ce/cme vÂÎp cognitive screening tools -...
TRANSCRIPT
CE/CME VÂÎPA S S O C I A T I O N
C M E
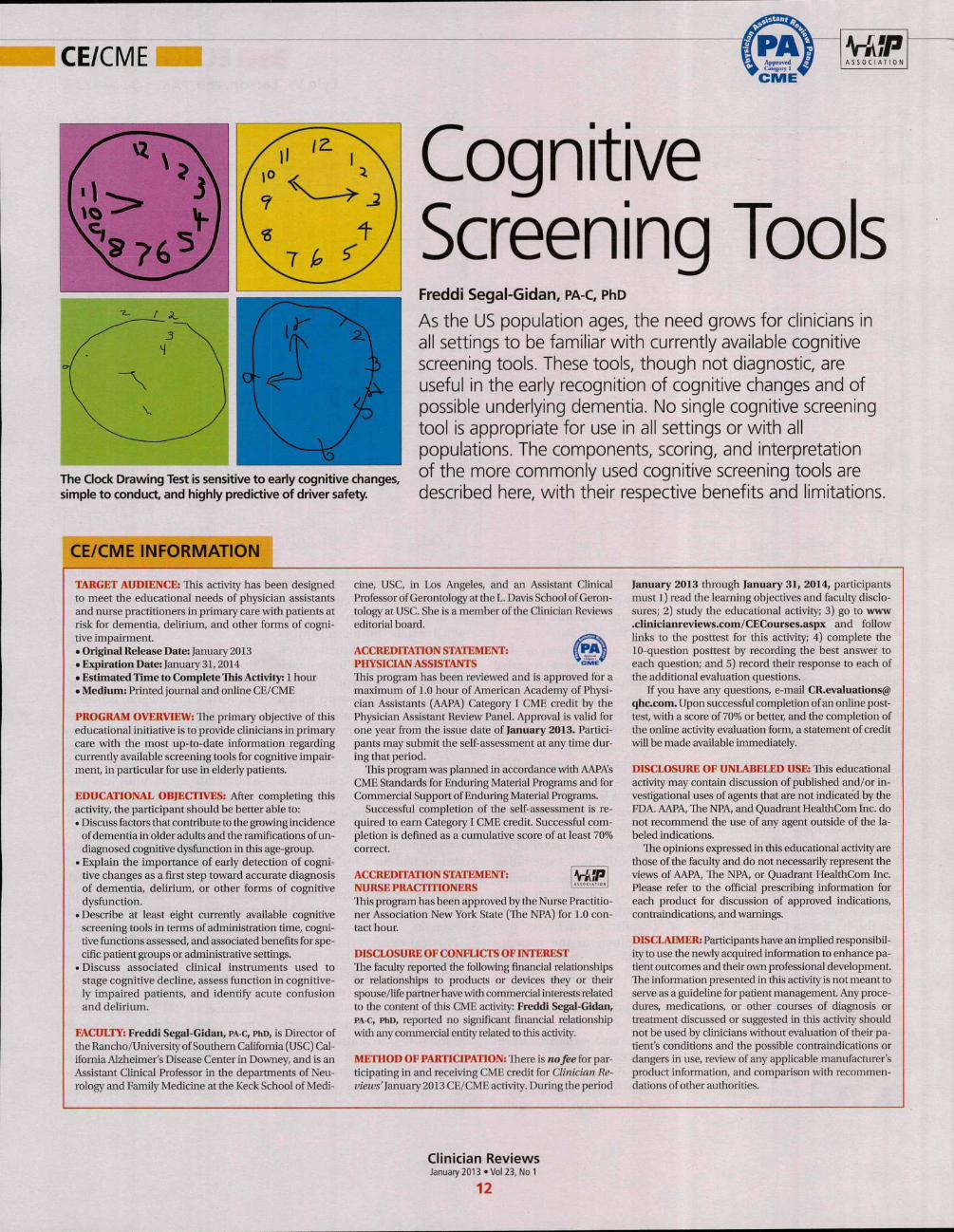
The Clock Drawing Test is sensitive to early cognitive changes,
simple to conduct, and highly predictive of driver safety.
CognitiveScreening ToolsFreddi Segai-Gidan, PA-C, PhD
As the US population ages, the need grows for clinicians in
all settings to be familiar with currently available cognitive
screening tools. These tools, though not diagnostic, are
useful in the early recognition of cognitive changes and of
possible underlying dementia. No single cognitive screening
tool is appropriate for use in all settings or with all
populations. The components, scoring, and interpretation
of the more commonly used cognitive screening tools are
described here, with their respective benefits and limitations.
CE/CME INFORMATION
TARGET AUDIENCE: lhis activity has been designed
to meet the educational needs of physician assistants
and nurse practitioners in primary care with patients at
risk for dementia, delirium, and other forms of cogni-
tive impairment.
• Original Release Date: January 2013
• Expiration Date: January 31, 2014
• Estimated Time to Complete This Activity: 1 hour
• Medium: Printed journal and online CE/CME
PROGRAM OVERVIEW: The primary objective of this
educational initiative is to provide clinicians in primary
care vAxh the most up-to-date information regarding
currently available screening tools for cognitive impair-
ment, in particular for use in elderly patients.
EDUCATIONAL OBJECTIVES: After completing this
activity, the participant should be better able to:
• Discuss factors that contribute to the growing incidence
of dementia in older adults and the ramifications of un-
diagnosed cognitive dysfunction in this age-group.
• Explain the importance of early detection of cogni-
tive changes as a first step toward accurate diagnosis
of dementia, delirium, or other forms of cognitive
dysfunction.
• Describe at least eight currently available cognitive
screening tools in terms of administration time, cogni-
tive functions assessed, and associated benefits for spe-
cific patient groups or administrative settings.
• Discuss associated clinical instruments used to
stage cognitive decline, assess function in cognitive-
ly impaired patients, and identify acute confusion
and delirium.
FACULTY: Ereddi Segal-Gidan, PA-C, PhD, is Director of
the Rancho/University of Southern California (USC) Cal-
ifornia Alzheimer's Disease Center in Downey, and is an
Assistant Clinical Professor in the departments of Neu-
rology and Family Medicine at the Keck School of Medi-
cine, USC, in Los Angeles, and an Assistant CUnical
Professor of Cerontology at the L. Davis School of Geron-
tology at USC. She is a member of the Clinician Reviews
editorial board.
ACCREDITATION STATEMENT:
PHYSICL\N ASSISTANTS
This program has been reviewed and is approved for a
maximum of 1.0 hour of American Academy of Physi-
cian Assistants (AAPA) Category I CME credit by the
Physician Assistant Review Panel. Approval is valid for
one year from the issue date of January 2013. Partici-
pants may submit the self-assessment at any time dur-
ing that period.
This program was planned in accordance with AAPA's
CME Standards for Enduring Material Programs and for
Commercial Support of Enduring Material Programs.
Successful completion of the self-assessment is re-
quired to earn Category I CME credit. Successful com-
pletion is deñned as a cumulative score of at least 70%
correct.
ACCREDITATION STATEMENT:
NURSE PRACTITIONERS
This program has been approved by the Nurse Practitio-
ner Association New York State (The NPA) for 1.0 con-
tact hour.
