wall on
the façade of the naturally ventilated subsidized ward tower. This
is to refine the façade system proposed in DD1 stage (Section
4.2.2). This is briefly presented in Section 4.2.3.1
2. Interdependency of air-
conditioned system and natural
ventilation system
To support the idea of enhancing the thermal comfort of roof
terraces, to facilitate its use as outdoor social space (Section 4.2.1),
detailed design of the spot cooling design was tested using CFD
simulation. This is briefly presented in 4.2.3.2
3. Interdependency of built
environment and natural systems
By discharging rainwater into Ponggol Pond, and utilizing
Punggol Pond water for irrigation and outdoor washing to
consume the use of portable water, reducing carbon footprint in
the process. This is briefly presented in 4.2.3.3
4. Resource efficiency within each
M&E system design
Finally, energy-efficient system and resource-efficient system
design is carried out for M&E engineering design. This is briefly
presented in 4.2.3.4
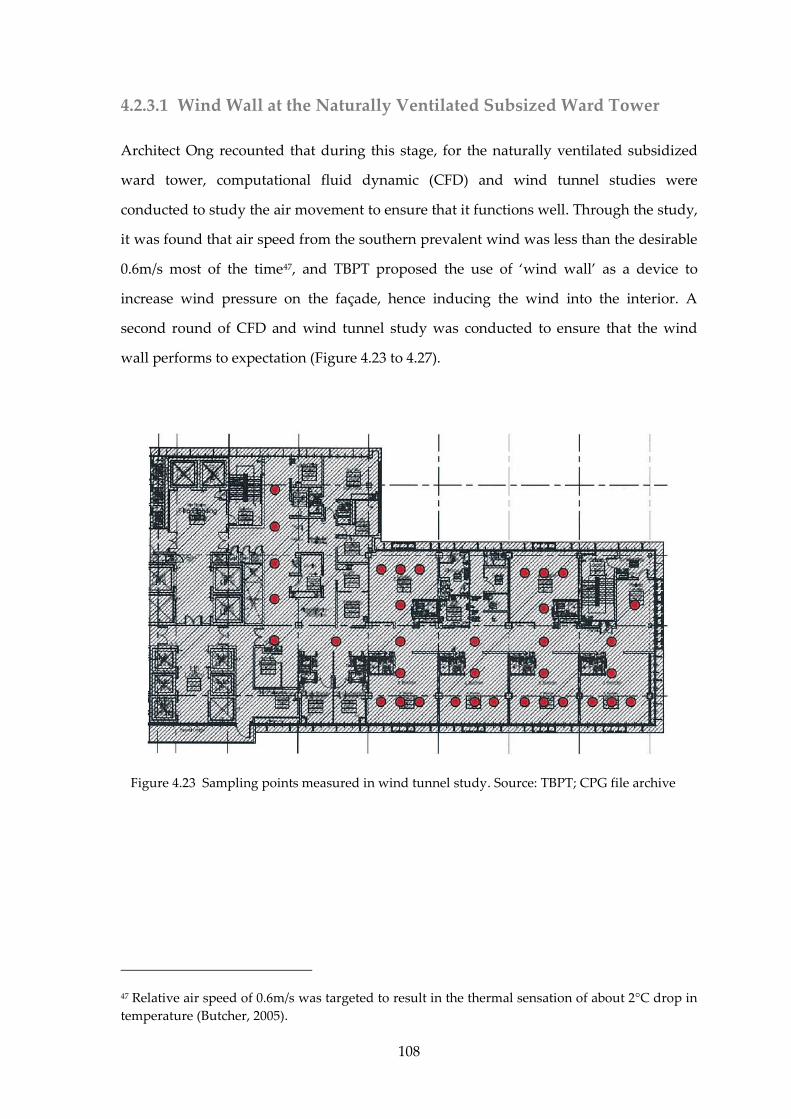
108
4.2.3.1 Wind Wall at the Naturally Ventilated Subsized Ward Tower
Architect Ong recounted that during this stage, for the naturally ventilated subsidized
ward tower, computational fluid dynamic (CFD) and wind tunnel studies were
conducted to study the air movement to ensure that it functions well. Through the study,
it was found that air speed from the southern prevalent wind was less than the desirable
0.6m/s most of the time47, and TBPT proposed the use of ‘wind wall’ as a device to
increase wind pressure on the façade, hence inducing the wind into the interior. A
second round of CFD and wind tunnel study was conducted to ensure that the wind
wall performs to expectation (Figure 4.23 to 4.27).
47 Relative air speed of 0.6m/s was targeted to result in the thermal sensation of about 2°C drop in
temperature (Butcher, 2005).
Figure 4.23 Sampling points measured in wind tunnel study. Source: TBPT; CPG file archive

109
Figure 4.24 A sample of the air velocity profile across a typical ward at 1.2m height @ open, 50%
open and closed conditions. Source: TBPT; CPG file archive.
Figure 4.25 A sample of the pressure coefficients chart across the façade of the subsidised ward
tower obtained as boundary conditions for the CFD study. Source: TBPT; CPG file archive

110
4.2.3.2 Detailed Deisgn of Spot Cooling at Roof Terraces: New Air
To enhance the thermal comfort of landscaped roof terraces (Section 4.2.1), spot cooling
was introduced by directing the cooled exhaust air from operating theatres into these
roof terrace spaces. Dilution, high-efficiency particulate air (HEPA) filter and UV
sterilization were techniques used to ensure infection control. Mechanical Engineer Toh
affectionately named the system ‘New Air’, and CFD (Figure 4.28 to Figure 4.32) and
Figure 4.26 1:20 Wind tunnel model used for the study. Source: TBPT; CPG file archive
Figure 4.27 Subsidized ward tower façade showing solar screen to provide shade and wind
wall to induce air movement. Greenery is also integrated into the façade to enhance visual relief.
Source: CPG Consultants Pte Ltd

111
evidence-based evaluation (Table 4.4) was performed at this stage to research the
outcome before its implementation. The adaptive re-use of ‘waste’ from one system
(exhaust air from air-conditioned operating theatre) to enhance another system
(naturally ventilated outdoor landscaped social space) demonstrates inter-dependency of
systems (Toh, interview sessions in Jan 2012).
Figure 4.28 Design drawing showing location of exhaust nozel integrated into the façade, and
the direction of throw to cool the landscaped roof terraces. Source: CPG Consultants Pte Ltd
Figure 4.29 CFD Simulation showing approximately 2°C reduction in temperature at the roof
terrace, delivering cooling sensation to users. Source: CPG Consultants Pte Ltd

112
Figure 4.30 CFD simulation showing the throw of exhaust nozzle, and the wind speed gradient.
A 2m/s wind speed is achieved at the end of the throw. Source: CPG Consultants Pte Ltd
Figure 4.31 Noise level (dBA) at various distances (m) from the nozzle diffuser. The noise level
at landscaped roof terrace at 5m away from nozzle diffuser is 43dBA, which is equivalent to
outdoor ambient sound level. Source: CPG Consultants Pte Ltd
57dBA
37dBA
27dBA
31dBA
25dBA
10 m
23dBA
0 m
20 m
30 m
40 m
50 m
5 m
43dBA
@L4 Roof Garden @L1 Lobby

113
Table 4.5 Evidence-based evaluation for ‘New Air’ (spot cooling at outdoor roof terrace). Source:
CPG Consultants Pte Ltd
Consider-
ations Reference
Standards
complied
with
1. Guidelines for Design and Construction of Healthcare Facilities, AIA 2006
2. HVAC Design Manual or Hospitals and Clinics, ASHRAE 2003
3. HTM 2025
4. Guidelines for Environmental Infection Control in Health-Care Facilities, CDC Atlanta
2003
5. Guideline for Preventing the Transmission of Tuberculosis in Health-Care Settings,
CDC
6. Meeting JCAHO’s Infection Control Requirements, JCI 2004
7. EPA Technical Brief on Biological Inactivation Efficiency In-Duct UVC Devices
8. CP13 Mechanical Ventilation and Air-conditioning in Buildings 1999
9. Guidelines for Good Indoor Air Quality in Office Premises, NEA 1996
Measures
implemen-
ted
1. Sufficient DiLUTION of Exhaust Air can be achieved through mixing with outdoor air.
Reduction of ambient temperature at 2 to 4 be achieved.
2. STERIL-AIRE UVC in-duct emitters for INFECTION CONTROL provide germicidal
irradiation with periodical monitoring of bacterial counts and fungal counts according
to NEA guidelines on Indoor Air Quality(IAQ) by accredited Laboratory. The Emitters
are Environmental Protection Agency(EPA) tested proven industrial-grade air
sterilizing system.
3. The application exceeds the CDC guidelines, HTM and other design codes for
treatment of OT exhaust air.
4. All OT exhaust fans are coupled with in-out Silencers for acoustic treatment
5. All UVC emitter performance are tracked by BMS for real-time monitoring(round the
clock) using radiometers linked to alarm and fault reporting
6. Due to UVC failure, the application can be suspended as and when required for
individual OT or multiple OT exhaust by diverting the nozzle diffusers to the sky
7. The complete application can also be suspended under pandemic outbreak situation.
Figure 4.32 Selection of component: Oscillating nozzle diffusers tested to ISO 5135 1997 and ISO
3741 1999 on sound power level performance to allow for better throw distribution.
Source: CPG Consultants Pte Ltd

114
4.2.3.3 Water Efficient Landscaping Irrigation System
The rainwater collected within the KTPH site is discharged into Yishun Pond, adjacent to
the site. The raw water (non-portable) from Yishun Pond is then used for landscape
irrigation and floor washing in KTPH, to reduce consumption on potable water48, hence
reducing carbon footprint. Essentially, the rainwater resource and irrigation needs of the
KTPH site were seen as part of the larger hydrological cycle. Newater, water recycled
from sewage was used as a backup water source for the irrigation system (See Figure
4.33 and 4.34). In the system, efficient drip irrigation system and rain sensors were
utilized to reduce wastage (Toh, interview sessions in Jan 2012).
48 Treatment and pumping of portable water consumes energy. By utilizing and replenishing raw
water at site, unnecessary energy consumption is eliminated.
Figure 4.33 Conceptual diagramme of irrigation system and built environment as part of
natural systems. Source: CPG Consultants Pte Ltd
Precipitation
Evapo-transpirationBuilt
Environment
Building-Integrated
Natural Environment
(Biophillic Architecture)
Rainwater Runoff
/Discharge
Rainwater
Reuse Pond
water source with
New water source as
backup
Rainwater
treatment
Reduced Carbon
Footprint

115
4.2.3.4 Resource-Efficient M&E System Design
Toh commented that for mechanical & electrical engineering (M&E) design, it would be
crucial at this stage to select the most efficient M&E equipment available in the market,
and checking with manufacturers that the equipment performs well as a system (See
Appendix VII). The M&E design was supported by:
1. Energy modeling was performed by the green consultant with simulation
parameters supplied by architect, mechanical and electrical engineers.
2. Based on the ETTV target agreed by the project team, architects confirmed the
window opening size and glazing material selection based on the appropriate
glazing properties e,g, shading coefficient, light transmittance, low-emissivity,
etc.
At this stage, green rating tools such as Green Mark metric were used to validate and
fine-tune green design. The measures adopted in KTPH are shown in Appendix VII to X.
Figure 4.34 Schematic of irrigation system, drawing water from Yishun.
Source: CPG Consultants Pte Ltd

116
4.3 Discussion: KTPH’s Integrated Design and Iterative Process
This chapter highlighted some examples of close collaboration between the medical
professionals and building professionals in the KTPH project. The design process in fact
continued to develop during the construction phase (See Appendix X), which is not the
focus in this dissertation. Through the examination of KTPH’s integrated design and
iterative process, it showed that even without having the benefits of referring to
structured IDP methodologies, by using a IDP methodology that was developed in-
house and customized by the project team to suit KTPH’s unique requirements, many of
the IDP elements and practice measures advocated had emerged and were practiced in
the KTPH design process. The evaluation matrices that summarize the comparison
between the IDP model and KTPH are shown in Table 4.5 and 4.6, with reference to the
Table 4.6 Comparison between WSIP Process Elements (2007) and KTPH Design Process
Stage Essential Elements in WSIP Process Stages (2007, p.8) Practiced in
KTPH IDP
1. Team
Formation “Fully engage Client in the design decision process.” Yes
“Assemble the right team.” Yes
Key attributes in team formation is ‘teachable attitude’; members
come on board not as experts but co-learners. Yes
2. Visioning “Align team around basic Aspirations, a Core Purpose, and Core
Values.” Yes
3. Objectives
Setting
“Identify key systems to be addressed that will most benefit the
environment and project” Yes
“Commit to specific measurable goals for key systems” Yes
Compile into a Sustainable design brief
Key attributes in objective setting is to involve all participants,
including the main financial decision maker, not unempowered
representative. Also, identify champions for the objectives and
issues.
Yes
4. Design Iteration “Optimization of the design of systems” Yes
Key attributes in objective setting is to “understand and make best
use of key systems in relationship to each other, to the goals, and
to the core purpose”, and “Iterate ideas and systems relationships
among team with all participants, including the main financial
decision maker.”
Yes
5. Construction &
Commissioning Not included in this study NA
6. Post-occupancy
Feedback Loops Not included in this study NA

117
process map of IDP model (Figure 4.2) and KTPH process map (Figure 4.1).
In Section 2.3.4.2, the importance of group dynamics supported by appropriate social,
team-based design techniques and methodologies has been presented. This is validated
by the experiences and reflections by the project team members who had participated in
the KTPH integrated design process. In reflection, however, there are also lessons to be
learnt. In the next concluding chapter, the KTPH built environment as an outcome of the
integrated design process, and purported as a sustainable healthcare architecture, is
evaluated with reference to various post-occupancy studies. It is followed by a
discussion on lessons learnt from the research so far, and further recommendations.
Table 4.7 Mapping KTPH’s integrated design process against the IDP model with reference to
Figure 4.1 and 4.2.
WSIP (2007)
Stages KTPH IDP Stages Comment
‘R1’ in Fig 4.2 ‘DC’ in Figure 4.1:
Design Competition
Research in KTPH design competition was
done in an integrated building design team,
but without involve-ment of users e.g.
clinicians
‘W1’ in Fig 4.2 ‘W1’ in Figure 4.1: Visioning Workshop This validates the IDP model for visioning.
- ‘W2’ in Figure 4.1: Masterplan Workshop
Masterplan is not an expressed stage in IDP
model. This can be considered as part of SD
in IDP model.
‘R2’ and ‘W2’
in Fig 4.2
‘MP’ in Figure 4.1: Masterplan Workshop
‘S1’ in Figure 4.1: Workshop + Sign off
masterplan
This validates the IDP model for
research/workshop.
‘R3’ and ‘W3’
in Fig 4.2
‘SD’ in Figure 4.1: Schematic Design
‘VE1’ in Figure 4.1: Value engineering
workshop 1
While KTPH’s iterative process is more
prolonged, it is due to the complexity of the
hospital typology. This more or less validates
the IDP model for research/workshop.
‘R4’ and ‘W4’
in Fig 4.2
‘DD1’ in Figure 4.1: Schematic Design
‘VE2’ in Figure 4.1: Value engineering
workshop 1
Design process in practice is more fuzzy, and
do not progress in distinct stages as in theory
(Lawson, 2005). DD1 in KTPH may indeed
be considered as an extended SD. This,
together with a second VE workshop
appears to validates the IDP model.
- ‘DD2’
Iterative design process in KTPH continued
into DD2. This reflects the complexity of a
hospital typology.
W5 ‘S2’
The decision workshop to confirm the
outcome of DD in both IDP model and
KTPH again validates the IDP model.
W6 CD and Construction Stage
KTPH’s integrated design process in fact
extended beyond DD, into the construction
stage, exploring other opportunities (See
Appendix IX).

118
Chapter 5.0: Conclusion
“The true value of an integrated process is an
improved building with less waste in its
production and operation. These better building
improvements include reduced operating costs,
rightsizing, the improved health and productivity
of the staff, and enhanced patient experience.”
Robin Guenther and Gail Vittori
“It is critical that we begin to move beyond green
buildings, even current generation of green
building tools, and embrace the concept of living
buildings or even restorative buildings.”
Bob Berkebile

119
Chapter 5.0 Conclusion
Following the last chapter, in which the KTPH iteration process was presented, this
chapter briefly evaluates the KTPH built environment as an outcome of the integrated
design process, i.e. as a sustainable healthcare architecture. It is followed by a
presentation of the lessons learnt from the research on the practice of integrated design
in KTPH, which provides the materials for a discussion. Following the discussion, a few
recommendations are made on future research directions.
5.1 KTPH: Sustainable Healthcare Architecture in Singapore
The evaluation of KTPH as a sustainable healthcare architecture is carried out based on
various post-occupancy studies (Table 5.1), and is presented in Section 5.1.1 to 5.1.4.
5.1.1 KTPH as a Green Building
KTPH was certified as a BCA Greenmark Platinum building (see Appendix XI) in 2010,
the highest recognition as a high performance, resource-efficient building in the
Singapore and tropical context (See Appendix VII to X). Its key building performance
characteristics are summarized in Table 4.7. Two positive observations of its
performance as a green building are:
1. A post-occupancy survey (Sng, 2011) have found that natural ventilation is a
viable strategy for both in-patients and nursing staff (See Appendix XIII).
2. BCA Green Mark requires that the actual building performance be submitted one
year after occupation, to confirm that the design measures are implemented. In
Table 5.1 KTPH: Post Occupancy Studies
S/No. Description
1. Preliminary energy consumption study conducted by CPG Mechanical Engineer Toh
Yong Hua.
2. Sng, P. L. (2011). In What Way Can Green Building Contribute to Human Wellness in
the Singapore Context? M Arch. National University of Singapore.
3. Wu, Z. (2011). Evaluation of a Sustainable Hospital Design Based on Its Environmental
and Social Outcomes. MSc. Cornell University.

120
preparation for the submission, CPG Mechanical Engineer Toh found that actual
metered energy consumption is in fact lower than energy modeling performed
during the design, with an average savings of 46.6% between July 2010 and Sep
2011. As of this writing, the data is still being analyzed.
Table 5.1 Key Building Performance Characteristics
(Guenther and Vittori, 2008, p. 173; CPG Green Mark submission document)
Category Description
Site
Extensive landscaping contributes to reducing heat island effets.
Naturally ventilated subsidized ward benefits from breeze from Yishun Pond.
Extensive tree planting.
Energy
Extensive use of natural ventilation (36% of floor area).
Naturally ventilated external corridor reduces space cooling demands.
Energy-efficient conventional M&E system design, resulting in energy reduction of
36.4% compared to baseline reference model.
Shading device on the façade to reduce solar heat gain.
Courtyard extends to basement to provide natural ventilation and daylight.
Water
Yishun Pond landscape and social amenities improved. Rainwater runoff from site is
discharge into Yishun Pond in compliance with sustainable drainage design.
Raw water from Yishun Pond is used for irrigation and outdoor washing.
Water-efficient fittings are used.
Indoor
Environmental
Quality
Naturally ventilated subsized ward tower is designed with shallow plan to maximize
cross ventilation.
Acoustic comfort was designed to meet performance objectives of stress-reducing
environment.
Indoor air is treated with UVC and anti-bacteria measures to meet infection control
objectives.
Naturally ventilated corridor engages landscape courtyard.
Lightshelves to maximize daylight in the interior.
Shading device on the façade to reduce solar heat gain.
Wind wall to improve natural ventilation.
Renewable
Energy
Solar thermal hot water system generating 21,000litres/day to fully meet hospital
needs.
130kWp photovoltaic system
Innovation
Self-sustaining ecological pond.
Achieve spot cooling for outdoor landscape roof terrace social spaces by making use
of HEPA-filtered exhaust air from operating theatres.
Dual refuse chutes for separation of recyclable waste.
Siphonic rainwater discharge system to reduce pipe size, hence reduce space wastage,
as well as to reduce noise.
Automatic waste and soft linen collection systems.
Auto tube cleaning system was used to reduce consumption by approximately 20%.
Composting machine was used to process food waste into fertilizer for roof and food
gardens.

