cellular degeneration and ageing susan rutherford and sarah christie
TRANSCRIPT
Cellular Degeneration and Ageing
Susan Rutherford and Sarah Christie

What are the factors affecting cellular ageing and degeneration? (5)
Genetic factors
Diet
Social conditions
Age-related disease
Ageing-induced alterations in cells
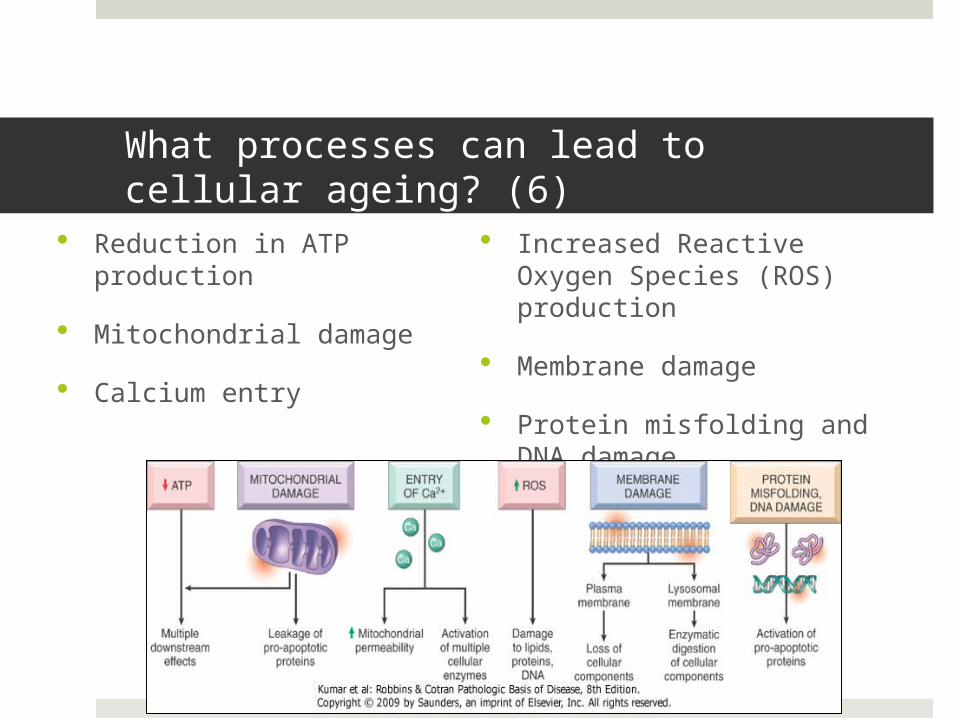
What processes can lead to cellular ageing? (6)
Reduction in ATP production
Mitochondrial damage
Calcium entry
Increased Reactive Oxygen Species (ROS) production
Membrane damage
Protein misfolding and DNA damage

What are the potential outcomes of cellular ageing? (3)
Reduced capacity to function
Reduced capacity to respond to injury
Cell death Apoptosis Necrosis

