catalyzing ihi open school students as agents of · pdf file ·...
TRANSCRIPT

Catalyzing IHI Open School Students as Agents of Change: Innovations to Educate and Activate the New
Generation of Leaders in Health Care
January 2016
RX FOUNDATION
GRANT SUMMARY &
LEARNING REPORT

Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 2
Table of Contents
Executive Summary: A Program, a Platform, and a Movement for Change 3 Part I: Goals and Outcomes of the Rx Foundation Grant 4
Part II: I-CAN Online Course for Leadership Development 7
Key Programmatic Lessons from Online Leadership Course 9
Evaluation Methods 10
Primary Outcomes 11
Secondary Outcomes 12
Additional Observations 16
Part III: I-CAN Mobilization Events for Movement Building 17
Activity Pages 17
Student Organizing and Leadership Academy 17
International Pledge-a-Thon 19
Key Learning from Mobilization Events 21
Part IV: Development and Improvement of an Internet-Based Platform for Sustainable 22
Collaboration and Change
I-CAN Web-Based Virtual Improvements 22
I-CAN Collaborations to Amplify Impact 22
Part V: Conclusions and Next Steps 24
Opportunities and Plans for Sustainability 25
Appendix 26
Selected Examples: Learners’ Experiences 27
Submitted by: Institute for Healthcare Improvement 20 University Road, 7th Floor Cambridge, MA 02138
Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 3
Executive Summary: A Program, a Platform, and a Movement for Change
In 2014, the Rx Foundation provided a two-year grant to enable the Institute for Healthcare
Improvement (IHI) Open School to organize and mobilize health professional students to make
population health improvements in their local settings (i.e. to activate “agents of change”). The IHI
Open School achieved this goal by developing the “IHI Open School Change Agent Network,” or I-
CAN.
I-CAN became, and continues to be, a student-driven movement to improve population health through
project-based leadership training, mobilization events, and an online platform. By December 2015, I-
CAN included more than 2,192 student leaders from more than 65 Chapters (local groups) in 35
countries that engaged more than 35,000 people in actions to advance population health. In the process,
I-CAN also drove IHI Open School innovations.
This learning report provides a summary of activities the IHI Open School and its students completed as
they created I-CAN. The report includes five parts: (1) an overview of project goals and outcomes; (2) a
review of the online leadership course; (3) a description of mobilization events intended to amplify I-
CAN’s reach, outside of the course; (4) the use of the virtual platform for collaboration and change and
(5) recommendations for next steps in integrating I-CAN as a sustainable component of IHI.
Building on the interim report submitted in Year 1, this final learning report focuses on I-CAN activities
in Year 2: (1) improvements to the online leadership course; (2) outcomes of mobilization events; (3)
and sustainable integration of the online platform within the IHI Open School’s core strategy, Chapter
network, and partnerships.
The measurement and evaluation team assessed student engagement, experiences, learning, and the
degree to which learning is translated into action. The methods are integrated in this report respective to
their associated activities.

Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 4
Part I: Goals and Outcomes of the Rx Foundation Grant
Despite a widespread emphasis on upstream determinants of health, the next generation of health
professionals encounter outdated curricula and support in their schools of study1. IHI Open School
students expressed a desire to learn how to address problems originating outside the walls of clinics and
hospitals, and said that they lacked the tools to do so.
In service of this need, IHI Open School students and external subject matter experts narrowed I-CAN’s
focus to population health. Because research has shown that clinical care generates only 20 percent of
the determinants of health, health care providers are increasingly asked to do more than care for the
patient in front of them. (See Figure 1 for additional detail.) In order to improve health outcomes and
reduce costs, providers are increasingly looking upstream to address the social determinants of health.
Figure 1: Population Health Driver Diagram
Source: County Health Rankings and Roadmaps website. “County Health Rankings Model,”
http://www.countyhealthrankings.org/resources/county-health-rankings-model
The I-CAN initiative had several mutually reinforcing, overarching goals. One was to help students take
widespread actions that led to better health. A second was to produce a generation of leaders skilled in
mobilization that could catalyze change and train others to follow in its footsteps. A third was to build
and nurture a vibrant community and a sustainable social infrastructure that IHI and IHI Open School
Chapters could use to create large-scale change.
1 Lueddeke, George R., and Manuel M. Dayrit. 2012. Transforming medical education for the 21st century: megatrends, priorities and change. London: Radcliffe.

Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 5
The IHI team built the initiative’s logic model on the hypothesis that IHI Open School students could
serve as catalysts for change at the frontlines of health if equipped with leadership skills, organizing
skills, change tactics a social web platform, and mobilization training (e.g., Figure 2).
Figure 2: Logic Model
At the outset, the IHI Open School set aims of enrolling 300 leaders in I-CAN’s project-based, online
leadership course, who would in turn collectively organize 3,000 students to take action in local
population health efforts. Those 3,000 students would then mobilize a total of 30,000 people in pledges
and actions to advance population health by December 2015 (e.g., Figure 3).
Figure 3: I-CAN Intended Levels of Engagement
Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 6
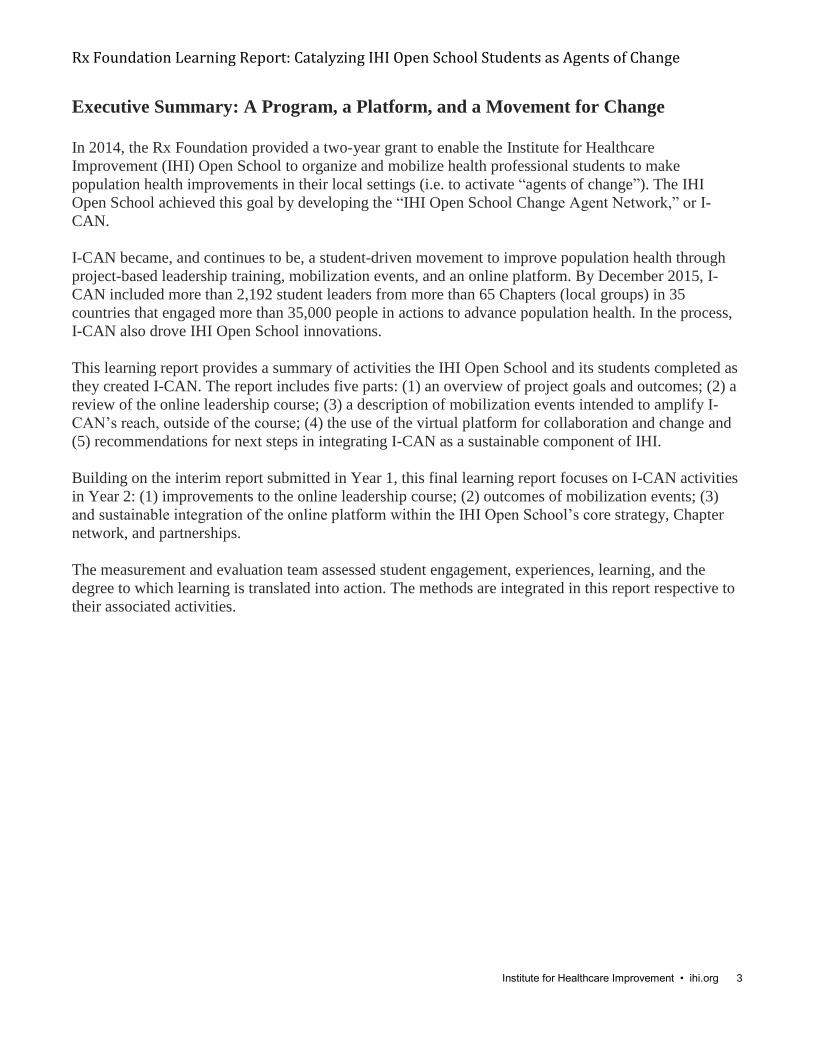
By the grant deadline, I-CAN included more than 2,192 student leaders taking action, representing 65
Chapters from 35 countries, and mobilized 35,505 people to make pledges. Put another way, each
student secured an average of 16 pledges in their local setting (e.g., Figure 4).
Figure 4: I-CAN Actual Levels of Engagement
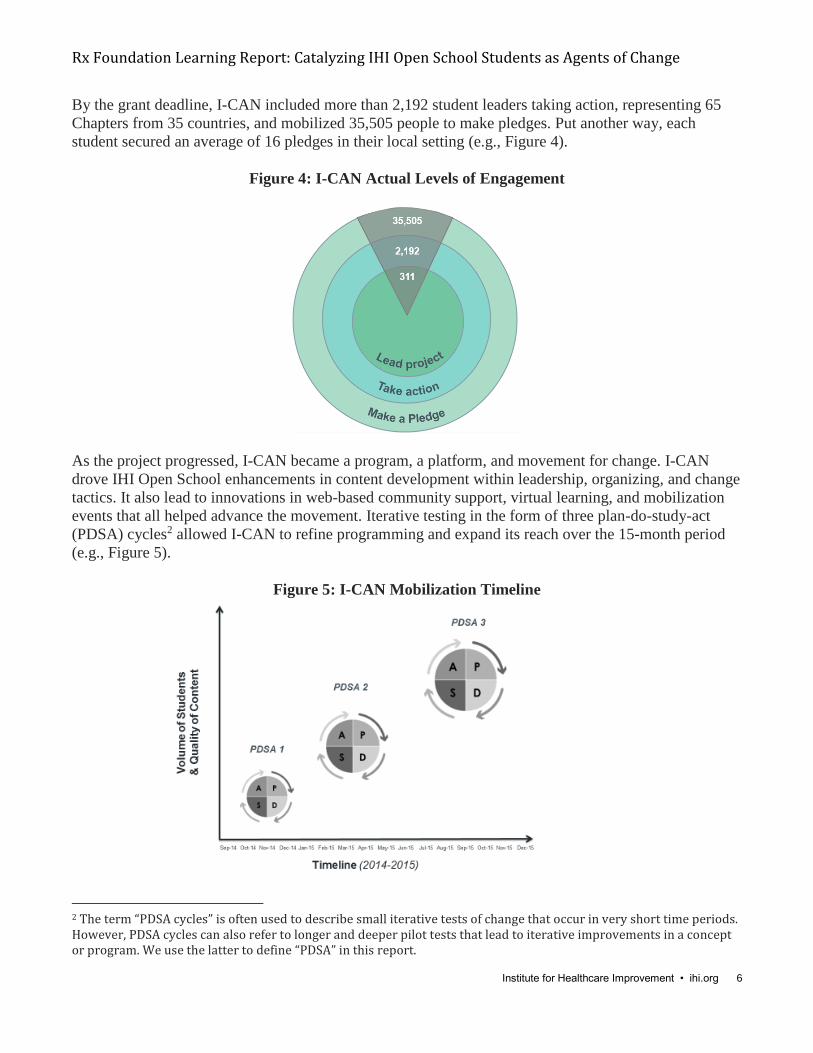
As the project progressed, I-CAN became a program, a platform, and movement for change. I-CAN
drove IHI Open School enhancements in content development within leadership, organizing, and change
tactics. It also lead to innovations in web-based community support, virtual learning, and mobilization
events that all helped advance the movement. Iterative testing in the form of three plan-do-study-act
(PDSA) cycles2 allowed I-CAN to refine programming and expand its reach over the 15-month period
(e.g., Figure 5).
Figure 5: I-CAN Mobilization Timeline
2 The term “PDSA cycles” is often used to describe small iterative tests of change that occur in very short time periods. However, PDSA cycles can also refer to longer and deeper pilot tests that lead to iterative improvements in a concept or program. We use the latter to define “PDSA” in this report.

Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 7
Part II: I-CAN Online Course for Leadership Development
I-CAN included the online leadership course, Leadership and Organizing to Improve Population Health,
which teaches health professional students essential skills for leading and organizing change. The
course, which was offered three times, provided students with the skills to drive mobilization efforts that
translated measurable aims into demonstrable improvements in health and health care in their local
settings. The course was semi-synchronous, meaning we released a new batch of content once a week so
that students would learn the material together
The goals of the course included:
Increase learners’ knowledge and skills in leadership, community organizing, population health,
and improvement science.
Facilitate learner-initiated improvement projects in communities around the world.
Activate a broad learning network of improvers.
Demonstrate how an interprofessional approach can create pathways to improvement.
Improve IHI Open School capability to mobilize future cohorts of learners.
Learners completed eight lessons that consisted of asynchronous video lectures, three 60-minute
synchronous webinars, and dedicated time for field work, during which learners applied the skills to
undertake improvement activities in local contexts. At various points, learners received real-time
coaching through virtual “office hours” and one-to-one calls with IHI faculty and coaches. More
information about the course is available on the website at www.ihi.org/ICAN.
Kate Hilton, JD, MTS, Senior Faculty at ReThink Health, served as the course’s lead faculty and author.
Supporting faculty included: Don Berwick, MD, MPP, FRCP, President Emeritus and Senior Fellow of
IHI; Derek Feeley, DBA, President and CEO of IHI; Mary Dolansky, PhD, RN, Associate Professor in
the School of Nursing at Case Western University; Wendy Madigosky, MD, MSPH, Associate Professor
of Family Medicine at the University of Colorado Denver; and Jessica Perlo, MPH, Senior Community
Manager of the IHI Open School.
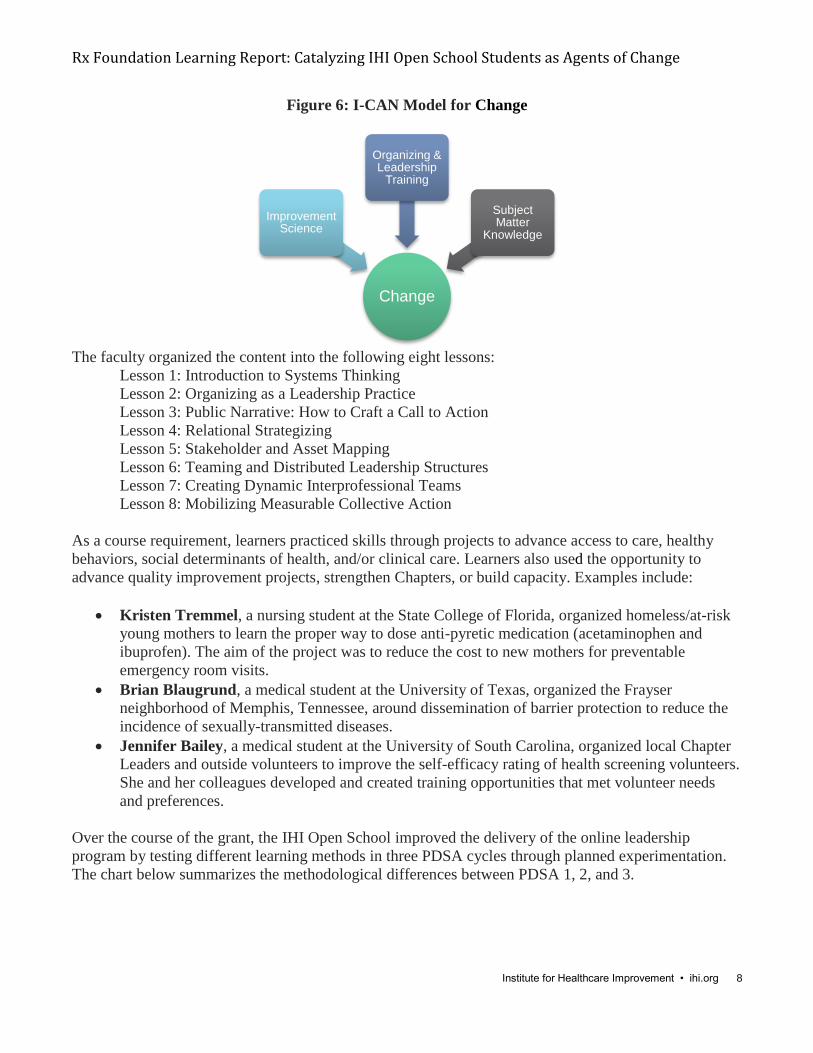
To empower students to become agents of change, the course faculty merged their expertise to create
content in three key areas: proven organizing practices, population health subject matter, and
improvement science (e.g., Figure 6).
Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 8
Figure 6: I-CAN Model for Change
The faculty organized the content into the following eight lessons:
Lesson 1: Introduction to Systems Thinking
Lesson 2: Organizing as a Leadership Practice
Lesson 3: Public Narrative: How to Craft a Call to Action
Lesson 4: Relational Strategizing
Lesson 5: Stakeholder and Asset Mapping
Lesson 6: Teaming and Distributed Leadership Structures
Lesson 7: Creating Dynamic Interprofessional Teams
Lesson 8: Mobilizing Measurable Collective Action
As a course requirement, learners practiced skills through projects to advance access to care, healthy
behaviors, social determinants of health, and/or clinical care. Learners also used the opportunity to
advance quality improvement projects, strengthen Chapters, or build capacity. Examples include:
Kristen Tremmel, a nursing student at the State College of Florida, organized homeless/at-risk
young mothers to learn the proper way to dose anti-pyretic medication (acetaminophen and
ibuprofen). The aim of the project was to reduce the cost to new mothers for preventable
emergency room visits.
Brian Blaugrund, a medical student at the University of Texas, organized the Frayser
neighborhood of Memphis, Tennessee, around dissemination of barrier protection to reduce the
incidence of sexually-transmitted diseases.
Jennifer Bailey, a medical student at the University of South Carolina, organized local Chapter
Leaders and outside volunteers to improve the self-efficacy rating of health screening volunteers.
She and her colleagues developed and created training opportunities that met volunteer needs
and preferences.
Over the course of the grant, the IHI Open School improved the delivery of the online leadership
program by testing different learning methods in three PDSA cycles through planned experimentation.
The chart below summarizes the methodological differences between PDSA 1, 2, and 3.
Change
Improvement Science
Organizing & Leadership
Training
Subject Matter
Knowledge

Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 9
Pedagogical
Methods
PDSA 1:
Fall 2014
PDSA 2:
Spring 2015
PDSA 3:
Fall 2015
Pre-course in-
person event
Yes No Yes
Registration No screening
process or
project
specification
required to
register
Application
specifying
project required
Application
specifying
project required
Duration 8 weeks 12 weeks 8 weeks
Initial 1:1 meetings Yes No Yes
Coaching calls 8 4 4
Assigned coach Yes No No
Peer coaching No Yes No
Faculty office hours No No Yes
Pre-requisite: Triple
Aim 101:
Introduction to
Population Health
No Yes Yes
Lecture transcripts No Yes Yes
User ability to
increase lecture
speed
No Yes Yes
Content
improvements
No Yes
(Orientation &
Lesson 7)
No
Re-engineered
discussion board
No No Yes
Key Programmatic Learning from the Online Leadership Course
Comparative Analysis of PDSA 1, 2, and 3 Pedagogical Methods
In testing the online course through three improvement cycles, the IHI team made an intentional
choice to invest a high level of coaching resources and internal support in the first cycle and a
lower level in the second. This planned experimentation enabled the team to determine the extent
to which various pedagogical methods resulted in effective learning. The team then adjusted
accordingly in the third cycle to provide leveraged support. Above all, the team attributes more
effective learning to initial 1:1 meetings focused on building relationships and improving project
design, as well as completion of the pre-requisite Open School course, Triple Aim 101:
Introduction to Population Health.
Course Design
The semi-synchronous course format combined with 1:1 meetings improved learner retention
and completion rates.

Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 10
The IHI Open School capacity to support and coach learners improved over time as
improvements were made to pedagogical methods.
Students showed demand for a “summer” cycle to participate in the course when they weren’t
burdened by academic time constraints.
Professionals and faculty showed an increasing demand for the course, as more applied over
time. In addition, a small number of professionals (15) who applied were admitted to the course
during PDSA cycle 3 at a price of $150. We are exploring this for future sustainability.
Building Capacity
Students are using the course to build student and Chapter leadership capacity to take action and
advance population health in their local contexts.
Students are building the efficacy of projects and their Chapters by enrolling new learners in the
course over multiple offerings.
Students are applying the leadership skills in projects beyond population health, including
quality improvement, Chapter formation, Chapter events, and regional conferences.
Students are initiating and building ongoing relationships between universities, colleges, and
local community organizations.
Students have developed a Chapter leadership team role to liaise and foster continued
relationships between schools and community organizations.
Some projects are scalable and are spreading to other Chapters.
The course has built a sustainable infrastructure for ongoing change for the Open School, IHI,
and its partners. The learning platform provides a vehicle for continued training, and through the
course of the grant the team has developed systems for on-going coaching and student activation.
Evaluation Methods
To evaluate each cycle of the online leadership course, the IHI Open School employed data-collection
methods, shown below. These methods enabled the IHI Open School to adapt the Kirkpatrick Four-
Level Training Evaluation Model3, aiming to achieve outcomes at levels 1-3 only.4 Our primary
outcome was the number of students enrolled in the course and the number of individuals they were able
to engage (or secure pledge commitments from). Our secondary outcomes were the learning results
reported by the students from the course.
Participation and certification data: Demonstrated the engagement of the learners in the online
course (Kirkpatrick Level 1).
Pre- and post-course self-assessments: Gathered self-assessed data on the learners’
expectations, satisfaction, achievement of learning objectives, and application of skills learned
(Kirkpatrick Levels 1-3).
3 Kirkpatrick, J., and W. Kirkpatrick. The Kirkpatrick Model. April 2009. Available at http://www.kirkpatrickpartners.com/OurPhilosophy/TheKirkpatrickModel. 4 Originally developed to evaluate the effectiveness of professional development and training programs, the Kirkpatrick Framework includes four levels of evaluation: participants’ experience (level 1), learning (level 2), action (level 3), and the improvement of outcomes (level 4). I-CAN’s online program does not measure the improvement of outcomes because each learner’s project is designed to achieve different population health outcomes in local settings.
Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 11
Practice assignments (Lessons 1-8) and final summary assignment: Provided qualitative data
on learners’ application of the skills in their contexts (Kirkpatrick Level 3).
Post-lesson and post-course coaching team “study” debriefs: Captured the coaches’ and
faculty’s qualitative insights on the delivery and learning at the end of each lesson and course
(Kirkpatrick Levels 1-3).
Primary Outcomes
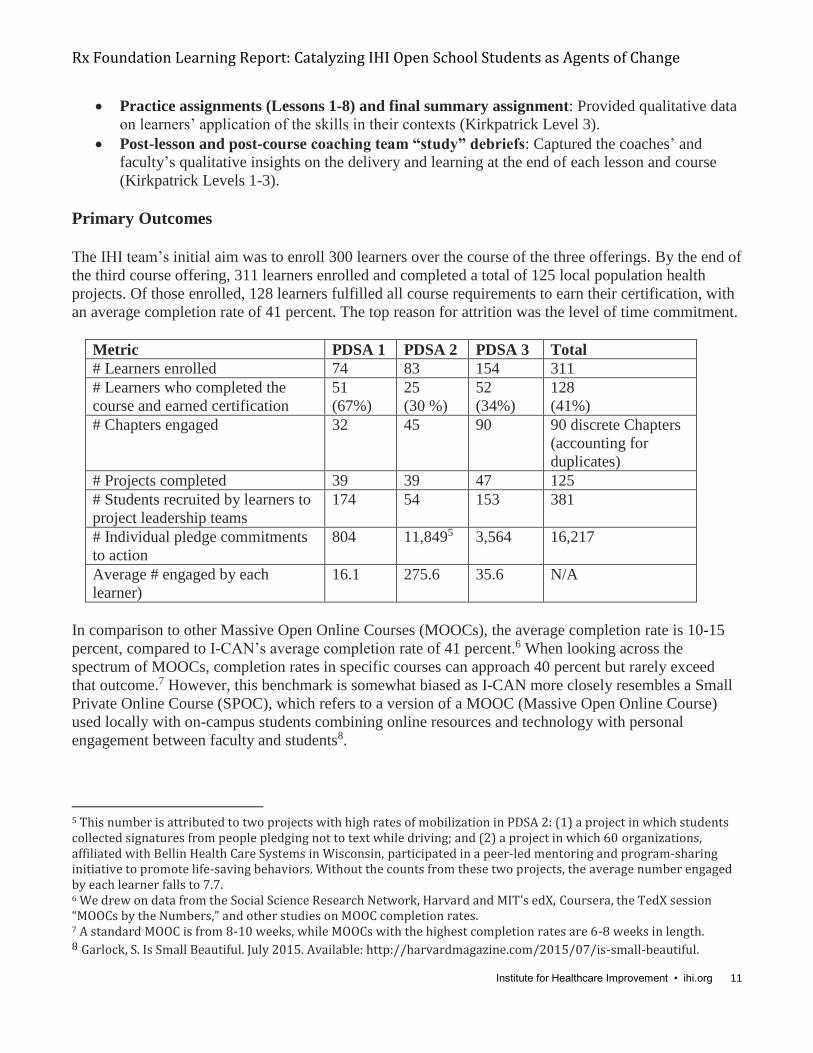
The IHI team’s initial aim was to enroll 300 learners over the course of the three offerings. By the end of
the third course offering, 311 learners enrolled and completed a total of 125 local population health
projects. Of those enrolled, 128 learners fulfilled all course requirements to earn their certification, with
an average completion rate of 41 percent. The top reason for attrition was the level of time commitment.
Metric PDSA 1 PDSA 2 PDSA 3 Total
# Learners enrolled 74 83 154 311
# Learners who completed the
course and earned certification
51
(67%)
25
(30 %)
52
(34%)
128
(41%)
# Chapters engaged 32 45 90 90 discrete Chapters
(accounting for
duplicates)
# Projects completed 39 39 47 125
# Students recruited by learners to
project leadership teams
174 54 153 381
# Individual pledge commitments
to action
804 11,8495 3,564 16,217
Average # engaged by each
learner)
16.1 275.6 35.6 N/A
In comparison to other Massive Open Online Courses (MOOCs), the average completion rate is 10-15
percent, compared to I-CAN’s average completion rate of 41 percent.6 When looking across the
spectrum of MOOCs, completion rates in specific courses can approach 40 percent but rarely exceed
that outcome.7 However, this benchmark is somewhat biased as I-CAN more closely resembles a Small
Private Online Course (SPOC), which refers to a version of a MOOC (Massive Open Online Course)
used locally with on-campus students combining online resources and technology with personal
engagement between faculty and students8.
5 This number is attributed to two projects with high rates of mobilization in PDSA 2: (1) a project in which students collected signatures from people pledging not to text while driving; and (2) a project in which 60 organizations, affiliated with Bellin Health Care Systems in Wisconsin, participated in a peer-led mentoring and program-sharing initiative to promote life-saving behaviors. Without the counts from these two projects, the average number engaged by each learner falls to 7.7. 6 We drew on data from the Social Science Research Network, Harvard and MIT’s edX, Coursera, the TedX session “MOOCs by the Numbers,” and other studies on MOOC completion rates. 7 A standard MOOC is from 8-10 weeks, while MOOCs with the highest completion rates are 6-8 weeks in length. 8 Garlock, S. Is Small Beautiful. July 2015. Available: http://harvardmagazine.com/2015/07/is-small-beautiful.

Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 12
In total, 311 learners recruited 381 other students to their project leadership teams. Together, over three
cycles, these students engaged a total of 16,217 people in commitments to advance population health in
local settings.9
Secondary Outcomes
K1: Experience/Reaction
Immediately following the last lesson of the course, the IHI team asked students to rate the degree to
which the course met their expectations using a three-point scale: did not meet expectations, met
expectations, exceeded expectations (e.g., Figure 7).
Figure 7: Kirkpatrick Level One– Experience/Reaction for PDSA Cycles 2 and 310
Overall, the course met or exceeded the learners’ expectations, with variation attributed to testing
different learning methods applied in each cycle. The relative decrease in the number reporting
“exceeded expectations” may be attributed to the 54% increase in the number of course participants
between cycles 2 and 3, resulting in lower engagement by the coaching team. Continued planned
experimentation will help us to determine the optimal learner-coach ratio for exceeding expectations.
K2: Learning
The IHI team taught students improvement methods and leadership skills, and encouraged students to
test them in local population health projects. The IHI team assessed students on their learning before and
after the course (e.g., Figure 8).11
9 The compiled figures are conservative, based only on self-reported data. In addition, 6-month and 12-month post-program assessments have not been completed to date. 10 PDSA 1 data is not included due to an omission in collecting this information for that cycle. 11 The results for figures 8 -10 are attributed to PDSA cycle 3 participants only as our assessment was improved to have participants – at the end of the course - rate their perceived level of understanding at the start and end of their learning. This change was made to overcome a cognitive bias in which participants mistakenly assess their ability to be much higher than it really is. Kruger, Justin; Dunning, David (1999). "Unskilled and Unaware of It: How Difficulties in Recognizing One's Own Incompetence Lead to Inflated Self-Assessments". Journal of Personality and Social Psychology 77 (6): 1121–34.

Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 13
Figure 8: Kirkpatrick Level Two – Assessment of Learning for PDSA Cycle 3
Students improved most significantly in understanding organizing as a theory of change. Students also
made impressive gains in how to structure distributed leadership, how to build the capacity to sustain
change, and knowledge of what action to take to improve the health of a population.
K3: Process / Behavior Change
Students modified their behavior by practicing the leadership and organizing skills in population health
projects and took measurable action in local contexts (e.g., Figure 9).
Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 14
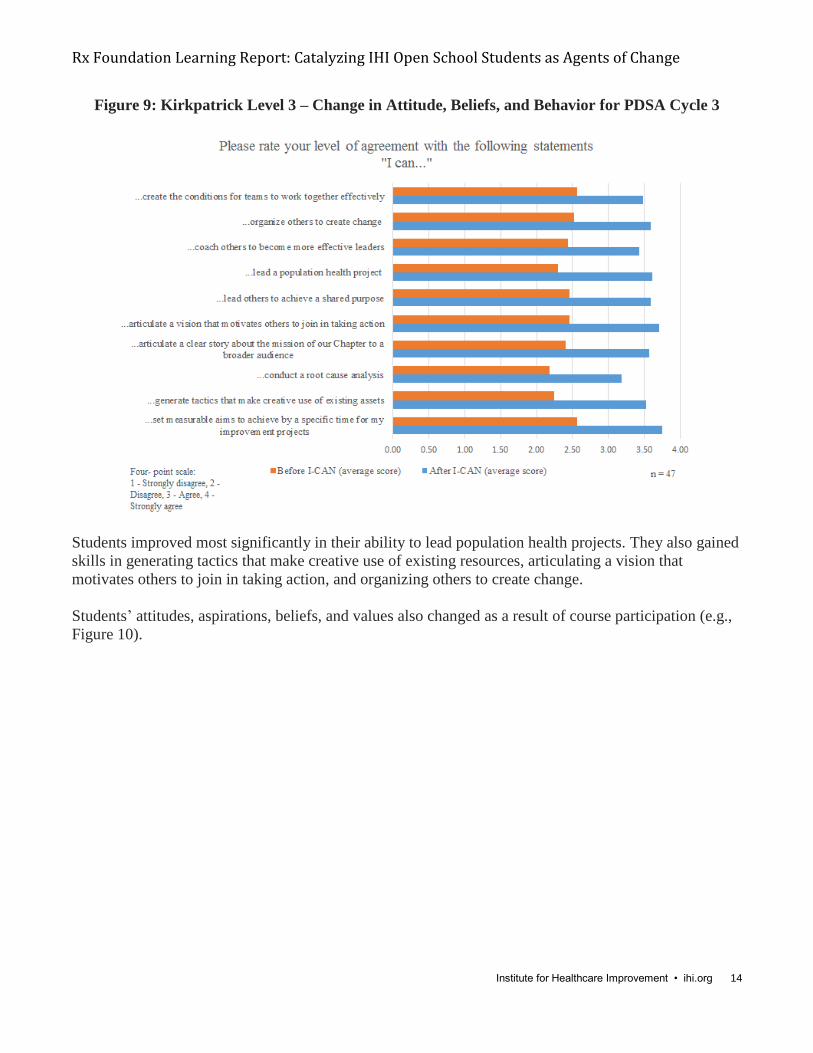
Figure 9: Kirkpatrick Level 3 – Change in Attitude, Beliefs, and Behavior for PDSA Cycle 3
Students improved most significantly in their ability to lead population health projects. They also gained
skills in generating tactics that make creative use of existing resources, articulating a vision that
motivates others to join in taking action, and organizing others to create change.
Students’ attitudes, aspirations, beliefs, and values also changed as a result of course participation (e.g.,
Figure 10).

Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 15
Figure 10: Kirkpatrick Level 3 – Change in Attitude, Beliefs, and Behavior for PDSA Cycle 3
Most notably, students felt more responsible for improving population health after participating in I-
CAN. Taken together, these shifts in behaviors and attitudes demonstrate the course’s ability to build
students’ leadership capacity and influence their beliefs about population health.
K4: Results
Because each student’s project was designed to achieve different population health outcomes in local
settings, the IHI team does not have an aggregate measure of K4 outcomes achieved. However,
anecdotal reports from students in their final assignments demonstrate that some projects resulted in
improved patient outcomes:
Stefanny Pazmino and Brianna Trent, two nursing students at the State College of Florida,
worked with faculty to lead projects that resulted in a reduction in patients’ hemoglobin A1C and
weight.
An interprofessional team of medical, dental, nursing, and health administration students from the University of Texas Health Sciences Center and Trinity University worked together at a
student-run refugee clinic in San Antonio to reduce wait times for patients by ten minutes,
ensuring efficient and timely medical care.
Ola Hassan, a master’s nursing student from the State College of Florida, engaged 39 patients
with high blood pressure and diabetes to commit to healthier lifestyle choices. To date, as she
continues to monitor outcomes, 16 of the 39 patients lost between six and eleven pounds; one
patient even decreased their blood pressure medication per physicians’ orders.
Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 16
Additional Observations The IHI team has made several additional observations as a result of student involvement in the course.
The team will continue to track it over time. For example:
Students from Portland State University, Oregon Health Sciences University, and Willamette
University have received funding to run an interprofessional student-led health clinic at a local
homeless shelter and resource center in Portland, Oregon. The students will work to address the
unmet need for clinical and social services in their community as identified by the organization.
They have recruited 25 interprofessional students to help organize and support this work.
Students from Emory University are building educational tools for a diabetes self-management
course created by learners in the second offering of the I-CAN course. In this new piece of their
work, they are pursuing funding to support and design new processes at their local clinic to
improve access to medications and supplies, as well as outpatient service for patients.

Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 17
Part III: I-CAN Mobilization Events for Movement Building
While students enrolled in the I-CAN online leadership course were responsible for securing more than
half of the 35,505 pledges, the IHI team targeted and engaged the rest of the IHI Open School
community through mobilization activities — a separate, second stream of work. This section of the
report focuses on I-CAN’s mobilization strategies in Year 2, including online activity pages, the Student
Organizing and Leadership Academy, and an International Pledge-a-Thon. (Please see Interim Report
for Year 1 mobilization activities.)
Activity Pages The IHI team developed online activity pages to broaden student reach and help interested students get
started. The goal of the activity pages was to compile a set of activities to enable students to build skills
and knowledge to improve population health.
Activity pages navigate students through the four drivers of health:
(1) Access to care: high cost, uninsurance, and access to clinics and providers
(2) Health behaviors: chronic disease, sexual activity, diet and exercise, and tobacco use
(3) Social determinants of health: poverty, housing, education, and community safety
(4) Clinical care: mental health, maternal and infant health, quality of care, and cultural competency
Each page included: (1) a definition of the problem; (2) an embedded video clip of Don Berwick, calling
students to action to address the topic area; (3) compiled resources and activities, reviewed by subject
matter experts, which enabled students to begin taking action; and (4) a list of existing I-CAN projects
and possible partnerships with other national campaigns.
To date, 1,048 students (and some professionals) have visited the activity pages to learn more and take
action in their local settings.
Student Organizing and Leadership Academy On August 20-21, 2015, the IHI team invited 31 student leaders, representing 24 Chapters, to the IHI
office in Cambridge, Massachusetts, for the Student Organizing and Leadership Academy. The
objectives of the program were to:
(1) Develop students’ ability to mobilize, recruit, and activate others to improve population health
(2) Build relationships and a lifelong network among IHI Open School Chapter Leaders committed
to improvement
(3) Give participants the skills and tools needed to lead change in their local Chapters
I-CAN faculty, Kate Hilton and Don Berwick, worked with the IHI team and students to design the
Student Organizing and Leadership Academy to equip participants with skills and strategies to mobilize
widespread action and “sprint” to 30,000 pledges. Program faculty also included Joe McCannon, Co-
Founder of the Billions Institute; James Moses, MD, MPH, Assistant Professor of Pediatrics, Boston
Medical Center; Rishi Manchanda, MD, Chief Medical Officer, Author; Andy Carson-Stevens, MD,
Patient Safety Research Lead, PRIME Centre Wales; and a collection of IHI staff members: Michael
Briddon, MA; Jessica Perlo, MPH; Katie McCormack; Gina Deitz; and John Gauthier.

Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 18
Prior to arrival, students pre-selected an area of interest among the drivers of health: (1) access to care;
(2) health behaviors; (3) social determinants of health; or (4) clinical care. At the event, students formed
interprofessional teams of four within respective areas and went into Harvard Square to practice
engaging others to take action. First, teams crafted aim statements defining how many people they
would target and what action they would take. They then developed the following “asks” (with the
number of commitments made in parentheses):
Access to care:
“Will you draw on the questions provided in the Choosing Wisely campaign to engage your
provider in dialogue around right care and costs at your next visit?” (74)
“Will you commit to sharing with one other person the difference that the state of Massachusetts
is spending on health care versus other social services?” (94)
Health behaviors:
“Will you pledge to get tested for sexually-transmitted infections (STIs) in the next three
months?” (60)
“Will you download and use the “my fitness pal” app on your smartphone to monitor your
calories?” (64)
Social determinants of health:
“Will you commit to learn more and share information about housing insecurity in Cambridge,
Massachusetts?” (96)
“Will you pledge to mentor one local youth to help prevent youth violence?” (51)
“Will you pledge to create a “circle of six” to protect yourself and others from domestic
violence? (95)
Clinical care:
“Will you participate with me in a mindfulness/de-stress activity right now?” (203)
In just 75 minutes in Harvard Square, 31 students mobilized a total of 737 people to action. Students
then developed social media and “upstreamist” tactics12 to complement the one-to-one relational
approach deployed on the streets. Students continue to tweet today at #ICANimprovehealth.
12 Rishi Manchanda, MD, founder and president of HealthBegins, defines an “upstreamist” as a health professional capable of seeing the social and environmental factors, such as social justice, and access to food and housing, that drive disease factors and health in individuals and communities. An “upstreamist” moves clinical care “upstream” to the source of the larger population problem rather than reacting to each individual presentation of the health problem.

Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 19
Here are some images from the mobilization day:
One hundred percent of participants at the Student Organizing and Leadership Academy “agreed” or
“strongly agreed” with the following statement: “After participating in this event, I have more
confidence in my ability to lead change.”13 Participants overwhelmingly offered positive comments
about the mobilization activity in Harvard Square, expressing that it helped them to move past the fear
of approaching others and to discover their ability impact behavior change in a short period of time.
Participants described the event as “inspiring,” “transformative,” “motivating,” and “life-changing.”
The International Pledge-a-Thon At the end of the Student Organizing and Leadership Academy, 11 interprofessional students from eight
Chapters formed the Step-In Team to spearhead a mobilization effort across all IHI Open School
Chapters. Their experience at the event motivated them to take on a leadership role to mobilize the
global community to advance I-CAN’s aims and improve population health.
This team designed a 30-day, international Pledge-a-Thon, inviting all 780 Chapters of the IHI Open
School Network to commit to mobilizing toward I-CAN’s goal of 30,000 pledges to improve population
health. The team developed an infographic and website (see below), as well as a social media strategy.
They hosted an I-CAN Twitter chat with Don Berwick, in which 164 users participated. Additionally,
the team organized inter-Chapter video challenges, similar to the successful ALS Ice Bucket Challenge,
to encourage other Chapters to improve health on their campuses and in their local communities.
13 68 percent of students “strongly agreed”; 32 percent “agreed.”

Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 20
Finally, the IHI Open School incentivized Chapters by offering four full scholarships to attend the IHI
27th Annual Forum in Orlando, Florida, to the Chapter with the most overall pledges.
Twenty-seven Chapters signed up to participate in the I-CAN Pledge-a-Thon, engaging 3,189 other
students on their campuses in mobilizing others. Together they secured 5,747 pledges from people to
improve population health across a variety of projects. Three Chapters also enrolled their Pledge-a-Thon
leadership teams in the third cycle of the I-CAN course.
Examples of Pledge-a-Thon Chapter projects included:
James Madison University secured 2,137 pledges from students to get their flu vaccines and
follow proper hygiene protocols.
The University of South Carolina focused on suicide prevention by securing 935 commitments
from people to understand and be able to identify the signs of suicide risk.
Portland State University, Oregon Health Sciences University, and Willamette University
Chapters joined forces to fight homelessness and housing insecurity by connecting 726 people to
civic engagement and volunteer opportunities. (Please see supporting visual below.)
Brock University secured 514 pledges from the community to stop texting while driving. (Please
see supporting visual below.)
Universidad Peruana Cayetano Heredia in Peru secured 560 pledges from community members
and health care professionals around preventative activities including vaccines, healthy lifestyle
choices, health screenings, and adherence to treatments.

Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 21
Key Learning from Mobilization Events
Mobilization events helped students exercise leadership to organize other students throughout the
IHI Open School Chapter network.
Mobilization events created an opportunity for students to participate in I-CAN without
completing the eight-week online course.
Mobilization events enabled students to activate a larger network through social media.

Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 22
Part IV: Development and Improvement of an Internet-Based Platform for
Sustainable Collaboration and Change
I-CAN is a platform for IHI organizational and student collaboration and improvement. The online
virtual learning platform is enabling students to collaborate globally with one another across Chapters
and build movements. The I-CAN platform also supports the IHI Open School and its students in
building external partnerships with faculty, professionals, and other organizations seeking to advance
health and health care improvement.
I-CAN Web-Based Virtual Improvements The IHI Team collaborated with the IHI engineering department to create an online platform to support
the learning program, drawing on examples from MOOC providers, Coursera and edX. The easy-to-
navigate system includes an in-page video player, a peer-evaluation structure and algorithm, a platform
for learners to upload and review assignments, a course calendar, a chat room for virtual “office hours”
with faculty, and discussion boards. The team made iterative improvements over the three cycles of the
online course. For example, in the third course offering, students benefited from threaded discussion
boards that allowed them to respond directly to one another.
On the mobilization front, the engineering team also supported the development of the online pledge
system, activity pages, embedded Twitter feed, and international Pledge-a-Thon.
In addition, the team made enhancements to the existing IHI user group functionality. New features
helped to facilitate the creation and sharing of ideas through project progress monitoring, data
aggregation features, and an improved user interface. Most notably, an interactive Chapter map now
connects users to the contact information of all IHI Open School Chapters around the world.
In addition to supporting I-CAN and the Chapter community, these technology developments and
enhancements will be useful for all future IHI learners.
I-CAN Collaborations to Amplify Impact The IHI Open School used I-CAN as a platform for collaboration with other internal and external
partners: university faculty, professionals, the 100 Million Healthier Lives effort, and the Pathway to
Pacesetters.
University Faculty
The IHI Open School tested the engagement of faculty in the online leadership training. Some faculty
used their involvement to advance interprofessional projects on their campuses with IHI Open School
students and other colleagues. Others directly used the I-CAN curriculum (or sections of it) in their own
courses. A handful of faculty are organizing interprofessional teams of students in their classrooms to
advance population health projects, drawing on I-CAN video clips, transcripts, and exercises as required
material.
Professionals
Students are using I-CAN to develop active partnerships with — and between — health care
organizations, social services, and community health organizations. I-CAN gives them the skills and
knowledge to build movements and lead innovative collaborations that can improve health and health

Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 23
care. They want to leverage these new resources to engage professional partners to work with them in
their communities. To date, I-CAN students have presented their work to professional audiences at IHI’s
26th and 27th Annual National Forums, IHI’s International Forum, Communities Joined in Action’s
Annual Conference, and on WIHI, a bi-weekly radio show at IHI.
In the second and third cycle of the online leadership course, the IHI Open School accepted a group of
15 professionals from different disciplines who work within health care systems and communities trying
to improve health. As future paying customers, this audience may contribute funding to ensure I-CAN’s
sustainability.
100 Million Healthier Lives
The IHI Open School has aligned the work and aims of I-CAN with an initiative IHI is supporting to
improve the health of 100 million people by 2020. This unprecedented collaboration is dedicated to
community health by convening patients, community members, and leaders across the domains of public
health, community health, health care, policy, academia, business, and finance. It is organized around
the core belief that long-term, large-scale results are possible only by working alongside communities.
I-CAN has contributed more than 30,000 pledges of action on population health to the 100 million
metric, and it serves as the “student hub” within the 100 Million Healthier Lives initiative. I-CAN
students were featured on monthly 100 Million Healthier Lives momentum calls in May and June 2015,
and they presented their contributions at its one-year celebration in September 2015. The IHI Open
School will continue to partner with 100 Million Healthier Lives to leverage I-CAN students as change
agents in future work.
Pathway to Pacesetters
Pathway to Pacesetters is a Robert Wood Johnson-funded program in partnership with IHI and 100
Million Healthier Lives. The program provides an online curriculum to support communities moving
along a pathway to improving health. Program leaders have incorporated the 8-week I-CAN curriculum
into their overall educational offerings.
Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 24
Part V: Conclusions and Next Steps
I-CAN has achieved the aims of the Rx Foundation grant by: (1) equipping committed student leaders
with skills and knowledge to organize local health improvements and (2) supporting students to mobilize
and build networks that will lead to more fruitful careers — and, more importantly, better outcomes for
patients. The interactive I-CAN platform, outlined in Part IV, bolstered both of these outcomes.
Conclusions from I-CAN include:
I-CAN is a course, a program, a movement, and a platform that develops and supports leaders
dedicated to advancing improvement in population health.
I-CAN is:
(1) Developing leaders: students are applying collaborative leadership skills in action as they
organize local health improvement projects.
(2) Building capacity: students are working interprofessionally in a learning community of
like-minded peers and professionals.
(3) Achieving aims: students are engaging others in a “culture of health” and improving
population health outcomes in local settings.
As a result of being involved in I-CAN, students report having a better understanding of health,
stronger Chapters, healthier campuses, and new campus relationships with community
organizations.
The rising generation of health professionals is pursuing health care to make people healthier —
to enable healthy lives in which people can do the things that matter most to them. As passionate
advocates for change, students are using I-CAN to redefine themselves no longer solely as health
care providers but leaders for health.
I-CAN is a core component of the IHI Open School strategy to advance students’ experiential
learning and action to improve health and health care.
Opportunities and Plans for Sustainability
With an eye toward I-CAN’s future, the IHI team is working on a number of strategies to ensure
sustainability and momentum:
IHI has a strategic priority to dramatically expand our global reach in the basics of improvement
capability, including the mobilization methods in I-CAN.
The IHI Open School will continue to offer I-CAN’s leadership course biannually to develop
students’ leadership skills, advance local improvement projects, build Chapter capacity, and
generate outcomes for population health and quality improvement.
The IHI Open School will pursue funding to support the I-CAN mobilization events such as the
Student Organizing and Leadership Academy to further integrate these into the IHI Open School
strategy to mobilize students to action within Chapters.
The IHI Open School will widen the scope of projects accepted into I-CAN’s online leadership
course to support students advancing improvement projects in quality and safety as well as
population health.
The audience for I-CAN’s online leadership course will expand to include students, faculty, and
professionals. Professionals will pay a fee that will partially offset the resources needed to

Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 25
support to I-CAN. Faculty will serve as force multiplier to get the tools into the hands of more
students taking action for improvement.
The IHI Open School can leverage I-CAN to partner with other similar organizations that can
enroll students to help them build collaborative leadership capacities to engage others in quality
improvement and population health. For example, the IHI Open School has engaged in early
conversations with the United States Surgeon General’s Office to support national mobilization
efforts in coming years.
As a platform and movement for change, the IHI Open School may select one (or more) focused
I-CAN campaigns in which students across all Chapters harness their resources toward one
collective action. The outcome of this type of focused campaign would be the same — and
thereby measurable — across all localities. In this way, the IHI Open School can continue to
marry its capacity to mobilize and train students with the necessity of creating a movement.
The IHI Open School will conduct six-month and one-year follow-up surveys to explore Level 3
and Level 4 of the Kirkpatrick metrics. For instance, the IHI Open School can further assess I-
CAN student projects that resulted in and sustained change, in addition to participants that have
altered the way they work on and with interprofessional teams and Chapters.

Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 26
Appendix
Selected Examples: Learners’ Experiences
The Tummy Time Project
In July 2014, Melissa Gilbreth, a second-year medical student at the University of South Carolina
(USC), created a tool to educate mothers of all ages (targeting mothers under the age of 20) on how,
why, and when to provide “tummy time” to their infants. (Melissa followed the American Academy of
Pediatrics’ (AAP) guidelines to define “tummy time.”) In an effort to decrease plagiocephaly and
torticollis, as well as to promote the development of infant head control for a successful progression
toward future gross motor milestones, Melissa enrolled in the first cycle of the I-CAN leadership course.
She initially set a modest aim to educate 100 expectant and new caregivers on tummy time by February
2015.
As Melissa identified and recruited other student leaders to join her team, they distributed leadership
responsibilities and developed a more audacious aim together: to educate expectant and new caregivers
on tummy time with a goal of 2,000 signed pledges to practice tummy time with infants. As new leaders
joined, they expanded the project’s scope to include an institutional review board (IRB) pilot research
study; developed educational materials (an award-winning video, pamphlets with AAP-approved
recommendations); created partnerships with centering pregnancy groups; recruited provider volunteers;
and expanded into Hispanic neighborhoods, including translating all educational materials into Spanish
and purchasing racially diverse dolls for role playing.
As Melissa reports:
The project is more audacious than I envisioned alone. We used the I-CAN curriculum to
develop shared leadership, identify common values, and connect to team members’ interests.
Through I-CAN, I personally became more purposeful in the development of relationships
between team members and am now better able to not only create a distributed model of
leadership, but cultivate it. … [For example,] we used the one-to-one meetings as a mechanism
for our leaders to reach out to team members, and then for our team members to recruit new
team members. We used personal narrative as a part of our one-to-one meetings to ensure that
people’s motivations matched the part of the project that they actively worked on. Together we
are drawing from our collective experiences and this has strengthened our vision. … I-CAN
guided me to develop a stronger sense of purpose in my project. It helped me keep an open mind
to all that others could offer and [as a result] the project has grown. I have learned how to
promote leadership from student volunteers, identify shared goals, and enable others to lead.
Over the course of the three cycles, six Tummy Time leadership team members completed the I-CAN
course, and more than 35 USC IHI Open School Chapter students participated in the project. The South
Carolina Healthy Birth Outcomes Initiative is working with the Tummy Time team to spread and scale
the effort across the state of South Carolina. Other IHI Open School students have asked the Tummy
Time team to help them replicate the project locally.
Stop the JMU Flu
A team of 10 student leaders from the IHI Open School Chapter at James Madison University (JMU) set
an aim to secure 2,000 signed pledges from other on-campus students to “stop the JMU flu” by
practicing proper hygiene and getting vaccinated between October 1 and November 15, 2015. The team

Rx Foundation Learning Report: Catalyzing IHI Open School Students as Agents of Change
Institute for Healthcare Improvement • ihi.org 27
enrolled in the third offering of the I-CAN leadership course and participated in the international Pledge-
a-Thon (see Part III), with a winning total of 2,137 people pledging to get vaccinated.
In the process, the JMU team mobilized 15 other student volunteers to canvass the campus, staff
volunteer tables, support the Maxim Health Services vaccination clinic, and volunteer at local
pharmacies such as CVS and Walmart. The students deployed tactics like setting up a competition
between student organizations, including Greek organizations and SafeRides, to collect the most
pledges. Each organization incentivized members to sign their pledge in ways that were meaningful to
them, securing close to 469 of the 2,137 pledges.
The team partnered with many other stakeholders, including student organizations, the Medical Director
at the University Health Center, the JMU Assistant Director of Marketing and Communications, the
JMU Coordinator of Organization Development, Student Activities, Involvement, and Health Services
Flu Vaccination Clinic. On the first day of their involvement, the students administered more vaccines
than in any two-day period since the vaccination program started. In fact, on the second day, the clinic
ran out of vaccines!
A team member remarked:
The biggest value that I saw from the I-CAN project was the leadership development and
experience that our students gained. We had a number of students volunteer to take on a
leadership role in our project that had limited leadership experience and they all grew into
themselves very nicely. Additionally, they learned the idea of network thinking and how to
inspire/mobilize people for a common aim. This experience led half of the leadership team to run
for positions on our Chapter’s leadership board, therefore spring boarding them into more
leadership experience.