cellularplasticitycascades:targetsforthe ... · cellularplasticitycascades:targetsforthe...
TRANSCRIPT

CDBC
Fpmulspwfst�a
Km
Blwci(arise2neaepb
F
A
R
0d
ellular Plasticity Cascades: Targets for theevelopment of Novel Therapeutics foripolar Disorder
arlos A. Zarate, Jr., Jaskaran Singh, and Husseini K. Manji
or a number of patients with bipolar disorder, current pharmacotherapy is generally insufficient. Despite adequate treatment,atients continue to have recurrent mood episodes, residual symptoms, functional impairment, psychosocial disability, and significantedical and psychiatric comorbidity. Drug development for bipolar disorder may occur through one of two approaches: the first is bynderstanding the therapeutically relevant biochemical targets of currently effective medications. Two promising direct targets of
ithium and valproate are glycogen synthase kinase-3 and histone deacetylase. The second path results from our understanding thatevere mood disorders, although not classical neurodegenerative disorders, are associated with regional impairments of structurallasticity and cellular resilience. This suggests that effective treatments will need to provide both trophic and neurochemical support,hich serves to enhance and maintain normal synaptic connectivity, thereby allowing the chemical signal to reinstate the optimal
unctioning of critical circuits necessary for normal affective functioning. For many refractory patients, drugs mimicking “traditional”trategies, which directly or indirectly alter monoaminergic levels, may be of limited benefit. Newer “plasticity enhancing” strategieshat may have utility in the treatment of mood disorders include inhibitors of glutamate release, N-methyl-D-aspartate antagonists,-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid potentiators, cyclic adenosine monophosphate phosphodiesterase inhibitors,
nd glucocorticoid receptor antagonists.ey Words: Antidepressant, bipolar disorder, depression, gluta-ate, plasticity, treatment
ipolar disorder is one of the most severely debilitating ofall medical illnesses and affects the lives and functioningof millions worldwide. Recent studies indicate that for a
arge percentage of patients, outcome is poor. Patients afflictedith bipolar disorder generally experience high rates of relapse,
hronicity, lingering residual symptoms, cognitive and functionalmpairment, psychosocial disability, and diminished well-beingFagiolini et al 2005; Revicki et al 2005; Tohen et al 2003). Inddition many deleterious health-related effects are now beingecognized. Bipolar disorder is increasingly being viewed as anllness not only with purely psychologic manifestations but as aystemic disease frequently associated with cardiovascular dis-ase, diabetes mellitus, obesity, and thyroid disease (Kupfer005). Despite these facts, little is known about the preciseeurobiological underpinnings of bipolar disorder, which isssential for the development of specific-targeted therapies thatre more effective, work rapidly, and are better tolerated thanxisting therapies. In this perspectives article, we discuss therospect of developing new medications for bipolar disorderased on two approaches:
1. Understanding the presumed therapeutically relevant bio-chemical targets of medications currently in use and usingthat knowledge to design new drugs directed at thesetargets. This includes not only direct biochemical targets,but also downstream targets that are regulated by chronicdrug administration (i.e., consistent with the clinical tem-poral profile).
rom the Laboratory of Molecular Pathophysiology, Mood and Anxiety Dis-orders Research Program, National Institute of Mental Health, Bethesda,Maryland.
ddress reprint requests to Dr. Carlos A. Zarate, Jr., 10 Center Drive, Mark O.Hatfield CRC, Unit 7 SE, Rm. 7-3445, Bethesda, MD 20892; E-mail:[email protected]
eceived July 19, 2005; revised October 6, 2005; accepted October 19, 2005.
006-3223/06/$32.00oi:10.1016/j.biopsych.2005.10.021
2. Understanding the pathophysiology of the illness (admit-tedly in its infancy) and using that knowledge to designtherapeutics to attenuate or prevent those pathologicprocesses.
Novel Therapeutic Targets Emerging from OurUnderstanding of the Mechanisms of Action ofExisting Agents
The drugs that have revolutionized the treatment of bipolardisorder are lithium and, more recently, valproate. They areeffective in the treatment of acute manic episodes, providereasonable protection against recurrent mood episodes, andhave modest antidepressant properties (Davis et al 2005; Keckand Manji 2002). Elucidation of the direct target(s) by whicheffective treatments stabilize an underlying dysregulation oflimbic and limbic-associated function also offers the potential todelineate the underlying pathophysiology of bipolar disorder.Several direct targets of lithium and valproate have been identi-fied (for a comprehensive review see Gould et al 2004). In thispaper, we only discuss glycogen synthase kinase-3 (GSK-3, adirect target of lithium) and histone deacetylase (a direct target ofvalproic acid) because several inhibitors are likely soon to beavailable to clinically test. As of this writing, there are no clinicallyavailable modulators of the other direct targets of lithium orvalproate. It should be noted that inositol monophosphatases(IMPases) may represent an important target for lithium’s actions;however, at this point, there are no selective central nervoussystem (CNS)-penetrant IMPases available for human use.
Glycogen Synthase Kinase-3GSK-3 is a serine/threonine kinase that is believed to be, in
general, constitutively active in cells, and is deactivated bysignals originating from numerous signaling pathways [for exam-p l e the Wnt pathway, PI-3= kinase (PI3K) pathway, protein kinaseA, protein kinase C, among many others] (Doble and Woodgett2003; Figure 1). Thus, the activity of GSK-3 can be regulated by
the action of a variety of other cellular signaling mechanisms,BIOL PSYCHIATRY 2006;59:1006–1020© 2006 Society of Biological Psychiatry

witt1tacerbai(
gta
FirfotGeiptfodapow
C.A. Zarate, Jr. et al BIOL PSYCHIATRY 2006;59:1006–1020 1007
hich serve to fine-tune this critical enzyme’s activity. Initialnterest in glycogen synthase kinase-3 (GSK-3) as a target for thereatment of mood disorders arose from the seminal observationshat lithium directly inhibited the enzyme (Klein and Melton996). More recent preclinical evidence implicates the modula-ion of GSK-3 in either the direct or downstream mechanism ofction of many other mood stabilizer and antidepressant medi-ations currently in use (see Gould and Manji 2005 and refer-nces therein). Notably, these medications have been shown toegulate the GSK-3 signaling cascade in vivo, and in areas of therain implicated in bipolar disorder. GSK-3 modulates apoptosisnd synaptic plasticity and probably circadian cycle by modulat-ng gene expression of proteins involved in these processesreviewed in Gould and Manji 2005; Gould et al 2004).
Very recent data from a variety of leading laboratories hasreatly strengthened the case for an important role for GSK-3 inhe pathophysiology/treatment of bipolar disorder (see Gouldnd Manji 2005 and references therein):
1. GSK-3 is markedly regulated by serotonin, dopamine, psy-
igure 1. Glycogen synthase kinase-3 (GSK-3) and intracellular signaling: Gnsulin-like growth factor (IGF-1) signaling, neurotrophic factor signaling,eceptor activates PI3 kinase mediated signaling, resulting in inhibition of Gactor 2B (eIF2B) while inhibiting insulin receptor substrate-1 (IRS-1; an inhibn central nervous system neurons; however, IGF-1 interacting with its
hrough tyrosine receptor kinase (Trk) receptors A, B, and C to activateSK-3’s neurotrophic effects, including transcription factors (e.g., heat shlement binding protein (CREB) and recently the proapoptotic Bcl-2 fam
nteract with the frizzled family of receptors and, through disheveled medroteins AXIN and adenomatous polyposis coli (APC). Normally active G
ion; however, when GSK-3 is inhibited in the Wnt pathway, �-cateninactor (TCF) to act as a transcription factor. �-catenin activity is modulatef an independent set of genes. As shown in the figure and described inirect and indirect effects on GSK-3 and GSK-3 regulated cell signalinntipsychotics, amphetamine, and selective serotonin reuptake inhibrocesses such as bioenergetics (energy metabolism), neuroplasticity, nther medications) may act by enhancing these processes through inhibith permission from Gould et al (2005).
chostimulants, and antidepressants and is at the nexus of
multiple neurotransmitter and signaling cascades putativelyinvolved in bipolar disorder.