DISCLOSURE OF CONFLICTS OF INTEREST
The faculty reported the following financial relationships
or relationships to products or devices they or their
spouse/life parmer have with commercial interests related
to the content of this CME activity: Freddi Segal-Gidan,
PA-C, PhD, reported no significant financial relationship
with any commercial entity related to this activity.
METHOD OF PARTICIPATION: There is no fee for par
ticipating in and receiving CME credit for Clinician Re-
views'January 2013 CE/CME activity. Duringthe period
January 2013 through January 31, 2014, participants
must 1) read the learning objectives and faculty disclo-
sures; 2) study the educational activity; 3) go to www
.clinicianreviews.com/CECourses.aspx and follow
links to the posttest for this activity; 4) complete the
10-question posttest by recording the best answer to
each question; and 5) record their response to each of
the additional evaluation questions.
If you have any questions, e-mail CR.evaluations@
qhc.com. Upon successful completion ofan online post-
test, with a score of 70% or better, and the completion of
the online activity evaluation form, a statement of credit
will be made available immediately.
DISCLOSURE OF UNLABELED USE: This educational
activity may contain discussion of published and/or in-
vestigational uses of agents that are not indicated by the
FDA. AAPA, The NPA, and Quadrant HealthCom Inc. do
not recommend the use of any agent outside of the la-
beled indications.
The opinions expressed in this educational activity are
those of the faculty and do not necessarily represent the
views of AAPA, The NPA, or Quadrant HealthCom Inc.
Please refer to the official prescribing information for
each product for discussion of approved indications,
contraindications, and warnings.
DISCLAIMER: Participants have an implied responsibil-
ity to use the newly acquired information to enhance pa-
tient outcomes and their own professional development.
The information presented in this activity is not meant to
serve as a guideline for patient management. Any proce-
dures, medications, or other courses of diagnosis or
tieatment discussed or suggested in this activity should
not be used by clinicians without evaluation of their pa-
tient's conditions and the possible contraindications or
dangers in use, review of any applicable manufacturer's
product information, and comparison with recommen-
dations of other authorities.
Clinician ReviewsJanuary 2013 • Vol 23, No 1
12

CE/CME
As our elderly populationcontinues to grow, theissues of screening forcognitive impairment
and early detection of dementiaare becoming increasingly im-portant. Cognitive impairment,particularly in individuals wholive alone, contributes to loss ofindependence, decreased qual-ity of life, and increased healthcare costs.' There are seriousand costly implications of un-recognized dementia, includingdelayed treatment of reversibleconditions, medication noncom-pliance for comorbid conditions,inaccurate and unreliable report-ing by patients, safety concerns,potential catastrophes, and in-creased risk for victimization.
Clinicians in all settings canexpect to care for increasingnumbers of older adults—manywith various degrees of cogni-tive difficulties. Such problems,especially if undetected, can sig-nificantly impact the ongoingmanagement of both acute andchronic medical problems. Inprimary care settings, it has beenreported, between 50% and 65%
>PRIMARYPOINT
L
Cognitive changes may herald early
dementia (eg, Alzheimer's disease) or
functional decline, or reveal an increased
risk for delirium.
of patients found to have cogni-tive deficits meeting the criteriafor dementia did not have a diag-nosis of dementia noted in theirmedical record.^
The annual Wellness examina-tion provided for under the Pa-tient Protection and AffordableCare Act-̂ (PPACA) for Medicare
Freddi Segal-Gidan is Director of
the Rancho/University of Southern
California (USC) California Alzheim-
er's Disease Center in Downey, and is
an Assistant Clinical Professor in the
departments of Neurology and Fam-
ily Medicine at the Keck School of
Medicine, USC, in Los Angeles, and an
Assistant Clinical Professor of Geron-
tology at the L. Davis School of Geron-
tology at USC. She is a member of the
Clinician Reviews editorial board.
beneficiaries is required to in-clude an assessment of cogni-tive function,"" but the Centers forMedicare and Medicaid (CMS)have not, to date, recommendedany specific screening instru-ment; examiners are expected tobase their assessment on obser-vation and reports from the pa-tient and other informants.^
WHY DO TESTING?The purpose of cognitive screen-ing tests is to aid the clinicianin early detection of cognitivechange as a first step toward ac-curate diagnosis—a process thatrequires further assessment.Such changes may herald thebeginning of a dementia, suchas Alzheimer's disease, or mayindicate an increased risk fordelirium, such as in the postop-erative setting,'' or functional de-cline with accompanying safetyconcerns.^ Early identificationof cognitive changes provides anopportunity for case finding, cri-sis avoidance, and identificationof patients for earlier interven-tion and management, includ-ing a discussion of goals with the
patient, and assur-ance that advancedirectives are com-plete and accurate.
It is well docu-mented that de-mentia remainsunderrecognized
and may indeed be the "silent ep-idemic" of this century.^ Currentestimates are that the incidenceof new cases of Alzheimer's dis-ease will double by 2050.̂ Addi-tionally, improvement in strokesurvival rates means that therewill likely be increases in vascu-lar and poststroke dementia, asone-third of stroke patients havebeen found to develop a progres-sive dementia.'"
The early detection of cogni-tive change offers benefits forboth patients and providers. Ifearly detection leads to a diag-nosis of dementia (regardless ofetiology), this can provide an ex-planation to patients and fami-lies regarding recent changes in
TABLE 1
Comparison of Sensitivity and Specificity of CognitiveScreening Tools for Detection of Dementia^''^^
Screening tool
Mini-Mental State Exam (MMSE)
Modified Mini-Mental StateExam (3MS)
Mini-Cog
Montreal Cognitive Assessment(MoCA)
Saint Louis University MentalStatus (SLUMS)
General Practitioner Assessmentof Cognition (GPCOG)
Memory Impairment Screen (MIS)
Clock Drawing Test
Sensitivity
69% - 9 1 %
83%-94%
76% - 99%
100%
92%-95%
82%
80%
88%
Specificity
87% - 99%
85% - 90%
8 9 % - 9 3 %
87%
76% - 8 1 %
83%
96%
71%Sources: Cullen et al. J Neurol Neurosurg Psychiatr. 2007^''; Smith et al. Can J Psychiatr.
2007^^; Tariq et a\. Am J Geriatr Psychiatry. 2006*; Brodaty et al. i Am Geriatri Soc 2002";
Buschke et al. Neurology. 1999^"; Lessig et al. Int Psychogeriatr. 2008.^'
function, mood, and behavior.A diagnosis of progressive de-mentia (eg, Alzheimer's disease,Lewy body disease, frontotem-poral dementia) provides an op-portunity for early medicationmanagement, review and sim-plification of ongoing chronicdisease management, and pre-vention of problems commonlyassociated with mismanage-ment. More importantly, earlydiagnosis of dementia enablespatients to be more involved inplanning for their own futurecare needs, such as execution ofadvance directives.
Cognitive screening may alsohelp in identification of the at-risk driver or those who shouldundergo further assessment forfitness to drive.'
WHO SHOULD BE SCREENED?There is no clear consensus onwho should undergo cognitivescreening or how frequently itshould be carried out. Screeningshould be targeted at individualswho are at greatest risk for eitherprogressive dementia or deliri-um. Advancing age is a knownrisk factor for dementia, but thereis no agreement on a specificage at which to initiate cognitivescreening. In patients older than80, there is a 25% to 50% preva-lence of dementia,'"'^ thus sug-
gesting that cognitive screeningshould be initiated before thisage. Furthermore, clinicians whoprovide medical care for patientsof advanced age must be increas-ingly attentive to the possiblepresence of cognitive decline.
