catalyst event report on identifying the gaps in dementia...
TRANSCRIPT
1
Catalyst Event Report on
Identifying the gaps in dementia research;
Opportunities for novel approaches through
collaborations
Aintree Race Course, Wednesday 22nd January 2014
2
CONTENTS PAGE
Purpose of the day 4
Presentations from Alistair Burns and Ann Johnson 5-6
Visual Minute start of the day 7
Convenor Reports:
Group 1 - How can research make a difference to the loss of friendships that
people with dementia currently experience possibly resulting in social isolation. 8
Group 2 - Post diagnostic support for people living with dementia and their families 9
Group 3 - Changing the name of dementia 10
Group 4 - How can we actively involve people with dementia and their
families in research and let them know about research findings?
Any examples? What has been the result/impact? 11
Group 5 - How do we evaluate the impact of staff training on the care/experience of
people with dementia 12
Group 6 - Involving people with a learning disability and their families/carers in
research 13
Visual minute session 1 14
Group 7 - The impact of the barriers of language, culture and faith to early diagnosis
and post diagnostic support for BME populations. 15
Group 8 - Early diagnosis of the dementias – molecular markers / brain imaging 16
Group 9 - Sharing data and information – How can we improve overall data sharing
and levels of inflation? 17
Group 10 - How do we create a more patient society, frustration with repetition? 18
Group 11 -How to inspire and inform young people about dementia and encourage
them to think about working with people with dementia as a career option. 19
Group 12 - How can technology (e.g. mobile technology, electronic data) support
people with dementia and their carers. 19
Group 13 - How can research result in reducing the fear that people living with dementia
experience every day (Ann Johnsons word terror) 20
Continued...
3
Group 14 - Dementia and criminal justice 21
Visual minute session 2 23
Group 15 - Keeping dignity as dementia progress’s 24
Group 16 - Support for family members – Problems and what is needed 25
Group 17 - What is the evidence for the effectiveness of interventions in dementia 25
Group 18 - Individualisation of solutions for people with dementia and support 26
Group 19 - Potential for continued employment for people with dementia 27
Group 20 - Do we have an evidence base for understanding whether staff delivering
care to residential elderly have sufficient training knowledge of dementia 28
Group 21- Family and friends, changes in relationships, roles, continuity and
discontinuity of wider social relationships. 28
Group 22 - The barriers between general community services and mental health s
ervices e.g. training of front line carers 29
Visual Minute session 3 31
Group 23 - Dementia – Dementias, disease sub types within ‘dementia’ individual
care for dementia subtypes 32
Group 24 - Sensory life day, work and development/ measurement 33
Group 25 - Remote, mobile, personalised technologies 34
Group 26 - Adapting mindfulness based practice for people with dementia and
measuring clinical efficacy in terms of quality of life - Emotional - Regulation 35
Summary / Next Steps 36
Visual minute—As a result of today 37
Feedback from Survey Monkey 38
Poster Feedback 40
Postcard Feedback 41

4
Catalyst Event Report on
Identifying the gaps in dementia research; opportunities for
novel approaches through collaborations
Aintree Race Course, Wednesday 22nd
January 2014
Purpose
The event brought together prominent people from
diverse backgrounds across the North West of Eng-
land who have an interest in dementia research. It
is hoped the event allowed attendees to begin collaborative work across their organizations, with a
view to developing innovative bids for National Institute for Health Research (NIHR) / EU funding.
The event was conducted using a forum known as ‘Open Space’. The method is designed to enable
people with mutual interests to meet and progress ideas in a short period of time. Participants have
control over what is discussed and can choose to include themselves in various forums generated on
the day. At the conclusion of the various forums, decisions are made about outcomes and further steps
to progress them. Participants are expected to contribute further via the networks developed on the
day.
A summary of the Open Space discussions, including the names of participants and those expressing an
interest in being contacted at a later date, form the basis of this workshop summary.
The discussions are not presented in any particular order and do not reflect the popularity or the merit
of the research themes. Some themes are closely interlinked and could be collated.
Visual minutes were made during the event by a team of artists and those minutes are also included in
this report.
5
Workshop Summary
Presentations
Dr Stuart Eglin, Director of NHS Research and Development North West, introduced the day and
went through the concept of the Catalyst event and how it was a highly participatory event. He stat-
ed that everybody attending the event had an interest in dementia and all would have something to
contribute. Stuart introduced the next speakers, Professor Alistair Burns National Director for De-
mentia at NHS England and Ann Johnson who is living with dementia.
Alistair Burns National Direction for Dementia at NHS England
(Summary)
Awareness of dementia has never been higher than it is currently and a lot of interest has been
generated that wasn’t happening 5 out of10 years ago. There has been interest from the general
public and the main point, now, is to change awareness into action.
The National Dementia strategy from 2009 has been running for 5 years.
The prime ministers challenge on dementia includes 2 important points:
1. For people over 55, dementia is the most feared illness. It is important to create a dementia
friendly community and the issue of awareness.
2. Diagnosis and the support people receive after diagnosis
It is important to try to raise the amount of money to enable research into dementia to take place.
For every £1.30 spent on research only 5p is spent on dementia research. We need to double it by
2015 and we are well on the way for that to happen.
We need to look at how we manage research in dementia and how to raise the profile. Money,
alone wouldn’t make much difference. The key thing is to get younger researchers to think of de-
mentia research as a career, (it’s as good as cancer research!) and to engage more mature re-
searcher’s as well.
There is lots of money for dementia right now, and it has never been a better time to do research.
There was the G8 Summit (December 2013) focusing on the social impact of dementia and remem-
bering that prevention is also important with regular exercise, a healthy diet and social interaction
playing a role.
We need to think of Dementia as a long term health condition.
6
Ann Johnson – Living with Dementia
‘ I have dementia but I have a life!’
(Summary)
Ann was a trained nurse and was diagnosed with dementia 8 years ago when she was 52 years old. She
now lives in a care home in Altrincham. She first went to see her GP about her symptoms in the Decem-
ber, and was diagnosed in October.
Anne talked through the strategies she uses that help her to deal with dementia on a daily basis, which
aren’t hi-tech, just simple things such as a talking watch, dictaphone and a tag that is worn with address
details in case she gets lost.
3 main things that keep her going:
Friends
Faith
Speaking/ talks to groups of people
Without these she would be lost. The talks give a purpose for living and she enjoys travelling all over the
country.
Anne is involved in part of the Dementia Strategy which was launched in 2009. She is also part of the
Prime Ministers dementia friendly group which enables her to meet many different people and connect
with people from different organisations. From this she has joined the Sainsbury’s retail group to help
them look at how they can help people with dementia. Lots of business’s are on board with this.
Anne has also received an honorary doctorate from the University of Bolton and also an MBE.
She challenged the group with “What can you do for me??’
7
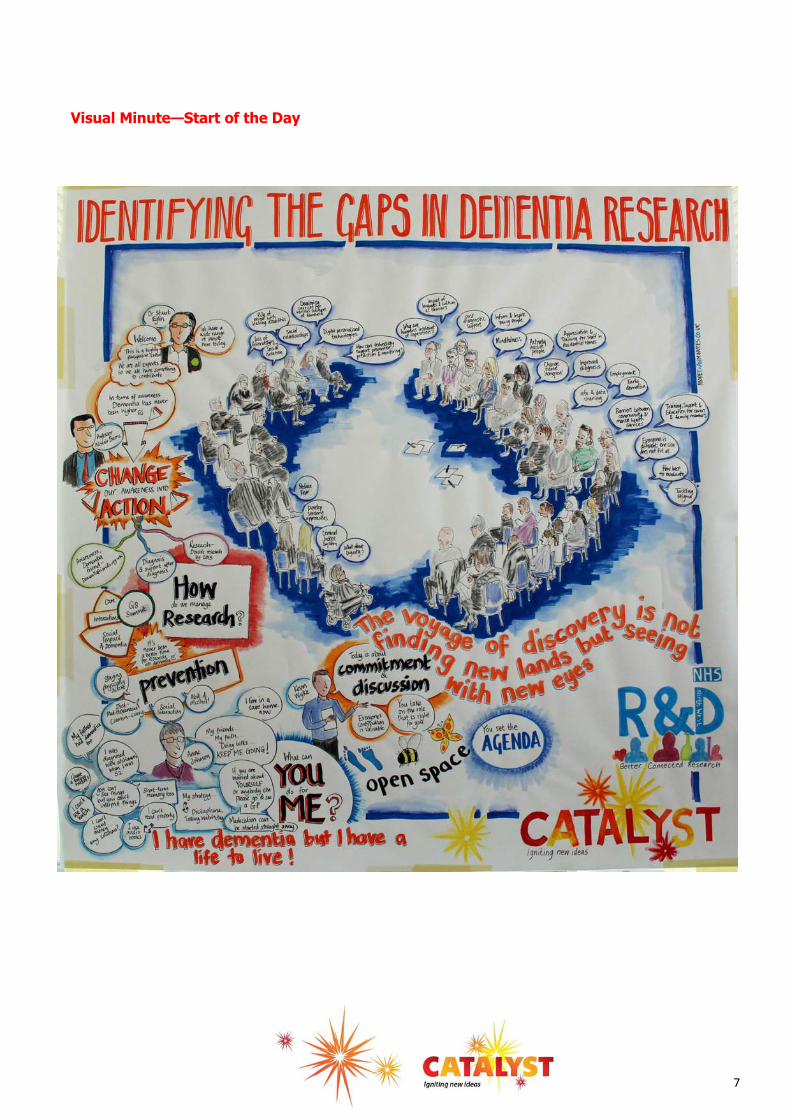
Visual Minute—Start of the Day