2. GSK-3 is a major regulator of apoptosis and cellular plas-ticity and resilience. Generally, increased activity of GSK-3is pro-apoptotic, whereas inhibiting GSK-3 attenuates orprevents apoptosis (for review, see Gould and Manji 2002;Jope and Bijur 2002). Preclinical studies in animal models ofAlzheimer’s disease have shown that GSK-3 inhibition hassalutary effects on the two major pathways implicated inAlzheimer’s disease, namely, the �-amyloid and hyperphos-phorylated tau cascades (Phiel et al 2003). As we discuss inmore detail later, there is emerging knowledge that bipolardisorder is associated with cell loss and atrophy, and thereis now considerable data demonstrating that lithium exertsneuroprotective effects. These effects are believed to bemediated in large part by inhibition of GSK-3 and upregu-lation of bcl-2 (Gould and Manji 2002; Jope and Bijur 2002).
3. GSK-3 has a major effect on regulating the circadian periodin diverse species, an effect it shares with lithium (Gould etal 2004). Treatment strategies are being developed based
regulates diverse signaling pathways in the cell. These include insulin andWnt signaling. Insulin signaling through its tyrosine receptor kinase (Trk). Inhibition of GSK-3 activates glycogen synthase and eukaryotic initiationf the insulin receptor). Insulin is generally thought to have minimal effectsate receptor appears to have similar functions. Neurotrophins (NT) actinase (AKT) and inhibit GSK-3. Many effectors have been implicated infactor-1 [HSF-1], C-Jun, and cyclic adenosine monophosphate) responseember BAX. In the Wnt signaling pathway, secreted Wnt glycoproteinssignaling, inhibit GSK-3. Stability of this process requires the scaffolding
phosphorylates �-catenin, leading to its ubiquitin dependent degrada-degraded, allowing for its interaction with T cell-specific transcriptionthe intracellular estrogen receptor (ER), which also affects transcription
text, medications useful for the treatment of mood disorders have boththways. This includes direct effects of lithium and indirect effects of(SSRIs). These distinct pathways have convergent affects on cellularenesis, resilience, and survival. Thus, our hypothesis is that lithium (and
of GSK-3. Gi refers to Gi/Go; Gq refers to Gq/G11. Modified and reproduced
SK-3andSK-3
itor ocognPI3 kockily miatedSK-3
is notd bytheg pa
itorseurogition
from a chronobiological model of bipolar disorder.
www.sobp.org/journal

bdcGseD
csb
T
C
D
S
P
Gm
ti
1008 BIOL PSYCHIATRY 2006;59:1006–1020 C.A. Zarate, Jr. et al
w
4. Recent animal behavioral data (from pharmacologic andgenetic models) have shown that manipulation of theGSK-3 signaling cascade produces both antimanic andantidepressant effects in models of depression or mania. Tothe best of our knowledge, other than lithium, this is theonly manipulation that has been demonstrated to exert bothantidepressant and antimanic effects.
5. Gonadal steroids play a major role in regulating the GSK-3signaling cascade.
6. Genetic variations in GSK-3 have been associated with ageof onset and response to sleep deprivation in patients withbipolar disorder (discussed in Gould and Manji 2005).Although independent replication of these findings isclearly necessary, these preliminary reports are encourag-ing indeed.
In view of their therapeutic effects not only in bipolar disorderut also in Alzheimer’s disease and other neurodegenerativeisorders, it is not surprising that numerous pharmaceuticalompanies are actively developing specific, brain penetrantSK-3 inhibitors. Examples of classes of GSK inhibitors are
ummarized in table 1. All but the thiadiazolidinones appear toxert their actions by being competitive with ATP (reviewed inorronsoro et al 2002; Martinez et al 2002).In attempting to achieve selectivity for GSK-3 inhibition it is
ritical to avoid side effects that may occur with GSK-inhibitionuch as cardiac hypertrophy and the potential risk for cancerecause of the concern that specific GSK-3 inhibitors may have
able 1. Examples of Candidate Drugs for the Treatment of Bipolar Disord
lass
irect targets of lithium and valproateGSK inhibitors
HDAC inhibitors
hared long-term biochemical target of lithium & valproatePKC inhibitors
utative plasticity enhancersInhibitors of glutamate release and AMPA potentiatorNMDA antagonistsAMPA receptor potentiators
mGluRGlucocorticoid synthesis inhibitorsGR II antagonist
HydrocortisoneDHEACRF 1R antagonist
Bcl-2 enhancer
Abbreviations: AMPA, �-amino-5-methyl-3-hydroxy-4-isoxazole propC, glucocorticoids; DHEA, dihydroepiandrosterone; GR, glucocorticoidetabotropic glutamate receptors; NMDA, N-methyl-D-aspartate receptor;
aDrugs/compounds are at different stages of development; some may haime may not be able to be used on a long-term basis because of treatment
t remains unclear whether it is due to its ability to inhibit GSK-3 and HDAC.ww.sobp.org/journal
carcinogenic properties (due to upregulation of the Wnt path-way, which is common in human cancers). However, epidemi-ological studies of lithium and preliminary rodent studies do notsuggest a major cancer effect (reviewed in Gould et al 2003,2004).
Histone Deacetylases: A Therapeutically Relevant Targetfor Valproate?
It has been appreciated for some time that many psychotropicagents may bring about their delayed therapeutic effects byregulating gene expression in critical neuronal circuits. In recentyears, a novel mechanism has emerged by which valproate mayregulate gene expression by acting as a histone deacetylase(HDAC) inhibitor. All of the human genome is packaged in thenucleus into chromatin, a dynamic macromolecular complexmade up of repetitive units, the nucleosomes. A single nucleo-somal core particle is composed of a fragment of DNA (146 bp)wrapped around a histone octamer formed by four histone part-ners, an H3-H4 tetramer and two H2A-H2B dimmers (Monneret2005). Histones are small basic proteins that, by complexing withDNA, form the nucleosome core. Histones can be in one of twoantagonist forms, acetylated or deacetylated, equilibrium regu-lated by the corresponding enzymes, histone acetylases (HATs),and histone deacetylases (HDACs). Acetylation of histones re-duces their affinity for DNA and is a major epigenetic regulator ofgene expression. Misregulation and aberrant activities of HATsand HDACs, due to overexpression, mutation, translocation, and
Drug/Compounda
inc, indirubins, maleimides, hymenialdesine, paullones, thiadiazolidones,synthetic phosphorylated peptide, azole derivatives
mall-molecular weight carboxylates (butyrate, valproic acid, sodiumphenylbutyrate), hydroxamic acids (trichostatin A [TSA]), suberoylanilide(SAHA) and LAQ-824, benzamides (MS-275, CI-994), epoxyketones(2-Amino-8-oxo-9,10-epoxydecanoic acid [AOE] and trapoxin B, cyclicpeptides (depsipeptide, apicidin), hybrid molecules (CHAP31, CHAP50))
amoxifen, LY33531, ruboxistaurin, rottlerin, indolocarbazoles, UCN-01,CGP41251, PKC412, bisindolylmaleimides, balanol,indolylindazolylmaleimides, aprinocarsen
iluzoleetamine, memantine, felbamate, zincenzoylpiperidone (aniracetam), benzoylpyrrolidines (Ampakines),
arylpropylsulfonamides (LY392098, LY451616), S18986roup III mGluR agonistsetoconazole, aminoglutethimide, metyraponeifepristone (RU-486), ORG 34517, ORG 34850, ORG 34116, AL082D06,cyproterone acetate
eptides (astressin, �-hel corticotropin releasing factor), small moleculenon-peptides (CP-154526, antalarmin, DMP-695, DMP-696, CRA-1000,R-121919, SSR-125543, NBI 35965, NBI 27914)
ramipexole
acid; Bcl-2, B cell lymphoma-2; CRF, corticotrophin releasing factor;tor; GSK, glycogen synthase kinase; HDAC, histone deacetylase; mGluR,protein kinase C.en tested for ‘proof-of-concept’ rather than for clinical use and others at this
ing side effects. Although valproate has plasticity enhancing characteristics
er
Z
S
T
RKB
GKM
P
P
ionicrecepPKC,ve be
-limit

ambnataaidw(g2
HHnCtrHmedomt(bli(
nhctfs
Fphcch arly lif(
C.A. Zarate, Jr. et al BIOL PSYCHIATRY 2006;59:1006–1020 1009
mplification, have all been implicated in oncogenesis (Drum-ond et al 2005). For all these reasons, HDAC inhibition haseen regarded as a promising anticancer drug target, and it isow well established that HDAC inhibitors display ability toffect several cellular processes that are dysregulated in neoplas-ic cells. Valproate, a mood stabilizer, is also an HDAC inhibitornd may cause spina bifida if taken during pregnancy. Gurvichnd colleagues (2005) found that valproate and other HDACnhibitors cause very similar and characteristic developmentalefects in Xenopus and zebrafish, whereas valproate analogsith poor inhibitory activity in vivo have little teratogenic effect
Gurvich et al 2005). Indeed, valproate is already being investi-ated as a treatment for cervical cancer (Chavez-Blanco et al005).