Individuals with subjectivememory complaints and thosewith a history of depression havebeen identified as being at highrisk for dementia.'^'" The Ameri-can Academy of Neurology rec-ommends cognitive screeningin any patient in whom cogni-tive impairment is suspected.'^This usually occurs when a fam-ily member or other individualclose to the patient (eg, employ-er, friend) becomes concernedabout changes in the patient'sthinking, behavior, or function.Additionally, older individualswho have recently undergonesurgery or been hospitalized area population at high risk for acutecognitive changes and should beconsidered candidates for mentalstatus screening.'"^^^
Another population for whomcognitive screening may be ap-propriate is patients with certainmedical conditions known to beassociated with dementia, as wellas any older person with unex-plained functional decline. Ex-amples of conditions associatedwith cognitive decline include
Clinician ReviewsJanuary 2013 «Vol 23, No 1
13
COGNITIVESCREENINGTOOLSI
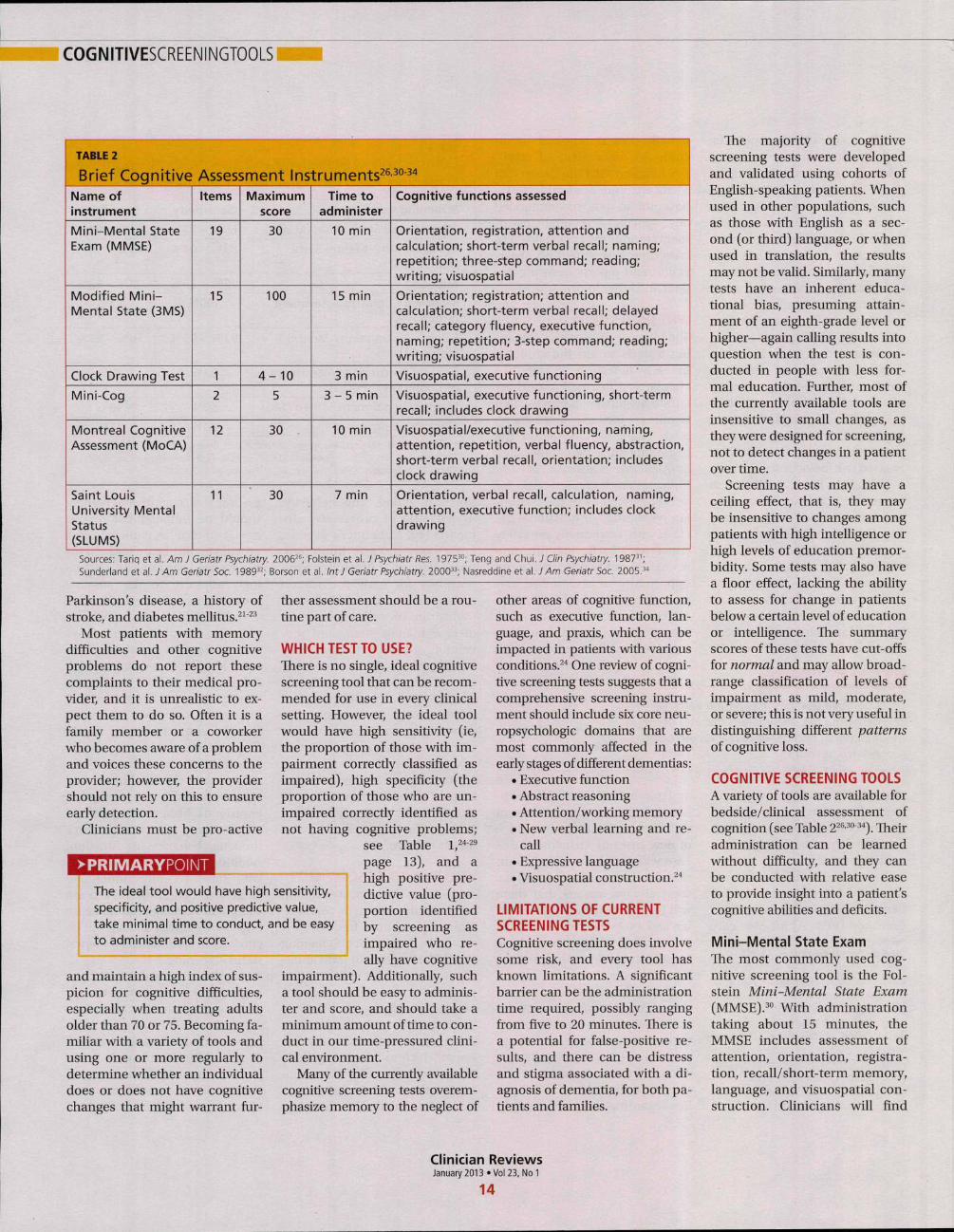
TABLE 2
Brief Cognitive Assessment Instruments^^-^^^''
Name ofinstrument
Mini-Mental StateExam (MMSE)
Modified Mini-Mental State (3MS)
Clock Drawing Test
Mini-Cog
Montreal CognitiveAssessment (MoCA)
Saint LouisUniversity MentalStatus(SLUMS)
Items
19
15
1
2
12
11
Maximumscore
30
100
4 - 10
5
30
30
Time toadminister
10 min
15 min
3 min
3 - 5 min
10 min
7 min
Cognitive functions assessed
Orientation, registration, attention andcalculation; short-term verbal recall; naming;repetition; three-step command; reading;writing; visuospatial
Orientation; registration; attention andcalculation; short-term verbal recall; delayedrecall; category fluency, executive function,naming; repetition; 3-step command; reading;writing; visuospatial
Visuospatial, executive functioning
Visuospatial, executive functioning, short-termrecall; includes clock drawing
Visuospatial/executive functioning, naming,attention, repetition, verbal fluency, abstraction,short-term verbal recall, orientation; includesclock drawing
Orientation, verbal recall, calculation, naming,attention, executive function; includes clockdrawing
Sources: Tariq et al. Am J Geriatr Psychiatry. 2006^''; Folstein et al. i Psychiatr Res. 1975™; Teng and Chui. J Clin Psychiatiy. 1987^';
Sunderland et a\.J Am Geriatr Soc. 1989^ ;̂ Borson et al. IntJ Geriatr Psychiatry. 2000^^; Nasreddine et al. 7 4m Geriatr Soc. 2005.3"
Parkinson's disease, a history ofstroke, and diabetes mellitus.̂ ''̂ -'
Most patients with memorydifficulties and other cognitiveproblems do not report thesecomplaints to their medical pro-vider, and it is unrealistic to ex-pect them to do so. Often it is afamily member or a coworkerwho becomes aware of a problemand voices these concerns to theprovider; however, the providershould not rely on this to ensureearly detection.
Clinicians must be pro-active
>PRIMARYPOINT
The ideal tool would have high sensitivity,specificity, and positive predictive value,take minimal time to conduct, and be easyto administer and score.
and maintain a high index of sus-picion for cognitive difficulties,especially when treating adultsolder than 70 or 75. Becoming fa-miliar v«th a variety of tools andusing one or more regularly todetermine whether an individualdoes or does not have cognitivechanges that might warrant fur-
ther assessment should be a rou-tine part of care.