121
5.1.2 KTPH: Embracing Social Sustainability
Post occupancy survey by Wu found that its natural environment has been the most
well-liked feature (Wu, 2011; see also Appendix XIV). This has directly or indirectly
contributed to the positive outcome of KTPH being a desirable social environment
(Ibid.), enhancing wellbeing for patients, their friends and families, visitors, public, as
well as healthcare workers.
Sng also found that these ‘wellness dimensions of World Health Organizations Quality
of Life’ (WHOQOL) are in fact missing from BCA Green Mark rating system (Ibid., p.
75). In focusing on technical performance of the built environment, Green Mark aims to
address the issues of reduced consumption of energy and resources, but it does not
address social and ecological dimensions of sustainability. Such are perhaps not the
current purpose of Green Mark rating system; but it also indicates that the objectives-
setting of social and ecological dimensions would have to be generated independently
from the Green Mark rating system, as has been demonstrated through the visioning and
objectives-setting efforts in the KTPH Project using the TBP framework (Section 3.3).
5.1.3 KTPH: Embracing Environmental Sustainability
By adopting an integrated approach in site planning, connecting the KTPH’s
environment with Ponggol Pond and the Yishun natural and community contexts, the
design has opened up opportunities for community and environmental stewardship for
KTPH, as follows:
1. Maximizing opportunities in creating a biophilic built environment (Appendix
VI).
2. Integrating with Yishun Pond environmentally and socially (Appendix XI & XV).
3. Fostering biodiversity, particularly an ecosystem that nurtures local butterflies
(Appendix XV).

122
KTPH management team has demonstrated track records and commitment in their
previous premise (AH) in fostering a biophilic environment and butterfly biodiversity
(See Appendix XV). By embracing the same approach in the much higher-density 3.5Ha
KTPH site that is one-third the size of the 13.5 Ha AH site, and having operated for
slightly more than a year, the outcome is still being monitored. What is interesting here
is that the design and operation of KTPH appears to move in a direction towards
environmental restoration/regeneration (Kellert, 2004; Birkeland, 2002; Reed and Malin,
2005; see Section 1.6.3).
5.1.4 KTPH: Mapping the Attributes of Sustainable Healthcare
Architecture and Integrated Design Approach
Summarizing from Section 5.1.1 to 5.1.3, ten sustainable attributes are identifiable in
KTPH, as summarized in Table 5.2. These attributes are mapped onto the Sustainable
Healthcare Architecture Model proposed in Section 2.3.5, as shown in Figure 5.1. This
diagramme put forth the case of KTPH as a positive example of sustainable healthcare
architecture in the Singapore context.
Table 5.2 Sustainability attributes of KTPH
S/No. Attributes Eco Soc Env
1 Green building reduces carbon footprint due to less non-renewable resources
consumed (Section 5.1.1; Appendix VII, VIII, IX, X, and XII)
2 Staff morale and productivity improves due to better physiological,
psychological and sociological well-beings (Section 5.1.2; Appendix XIV)
3 High-performance green building reduces expenditure on utilities, resulting
in life cycle savings (Section 5.1.1; Appendix VII, VIII, IX, X, and XII)
4 Patient well-being, faster recovery (Section 1.6.2; Appendix VI and XIV)
5 Hospital clinician/staff well-being (Section 1.6.2; Appendix VI and XIV)
6 Family/visitor/public well-being (Section 1.6.2; Appendix V and XIV)
7 Community participation through community stewardship programmes
(Section 5.1.2; Appendix XIV and XV)
8 Biophilic environment, creating symbiotic relationship between human and
nature (Section 1.6.3; Appendix VI)
9 Ecological integration between KTPH and Yunshun Pond (Section 1.6.3;
Appendix VI, XI and XV)
10 Fostering biodiversity through environmental stewardship (Section 1.6.3;
Appendix VI and XV)
Eco = Economic Sustainability
Soc = Social/Human Wellness Sustainability
Env = Environmental/Ecological Sustainability

123
Keeler and Burke have stated, “Integrated building design is the practice of designing
sustainably” (2009). The evaluation in this section validates that the integration design
approach is highly relevant and practicable to the healthcare architecture, at least in the
Singapore context. This has been demonstrated in the KTPH case study as characterized
by attributes summarized in Table 5.3.
Figure 5.1 KTPH: Sustainable Attributes mapped onto the Sustainable Healthcare Architecture Model.
Reduced Carbon Footprint
Staff Morale & Productivity
Life Cycle Savings
Patient Well-being
Hospital Staff Well-being
Family/Visitor Well-being
Community Participation
Biophilic Environment
Ecological Integration
Fostering Biodiversity
Eco-DesignBiophilic Built Environment
Built environment that integrates with natural and ecological systems
Environmental Sustainability
Green BuildingHigh-performance
Built environment as holistic, bioclimatic system of systems
Economic SustainabilityEvidence-Based WellnessCommunity-Stewardship
Built environment that supports integrated healthcare and social systems
Social Sustainability
Table 5.3 Integrated design attributes of KTPH
S/No. Attributes Reference
1 A building typology exhibiting complexity in functions. Section 1.1, 3.4.6
2 A project that has many stakeholders, spanning client (MOH), hospital
management (AH/KTPH), user groups, building consultants, contractors,
building authorities, agencies overseeing the community (PUB, HDB, NParks).
Section 3.3, 3.4
3 Early recognition and establishment of a multi-disciplinary team, comprising a
core project team supported by diverse expertise and user groups. Section 3.4
4 A triple-bottom-line approach, balancing economic and building performance,
social and human wellness, and environmental and ecological stewardship. Section 3.3
5 A robust visioning and objective setting process. Section 3.3
6 Some degree of success in mindset change. Section 4.3
7 A team-base, collaborative, integrated design process alternating
individual/small group research/design iterations and all stakeholders’
workshops, with an emphasis on ‘partnership’ and team work.
Section 4.1 to 4.3
8 Delivered a sustainable healthcare architecture as an integrated design
outcome. Section 5.1

124
5.2 Lessons Learnt on the Practice of Integrated Design from the
KTPH Case Study
Based on the documentation study and interviews from the project team members, the
lessons learnt are as follows:
1. Briefing is a continuous process that intertwines with the design process.
2. Entrenched practice among building professionals.
3. Mindset change was not homogeneous among team members.
4. Lack of integrated design process toolkit.
5. Fragmentary design and documentation platform.
6. Issues related to contractor appointed via conventional approach.
5.2.1 The KTPH Briefing Process
The KTPH case study demonstrated that a close collaboration between the medical
professionals and building professionals had developed in the project. The design
process from masterplan, through schematic design, design development phases and
extended into contruction phase may be thought about as a long, collective dialogue,
allowing the stated objectives at the start of the project to be played out against other
constraints that are not apparent in the initial brief. These includes building authorities’
requirements, budget, specific operational requirements that are only becoming visible
as building designers present the proposed internal layout, etc. As Lawson proposes,
Briefing is now generally regarded as a continuous process rather than one
which takes place exclusively at the start of the project.” (Lawson, 2004. p. 13)
The eventual developed brief listed more than 440 specific requirements, categorized
under 15 categories, much more than the 31 objectives under 9 categories at objective
setting stage (Section 3.3; CPG file document)49.
49 Updated brief compliance checklist dated Mar 2007.

125
This highlights one of the key challenges in the design of healthcare architecture:
complexity. It also illustrates that design requirements, problems or constraints are
extremely difficult to be comprehensively stated, especially at the start of the project.
Very often, they are developed and defined as the possible solutions are being tossed
about (Lawson, 2005, p. 120). Hence, KTPH demonstrated that for large scale and
complex project, there is a need for close collaboration with stakeholders, experts from
different disciplines, and key decision makers in the iterative process, because problems
often only emerged after tentative solutions are proposed (See Appendix II on team-
based design iteration).
5.2.2 Entrenched Practice among Building Professionals
Aside from the close collaboration between the medical and building professionals, the
project team members had highlighted in the focus group discussions that they
experienced a tendency among some building professionals to lapse into the
conventional behavior of linear, parallel processes. As a result, there are instances where
more straight forward design issues that building professionals could resolve among
themselves are less satisfactorily done, when far more complicated issues that require co-
learning between the healthcare and building professionals were resolve far more
satisfactorily. One likely explanation is that building professionals made assumptions
based on past experience and cut back on coordination with each other as they succumb
to time pressure; especially after committing huge amount of time and resources in the
co-learning process with the medical professionals.
This behavior tendency had occasionally crept into dealings with the medical
professionals as well. KTPH’s Wai said that one short coming of the project team
members becoming very familiar and friendly with the KTPH staff, especially towards
the later phases of the project, is the tendency for individual building professionals to
seek consent from end users to resolve localized problems quickly, without seeking the
consent of the HPT or other inter-related departments. In other words, the problems may
not have been resolved systematically or holistically. This reveals that linear-thinking,
being an entrenched mode of thinking, is not easily replaced by system-thinking.

126
5.2.3 Issues Related to Mindset Change
Gathering from the interviews, it suggests that the mindset change among team
members was also not consistent: Some are more prepared to embrace collaboration and
adopt an open-minded attitude; others less so. This may be heavily influenced by the
background and personality of individual team members, and the organizational culture
where they belong to. In addition, the visioning and objective setting were heavily
focused on the healthcare perspective. With the benefit of hindsight, some sharing or
workshop emphasizing on system-thinking, e.g. between healthcare operation and built
environment, between nature and built environment, and between building systems
within the built environment, at the very early stage of the design process would have
been beneficial.
5.2.4 Lack of Integrated Design Process Toolkit
The Integrated design process guide or toolkits, some of which were briefly explored in
Section 2.3, were not available to the KTPH project team during the project. It is believed
that such toolkit would have provided a more systematic guide to better manage the
integrated design process.
5.2.5 Fragmentary Design and Documentation Platform
Computer aided design (CAD) was used as the predominant design and documentation
platform, supported by manual sketches, disparate software analysis tools and building
performance simulation software. This had resulted in a fragmentary design and
documentation process that has typically been troubling the building industry:
coordination between different sets of drawings. The complexity of the hospital
programme has simply compound the problem and hence workload.

127
5.2.6 Issues Related to Contractor Appointed via Conventional
Approach
As the contractor was appointed in the conventional design-bid-build approach, they
were not included in the practice of integrated design. Coming on board after the tender
award, they had certainly missed most of the design iteration processes, where insights
and purpose of the project were reiterated through group dynamics and narration.50 In
addition, in keeping with the prevalent practice in the Singapore construction industry, a
large amount of construction detailed drawings were contractually the responsibilities of
the contractors, through the submission of shopdrawings to be checked by the building
professionals. In reality, the contractors simply could not cope with the demand of
designing and managing construction at the same time, especially under the intense
pressure of a fast track building programme. As a result, a significant degree of the early
good design intention faced implementation hurdles. A case in point is the need to lower
part of the ceiling heights in the wards due to the need to accommodate the M&E
services in the ceiling space, affecting the amount of daylight entering the wards.51
5.3 Discussion: the Practice of Integrated Design
Arising from the lessons learnt, further questions may be framed using Batshalom and
Reed’s IDP Mental Model (Figure 5.2), as follows:
1. Who is the leader in integrated design? Specifically, without the leadership from
AH/KTPH CEO Liak Teng Lit, would the outcome for KTPH be the same? Can
we expect the architects, recognized as the leader of the building professionals, be
able to perpetuate the sustainability agenda and integrated design leadership
roles?52
50 Appendix II provides a theoretical reference on importance of team-based design iteration,
group dynamics, client’s role in team-based design process, and conversation in team-based
design process. 51 With the benefit of hindsight, such occurrence may have been avoided if BIM was used to
coordinate the design during design development stage. This is indeed being done in some of
Singapore and CPG’s current projects. 52 Refer also to Section 2.3.1 and footnote 15.

128
2. In the process of carrying out this research, one major challenge was the
investigation of the iterative process. As much of the iterative process was done
through conversation or narration, which were never completely and
comprehensively recorded in practice, the only way to investigate is via
interview based on project team members’ recollection. To facilitate the iterative
investigation or reflection, how can the conversational or narrative aspects of
design process be better documented?
3. Without participation from contractor, the integrated design process is
incomplete. How can Singapore develop a procurement method that allows
earlier participation of the contractors and fabricators?
4. How would most holistic process change, e.g. as proposed in AIA’s integrated
project delivery (AIA, 2007) benefit integrated design and sustainable
architecture? How would it impact Singapore’s practice and industries?
There are no immediate answers to these questions, but they serve as good starting
points as research areas in the knowledge and practice of integrated design, as
recommended in the next section.
Figure 5.2 KTPH Integrated design process: questions framed with the IDP Mental Model
Who is the
leader in the
sustainability
and
integrated
design
approach?
How can the
narrative
aspect of
design
process be
better
documented?
How can
Singapore
develop a
procurement
method that
allows earlier
participation of
the contractors
and fabricators?
How would a
holistic process
change
including a
design and
documentation
platform
facilitate
sustainable
architecture?

129
5.4 Recommendations
Through the insights gained from the research, the following recommendations are
made to advance the knowledge and practice of integrated design in healthcare
architecture in the Singapore context:
1. To research into the construction and commissioning aspects of KTPH and their
impacts on the operational outcomes.
2. To conduct post-occupancy research along the triple-bottom-line approach on
KTPH’s sustainability performance, as proposed in Table 5.4. Such research will
contribute to building up the body of works necessary to support evidence-based
design premised in Singapore.
3. Conduct research into the narrative or ‘design as conversations’ (Lawson, 2005)
aspects of the integrated design process, to better understand how design though
processes and decisions are arrived at in a group setting. It will contribute to the
knowledge and hence practice of integrated design, and perhaps even spawn a
Table 5.4 Areas of study proposed for sustainability performance of KTPH
S/No. Attributes Eco Soc Env
1 Building performance in terms of energy and water saving benchmarked
against local and international data.
2 Measurement of clinician/staff morale and productivity improves due to
better physiological, psychological and sociological well-beings.
3 Measurement of patient well being and recovery time due to the social and
environmental (i.e. biophllic) attributes of KTPH.
4 Measurement of family and visitor well being due to the social and
environmental (i.e. biophllic) attributes of KTPH.
5 Effectiveness of community participation in KTPH’s community stewardship
programmes due to the social and environmental attributes in KTPH
6 Enhancement of ecological outcome, e.g. improvements in biodiversity
Eco = Economic Sustainability
Soc = Social/Human Wellness Sustainability
Env = Environmental/Ecological Sustainability

130
new field of ‘integrated design management’. 53 This may provide valuable
insights in leveraging on architect’s skills as “three-dimensional problem solvers”
(Williams, 2007, p. 14) to also be an IDP champion and/or facilitator (Section
2.3.3.1).
4. To consider and research into holistic process change suitable for the Singapore
context, for example:
Collaborative practice model with BIM as the information platform (e.g.
integrated project delivery (IPD) as proposed by AIA, 2007; see Appendix III);
Early involvement of contractor and fabricator as stakeholders. This will
require a re-thinking in the procurement and execution method for building
contracts, e.g. IPD and lean construction principles (Abdelhamid, 2008) 54.
Just as lean principles have been appropriated in the manufacturing and
healthcare practices (Carpenter, 2012), 55 the emerging application of ‘lean
principles’ in the design (Haynes, 2012) 56 and construction practices
(Abdelhamid, 2008) warrants further studies.
53 Sinclair (2008) commented that “there are very few books devoted to the management of the
architectural design process” (p. 1), and design management is “the discipline of planning,
organising and managing the design process to bring about the successful completion of specific
project goals and objectives” (Ibid., p. 4). The same rigour must surely be extended to the
integrated design process. 54 Lean construction refers to a production philosophy to minimize waste of materials, time, and
effort in order to generate the maximum possible amount of value. It requires the collaboration of
all project participants, client, consultants, contractors, facility managers, and users at early stages
of the project. This requires a new contractual arrangement where constructors and perhaps
facility managers play a role in informing and influencing the design (Abdelhamid, 2008). 55 In “Lean-Led Design: Rules of the Road”, Teresa Carpenter proposed that lean principles be
adopted as “a systematic approach to healthcare architectural design that focuses on defining,
developing and integrating safe, efficient, waste-free operational processes in order to create the
most supportive, patient-focused physical environment possible.” (Lean Healthcare Exchange,
2012) 56 In ”Adopting Lean Practices in the Architectural/Engineering Industry”, David Haynes
proposed that “lean processes in the manufacturing world could be translated in the AEC
industry through BIM” (AECbytes Viewpoint #63). He proposed that “Lean Design adopts
principles from business processes such as Six Sigma and Lean, and uses workflow techniques
that include workflow principles of Integrated Project Delivery (IPD),” by combining the data rich
information in a BIM project with new workflow techniques to increase efficiency and reduce
waste [and] become more integrated in the project and gain greater customer satisfaction.” (Ibid.)