Whereas dysregulation and aberrant activities of HATs andDACs may lead to cancer in the CNS, the loss of HAT andDAC regulation has been demonstrated to be involved ineuronal dysfunction and degeneration (Langley et al 2005).onsistent with this, a number of observations clearly establish
hat the HATs CBP and p300 (HAT family proteins) play vitaloles in the development, function, and survival of neurons. CBPAT activity has been identified also as a critical component ofemory consolidation (Korzus et al 2004). Furthermore, Rouaux
t al (2003), using an in vitro model of cell death (i.e., activity-eprived cerebellar granule neuron apoptosis) showed that theverexpression of either CBP or p300 is neuroprotective. Oneechanism by which CBP and p300 are suggested to contribute
o neuronal survival is through the transcription factor CREBcyclic adenosine monophosphate [cAMP] response elementinding protein). CREB binds to CREB-response elements (CREs)ocated in the promoters of number of genes largely implicatedn neuroprotection, such as bcl-2 (Wilson et al 1996) and BDNFFinkbeiner et al 1997; Tao et al 1998).
In recent years, there has been an increased interest in epige-etics, which is defined as the study of mitotically or meioticallyeritable variations in gene function that cannot be explained byhanges in DNA sequence (Kato et al 2005). Epigenetics purportso define the molecular mechanisms by which different cellsrom different tissues of the same organism, despite their DNA
igure 2. Histone deacetylase (HDAC) inhibitors and epigenetics: a putativermanently alter gene expression, thus subsequently affecting behavior. Bistones modify the local chromatin structure, providing access to transcripthanges are stable but potentially reversible over time. The figure depicts eircumstances that gene expression is decreased. Notably, this raises the inave the potential to reverse some of the deleterious epigenetic effects of e
2002). HATs, histone acetylases; VPA, valproate.
equence identity, exhibit very different cellular phenotypes and
perform very different functions. It is presumed that phenotypicand functional differences are the cumulative result of a largenumber of developmental, environmental, and stochastic events,some of which are mediated through the epigenetic modifica-tions of DNA and chromatin histones. DNA methylation involvescovalent binding of a methyl group to cytosines by enzymescalled DNA methyltransferases; following promoter methylation,gene transcription is generally (but not always) suppressed.Methylation of DNA also interacts with a second, and perhapsmore dynamic, level of epigenetic regulation, namely a largevariety of posttranslational modifications to histones, such asacetylation, methylation, phosphorylation, and ubiquitination(for review, see Petronis 2004; Figure 2.
Epigenetic regulation is thus one of the molecular substratesfor “cellular memory” that may help gain understanding of howenvironmental affect results in temporally dissociated alteredbehavioral responses. As discussed, valproate is known to be anHDAC inhibitor, raising the possibility that this direct target mayplay a role in some facets of its therapeutic effects or side effects(notably teratogenicity or impact on polycystic ovarian disease).
With respect to the potential role of HDAC inhibitors inpsychiatric disorders, Weaver and colleagues (2004) have under-taken an elegant series of studies on epigenetic programming bymaternal behavior. They reported that increased pup licking andgrooming (LG) and arched-back nursing (ABN) by rat mothersaltered the offspring epigenome at a glucocorticoid receptorgene promoter in the hippocampus. Offspring of mothers thatshowed high levels of these behaviors were found to havedifferences in DNA methylation compared with offspring of“low-LG-ABN” mothers. These differences were reversed withcross-fostering, persisted into adulthood, and were associatedwith altered histone acetylation. Central infusion of a HDACinhibitor removed the group differences in histone deacetylation,DNA methylation, and hypothalamic–pituitary–adrenal (HPA)responses to stress. Thus, the authors showed that an epig-enomic state of a gene can be established through behavioralprogramming, and it is potentially reversible. This line of re-search is interesting in that the sequelae of early life stressorsoften seen in patients with bipolar disorder (Leverich et al 2003)
in cellular memory. Epigenetic changes represent a mechanism that canecreased methylation of DNA (CH3) and increased acetylation (OCH2CH3) ofctors that results in upregulation of the gene transcription. Such epigeneticnmental stimuli increasing gene expression, but it is equally likely in someng possibility that central nervous system–penetrant HDAC inhibitors maye events. Modified and reproduced with permission from Gurvich and Klein
e roleoth dion fanviro
trigui
may be amenable to treatment with HDAC inhibitors. Recent
www.sobp.org/journal

sanhsn(laHomitpi2dccarid
r
PBC
a(fphaeioccsmtcscp
itr(aieipsbt
1010 BIOL PSYCHIATRY 2006;59:1006–1020 C.A. Zarate, Jr. et al
w
tudies have also suggested that the downregulation of Reelinnd GAD(67) expression in cortical interneurons in schizophre-ia and bipolar disorder patients may be mediated by epigeneticypermethylation of the respective promoters caused by theelective increase of DNA-methyltransferase 1 in GABAergiceurons (Tremolizzo et al 2005). Tremolizzo and associates2005) investigated whether methionine-induced epigenetic ree-in promoter hypermethylation and the associated behaviorallterations can be reduced by valproate in doses that inhibitDACs. They found that not only did valproate prevent methi-nine-induced reelin promoter hypermethylation and reelinRNA downregulation but also corrected deficits in prepulse
nhibition and social interaction. Finally, the appreciation thatranscriptional dysregulation may contribute to the molecularathogenesis of Huntington’s disease has led to a trial of HDAC
nhibitors in a Huntington’s disease mouse model (Ferrante et al003; Hockly et al 2003). Ferrante et al and Hockly et al observedramatically improved motor impairment concomitant with in-reases in histone acetylation in the brain. In toto, althoughonsiderable additional research is needed, with our growingppreciation of gene–environment interactions, these studiesaise the intriguing possibility that HDAC inhibitors may have anmportant role in the treatment of complex neuropsychiatricisorders, including bipolar disorder.
Table 1 summarizes the HDAC inhibitors, which are alsoeviewed by Drummond et al (2005).
rotein Kinase C Signaling Cascade: A Sharediochemical Target for the Actions ofhronic Lithium and Valproate
Because chronic administration of mood stabilizers bringsbout numerous biochemical effects, our laboratory and othersCoyle and Duman 2003) have established several criteria thatindings should meet to maximize the likelihood of their thera-eutic importance. First, it is a common effect of the structurallyighly dissimilar antimanic agents lithium (a monovalent cation)nd valproate (an 8-carbon branched fatty acid). Second, theffects occur in limbic and limbic-related regions known to benvolved in critical affective neuronal circuits. Third, the effectsccur at therapeutic concentrations in vivo. Fourth, similar to thelinical therapeutic effects, the changes are observed only afterhronic (and not acute) administration. Finally, the effects arepecific for mood stabilizers. Although it is impossible to deter-ine whether similar effects occur in the human brain in vivo,
hese experimental conditions attempt to mimic this situation aslosely as possible. Both lithium and valproate bring abouttrikingly similar effects on the protein kinase C (PKC) signalingascade, effects that may be most relevant to their antimanicrofile (Manji and Lenox 1999).