WHICH TEST TO USE?There is no single, ideal cognitivescreening tool that can be recom-mended for use in every clinicalsetting. However, the ideal toolwould have high sensitivity (ie,the proportion of those with im-pairment correctly classified asimpaired), high specificity (theproportion of those who are un-impaired correctly identified asnot having cognitive problems;
see Table l,̂ ''-̂ ^page 13), and ahigh positive pre-dictive value (pro-portion identifiedby screening asimpaired who re-ally have cognitive
impairment). Additionally, sucha tool should be easy to adminis-ter and score, and should take aminimum amount of time to con-duct in our time-pressured clini-cal environment.
Many of the currently availablecognitive screening tests overem-phasize memory to the neglect of
other areas of cognitive function,such as executive function, lan-guage, and praxis, which can beimpacted in patients with variousconditions. '̂' One review of cogni-tive screening tests suggests that acomprehensive screening instru-ment should include six core neu-ropsychologic domains that aremost commonly affected in theearly stages of different dementias:
• Executive function• Abstract reasoning• Attention/working memory• New verbal learning and re-
call• Expressive language• Visuospatial construction.^*
LIMITATIONS OF CURRENTSCREENING TESTSCognitive screening does involvesome risk, and every tool hasknown limitations. A significantbarrier can be the administrationtime required, possibly rangingfrom five to 20 minutes. There isa potential for false-positive re-sults, and there can be distressand stigma associated with a di-agnosis of dementia, for both pa-tients and families.
The majority of cognitivescreening tests were developedand validated using cohorts ofEnglish-speaking patients. Whenused in other populations, suchas those vwth English as a sec-ond (or third) language, or whenused in translation, the resultsmay not be valid. Similarly, manytests have an inherent educa-tional bias, presuming attain-ment of an eighth-grade level orhigher—again calling results intoquestion when the test is con-ducted in people with less for-mal education. Further, most ofthe currently available tools areinsensitive to small changes, asthey were designed for screening,not to detect changes in a patientover time.
Screening tests may have aceiling effect, that is, they maybe insensitive to changes amongpatients with high intelligence orhigh levels of education premor-bidity. Some tests may also havea fioor effect, lacking the abilityto assess for change in patientsbelow a certain level of educationor intelligence. The summaryscores of these tests have cut-offsfor normal and may allow broad-range classification of levels ofimpairment as mild, moderate,or severe; this is not very useful indistinguishing different patternsof cognitive loss.
COGNITIVE SCREENING TOOLSA variety of tools are available forbedside/clinical assessment ofcognition (see Table 2'^^'^-^). Theiradministration can be learnedwithout difficulty, and they canbe conducted with relative easeto provide insight into a patient'scognitive abilities and deficits.
Mini-Mental State ExamThe most commonly used cog-nitive screening tool is the Fol-stein Mini-Mental State Exam(MMSE).̂ " With administrationtaking about 15 minutes, theMMSE includes assessment ofattention, orientation, registra-tion, recall/short-term memory,language, and visuospatial con-struction. Clinicians will find
Clinician ReviewsJanuary 2013 • Vol 23, No 1
14

CE/CME
this tool most useful in assess-ing the individual with suspect-ed early dementia and to followprogression through the earlyand middle stages of cognitivedecline in those with Alzheim-er's disease and related dement-ing disorders.
The maximum score is 30points, with impairment suspect-ed in suhjects whose score is 25or lower. The MMSE is highly de-pendent on verhal memory, andit does not include any tests ofexecutive function; performancecan he influenced hy educationand cultural background. A for-mula has been developed thattakes age and education into ac-count, allov«ng for correctionof the score" (see Table 3"^''). TheMMSE is currently a proprietarydocument requiring payment forits use.
The Modified Mini-MentalState Exam (3MS)̂ ' expandsupon the MMSE with the addi-tion of items that address remotememory, delayed recall, list gen-eration, and judgment and rea-soning. With a maximum score of100 points, it allows for partiallycorrect responses to be scored.For example, on verbal recall,cuing and choices are provided,with subsequent correct answersawarded partial points (ie, 1 or 2points out of a 3-point maximumscore per recall item). Cognitiveimpairment is defined by a scoreof 85 points or less.
The 3MS may be more sensitivein identification of early demen-fia than is the MMSE. The 3MS'sexpanded item scoring may behelpful in differentiating betweensome ofthe clinical dementia sub-types, such as Alzheimer's versusvascular dementia.-̂ ''
Clock Drawing Test
The Clock Drawing Test (CDT) isperhaps the simplest test to ad-minister.̂ '̂̂ ^ The patient is givena blank sheet of paper and askedto draw a large circle, then to writenumbers inside the circle so that itresembles a face of a clock. Oncethis is completed, the patient is in-structed to "draw the hands on the
clock to read ten past eleven."There are multiple scoring sys-
tems for the CDT,-̂ '22,37 ̂ ^^^^ points
given for accuracy of placement ofthe numbers and the size and po-sition of the hands. Lower scoresgenerally indicate greater impair-ment. The advantages of the CDTare that it is not very threatening, itis very sensitive to changes in ear-ly Alzheimer's disease, and its ad-ministration requires little train-ing.̂ ^ It has also been shovm to behighly predictive of driver safety.̂ ^
The CDT is most appropriatefor screening in busy practicesand other settings (eg, healthfairs) where further evaluationcan be relied upon to identity anyfalse-positive test results.
Mini-Cog Test
The Mini-Cog Test (with instruc-tions available at http://geriatrics.uthscsa.edu/tools/MINICog.pdf ) includes the clock-draw-ing task and a three-word recall,with a simple scoring algorithm.^'Ability to recall all three words, orto recall one or two words withnormal results on the clock test,represents a negative screeningresult for dementia. Conversely,an inability to recall any of thethree words, or ability to recallonly one or two words with an ab-
>PRIMARYPOINT
TABLE 3Formula Correction for MMSE (MMSE Adjusted,or
MMSAdj = Raw MMS - [0.471 x (education - 12)] H- [0.131 x (age - 70)]Example: A 78-year-old patient with 9 years of education
scores 21/30 on MMSE.
MMSAdj = 21 - [0.471 x (9 - 12)] + [0.131 x (78 - 70)]
= 21 -[0.471 x(-3)]-H [0.131 x(8)]
= 21-(-1.413) H-(1.048)
= 21 4- 1.413 + 1.048
= 23.461
Source: Mungas et al. Neurology. 1995.̂
lates easily for use in other lan-guages,33,39
Tbough not diagnostic, these tools detect
early cognitive change, representing a
first step toward accurate diagnosis of
dementia or other impairment.
normal clock test, is considered apositive screen for dementia. TheMini-Cog is a good tool for identi-fication of early dementia, but notuseful for following changes in in-dividuals identified vwth cognitiveimpairment.