8
Convenor reports
Group 1 - How can research make a difference to the loss of friendships that people with dementia currently experience possibly resulting in social isolation.
Convenor – Sue Clarke and Ann Johnson
Participants -
Pauline Banks -University of West Scotland,
Michelle Collins – Person Shaped Support
Sally Spencer - Editor for the Cochrane Group
Tony Gatrell – Dean Lancaster University
Tracy Collins – Occupational Therapist – University of Salford
Christine Milligan – Lecturer University of Lancaster
Stephanie Tierney – Manchester University
Key points from the discussion:
Why it is that friends disappear, what causes them to withdraw? Is it fear? Perhaps people don’t know what to say, similar to bereavement/divorce?
Is this the case for other disease/conditions?
We all need social contact/networks/friendships’
People who have had the worst quality of life are the most socially isolated.
Befriending services extremely helpful volunteers are matched up with a person with dementia with similar interests.
People’s self-awareness in conversation with people with dementia is key – not to be embar-rassed if there is no answer/inappropriate answer. Don’t jump in if a person is struggling for words.
Loss of friendships impact on carers and families as well.
If anything is wrong you find out who your friends are
People in the public eye need to speak out when they have dementia
Social activity needs to be meaningful. That also maintains respect and dignity of the person

9
Next steps:
Research into importance of not becoming socially isolated.
Different levels of friendships
Research into befriending
Continue the conversation about dementia, open and honest to dispel the myths and the stigma to help reduce the fear.
Social networks may need to be maintained differently – virtual links and technology
Group 2 - Post diagnostic support for people living with dementia and their families
Convenor – Hilda Hayo
Participants
Gill Drummond -Caroline Hampson (OT) - Nicola Jarvis (L.D –Psychologist) - Joanne Singleton—Damien Mentali – (Neuro Science) - Rumona Dixone
Key points from the discussion:
What about people who do not want a diagnosis?
What happens after diagnosis – Timely? – Ongoing?
How can we support families? – Top Tips, Lists/Sheets ( under evaluation)
Nursing Home and Day Service Support
Working group – MDT with dementia
Individual tips
Up to date information – should be communicated through talking, explaining rather than depend-
ing on papers and people finding out for themselves.
Interactive and applied
Positive role models – paid person living with dementia to share his experience with others.
Research needed about peer support
Best practice models of post diagnostic support needed
Hearing people synthesise evidence (CLAHRC Research)
Pre- diagnostic support - what happens immediately before?
What are the triggers for seeking diagnosis
What about genetic disorders
Scotland – 12 month post diagnostic support
Are outcomes better if the diagnosis is accepted and worked with
10
Inundated with written information but lacking in support– consistency can be difficult
Finances play a part in decisions
Respite care – model in Australia - family member and friend both attend
Who is going to fund it?
Next steps:
Explore models of best practice for post diagnostic support
Ask families want they need and people living with dementia and how their situation could be
improved?
Group 3 - Changing the name of dementia
Convenor – Alistair Burns
Participants
Pauline Parker -Pamela Duffy - Andrew Garrity - Rebecca Jones - Sarah Butchard -
Ricky Wallace - Lorraine Trainer - Gillian Southgate
Key points from the discussion:
It is more about stigma than about the name - you can call it what you want
Promote living well with dementia
Education –children – shops –clinicians – to reduce the fear and exclusion
Negative association with treatment/decline
Billboard campaign in Liverpool was very positive
Carers can see/experience more stigma than the person living with dementia
Biggest fear is the fear of going into a care home
Change the underlying issues/views of dementia rather than change the name
Ability of people to associate themselves / their loved ones with people with dementia
Possibly early in the journey to changing attitudes
Lots of awareness raising but yet to change attitudes
Dementia is brain failure
In the USA name changed to neuro- cognitive disorder
Next steps:
Education for many but specifically for young people
JK Rowling to get involved with younger people
Work with businesses to encourage them to be more dementia friendly e.g supermarkets