PKC is highly enriched in brain, where it plays a major rolen regulating both pre- and postsynaptic aspects of neuro-ransmission. It is now known to exist as a family of closelyelated subspecies, has a heterogeneous distribution in brainwith particularly high levels in presynaptic nerve terminals),nd plays a major role in the regulation of neuronal excitabil-ty, neurotransmitter release, and long-term alterations in genexpression and plasticity. A considerable amount of biochem-cal data supports the potential involvement of PKC in theathophysiology and treatment of bipolar disorder. Evidenceupporting this are changes in PKC and its substrates inipolar patients and changes in PKC signaling pathways after
reatment with lithium or valproate (Manji and Lenox 1999;ww.sobp.org/journal
Young et al 1999). It is noteworthy that psychostimulants,which are capable of triggering manic episodes in susceptibleindividuals and induce maniclike behaviors in rodents, areknown to activate PKC. Thus, the evidence suggests that twostructurally dissimilar antimanic agents, lithium and valproate,attenuate PKC function in a therapeutically relevant timeframe, whereas promanic psychostimulants activate PKC (Fig-ure 3). These data suggest that PKC modulation plays a criticalrole in the treatment of mania. Most recently, Birnbaum andassociates (2004) have demonstrated that excessive activationof PKC dramatically impaired the cognitive functions of theprefrontal cortex, exposure to stress activated PKC and re-sulted in prefrontal dysfunction, and inhibition of PKC (in-cluding indirectly with mood stabilizers) protected cognitivefunction. Pharmacologic inhibition of PKC results in manybehavioral changes similar to the ones induced by moodstabilizers. These include an attenuation of hyperactivity,risk-taking behavior, and hedonic drive (Einat and Manji, inpress).
These findings led to a single-blind clinical trial investigat-ing possible antimanic properties of the PKC inhibitor tamox-ifen (Bebchuk et al 2000). Although best known for itsantiestrogenic properties, tamoxifen is also a potent PKCinhibitor at high concentrations. Initial results are encourag-ing, finding that tamoxifen treatment resulted in a significantdecrease in manic symptoms (Bebchuk et al 2000). Largerdouble-blind placebo-controlled studies of tamoxifen are inprogress.
PKC has multiple isoforms, and PKC-mediated cellularprocesses are tissue- and isoform-specific. This has allowedthe modulation of function of individual isozymes. The pos-sible development of isozyme-specific drugs for therapeuticuse has led to advances in the treatment of certain conditions.For example, selective PKC inhibitors are currently beingtested to treat diabetic complications (for review, see Frank2002 and Wheeler 2003) and examples are provided in Table1. It remains unclear at this early stage of development whichof these drugs cross the blood–brain barrier and whether thespecific isozymes they inhibit are relevant to brain diseases.Compounds with properties similar to these may be used aspotential medications for the treatment of bipolar disorder.
Understanding the Pathophysiology of the Illnessto Design Therapeutics to Attenuate or Preventthe Pathological Process: Evidence for Impairmentsof Structural Plasticity and Cellular Resilience inMood Disorders
Historically, the brain systems receiving the greatest attentionin neurobiologic studies of mood disorders are the monoamin-ergic neurotransmitter systems, which are extensively distributedthroughout the network of limbic, striatal, and prefrontal corticalneuronal circuits. Such circuits are thought to support the behavioraland visceral manifestations of mood disorders (Drevets 2001;Nestler et al 2002). Although these neurotransmitter systemsundoubtedly play an important role in mediating some of thesigns/symptoms of bipolar and other mood disorders, the lack ofsignificant advances in our ability to develop improved thera-peutics for these devastating illnesses has led to the investigationof the putative roles of intracellular signaling cascades andsynaptic plasticity. “Neuroplasticity” subsumes diverse processesof vital importance by which the brain perceives, adapts to, and
responds to a variety of internal and external stimuli. The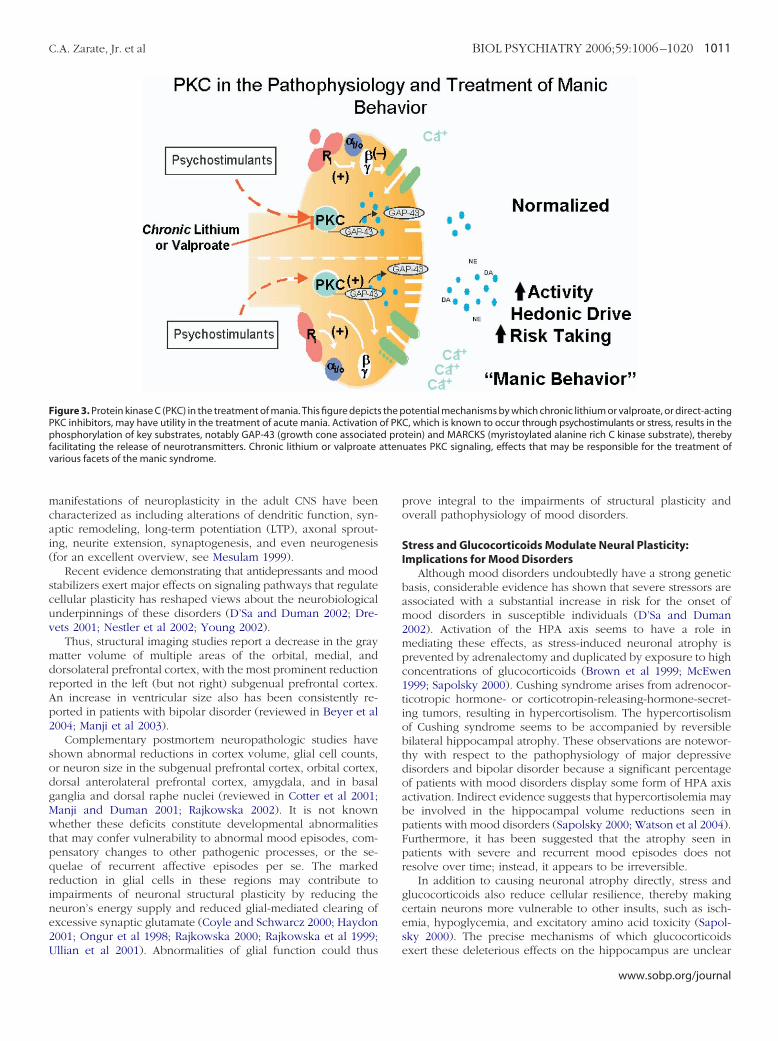
mcai(
scuv
mdrAp2
sodgMwtpqrine2U
FPpfv
C.A. Zarate, Jr. et al BIOL PSYCHIATRY 2006;59:1006–1020 1011
anifestations of neuroplasticity in the adult CNS have beenharacterized as including alterations of dendritic function, syn-ptic remodeling, long-term potentiation (LTP), axonal sprout-ng, neurite extension, synaptogenesis, and even neurogenesisfor an excellent overview, see Mesulam 1999).
Recent evidence demonstrating that antidepressants and moodtabilizers exert major effects on signaling pathways that regulateellular plasticity has reshaped views about the neurobiologicalnderpinnings of these disorders (D’Sa and Duman 2002; Dre-ets 2001; Nestler et al 2002; Young 2002).
Thus, structural imaging studies report a decrease in the grayatter volume of multiple areas of the orbital, medial, andorsolateral prefrontal cortex, with the most prominent reductioneported in the left (but not right) subgenual prefrontal cortex.n increase in ventricular size also has been consistently re-orted in patients with bipolar disorder (reviewed in Beyer et al004; Manji et al 2003).
Complementary postmortem neuropathologic studies havehown abnormal reductions in cortex volume, glial cell counts,r neuron size in the subgenual prefrontal cortex, orbital cortex,orsal anterolateral prefrontal cortex, amygdala, and in basalanglia and dorsal raphe nuclei (reviewed in Cotter et al 2001;anji and Duman 2001; Rajkowska 2002). It is not knownhether these deficits constitute developmental abnormalities
hat may confer vulnerability to abnormal mood episodes, com-ensatory changes to other pathogenic processes, or the se-uelae of recurrent affective episodes per se. The markededuction in glial cells in these regions may contribute tompairments of neuronal structural plasticity by reducing theeuron’s energy supply and reduced glial-mediated clearing ofxcessive synaptic glutamate (Coyle and Schwarcz 2000; Haydon001; Ongur et al 1998; Rajkowska 2000; Rajkowska et al 1999;
igure 3. Protein kinase C (PKC) in the treatment of mania. This figure depictsKC inhibitors, may have utility in the treatment of acute mania. Activationhosphorylation of key substrates, notably GAP-43 (growth cone associate
acilitating the release of neurotransmitters. Chronic lithium or valproatearious facets of the manic syndrome.
llian et al 2001). Abnormalities of glial function could thus
prove integral to the impairments of structural plasticity andoverall pathophysiology of mood disorders.