The Mini-Cog has been shownto have sensitivity and specific-ity similar to those of the MMSE,but it is much briefer and easier toadminister. It is also less prone tolanguage or ethnic bias, makingit appropriate for patients with awide variety of backgrounds andeducational levels, and it trans-
Montreal CognitiveAssessment
The Montreal Cognitive Assess-ment (MoCA) was originallydesigned as a brief screeninginstrument for mild cognitiveimpairment.̂ "* It is a single-page,30-point test, available in mul-tiple languages (with several ver-sions in some languages) at www.mocatest.org. The MoCA includesassessment of short-term memo-ry, visuospafial ability, executivefunction, attention, concentra-tion, working memory, language,and orientation. A score of 25 or
lower is consideredsubnormal.
By design, theMoCA is useful fordetecting subtledeficits that may be
i missed in patientswho are highly
educated, who score within thenormal range on MMSE (> 25), orwho have prominent executivedysfunction. The test has beenshown to have excellent sensitiv-ity in identification of early/mildcognitive changes and high test-retest reliability, and it is consid-ered an excellent screening toolfor detection of cognitive impair-ment in a busy clinical setting.'"'
Saint Louis UniversityMental StatusThe Saint Louis University Men-tal Status (SLUMS) has also been
shown to have better sensitivitythan the MMSE for early cog-nitive changes.-** This 11-itemtool, with a maximum score of30 points, includes assessmentof seven cognitive domains: ori-entation, recall, attention, cal-culation, fiuency, language, andvisuospatial construction. Thefive-item delayed recall in theSLUMS has been shown to be anexcellent discriminator of thosewith normal cognition ver-sus mild cognitive change. It isavailable for general use with nofee; currently, it is widely usedby the Veterans Administrationsystem.'"
General PractitionerAssessment of Cognition
The General Practitioner Assess-ment of Cognition (GPCOC)̂ ^ isa unique two-part tool that in-cludes questions for the patientand for someone who knows thepatient well ("informant"). Thepatient items include memory/recall, orientation, and visuo-spatial tasks. The six informantquestions ask about recall, lan-guage, and functional abilities.The GPCOG has been shown tohave sensitivity and specificitysimilar to those ofthe MMSE '̂; asits name indicates, it is designedand best suited for screening in afamily medicine or general inter-nal medicine practice.
Memory Impairment Screen
The Memory Impairment Screenuses a four-item mem-
Clinician ReviewsJanuary 2013 • Vol 23, No 1
15
COGNITIVESCREENINGTOOLS
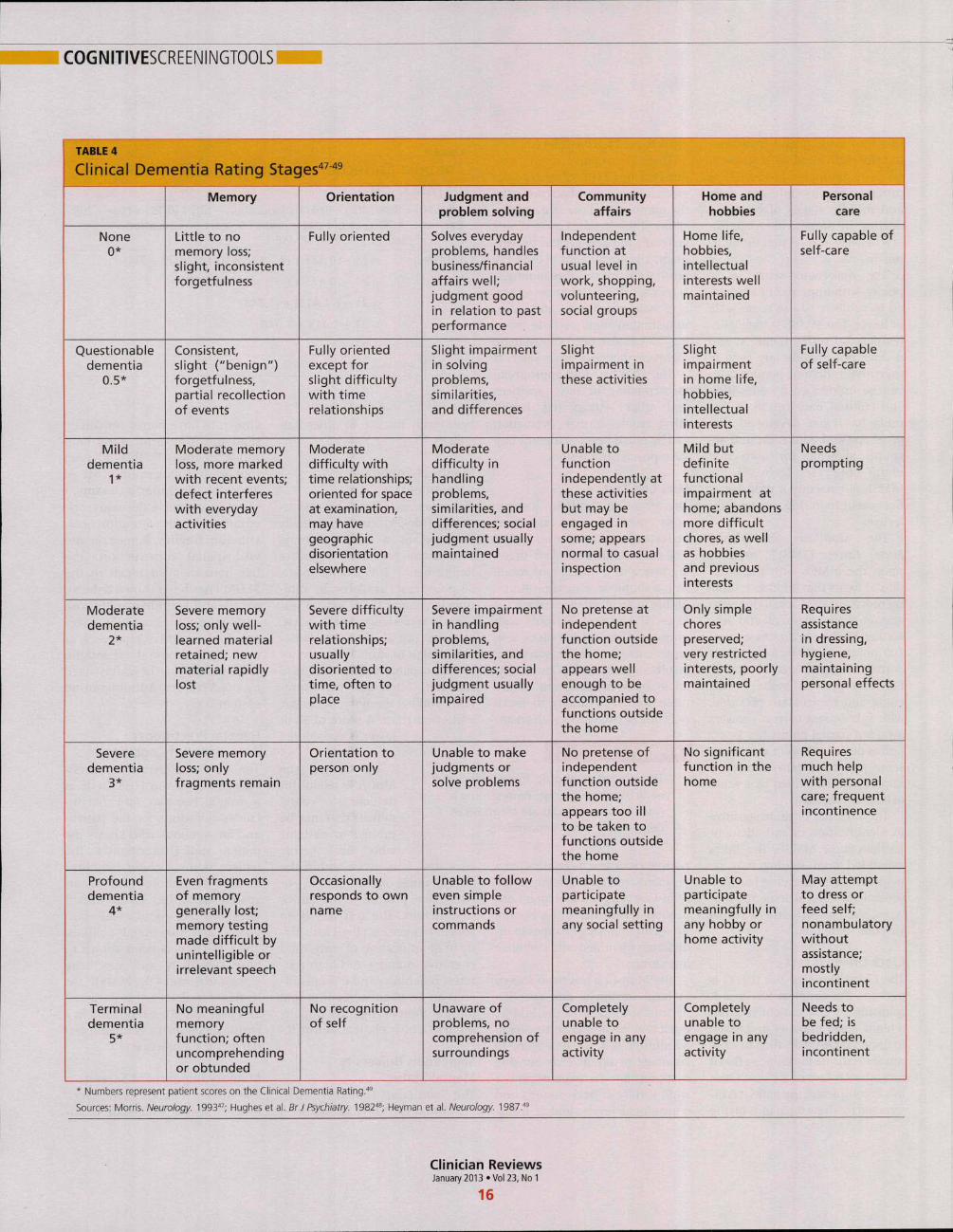
TABLE 4
Clinical Dementia Rating Stac
None0*
Questionabledementia
0.5*
Milddementia
1*
Moderate
dementia2*
Severedementia
3*
Profounddementia
4*
Terminaldementia
5*
Memory
Little to nomemory loss;slight, inconsistent
forgetfulness
Consistent,slight ("benign")
forgetfulness.partial recollectionof events
Moderate memory
loss, more markedwith recent events;defect interferes
with everydayactivities
Severe memoryloss; only well-learned materialretained; new
material rapidlylost
Severe memoryloss; only
fragments remain
Even fragmentsof memorygenerally lost;memory testingmade difficult byunintelligible orirrelevant speech
No meaningfulmemoryfunction; oftenuncomprehendingor obtunded
1^547-49
Orientation
Fully oriented
Fully oriented
except forslight difficultywith timerelationships
Moderate
difficulty withtime relationships;
oriented for spaceat examination.may havegeographicdisorientation
elsewhere
Severe difficultywith timerelationships;usually
disoriented totime, often to
place
Orientation toperson only
Occasionallyresponds to ownname
No recognition
of self
Judgment andproblem solving
Solves everydayproblems, handlesbusiness/financial
affairs well;judgment good
in relation to pastperformance
Slight impairment
in solvingproblems.similarities.and differences
Moderate
difficulty inhandling
problems.similarities, anddifferences; socialjudgment usuallymaintained
Severe impairmentin handlingproblems.similarities, and
differences; socialjudgment usually
impaired
Unable to makejudgments orsolve problems
Unable to followeven simpleinstructions or
commands
Unaware ofproblems, nocomprehension of
surroundings
Communityaffairs
Independentfunction at
usual level inwork, shopping.