11
Group 4 - How can we actively involve people with dementia and their families in research and let them know about research findings? Are there any examples? What has been the
result/impact of involving people in research?
Convenor – Melanie Chapman
Participants
Pauline Banks - Gav Cross - Lisa Woods - Chris Edwards - Christine Milligan -
Katrina Forsyth - Lorraine Trainer - Carol Taylor - John Keady -Dave Jones - Ricky Wallace
Stephanie Tierney - Chris Sew
Key points from the discussion:
Examples of involving people with dementia: The Scottish Dementia Working Group - people with dementia are involved when starting re-
search and developing projects. This has led to changes in design. Sue Burn is to do research on people who develop dementia when working.
Researchers at Manchester University have received ESRC funding to look at how to involve peo-ple in research. They have not been able to find courses or anything to empower people with dementia to take part. Creative methods may be useful.
Christine Milligan gave examples of co-research with older people; however, the ‘dementia nut still has to be cracked’. She has worked with older people to design and to carry out research. There are issues around training –if people receive a lot of training they are no longer just mem-bers of public/naive researchers. Can people only be naive researchers once?
Model of older people as researchers looking at gaps in services and designing services and peo-ple with dementia have been included.
Does the North West People in Research Forum include people with dementia?
Gav Cross – it feels like being on a journey. As a commercial entity his company, Immersive Spaces, has access to development money. He is thinking about how to support people with de-mentia to be part of product development. They are using projection lights and sound to change the environment (for example, with Mersey care exploring how immersive experience can contrib-ute to wellbeing, memory, conversation etc. They are holding group sessions to see if it has im-pact on evening experience (sun-downing) and whether it will reduce the medication needed.
Lisa Woods –product development has been significantly changed by involving people at the be-ginning of development process up to the end.
Dave Jones – would aspire to involve people in research. Areas for research would be carer sup-port, measuring outcomes for families, people using offender services who have dementia.
Issues around involving people with dementia
Ethical issues and gatekeeping issues may be challenging
The length of time it takes to gain funding and carry out research projects can take can be a par-ticular problem when involving people with dementia.
12
It is important to:
Listen effectively
Make sure the person has support (e.g. family/professional/carer)
Consider when people would be happy to take part. It may be that people with dementia can be part of a project but not involved in all of it, dipping in and out of a research project as their needs change
Group 5 - How do we evaluate the impact of staff training on the care/experience of people
with dementia
Convenor – Claire Surr
Participants
Dave Jones - John Keady - Graham Smith - David Powell - Andy Pownall
Key points from the discussion:
Sustainability and staff turnover – impact on outcomes.
Many areas have dementia strategies and dementia training – many providers asking is it effective and cost effective training? How do I choose what I purchase?
How do people respond to particular scenarios? Might lead to more insight into how people might change their behaviour?
What can you train? E.g. compassion select for it, can you train people to be compassionate?
Seeing training as continual development –organisations that support supervision and reflective practice.
Things get in the way of implementing training.
Lack of validated measures
What do people with dementia want? What is their view on the service they receive? How do we capture this?
Consensus on measures being used would be helpful - sharing of what is being used.
Evaluation – or lack of evaluation is common place. Many things occur without proper evaluation.
People can fear evaluation in case it is not shown to be effective.
Evaluation needs to be meaningful
What do we expect to achieve? Are we being over ambitious, should we expect less?
Is it possible to do something meaningful/valid? Too many other things that impact on care.
Being clear about what we expect the training to achieve. E.g. better care plans not necessarily better care.
13
Next steps:
Be honest about what training might be able to achieve and what not – what can we measure?
Sharing of existing tools, measures and approaches – consensus or recommended approaches.
Explore funding and resources to support evaluation of impact of training
Develop some scenario based measures to assess potential changes to behaviour
Group 6 - Involving people with a learning disability and their families/carers in research
Convenor – Nicola Jervis
Participants
Melanie Chapman - Chris Sewards - Noreen O’Sullivan - David Alsop
Key points from the discussion:
Ethics around testing people with Downs Syndrome – consent e.g. drug trials around dementia trails
Challenge = adapting materials
Challenge getting funding and consent
Smaller populations
Could we do some research with carers just what they would like?
What about research with friends of people with dementia, people with a learning difficulty who live with them?
People combining together
Next steps:
Speak to carers to see if they would be interested – pilot data
Service evaluations
Speak to people with a learning disability.
14
Visual Minute—Session 1

15
Group 7 - The impact of the barriers of language, culture and faith to early diagnosis and post diagnostic support for BME populations.
Convenor - Dee Abimbola
Participants
Sue Clarke - Ann Johnson - Di Burbridge - Jill Drummond - Colin Ling - Nick Ponsillo
Key points from the discussion:
Stigma is a big issue in many discussions around dementia and others
Improved awareness of dementia now in China and other countries
No word for dementia in many cultures, hence this promotes the stigma as it gets ignored
Question: is there a carry-over effect from situations in countries of origin?
Expectations of culture around care giving?
Expectations are not the same in different cultures
Can cultural awareness sessions improve care giving?
People whose memories are fading take themselves out of social settings/situations to save family members the embarrassment
What is the best way to ensure early diagnosis? –Information programmes? – Translations?- Educa-tion/awareness?
Providers need to work more closely with 3rd sector BME organisations
Insufficient BME representation among health care professionals
Some communities perceive caring roles as low level jobs
Next steps:
Stigma should be out
People will feel more confident to come forward and express their concerns around dementia
‘’Worthwhile event – time used effectively
with positive results – thanks!’’
‘’Enjoyed the day very much and
excellent facilitation. Its heart was in the
right place and the facilitator was very
good, excellent. Thank you for the
opportunity’’