131
Appendix I: Roles of Team Members By Design Phases
“During conceptual design, the owner is convinced
that the design team has a vision worth pursuing.
During the schematic design, the design team
convinces itself that the vision sold to the owner is
in fact feasible.”
Alison Kwok and Walter Grondzik

132
Appendix I
Source: Roadmap for the Integrated Design Process, p.107

133
Appendix I (Cont’d)
Source: Roadmap for the Integrated Design Process, p.108

134
Appendix I (Cont’d)
Source: Roadmap for the Integrated Design Process, p.109

135
Appendix I (Cont’d)
Source: Roadmap for the Integrated Design Process, p.110

136
Appendix II: Iterative Process in Integrated Design
“An iterative process allows communication at
every level, so that each team member’s design
decisions can be informed by an understanding of
how their works relate to the whole.”
7group and Bill Reed

137
Appendix II
II. Iterative Process in Integrated Design
By drawing from literature, this Appendix explores that iterative process in integrated
design as follows:
1) Design iteration in theory;
2) Team-based design iteration;
3) Various iteration methodologies to support integrated design.
1.0 Design Iteration in Theory
In ‘How Designers Think’, Bryan Lawson (2005), with inferences from earlier literature,
identified that design is an outcome of cognitive process, production process and
evaluation process; and often intertwines with these processes is the briefing process.
These are explored in Section 1.1 to 1.4.
1.1 The Cognitive Process
In the cognitive process, two types of thought processes are the most important in
design: reasoning/problem-solving and imaginative thinking. The former “requires more
attention to the demands of the external world” whilst the latter “is primarily concerned
with satisfying inner needs through cognitive activity which may be quite unrelated to
the real world” (Lawson, 2005, p. 138). This appears to echo the reseach/analysis phase of
the integrated design process (Dissertation Section 2.3.34).
1.2 The Production Process
A skilled or mature designer, with an ability to control the direction of his/her thinking,
is able to steer the thinking towards a desirable outcome, i.e. production. The two major
categories of productive thoughts are convergent and divergent production, the former
being the outcome of largely rational and logical processes, whilst the latter being the
outcome of largely intuitive and imaginative processes. “Design clearly involves both
convergent and divergent productive thinking, and studies of good designers at work

138
have shown that they are able to develop and maintain several lines of thoughts in
parallel” (Ibid., p. 143).
Lawson has also pointed out by way of the process of designing a window (Fig II-1) that
good design is often an outcome of integration. When dealing with a design as complex
as a building, in which there are many inter-related issues (or for Lawson, constraints),
there are many possibilities towards a well-integrated solution, and designers tend to
deal with it in two ways: generation of alternatives and by employing several ‘parallel
lines of thoughts’. ‘Parallel lines of thought’ is a phrase first used by Lawson (1993) to
describe a parallel examination into different aspects of the same design, for example,
“investigating detail and large scale issues in parallel” (Lawson, 2005, p. 212), or say,
developing and sustaining “many incomplete and nebulous ideas about various aspects
of their solutions” (Ibid., p. 212), and traits of creative thought processes are often
observed in both. At this juncture, it is also important to recognize that in the generation
Figure II-1 The whole host of issues to be considered in designing a window: one of the many
component and part of some inter-related systems in a building. Source: Lawson, 2005, p. 59
Appendix II (Cont’d)

139
of these alternatives, the designers are guided by their individual interests, approaches
and strategies as well as responding to requirements or constraints imposed by
legislation, clients, other consultants, and users (directly or indirectly); there are hence
many possible routes in the creative thought process (Ibid.). The generation of multiple
alternatives of thoughts allows the interplay between the values, issues, requirements,
problems and constraints to be tested visually, either as diagrammes, 2D drawings or 3D
visual rendering, on paper or computer/video display, as well as through conversation
(Ibid.). With reference to the integrated design process, this may possibly take place in
the reseach/analysis phase, or the workshop/charrette sessions of the integrated design
process (Dissertation Section 2.3.3.4).
1.3 The Briefing Process
Intertwines in the production process is often, but not always, a parallel process known
as the briefing process (Ibid.). In theory, the idealized design process assumes that a clear
design brief is established before the design even started. This assumption is based on
the premise that the design end product is a solution to some sort of problems, or needs,
hence the design problems or needs have to be defined up front (Ibid.). In practice,
however, it is found that design problems are often never fully described at the start of
the design process. Even if it is described in details, it often changes and evolves, because
the design process actually begins to develop the brief as it formulates a solution (Ibid.).
This is because good design often deal with the multiplicity of the values, issues,
requirements, problems and constraints by employing “a very few major dominating
ideas which structure the scheme and around which the minor considerations are
organized.” (Ibid., p. 189) The early generation of alternatives or parallel lines of
thoughts allows the interplay of values, issues, requirements, problems and constraints
to be tested and visually communicated with the project stakeholders: clients,
consultants, and sometimes builders and users. Such iterative process often helps to
shape and crystallize the brief:
Appendix II (Cont’d)

140
“…both empirical research and anecdotal evidence gathered from practising
designers suggest that the early phases of design are often characterised by what
we might call analysis through synthesis. The problem is studied not in minute
detail but in a fairly rough way as the designer tries to identify not the most
important (to the client) issues, but the most crucial in determining form. Once a
solution idea can be formulated, however nebulous it may be, it can be checked
against other more detailed problems.” (Lawson, 2005, p.p. 197-198)
“It is interesting that these and other designers studied who use the generation of
alternatives, often show them to their clients. This seems to become part of the
briefing process; a way of drawing more information out of the client about what
is really wanted.” (Ibid., p. 210)
An understanding of the briefing process in KTPH may be gained by reading Sections
3.3 and 5.2.1 of this dissertation.
1.4 The Evaluation Process
Eventually, the ideas produced will need to be evaluated, and decisions of which ideas
to be adopted and integrated into a holistic solution will have to be made. “Designers
must be able to perform both objective and subjective evaluations and be able to make
judgements about the relative benefits of them even though they may rely on
incompatible methods of measurement” (Ibid., p. 298). For the integrated design process,
this is recommended to take place in the all-stakeholders workshop sessions
(Dissertation Section 2.3.3.4).
2.0 Team-Based Design Iteration
So far, the designer has largely been described as a person. With the exception of small
scale projects e.g. single-family house, building projects usually involve many people in
a design team, comprising architects, who are likely to have team members focusing on
different aspects of the project, as well as civil & structural engineers, mechanical &
Appendix II (Cont’d)

141
electrical engineers, and possibly many other specialized consultants, such as quantity
surveyor, landscape architect, interior designer, lighting consultant, acoustic consultant,
etc. Many of them will handle a certain aspects of design.
This brings about a second characteristic of design in practice, which is vital to team-
based integrated design process: besides being a cognitive process, design is also a social
process, “in which the rapport between group members can be as significant as their
ideas.” (Ibid, p. 240)
“Both the individual specialist teams and the overall project team can be seen to
exhibit group dynamics, and to behave not just as a collection of individuals. An
examination of professional diaries is likely to show that most architects spend
more time interacting with other specialist consultants and fellow architects, then
working in isolation.” (Ibid., p.239)
2.1 Group dynamics
It is hence worthwhile to explore the notion of group dynamics. A group acts “not just as
a collection of individuals, but also in a manner somehow beyond the abilities of the
collective individual talents” (Ibid., 239). What characterize a group are:
1) They share a common goal;
2) They develop a set of norms, which guide their behavior and activities;
3) They develop interpersonal relationships.
The development of group norms leads to a suppression of the individuality of its
members, “in favour of an expression of attachment to the group” (Ibid., p.244). As
norms developed over time, often through conflict resolution, it results in a common
perception of the group’s goal and individuals acquiring and accepting roles within the
group, and these “roles simultaneously often help to facilitate the business of the group
and become part of the folklore which binds the group together” (Ibid., p. 246).
Appendix II (Cont’d)

142
Many high-performing design practices are found to be also strong social groups,
formed after overcoming internal strives or external challenges. They developed “shared
language and common admiration for previous design work” (Ibid., p. 250), and relied
heavily on the “sharing of concepts and agreed use of words which act as a shorthand
for those concepts.” (Ibid., p. 250) The intensity of the design process demands that such
shorthand be used during conversations. At the same time, the social nature of team
work, the communication and co-operation in realizing design as a collective process is
rewarding for many designers (Ibid.).
2.2 The Client’s Role in Team-Based Design Process
The benefits of group dynamic often extend to include the client:
“Behind every distinctive building is an equally distinctive client.” (Michael
Wilford, in Lawson, 2005, p. 254)
Many designers value continual engagement with the client, in the process developing a
trusting relationship with client. From the client’s perspective, trust is needed because
building professionals are designers that clients “expect to be protected from his or her
own ignorance by such a professional” (Lawson, 2005, p. 255). From the designers’
perspective, without trust, creativity and innovation in design is unlikely to take place,
as any thought or process perceived as uncertain, ambiguous, and vague, will be
doubted or rejected by the client, which undermines the very nature of the divergent
thinking process (Ibid.).
In big projects, client is often also represented by a group or committee. Needless to say,
client group or committee that experiences frequent changes in its members would suffer
setback in the trust-building process, as well as potential reduction in commitment to the
project by both client and designer (Ibid.).
Appendix II (Cont’d)

143
2.3 Conversation and Perception in Team-Based Design
During the production process, it is noteworthy that “good designers are able to sustain
several ‘conversations’ with their drawings, each with slightly different terms of
reference, without worrying that the whole does not yet make sense. This important
ability shows a willingness to live with uncertainty, consider alternative and perhaps
even conflicting notions, defer judgement, and yet eventually almost ruthlessly resolve
and hang on to the central idea” (Ibid., p. 219). While such traits are valuable to an
individual designer, the ability to conduct design as a conversation becomes even more
crucial in a team design process.
In large or complex project e.g. hospital in which a multi-disciplinary design team is
required, including professionals and experts from different fields, increased
conversations between team members enable the following to take place:
1) Build up trust;
2) Identify the central elements of the design through a narrative process (Ibid., p.
267);
3) ‘Negotiate’ to reconcile conflicts in ideas and concepts, enabling the team to
navigate from problem to solution. “The parties come into the negotiation taking
different views and having different objectives but with a willingness to reach
some form of agreement that all parties can accept” (Ibid., p.271)
4) To communicate shared experience, e.g. shared concepts, past problems and
solutions, etc. These shared concepts are transmitted via conversational
‘shorthand’ to facilitate the intense iteration process in design. At the same time,
such shared experience helps to forge social bond between the design team
members.
Appendix II (Cont’d)

144
2.4 The Problem and Solution Views in Team-Based Design
The conversational nature of the design process is seen also in the ‘negotiation between
problem and solution’. This leads to the heart of the design process, which led Lawson to
state that:
“...designers tend to be ‘solution focused’ rather than ‘problem focused’ in their
approach…they tend to acquire considerable stores of knowledge about solutions
and their possibilities and affordances.
So designers have the task of negotiating reconciliation between these two views
of the situation they are dealing with. The problem view is expressed generally in
the form of needs, desires, wishes and requirements. The solution view on the
other hand is expressed in terms of the physicality of materials, forms, systems
and components…We do not see designing as a directional activity that moves
from problem through some theoretical procedure to solution. Rather we see it as
a dialogue, a conversation, a negotiation between what is desired and what can
be realized” (Ibid., p.p. 271-272).
Conversation 57 is engaged between the designer and his/her sketches, drawings,
computer visualization. In team-based design, conservation through words as well as
drawings and visual representation is likewise engaged between the designer and
paying client, between fellow designers, and between designer and users. In an extensive
process, the conversation may also be engaged between the designer and builder, and
between the designer and product/component manufacturer. The early involvement of
builders and manufacturers are advocated in the integrated design approach, and the
experience from KTPH appears to support such an advocacy. In the KTPH project, the
conventionally appointed contractors, being late comer on the project, did not enjoy the
57 This ‘conversation’ may also be understood as ‘iteration loops’ (Heiselberg and van der Aa,
2010).
Appendix II (Cont’d)
145
benefits of early involvement and hence understanding the design objectives and
processes (See Chapter 5 of this dissertation).
It is also important to note that:
1. Design problems tend to be organized hierarchically (Lawson, 2005, p. 121).
While there is no fixed or logical sequence to tackle the problems, it is generally
sensible to tackle the problems that imposed the most constraints, before
progressing to those with lesser constraints. This is supported by van der Aa,
Heiselberg and Perino’s interative design model (Section 3.2 of this Appendix),
and validated through the examples examined for the KTPH case study: the site
layout and massing form and proportion was first determined in the masterplan
stage, followed by envelope design for the various blocks in the schematic and
early design development stage, before system design and component design in
the late design development stages were carried out.
2. Design problems58 require subjective interpretation (Lawson, 2005, p. 120-121).
What seems important to one client in one project may not be necessary so to
another client or in another project. Communication and establishing mutual
understanding is required.
Lawson has also written about the continuous and interacting relationship between
problem-definition and solution-finding in the design process:
1. Since design problems cannot be comprehensively stated, there are an
inexhaustible number of design solutions (Lawson, 2005, p. 121).
2. There is no ‘one best’ solution to design problems; many acceptable solutions are
possible, “each proving more or less satisfactory to different client and users”
(Lawson, 2005, p. 121-122).
58 ‘Design problems’ here may also be understood as ‘design requirements’, ‘design constraints’,
‘design issues’, and/or ‘design challenges’.
Appendix II (Cont’d)

146
3. Design solutions are often holistic responses (Lawson, 2005, p. 122).
4. Design solutions are a contribution to knowledge (Lawson, 2005, p. 122).
5. Design solutions are parts of other design problems (Lawson, 2005, p. 122-123).
This leads to the need to involve stakeholders, experts from different disciplines, and key
decision makers in the iterative process, because problems often only emerged after
tentative solutions are proposed. This is especially the case for a large, complex project
with highly specific requirements such as a hospital.
2.5 Mindset and Cultural Change Needed in Team-Based Integrated
Design
The problem-solution model of the design process is also put forth by Michael Brawne
(2003), who sees a parallel in the cyclical design sequence in the Popperian59 sequence of:
P1 TS EE P2 (Problem recognition, Tentative Solution, Error Elimination, best
corroborated solution which becomes the problem to the next sequence). It is important
to note that in the design process, “the starting problem can occur both within and
outside architecture but more often than not manifests itself as a problem in architecture
irrespective of its origin…We start with a verbally stated problem but very soon have to
shift into non verbal-thinking” (Brawne, 2003, p.p. 33-35). This underscores the
quintessence of architectural design: the need to recognize a host of problems (often
fragmentary and inter-contradicting), which are initially describable only in words (and
sometimes inaccurately described or scantly described), test it through one or more
tentative solutions (multiple line of thoughts) that are by necessity expressed in ‘non-
verbal’ terms (e.g. drawings, computer models, physical models), before it could be
evaluated (‘error-elimination’; is it acceptable to client? Does it comply with codes and
59 Named after Sir Karl Raimund Popper. In ‘All Life is Problem Solving’, the Popperian sequence
(PS1 TT EE PS2) was proposed as a model for scientific advancement, in which the degree
of ‘truth’ in scientific theories are only true for its time (TT, tentative theories); further research
and processes (EE, error elimination) will always yield better theories. In such cyclical process,
scientific knowledge thus advances from lower grade problem situations towards higher grade
ones (PS1 to PS2).
Appendix II (Cont’d)

147
regulations? Are there conflicts between different disciplines?), before it is deemed to be
acceptable for further development (a holistic ‘corroborated solution’; an overall solution
that integrates the host of solutions to the problems that had been recognized).
It is also noteworthy to note that in “the design sequence P1 to P2, a great many initial
problems are self imposed and often arise from visual choices” (Ibid., p. 259). He
described the way many architects design:
“Before we use models in the tentative solution, in the design stage, we are
involved in problem selection. We cannot and do not solve all the problems
which exist at that time in that project…There are the demand set by the brief
which require resolution but in addition to that we ourselves see problems or
have leanings to particular resolutions which makes for individual
responses…Problem recognition and what is imaginable are conditioned by the
world around us.
It is the severity and nature of the self-imposed problems which are the test of
architectural greatness. To satisfy the architectural programme of space,
adjacencies, circulation, service provision and so on is a difficult and necessary
task. It is the basis of much design. In the last resort, however, it is a
journeyman’s task…Poetry and delight are the task of the master and arise from
self-imposed necessities. It is also the solution of the problems which we set
ourselves which produces the greatest agonies and delight of design.” (Brawne,
2003, p. 62)
What Michael Brawne has just described, is perhaps the ‘secret’ to how architects have
rather universally been taught and practiced; the values first transferred from teacher to
student in architectural school, and later from master to apprentice in practice. It is by
nature a rather self-centred process, which presents a challenge to the integrated design
process (IDP), as IDP demands that architects fundamentally alter their role, to listen and
be open-minded to admit inputs from many other sources. “But giving up control goes
Appendix II (Cont’d)

148
against everything architects are taught” (Deutsch, 2011, p. 136). Feedback received from
green consultant Alvin Woo from CPGreen, CPG Consultants’ environmental
sustainability studio appears to reflect this, “Many of the external enquiries requesting
for our involvement are projects that architectural concept design have been determined.
There is often a limit to what we could offer, especially in passive response to site and
climate, without requiring some fundamental changes to the architectural concept.”
On the other hand, there is a reluctance among the engineers to contribute in a more
broad-based manner. Some, if not most practising engineers in Singapore appeared to
have been conditioned to start thinking only after the architectural concept design had
been generated and handed off to them. The other common trait observed from M&E
engineers, perhaps reflecting the challenges they are confronted with, is the tussle
between the concern for ‘under-performing design’ and the need for ‘innovative
engineering approach’ which is often perceived as ‘untested method’, ‘high risks’, and
‘unknown liabilities’. In addition, the disconnect between the engineers and the
construction and manufacturing companies in Singapore practice further exacerbates the
problem. While engineers provide general design, the actual design and installation had
to be tendered out and worked on by the contractors and manufacturers who won the
tender, based on the actual product or construction method used. The opposing
positions between the clients (who wish to pay less) and contractors/manufacturers (who
wish to claim for more) often leads to adversities and disputes, with engineers caught
out between two parties. In the healthcare context, complexity in the M&E systems
simply further amplifies the challenges.
Jerry Yudelson pointed out that,
“Integrated design is not as easy as changing your shirt every day; old habits die
hard. To me, it appears that air-conditioning has made mechanical engineers
reactive for decades, because no matter how the architect designs the building,
they can still provide more or less adequate comfort by adding air-conditioning
tonnage. There are also the risks of trying new things; every departure from
Appendix II (Cont’d)

149
‘normal’ design practices, no matter how intelligent, runs the risk of a lawsuit if
things don’t work out as planned. To make integrated design work, the team
often has to challenge prevailing codes. This is how progress is made, but it isn’t
easy or fast.” (Yudelson, 2009, p. 63)
As a result, for the integrated design approach to be successful, it has to start with
mindset change and alignment from all stakeholders, including client, architect,
engineers, specialist consultants, users, and many other stakeholders (See Section 2.3.2 of
this dissertation). The mindset change needs to be supported by social techniques:
fostering collaborative spirit through a healthy, encouraging and trusting social process
and group dynamics as explored in Section 2.1 to 2.3 of this Appendix, and Section
2.3.4.2 of this dissertation. In addition, the team-based iterative process may be facilitated
by iterative tools or methodologies, which are explored in the next section.
3.0 Methodologies in Integrated Design Iteration
The design iteration methodology is an emerging field, and this section examines some
of the methodologies, as follows:
1) ‘Integrated Design Process’ (IDP) by Sustainable Built Environment (iiSBE)
2) ‘Strategies for Integrative Building Design’ (Heiselberg and van der Aa, 2010)
3) ‘Rethinking the Design Process’, a presentation by Konstrukt (2006)
3.1 ‘Integrated Design Process’ (IDP) by Sustainable Built
Environment (iiSBE)
The International Initiative of Sustainable Built Environment’s (iiSBE) ‘Integrated Design
Process’ (IDP) claimed that IDP “contains no elements that are radically new, but
integrates well-proven approaches into a systematic total process” (Larssons, 2004, p. 2).
The salient point to highlight in the iiSBE IDP process is the presence of ‘feedback loops’
in its process (Figure II-2), which is a form of team-based iterative process.
Appendix II (Cont’d)

150
Appendix II (Cont’d)
The feedback loops in Figure II-2 illustrate the inter-activity between building envelope
design, daylighting/lighting design, power design, ventilation, heating, and cooling
design. Throughout the iteration, the focus is on the performance targets established for
a broad range of parameters and as consensus between designers and client (Ibid., p.p. 2-
3). Specific recommendations by IDP pertaining to team-based iteration include:
1) “Iterate the process to produce at least two, and preferably three, concept design
alternatives, using energy simulations as a test of progress, and then select the
most promising of these for further development” (Ibid., p. 3).
2) “Budget restrictions applied at the whole-building level, with no strict separation
of budgets for individual building systems, such as HVAC or the building
structure… extra expenditures for one system, e.g. for sun shading devices, may
reduce costs in another systems, e,g, capital and operating costs for a cooling
system” (Ibid., p. 2).
Figure II-2 iiSBE Integrated Design Process. Source: iiSBE (Larsson, 2004)

151
3) “[T]he addition of a specialist in the field of energy engineering and energy
simulation” (Ibid., p. 2).
4) “[T]esting of various design assumptions through the use of energy simulations
throughout the process, to provide relatively objective information on this key
aspect of performance” (Ibid., p. 2).
3.2 ‘Strategies for Integrative Building Design’
Heiselberg and van der Aa’s (2010) model of the iteration loop has been briefly presented
in Section 2.3.3.4 of the dissertation. The objective of the iteration is to achieve what they
termed as “responsive building concepts” (Ibid., p. 2), which refer to
“[D]esign solutions in which an optimal environmental performance is realized
in terms of energy performance, resource consumption, ecological loadings and
indoor environmental quality. It follows that building concepts are design
solutions that maintain an appropriate balance between optimum interior
conditions and environmental performance by reacting in a controlled and
holistic manner to changes in external or internal conditions and to occupant
intervention and that develop from an integrated multidisciplinary design
process” (Ibid., p. 2).
They proposed that an integrated building concept can be defined to consist of three
parts: an architectural building concept, structural building concept, and an energy and
environmental building concept (Ibid., p. 2, Figure II-3).
Figure II-3 Integrated Building Concept. Source: Heiselberg and van der Aa (2010).
Appendix II (Cont’d)

152
Appendix II (Cont’d)
To achieve that, a multi-disciplinary approach is required to develop various design
strategies (Ibid., p. 6, Table II-1), from macro to micro, from broad-based to specific
details, through the design phases (Ibid., p. 8, Figure II-4).
Table II-1 Typical design considerations at each design phase.
Source: Heiselberg and van der Aa (2010).