What 3 changes can lead to cellular ageing?
Decreased cellular replication Due to e.g. p16INK4a, DNA damage
Accumulation of metabolic and genetic changes
E.g. balance between metabolic damage and repair
Reactive Oxygen Species – injures cells by (3):
1. Membrane lipid peroxidation2. Interaction with proteins3. DNA damage
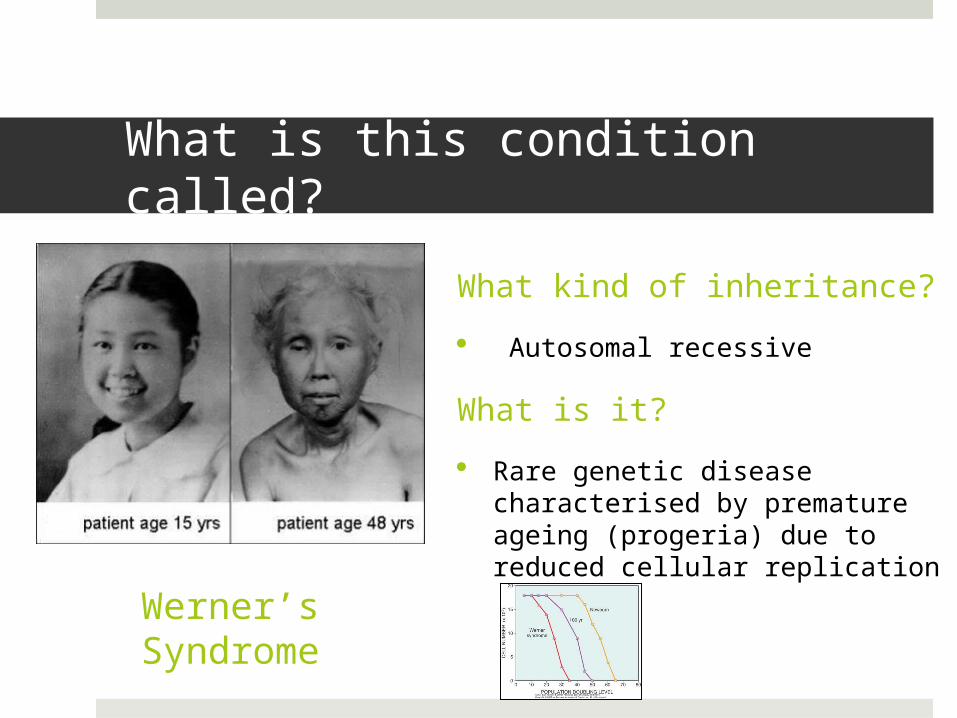
What is this condition called?
What kind of inheritance?
Autosomal recessive
What is it?
Rare genetic disease characterised by premature ageing (progeria) due to reduced cellular replication
Werner’s Syndrome

Friedrich’s Ataxia
Type of inheritance?
Autosomal recessive
What happens?
Spinocerebellar degeneration -> axonal loss and gliosis
What causes it?
GAA trinucleotide repeat leads to expression of frataxin (mitochondrial protein)
Leads to mitochondrial dysfunction -> decreased ATP -> ROS -> DNA damage

Friedrich’s AtaxiaSigns/Symptoms
Muscle weakness in limbs
Loss of co-ordination
Cerebellar signs: nystagmus, fast saccadic eye movements, truncal ataxia, dysarthria. Dysmetria
LMN lesion: absent deep tendon reflexes
Pyramidal: extensor plantar reflexes (UMN symptom), distal weakness
Dorsal column: Loss of vibratory
sensation and proprioception
Often get cardiac involvement e.g. cardiomegaly, hypertrophy, murmurs.
Typical patient presentation:
20s-30s
Slow, progressive staggering/stumbling, frequent falls
Often associated with diabetes
Amylotrophic Lateral Sclerosis
Type of motor neuron disease
Pathogenesis? Genetic mutation – superoxide dismutase-1 enzyme
(SOD1) SOD1 = antioxidant. Protects cells against free radicals
(superoxide) Leads to reduced ability to detoxify cells OR Misfolded proteins -> ER stress -> cell injury Get loss of myelinated fibres in corticospinal tract

Amylotrophic Lateral Sclerosis
Characteristic presentation? Progressive disorder Weakness and or muscle atrophy (UMN/LMN
lesions) Dysphagia, cramping, stiffness of muscles Slurred/nasal speech

Recent diagnosis of motor neuron disease
What should the patient be considering about their care? (3)
Power of attorney
Advanced care planning
Advanced decision to refuse care

Alzheimer’s disease
Most common form of dementia
What might you see on CT? (3) Cortical atrophy (especially temporal) Widened sulci Enlarged ventricles
What are the histological changes seen in AD? (2)
Tau tangles (tau protein) Beta-amyloid plaques

Dementia
If you suspect dementia, what reversible causes would you want to rule out?
Substance abuse Hypothyroidism Space-occupying intracranial lesions Normal pressure hydrocephalus Syphilis Vitamin B12 deficiency Folate deficiency Pellagra
Vitamin B3 deficiency Causes 3Ds: Dementia, diarrhoea, dermatitis (+ death)

Thanks for listening!
Questions?