16
Group 8 - Early Diagnosis of the dementias – molecular markers / brain imaging
Convenor - David Allsop
Participants
Richard Jagger - Claire Surr - Dee - Stephanie Tierney - Gillian Drummond
Key points from the discussion:
Moving towards early diagnosis based on molecular markers, brain imaging etc (MCI – Convert-ers)
EEG might be useful (Richard Jagger) Mobile EEG unit, cheaper than brain imaging.
Who would you test? At risk groups? Could you repeat a test?
Would you want to know?
Would you really want to know if you were going to develop dementia in 10 years time?
What would you do? Life style changes, repositioning of drugs, diet and exercise.
Different type of drug trial – test on MCI people
Next steps:
Form ‘bio marker interest group’
EEG Studies on dementia?
17
Group 9 - Sharing data and information – How can we improve overall data sharing and lev-els of inflation?
Convenor - Andy Pownell
Participants
Lynne Goodacre - Nicola Fletcher - Chris Stewarts - Carmel Dickinson
Key points from the discussion:
Better system of referral for different groups of people
Using technology – how we handle data sharing patient’s needs – how we access data
Inflation on carers of dementia
Simple problem, simple solution
Developing the technologies awareness campaign, GP NHS emergency services
So many different data storage systems
A consistent informed approach to sharing data
Easy participant access
Do not want to hide behind ‘data protection’
Create a data hub all agencies can access
Understand each agencies constraint
Sharing data is the way forward
Individuals make a difference not agencies and that
very often an individual will share data/ inform to achieve a common goal
Need to share data to ‘save lives’
Easy to see why different agencies have data
No one has died because we shared data but people have died because we have not
Next steps:
The development of a project amongst different agencies to look at how we can share data and ac-cess different groups of individuals as well as safeguarding staff
‘’Good day, well run, lots of
opportunities to contribute.
Hope it leads to great studies’’
‘’A fantastic day; well put together and
thought through. Excellent mix of people
with a range of knowledge and expertise.
I have learnt an awful lot and feel more
informed and provoked into action than
when I walked through the door, very
important to have both Anne and
Daphne here to ground our discussions in
reality and give a more informed
perspective.’’
18
Group 10 - How do we create a more patient society, frustration with repetition?
Convenor - Helen Morris
Participants
Ruth Eley - Dee Abimbola - Daniella Montaldi
Key points from the discussion:
Research Supermarkets
Speak of life and coercion towards self-service. Development of slow lanes in super markets is not just about disability – Social till.
Speed and access society from the internet. The young exercise memories in different ways – pass-words etc.
IT intergenerational work- bridge across generations that build skill of patience and understanding of dementia challenges (memory from one week to the next)
Could the inverse be true? Because children do not need and use memory much (access to the in-ternet etc.) that they may not be so hung up on it.
Research across generations, finding trigger points for frustration and analysis – causation / cooper-ation v responsibility.
Then research strategies to negotiate the stress.
Research suggests longitudinal
Primary – Families/ care workers/ social worker/ nurses/ care home workers (intense experience)
Secondary – Police/ fire/ superstores/ banks/ transport etc (sporadic experience)
Research into volunteering as a pathway to improved patience and capacity to work with people and cascade attitude to families etc.
Research through life story network – people who have been through the process and produced life story books
People from cultures where pace of life is slower and then dropped into society that allows no time.
Research into psychology:
Brains tend to look novelty – survival and evolution, so frustrated that we cannot move on but we all have a favourite work programmes, poetry , children’s games – we like predictability to be in control
Why can’t we translate these into patience??
Next steps:
Research with young people, cross generalisation / different cultures
Why some repetition is therapeutic and some frustrating.
Research into volunteering / life story as a way of developing patience
Research into alternative sound spaces to allow for time, slow lanes in supermarkets?
Research into ways of learning and how then affect our attitudes towards memory loss

19
Group 11 -How to inspire and inform young people about dementia and encourage them to think about working with people with dementia as a career option.
Convenor - Ruth Eley
Participants
Michelle Collins
Key Points from the discussion
Health champions, gone into Belvedere School. 10 pupils, now to whole sixth form group. 6 week course in Broad Green Comp PSS
Do we need to start with top juniors? Use health champions, could organise around dementia.
Using IT as a vehicle for engagement skills and expertise for younger people.
Recruiting people with right values is challenging, especially when they are pushed into applying by job centres/ benefit challenges.
Explore what children know about dementia in different year groups, different localities
PM challenge – educational resource for schools about dementia
Need for better information for children and young people about dementia, not much around?
Next steps
LSN and PSS to explore possibilities for joint work/ funding opportunities
Identify if anyone else is interested in this as a research topic?
Group 12 - How can technology (e.g. mobile technology, electronic data) support people with dementia and their carers.
Convenor - Carmel Dickinson
Participants
Gav Cross - Alicia Ridout - Tony Gatrell - Gillian Drummond - Rumona Dickson- Grahame Smith - Stepha-nie Tierney - Bill Ollier - Melanie Chapman
Key Points from discussion:
For patient/ for carers – memory enabling technology for second person to use
Is it ethical to monitor people or to use the aggregated data?
Where is the technology? How can people know about it
Anonymised GP data is beginning to be available
Need for agile prototyping and iterative trials
Can’t be technology led, what do dementia patients feel they need? Also families and health carer
needs
Who pays for technology? ‘Mood Lighting’

20
Inventions can’t be technology led, must be based on need of patients/ families / carers
Technology as ‘scaffolding’ to support activities and social networks – avoiding social isolation for patients and carers. Choice and control is important in determining acceptability.
The ethics of monitoring technologies and maintaining data ownership.
Some issues include: How do health and social care professionals know what technology is available?
Where is the evidence?
What is the business model?
Need for agile prototyping and iterative trials
Can technology used at home be transferred to care home? ‘’Ghettoes of technology’’
Where is the evidence? What is the business model?
Technology to maintain and sustain friendships and social networks – Scaffolding/ choice/ control.
Priorities for remembering – object recognition and enabling to maintain social links
Successful interventions with patient and carer networks – keeping data ownership
‘My Liverpool’
Addressing social isolation for patients / carers. Prompts on TV, input from family. Addressing the individual’s fears.
Will there be ‘ghettoes of technology’ e.g. care homes may not allow people to use technologies they are accustomed to
Group 13 - How can research result in reducing the fear that people living with dementia experience every day (Ann Johnsons word terror)
Convenor - Sue Clarke and Ann Johnson
Participants
Tracy Collins - Pauline Parker - David Powell - Rebecca Jones
Key points from discussion
Finding a cure
Education
Having someone in your life makes all the difference?