153
Similarly, Heiselberg and van der Aa propose that ‘iteration loops’ (Figure II-5) are
expected to characterize each of the design phases, allowing ‘tasks’ (‘problems’ in Section
2.4 of this Appendix) and ‘results’ (‘solutions’ in Section 2.4 of this Appendix) to be
iterated “taking into consideration input[s] from other specialists, influences from
context and society that provide possibilities and/or limitations to design solutions as
well as evaluates the solutions according to the design goals and criteria” (Ibid., p. 8).
Figure II-5 ‘Iteration loops’ as proposed in ‘Strategies for integrative building design’ (van der
Aa, Heiselberg and Perino, 2011). [This author is of the view that ‘Coal’ in the diagramme is a
typological error and show read as ‘Goal’ instead].
Appendix II (Cont’d)
Figure II-4 Iterative Process. Source: Heiselberg and van der Aa (2010).

154
3.3 ‘Rethinking the Design Process’
In ‘Rethinking the Design Process’, a presentation by Konstrukt (2006), they propose that
integrated design is a “systems approach [that] has the potential to create buildings with
lower first costs and large energy savings” (Ibid., slide 2), and that the “fundamental
process of integrated design is the search for synergies. Synergistic strategies create
benefits greater than the sum of the individual design decisions” (Ibid., slide 3). Their
primary concern is building energy consumption, which is defined as a function of
climate, building use, and site & building design (Figure II-6).
They presented a succinct approach – a ‘design attitude’– of a double strategy of (Figure
II-7):
1) Reducing energy load demand, say by 50% e.g. through good bioclimatic and site
response, adopts passive design strategies, right-sizing of user receptacle load,
etc;
2) Doubling system efficiency.
Figure II-6 Building energy loads as presented in ‘Rethinking the Design Process’.
Source: Konstruct (2006).
Appendix II (Cont’d)

155
Such thinking conceptually demonstrates that an ambitious objective of reducing energy
consumption to 25% of a typical, conventional design is plausible, and along the way
perhaps even resulting in cost saving in the system designs (Ibid.). This simple and
succinct approach is indeed an effective way to establish the right shared ‘mindset’
among the stakeholders, an important first step that leads to team visioning and setting
high objectives. Such objectives have to be supported by team collaboration and
integrated design. Konstruct proposed a model to understand the components of
integrated design process, comprising: design topics, iterative process, energy topics,
and tools & data to find synergies (Figure II-8 and Figure II-9). While not explicitly
stated, the iterative process is expectedly multi-disciplinary and team-based, in order to
meet the diverse range of knowledge and skill sets needed for the problem definition,
solution finding, and search for synergies (Figure II-9).
“The heart of the integrated design process…is the search for synergies between
two or more attributes of climate, use, design, and systems, that will result in
combined performance, exceeding the sum of their individual performances, and
reduce project first cost and operating expense.”
(Konstruct, 2006)
Appendix II (Cont’d)
Figure II-7 Approach to reduce energy consumption as presented in ‘Rethinking the Design
Process’. Source: Konstruct (2006), slide 10.

156
Figure II-9 The search for synergies between two or more attributes of climate, use, design, and
systems as presented in ‘Rethinking the Design Process’. Source: Konstruct (2006).
Figure II-8 Components of integrated design process presented in ‘Rethinking the Design
Process’. Source: Konstruct (2006).
Appendix II (Cont’d)

157
Appendix III: Building Information Modelling
“A BIM methodology seeks to adapt to the added
layers of information, allowing new methods of
data exchange and communication amongst all the
stakeholders in a project. This can be the design
team (designers and consultants), builders
(contractors and subcontractors), and owners
(developers and facility managers)…The goal of a
BIM methodology is to allow an overall view of the
building or project by including everything in a
single-source model.”
Eddy Krygiel and Bradley Nies

158
Appendix III
III. Building Information Modeling
By drawing from literature, this Appendix briefly explores the relationship between
building information modeling (BIM) and integrated design, sustainable design and its
relevance to practice, as follows:
1) Brief Definition of BIM.
2) BIM, integrated design and sustainable design
3) BIM and integrated project delivery (IPD) (AIA, 2007).
1.0 Brief Definition of BIM
Krygiel and Nies (2008) defined BIM as, “an emerging tool in the design industry that is
used to design and document a project, but is also used as a vehicle to enhance
communication among all the project stakeholders” (p. 25). It is first and foremost an
informational technological (IT) platform for building design and documentation with
the characteristics summarized in Table III-1.
But more importantly, it entails an entire re-think in workflow in order to fully harness
its benefits (Table III-2). The main challenge being confronted in the industry, is not
technological in nature, but a resistance to work flow change due to mindset and attitude
(Deutsch, 2011, p. x; Figure III-1 and III-2). Since it needs to be approached as a change in
“method and workflow” (Krygiel and Nies, 2008, p. 43), it shares many similarities with
the need for mindset change in integrated design, as presented in the next section.
Table III-1 Characteristics of BIM.
S/No. Event
1. “BIM is information about the entire building and a complete set of design documents stored in an
integrated database” (Ibid, p.26) [Italic emphasis by author].
2. “All the information is parametric and thereby interconnected” (Ibid, p.26) [Italic emphasis by
author].
3. “Any changes to an object within the model are instantly reflected throughout the rest of the project
in all views” (Ibid, p.26) [Italic emphasis by author].
4. “A BIM model contains the building’s actual constructions and assemblies rather than a two-
dimensional representation of the building that is commonly found in CAD-based drawings”
(Ibid, p.26) [Italic emphasis by author].
5. “A BIM model can be holistically used throughout the design process and the construction
process.” (Ibid, p.27).
6. BIM methodology allows

159
Appendix III (Cont’d)
Table III-2 Benefits of BIM. Source: Krygiel and Nies (2008)
S/No. Event
1. 3D Simulation versus 2D representation (Ibid, p.34): permitting clashes of building
elements and components to be viewed in virtual 3D space on computer display.
2. Accuracy versus estimation (Ibid, p.34): By allowing the building design to be
constructed virtually before its physical implementation, “BIM adds a layer of accuracy
to both building quantities and qualities” (Ibid, p.p. 34-35).
3. Efficiency versus redundancy (Ibid, p. 35): By adding building objects to the design
once, instead of drawing the same object in different views, time saving is achievable.
4. Intelligent representation: “A BIM model contains the building’s actual constructions
and assemblies rather than a two-dimensional representation of the building that is
commonly found in CAD-based drawings” (Ibid, p.26) [Italic emphasis by author].
5. Project lifecycle: “A BIM model can be holistically used throughout the design process
and the construction process.” (Ibid, p.27)
6. Integrated document: “As all of the drawings in a BIM model are placed within the
single, integrated database or model, document coordination becomes relatively
automatic” (Ibid, p.38).
7. Design visualization: Since the model is in 3D, it can be viewed and turn around for
visual examination, unlike 2D drawings which are susceptible to subjective
interpretation and miscommunication, especially if lay persons (e.g. users) are involved
(Ibid, p.38).
8. Material database: Since BIM model is also a database of the virtual building, if the
models of building components and assemblies are created with their physical
properties, automation of scheduling and quantity take off can be achieved (Ibid, p.39).
9. Sustainable strategies: The building geometry from the model may be used internally
within BIM or exported for analysis to support sustainable design, e.g. energy modeling
and daylight modeling (Ibid, p.40).
10. Construction planning: Contractor familiar with BIM can utilize the model for
visualization, planning and coordination, to avoid errors and waste during
implementation. It may also facilitate digital workflow from design to fabricator, since
the information is all in 3D (Ibid, p.40).
11. Postoccupancy and facilities management: The BIM model may be utilized by building
owner and facilities managers for asset management and equipment tracking (Ibid,
p.40).
Figure III-1 Common erroneous perception is that BIM is primarily a technology change (left).
Instead, Deutsch (2011) argued that in reality, BIM is about sociological change, involving
“practical, attitudinal, and behavioral changes.” Source: Deutsch (2011), p. x.

160
Appendix III (Cont’d)
2.0 BIM, Integrated Design and Sustainable Design
The case for integrated design has been made in Chapter 2 of this dissertation. The
causes that give rise to the needs for integrated design and BIM are in fact quite the same:
specialization and fragmentation of the building knowledge and technologies, and hence
a need for integration. To support sustainable design, new specialized knowledge and
‘design layer’ e.g. solar analysis model, energy model, daylighting model have indeed
added additional design layers and complexity to the traditional physical design model,
digital design model, authority submission documentation and construction
documentation (Ibid, p.p. 46-52; Figure III-3). All intent and purpose of BIM is to
facilitate and streamline an integrated workflow (Figure III-4). As BIM processes
Figure III-2 “The business and technology cases for BIM and integrated design have already
been made. It is time to make the social case for firm culture, including working relationships,
interactions, and intelligence.” Source: Deutsch (2011), p. xi.
Figure III-3 Layers of design information. Source: Krygiel and Nies (2008), p. 55.

161
becomes truly ‘owned’ in practice, higher productivity, higher quality work, and new
possibilities, e.g. integrated design and sustainable design become attainable (Deutsch,
2011; Figure III-5).
Appendix II (Cont’d)
Figure III-5 BIM as processes. Deutsch (2011), p. 6.
Figure III-4 BIM Roadmap. Source: Krygiel and Nies (2008), p. 52.

162
Appendix III (Cont’d)
3.0 BIM and Integrated Project Delivery
Developed by the American Institute of Architects (AIA), Integrated Project Delivery
(IPD) “is a project delivery approach which integrates people, systems, business
structures and practices into a process that collaboratively harnesses the talents and
insights of all participants to optimize project results, increase value to the owner, reduce
waste, and maximize efficiency through all phases of design, fabrication and
construction” (AIA IPD Guide, 2007). It has an ambitious aim to not only incorporate
design into its process, but goes beyond that to attempt to bridge the gap between design
and construction (Ibid.)
In the IPD process map (Figure III-6), the full project team is identified and involved
much earlier in the process, including the builders and fabricators. More time is spent in
the design phase, to allow team-based integrated design process to take place, with ideas
Figure III-6 Integrated Project Delivery Process versus Traditional Process
Source: Integrated Project Delivery: A Working Definition, (2007), pp. 4.

163
supported by and tested out using a variety of tools, e.g. sketches, technical calculations,
computer modeling and simulations. In contrast, the documentation, buyout (client
approval) and agency (authority approval) phases require less time based on a set of
well-resolved detailed design document (IPD Working Definition, 2007).
Although it is not a mandatory tool, BIM is explicitly stated and promoted in IPD. Figure
III-7 by Autodesk, a BIM software vendor, illustrates the utilization of BIM throughout
the IPD project life cycle.
IPD represents a substantial industry-wide process change, and its principles, values and
relevance for the Singapore context need to be further examined.
Appendix III (Cont’d)
Figure III-7 Integrated Project Delivery with BIM. Source: Autodesk (2008).

164
Appendix IV: Design Consortium of the KTPH Project
“The process and science of building design has
become increasingly more complicated in recent
years. It has continually become less possible for
designers to work without the aid of other
specialists, be they consultants or contractors.
The trend toward concentrated areas of expertise
has led to a growing movement to combine the
owner, designer, contractor, consultants, and key
subcontractors into an integrated design team.”
Eddy Krygiel and Bradley Nies

165
Appendix IV
IV Design Consortium of the Khoo Teck Puat Hospital Project
Key Project Team Members (team members interviewed in focus group discussions are
highlighted in bold)
Role Company Name
Khoo Teck Puat Hospital Users
(Medical Professionals) AHPL
Liak Teng Lit
Chew Kwee Tiang
Pang Weng Sun
Francis Lee
Wong Moh Sim
Low Beng Hoi
Yen Tan
Ng Kian Swan
Donald Wai
Koh Kim Luan
Cynthia Ong
Sim Siew Ngoh
Esther Yap
Lye Siew Lin
Poh Puay Yong
Rosalind Tan
Project Manager PMLink Pte Ltd
Chong Choon San
Tan Kok Siong
Puah Chin Yee
Yip Sing Keat
Jean Yeo Fei Shien
Albin John
Building Professionals
Project Director/Architect CPG Consultants Pte Ltd Lee Soo Khoong
Architect CPG Consultants Pte Ltd
Lim Lip Chuan
Pauline Tan
Jerry Ong
Kanda Narasimhan
Cherilyn Chan Yin Yuet
Mahesh M G
Healthcare Architectural
Consultant RMJM Hillier
Peter Schubert
Sung Won Lee
Noah Burwell
Medical Planner Medical Planning Research (MPR)
International Ray Skorupa
Civl & Structural Engineer CPG Consultants Pte Ltd
Soon Chern Yee
Tan Swee Keng
Sumay Tan
Mechanical Engineer CPG Consultants Pte Ltd
Toh Yong Hua
V Devaraja
Heng Chen Han
Electrical Engineer CPG Consultants Pte Ltd Wong Lee Phing
Melvin Yap
Green Building Consultant Total Building Performance Team Dr Lee Siew Eang
Landscape Consultant Peridian Asia Pte Ltd Glenn Bontigao
Quantity Surveyor CPG Consultants Pte Ltd
Yeo Tiong Yeow
Tan Hui Choo
Raymond Koh Kok Yong
Interior Design Consultant Bent Severin & Associates Pte Ltd Grace Soh, James Wong
Facade Consultant Aurecon Singapore (Pte) Ltd Lily Low, Sigmund Mendiola
Wayfinding Consultant Space Syntax Australia PTY Ltd Martin Butterworth
Signage Consultant Design Objectives Pte Ltd Ronnie Tan, Lawrence Tong

166
Appendix V: Interview Guide
“What is this mysterious label and what does it
mean? How do you know you really are practicing
integrative design or not? How does a client know
who to believe when selecting a team?”
Barbra Batshalom

167
Appendix V
A. Based on Whole System Integrated Process (WSIP, 2007), the process stages in IDP may be categorized
as follows:
Stage Elements
1. Team Formation “Fully engage Client in the design decision process.”
“Assemble the right team.”
Key attributes in team formation is ‘teachable attitude’; members come on board not as experts
but co-learners.
2. Visioning “Align team around basic Aspirations, a Core Purpose, and Core Values.”
3. Objectives Setting “Identify key systems to be addressed that will most benefit the environment and project”
“Commit to specific measurable goals for key systems”
Compile into a Sustainable design brief
Key attributes in objective setting is to involve all participants, including the main financial
decision maker, not unempowered representative. Also, identify champions for the objectives
and issues.
4. Design Iteration “Optimization of the design of systems”
Key attributes in objective setting is to “understand and make best use of key systems in
relationship to each other, to the goals, and to the core purpose”, and “Iterate ideas and systems
relationships among team with all participants, including the main financial decision maker.”
5. Construction &
Commissioning
“Follow through during the Construction Process.”
“Commission the project.”
6. Post-occupancy Feedback
Loops
“Maintain the system.”
“Measure performance and respond to feedback - adjust key aspects of the system accordingly.”
B. Based on Roadmap for the Integrated Design Process (Roadmap IDP, 2007), team organization are
compared between conventional and integrated design team:
1.
2.
Q Which one do you think better describe KTPH design/project team organization? Answer (1 or 2): _______

168
Appendix IV (Cont’d)
C. Based on Whole System Integrated Process (WSIP, 2007), team organization are compared between
conventional and integrated design team:
1.
2.
Q Which one do you think better describe KTPH design/project design process? A: ______________
D. Are you familiar with the following integrated design/whole design process or methologies:
S/No. Factors During KTPH
project (Yes/No)
Now
(Yes/No)
1. iiSBE’s C2000 Program to Integrated Design Process (IDP) (Larsson, 2004). A roadmap
basing on the IDP, developed by Busby Perkins+Will and Stantec Consulting for the British
Columbia Green Building Roundtable, Canada
2. The Integrative Process (7Groups et al, 2009) that seeks to optimize ‘the interrelationships
between all the elements and entities associated with building projects in the service of
efficient and effective use of resources.’
3. Whole Systems Integrated Process Guide for Sustainable Buildings & Communities
(ANSI/MTS Standard WSIP 2007). Developed by a committee of practitioners and gained
approval as a public standard in US, it ‘codifies the meaning, importance, and practice
structure of an Integrated Design Process’.
4. Road Map for the Integrated Design Process’ (Busby Perkins+Will and Stantec Consulting,
2007). Developed for British Columbia Green Building Roundtable, Canada, to serve as an
industry practice guide. It is divided into two parts: Part One: Summary Guide; and Part
Two: Reference Manual. Part One provides an overview of IDP, while Part Two is intended
to serve as a reference manual.
5. The Integrated Design Process in Designing with Responsive Building Elements (van der Aa,
Heiselberg and Perino, 2011). Published under the IEA (International Energy Agency)
Energy Conservation in Buildings and Community Systems (ECBCS) Programme.
6. The Whole Building Design Guide (WBDG) (Prowler, 2011) is a web-based Whole Systems
Integrated Process Guide for Sustainable Buildings & Communities (ANSI/MTS Standard
WSIP 2007). Developed by a committee of practitioners and gained approval as a public
standard in US, it ‘codifies the meaning, importance, and practice structure of an Integrated
Design Process’.
7. Integrated Project Delivery (IPD) developed by American Institute of Architects (Integrated
Project Delivery: A Guide, 2007).
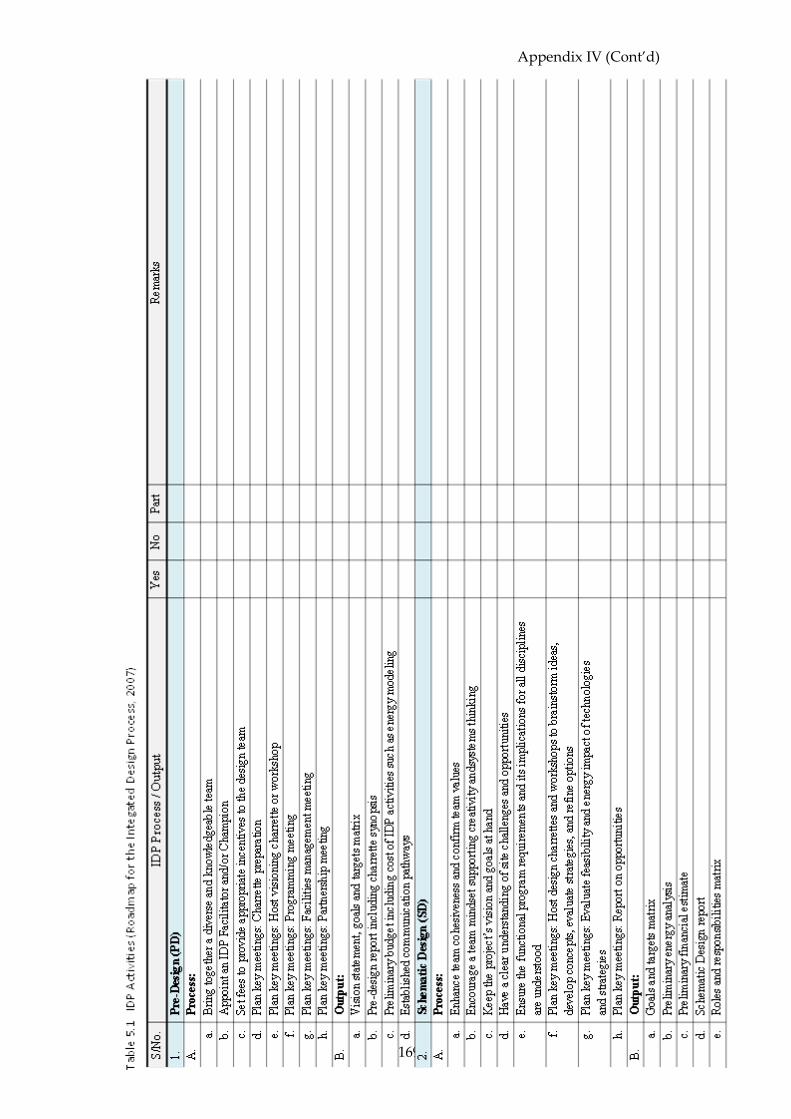
169
Appendix IV (Cont’d)

