cellular therapies in acute lymphocytic leukemia
TRANSCRIPT
ELIZABETH J SHPALL, MDHouston, USA
• Professor of Medicine and Chair of Cord Blood Transplant Program, UT MD Anderson Cancer Center
• As a nationally recognized expert in stem cell transplantation, Medical Director of the GMP Cell Therapy Laboratory since 2002, and the Director of the Cord Blood Bank (CBB) at M. D. Anderson Cancer Center since 2004, Dr. Shpall's research covers a range of applications, among them: leukemia, lymphoma treatment, anti-tumor immunity enhancement, and tissue repair. Dr. Shpall’s influence is felt beyond the Texas Medical Center. She is the current vice-president of FACT Netcord, having chaired their Cord Blood Standards Committee since 1999, and she was the founding president and has been a board member of the Foundation Accreditation of Hematopoietic Cell Therapy since 1995.
Cellular Therapy for ALL with Chimeric Antigen Receptors
Elizabeth J. Shpall MD
•

Roadblocks to Successful Cellular Immunotherapy for ALL
PROBLEM
•Targeting
•Expansion ex vivo
•Proliferation in the host
•Persistence
•Effector:Target ratio – create sufficient effector cells for clinical success
SOLUTION
•CAR or TCR
•GMP cell culture
•?Young T cells
•?Memory T cells
•Ideally, there would be an efficacy signal, not just safety, in phase 1
Abbreviations: CAR, chimeric antigen receptor; GMP, good manufacturing practice; TCR, T-cell receptor

Gene Transfer of CARs Eshhar et al; PNAS 1993
Intracytoplasmic
vscFv v
Spacer
Linker
vLvLvLvH
abTcR complexge edzz
Monoclonal antibody
Monoclonal antibody
T or NK Cell
Tumor Tumor
Antigen
CARCAR
CARs combine an antibody binding domain (scFv) that recognizes a desired tumor associated antigen with one or more T-cell receptor signaling endodomains. Forced expression of CAR on the T-cell surface leads to activation of T cells through CD3ζ CD28 and/or CD137.
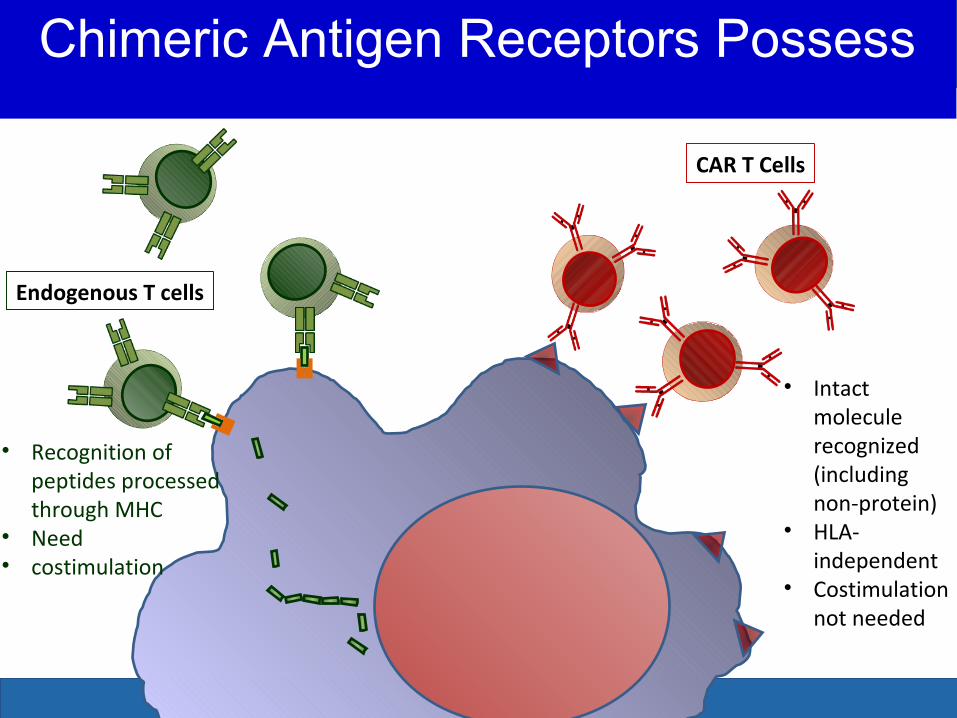
Chimeric Antigen Receptors Possess Advantages Over Endogenous
Receptors
• Intact molecule recognized (including non-protein)
• HLA-independent
• Costimulation not needed
CAR T Cells
Endogenous T cells
• Recognition of peptides processed through MHC
• Need• costimulation
Chimeric Antigen Receptors Possess