21
Psychological interventions help to develop coping strategies
Social intervention – people with dementia and carers/ families should have someone who they can talk to.
Looking at individual’s and their history / background, this will determine their experience of de-mentia
Can be re active depression to their situation psychological therapies not always effective as people with dementia might forget what was said or what coping strategies had been developed. Take notes or recording the session can help with this.
Interactive technologies could help. Ways to reassure people/ reduce isolation. May help to slow progression of dementia
Intergeneration understanding / support of families. Dementia friend’s information sessions. Fear can be reduced through meaningful social engage-
ment/ occupation
Public figures / messages need to be about living more positively with dementia. Next Steps
Encouraging people to become dementia friends
Make psychological interventions available to people with dementia earlier on
Raise awareness and educate carers to be able to support / intergenerational understanding
Have a range of coping mechanisms to choose from
Develop services for younger people / appropriate environments
Awareness raising in churches / faith groups on dementia friendly communities.
Group 14 - Dementia and criminal justice
Convenor -Katrina Forsyth
Participants
Dave Jones - Pauline Banks - Lynne Goodacre
Key points from discussion
No screening in prison, not joined up for dementia.
Prison culture v health care culture (human rights) managing security v providing health care.
No mental health services in prison – old age psychiatry.
No policy for identifying and managing dementia in prison
No joined up / referral services – difficult to make referrals to specialised services in the community
22
Older person assessments need to be evidence based.
Relying on staff to identify isn’t ideal for training.
Duty of care.
Equivalence of care – dementia care in prison should be equivalent to the community.
Ethical issues with dementia
Grouping older prisoners together - pro’s access specialised services v con’s being away from family.
Growing problem, older prisoners are the fastest growing group
Challenges of frailty coupled with dementia
Dementia is criminal justice system is an under researched area.
Next Steps
Understanding prevalence / scope of the problem
UK wide
Developing care pathways for dementia /networks
Access to specialised old age psychiatry
23
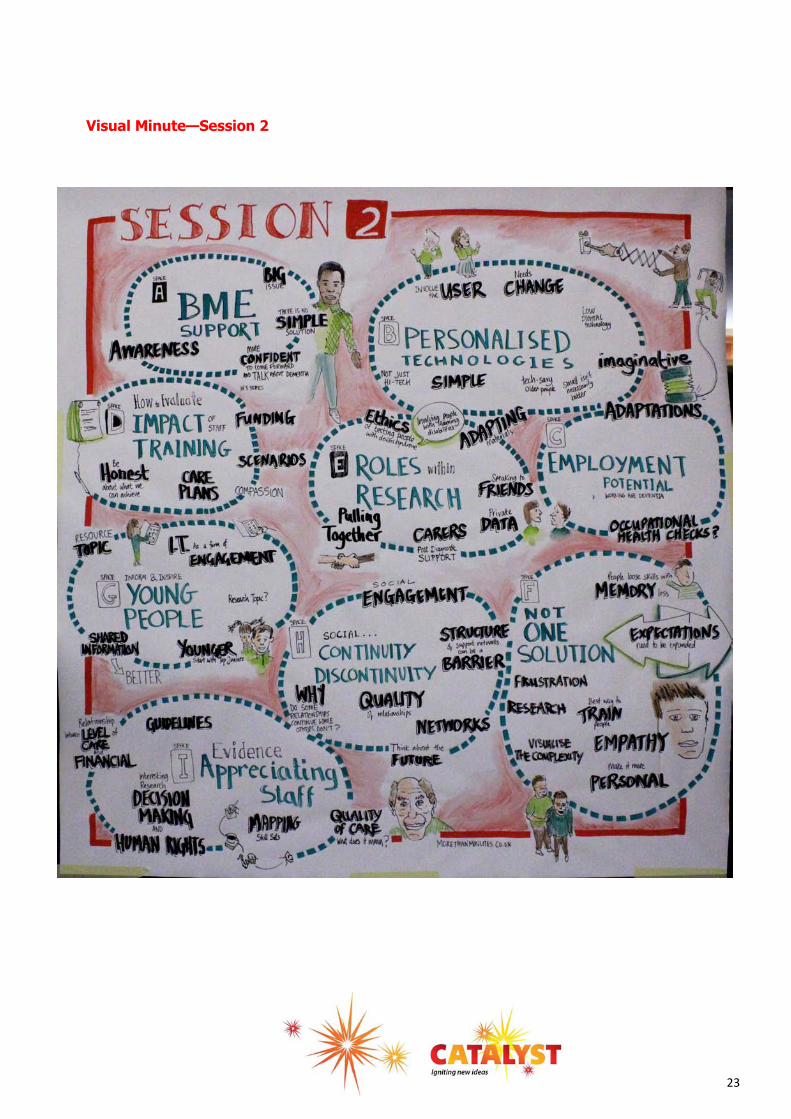
Visual Minute—Session 2
24
Group 15 - Keeping dignity as dementia progress’s
Convenor-Joanne Singleton
Participants -
Nicola Fletcher - Dee - Sarah Butchard - Di Burbidge - Liz Postlethwaite
Key points from discussion
Keeping dignity should not need to be discussed/ planned but automatic
Managing both,
Individually focused on each person to the standard of ‘their norm’
Information gathering for person/ family
Acknowledging faith of person / specific needs to promote dignity e.g. wash/ showers
Person centre care
Personalisation not working – still task centered
Detailed information of person needed
Finances of local authorities
Choice of what funding is spent on
Choices not right
Hospitalisation – losing mobility and control
Next steps
How do we understand and identify in the absence of memory - needs to be looked at.
How do ‘we’ and those with dementia identify themselves?
Need to create associations that is it something that affects us all.
‘Frameworks’ need to be developed to support dignified decisions.
Person centred – changes needed from ground up to respect
How can empathy be captured and understood
Look at empowering care workers
Who supports dignity
Support network being respected for their decisions
Long term decision not being respected
Research and identify with dignity
Ability to remain engaged in society