170
Appendix IV (Cont’d)

171
Appendix IV (Cont’d)

172
Appendix V (Cont’d)

173
Appendix VI: Evidence-Based Design Principles
“Good design, that is evidence-based, does not cost
money but will show significant savings over the
life-cycle of the building, as well as improving the
quality of life for all occupants.”
Bryan Lawson

174
Appendix VI
VI. Evidence-Based Design Principles
The integration of natural and landscape elements in KTPH’s site planning and layout
had facilitated the following benefits supported by the following evidence-based design
studies:
1. Positive effects of natural environment in the healthcare environment.
2. Improves way-finding leading to reduced stress.
1.0 Positive Effects of Natural Environment in Healthcare
Environment
The biophilia hypothesis suggests that there is an inborn affinity within humankind with
nature and living systems, including plant life, animals, as well as climatic elements e.g.
the sun and natural light and warmth, breeze, sound, and so on (Wilson, 1984; Kellert et
al, 1993; Kellert, 2004). The hypothesis has found support in parallel studies in the field
of environmental psychology, which examines the inter-relationship between human
and physical environment, be it natural or constructed (Section 1.6.2). One of the
findings is, not only is humankind aesthetically attracted to nature and living systems,
the sensing of with these features is also found to have positive effects on human
functioning and reduces stress (Bell, 2001; Bechtel, 2002). According to Ulrich (2002), the
healing properties of nature and natural systems have long been known, but have been
overshadowed by advances and focuses in medical technology and science, as well as
concerns for operational efficiency. The mounting evidenced-based studies more
recently have nonetheless strengthened the case for bringing nature into healthcare
environment to achieve the benefits as briefly explored in Section 1.1 to 1.5.
1.1 Speeding Up Patient Recovery and Enhancing Patient Well-being
Research has shown that stress and psychosocial factors can significantly affect patient
health recovery (Ulrich, 2001; Dellinger, 2010). Since human responds psychologically
and physiologically to nature and landscape positively (Ulrich, 1986), integrating nature

175
and landscape into healthcare built environment e.g. through the notion of the healing
garden (Ulrich, 1999, 2002; Shermana et al, 2005), or simply giving access to view
through window to nature and natural system have led to better postoperative outcome,
including “the need for less pain medication, shorter lengths of stay, and few minor
complications,…and generally reported better emotional well-being (Ulrich, 1984;
Dellinger, 2010).
Based on the mounting evidence, Dellinger (2010) recommended that: “When
designers plan a healthcare facility, they need to make actual nature, such as healing
gardens or landscaped areas with private setting, or the suggestion of nature
(through photos, murals, or sculpture), as integral part of the design” (p.64). Other
studies suggested the use of water features as a positive distraction, even briefly, that
cause positive emotional response (Joseph, 2006). Figure 3.3 and 3.4 illustrate the
various ways in which KTPH had integrated nature, landscape and water feature
into its built environments.
Figure VI-1 View to nature: Yishun Pond viewed from the Central Courtyard.
Source: CPG Consultants Pte Ltd
Appendix VI (Cont’d)

176
Appendix VI (Cont’d)
1.2 Well-being for Clinicians and Staff
Healthcare environment as a workplace is stressful to its workers. Post-occupancy
evaluations of four hospital gardens in California revealed that nurses and healthcare
workers are able to achieve pleasant escape and recuperate from stress by using the
gardens (Cooper-Marcus and Barnes, 1995). Providing windows with view also help
staff stay oriented with regards to time of day and weather condition, achieving better
well-being (Dellinger, 2010). Studies also showed that daylight penetration improves
nursing productivity (Rechel and McKee, 2008). In support of this, all wards in KTPH are
provided with window and view out.
1.3 Well-being for Family, Visitors and Public
Studies have shown that patient recovery and well-being are enhanced by social support
and family care (McCullough, 2010, p.82). As family members providing care and
support to the patient likewise experience stress and anxiety, it is important that their
well-being is also addressed. Post-occupancy studies have revealed that patients’ family
who use hospital gardens also experienced positive mood change and reduced stress, as
well as higher satisfaction with overall quality of care (Whitehouse et al., 2001).
Figure VI-2 Private seating corner around water as therapeutic modality: Courtyard at Basement
1 in Khoo Teck Puat Hospital featuring a small landscape pond. Source: CPG Consultants Pte Ltd

177
Appendix VI (Cont’d)
1.4 Economic Sustainability
The cost in healing gardens is relatively low as compared to healthcare equipment,
procedures and technologies. In addition, by speeding up patient recovery, it reduces the
cost of delivering healthcare services (Ulrich, 2002), hence also enhancing economic
sustainability. In addition, a 2004 CABE Healthcare report (2004) based on survey of
nursing clinicians found that external space is important to recruitment (p. 17), retention
(p. 22) and performance of nursing clinicians (p. 27). These suggest that access to and
integration of natural environment with healthcare environment contributes not only to
human wellness, but also economic sustainability.
The above benefits with support from evidence-based studies strongly suggest that
wherever possible, natural and landscape elements should be integrated into the design
of healthcare architecture, with KTPH being one example demonstrating such an
outcome.
1.5 Improves Way-Finding to Reduce Stress
Spatial disorientation causes stress, and as a result negatively impact patients’ healing
outcome and staff working in healthcare environment (Ulrich et al, 2004). The need to
give directional information by other than front desk information staff has also resulted
in hidden costs to many hospitals (ibid.). Integrated and holistic way-finding systems
help to reduce stress and economic loss related to way-finding.
In addition to providing greenery for human well-being, the central courtyard in KTPH
simplifies way-finding by enabling building users to relate to the lush central greenery
through external corridors and ample exterior windows from within the rooms (Figure
VI-4). Escalators and lift lobbies are also opened into the central courtyard, providing
users with a pleasant visual cue to orientation. Open circulation system are brightly lit,
and public furniture provided for activity and rest are placed to face the courtyard to
maximize its calming and healing properties.

178
Appendix VI (Cont’d)
Figure VI-4 Public furniture with good access to the Courtyard and Yishun pond views.
Source: CPG Consultants Pte Ltd
Figure VI-3 Easy wayfinding: External corridors surrounding the Courtyard are brightly lit,
easy to orientate and laced with landscape to create a biophilic environment.
Source: CPG Consultants Pte Ltd)

179
Figure VI-5 Courtyard at Ground level in Khoo Teck Puat Hospital is filled with lush sustainable
local plant types to achieve evidence-based supportive environment for patients, staff and visitors.
Source: CPG Consultants Pte Ltd

180
Appendix VII: Energy-Efficient Active Design Measures
“In integrated design, buildings aren’t seen as one-
off, independent entities made up of separate
building systems and isolated from their
surroundings – but instead as part of a holistic
process, an interdependent, living part of the
environment into which it is placed and belongs."
Randy Deutsch

181
Appendix VII
VII. Energy-efficient active design measures
The estimated energy consumption for KTPH’s proposed design is 36,059,410.23kWh per
annum, a saving of 36.4% as compared to the baseline reference model of
56,670,006.47kWh per annum (CPG Greenmark submission report). The following
energy-efficient active design measures were reportedly adopted in KTPH based on
CPG’s Greenmark submission report.
1.0 Energy-efficiency air-conditioning system
KTPH was designed to be served by chilled water central plant room system with 5
numbers of 900Ton centrifugal chillers served with AHUs and FCUs. Heat recovery
systems were used to reduce energy loss. The individual efficiencies of the air-
conditioning system were as follows:
1. 900Ton Chillers: 0.49kW/Ton
2. Chilled water pumps: 0.080kW/Ton
3. Condenser water pump: 0.049kW/Ton
4. Cooling tower: 0.042kW/Ton (0.2205kW/L/Sec)
5. Plant room efficiency: 0.49+0.08+0.049 = 0.619kW/Ton
6. System efficiency: 0.49+0.08+0.049+0.042 = 0.661kW/Ton
The plant room efficiency was benchmarked against Singapore Standard SS530, under
which the minimum efficiency of the plant room was 0.782kw/Ton. The KTPH design
was hence 20.8% more efficient. Under SS530, the cooling tower efficiency was
0.31kW/L/s, hence the KTPH design was 28.8% more efficient.
2.0 Energy-efficiency lighting system
To conserve energy, high-efficiency T5 lighting with electronic ballasts was used for
general lighting, along with other high-performance, high-efficient lighting. The total
design wattage was 1,340.5kW compared to 1,463kW reference design, i.e. a saving of
8.4%.

182
Appendix VII (Cont’d)
3.0 Energy-efficiency carpark mechanical ventilation system
The mechanical ventilation system of the Basement 2 carpark is monitored with CO2
sensor. This conserves energy by ensuring that the mechanical ventilation system was
only turn on when required.
4.0 Natural ventilation to common areas
Wherever possible, the common areas were designed to ventilate passively, through
natural ventilation:
1. Staircase: 71% natural ventilation, 29% mechanical ventilation
2. Corridors: 30% natural ventilation, 1% mechanical ventilation, 69% air-
conditioning
3. Toilets: 100% mechanical ventilation
4. Atriums: 100% natural ventilation
5.0 Energy-efficient lifts and escalators
All lifts in KTPH utilise variable-voltage, variable-frequency (VVVF) motor drive to save
energy by matching the energy consumption with the system demand.
All escalators were embedded with motion/step-sensor to conserve energy when traffic
volume is low.
6.0 Energy-efficient practices and measures
Other energy-efficient features include the use of:
1. Heat pipe
2. Integrated building monitoring system monitoring measures

183
Appendix VIII: Water-Efficient Considerations
“Water is essential to life. It is hygienic, aesthetic,
spiritual, life sustaining, and symbolic.”
Stephen Verderber
184
Appendix VIII
VIII. Water-efficient considerations
The following water-efficient measures were reportedly adopted in KTPH based on
CPG’s Greenmark submission report.
1.0 Efficient water fixtures & fittings
Water efficient fittings rated based on Singapore Public Utilities Board’s (PUB) Water
Efficiency Labeling Scheme (WELS) were used. Most of the fittings were rated as
‘excellent’, as follows:
Fittings with ‘Excellent’ rating: 2,085 units (59.9%)
Fittings with ‘Very Good’ rating: 733 units (21.0%)
Fittings with ‘Good’ rating: 23 units (0.7%)
Fittings without rating (mostly special medical equipment): 642 units (18.4%)
2.0 Water usage and leak detection
Water meters were installed to monitor the portable water usage. The water meters were
linked to Building Management System (BMS) for intelligent monitor.
3.0 AHU condensate water is recycled to be used for cooling towers
Condensate water from AHU was collected and used as cooling tower make-up water.
Besides helping to reduce the amount of make-up water needed, the lower water
temperature of the condensate water also raises chiller efficiency.
4.0 Water Efficient Landscaping Irrigation System
Rainwater collected within the KTPH site was fed to Yishun Pond, adjacent to the site.
The raw water (non-portable) from Yishun Pond was used for landscape irrigation in
KTPH, to reduce consumption on potable water. Newater, water recycled from sewage is
used as a backup water source for the irrigation system.

185
Appendix IX: Indoor Environmental Quality
“Give all building occupants environmental comfort
and, most importantly, control over that comfort –
this most obviously involves heat and light. However
it also includes sound. Hospitals are notoriously noisy
places. Some of Ulrich’s research has shown that
patients in a cardiac unit had their heart rates
significantly reduced by decreasing background
sound levels. Giving patients bedhead controls of
lights, blinds, curtains and doors is really very cheap
to do and remarkably effective in reducing stress
levels.”
Bryan Lawson

186
Appendix IX
IX. Indoor environmental quality
The following indoor environmental quality measures were reportedly adopted in KTPH
based on CPG’s Greenmark submission report.
1.0 Thermal Comfort
The air-conditioned spaces were designed to allow for cooling load variations due to
fluctuation in ambient air temperature to ensure consistent indoor temperature for
thermal comfort. The indoor air temperature was designed to be within 22.5°C and
25.5°C with relative humidity of less than 70%.
2.0 Acoustic Comfort
With acoustic consultants’ advice, the ambient sound level of KTPH was designed to
between 40dB and 50dB in all occupant areas. The measures included were:
Walls, partitions and doors specified to STC 35dB, 40dB, 45dB and 50dB
standards, where appropriate;
Acoustic ceiling tiles specified to minimum noise reduction coefficient (NRC) of
0.5;
Check for test reports of materials’ acoustic properties;
All wall perforation and duct penetration sealed with approved details to prevent
sound bridge/leak;
Use low-noise ceiling fan for subsidised ward areas;
Conduct acoustic commissioning for critical areas.

187
Appendix IX (Cont’d)
3.0 Indoor air quality
UVC Emitters60 was installed in the supply air duct just after the cooling coil, to kill all
pathogens. This improved the indoor air quality and helps to keep the cooling coil clean.
A radiometer was used to monitor the performance of the UVC emitter.
The AHU coils were pre-treated with titanium dioxide (TiO2), an anti-bacteria, anti-
odour and self-cleaning agent to eliminate bacteria and mould growth in the cooling
coils. As a result, it reduced the need for cleaning, as well as risk of sick building
syndrome.
Figure VIII-1 Schematic diagramme of a typical AHU in KTPH, showing the locations of UVC
emitter, radiometer and CO2 sensor. Source: CPG Consultants Pte Ltd
60 UVC refers to a type of ultraviolet (UVC) energy. The "C" wavelength is the most effective
germicide in the UVC spectrum. UVC Emitters are devices that generate UVC rays to kill germs.

188
Appendix X: Renewable Energy Systems &
Other Innovation Measures
“In the service of healing people, healthcare
institutions use a tremendous amount of energy,
the conventional production of which is associated
with public health hazards. Fortunately, solutions
exist to reduce and even eliminate this paradox,
while also reducing operating costs, enhancing
patient outcomes, and boasting staff productivity.”
Alexis Karolides

189
Appendix IX
X. Renewable Energy Systems & Other Innovation Measures
The following renewable energy ststem and other innovation measures were reportedly
adopted in KTPH based on CPG’s Greenmark submission report.
1.0 Solar thermal system
Vacuum tube solar thermal system is utilised to generate the hot water usage
requirements of the hospital. The solar thermal system and solar heat pumps produce
was designed to fully meet the hot water requirements of the hospital (21,000 litres/day).
This resulted in a saving of 780kWh/day of electricity and the space for boiler was
eliminated.
Figure X-1 Vacuum tube solar thermal system in KTPH is used to generate hot water
Source: CPG Consultants Pte Ltd
2.0 Photovoltaic system
A 130kWp photovoltaic system, occupying a roof area of 1,200m2 is designed and
installed. It is estimated to generate approximately 150,000kWh of energy per year (See
Figure X-2).

190
Appendix IX (Cont’d)
Figure X-2 Photovoltaic system installed at the rooftop of KTPH to maximise solar exposure
and electricity output. (Source: CPG Consultants Pte Ltd)
3.0 Other Green and Innovative Features
3.1 Self-sustaining Ecological Pond
The water feature in Basement 1 of the courtyard was designed as an eco-pond,
essentially an ecologically self-sustaining pond that blended into the landscape. Besides
enhancing the environmental quality, it was also educational in promoting the concept
of sustainability.
The filtration of the Eco-pond was powered by a light mechanical pump. A diverse range
of marginal and water plants and small fishes form the eco-system, but only small fishes
were used, so that the system was able to handle the waste generated.
The water supply of the pond was from rainwater collected from the roof, filtered by the
roof garden. Excess water was fed to the water-efficient irrigation system.

191
Appendix IX (Cont’d)
Figure X-3 Eco-pond (Source: CPG Consultants Pte Ltd)
3.2 Other Innovative Green Features
Other green features that have been provided in KTPH were:
1. Dual refuse chutes for separation of recyclable waste.
2. Siphonic rainwater discharge system to reduce pipe size, hence reduce space
wastage, as well as to reduce noise.
3. Automatic waste and soft linen collection systems.
4. Auto tube cleaning system was used to reduce consumption by approximately
20%.
5. Composting machine was used to process food waste into fertilizer for roof and
food gardens.

192
Appendix XI: Integrated Design during
Construction Phase
“If we are to understand and build upon the
integration between nature and human nature,
between the built and natural environments, we
need to rethink our attitude towards the practice of
design and of construction."
Eddy Krygiel and Bradley Nies

193
Appendix X
XI. Integrated Design during Construction Phase
1.0 Placemaking
The integrated design effort continued even during construction. While the main
structure and architectural work was in progress, one of the areas of design focus for the
KTPH HPC and the building professionals was ‘place-making’ in the social and
landscape spaces, so as to meet the objective of healthcare built environment as a socially
sustaining therapeutic environment. From a design coordination minutes dated 17th June
2009, KTPH’s COO Chew “reiterated that the place-making is a process of creating a
natural gathering place with the right look and feel to put people at ease when they
come into the hospital grounds…The hospital grounds should offer a healing
environment for the patient’s family members to comfort each other. Spaces need to be
designed for events to happen” (CPG file archive). CPG Architect Pauline Tan recounted
that more than twenty locations were identified, with provisions made for lighting,
power point and routing for cables, LAN, water point, audio system with pipe-in music
wherever possible, ventilation, thermal comfort (e.g. spot cooling of roof terraces
presented in Section 4.2.1) and acoustics, mobile art and banners etc.
Figure XI-1 Positive image of AH and nature in KTPH lift interior.

