cauti: lessons learned from the hac penaltyatomalliance.org/wp-content/uploads/2015/04/cauti.pdf ·...
TRANSCRIPT

4/8/15
1
Kim Roberts
Infection Control Manager
OCH Regional Medical Center
CAUTI: Lessons Learned from the HAC Penalty
April 14, 2015
CAUTI: Lessons learned from the HAC penalty
“Did you hear the news…?!”

4/8/15
2
I hope others will learn from our experience with the HAC penalty. Our story began like this…

4/8/15
3
HAC Penalty Calculation • Domain 1 Score • Jul 2011 - Jun 2013 • Patient Safety Indicator
(PSI 90) composite measures (8 items): v Pressure ulcer v Iatrogenic pneumothorax v CVC-related bloodstream infection v Postoperative hip fracture v Perioperative pulmonary embolism
or DVT v Postoperative sepsis v Postoperative wound dehiscence v Accidental puncture or laceration
Our score was 3
Weighted at 35% of overall HAC score.
• Domain 2 Score • Jan 2012 - Dec 2013
• CLABSI v This score calculated for any ICU with >1.0 “expected” infections. v We had less than 1 “expected” infection, so this data was not used.
• CAUTI v This score calculated for any ICU with >1.0 “expected” infections v We had 1.747 expected infections. v Since we didn’t have a CLABSI score, the CAUTI score counted for the entire Domain 2 score.
Our score was 10 Weighted at 65% of overall HAC score.
HAC Penalty Calculation • Hospital data was ranked into performance “deciles” • Scores of 1-10, based on which decile you fall into
v Lower scores are better • Domain 1 (35% of overall score). Our score was 3 • Domain 2 (65% of overall score). Our score was 10 • Hospitals received penalty if overall HAC score > 7
v Our combined score was 7.55 (see below)

4/8/15
4
Statistical Power Would 1 fewer infection have changed our score on Domain 2? CMS used a ratio of actual vs. "expected" infections. # actual CAUTI / # expected CAUTI 5 / 1.747 = 2.862 4 / 1.747 = 2.290 The 10th performance decile included scores between 2.013 to 6.000 Even after subtracting one infection, our CAUTI score was in the 10th decile. The 9th performance decile included scores between 1.564 to 2.013 What would the number have been with 2 fewer infections? 3 / 1.747 = 1.717 With a score of 9 on Domain 2 (weighted at 65% of total HAC score), and the score of 3 on Domain 1 (weighted at 35%), it would put us below the magic number 7 that CMS set as the threshold for the penalty. HAC Penalty Formula: (Domain 1 Score * Domain 1 weight) + (Domain 2 Score * Domain 2 weight) = Total HAC Score Our score was calculated as: (3 * 0.35) + (10 * 0.65) = 7.55 We were penalized because this score was > 7
The lesson learned was that we needed 2 fewer CAUTI infections during 2012-2013 to avoid the HAC penalty: (3 * 0.35) + (9 * 0.65) = 6.9 That’s less than the threshold for the penalty (less than 7)
Device Days The ITS department developed an automated
system to help record the # of inpatients on each unit, and the # of devices in use at same time every day:
• ICU • Inpatient Medical Ward • Inpatient Surgical Ward • Postpartum / Pediatric Ward
Can do weekly sampling method if average # device days > 75 per month

4/8/15
5
Culture Surveillance
• The Infection Control department reviews all culture reports.
• When we identify a positive urine culture, we check whether the UTI was present-on-admission (POA), and whether the infection meets the HAI or CAUTI definitions, per NHSN.
• We track what types of organisms are causing CAUTIs at our facility (next slide) à
CAUTI organisms
20%
20%
40%
20%
Proteus vulgaris
Providencia stuartii andKlebsiella oxytocaE. coli
MRSA
Culture Surveillance