25
Family not always respected
Dignity is different for each person
Group 16 - Support for family members – Problems and what is needed
Convenor Daniela Montaldi
Participants
Michelle Collins - Mike Taylor - Ruth Eley - Hilda Hayo - Andy Pownell- Lisa Woods
Key points from discussion
Infrastructure limitations
Good Memory clinic should include family but lack of standardisation means information is often out of date.
‘I’m at my wits end, I don’t know what to do or who to approach’
Lack of knowledge in some areas of care provision and consistency
Don’t follow pathway through life as with other long term illness’s. No clinical / social support
Detailed discussion of current practice in Liverpool Next Steps
Regional hubs – with national standards Sharing best practice
Education
Delivery of information
Make information accessible Clarity
Consistency (consistency of content but individually selective)
Availability
One port of call for family members
No automated answer systems
Resources needed so NHS, local authorities and research bodies need to come together
Group 17 - What is the evidence for the effectiveness of interventions in dementia – where are the gaps in the evidence base?
Convenor - Sally Spencer
Participants
Claire Surr - Allan Grogan - Noreen O Sulivan - Richard Jagger - Liz Postelthwaite - Nicola Jervis - David Allsop - Caroline Hampson - Carol Taylor
26
Key points from discussion
Evidence should take into account the population and diversity
Polypharmacy and adherence – why people do and don’t adhere with medications?
Trials should include adherence outcomes
Adherence may be influenced by peer support
No trials of memantine in learning disabilities and dementia – need to include co – morbidity in eval-uation.
Head to head trials to establish comparative efficiency, explanatory work prescribing practices.
Look at complex interventions – core outcome set for inclusion in studies – evidence base to identify
Overview on dementia research
Need for social isolation evidence base
Methodologically – Evidence base should take into account: population and diversity
Identify core outcome set to inform future studies. Next Steps
Need evidence on:
Complex interventions and identifying those components through the evidence base
Evidence for remediating poor adherence to interventions
What is evidence for effectiveness of medicines in relation to polypharmacy
Need evidence on comparison between interventions
Use current evidence base to develop a ‘one stop’ document on research i.e. an overview of demen-tia research
Group 18 - Individualisation of solutions for people with dementia and support
Convenor - Daphne Wallace
Participants
Mike Taylor - Helen Morris
Key points from discussion:
Memory issues are different for different conditions, lost skills that work with memory, visually can be difficult.
Loss of skill – when once gifted can lead to frustration. Not just about ‘memory’ registering new in-formation but loss of memory based skills – knocking things over/ into things.
Expectations need to be expanded to understand loss. The person is different and the disease pro-cess will be different.
27
Research into developing support with continuity so that the person can be better understood by another person instead of a multiplicity of small tasks completed.
Over lapping with the work of life, story work and understanding the background and life of the per-son concerned – understanding the importance of ritual.
Some of the paradoxes of information sessions for dementia awareness, general findings, results of dementia but that each person is different.
Parallels with people’s response to pain and research into this aspect. Next Steps
Research into the best way to train people about the complexities over and above general observa-tions
Visualise the complexities first, then look at common themes/ occurrences, will this develop more empathy – make it more personal from the start?
Group 19 - Potential for continued employment for people with dementia
Convenor - Pauline Banks
Participants
Nicola Fletcher - Katrina Forsyth - Gillian Southgate - Stephanie Tierney
Key Points from the discussion
Use of adaptations – need to be geared to specific roles
Need to demonstrate tasks to businesses that is going to benefit them
Challenge stigma – hindrance to seeking diagnosis
Depends on job and level of responsibility
Importance of driving
Loss of identity
Will companies want to commit to supporting people – resource implications
Costs with increasing number of people
People as an individual, might need to look at each case Next Steps
Find people who are still in work – how many people are there
Include dementia in occupational health checks
Try to look at good practice
Awareness raising amongst employers/ HR that problems could be associated with dementia.
28
Group 20 - Do we have an evidence base for understanding whether staff delivering care to residential elderly have sufficient training knowledge of dementia
Convenor - Bill Ollier
Participants
Rhys Davies - Sarah Butchard - Liz Postlethwaite
Key points from discussion
Staff decision making in nursing care NIHR human rights approach to care – working with DenDron and University of Liverpool.
In difficult decision making in all types of staff – assessment of an intervention (training package)
Are the instincts of people working in mental infrastructure different to those in nursing care – well-being of residents
Health economy of this
Use QUALD for outcome and dementia care and relatives intervention
Has anyone done research to map / audit the skill sets / competencies for staff in different care homes/ settings – do we know level of qualifications? Knowledge of dementia/ awareness etc?
Are there agreed minimum guidelines for what experience / knowledge/ qualifications for staff work-ing in different care / dementia settings – if not why not?
Interesting to investigate the relationship between level of care / training and financial basis for providing care
Do we know what we mean by ‘quality’ for dementia care. Issue of delivering care for the same sex care for the elderly/ dementia.
Next steps
Focus groups?
Forumulate research questions
Develop national guidelines
Define expected levels of care
What is the best model for people being looked after, should people with dementia be with demen-tia cases or in a home without dementia sufferers?
Group 21- Family and friends, changes in relationships, roles, continuity and discontinuity of wider social relationships.
Convenor - Tracey Collins
Participants
Andrew Garrity- Pam Duffy - Allan Grogan - Hilda Hayo
Key points from discussion:
Person with dementia and carer perspectives, family, friends fall away
Why do some social connections continue and others not?
29
Quality of relationships
Normalisation – life engagement important
Flexibility of services to allow continuity
Lose of control – structure of day
Create new experiences
Establish new networks
Individualised support
Balance risk management with choice and integrative engagement
Do ‘with’ not ‘for’
Next steps
Why do some relationships continue and some not quality of relationships
Does a flexible approach from support services etc allow a greater engagement with life/ social net-works / continuity
Explore the creation of new networks and experiences – living well with dementia – normalisation and life engagement – important future and here and now importance.
Group 22 - The barriers between general community services and mental health services e.g. training of front line carers
Convenor - Rhys Davies
Participants
Chris Ling - Di Burbidge - Allan Grogan - Nick Ponsillo - Daphne Wallace - David Rog Bill Ollier
Key Points from discussion
‘Blocking’ of time for staff to undertake tasks as a problem
What they want – different individuals
How to cope with low staff levels
Aptitude test for staff? Induction process Funding Contracts Interpersonal Skills Same people
Training – Home carers/ general managers
Research: Surveys / Intervention
GP Interface – poor
Diet nutritional – sales of nutrition in RH
Delivery of medication
30
Currently barriers to ‘specialist’ medical or ‘mental health’ skills being brought to bear in general so-cial services
Home care settings/ patients own homes
Voluntary organisations
General practice
Care homes
Acute general hospitals
Timing, care, personal care, meals, activities (music etc)
Deal with confrontational behaviour
Individual v groups e.g in care home/ client list of care agency
Currently barriers to ‘specialist’ medical or ‘mental health’ skills being brought to bear in general social services
Home care settings/ patients’ own homes
Voluntary organisations
General practice
Care homes
Acute general hospitals
Timing, care, personal care, meals, activities (music etc)
Deal with confrontational behaviour
Individual v groups e.g in care home/ client list of care agency
Challenges –
Contracts/ targets
Induction days / aptitude tests
Staff – keen on training in general, funding levels/ funding of staff
Time saving from good practice
Skill set in nursery nursing
Use of microchip technology to monitor drug taking.
Research questions at all levels
31
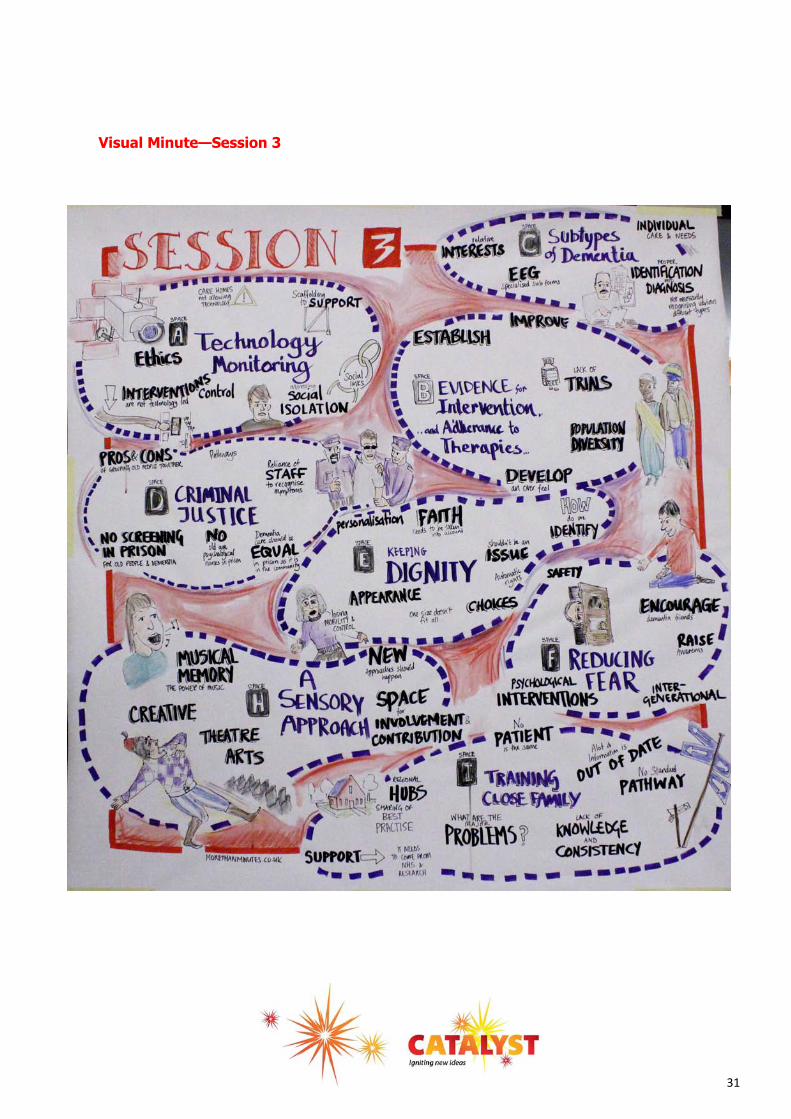
Visual Minute—Session 3