Redirecting the Specificity of T cells
• Gene transfer technology is used to stably express CARs on T cells, conferring novel antigen specificity
• Transduction:
– Many retroviral
– Some now using lentiviral
– Non-viral Sleeping Beauty system
• Temporary modification with RNA transfection
• Suicide systems
Viral or nonviral vector
T cell
CD19
Native TCR
Tumor cell
CTL019 cell
Dead tumor cell
Anti-CD19 CAR construct

Evolution of CARs with additional costimulatory domains
Dotti et al. 2009
this is text
this is hhh
ext tt
ext
Classic CARs Sports CARs Muscle CARs
Sadelain, et al. Cancer Discov. 2013

CART19: Chimeric Antigen Receptor T cells against CD19

• Clinical scale up: no feeder cells required
• Expansion >106-fold
• Repertoire preserved
• T cells persist after infusion
• Maintains function and homing of T cells
• Induction of telomerase: minimizing replicative senescence
Levine et al J Immunol 1997; Carroll et al Science 1997; Weng et al Imm Rev 1997; Humeau et al Mol Ther 2004
Properties of Anti-CD3/CD28 Costimulated Expansion System

Sleeping Beauty system to genetically modify T cells to target CD19 via CAR
Transposon (Donor) sequences flanked by inverted repeats are integrated into genome
Transposase (Helper) expression is transient
Plasterk RH, Cell 74(5):781, 1993Ivics Z, et al, Cell 91 (4):501, 1997
Nucleus
Transposase
Transposon
CAR
Cytoplasm
Laurence Cooper Laboratory
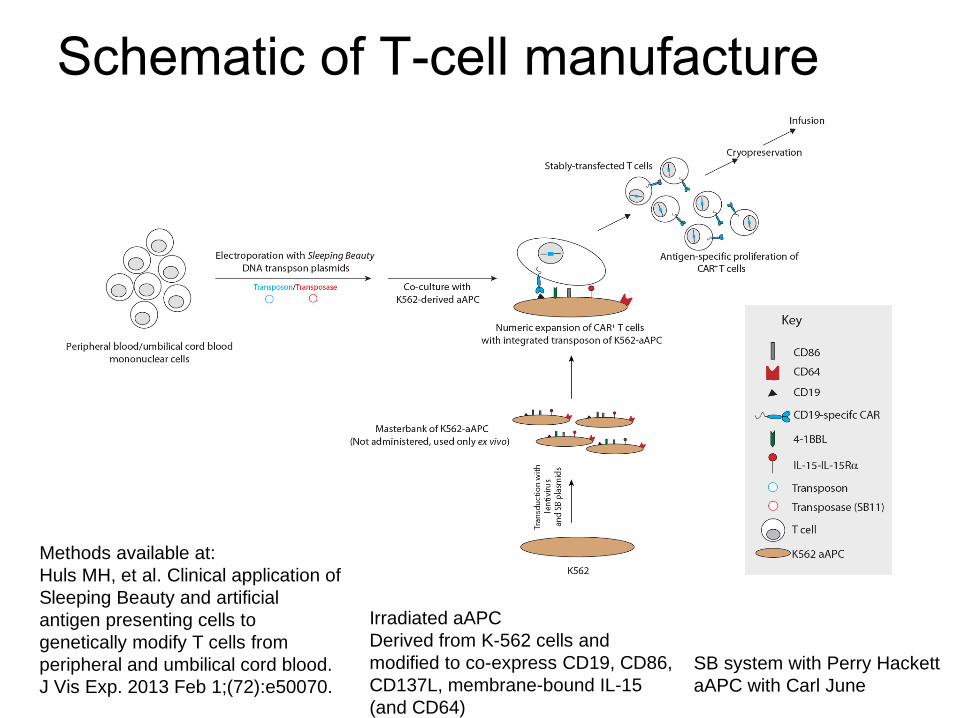
Schematic of T-cell manufacture
Methods available at:Huls MH, et al. Clinical application of Sleeping Beauty and artificial antigen presenting cells to genetically modify T cells from peripheral and umbilical cord blood. J Vis Exp. 2013 Feb 1;(72):e50070.
SB system with Perry HackettaAPC with Carl June
Irradiated aAPCDerived from K-562 cells and modified to co-express CD19, CD86, CD137L, membrane-bound IL-15 (and CD64)