volunteering.
social groups
Slight
impairment inthese activities
Unable tofunctionindependently at
these activitiesbut may be
engaged insome; appears
normal to casualinspection
No pretense at
independentfunction outsidethe home;
appears wellenough to beaccompanied to
functions outsidethe home
No pretense ofindependent
function outside
the home;appears too illto be taken tofunctions outsidethe home
Unable to
participatemeaningfully inany social setting
Completely
unable toengage in any
activity
Home andhobbies
Home life.hobbies.
intellectualinterests well
maintained
Slight
impairmentin home life.
hobbies.intellectual
interests
Mild but
definitefunctional
impairment athome; abandons
more difficultchores, as well
as hobbiesand previous
interests
Only simple
chorespreserved;very restricted
interests, poorlymaintained
No significant
function in the
home
Unable to
participatemeaningfully inany hobby or
home activity
Completely
unable toengage in any
activity
Personalcare
Fully capable ofself-care
Fully capable
of self-care
Needs
prompting
Requires
assistancein dressing.hygiene.
maintainingpersonal effects
Requires
much help
with personal
care; frequentincontinence
May attempt
to dress orfeed self;nonambulatory
without
assistance;
mostlyincontinent
Needs to
be fed; isbedridden.
incontinent
* Numbers represent patient scores on the Clinical Dementia Rating."'
Sources: Morris. Neurology. 1993"'; Hughes et al. BrJ Psychiatry. 1982*; Heyman et al. Neurology 1987.""
Clinician ReviewsJanuary 2013 «Vol 23, No 1
16

CE/CME
TABLE 5
Comparison of Cognitive Screening Tool Scores byImpairment Level/Stage^O'̂ ^^^^^
Screening tool
Mini-Mental State Exam (MMSE)
Modified Mini-Mental State Exam (3MS)
Montreal Cognitive Assessment (MoCA)
Clinical Dementia Rating (CDR)
Preclinical
26-30
92-100
22-26
0.5
Mild/early
19-25
80-91
16-21
1.0
Moderate/middle
1 0 - 18
61 - 7 9
5 - 1 5
2.0
Severe/late
< 10
<61
< 5
3.0Sources: Folstein et al. 7 Psychiatr Res. 1975^°; Teng and Chui. J Clin Psychiatry. 1987^'; Nasreddine et al. 7 Am Geriatr Soc. 20053"; Morris.
Neurology. 1993."'
ory recall with simple scoring of0 to 8, based on the formula: 2x[the number recalled spontane-ously) + (the number recalledwith cuing). It takes less thanfive minutes to administer, mak-ing it a useful tool to screen forsuspected memory problems ina busy setting, such as an emer-gency room. However, the solereliance on memory, withoutscreening for any other areas ofcognition (especially executivefunction or visuospatial copying),significantly limits the usefulnessof the MIS as a general cognitivescreening tool.
Telephone Interview forCognitive StatusThe cognitive screening instru-ments described thus far wereall designed to be administeredin person in a medical setting(office, clinic, or hospital). The11-item Telephone Interview forCognitive Status (TICS)''̂ wasdeveloped as a brief (taking lessthan 10 minutes) standardizedtest of cognitive function, spe-cifically suited for situations inwhich in-person screening is notpossible (eg, for patients whoare unable to appear in personfor clinical follow-up).''̂ '"' Themodified TICS (TICS-M), whichincludes 13 items, has beenshown to have less of a ceiling ef-fect than the MMSE.'*'̂ It has alsobeen shown to be a cost-effectivescreening tool for mild cognitiveimpairment."^
ASSOCIATED CLINICALINSTRUMENTSThe Clinical Dementia Rating(CDR) scale is a useful tool for
staging cognitive decline, regard-less of the patient's diagnosis.''^It uses a O-to-5 rating system inwhich 0 is considered normaland 5 represents profound im-pairment/total dependence (seeTable 4,*'« page 16). The CDRrating system addresses threeareas of cognition (memory, ori-entation, judgment) and threeareas of function (community af-fairs, home and hobbies, person-al care). This tool is very helpfulto explain to families where anindividual with cognitive im-pairment is in the course of thedisease, and what to expect andplan for in the future as the con-dition progresses. A compari-son of CDR level and cognitivescreening test scores is presentedin Table 5.3»'3i.34,49
The Functional AssessmentStaging Test (FAST) focuses onthe functional ability of the indi-vidual with cognitive deficits.̂ "It is a 16-item scale with scoresfrom 0 to 7. Included in this toolare subscales addressing themore severely impaired levels as-sociated with advanced dementia(eg, 6: dressing, bathing, toileting;and 7: speech and locomotion).The FAST has been adopted byCMS for use in evaluating nurs-ing home residents and hospicepatients.
Another tool that should befamiliar to clinicians who workwith cognitively impaired indi-viduals is the Confusion Assess-ment Method (CAM).51 The CAMwas developed to aid in identifi-cation and recognition of acuteconfusion and delirium, whichoften occur in older, hospitalizedindividuals. Four features are as-
sessed in five minutes throughobservation and a brief in-personinterview:
(1) Altered mental status frombaseline (acute in onset orfluctuating)
(2) Inattention(3) Disorganized thinking(4) Altered level of conscious-
ness (eg, hyperalert, lethar-gic, somnolent).
Delirium is considered presentif there is evidence of features 1and 2, and either 3 or 4 (or both)."
CONCLUSIONClinicians in all settings need to
become familiar with the use and
interpretation of readily available
instruments for cognitive screen-
ing. None of the tools reviewed is
diagnostic in itself, and no one tool
is appropriate for all patients in all
settings. Familiarity with the com-
ponents of the most commonly
used cognitive screening tools and
associated clinical instruments
will aid the clinician in the appro-
priate use and interpretation of
these to improve clinical care and
outcomes for patients. CR
Happy New Yearfrom Clinician Reviews!
Our CE/CME posttestcan be taken free
or viewed atvvww.clinicianreviews.com/CECourses.aspx
REFERENCES1. Alzheimer's Association. 2012 Alzheimer's
Disease Facts and Figures, www.alz.org/down
loads/facts_figures_2012.pdf. Accessed Decem-
ber 11, 2012.
2. Boustani M, Peterson B, Hanson L, et ai.
Screening for dementia in primary care: a sum-
mary of the evidence for the US Preventive Ser-
vices Task Force. Ann Intern Med. 2003;138
(11);927-937.
3. Patient Protection and Affordable Care Act of
2010, HR 3590,111th Cong, Public Law 111-148.
www.gpo.gov/fdsys/pkg/PLAW-111publ148/
pdf/PLAW-111 publ148.pdf. Accessed December
11,2012.
4. Congressional Research Service. Medicare
provisions in PPACA (P. L. 111-148; 2010). http://
assets.opencrs.com/rpts/1 M48_20100421.pdf.
Accessed December 11, 2012.