32
Potential Research questions: What is the current provision of dementia training in social
services?
What individual training provided?
What interventions help?
Mindfulness?
Time management
Altered targets for care quality
Optional budgets
Microchip to monitor drug intake
What is cost saving of interventions to improve dementia skills in general service setting?
Current models – can quality / cost aspects and in different regions to compared?
Group 23 - Dementia – Dementias, disease sub types within ‘dementia’ individual care for de-mentia subtypes
Convenor - Rhys Davies
Participants - Richard Jagger
Key points from discussion
How knowledge of disease types may be important for care
Importance of biology of dementia
Young onset dementia
Training of practitioners in mental health teams
MA treatment services
Diagnosis framework
Movement disorders – cannot tap into same services
How many patients are diagnosed with one of the dementias
Crucial for research selection.
The right diagnosis for biological reactions and clinical trials and correct supportive treatment.
Crucial for research selection.
Research questions:

33
What proportion of patients with a dementia diagnosis have a specific disease diagnosis?
Are diagnosis more delayed in unusual sub types of dementia
Does dementia training as it exists encompass information about different forms of dementia?
Issues of ensuring correct diagnosis in patients entering clinical trials
EEG as a biomarker for cognitive disorders
How can specialised forms of EEG (e.g event related potentials) be made to un harm biological diag-nosis / subtyping?
Other biomarkers in differentiating sub types of dementia.
Group 24 - Sensory life day, work and development/ measurement
Convenor - John Keady
Participants
Nick Ponsillo - Daphne Wallace - Helen Morris - Christine Milligan - Chris Edwards
Key points from discussion
Sense are very important, laughter as an example of engagement
The emotional power of memories after sensory experiences such as touch, smell, hearing, texture etc.
Arts bases measurements – singing and music
Video and photo elicitation as evoking memories.
The ‘musical’ memory tied into the life circle.
Sensory work is complex but importance of being ‘in the moment’; this should be the key to understanding evaluation. This could be a new active process based on multi-sensory experience built around individ-ual / relational work.
Currently, we don’t know how to do this – new methodologies needed
If you experience, you can understand, if you read and repeat you cannot.
Eye contact, recognition, body movement, gestures are all important dimensions to the engagement of the human person living with de-mentia
People with dementia need space for involvement and contribution.
Next Steps
‘’Excellent organisation
and format which kept it
interesting and offered
something for everyone to
engage in ‘’
‘’Talking to the Cochrane
Dementia Group Editorial
board in terms of setting
future topic priorities as a
consequence of output
from the event. ‘’
34
Bottom up approach – visual methods/ participation
Innovative methodologies
Sensory experiences
Sensory forms of evacuation
Need to find out what is going on before we start: form a ‘working group?’
The sensory tool should include elements of being:
1) Audio/activity based;
2) creative tapping into the senses and the person’s ‘musical memory’;
3) Innovative and use ‘in the moment’ visual methods to document engagement.
Potential PHD project
Group 25 - Remote, mobile, personalised technologies
Convenor - Tony Gatrell
Participant’s
Daniella Montaldi - Carmel Dickinson - Pauline Parker - Joanne Singleton - Sally Spencer -Alicia Ridout - Carol Taylor - Lisa Woods - Caroline Hampson - Christine Milligan
Key points from discussion
Intriquitous mobile phone need to involve user as technology could be counterproductive – possibly frightening. Needs can change very quickly. Technology doesn’t need to be ‘high tech’ expensive and plenty of experts are out there.
New opportunities in wearable technologies (GPS enable wristbands) with high degree of intelli-gence
Current issue of older people being not tech savvy but this will change so there are short term and long term issues.
What are user preferences- for appropriate surveillance / getting lost?
What is intrusive
Personalisation matters – not everyone has identical needs
Be imaginative e.g. embed new technologies in old devices and small isn’t necessarily beautiful (eye, motor problems, co – morbidities)

35
Group 26 - Adapting mindfulness based practice for people with dementia and measuring clinical efficacy in terms of quality of life - Emotional - Regulation - Cognitive variables
(e.g.memory) - Physiological variables (e.g. effect on brain structures e.g. hioppocampus)
Convenor - David Powell
Participants
Noreen O Sulivan - Grahame Smith - Gillian Southgate - Alicia Ridout - Liz Postlethwaite
Key points from discussion
Work done so far is fragmented, usefulness of review of published and un published work – possible publication
Unpublished with survey of services and mindfulness networks
Broad approach to thinking through how adaptations may be made – e.g. understanding practices from Buddhism not so far used in ‘secular mindfulness’
Tension around the intensiveness of research in this area, reductionism impoverishes capacity to really understand the impact for people.
Problem of a consensual definition of mindfulness (some distinct) for research purposes
Understanding ‘good practice’ re creative approaches that emphasis focussed purposeful activity ‘in the moment’ (something can be done in care homes)
? relevant outcome measures
?Qualitative and quantitative (mixed methods) ‘ hard’ measures neuroimaging
What range of outcome measures would an appropriate in-tervention be measured against?
The challenge of helping people to maintain mindfulness practice? So what are the obstacles? What helps?
How can mindfulness practice be more easily integrated into day to day life.
Relatively understanding how something like mindfulness practice can be integrated into activities in care homes etc and what effect this has
Likely large variations in response to any mindfulness intervention
?focus on intervention on earlier stages Next Steps
Further re thinking involves others. Beginning to bring together the mindfulness and dementia com-munities.
Locally small scale defined projects – some offered to students looking for research ideas in HEI’s (e.g. clinical psychology trainees)
Do we have experts for systematic review including survey data
‘’More of this type of event please,
structure, delivery, style, content,
engagement, inside out agenda
setting, short & sharp sessions,
choice of where I invested my time -
excellent event.’’