4/8/15
6
CAUTI Prevention • Foley assessments
v Observe and evaluate nurses performing Foley catheter insertions
v Product evaluation: ü What types of catheters are in use at our
facility, what features do nurses prefer, talk to staff about their catheter experiences
ü Compare various catheter trays ü Ask other facilities what products they are
using. Get advice and recommendations.
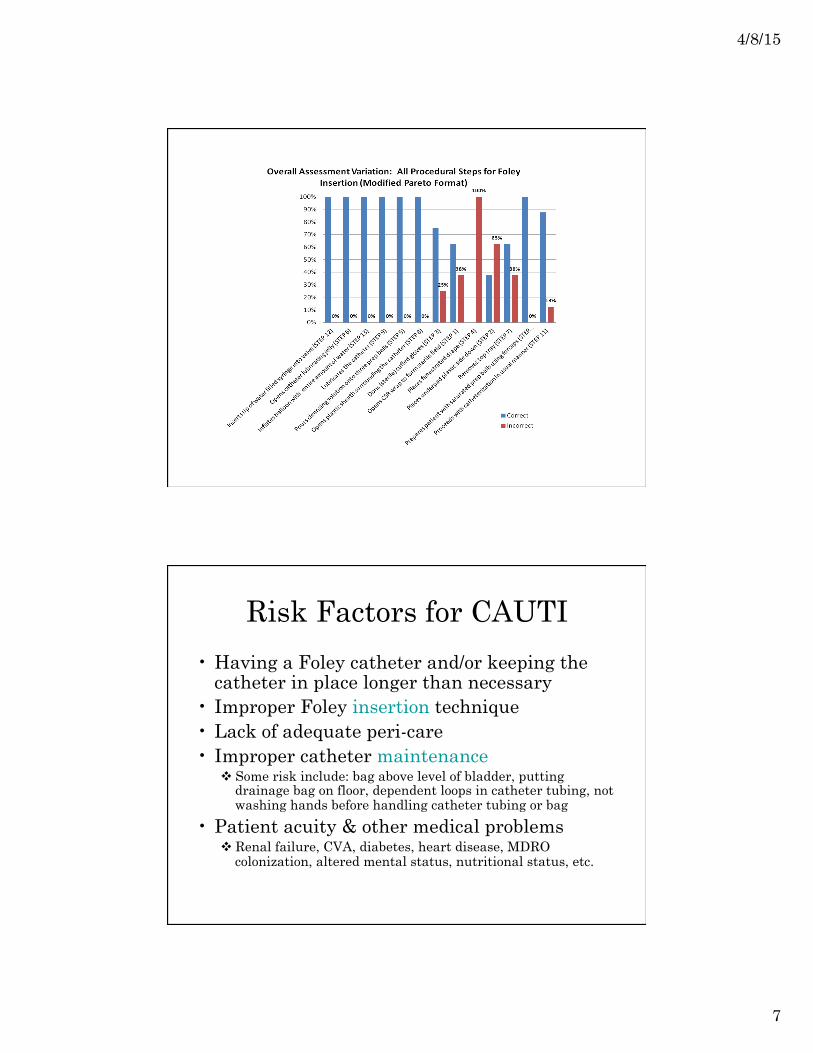
Foley Insertion Assessment Table 1: Foley Inser0on Steps per Direc0ons for Use (DFU) Correct Incorrect
Opens CSR wrap to form sterile field (STEP 1) 63% 38% Places underpad plas@c side down (STEP 2) 38% 63% Dons (sterile) cuffed gloves (STEP 3) 75% 25% Places fenestrated drape (STEP 4) 0% 100% Pours cleansing solu@on onto three prep balls (STEP 5) 100% 0% Opens catheter lubrica@ng jelly (STEP 6) 100% 0% Removes top tray (STEP 7) 63% 38% Opens plas@c sheath surrounding the catheter (STEP 8) 100% 0% Lubricates the catheter (STEP 9) 100% 0% Prepares pa@ent with saturated prep balls using forceps (STEP 10) 100% 0% Proceeds with catheteriza@on in usual manner (STEP 11) 88% 13% Inserts @p of water filled syringe into valve (STEP 12) 100% 0% Inflates balloon with en@re amount of water (STEP 13) 100% 0%
4/8/15
7
Risk Factors for CAUTI
• Having a Foley catheter and/or keeping the catheter in place longer than necessary
• Improper Foley insertion technique • Lack of adequate peri-care • Improper catheter maintenance
v Some risk include: bag above level of bladder, putting drainage bag on floor, dependent loops in catheter tubing, not washing hands before handling catheter tubing or bag
• Patient acuity & other medical problems v Renal failure, CVA, diabetes, heart disease, MDRO
colonization, altered mental status, nutritional status, etc.

4/8/15
8
All Years Combined CAUTI
0
1
2Jan-12
Feb-12
Mar-12
Apr-12
May-12
Jun-12
Jul-12
Aug-12
Sep-12
Oct-12
Nov-12
Dec-12
Jan-13
Feb-13
Mar-13
Apr-13
May-13
Jun-13
Jul-13
Aug-13
Sep-13
Oct-13
Nov-13
Dec-13
Jan-14
Feb-14
Mar-14
Apr-14
May-14
Jun-14
Jul-14
Aug-14
Sep-14
Oct-14
Nov-14
Dec-14
Jan-15
Feb-15
Date
Num
ber C
AUTI
Device Utilization
Expected CAUTI
Actual CAUTI
CAUTI originally reported to NHSN in October 2013 was removed after further chart review determined the UTI was present-‐‑on-‐‑admission.
Key Lessons Learned
• Know how your data is being collected and evaluated. BE A STATISTICAL GEEK.
• Know how your data is being used by CMS. • Verify best-practices & staff knowledge. • Check for consistent performance. • Share significant data with medical staff,
front-line clinical staff, and administration. COMMUNICATE & COLLABORATE
• Be proactive. Don’t be the “last to know.” Get ahead of the story. Have your talking points ready!

4/8/15
9
We learned some valuable lessons. If I could go back in time… this is how I wish the conversation had started.
NHSN Definitions
• http://www.cdc.gov/nhsn/pdfs/pscManual/7pscCAUTIcurrent.pdf (modified April 2015)

4/8/15
10
Some CAUTI Resources
• APIC Guide to Preventing CAUTI: http://apic.org/Resource_/EliminationGuideForm/6473ab9b-e75c-457a-8d0f-d57d32bc242b/File/APIC_CAUTI_web_0603.pdf
• CDC CAUTI Toolkit: http://www.cdc.gov/HAI/pdfs/toolkits/CAUTItoolkit_3_10.pdf
• Targeted Assessment for Prevention (TAP): http://www.cdc.gov/hai/prevent/tap.html
• On the CUSP: Stop CAUTI http://www.onthecuspstophai.org/on-the-cuspstop-cauti/
Feel free to contact me about CAUTI
Kim Roberts Infection Control Manager
OCH Regional Medical Center Starkville, Mississippi
(662) 615-2820 [email protected]

4/8/15
11
Thank You
21
For more information contact your state’s QIN-QIO representative:
This material was presented on behalf of atom Alliance, the Quality Innovation Network-Quality Improvement Organization (QIN-QIO), coordinated by Qsource for Tennessee, Kentucky, Indiana, Mississippi and Alabama under a contract with the Centers for Medicare & Medicaid Services (CMS), a federal agency of the U.S. Department of Health and Human Services. Content does not necessarily reflect CMS policy. 15.SS.MS.02.001E