Stress and Glucocorticoids Modulate Neural Plasticity:Implications for Mood Disorders
Although mood disorders undoubtedly have a strong geneticbasis, considerable evidence has shown that severe stressors areassociated with a substantial increase in risk for the onset ofmood disorders in susceptible individuals (D’Sa and Duman2002). Activation of the HPA axis seems to have a role inmediating these effects, as stress-induced neuronal atrophy isprevented by adrenalectomy and duplicated by exposure to highconcentrations of glucocorticoids (Brown et al 1999; McEwen1999; Sapolsky 2000). Cushing syndrome arises from adrenocor-ticotropic hormone- or corticotropin-releasing-hormone-secret-ing tumors, resulting in hypercortisolism. The hypercortisolismof Cushing syndrome seems to be accompanied by reversiblebilateral hippocampal atrophy. These observations are notewor-thy with respect to the pathophysiology of major depressivedisorders and bipolar disorder because a significant percentageof patients with mood disorders display some form of HPA axisactivation. Indirect evidence suggests that hypercortisolemia maybe involved in the hippocampal volume reductions seen inpatients with mood disorders (Sapolsky 2000; Watson et al 2004).Furthermore, it has been suggested that the atrophy seen inpatients with severe and recurrent mood episodes does notresolve over time; instead, it appears to be irreversible.
In addition to causing neuronal atrophy directly, stress andglucocorticoids also reduce cellular resilience, thereby makingcertain neurons more vulnerable to other insults, such as isch-emia, hypoglycemia, and excitatory amino acid toxicity (Sapol-sky 2000). The precise mechanisms of which glucocorticoids
otential mechanisms by which chronic lithium or valproate, or direct-actingC, which is known to occur through psychostimulants or stress, results in thetein) and MARCKS (myristoylated alanine rich C kinase substrate), therebyuates PKC signaling, effects that may be responsible for the treatment of
the pof PKd proatten
exert these deleterious effects on the hippocampus are unclear
www.sobp.org/journal

birsd1Binpabiplendstsbc2cBedmtv
N
lr1aev(tc2a
tmaaolminmNotmc(b
1012 BIOL PSYCHIATRY 2006;59:1006–1020 C.A. Zarate, Jr. et al
w
ut likely involve the facilitation of glutamatergic signaling andnhibition of glucose transport (Sapolsky 2000). The reduction ofesilience of hippocampal neurons might also reflect the propen-ity for various stressors to decrease the expression of brain-erived neurotrophic factor (BDNF) in this region (McEwen999; Sapolsky 2000). Together with other neurotrophic factors,DNF is necessary for the survival and function of neurons,
mplying that a sustained reduction of these factors could affecteuronal viability. Neurotrophic factors are now known toromote cell survival largely by suppressing intrinsic, cellularpoptotic machinery. This process of cell survival occurs throughinding of these factors to membrane receptors and regulation ofntracellular signal transduction pathways that can control apo-tosis, including regulation of Bcl-2 family members. Accumu-
ating data suggest that not only is Bcl-2 neuroprotective, it alsoxerts neurotrophic effects and promotes neurite sprouting,eurite outgrowth, and axonal regeneration. Recent studies haveemonstrated that severe stress exacerbates stroke outcome byuppressing Bcl-2 expression (Devries et al 2001). In this study,he stressed mice expressed �70% less Bcl-2 mRNA than un-tressed mice after ischemia. Furthermore, stress greatly exacer-ated infarct in control mice but not in transgenic mice thatonstitutively expressed increased neuronal Bcl-2 (Devries et al001). Finally, high corticosterone concentrations were signifi-antly correlated with larger infarcts in wildtype mice but not incl-2-overexpressing transgenic mice. Thus, enhanced Bcl-2xpression appears to be capable of offsetting the potentiallyeleterious consequences of stress-induced neuronal endanger-ent, which suggests that pharmacologically induced upregula-
ion of Bcl-2 may have considerable utility in the treatment ofarious disorders.
eurotrophic and Neuroprotective Effects of LithiumRecent studies have shown that lithium robustly increases the
evels of the cytoprotective protein Bcl-2 in various areas ofodent brain and in cells of human neuronal origin (Chen et al999; Chen and Chuang 1999). Consistent with its effects on Bcl-2nd GSK-3�, lithium, at therapeutically relevant concentrations,xerts cytoprotective effects against the deleterious effects of aariety of insults, including glutamate, N-methyl-D-aspartateNMDA)-receptor activation, serum/nerve growth-factor depriva-ion, radiation, striatal quinolinic acid infusion, and middleerebral artery occlusion (Chen and Chuang 1999; Manji et al000). Lithium also enhances hippocampal neurogenesis in thedult rodent (Chen et al 2000).
To determine whether lithium exerts neurotrophic effects inhe human brain in vivo, recent studies have used protonagnetic resonance spectroscopy to quantify the levels of N-
cetylaspartate ([NAA] a putative marker of neuronal variabilitynd function; Bates et al 1996; Tsai and Coyle 1995. Four weeksf lithium treatment produced a significant increase in NAAevels, effects that were localized almost exclusively to grayatter (Moore et al 2000). These findings provide intriguing
ndirect support for the contention that chronic lithium increaseseuronal viability, and function in the human brain. Further-ore, an approximately .97 correlation between lithium-inducedAA increases and regional voxel gray matter content wasbserved, thereby providing evidence for co-localization withhe regional specific bcl-2 increases observed (e.g., gray vs. whiteatter) in the rodent brain cortices. These results suggest that
hronic lithium not only may exert robust neuroprotective effectsas has been demonstrated in a variety of preclinical paradigms)
ut also neurotrophic effects in humans. A follow-up volumetricww.sobp.org/journal
magnetic resonance imaging (MRI) study demonstrated that 4weeks of lithium treatment produced a significantly increasedtotal gray matter content in the human brain (Moore et al 2000),indicating an increase in the volume of the neuropil (themosslike layer comprising axonal and dendritic fibers that occu-pies much of the cortex gray-matter volume). Taken together,these clinical studies support the hypothesis that some of thetherapeutic actions of lithium may involve hitherto underappre-ciated neurotrophic and neuroprotective effects. To investigatethe clinical significance of these findings, a longitudinal high-resolution volumetric MRI study in well-characterized depressedbipolar subjects has recently been undertaken (Moore et al,unpublished data). Total brain gray matter, prefrontal graymatter, and left subgenual prefrontal gray matter were deter-mined using validated semiautomated segmentation and regionof interest methodology in the patients at baseline (medicationfree) and after 4 weeks of blinded lithium treatment. Significantincreases in total brain gray matter in bipolar subjects wereobserved following chronic lithium administration, and regionalanalyses in the bipolar subjects revealed significant differencesbetween responders (� 50% decrease on the Hamilton Depres-sion Rating Scale) and nonresponders; only responders showedincreases in gray matter in the prefrontal cortex and left sub-genual prefrontal cortex. Together, these data suggest thatpharmacologic strategies that enhance cellular plasticity andresilience may have utility not only for the long-term course ofthe illness but also for the treatment of the acute illness.
We now turn to a discussion of several plasticity enhancingstrategies currently under investigation in bipolar disorder.
Glutamatergic StrategiesOne major neurotransmitter system regulated by glucocorti-
coids is the glutamatergic system. Regulated either via glucocor-ticoids or through alternative mechanisms, abnormal activity ofthe glutamatergic system represents a likely contributor to im-pairments in brain neuroplasticity and cellular resilience ob-served in patients with bipolar disorder. Glutamate is the majorexcitatory synaptic neurotransmitter in the brain and has severalimportant roles including mediating neurotransmission acrossexcitatory synapses and regulating numerous physiologic func-tions in the mammalian CNS such as synaptic plasticity, learning,and memory (Bannerman et al 1995; Collingridge 1994; Col-lingridge and Bliss 1995; Watkins and Collingridge 1994). Severaltreatment strategies have been implemented to reduce gluta-mate-mediated excitotoxicity, which results in robust neuropro-tective effects in a variety of preclinical paradigms; however, theevidence in humans with neurodegenerative disease is moreequivocal. The same antiglutamatergic neuroprotective strategiesused for these neurodegenerative disorders may have an impor-tant role in patients with mood disorders and are currently beingtested in “proof-of-concept” studies in patients with mood disor-ders (for review, see Ketter and Wang 2003; Zarate et al 2002;Figure 4B). Glutamate exerts its action at the presynaptic andpostsynaptic level through the stimulation of specific receptorsthat can be classified by structural characteristics (Figure 2): thefirst group, ionotropic glutamate receptors, are ion channels thatwhen stimulated open the channel pore allowing sodium, po-tassium, or calcium to flow freely into the cell. This opening ofthe pore changes the polarization of the neuronal surface andoften activates intracellular signaling pathways. The secondgroup, metabotropic receptors, are G-protein-coupled receptorsthat exert their actions through second messenger pathways.