Authors Target Disease N Positive Outcomes
City of Hope 2010
Follicular lymphoma (FL)
2 --
NCI 2010 FL 1 1 PR
BCM 2011 DLBCL, FL 6 --
U. Penn 2011 CLL 3 2 CR 1 PR
Memorial SK2011
CLL, ALL 9 1 PR, 1 cCR
CARs Targeting CD19Initial Results: 2010, 2011

Author CD19+ DiseaseN infused
Vector/Activation
Endo-domain
Chemo CAR+ cell
Response Persist Key Pts
CruzBCM152
Post Allo9
RetrovirusEBV/CMV/Adeno
CD28/CD3z
None Donor T 2/6 DLI bulk PR->PD3/3 adult 100% CR
9 wks Novel CARBispecific Trivirus
DavilaMMSK69
ALL13 Adults
RetrovirusCD3x28 b
CD28/CD3z
Lymphodepleting
Auto-pbpc106/Kg
10/12 MRD-6 revers CS83% CR
NR Potent bridge to SCT
GruppPenn67
ALL16 Peds 4 Adults
LentivirusCD3x28 b
41BB/CD3z
Lymph-depleting
Auto-PB 11Post Allo107-108/Kg
14/1782% CRCS in responders
1-15+Mos respon
PotentNo GVH with hx
KalosPenn163
CLL -24ALL-14ped3 adults
LentivirusCD3x28 b
41BB/CD3z
Lymph-depleting
Auto-PB 5CR 7PR 50% CR 8/17 47%
Max5%All resp and SD
Deep seq CRs
LeeNCI, Peds614
CD19+ALL 7NHL1
RetrovirusCD3x28 b.
CD28/CD3z
Flu-Cy Auto-PBPre/Post Allo 4/4
ALL CR5/771%
All pts1-38%55days
ActiveFreshInfusion
ASH 2013 CAR Clinical Abstracts

• Disease Target: CD19+ B ALL
• Subjects: 16 adults
• Vector: Retrovirus
• Manufacturing: CD3/28 Beads
• Signaling Endodomains: CD28 and CD3 zeta
• Pre T Cell Prep: Cyclophosphamide
• Overall 14 CR (88%) – higher than salvage chemo (44%)
• CAR T cells associated with CRS
Chimeric Antigen Receptor (CAR)Memorial Sloan Kettering Experience (Davila et al 2014)
U. Penn Experience (Maude et al 2014)
• Disease Target: CD19+ B ALL
• Subjects: 25 between 5-22, and 5 older adults
• Vector: Lentivirus
• Manufacturing: CD3/28 beads
• Signaling Endodomains: 41BB and CD3 zeta
• Pre T Cell Prep: None, Cy/VP, Flu/Cy, Etoposide/Cytarabine, Cyclophosphamide, CVAD-B, CVAD-A, or clofarabine
• 27 CR (90%), 6 month EFS 67%, overall survival 78%
• T cells detectable in blood, bone marrow, and CSF of patients who responded
• All patients had CRS (mild to moderate in 22/30, severe in 8)
University of Pennsylvania Experience (Maude et al 2014)

Modified T cells detectable at high levels by flow cytometry with longer peristence
Grupp, et al. NEJM 2013