36
Summary
This summary is for the purposes outlined at the outset; that is to make notes of the dialogue and to cir-culate this to the participants as a reminder of discussions and to locate individuals who were involved or who have since expressed an interest to be kept informed.
There are several themes common across different groups. These include: Support for family and cares, training for care staff, treatment interventions and evaluation of theses interventions, stigma and main-taining dignity.
It is also suggested, to further increase the success of the event that those who want to lead research could provide a short summary to be sent to attendees of the event in case any of the research ideas were missed on the day. Next steps
The Event Report will be circulated to participants and other interested parties. It will also be available to the general public on our website. Contact details will be circulated to Discussion Convenors on request to facilitate the further development of the proposals outlined. NHS R & D North West may contact Discus-sion Convenors to ascertain what additional support is required to maintain momentum and track pro-gress of bid development / successful application for research funding. NHS R&D North West would appreciate on going feedback with regards to the progress of any of the is-sues raised on the day from any of the people who attended the event even if they were not a convenor. Thank you to everyone who attended on the day and contributed to all the discussions detailed in this re-port and a big thank you too all convenors for raising their question. ‘’The greatest value was in the fact that people had the opportunity to discuss issues that were important to them as
well as listening to someone with a lived experience of dementia. ‘’
‘’Very productive event and great artwork! ‘’
‘’More of this type of event please, structure, delivery, style, content, engagement, inside out agenda setting, short
& sharp sessions, choice of where I invested my time - excellent event.’’
‘’Excellent organisation and format which kept it interesting and offered something for everyone to engage in ‘’
‘’Talking to the Cochrane Dementia Group Editorial board in terms of setting future topic priorities as a consequence
of output from the event. ‘’
37
Visual Minute—’As a result of today…’
38
Feedback from Survey Monkey
Did you find the day useful, if so what?
Very interesting to hear from Alistair and Anne, and to work with such a range of people
The structure of the day was democratic and encourages participation - much better than being
spoken to all day.
Excellent day well planned and facilitated
Yes by virtue of being able to both listen and talk
The greatest value was in the fact that people had the opportunity to discuss issues that were im-
portant to them as well as listening to someone with a lived experience of dementia.
Great to connect, reconnect and think. We don't get to do enough of those!
Yes, good opportunity to compare ideas and discuss possibilities for further research.
Networking & discussing thorny issues
The day was very valuable. In particular it was great to meet with a wide variety of people who are
all interested in the same topics.
Really valuable use of time from a networking perspective and the sharing of knowledge from very
different people
Very useful in making new contacts and knowledge sharing
In terms of taking things forward, what plans have you got?
Consider developing a sensory instrument for measuring effectiveness in dementia care
developed partnership agreements with agencies directly engaged with dementia clients
reconnecting with people I met to further aims of my project
Raising concern about medication overload
Wishing to run similar sessions with the community groups I work with at the moment
Meeting 3 people I met on the day
I am already involved in some research
Talking to the Cochrane Dementia Group Editorial board in terms of setting future topic priorities as
a consequence of output from the event.
I plan to work with a wider range of NHS organisations
one meeting re carer research
Ideas for further research with collaborators but this needs facilitation from the organising group
offer advice to people about submitting applications
Continue to search for funding for raising awareness within the Chinese community and developing
culturally appropriate dementia support services
39
Did you make any connections on the day and how will this assist you in your future work?
Yes, I will email people re possible collaborations
Yes, and was able to catch up with some existing contacts too.
Yes many - research input for evaluation of the project, materials for Dementia Friends Sessions
from ambassadors
I made connections with the Alzheimer’s Society from Manchester and I hope to keep communi-
cating with them
I met someone who wishes me to work with him on some work he is planning.
Yes, with Carmel Dickinson and Rumona Dickson in particular. This will contribute to development
of the evidence base for dementia therapies and interventions
I made contacts with a number of local NHS organisations and at the University of Lancaster that I
am contacting to arrange to work with them
I made some good connections, which may help to inform my practice in the future.
possible future connections
Made connections in both academia but also in other sectors
I have informed people about the role of the Research Design Service
yes the mix and diversity of people attending really worked
yes guest speaker has offered to deliver a talk to our Luncheon Club members
Any other comments
If anything the title was misleading - it wasn’t so much about identifying gaps, but in sharing
knowledge and building connections
Really powerful event format - so many ideas in such a short time. Hope some real research pro-
jects move forward as a result
Meeting format was excellent, however perhaps less groups but one more session during day?
Thank you for a well thought out and excellently run event
Excellent event. Well facilitated - delighted to have been there.
A very well organised day.
Very productive event and great artwork!
more service improvements than innovative research but good all the same
Excellent idea to have Anne Johnson talking about living with dementia
It would be nice to have more clinicians and commissioners present at these meetings. Some of
the comments/discussions were a little removed from what actually happens in the real world. If
we are to truly move forward, I feel that engaging with the people who deliver what the research
finds and who commission services might mean that some of the work carried out in the academic
world translates better to clinical practice.

40
FEEDBACK
Please tick the face which best represents the following:
Venue
Food
Speaker
Debates
Any other comments Worth the 8 hours travel!
Great day—Thank you
Would like to have seen more medical
people make a contribution
Really good event—thanks
41
Postcard Feedback
Worthwhile event – time used effectively with
positive results – thanks.
Today has been a really enjoyable experience
which provided opportunities to discuss im-
portant issues within the field of dementia
care. There were some great ideas discussed
and concerns raised and while it is fantastic
to have these conversations and move for-
ward with the research, I feel that the com-
missioners of services should be included as
they need to provide the funding!
Enjoyed the day very much and excellent fa-
cilitation. Its heart was in the right place and
the facilitator was very good, excellent. Thank
you for the opportunity
An Informative and useful day, good venue,
well organised
An excellent way to hold and event. Interest-
ing, stimulating and inspiring.
Great event, well facilitated, good networking,
great lunch, good ideas to take forwards, cold
until lunch time in the room (not the best
acoustics either!!)
A fantastic day; well put together and thought
through. Excellent mix of people with a range
of knowledge and expertise. I have learnt an
awful lot and feel more informed and pro-
voked into action than when I walked through
the door, very important to have both Anne
and Daphne here to ground our discussions in
reality and give a more informed perspective.
Thanks for a really beneficial day. Well-
structured and organised. Produced copious
information. Can’t wait to see the report
Really worthwhile event Imaginatively organ-
ised with a good mix of interesting, engaged
people. Excellent accessible venue( once
room warmed up) good refreshments. The
acid test will be whatever new grant applica-
tions emerge
Very accessible, good opportunities. Art work
an aid to memory, good sharing of
knowledge, feedback on groups, too much
choice – good, range of topics, could not
have asked for more, venue chilly, people
need teaching how to use a microphone,
good size room.
Inspiring and energised day, thank you
Good day, well run, lots of opportunities to
contribute. Hope it leads to great studies
Great day, delighted it has included the crea-
tive and the imaginative. An exciting scope of
possibility for people with dementia and their
communities. Thank you
Overall a very good day, would like to hear
the outcomes of groups I could not get to.
Worst thing was the extreme temperatures.
Please add in:- research into identifying ad-
vance permission for research involvement to
reduce barriers to inclusion for the important
group of people with advanced dementia, in-
corporating ethics, very useful session and a
lot of new thoughts and connections.