Therapeutics can target these receptors; it is additionally possible
titsiTed
I
bc(atweo(dwtaa
ztdaatiriCei
C.A. Zarate, Jr. et al BIOL PSYCHIATRY 2006;59:1006–1020 1013
o target the release of glutamate before it binds to either theonotropic or metabotropic receptors. Therapeutics directed athese targets may result in modulation of the glutamatergicystem and ultimately to mood-enhancing effects. These agentsnclude riluzole, memantine, ketamine, felbamate, and zinc.esting different glutamate-modulating agents that affect differ-nt components of glutamatergic neurotransmission may helpiscern what aspects of this system are most relevant.
nhibition of Glutamate ReleaseLamotrigine. Clinical evidence that modulation of glutamate
rain levels may be important in the treatment of mood disordersomes from the clinical use of the anticonvulsant lamotrigineCalabrese et al 1999). Lamotrigine is approved by the U.S. Foodnd Drug Administration (FDA) as monotherapy and adjunctiveherapy for epilepsy and for the maintenance treatment of adultsith bipolar disorder. Although lamotrigine has multiple cellularffects, it is postulated that an inhibition of an excessive releasef glutamate appears to be important to its mechanism of actionCalabresi et al 1996; Leach et al 1986; Wang et al 1996). Studyingrugs that also inhibit release of glutamate would help discernhether this mechanism of action might be relevant to the
herapeutic action of lamotrigine. There is now evidence thatnother drug that inhibits the release of glutamate (riluzole) alsoppears to have antidepressants properties.
Riluzole. Riluzole (2-amino-6-trifluoromethoxy benzothia-ole) is a neuroprotective agent with anticonvulsant propertieshat easily crosses the blood–brain barrier. Riluzole is the onlyrug currently approved by the FDA for the treatment ofmyotrophic lateral sclerosis (ALS). It is neuroprotective innimal models of Parkinson’s disease, NMDA receptor hypofunc-ion neurotoxicity, ischemia, and traumatic CNS injury (reviewedn Zarate et al 2002). Riluzole does not act directly on the NMDAeceptor but rather inhibits release of glutamate through both thenhibition of voltage-dependent sodium channels in mammalianNS neurons and P/Q-type calcium channels (reviewed in Zaratet al 2002). Other reported mechanisms of action of riluzole
nclude its ability to increase clearance of glutamate from thesynaptic space through enhancement of the reuptake process(Frizzo et al 2004) and its effect at �-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid potentiators (AMPA) receptors (DeSarro et al 2000). Recent studies have shown that riluzolestimulates the synthesis of growth factors including BDNF incultured mouse astrocytes (Mizuta et al 2001).
Supporting the viability of riluzole in treatment-resistantdepression are two studies. The first study was a 6-weekopen-label study with riluzole in treatment-resistant DSM-IVmajor (unipolar) depression (Zarate et al 2004a). After a1-week drug-free period, 19 subjects received riluzole at amean daily dose of 169 mg. All patients had previously failedto respond to at least one antidepressant and more than halfwere considered Stage II of treatment-resistance. Significantimprovement in depressive symptoms as measured by theMontgomery–Asberg Depression Rating Scale (MADRS) oc-curred on weeks 3 through 6 for all patients. In addition,significant improvements occurred in anxiety symptoms. Thesecond study was an 8-week open-label study with riluzole in14 patients with treatment-resistant DSM-IV bipolar depres-sion. All patients had previously failed to respond to adequatetrials of at least two antidepressants and at least 4 weeks oflithium or valproate. Patients received riluzole at a mean dailydose of 171 mg and significant improvement in MADRS scoresoccurred at weeks 5 through 8 for all patients. The responseand remission rates at week 8 for the intent to treat sample was50%. Four subjects (29%) had previously failed to respond tolamotrigine. Of these, one failed to respond to riluzole, 1 hada partial response to riluzole, and two achieved remission.Overall riluzole was well tolerated in these two trials. Thesepreliminary results need to be confirmed in controlled studies.
Ionotropic Glutamate ReceptorsThree subgroups of glutamatergic ion channels have been
identified using their pharmacologic ability to bind differentsynthetic ligands, each composed of a different set of sub-
Figure 4. (A) Cellular mechanisms underlying thedeleterious effects of stress and episodes of depres-sion and mania. This figure depicts the multiplemechanisms by which stress (and perhaps depres-sive episodes) may attenuate cellular resiliency,thereby resulting in atrophy, death, and endanger-ment of hippocampal neurons. NMDA, N-methyl-D-aspartate glutamate receptor; GR, glucocorticoidreceptor; BDNF, brain derived neurotrophic factor.Modified and reproduced, with permission fromManji et al (2003). (B) Modulation of glutamatergicthroughput: therapeutic effects. This figure depictsthe hyperglutamatergic state associated with re-gional atrophic changes and disruption of criticalneuronal circuitry. Modulators of glutamatergicthroughput may serve to reverse illness-related at-rophy, thereby reinstating the critical circuitry mod-ulating affective, cognitive, motoric and neuroveg-etative functioning. Modified and reproduced, withpermission from Nestler et al (2002).
units: NMDA receptors, �-amino-3-AMPA receptors, and kai-
www.sobp.org/journal

nt
rimsapitiwtZrNosi
tct(2ttmtwMctgupc(cNsddt
assg(
tir(t
wtooa
1014 BIOL PSYCHIATRY 2006;59:1006–1020 C.A. Zarate, Jr. et al
w
ate (KA) receptors. The latter two groups are often referredo together as the non-NMDA receptors.
NMDA Receptor. A growing body of preclinical and clinicalesearch suggests that the NMDA receptor complex may benvolved in the pathophysiology of mood disorders and theechanism of action of antidepressants and possibly mood
tabilizers (reviewed in Zarate et al 2002). The NMDA receptorntagonists such as MK-801 and AP-7 and an AMPA receptorotentiator have been shown to have antidepressant properties
n animal models of depression, including the forced swim test,he application of inescapable stressors, and tail suspensionmmobility tests, in animals exposed to chronic mild stress, asell as in the learned helplessness models of depression; effects
hat are comparable to the tricyclic antidepressants (reviewed inarate et al 2002). MK-801 increases neurogenesis in the brains ofats (Cameron et al 1995). There is evidence that the high-affinityMDA receptor antagonist ketamine has efficacy in the treatmentf depression. Berman and colleagues (2000) reported that aingle dose of the NMDA receptor antagonist ketamine resultedn rapid antidepressant effects in seven patients with depression.
Memantine. Memantine has anticonvulsant and neuropro-ective properties and has been shown in double-blind placeboontrolled studies to be effective in reducing clinical deteriora-ion in Alzheimer’s, vascular, and mixed dementia of all severitiesAreosa and Sherriff 2003; Orgogozo et al 2002; Reisberg et al003). Chemically, memantine is a 1-amino-3,5-dimethyladaman-ane of the adamantine class, a compound that can easily crosshe blood–brain barrier. Memantine is neuroprotective in animalodels of Alzheimer’s disease, ischemia, and CNS trauma. Meman-
ine is a noncompetitive voltage-dependent NMDA antagonistith a receptor effect comparable to MK-801 (Bormann 1989).emantine appears to block the NMDA-receptor-associated ion
hannel only when it is open for long periods, thus promotinghe view that it may be specific for blockade of pathologiclutamate release. Because of this mechanism of action, thentoward effects of pathologic concentrations of glutamate arerevented to a greater extent than the effects of physiologiconcentrations, which are relatively spared with memantineChen and Lipton 1997; Chen et al 1998). Memantine is an idealandidate drug to examine whether a low- to moderate-affinityMDA antagonist has antidepressant effects because it is fairlyelective to the NMDA receptor at doses of 5–20 mg/day. At theseoses, memantine has low to negligible affinity for GABA, benzo-iazepine, dopamine, adrenergic, histamine, and glycine recep-ors and for voltage-dependent Ca 2�, Na�, or K� channels.
