cauda equina by hugh pelc bsc, mbbs, mrcs, mrcgp
TRANSCRIPT

Cauda Equina
By Hugh Pelc Bsc, MBBS, MRCS, MRCGP

This is a serious business
Cauda equina syndrome occurs in approximately 2% of cases of herniated lumbar discs
The cauda equina are LOWER motor neurones and sensory nerve roots.
They do not show good healing compared to UPPER motor neurones
Good evidence suggests surgery should be performed within 24h of the onset of symptoms
Complications of untreated/delayed treatment include incontinence and sexual dysfunction.
More than 1000 operations/y performed in England alone i.e. NOT RARE
Average litigation payout 336,000 GBP

Aims
Understand anatomy pertinent to Cauda Equina syndromeUnderstand what Cauda Equina Syndrome isKnow the important symptoms of Cauda EquinaKnow the important aspects of examination for Cauda EquinaKnow when referral is indicated
Educators love aims and objective slides
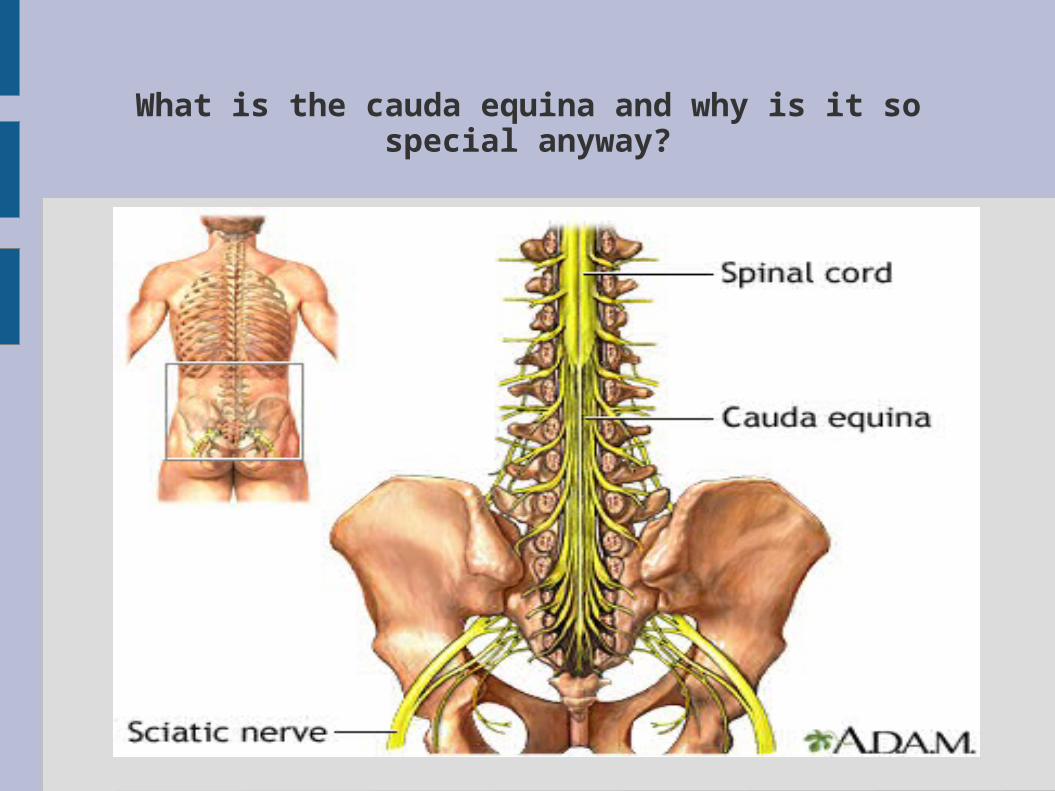
What is the cauda equina and why is it so special anyway?
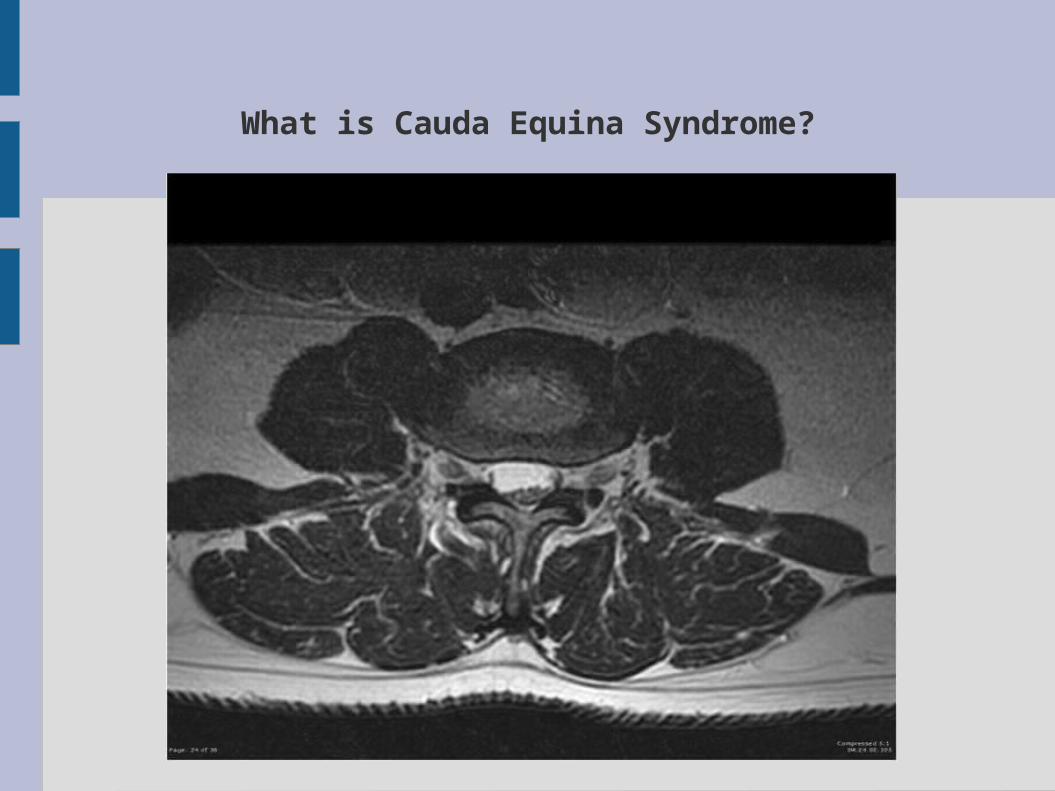
What is Cauda Equina Syndrome?