NCI Experience (Kochenderfer et al 2014)
• Disease Target: CD19+ B cell malignancies (DLBCL, indolent lymphomas, CLL)
• Subjects: 15 adults
• Vector: Retrovirus
• Manufacturing: 10-Day Culture
• Signaling Endodomains: CD28 and CD3 zeta
• Pre T Cell Prep: Cyclophosphamide and fludarabine
• 8 CR, 4 PR, 1 SD, 2 not evaluable
• Acute toxicities (fever, hypotension, delirium, neurotoxicity) resolved within 3 weeks; 1 patient died 16 days post infusion
• 1st successful treatment of DLBCL with anti CD19 CAR T cells
NCI Experience (Kochenderfer et al 2014)

Pediatrics NCI Experience (Lee et al 2014)
• Disease Target: CD19+ ALL or Non-Hodgkin’s lymphoma
• Subjects: 21 children and young adults (1-30 years of age)
• Vector: Retrovirus
• Manufacturing: Bead Stimulated 11 Day Culture
• Signaling Endodomains: CD28 and CD3 zeta
• Pre T Cell Prep: Cyclophosphamide and fludarabine
• 12 CR (MRD Neg), 1 CR, 1 Cri, 3 SD, 4 PD
• All toxicities fully reversible
Peds NCI Experience (Lee et al 2014)

MD Anderson Kebriaei et al. 2014: Lymphodepletion and Sleeping Beauty Autologous CAR+ T Cells for Active Disease
Age Dx Stage CAR-T source
Dose Level
(%) CAR expression
Ds. Status post CAR
Toxicity
33 ALL Refractory relapse MSD 106/m2 94.0 Progressed, 1 mo. None
25 ALL s/p haploHCT,Refractory Haplo 106/m2 95.0 Progressed, 6 mo. None
53 NHL Recurrent MSD 106/m2 58.3 Cru, 6 mo. None
21* ALL s/p alloHCT, Rel 3 MSD 107/m2 96.8 Progressed, 9 mo. None
31* ALL s/p alloHCT, Rel 2 MSD 107/m2 93.4 CR, 1 mo. VOD/GVHD
23* ALL s/p alloHCT, Rel 2 MSD 5x107/m2 96.5 Progressed, 1 mo. None
58 ALL s/p alloHCT, CR2, MRDpos alloSelf 5x108/m2 76.7 CR, 6 mo. None
52 NHL s/p autoHCT, refractory Self 5x108/m2 89.7 Progressed, 1 mo. None
29 ALL s/p alloHCT, CR3, MRDpos alloSelf 5x108/m2 90.1 CR, 3 mo. GVHD
76 CLL Refractory relapse Self 5x108/m2 31.5 Stable, 12 mo. None
63 CLL Refractory relapse Self 5x108/m2 57.3 Progressed, 1 mo. None
76 CLL Refractory relapse Self 5x108/m2 32.9 Progressed, 2 mo. None
31 ALL s/p alloHCT, refractory CNS
alloSelf 5x109/m2 88.9 CNS progressed, 1 mo.
None
63 CLL s/p alloHCT, refractory alloSelf 5x109/m2 92.2 Too early None
N=14 pts treated, 5 with disease regression med. 6 mo follow-up

• Extraordinarily high ferritin levels after highly active CAR infusion suggest MAS/HLH/CRS
• 16,000 to 415,000 in Penn studies
• Mild coagulopathy, transaminitis
• Elevated D-dimer and low fibrinogen
• High fevers, hypotension
• Moderate marrow hematophagocytosis
Macrophage Activation Syndrome (MAS) Hemophagocytic Lymphohistiocytosis (HLH)Cytokine Release Syndrom (CRS) “Storm”

Cytokine Release Syndrome (CRS)
• Can be significant, but highly variable across patients and studies
• May or may not scale with dose, may scale with disease burden
• ? Different with different diseases
• Different in the era of highly active CAR cell therapy
• IL-6 is an important driver of toxicity
• Entirely reversible with cytokine blockade
– IL-6R blocking agent tocilizumab