In preclinical studies, Moryl and colleagues (1993) describeddose-dependent decrease in the immobility time in the forced
wim test in rats following administration of memantine. Aynergistic effect was seen when imipramine and fluoxetine wereiven jointly with memantine to rats in a forced swim test studyRogoz et al 2002).
We recently completed a double-blind, placebo-controlledrial of memantine in patients with major depression (Zarate et al,n press). In this study, 32 patients (mean age � 47 years) wereandomized to memantine 5–20 mg/day (n � 16) or placebon � 16). The linear mixed models for total MADRS showed noreatment effect. Similarly, no antianxiety effect was found.
Although no significant antidepressant effects were foundith the low- to moderate-affinity NMDA antagonist memantine,
his finding does not exclude the possibility that antidepressantr mood-stabilizing effects might occur using much higher dosesf memantine or if used synergistically in combination with other
gents (e.g., antidepressants, lamotrigine). At higher doses ofww.sobp.org/journal
memantine, however, it becomes nonselective for the NMDAreceptor and binds to other receptors (discussed earlier) some ofwhich have been implicated in the mechanism of action ofcurrently available antidepressants. Finally, it is possible thathigher-affinity NMDA antagonists such as ketamine may haveantidepressant properties.
Studies in progress are examining the possible therapeuticvalue of other NMDA receptor antagonists including ketamine,felbamate, and zinc.
AMPA Receptors. The AMPA receptors are a subfamily ofionotropic glutamate receptors that mediate the fast componentof excitatory neurotransmission, which, like NMDA receptors,are involved in learning and memory. Several classes of com-pounds can allosterically modulate AMPA receptors. These com-pounds (so-called AMPA receptor positive modulators or AMPAreceptor potentiators [ARPs]) do not activate AMPA receptorsthemselves but slow the rate of receptor desensitization ordeactivation in the presence of an agonist (e.g., glutamate andAMPA; for review, see Bleakman and Lodge 1998; Borges andDingledine 1998). AMPAkines, a subclass of ARPs, are smallbenzamide compounds that allosterically produce positive mod-ulation of AMPA receptors are being studied in cognition,anxiety, stroke, Parkinson’s disease, and depression (reviewed inBlack 2005). Table 1 summarizes AMPA potentiators that pene-trate the blood–brain barrier (for review, see also Black 2005).Aniracetam was found to have antidepressant properties in theforced swim test (Black 2005). Studies have shown that thebiarylpropylsulfonamide ARPs (LY392098 and LY451616) haveantidepressant effects in animal models of depression (includingthe application of inescapable stressors, forced swim test, andtail-suspension-induced immobility tests), in learned-helpless-ness models of depression, and in animals exposed to chronicmild stress procedure (Li et al 2001). In one of these preclinicalstudies, the AMPAkine Ampalex was reported to have a morerapid effect (during the first week of treatment) than fluoxetine(after 2 weeks; Knapp et al 2002). In contrast to traditionalantidepressants, this group of compounds does not appear toaffect the extracellular concentration of monoamines (Skolnicket al 2001). They can, however, enhance the neurotrophicactions of BDNF mRNA and protein in primary neuronal cultures(Lauterborn et al 2000, 2003). Modulation of neurotrophic factorexpression and altering the rate of neurogenesis may be criticalfactors in understanding the therapeutic effects of antidepres-sants and mood stabilizers in mood disorders. In support,chronic treatment with the AMPA receptor potentiator LY451646increased progenitor cell proliferation in the dentate gyrus in adose-dependent manner. The antidepressant-like activity ofARPs in animals may be attributed, at least in part, to theregulation of cell proliferation in the hippocampus (Bai et al2003). Another ARP that is being investigated in depression isS18986, which has also been reported to increase BDNF expres-sion (Lauterborn et al 2000, 2003).
Metabotropic Glutamate Receptors. Three groups compris-ing eight G-protein-coupled metabotropic glutamate receptors(mGluRs) mediate slower modulatory actions of glutamate onneurotransmitter release and cell excitability. Activation ofmGluR leads to a variety of cellular responses, including theinhibition of calcium and potassium currents, presynaptic mod-ulation of synaptic transmission, and postsynaptic interactionwith ionotropic glutamate receptors (Anwyl 1999; Baskys et al1990; Ikeda et al 1995). The mGluRs are involved in the earlyphase of memory formation and the mechanism of long-term
depression (Riedel et al 2003; Salinska and Stafiej 2003; Tan et al
2tnrmpSmeTlImld
To
doheeoms
codibrffo3tnata
nbaliHscr
oCsrbmwau
C.A. Zarate, Jr. et al BIOL PSYCHIATRY 2006;59:1006–1020 1015
003). Group I mGluRs have been found to exhibit potentialherapeutic effects in CNS disorders related to excess excitatoryeurotransmission such as epilepsy, pain, and ischemia (foreview, see Nicoletti et al 1996). Preclinical studies suggest thatGlu 2/3 agonists have antianxiety, antipsychotic, and neuro-rotective properties (Maiese et al 2000; Palucha et al 2004;choepp 2001). Selective activation–antagonism of variousGluRs can lead to anxiolytic-like effects, antidepressant-like
ffects or both (Chojnacka-Wojcik et al 2001; Spooren et al 2000;atarczynska et al 2001a, 2001b). Recently, Palucha and col-
eagues (2004) reported the antidepressant-like effects of groupII mGluR agonists in the behavioral despair test. The possibleechanism by which the group III mGluR agonists have anxio-
ytic- and antidepressant properties may be due to their ability toepress glutamate release in excitatory synapse.
he HPA Axis as a Target for the Developmentf Novel Therapeutics
Drugs that modulate HPA axis activity and have been tested inepression include inhibitors of glucocorticoid synthesis, antag-nists of the glucocorticoid receptor (GR) (Belanoff et al 2002),ydrocortisone, dexamethasone (Arana and Forbes 1991; Aranat al 1995), and dehydroepiandrosterone (reviewed in Quirozt al 2004). Some of these drugs have been investigated for prooff concept, and it is expected that modified and improvededications would lack some of the limiting side effects ob-
erved with these compounds.Glucocorticoid Synthesis Inhibitors. Treatment with glu-
ocorticoid synthesis inhibitors (e.g., ketoconazole) has beenbserved to ameliorate depression rapidly in treatment-resistantepression (reviewed in Quiroz et al 2004); examples are providedn Table 1. Most recently, in a double-blind, randomized, place-o-controlled study 63 inpatients with major depression wereandomized to receive either placebo or metyrapone (1 g/d)or the first 3 weeks of a 5-week trial with nefazodone orluvoxamine. A higher proportion of patients receiving metyrap-ne showed a positive treatment response at day 21 and at day5 compared with placebo patients. The clinical course of patientsreated with metyrapone showed an earlier onset of action begin-ing in the first week. The plasma concentrations of corticotropinnd deoxycortisol were significantly higher during metyraponereatment, whereas cortisol remained largely unchanged (Jahn etl 2004).
Corticotropin-Releasing Factor (CRF) 1 Receptor Antago-ists. A number of small molecule CRF 1R antagonists haveeen evaluated using in vivo paradigms in animal models ketottenuate CRF-induced corticotropin release (Saunders and Wil-iams 2003). Several classes of CRF 1R inhibitors have beendentified (examples are provided in Table 1; for review, seeolmes et al 2003; Saunders and Williams 2003). Preclinical
tudies have shown that CRF 1 antagonists reduce CRF-inducedorticotropin release and CRF-induced cAMP production (foreview, see Saunders and Williams 2003).