194
Appendix XI (Cont’d)
2.0 Interior Design
In interior design, artworks and images from the lush greenery in KTPH’s previous
premise (AH) were displayed (Figure XI-1), to create positive, therapeutic impression
(verderber, 2010, p. 132). For example, the lit ceiling panel of the lift car. This again
demonstrated collaboration between the medical staff with intimate memory of AH and
building professional e.g. interior designers, M&E engineers and contractors.
3.0 Yishun Pond Community Project
The integrated, whole-system thinking went beyond the close collaboration between
medical and building professionals. Architect Lim recalled, “During the construction of
the hospital in 2007, KTPH embarked on a community project to rejuvenate Yishun
Pond. At that time there was no budget for any landscaping works on the pond. KTPH
adopted the Yishun pond and convinced other government agencies through their
respective programmes, namely HDB (Remaking Our Heartland), NParks (routine
landscape programme), and PUB (ABC Waters) to co-finance the Yishun Pond
rejuvenation works for the community and patients. CPG Consultants and Peridian Asia
were also appointed to carry out an integrated landscape design involving multiple
agencies for the boardwalk, tower, overhead bridge and landscape around the Yishun
Pond that also connects well with the KTPH landscaped area. Though the hospital was
operational in 2010, the comprehensive healing environment was fully realized with the
completion of the Yishun Pond in 2011.”61 In this instance, a positive, integrated outcome
for community benefits was achieved through a willingness to collaborate amongst the
governmental agencies, brought about by KTPH’s CEO Liak’s social influence and skills.
61 Interview session held in Jan 2012.

195
Appendix XII: KTPH’s BCA Green Mark Performance
“[G]reen building rating systems and other practice
tools are necessary as part of a building’s integrated
design process."
Marian Keeler and Bill Burke

196
Appendix XII
XII. KTPH’s BCA Green Mark Performance
BCA Green Mark’s Non-Residential Building (NRB) Version 3.0 (GM NRB 3.0), part of
the Singapore national green rating system, was used as a tool to guide the green
building design for KTPH. It was certified as Green Mark Platinum in 2010, the highest
award under the BCA Green Mark Scheme. The assessment criteria of GM NRB 3.0 is
shown in Figure XI-1. It could be seen that energy efficiency is an important
consideration for GM NRB 3.0, requiring a minimum score of 30 points, while all the
other four criteria (water efficiency, environmental protection, indoor environmental
qualities and other green features) must achieve a minimum score of 20 points in order
to achieve the minimum score of 50 points, which is mandatory for Singapore since 2008.
KTPH achieved a score of 71.35 points for energy efficiency measures (Figure XII-2), out
of which GM NRB 3.0 accords a maximum of 50 points. The design consumes 36.4% less
energy then the baseline reference model. Under GM NRB3.0, the design also scored
maximum points for:
1. Building Envelope – ETTV
2. Air-Conditioning System
3. Building Envelope – Design/Thermal Parameters
4. Natural Ventilation
On the other hand, it scored a low 4.69 out of a total of 20 points (Figure XII-2) in the use
of renewable energy. Solar thermal for hot water and photovoltaic panel for electricity
were used in limited application, due to a need for budget management.
Maximum scores were also achieved for many other categories, including ‘Greenery’,
which is a main feature in KTPH. Categories where less than maximum scores were
achieved are: ‘Water efficient fittings’ (6.08 out of 8), ‘Sustainable Construction’ (4.5 out
of 14), and indoor air pollutants (1 out of 2). The score indicates that there are certainly
rooms for improvement in terms of sustainable construction.

197
Appendix XII (Cont’d)
Figure XII-1 BCA Green Mark Non-Residential Building Version 3.0 Assessment System.
Source: Building Control Authority (BCA), Singapore.

198
Appendix XII (Cont’d)
Figure XII-2 KTPH’s BCA Green Mark Energy Efficiency Score under NRB 3.0 Scoring System.
Source: CPG Consultants Pte Ltd.

199
Appendix XIII: Thermal Comfort Outcome of KTPH’s
Bioclimatic and Natural Ventilation Strategies
“Passive Mode requires an understanding of the
climatic conditions of the locality, then designing
not just to synchronize the built form’s design with
the local meteorological conditions, but to optimize
the ambient energy of the locality into a building
design with improved internal comfort conditions
without the use of any electro-mechanical systems."
Ken Yeang

200
Appendix XIII
XIII. Thermal Comfort Outcome of KTPH’s Bioclimatic and
Natural Ventilation Strategies
The potential and challenges of harnessing natural ventilation as a passive design
strategy, in order to balance the various needs: reduce energy usage, health and safety
e.g. infection control, human comfort, and meeting policy requirements e.g. subsidized
patient wards, have been discussed in Section 1.5.1. Due to its benefits, natural
ventilation is an important ventilation strategy for public hospital in Singapore, with
65% of public hospital being naturally ventilated (Lai-Chuah, 2008).
In his dissertation, Wu (2011) conducted post-occupancy survey over three hospital with
ventilated wards, namely, KTPH, completed in 2010; AH, built more than 70 years ago in
1934; and CGH, built more than 14 years ago in 1997 (Wu, 2011). It was found that
patients in the air-conditioned (for private ward patients) and naturally ventilated (for
subsidized patients) wards had equally high acceptability of the thermal environment in
KTPH (Figure 3.16). “Both CGH and KTPH met the ASHARE 55-2010 thermal
satisfaction requirement for their air-conditioned and naturally ventilated wards” (ibid.
p. 71). With regards to nursing clinicians, Wu’s survey found that none met the ASHARE
55-2010 standard requirements, but KTPH provided conditions that satisfied more
clinicians (77.4%) then CGH (64.3%) and AH (30.8%)(Figure XIII-1; ibid, p. 76). Wu
attributed this to the higher activity level performed by nursing clinicians as compared
to patients (p. 104). KTPH’s acceptability of 77.4% is also very close to ASHARE 55-
2010’s requirement of 80% acceptability.
Interestingly, Wu also found that there is insignificant difference in the satisfaction level
between patients in the naturally ventilated ward and the air-conditioned ward (Figure
XIII-2; Ibid., p. 101). This finding validated that with thoroughly considered bioclimatic
design, it is viable to design healthcare wards using NV, with ventilation at nurse station
enhanced by fan with localized control.

201
Appendix XIII (Cont’d)
Wu attributed the performance outcome of the KTPH’s built environment to its
integrated sustainable design strategies, encompassing site planning, venturi effect of the
courtyard, landscaping, building shape and layout, building envelope, façade design,
central atrium, interior design, and partial energy recovery through recycling of cooled
air (Wu, 2011; Table XI-1).
Figure XIII-1 Patient acceptability of thermal environment in CGH and KTPH.
Source: Wu, 2011, pp. 71.
Figure XIII-2 Nursing Clinician Acceptability of Thermal Environment in CGH and KTPH.
Source: Wu, 2011, pp. 76.

202
Appendix XIII (Cont’d)
Table XIII-1 Sustainable Design Strategies Employed in Khoo Teck Puat Hospital for Thermal
Comfort in Naturally Ventilated Area. Source: Wu, 2011, p. 130-131

203
Appendix XIII (Cont’d)
Table XIII-1(Cont’d) Sustainable Design Strategies Employed in Khoo Teck Puat Hospital for
Thermal Comfort in Naturally Ventilated Area. Source: Wu, 2011, p. 130-131

204
Appendix XIV: Evaluating Human Wellness and Social
Sustainability of KTPH
“Often, additional organizational social benefits is
achieved through an integrated design process that
engages a wide range of stakeholders, where the
building design is viewed as only one component
of an institution-wide environmental improvement
initiative that involves everyone.”
Robin Guenther and Gail Vittori

205
Appendix XIV
XIV. Evaluating Human Wellness and Social Sustainability of
KTPH
1.0 Post-Occupancy Survey (Sng, 2011)
Through a post-occupancy survey, Sng P. L.’s dissertation (2011) reported that besides
being a Green Mark Platinum certified green building, KTPH has “provided for natural
and social environments well to a reasonably large extent” (p. 74). From among sixteen
features, the most noted and welcome features of KTPH, in ascending order, are (Sng,
2011, p. 61; Figure XIII-1):
Figure XIII-1 Number of times being mentioned as a group description (constructs) and number of
times being chosen as a top priority group. Source: Sng, 2011, pp. 60.
206
Appendix XIV (Cont’d)
1. ‘Natural Scenery’;
2. ‘With Families and Friends’ in combination with ‘Recreational Activities’
3. ‘With Families and Friends’ in combination with ‘Walking and Viewing’
4. ‘Relax’ which indicates the effectiveness of KTPH’s premise as a ‘healing
environment’.
1.1 Natural Scenery
The integration of nature into the KTPH premise, an outcome due to the biophilic
approach taken by KTPH and its design team, was found by Sng62 to be the most well-
like feature. It was also deemed to be the most important among all the features. In
addition, the survey also found that “people prefer the positive feeling that nature offers,
rather than manicured gardens” (Ibid., p. 67). This validates both the biophilia
hypothesis (Wilson, 1984; Kellert et al, 1993; Kellert, 2004; see also Appendix V), as well
as the KTPH CEO Liak Teng Lit’s personal belief. Based on CPG Architect Jerry Ong’s
account, besides the aforesaid reason, Liak also believed that by using local plant types
in a natural setting, it require less intervention and efforts for the plant ecology to thrive.
This is not only more ecologically friendly, but results in lower maintenance as well
(Ong, interview session in Jan 12).
1.2 A Relax, Therapeutic Environment to Foster Social Activities
Social or communal activities are the next well like feature in KTPH, indicating that its
premise “is well provided for people” (Sng, 2011, p. 67). The association of its premise
with experience such as ‘With Families and Friends’, ‘Recreational Activities’, ‘Walking
and Viewing’ and ‘Relax’ may imply that people enjoy the premise as a social setting, as
supported by its natural environments. This appears to support the evidence-based
design principles with regards to well-being for family, visitors and public (Whitehouse
et al., 2001; see 1.3 in Appendix V) and well-being for clinicians and staff (Cooper-
Marcus and Barnes, 1995; Dellinger, 2010; See 1.2 in Appendix V).
62 Sng used multidimensional scaling (MDS) to plot the data collected for interpreting the results.

207
Appendix XIV (Cont’d)
1.3 Inadequacy of Green Mark Rating System
Sng also found that these ‘wellness dimensions of World Health Organizations Quality
of Life’ (WHOQOL) are in fact missing from BCA Green Mark rating system (Ibid., p.
75). As a result, in focusing on technical performance of the built environment, Green
Mark is able to promote building design as a system of building sub-systems, but
inadequate to address social and ecological dimensions of sustainability. This is perhaps
not the current purpose of Green Mark rating system. Nonetheless, it also indicates that
the objectives-setting of such wellness dimensions would have been to be generated
independently from the Green Mark rating system; in the case of KTPH, it was through
the vision of the KTPH leadership and a systematic objective-setting exercise by
employing the Total Building Performance framework (See Section 3.3).
2.0 Fostering Sustainability through Community Stewardship
Section 1.6.2.2 presented the opportunities for a sustainable healthcare institution to
open up its premise to connect, engage and be enjoyed by its neighbourboods and
communities, and encourage community participation in environmental, social and
healthcare programmes. The connectivity created between KTPH, Yishun Pond and its
neighbourhoods has open up such opportunities, allowing volunteer services (Table
XIII-1), community, social and partnership programmes (Table XIII-2), partnership
programmes, etc to make use of KTPH’s premise. Fostered by KTPH’s biophillic, user-
friendly public spaces and amenities, the increasing community participations since the
opening of KTPH in 2010 demonstrate its potentials in fostering social sustainability at
the community level.
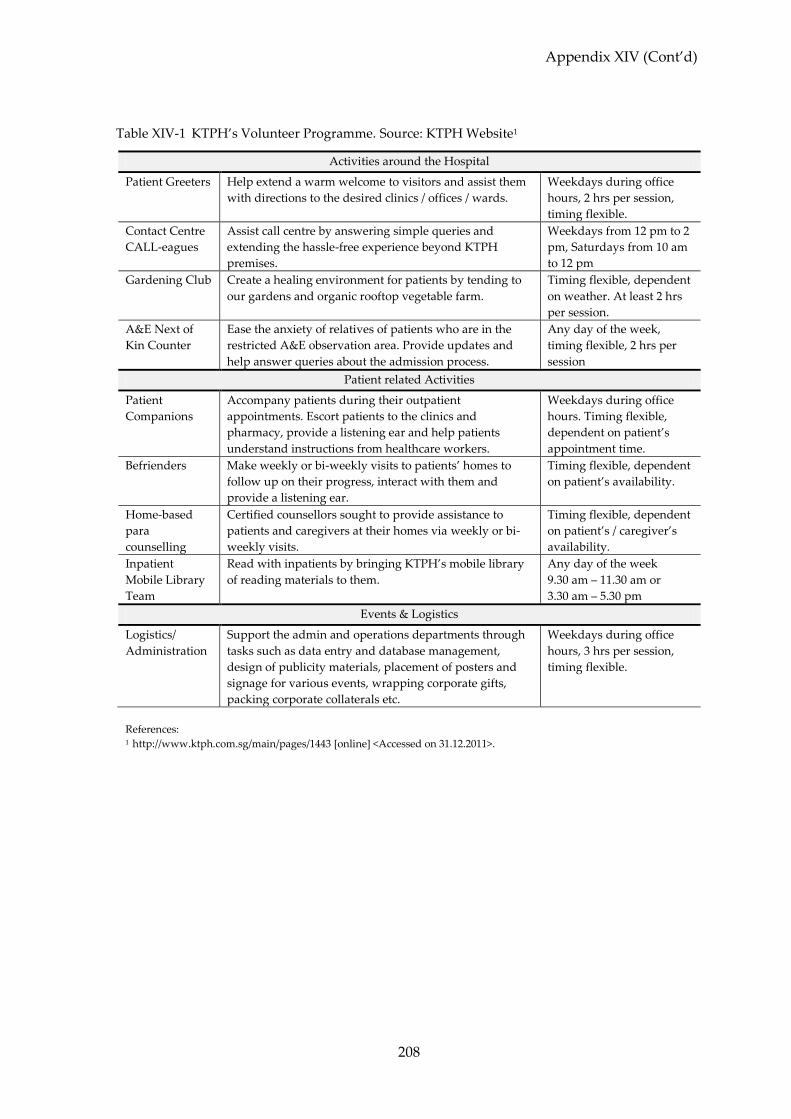
208
Appendix XIV (Cont’d)
Table XIV-1 KTPH’s Volunteer Programme. Source: KTPH Website1
Activities around the Hospital
Patient Greeters Help extend a warm welcome to visitors and assist them
with directions to the desired clinics / offices / wards.
Weekdays during office
hours, 2 hrs per session,
timing flexible.
Contact Centre
CALL-eagues
Assist call centre by answering simple queries and
extending the hassle-free experience beyond KTPH
premises.
Weekdays from 12 pm to 2
pm, Saturdays from 10 am
to 12 pm
Gardening Club Create a healing environment for patients by tending to
our gardens and organic rooftop vegetable farm.
Timing flexible, dependent
on weather. At least 2 hrs
per session.
A&E Next of
Kin Counter
Ease the anxiety of relatives of patients who are in the
restricted A&E observation area. Provide updates and
help answer queries about the admission process.
Any day of the week,
timing flexible, 2 hrs per
session
Patient related Activities
Patient
Companions
Accompany patients during their outpatient
appointments. Escort patients to the clinics and
pharmacy, provide a listening ear and help patients
understand instructions from healthcare workers.
Weekdays during office
hours. Timing flexible,
dependent on patient’s
appointment time.
Befrienders Make weekly or bi-weekly visits to patients’ homes to
follow up on their progress, interact with them and
provide a listening ear.
Timing flexible, dependent
on patient’s availability.
Home-based
para
counselling
Certified counsellors sought to provide assistance to
patients and caregivers at their homes via weekly or bi-
weekly visits.
Timing flexible, dependent
on patient’s / caregiver’s
availability.
Inpatient
Mobile Library
Team
Read with inpatients by bringing KTPH’s mobile library
of reading materials to them.
Any day of the week
9.30 am – 11.30 am or
3.30 am – 5.30 pm
Events & Logistics
Logistics/
Administration
Support the admin and operations departments through
tasks such as data entry and database management,
design of publicity materials, placement of posters and
signage for various events, wrapping corporate gifts,
packing corporate collaterals etc.
Weekdays during office
hours, 3 hrs per session,
timing flexible.
References: 1 http://www.ktph.com.sg/main/pages/1443 [online] <Accessed on 31.12.2011>.

209
Appendix XV: KTPH’s Environmental Stewardship
“For more than 99 percent of human history people
have lived in hunter–gatherer bands totally and
intimately involved with other organisms. During
this period of deep history, and still further back
they depended on an exact learned knowledge of
crucial aspects of natural history. . . . In short, the
brain evolved in a biocentric world, not a machine-
regulated world.”
Edward Osborne Wilson
210
Appendix XV
XV. KTPH’s Environmental Stewardship
By adopting an integrated approach in site planning, connecting the KTPH’s
environment with Ponggol Pond and the Yishun natural and community context, the
design opens up opportunities for community and environmental stewardship for
KTPH, as discussed in Section 1.0 to 3.0:
4. Maximizing opportunities in creating a biophillic built environment (Section 1.0).
5. Integrating with Yishun Pond environmentally and socially (Section 2.0).
6. Fostering biodiversity (Section 3.0).
1.0 Biophilic Built Environment
Some Yishun residents, including retired farmers in the Yishun community (Wu, 2011, p.
108) had volunteered to tend to the rooftop vegetable and fruit gardens at KTPH (AHa!
Mar-Apr 2010, p. 11; Figure XIV-1, XIV-2). One key volunteer with green fingers, 68-year
old Mdm Lim Chew Eng, who also tends to community farm in Yishun town, shared her
experience and help create an urban farm in the hospital (Ibid.). The produce such as
“tomatoes, melons, and bananas” (Wu, 2011, p. 107) is shared between volunteers and
the hospital kitchen, and composted food waste from the hospital kitchen provided
fertilizer for the crops (Ibid, p.107). KTPH reported that:
KTPH’s “Chief Gardener”, Rosalind Tan, who oversees the volunteer gardeners
said that residents were keen to get involved and brought their friends along. She
welcomes them and others too…Urban farming on the rooftop not only provides
the hospital’s kitchen with an organic food source for our patients, it also reduces
the temperature of the building and involves the community in caring for our
patients and the environment. (Alexandra Health Newsletter AHa! Mar-Apr
2010, p. 11)

211
Appendix XV (Cont’d)
Besides vegetable gardening, many other biophilic features including therapeutic
gardens, patios, balconies, terraces (Figure XIV-4), courtyards (Figure XIV-3), and water
as therapeutic modality (Figure 3.3, 3.18, 3.19), etc that Verderber (2010) has
recommended for the hospital environment, with KTPH providing some examples.
Figure XIV-1 Rooftop vegetable gardens at Khoo Teck Puat Hospital
Source: CPG Consultants Pte Ltd
Figure XIV-2 Yishun resident volunteers led by Rosalnd Tan (Second from right) working on the
“Urban Farm” above KTPH. Source: Alexandra Health Newsletter AHa! Mar-Apr 2010, p. 11

212
Appendix XV (Cont’d)
In his thesis, Kong (2005) “suggests that gardening, people, and environment form a
triangle of interrelationships…where one stimulates the other” (Bay and Ong, 2006, p.
75). As participants tend to the KTPH urban farm with care and interest, creating a sense
of community ownership, the “plant in turn improve the environment, the activity
increases, improving the casual knowing of neighbours and sense of community, and
thus in turn encourage more interest in gardening [and/or farming]”(Ibid., p. 75). Nature
and community henceforth develops a symbiotic relationship.
Figure XIV-3 Interrelationships of gardening in semi-open space, people and climate in tropical high-
rise housings. Source: P. Kong in Bay and Ong, 2006, p. 75.
Figure XIV-4 Rooftop gardens, balconies, patios at KTPH help reduce the indoor temperature and
mitigate urban heat island effect. Source: CPG Consultants Pte Ltd