5. Medicarelnteractive.org. Annual Wellness
visit, www.medicareinteractive.org/page2.php
?topic=counselor&page=script&script_id=1717.
Accessed December 11, 2012.
6. Marcantonio ER, Goldman L, Mangione CM,
et aL A clinical prediction rule for delirium after
elective noncardiac surgery. JAMA. 1994;271
(2):134-149.
7 Molnar FJ, Patel A, Marshall SC, et al. Clinical
utility of office-based cognitive predictors of fit-
ness to drive in persons with dementia: a sys-
tematic review. J Am Geriatr Soc. 2006;54(12):
1809-1824.
8. Chodosh J, Petitti DB, Elliott M, et aL Physician
recognition of cognitive impairment: evaluating
the need for improvement. J Am Geriatr Soc.
2004;52(7):1051-1059.
9. Hebert LE, Beckett LA, Scherr PA, Evans DA.
Annual incidence of Alzheimer disease in the
United States projected to the years 2000
through 2050. Alzheimer Dis Assoc Disord.
2001;15(4):169-73.
10. Hénon H, Durieu I, Guerouaou D, etal. Post-
stroke dementia: incidence and relationship to
prestroke cognitive decline. Neurology 2001;57
(7):1216-1222.
11. Plassman BL, Langa KM, Fisher GG, et aL
Prevalence of dementia in the United States: the
aging, demographics, and memory study. A/eu-
roepidem/o/ogy. 2007;29(1-2):125-132.
12. Fitzpatnck AL, Kuller LH, Ives DG, et al. Inci-
dence and prevalence of dementia in the Cardio-
vascular Health Study. J Am Geriatr Soc. 2004;
52(2):195-204.
13. Reisberg B, Gauthrie S. Current evidence for
subjective cognitive impairment (SCI) as the pre-
mild cognitive impairment (MCI) stage of subse-
quently manifest Alzheimer's disease. Int Psy-
chogeriatr. 2008;20(1):1-16.
14. Ownby RL, Crocco E, Acevedo A, et al.
Depression and risk for Alzheimer disease: sys-
tematic review, meta-analysis, and metaregres-
sion analysis. Arch Gen Psychiatry. 2006;63(5):
530-538.
15. Petersen RC, Stevens JC, Ganguli M, et al.
Practice parameter: early detection of dementia:
mild cognitive impairment (an evidence-based
review): Report of the Quality Standards Sub-
committee of the American Academy of Neurol-
ogy. Neurology 2001;55(9):1133-1142.
16. Demeure MJ, Fain MJ. The elderly surgical
patient and postoperative delirium [published
correct ion appears in J Am Coll Surg.
2007;204(1):191j. i / i m Coll Surg. 2006;203(5):
752-757.
17. Ehlenbach WJ, Hough CL, Crane PK, et al.
Association between acute care and critical ill-
ness hospitalization and cognitive function in
older adults, JAMA. 2010;303(8):763-770.
18. Terrando N, Brzezinski M, Degos V, et al.
Perioperative cognitive decline in the aging pop-
ulation. Mayo Clin Proc 2011;86(9):885-893.
19. Avidan MS, Evers AS. Review of clinical evi-
dence for persistent cognitive decline or inci-
Clinician ReviewsJanuary 2013 • Vol 23, No 1
17
COGNITIVESCREENINGTOOLSI
dent dementia attributable to surgery or gen-
eral anesthesia. J Alzheimers Dis. 2011;24(2):
201-216.
20. Wilson RS, Hebert LE, Scherr PA, et al.
Cognitive decline after hospitalization in a
community population of older persons. Neu-
rology. 2012;78(13):950-956,
21. Milne A, Culverwell A, Guss R, et al.
Screening for dementia in primary care: a
review of the use, efficacy and quality of mea-
sures. Int Psychogeriatr. 2008;20(5):911-926.
22. Chou KL, Amick MM, Brandt J, et al; Par-
kinson Study Group Cognitive/Psychiatric
Working Group. A recommended scale for
cognitive screening in clinical trials of Parkin-
son's disease. Mov Disord. 2010;25(15):2501-
2507.
23. Murthy SB, Jawaid A, Schulz PE. Diabetes
mellitus and dementia: advocating an annual
cognitive screening in patients with diabetes
mellitus. J Am Geriatr Soc. 2008;B6(10):
1976-1977.
24. Cullen B, O'Neill B, Evans JJ, et al. A review
of screening tests for cognitive impairment.
J Neurol Neurosurg Psychiatry. 2007;78(8):
790-799.
25. Smith T, Gildeh N, Holmes C. The Mon-
treal Cognitive Assessment: validity and utility
in a memory clinic setting. Can J Psychiatr.
2007;52 (5):329-332.
26. Tariq SH, Tumosa N, Chibnall JT, et al.
Comparison of the Saint Louis university men-
tal status examination and the mini-mental
state examination for detecting dementia and
mild neurocognitive disorder: a pilot study.
y. 2006;14(11):900-910.
27. Brodaty H, Pond D, Kemp NM, et al. The
GPCOG: a new screening test for dementia
designed for general practice. J Am Geriatr
Soc. 2002;50{3):530-534.
28. Buschke H, Kulansky G, Katz M, et al.
Screening for dementia with the memory
impairment screen. Neurology. 1999;52(2):
231-238.
29. Lessig MC, Scanlan JM, Nazemi H, Borson
S, Time that tells: critical clock-drawing errors
for dementia screening. Int Psychogeriatr.
2008; 20(3):459-470.
30. Folstein MF, Folstein SE, McHugh PR. Mini-
mental state: a practical tool for grading the
cognitive state of patients for the clinician.
J Psychiatr Res. 1975;12(3):189-198.
31. Teng EL, Chui HC. The Modified Mini-Men-
tal State {3MS) examination. J Clin Psychiatry
1987;48(8):314-318.
32. Sunderland T, Hill JL, Mellow AM, et aL
Clock drawing in Alzheimer's disease. A novel
measure of dementia severity. J Am Geriatr
Soc. 1989;37(8):725-729.
33. Borson S, Scanlan J, Brush M, et al. The
Mini-Cog: a cognitive 'vital signs' measure for
dementia screening in multi-lingual elderly. Int
J Geriatr Psychiatry 2000;15{11):1021-1027.
34. Nasreddine ZS, Phillips NA, Bédirian V, et al.
The Montreal Cognitive Assessment, MoCA: a
brief screening tool for mild cognitive impair-
ment. J/\m Geriatr Soc. 2005;53(4):695-699.
35. Mungas D, Marshall SC, Weldon M, et al.
Age and education correction of the Mini-
Mental State Examination for English- and
Spanish-speaking elderly. Neurology 1996;46
{3):700-706.
36. Grace J, Nadler JD, White DA, et al. Folstein
vs modified Mini-Mental State Examination in
geriatric stroke: stability, validity, and screening
utility. Arch Neurol. 1995;52(5):477-484.
37. Shulman Kl, Gold DP, Cohen CA, Zucchero
CA. Clock-drawing and dementia in the com-
munity: a longitudinal study. IntJ Geriatr Psy-
chiatry 1993;8(6):487-496.
38. Diegelman NM, Gilbertson AD, Moore JL,
et al. Validity of the Clock Drawing Test in pre-
dicting reports of driving problems in the
elderly. BMC Geriatr. 2004:4:10.