Disc Bulge
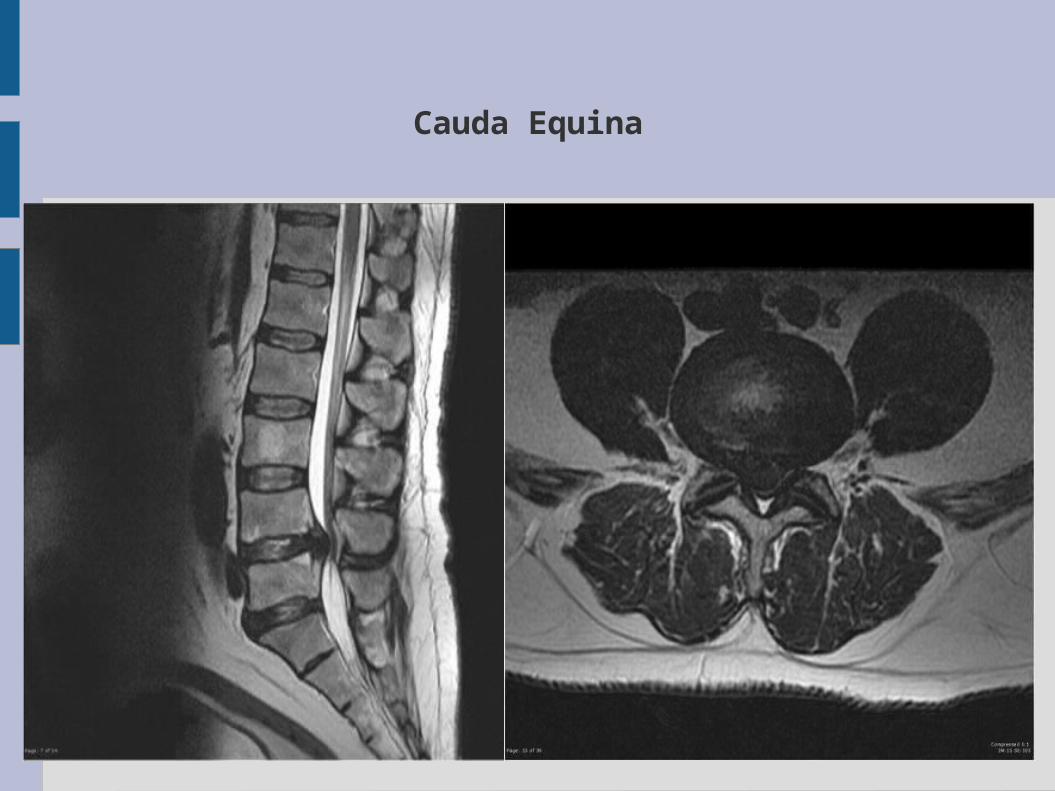
Cauda Equina

Why is it so bad?
The disc squishes all of the nerve roots This therefore includes those innervating the bladder,
bowels and genitals Consequently incontinence, global weakness/paralysis and
sexual dysfunction are risks Don't forget these are lower motor neurones and heal badly
This is a “chunk and check” slide

Classic History
Develops rapidly over hours-days Sometimes on background of established sciatica Here are the “classic signs”:
ParaesthesiaeMotor abnormality1)Bilateral sciatica2)Altered perineal (peri-anal) sensation3)Absence of urge to micturate4)Urinary retention/incontinence (overflow)5)Faecal incontinence/constipation6)Altered genital sensation7)Sexual dysfunction (i.e. erectile dysfunction)

Hang on a minute...
How do we know that altered perianal sensation or any other “classic sign” is not from normal sciatica?
i.e. from a paracentral disc bulge

Because there aren't any discs below the L5/S1 disc
So the S2 root cannot be compressed by a paracentral disc bulge
Nor can the S3,4 or 5 roots!
Innervation of perianal sensation/bladder function/bowel function/genital sensation is all from lower sacral nerve roots
HISTORY: What to ask
Step 1: Confirm that this really is sciatica – i.e. dermatomal shooting pain extending below the kneeIt is unlikely to be sciatica if there is no pain below the knee95% disc prolapse occurs at L4/5 or L5/S1If there is no pain below the knee establish the dermatome
carefully
Step 2: Ask for the “classic signs”.

HISTORY: What do we really need to ask?
“Do you still notice the urge to pee?” “Have you wet yourself at all” “Do your privates still feel normal when you wipe?” (female) “Does your penis feel tingly?” and “Have you started
having trouble getting erections?” (male) “Do you ever get the pain in the other leg?” “How are your bowels?” “Have you noticed any pins and needles around your back
passage?”
BEWARE: codeine, previous incontinence/ED, pain that isn't sciatica
“You might have trapped a nerve”“The nerve causes pain in your leg but it might also control your bladder, bowel or private parts”

HISTORY: Summary
Establish a history of dysfunction in a nerve supplied by S2 or lower.
BladderBowelGenitalsPerineum
“This is a chunk and check slide”
EXAMINATION: What should we do?
STEP 1: Establish sciaticaCheck for dermatomal paraesthesiaeCheck for myotomal weakness
STEP 2: Special tests to help establish sciaticaSLR until pain ellicitedDoes ankle dorsiflexion worsen pain?Does knee flexion improve pain?
STEP 3: Consider testing hip rotation/knee movements.

If they admitted to any “classic signs”
Glove up people, you're going in.

EXAMINATION: Summary
Establish SciaticaPR if they admitted to “classic signs” in the history
“This is a chunk and check slide”

Indications for Referral/MRI
Presence of any “classic signs”Just 1 will do.


Lower Limb Neuro Examination
L2 – Hip flexionL3 – Knee extensionL4 – Ankle DorsiflexionL5 – Hallux dorsiflexionS1 – Ankle Plantarflexion
All posterior muscles are S1 (e.g. knee flexion)