213
Appendix XV (Cont’d)
2.0 Integration with Yishun Pond
KTPH adopted the Yishun pond in 2005 under Public Utilities Board (PUB)’s ‘Our
Waters Programme’, and participated actively in plans to transform it into a green lung,
e.g. organizing regular pond clean-ups of areas around the pond (AHa! Sep-Oct 2010, p.
2)63. With the opening of KTPH, through a collaboration between National Environment
Agency (NEA), PUB, National Parks Board (NPB) and Alexandra Health (KTPH’s
holding company), improvement work was carried out at Yishun Pond “to turn it into an
intergenerational, health promoting garden that will be integrated with the hospital”
(Ibid.).
It provided more and better park facilities for residents living in the surrounding Yishun
communities to exercise and interact. Marshlands created along the shore softens the
water edge and improve water quality by filtering pollutants through the use of aquatic
plants, as well as attracting wildlife and enhancing biodiversity. “A barrier-free lakeside
promenade was built to connect KTPH’s central courtyard to the garden” (Ibid.),
providing more opportunities for KTPH to spread health promoting messages among
patients and Yishun residents (Ibid.).
PUB’s Active, Beautiful, Clean Programme (ABC) launced in 2006 is a “strategic
initiative to improve the quality of water and life by harnessing the full potential of our
waterbodies…by integrating the drains, canals and reservoirs with the surrounding
environment in a holistic way” (ABC Guidelines, p. 4). Under the ABC programme, built
environment that harness water sensitive urban design and sustainable drainage
principles may be ABC certified, and KTPH is ABC-certified in 2010. The following
reasons were cited (PUB):64
1. Planter boxes and green roofs detain and treat 12% of rain water run-off that is
harvested for reuse.
63 Alexandra Health Newsletter, AHa! Sep-Oct 2010, p. 2 64 PUB Website: http://www.pub.gov.sg/abcwaters/ABCcertified/Pages/2010.aspx#a6

214
Appendix XV (Cont’d)
2. A green wall and terraced landscape enhances the lushness of the area while
resting and seating facilities along streams and water features bring people closer
to water.
3. Integration with the nearby Yishun Pond, with extensive plantings providing a
tranquil and scenic environment for the hospital’s patients and visitors while
creating a suitable habitat for birds and butterflies.
4. Collaborates with schools and institutions in programs such as Earth Day to
spread educational messages.
3.0 Fostering Biodiversity
“Sustainable development and the preservation of biodiversity are important
components of KTPH’s environmental philosophy. Vast areas of KTPH have
been earmarked for landscaping and planting to encourage the creation of
habitats and a healthy environmental ecosystem.” (KTPH) 65
The core KTPH management and team migrated from Alexandra Hospital (AH), 66
including Rosalind Tan, KTPH’s “Chief Gardener”. As reported (TODAY, 2007), 67 she
was a senior executive at AH’s operations department, and since 2000, she has led the
AH team in transforming “12 hectares of the hospital grounds, bringing in 500 species of
trees and shrubs, aromatic flowers, water features — even a butterfly trail that boasts 100
species.” (Ibid.) For her contributions towards environmental sustainability, she was
awarded the inaugural EcoFriend Award by the National Environment Agency.
AH’s garden is popular on weekends, “with former patients bringing their families there
for a stroll, and members of nature societies using it as a study ground” (Ibid.; Table XV-
1)
65 KTPH Website: http://www.ktph.com.sg/main/explore_ktph_pages/232 66See ‘History of Alexandra Hospital’. In: Alexandra Hospital Website. [online] Available at:
<http://www.alexhosp.com.sg/index.php/about_us/our_history> [Accessed 31.12.2011] 67 See Chang, C. (2007). Solace in the hospital grounds. In Channel News Asia Website. [online]
Available at: <http://www.channelnewsasia.com/stories/singaporelocalnews/view/282365
/1/.html> [Accessed 31.12.2011]

215
Appendix XV (Cont’d)
Table XV-1 Nature Activities and Reports of Alexandra Hospital’s garden and butterfly sighting.
Date. Event
30.07.2005 Perry, M. Alexandra Hospital opens new garden of medicinal plants. Channel News Asia
(http://www.wildsingapore.com/news/20050708/050730-1.htm#cna1)
16.10.2005 Perry, M. Alexandra Hospital garden has plants that heal, thrill or kill. Channel News
Asia (http://www.wildsingapore.com/news/20050708/050730-1.htm#cna1)
20.03.2007 Baron, G. Locally Extinct Butterfly Sighted at AH! Singapore Nature Society Butterfly
Interest Group (http://bignss.blogspot.com/2008/03/new-species-sighted-at-
alexandra.html)
04.04.2008 Wong, W. Euphorbia in Bloom @ Alexandra Hospital & Other Happenings. Garden with
Wilson (http://gardeningwithwilson.com/2008/04/04/euphorbia-in-bloom-
alexandra-hospital-other-happenings/)
27.07.2008 Khew, S. K. Butterfly Photography at our Local Parks. Butterflies of Singapore
(http://butterflycircle.blogspot.com/2008/07/butterfly-photography-at-our-
local.html)
28.07.2008 Commander. Shooting at Alexandra Hospital Butterfly Trail. Butterfly Circle
(http://www.butterflycircle.com/?p=17)
12.11.2008 Wong, W. Alexandra Hospital’s Garden Party. Garden with Wilson
(http://gardeningwithwilson.com/2008/11/12/alexandra-hospitals-garden-party/)
15.02.2009 Mantamola. Butterfly Park @ Alexandra Hospital. Manta blog
(http://mantamola.blogspot.com/2009/02/butterfly-park-alexandra-hospital.html)
28.05.2009
29.05.2009
National Parks Board. Creating Butterfly-Friendly Habitats.
(http://www.nparks.gov.sg/cms/index.php?option=com_content&view=
article&id=172&Itemid=129)
05.12.2009 ItchyFingers. A Visit to the Hospital.
(http://myitchyfingers.wordpress.com/2009/12/05/a-visit-to-the-hospital/)
16.02.2010 Seah, J. Alexandra Hospital Butterfly Trail, S'pore. Singapore Fauna and Flora
(http://www.flickr.com/photos/j_for_joyce/sets/72157623471951042/)
31.03.2011 Khew, S. K. and Tan, E. Return of a Magnificent Giant. Butterflies of Singapore
(http://butterflycircle.blogspot.com/2011/03/return-of-magnificent-giant.html)
02.04.2011 Lim, S. et al. Alexandra Hospital Butterfly Trail. Informal Macro Outing Group
(http://npssimog.blogspot.com/2011/04/82011-alexandra-hospital-butterfly.html)
22.07.2011 Starmer, C. F. Adventures with curiosity and learning.
(http://frank.itlab.us/photo_essays/wrapper.php?jul_22_2011_ahbt.html)
30.11.2011 Gan, W. C. Singapore’s Winged Wonders. Singapore Kopitiam
(http://www.singaporekopitiam.sg/places-and-heritage/places/wildlife-and-
nature/item/1001-singapores-winged-wonders)
12.02.2012 Mariano, M. Hospital Butterfly Trail. (http://flickeflu.com/set/72157626141292182)
Unknown Wong, C. P. Alexandra Hospital Butterfly Garden
(http://www.pbase.com/gohorses/alexandra_hospital_butterfly_garden)
Unknown Regular guided walk at AH by Butterfly Interest Group
(http://butterfly.nss.org.sg/home/butt_walks.htm)

216
Appendix XV (Cont’d)
The success of AH’s butterfly trail was by no means an accident. According to a life-long
butterfly enthusiast based in Singapore (Khew, 2008)68, it was a project started in 2002 led
by Rosalind, an occupational therapist who had drawn from her experience that a
butterfly garden could help in a patient's recovery, validating the biophilia hypothesis
and evidence-based studies on positive distraction (Lahood and Brink, 2010, Delinger,
2010):
Butterflies have so many colours and patterns. Seeing them gives patients
optimism and distracts them from their illnesses,' she said (Khew, 2008)
“Vast areas of KTPH were earmarked for landscaping to encourage the creation of
habitats and a healthy environmental ecosystem. The hospital planning committee
sought to increase the indigenous wild life biodiversity by introducing native species of
plants in the hospital’s landscaping.” (Wu, 2011, p. 109) with life-long passion from staff
member like Rosalind Tan, its environmental philosophy and stewardship looks likely to
bring new success, as the management had set a biodiversity target for KTPH:
100 species of butterflies, birds, fishes, flowering plants, fruit trees, native trees,
edible plants and fragrant plants. Yes, all 800 of them (Ong, J, 2010)69
Such ambitious objectives are not likely to be set without a collective will driven by a
collective, shared vision and mindset of environmental stewardship, as suggested by
Batshalom and Reed (see Section 2.3.2 and Figure 2.3). To succeed, however, it also
necessitates a process of value sharing and transfer, from KTPH to the building
professionals, to ensure that the design of the built environment outcome supports such
vision. This is presented in Chapter 3 of the dissertation.
68 Khew, S. K. aka Commander, leads the butterfly interest group ‘Butterflies of Singapore’. He is
also this authors’ colleague in CPG. Source: http://www.butterflycircle.com/forums/
showthread.php?t=6993 69 Ong, J is the architect involved in the KTPH Project. Source: http://blog.cpgcorp.com.sg/?p=69

217
Bibliography
A) Books
7Group, Reed, B. (2009), “The Integrative Design Guide to Green Building: Redefining the
Practice of Sustainability”, John Wiley & Sons, New Jersey.
Almusaed, A. (2011), “Biophilic and Bioclimatic Architecture: Analytical Therapy for the Next
Generation of Passive Sustainable Architecture”, Springer-Verlag, London.
Bauer, M., Mösle, P., Schwarz, M. (2010), “Green Building: Guidebook for Sustainable
Architecture”, Springer.
Bay, J. H., Ong, B. L. (2006), “Tropical Sustainable Architecture: Social and Economic
Dimensions”, Architectural Press, Oxford.
Bechtel, B. R., Churchman, A. (2002), “Handbook of Environmental Psychology”, John Wiley
& Sons, New York.
Bell, P. A., Greene, T. C., Fisher, J.D., & Baum, A. (2001), “Environmental psychology (5th
edition)”, Fort Worth, Harcourt College Publishers
Bokalders, V., Block, M. (2010), “The Whole Building Handbook”, Earthscan, UK & USA.
Boubekri, M. (2008), “Daylighting, Architecture and Health: Building Design Strategies”,
Architectural Press, UK & USA.
Brawne, M. (2003), “Architectural Thought: The Design Process and the Expectant Eye”,
Architectural Press, Oxford.
Birkeland, J. (2002), Design for Sustainability: A Sourcebook of Integrated, Eco-logical
Solutions, Earthscan, UK & USA.
Cooper-Marcus, C. and Barnes, M. (1999), “Healing Gardens: Therapeutic benefits and design
recommendations”, New York, Wiley.
Dellinger, B. (2010), Chapter 3 ‘Healing Environments’ in “Evidence-Based Design for
Healthcare Facilities”, Sigma Theta Tau International, Indianapolis.
Deutsch, R. (2011), “BIM and Integrated Design: Strategies for Architectural Practice”, John
Wiley & Sons, New Jersey.

218
Bibliography (Cont’d)
Edwards, B. (2010), “Rough Guide to Sustainability: A Design Primer (Third Edition)”, RIBA
Publishing, London.Graham, P. (2003). “Building Ecology: First Principles for a
Sustainable Built Environment”. Blackwell Science: Oxford.
Guenther, R., Vittori, G. (2008), “Sustainable Healthcare Architecture”. John Wiley & Sons,
New Jersey.
Hillier, B. (1999), “Space is the Machine: A Configurational Theory of Architecture”,
Cambridge University Press.
Hyde, R. (2008), “Bioclimatic Housing: Innovative Design for Warm Climates”, Earthscan,
London.
Keeler, M., Burke, M. (2009), “Fundamentals of Integrated Design for Sustainable Building”,
John Wiley & Sons, New Jersey.
Kellert, S., Wilson, E. (ed) (1993), “The Biophilia Hypothesis”, Island Press, Washington.
Kellert, S. R., Heerwagen, J. H., Mador, M. L. (ed) (2008), “Biophilic Design: The Theory,
Science, and Practice of Bringing Buildings to Life”, John Wiley & Sons, New Jersey.
Krygiel, E. and Nies, B. (2008), “Green BIM: Successful Sustainable Design with Building
Information Modeling”, Wiley Publishing, Indianapolis.
Kwok, A. G. and Grondzik, W. T. (2007), “The Green Studio Handbook”, Architectural
Press, Oxford.
Lawson, B. (2004), “What Designers Know”, Architectural Press, Oxford.
Lawson, B. (2005), “How Designers Think: The Design Process Demystified (Forth Edition)”,
Architectural Press, Oxford.
LaHood, S. and Brink, M. V. (2010), Chapter 2 ‘Aesthetics and New Product
Development’ in “Evidence-Based Design for Healthcare Facilities”, Sigma Theta Tau
International, Indianapolis.
McCullough, C. (ed) (2010), “Evidence-Based Design for Healthcare Facilities”, Sigma Theta
Tau International, Indianapolis.
Olgyay, V. (1963), “Design with climate: bioclimatic approach to architectural regionalism”,
Princeton University Press, Princeton, New Jersey.
Riggs, J. L. (1982), “Engineering economics”, McGraw-Hill, New York.

219
Bibliography (Cont’d)
Sinclair, D. (2008), “Leading the Team: An Architect’s Guide to Design Management”, RIBA
Publishing, London.
Szokolay, S. (2008), “Introduction to Architectural Science (Second Edition)”, Elsevier, UK.
Tzonis, A. (2006), Chapter 2 Rethinking Design Methodology for Sustainable Social
Quality, in Bay, J. H., Ong, B. L. (2006), “Tropical Sustainable Architecture: Social and
Economic Dimensions”,. Architectural Press, Oxford.
Ulrich, R. S., Lawson, B., & Martinez, M. (2003). “Exploring The Patient Environment: An
NHS Estates Workshop”. The Stationery Office: London
Verderber, S. (2010), “Innovations in Hospital Architecture”, Routledge, New York.
Williams, D. E. (2007), “Sustainable Design: Ecology, Architecture, and Planning”, John
Wiley & Sons, New Jersey.
Wilson, E. (1984), “Biophilia”, President and Fellows of Harvard College, USA.
Yeang, K. (2006), “Ecodesign: A Manual for Ecological Design”, John Wiley & Sons.
Yeang, K., Woo, L. (2010), “Dictionary of Ecodesign”, Routledge, London & New York.
Yudelson, J. (2009), “Green Building through Integrated Design”, McGraw-Hill, USA.
B) Journal Articles
Abdelhamid, T.S., El-Gafy, M., and Salem, O. (2008), Lean Construction: Fundamentals
And Principles, American Professional Constructor Journal.
Gauld, R., Ikegami, N., Barr, M. D., Chiang, T. L., Gould, D., Kwon, S. (2006), Advanced
Asia’s health systems in comparison, Health Policy, 79, p.p. 325–336. Elsevier.
Hartkopf, V., Loftness, V. (1999), Global relevance of total building performance,
Automation in Construction, 8, p.p. 377 – 393, Elsevier.
Hartkopf, V., Loftness, V., Mill, P. A. D. (1986), The Concept of Total Building
Performance and Building Diagnostics in Building Performance: Function,
Preservation, and Rehabilitation, David, G., Ed., p.p. 5 – 22, American Society of Testing
and Materials, Philadelphia.
Lai-Chuah, R. (2008), A Class Apart, World Health Design, April ed., p.p. 30-35.

220
Bibliography (Cont’d)
Lawson, B. (1993), Parallel lines of thought, Languages of Design 1(4), p.p. 357–366.
Lim, M. K. (2003), Shifting the burden of health care finance: a case study of public–
private partnership in Singapore, Health Policy, 69, p.p. 83–92, Elsevier.
Millard W. B. (2007). The cost of koi: evidence-based design in emergency medical
facilities. Annals of Emergency Medicine, Volume 50, No. 3, p.p. 267-271.
Rechel, B., Buchan, J., McKee, M. (2008), The impact of health facilities on healthcare
workers’ well-being and performance. International Journal of Nursing Studies, 46, p.p.
1025 – 1034.
Sailer, K., Budgen, A., Lonsdale, N., Turner, A., and Penn, A., (2010), Pre and Post
Occupancy Evaluations in Workplace Environments: Theoretical Reflections and
Practical Implications, Journal of Space Syntax, Volume 1, Issue 1, p.p. 199-213, Bartlett
School of Graduate Studies and Spacelab.
Shermana, S. A., Varnib, J. W., Ulrich, R. S., Malcarned, V. L. (2005), Post-occupancy
evaluation of healing gardens in a pediatric cancer center, Landscape and Urban
Planning, 73, p.p. 167 – 183, Elsevier.
Ulrich, R. S. (1984), View through a window may influence recovery from surgery,
Science, 224(4647), p.p. 420-421.
Ulrich, R. S., (1986), Human Responses to Vegetation and Landscape, Landscape and
Urban Planning, 13, p.p. 29 – 44, Elsevier.
Ulrich, R. S. (1991), Effects of interior design on wellness: Theory and recent scientific
research, Journal of Health Care Interior Design, 3(1), p.p. 97-109.
Ulrich, R. S. (1999), Effects of gardens on health outcomes: Theory and research, C.
Cooper Marcus & M. Barnes (Eds.), Healing gardens, p.p. 27-86, New York, Wiley.
Ulrich, R. S., & Gilpin, L. (2003), Healing arts: Nutrition for the soul. In S. B. Frampton, L.
Gilpin & P. Charmel (Eds.), Putting patients first: Designing and practicing patient-
centered care, p.p. 117-146, San Francisco, Jossey-Bass.
Ulrich, R. S. (2006), Evidence Based Healthcare Architecture, Medicine and Creativity, 368,
p.p. 538 – 539.
Whitehouse, S., Varni, J. W., Seid, M., Cooper-Marcus, C., Ensberg, M. J., Jacobs, J. R., et
al (2001), Evaluating a children's hospital garden environment: Utilization and
consumer satisfaction, Journal of Environmental Psychology, 21(3), p.p. 301-314.

221
Bibliography (Cont’d)
C) Conference Papers, White Papers & Technical Reports:
Almusaed, A. (2011), “Biophilic Architecture: Towards a New Potential of Healthy
Architecture”, Rethinking Sustainable Construction 2006: Next Generation Green
Buildings, Sarasota, Florida, USA 19 – 22 September 2006. Internet WWW Page at:
<http://www.cce.ufl.edu/rsc06/ paper_pres.html> (Accessed 12.11.2011)
Bay, J. H. (2004), “Socio-climatic Design for High-Rise Dwellings”, The 21th Conference on
Passive and Low Energy Architecture, Eindhoven, The Netherlands, 19 – 22 September
2004.
Cheng, T. F. (2011), “BCA BIM Roadmap”, BuildingSmart BIM International Conference
Conference, Singapore, 21 September 2011.
Ismail, L. H., Sibley, M. (2006), “Bioclimatic Performance of High Rise Office Buildings:
A Case Study in Penang Island”, The 23rd Conference on Passive and Low Energy
Architecture, Geneva, Switzerland, 6-8 September 2006.
Heiselberg, P., Ad van der Aa (2010). Strategies for Integrative Building Design. In:
Conference: The Future for Sustainable Built Environments with High Performance Energy
Systems. Munich, Germany 19 - 21 Oct 2010. WWW Page at: <http://www.conference.
annex49.de/vortraege/05_Heiselberg.pdf> and <http://vbn.aau.dk/files/43876359/
Strategies_for_Integrative_Building_Design.pdf > (Both accessed 26.06.2011).
Jahnkassim, P. S., Ip, K. (2006), “Linking bioclimatic theory and environmental
performance in its climatic and cultural context – an analysis into the tropical
highrises of Ken Yeang”, The 23rd Conference on Passive and Low Energy Architecture,
Geneva, Switzerland, 6-8 September 2006.
Kellert, S. R. (2004), “Beyond LEED: From Low Environmental Impact to Restorative
Environmental Design”, keynote address, Greening Rooftops for Sustainable
Communities Conference, Portland, USA 4 June 2004.
Liak, T. L. (2009). “Planning for a Hassle-Free Hospital: The Khoo Teck Puat Hospital”,
6th Design & Health World Congress 2009, Singapore, 25-27 June 2009. Internet WWW
Page at: <http://www.designandhealth.com/Events/Singapore-Congress-2009.aspx>
Tucci, J. (2004), “The Singapore Health System – Achieving Positive Health Outcomes
With Low Expenditure”, Watson Wyatt Healthcare Market Review, October 2004.