Tocilizumab (Actemra)• IL-6 receptor antagonist
• Blocks IL-6 mediated effects
• Indicated in:– juvenile idiopathic arthritis (JIA)– Rheumatoid arthritis (RA)– In Japan, indication for Castleman’s Disease
• Typically given monthly
• Rare side effects of transaminitis and neutropenia
• Penn uses 8 mg/kg

Blinatumomab (CD3-CB19 BITE) causes HLH/MAS as well,reversible w/ tocilizumab
Elevated cytokines•IL-10 (5338 pg/mL)•IL-6 (681 pg/mL)•INF-γ (192 pg/mL)•IL-2R (4872 pg/mL)
David Teachey, Stephan Grupp. Blood, 2013
Blinatumomab (CD3/CD19 Bite) causes HLH/MAS as well, reversible w/ tocilizumab

Neurotoxicity issues
• Seen in several CD19 trials:– NCI
– CHOP/U. Penn– CD19-CAR-T and Blinatumomab
• Self-limited, generally untreated, fully resolves
• ? Related to CRS
• Not prevented by tocilizumab

• CD19-directed CAR T cells
• Adverse events related to cytokine release syndrome occur --- but most are manageable
• Partnerships with industry bring technology closer to being part of clinical care
• In July 2014, FDA designated CTL019 CAR T cells with “breakthrough therapy” status
• Improvements in CAR therapies underway
CAR Therapy: Summary Recent Trials

• Persistence: Correlates with Outcome
• Vector
• sCFv or Endodomain Construction
• Bulk of Disease
• Cell Type Modified (auto vs allo)
CAR Therapy: Outstanding Issues

CAR Therapy: Outstanding Issues
• Ex Vivo Expansion
• CD3x28 Beads
• OKT3/IL2
• Antigen Presenting Cells
• Cytokines
• Duration of Ex Vivo Culture
• Pre-Infusion Therapy: Lymphopenia? Treg Decrease?
• No Therapy
• Lymphodepleting Chemotherapy
• Stem Cell Transplant
CAR Therapy: Oustanding Issues

CAR Therapy: Outstanding Issues
• Homing
• CNS
• Other Sanctuarial Sites
• On Target Toxicity: B Cell Aplasia, Cytokine Storm Syndrome
• Tocilizumab
• Conditional Ablation: Caspase, HSV-TK
CAR Therapy: Oustanding Issues

• Consolidate patients with MRD
What is the Potential for CAR Therapy in ALL?
• Reinduce remission
• Produce MRD(-) state prior to SCT (Bridge to SCT)
• Multicenter trial/s in pediatric ALL are enrolling
Potential Roles for CAR Therapy in ALL

Acknowledgements
Richard Champlin Katy Rezvani Ian McNieceLaurence Cooper Marcos de Lima Amin AlousiSimrit Parmar Chitra Hosing Nina ShahBorje Andersson Michael Andreeff Simon RobinsonSteven Kornblau Yago Nieto Hong Yang Roy Jones Mark Munsell Xiaoying Liu Martin Korbling Paolo Anderlini Qaiser BashirJeffrey Molldrem Patrick Zweidler-McKay Michael ThomasPartow Kebriaei Sue Armitage Tara SadeghiLaura Worth Demetri Petropoulos Indreshpal KaurMark Munsell Sairah Ahmed Muzaffar QazilbashQing Ma Issa Khouri Jared BurksLisa St John Beatriz Martin-Antonio Gabriela Rondon Doyle Bosque Lori Griffin Kai CaoRima Saliba Peter Thall Betul Oran
Funding NCI R01- CA061508NCI PO1- CA148600
CPRIT RP100469CPRIT RP 100430
CLL Global Research FundHRSA 234200737
Funding NCI R01- CA061508NCI PO1- CA148600
CPRIT RP100469CPRIT RP 100430
CLL Global Research FundHRSA 234200737
Catherine Bollard
Michael KeatingWilliam Wierda

Redirected by gene transfer
*
Ex Vivo Approaches for Adoptive T Cell Therapy