39. Borson S, Scanlan JM, Watanabe J, et al.
Simplifying detection of cognitive impairment:
comparison of the Mini-Cog and Mini-Mental
State Examination in a multiethnic sample. J
Am Geriatr Soc. 2005;53(5):871-874.
40. Harkness K, Demers C, Heckman GA,
McKelvie RS. Screening for cognitive deficits
using the Montreal Cognitive Assessment Tool
in outpatients > 65 years of age with heart
failure [published correction appears in Am J
Cardiol. 2012;109(10):1537]. Am J Cardiol.
2011,107(8): 1203-1207.
41. Cruz-Oliver DM, Malmstrom TK, Allen CM,
et al. The Veterans Affairs Saint Louis Univer-
sity mental status exam (SLUMS exam) and the
Mini-mental status exam as predictors of
mortality and institutionalization. J Nutr
Health Aging. 2012;16(7):636-641.
42. Brandt J, Spencer M, Eolstein M. The Tele-
phone Interview for Cognitive Status. Neuro-
psychiatry Neuropsychol Behavioral Neurol.
1988, 1(2):111-117.
43. Welsh KA, Breitner JCS, Magruder-Habib
KM. Detection of dementia in the elderly
using Telephone Screening of Cognitive Sta-
tus. Neuropsychiatry Neuropsychol Behav
Neurol. 1993; 6:103-110.
44. Plassman BL, Newman TT, Welsh KA, et al.
Properties of the Telephone Interview for Cog-
nitive Status: application in epidemiological
and longitudinal studies. Neuropsychiatry
Neuropsychol Behav Neurol. 1994;7(3):235-
241.
45. de Jager CA, Budge MM, Clarke R. Utility
of TICS-M for the assessment of cognitive
function in oider adults. Int J Geriatr Psychia-
try 2003;18(4):318-24.
46. Cook SE, Marsiske M, McCoy KJ. The use
of the Modified Telephone Interview for Cog-
nitive Status (TICS-M) in the detection of
amnestic mild cognitive impairment. J Geriatr
Psychiatry Neurol. 2009;22(2):103-109.
47. Morris JC. The Clinical Dementia Rating
(CDR): current version and scoring rules. Neu-
rology 1993;43(11):2412-2414.
48. Hughes CP, Berg L, Danziger WL, et al. A
new clinical scale for the staging of dementia.
Br J Psychiatry 1982;140:566-572.
49. Heyman A, Wilkinson WE, Hurwitz BJ, et
al. Early-onset Alzheimer's disease: clinical
predictors of institutionalization and death.
Neurology 1987;37(6):980-984.
50. Reisberg B. Functional assessment staging
(FAST). Psychopharmacol Bull. 1988;24(4):
653-659.
51. Inouye SK, van Dyck CH, Alessi CA, et al.
Clarifying confusion: the Confusion Assess-
ment Method: a new method for detecting
delirium. Ann Intern Med. 1990;113(12):941-
948.
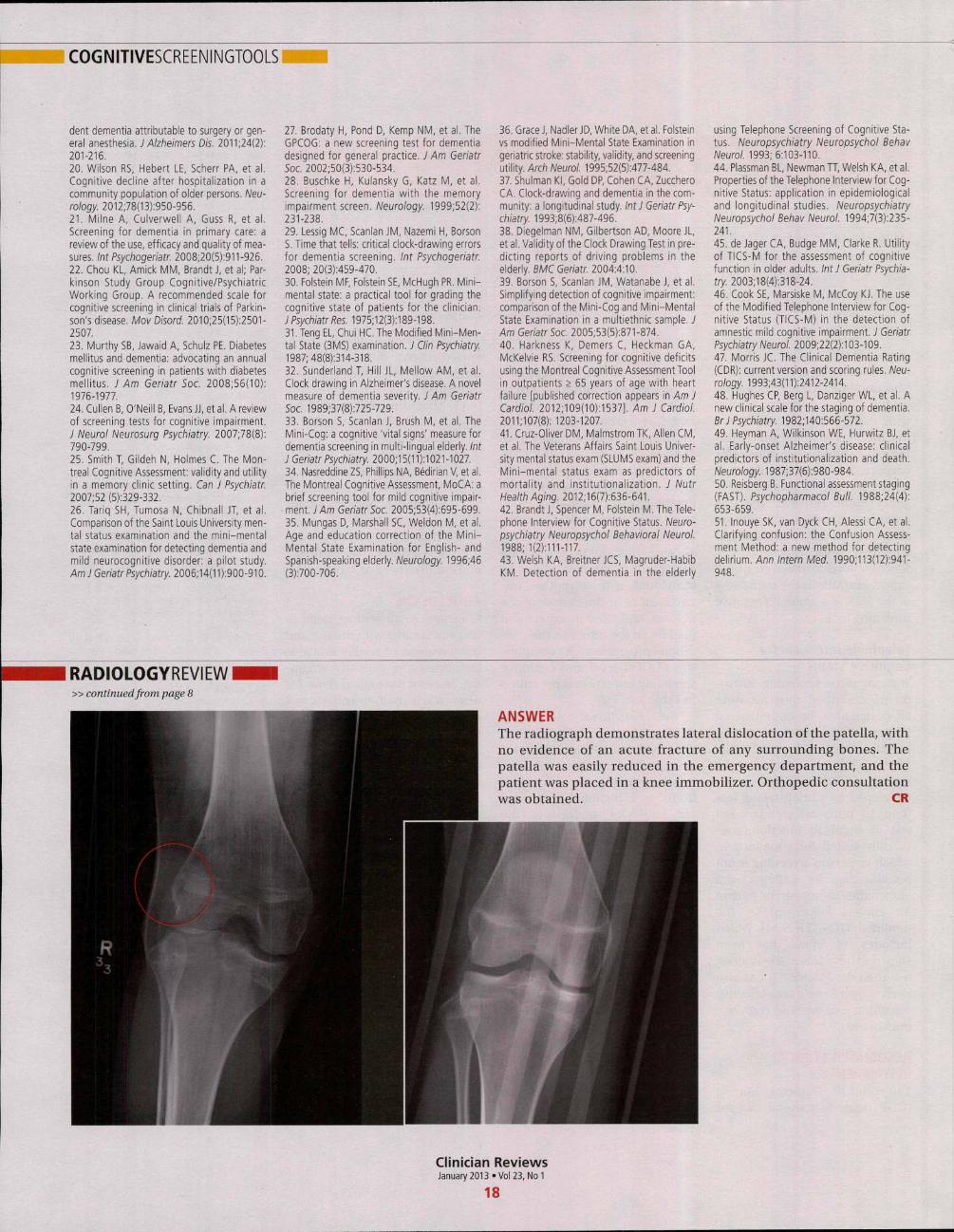
RADIOLOGYREVIEW» continued from page 8
ANSWERThe radiograph demonstrates lateral dislocation ofthe patella, with
no evidence of an acute fracture of any surrounding bones. The
patella was easily reduced in the emergency department, and the
patient was placed in a knee immobilizes Orthopedic consultation
was obtained. CR
Clinician ReviewsJanuary 2013 «Vol 23, No 1
18
Copyright of Clinician Reviews is the property of Quadrant HealthCom Inc. and its content may not be copied
or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission.
However, users may print, download, or email articles for individual use.