222
Bibliography (Cont’d)
Ulrich, R. S. (2000), “Evidence Based Environmental Design for Improving Medical
Outcomes”, McGill University Health Centre, Healing by Design: Building for Health
Care in the 21st Century, Montreal, Canada 20 - 21 Sep 2000. Internet WWW Page at:
<http://muhchealing.mcgill.ca/english/ Speakers/ulrich_p.html> (Accessed 27.06.2011).
Ulrich, R. S. (2002), Health Benefits of Gardens in Hospitals, International Exhibition
Floriade 2002, Floriade, Netherlands 20 - 21 Sep 2000. Internet WWW Page at:
<http://www.greenplantsforgreenbuildings.org/attachments/contentmanagers/25/Hea
lthSettingsUlrih.pdf> (Accessed 27.06.2011).
Ulrich, R. S., Quan X., Zimring, C., Joseph, A., Choudhary, R. (2004), The Role of the
Physical Environment in the Hospital of the 21st Century: A Once-in-a-Lifetime
Opportunity, Report to The Center for Health Design for the Designing the 21st
Century Hospital Project. WWW Page at: <http://www.rwjf.org/files/publications/
other/RoleofthePhysicalEnvironment.pdf> (Accessed 27.10.2011].
World Health Organization (2008), The world health report 2008: primary health care now
more than ever.
D) Technical Reports
CABE Healthcare report. (2004), The role of hospital design in the recruitment, retention and
performance of NHS nurses in England, Prepared by: PricewaterhouseCoopers in
association with University of Sheffield and Queen Margaret University College,
Edinburgh.
Design Business Case Study: Alexandra Hospital. (2009), Design Singapore Council:
Singapore. WWW Page at: <http://www.designsingapore.org/Files/Bcs/
Alexandra_Hospital.pdf> (Accessed 31.12.2011)
Kleczkowski, B. M. & Pibouleau, R. (ed) (1983). Approaches to Planning and Design of
Health Care Facilities in Developing Areas. World Health Organization: Switzerland.
Lawson, B., (2005), Evidence-based Design for Healthcare, Business Briefing: Hospital
Engineering & Facilities Management, Issues 2, p.p. 25-27, Touch Briefings
Singer, B. C., Tschudi, W. F. (2009). High Performance Healthcare Buildings: A Roadmap
to Improved Energy Efficiency. Lawrence Berkeley National Laboratory. WWW Page
at: < hightech.lbl.gov/documents/healthcare/lbnl-2737e.pdf> [Accessed 27.10.2011].
Reed, B., Todd, J. A., Malin, A. (2005). Expanding Our Approach to Sustainable Design: An
Invitation. Building Green Inc: Brattleboro.

223
Bibliography (Cont’d)
Rossi, R. M., Brown, D., Park, B., Boser, R. (2009). The Integrated Design Process On Paper
and In Practice: A Case Study. Illinois State University.
World Health Organization (2009). System Thinking for Health Systems Strengthening.
E) Theses
Ng J. C. (2005), Development of Total Building Performance (TBP) Assessment System for
Office Building, MSc. Department of Building, National University of Singapore.
Kong, P. (2005), Gardening in Semi-open Spaces in Tropical High-Rise Housing: Environmental
and Social Benefits, Masters of Arts (Architecture) thesis.
Sng, P. L. (2011), In What Way Can Green Building Contribute to Human Wellness in the
Singapore Context? M Arch. National University of Singapore.
Wu, Z. (2011), Evaluation of a Sustainable Hospital Design Based on Its Environmental and
Social Outcomes, MSc. Cornell University.
F) Guides, Brochure, Pamphlets and Newsletters
ABC Waters Design Guidelines (2011, 2nd ed.), Public Utilities Board: Singapore.
American Institute of Architects (2007), Integrated Project Delivery: A Guide. USA.
American Institute of Architects (2007), Integrated Project Delivery: A Working Definition.
USA.
ANSI MTS 1.0 WSIP Guide (2007), Whole System Integrated Process Guide for Sustainable
Buildings and Communities, ANSI, USA.
Busby Perkins+Will and Stantec Consulting (2007), Roadmap for the Integrated Design
Process, British Columbia Green Building Roundtable, Canada.
Butcher, K. (2005), Natural Ventilation in Non-Domestic Buildings. CIBSE. Internet WWW
Page at http://www.ihsti.com/CIS (UK Construction Information Service) (Accessed
22.08.2010].
Centre for Total Building Performance – First building research centre devoted to
building performance studies in the tropics, Synectics Aug 2001, p.p. 1-3, National
University of Singapore.

224
Bibliography (Cont’d)
Cheong, H. F. (2001), The Synectic Approach to Building, Synectics Aug 2001, p. 1,
National University of Singapore.
CIBSE Guide A: Environmental Design. (2006), CIBSE, UK.
Cohen, J. (2010), Integrated Project Delivery: Case Studies, AIA, USA.
Cole, J. Hatten, M. Integrating Engineering & Performance Modeling Into the Design Process.
BetterBricks, USA.
Green Building Platinum Series: Building Planning and Massing (2010), Building Control
Authorities, Singapore.
Guide to the Design and Construction of High Performance Hospitals, BetterBricks, USA.
Guidelines on External Thermal Transfer Value for Buildings. (2004), Building Control
Authorities, Singapore.
Health Technical Memorandum 07-07: Sustainable Health and Social Care Buildings. (2009),
Department of Health, UK.
ISO 14040 (2006). Environmental management – Life cycle assessment – Principles and
framework, International Organisation for Standardisation (ISO), Geneve
Larsson, N. (2004), The Integrated Design Process, iiSBE, Ottawa.
Lim, J. (2007), Getting It Right – The Challenge of Healthcare Planning, Singapore
Medical Association Newsletter Insight, Oct 2007, Vol 39 (10).
Mason, T. (2006), Designed with Care: Design and Neighbourhood Health Care Buildings,
CABE, London.
Ofori, G. (2003), New Performance-based Procurement Approach through Total Building
Performance, Synectics Nov 2003, p. 1, National University of Singapore.
Ray, D. Healthcare: A Business and Ethical Case for Sustainability, BetterBricks, USA.
Rennie, D. and Parand, F. (1998), Environmental Design Guide, BRE, London.
Total Building Performance in Action, Synectics Nov 2003, p.p. 4-5. National University
of Singapore, Universal Design Guide (2007), Building Control Authorities, Singapore.

225
Bibliography (Cont’d)
van der Aa, A., Heiselberg, P., and Perino., M. (2011), Designing with Responsive Building
Elements, Aalborg University, Denmark.
Whole System Integration Process (WSIP), The Institute for Market Transformation to
Sustainability, Washington
Zimmerman, A. Integrated Design Process Guide, CMHC, Canada.
G) Electronic Sources and Websites:
About BCA Green Mark Scheme. WWW at Building Control Authorities, Singapoe.
Internet WWW page at: <http://www.bca.gov.sg/greenmark/green_mark_
buildings.html> (Accessed 23.01.2012. Created 2006. Revised 15.12.2011).
Carpenter, T. Lean-Led Design: Rules of the Road. WWW at Lean Healthcare Exchange.
Internet WWW page at: <http://www.leanhealthcareexchange.com/> (Accessed
29.01.2012. Created 26.01.2012)
Carr, R. Healthcare Facilities. WWW at Whole Building Design Guide. Internet WWW
page at: < http://www.wbdg.org/design/health_care.php> (Accessed 26.10.2011.
Revised 30.12.2010).
Carr, R., Hospital. WWW at Whole Building Design Guide. Internet WWW page at: <
http://www.wbdg.org/design/hospital.php> (Accessed 26.10.2011. Revised
21.04.2011).
Carr, R., Hospital. WWW at Centre for Sustainable Healthcare. Internet WWW page at:
<http://www.wbdg.org/design/hospital.php> (Accessed 26.10.2011. Revised
21.04.2011).
Centre for Total Building Performance. WWW at BCA-NUS Centre for Total Building
Performance. Internet WWW Page at: <http://www.ctbp.bdg.nus.edu.sg/main.htm>
(Accessed 27.06.2011).
Chang, G., Solace in the hospital grounds. WWW at Channel News Asia Website. Internet
WWW page at: <http://www.channelnewsasia.com/stories/singaporelocalnews/
view/282365 /1/.html> (Accessed 31.12.2011. Posted 15.06.2011).
Developing a Vision for Sustainable Healthcare Building. WWW at Sustainable Healthcare
Network Website. WWW Page at: <http://www.shine-network.org.uk/
?p=mod_contents&mod=4> (Accessed 08.01.2012)

226
Bibliography (Cont’d)
Energy Studies in Buildings Laboratory, University of Oregon, and Konstrukt, Rethinking
the Design Process, presentation. WWW at Betterbricks: Design Approach. Internet
WWW Page at: <http://www.betterbricks.com/graphics/assets/documents/IED-
Rethinking_Design.pdf> (Accessed 25.06.2011).
Fuller, S., Life-Cycle Cost Analysis (LCCA). WWW at The Whole Building Design Guide.
Internet WWW page at: <http://www.wbdg.org/resources/lcca.php> (Accessed
10.01.2012. Revised 28.06.2010).
FuturArc Showcase, Khoo Teck Puat Hospital: Healing Gardens. WWW at The Whole
Building Design Guide. Internet WWW page at: <http://www.futurarc.com/
previous_edition/ktph_suoire.cfm> (Accessed 25.11.2011).
Haynes, D. Adopting Lean Practices in the Architectural/Engineering Industry. WWW at
AECbytes. Internet WWW page at: < http://www.aecbytes.com/viewpoint/2012/
issue_63.html> (Accessed 29.01.2012. Created 18.01.2012)
History of Alexandra Hospital. WWW at Jurong Health Alexandra Hospital. Internet
WWW page at: <http://www.alexhosp.com.sg/index.php/about_us/our_history>
(Accessed 31.12.2011).
Integrated Design: The Best Path to Highly Efficient Buildings Website. WWW at Betterbricks.
Internet WWW Page at: <http://designsynthesis.betterbricks.com/> (Accessed
25.06.2011. Revised 2010).
Integrated Design: Synergy Case Studies. WWW at Betterbricks. Internet WWW Page at:
<http://designsynthesis.betterbricks.com/synergy-case-studies> (Accessed 25.06.2011.
Revised 2010).
Integrated Design: Tools and Resources. WWW at Betterbricks. Internet WWW Page at: <
http://www.betterbricks.com/design-construction/tools/integrated-design-process-
tools> (Accessed 25.06.2011. Revised 2010).
Healthcare. WWW at Space Syntax website. Internet WWW Page at
<http://www.spacesyntax.com/projects-clients-partners/building-planning-
design/healthcare/> (Accessed 31.12.2011.)
Khoo Teck Puat Hospital Specialties and Services: Diabetes. WWW at Khoo Teck Puat
Hospital. Internet WWW Page at <http://www.ktph.com.sg/main/
specialties_n_services/4/6> (Accessed 31.12.2011. Created 2010)

227
Bibliography (Cont’d)
Khoo Teck Puat Hospital Specialties and Services: Overview. WWW at Khoo Teck Puat
Hospital. Internet WWW Page at < http://www.ktph.com.sg/main/pages> (Accessed
31.12.2011. Created 2010)
Prowler, D., Whole Building Design. WWW at The Whole Building Design Guide. Internet
WWW Page at: < http://www.wbdg.org/wbdg_approach.php> (Accessed 10.07.2011.
Updated 13.05.2011).
Rostenberg, B., Baum, M., Shepley, M., Ginsberg, R., Sustainability and Evidence: The
intersection of evidence-based design and sustainability. WWW at World Health Design.
Internet WWW Page at: <http://www.worldhealthdesign.com/sustainability-and-
evidence.aspx> (Accessed 5.11.2011).
Smith, R. and Watkins, N., Therapeutic Environments. WWW at The Whole Building
Design Guide Website. WWW Page at: <http://www.wbdg.org/resources/
therapeutic.php> (Accessed 10.01.2012. Updated 18.06.2010).
The Total Building Performance Approach. WWW at BCA-NUS Building Energy
Information and Research Centre Website. Internet WWW Page at:
<http://www.bdg.nus.edu.sg/ buildingenergy/regulations/index.html> (Accessed
27.06.2011).
Todd, J. A., Planning and Conducting Integrated Design (ID) Charrettes. WWW at The
Whole Building Design Guide. Internet WWW Page at: <http://www.wbdg.org/
resources/charrettes.php> (Accessed 24.06.2011. Revised 28.12.2009)
Todd, J. A., Measuring Performance of Sustainable Buildings. WWW at The Whole Building
Design Guide Website. Internet WWW Page at: <http://www.wbdg.org/index.php>
(Accessed 25.06.2011. Updated 13.05.2011).
Todd, V., Making the Mental Shift to Integrated Project Delivery, WWW at IPD Seminar
series presentation. Internet WWW Page at: <http://www.ipd-
ca.net/PDFs/Sanvido%20Mental%20Shift.pdf> (Accessed 27.06.2011).
Trajectory of Environmentally Responsive Design, (2006). WWW at Integrative Design
Collaborative. Internet WWW Page at: <http://www.integrativedesign.net/
resources.htm> (Accessed 19.12.2011).
WBDG Aesthetics Subcommittee, Engage the Integrated Design Process. WWW at The
Whole Building Design Guide. Internet WWW page at: <http://www.wbdg.org/
design/engage_process.php> (Accessed 24.06.2011. Revised 30.10.2010).

228
Bibliography (Cont’d)
H) Unpublished Documents
Alexandra Hospital @ Yishun (Dec 2005). Tender briefing material design competition
for Alexandra Hospital at Yishun, which was later renamed as Khoo Teck Puat
Hospital. CPG file archive.
Minutes of Khoo Teck Puat Hospital Planning Committee (HPC) Meeting. CPG file
archive.
Architectrural Powerpoint presentation slides and file document during design
completion, masterplan, concept design, and design development stages. CPG file
archive.
Mechanical & Electrical Engineering Powerpoint presentation slides and file document
during design completion, masterplan, concept design, and design development
stages. CPG file archive.
Green Mark Powerpoint presentation slides and file document during design
completion, masterplan, concept design, and design development stages. CPG file
archive.
I) Chapter Page Quotations
Chapter 1:
Upper: Schettler, T. “From Medicine to Ecological Health”, in: Guenther, R., Vittori, G.
(2008), “Sustainable Healthcare Architecture”, John Wiley & Sons, New Jersey, p. 68
Lower: Guenther, R., Vittori, G. (2008), “Sustainable Healthcare Architecture”, John Wiley &
Sons, New Jersey.
Chapter 2:
Upper: Reed, B. “Integrative Design Process: Changing Our Mental Model”, in:
Guenther, R., Vittori, G. (2008), “Sustainable Healthcare Architecture”, John Wiley &
Sons, New Jersey, p. 133.
Lower: Zimmerman, A. Integrated Design Process Guide, CMHC, Canada, p. 4.
Chapter 3:
Upper: Khaw B. W. In: Liak, T. L. (2009). “Planning for a Hassle-Free Hospital: The Khoo
Teck Puat Hospital”, 6th Design & Health World Congress 2009, Singapore, 25-27
June 2009.
Lower: Verderber, S. (2010), “Innovations in Hospital Architecture”, Routledge, New
York.

229
Bibliography (Cont’d)
Chapter 4:
Upper: Or, D. In: Guenther, R., Vittori, G. (2008), “Sustainable Healthcare Architecture”,
John Wiley & Sons, New Jersey, p. 135.
Lower: Heinfeld, D. In: Yudelson, J. (2009), “Green Building through Integrated Design”,
McGraw-Hill, USA, p. 69.
Chapter 5:
Upper: Guenther, R., Vittori, G. (2008), “Sustainable Healthcare Architecture”, John Wiley &
Sons, New Jersey, p. 154.
Lower: Berkebile, B. In: Guenther, R., Vittori, G. (2008), “Sustainable Healthcare
Architecture”, John Wiley & Sons, New Jersey, p. 19.
Appendix I: Kwok, A. G. and Grondzik, W. T. (2007), “The Green Studio Handbook”,
Architectural Press, Oxford, p. 18.
Appendix II: 7Group, Reed, B. (2009), “The Integrative Design Guide to Green Building:
Redefining the Practice of Sustainability”, John Wiley & Sons, New Jersey, p. 68.
Appendix III: Krygiel, E. and Nies, B. (2008), “Green BIM: Successful Sustainable Design
with Building Information Modeling”, Wiley Publishing, Indianapolis, p. 32.
Appendix IV: Krygiel, E. and Nies, B. (2008), “Green BIM: Successful Sustainable Design
with Building Information Modeling”, Wiley Publishing, Indianapolis, p. 53.
Appendix V: Batshalom , B. In: 7Group, Reed, B. (2009), “The Integrative Design Guide to
Green Building: Redefining the Practice of Sustainability”, John Wiley & Sons, New Jersey,
p. 16.
Appendix VI: Lawson, B., (2005), Evidence-based Design for Healthcare, Business
Briefing: Hospital Engineering & Facilities Management, Issues 2, p. 27.
Appendix VII: Deutsch, R. (2011), “BIM and Integrated Design: Strategies for Architectural
Practice”, John Wiley & Sons, New Jersey, p. 138.
Appendix VIII: Verderber, S. (2010), “Innovations in Hospital Architecture”, Routledge,
New York, p. 52.
Appendix IX: Guenther, R., Vittori, G. (2008), “Sustainable Healthcare Architecture”, John
Wiley & Sons, New Jersey, p. 119.
Appendix X: Karolides, A. “Energy Use, Energy Production, And Health”. In: Guenther,
R., Vittori, G. (2008), “Sustainable Healthcare Architecture”, John Wiley & Sons, New
Jersey, p. 286.

230
Bibliography (Cont’d)
Appendix XI: Krygiel, E. and Nies, B. (2008), “Green BIM: Successful Sustainable Design
with Building Information Modeling”, Wiley Publishing, Indianapolis, p. 56.
Appendix XII: Keeler, M., Burke, M. (2009), “Fundamentals of Integrated Design for
Sustainable Building”, John Wiley & Sons, New Jersey, p. 231.
Appendix XIII: Yeang, K. “Green Design in the Hot Humid Tropical Zone”, in: Bay, J. H.,
Ong, B. L. (2006), “Tropical Sustainable Architecture: Social and Economic Dimensions”,
Architectural Press, Oxford, p. 53.
Appendix XIV: Guenther, R., Vittori, G. (2008), “Sustainable Healthcare Architecture”, John
Wiley & Sons, New Jersey, p. 119.
Appendix XV: Kellert, S., Wilson, E. (ed) (1993), “The Biophilia Hypothesis”, Island
Press, Washington, p. 32.