Antalarmin, a novel pyrrolopyrimidine compound, given inral doses of 20 mg/kg in primates, significantly diminished theRF-stimulated corticotropin release and the pituitary–adrenal,ympathetic, and adrenal medullary responses to stress. It alsoeversed stress-induced inhibition of exploratory and sexualehaviors (Habib et al 2000). Using the chronic stress model inice, both antalarmin (10 mg/kg) and fluoxetine (10 mg/kg)ere found to improve measures of physical state, weight gain,nd emotional response in the light-dark test compared with
ntreated stressed animals (Ducottet et al 2003).Developed by Pfizer, CP-154,526 has been evaluated inanimal paradigms for anxiety. It has similar high penetrability asantalarmin and decreases synthesis of CRF in the paraventricularnucleus (Seymour et al 2003). Mansbach et al (1997) showed itsefficacy in the learned helplessness model of depression in rats.SSR125543A is a 2-aminothiazole derivative that displays highaffinities for human CRF R1 receptors; it has shown efficacy in theforced swim test model and in chronic mild stress model in ratsin a study comparing it to antalarmin and fluoxetine (Griebel et al2002). In other studies, CRA 1000, a nonpeptide pyrimidine CRF 1antagonist being developed by Taisho Pharmaceuticals (Okuyamaet al 1999), reduced immobility in the learned helplessness para-digm in male Wistar rats when given by intraperitoneal injection(Harro et al 2001). Developed by Dupont, DMP696 is a selective,potent, and highly bioavailable nonpeptide CRF 1R antagonist. Ithas been tested in behavioral models of anxiety and is being testedin behavioral paradigms for depression (Li et al 2003).
In an open-label trial, R-121919 reduced anxiety and depres-sive symptoms in patients with major depression (Zobel et al2000). The clinical development of the compound was discon-tinued, probably because of elevated liver function tests (Kunzelet al 2003).
Dehydroepiandrosterone. Dehydroepiandrosterone (DHEA)serves as a precursor for both androgenic and estrogenic ste-roids; together with its sulphated form (DHEA-S), it is secreted bythe adrenal gland and also produced in the CNS. Thus, DHEAand DHEA-S are neuroactive steroids that have a number ofeffects that can be described as functional antagonism of theactions of glucocorticoids (DHEA does not directly interact withthe glucocorticoid receptor, and there is no known receptorfor DHEA in any tissue). It has been reported to have antide-pressant efficacy in dysthymic and depressed patients (reviewedin Quiroz et al 2004).
In a recent double-blind, randomized placebo-controlledcrossover study involving 23 men and 23 women with midlife-onset major or minor depression given DHEA (90–450 mg/day)for 6 weeks was found to be superior to placebo in reducingdepressive symptoms (Schmidt et al 2005).
GR Antagonist. Mifepristone (RU-486) is a nonselective antag-onist of the GR receptor that has been reported to have antide-pressant and antipsychotic properties in patients with psychoticdepression (Belanoff et al 2002; reviewed in Quiroz et al 2004).In a recent double-blind, placebo-controlled crossover study,Young and colleagues (2004) compared mifepristone (600 mg) toplacebo in 20 subjects with bipolar depression. They found notonly improvements in depressive symptoms with mifepristonebut also benefits for cognitive functioning, specifically in spatialmemory. This is especially noteworthy because the same inves-tigators failed to find cognitive benefits with mifepristone inpatients with schizophrenia (Gallagher et al 2005), suggestingthat the cognitive enhancing properties of this drug might belimited only to patients with mood disorders. Ongoing controlledtrials of mifepristone are underway in psychotic depression. Suchstudies will help clarify the extent of its antidepressant andantipsychotic effects in patients with psychotic depression andbipolar disorder. Examples of other GR antagonists being devel-oped are provided in Table 1.
Strategies to Enhance Neurotrophic Factor Signaling
Seminal work from the Duman laboratory has shown thatantidepressants regulate neurotrophic signaling cascades (D’Sa
and Duman 2002; Duman et al 1997). Different classes of long-termwww.sobp.org/journal

auappituceipndanaprrf
if(iir1rpatta11sP(eclmab
iPraoCHiMad
Bill
1016 BIOL PSYCHIATRY 2006;59:1006–1020 C.A. Zarate, Jr. et al
w
ntidepressant treatments, including norepinephrine (NE) re-ptake inhibitors, selective serotonin reuptake inhibitors (SSRIs),nd electroconvulsive seizure, upregulate CREB and BDNF ex-ression, which indicates that CREB and BDNF are commonostreceptor targets of these therapeutic agents; furthermore, the
ncrease was only seen with chronic use, which corresponds tohe onset of action of these medications. More evidence that linkspregulation of these pathways and antidepressant activityomes from behavioral models (D’Sa and Duman 2002; Nestlert al 2002). Chronic, but not acute, antidepressant treatment alsoncreases neurogenesis of dentate gyrus granule cells. At thisoint, it is unclear what role the regulation of hippocampaleurogenesis plays in the pathophysiology and treatment ofepression (for a critique, see Sapolsky 2004). Nevertheless, theccumulating evidence strongly supports the contention thateurotrophic effects play an important role in the actions ofntidepressants and mood stabilizers. The trophic effects areostulated to reverse illness-related atrophic changes, therebyeinstating the neurochemical throughput in critical circuitryegulating affective, cognitive, motoric, and neurovegetativeunctions.
One approach to enhance the activity of CREB is to use annhibitor of phosphodiesterase (PDE), the enzymes responsibleor the breakdown of cAMP. In this context, Takahashi et al1999) demonstrated that chronic antidepressant administrationncreases the expression of cAMP-specific PDE 4A and 4Bsoforms; these effects likely represent a compensatory “counter-egulatory” response to the chronic antidepressants (Nibuya et al996). This study suggests that PDE4A and PDE4B may beelevant targets for development of agents that possess antide-ressant effects either as monotherapy, or in combination withgents that increase intrasynaptic monoamine levels because ofhe possible synergism of effects on the cAMP cascade. Indeed,he idea that PDE inhibitors may have potential antidepressantctivity is not new and was initially proposed by Wachtel in the980s (Wachtel and Schneider 1986). In the 1980s and early990s, a number of open and controlled clinical trials demon-trated that rolipram, a specific inhibitor of the high-affinity cAMPDE4, may have antidepressant efficacy in depressed patientsreviewed in Manji et al 2003). In addition, there is somevidence that rolipram may have a faster onset of responseompared with standard antidepressants. Although the overalliterature on the use of rolipram is suggestive that PDE inhibitorsay have antidepressant efficacy and may have a faster onset of
ction, the potential use of rolipram for depression was limitedecause of side effects such as nausea and emesis.
Recent studies demonstrating that PDE4 is expressed innflammatory cells such as eosinophils and that inhibition ofDE4 downregulates the inflammatory response has generatedenewed excitement about the possible utility of this class ofgents in the treatment of diseases such as asthma, chronicbstructive pulmonary disease (COPD), rheumatoid arthritis,rohn’s disease, and multiple sclerosis (Dyke and Montana 2002;uang et al 2001). Second-generation compounds with markedly
mproved tolerability are rapidly being developed (Dyke andontana 2002; Huang et al 2001), and it is anticipated that the
vailability of CNS-penetrant PDE4 inhibitors may lead to theevelopment of a novel class of antidepressants.
Human phase I and II trials of recombinant methionyl humanDNF have already been undertaken wherein BDNF was admin-
stered by intrathecal infusion to patients with amyotrophicateral sclerosis (Ochs et al 2000). Unfortunately, treatment-
imiting side effects were encountered at higher doses, preclud-ww.sobp.org/journal
ing further study. The recent report of dysregulation of severalfibroblast growth factor (FGF) system transcripts in frontal corti-cal regions of brains from human subjects with major depressivedisorder suggests that this growth factor family may also repre-sent an important target for the development of novel therapeu-tics (Evans et al 2004).
An increasing number of strategies are being investigated todevelop small molecule switches for protein–protein interac-tions, which have the potential to regulate the activity of growthfactors, mitogen-activated protein (MAP) kinase cascades, andinteractions between homo- and heterodimers of the Bcl-2 familyof proteins (Figure 5). Bcl-2 has traditionally been viewed as a“long-term neuroprotective protein”; however, it is a key regu-lator of mitochondrial function, and there is a growing appreci-ation of the diverse functions that mitochondria play in regulat-ing integrated CNS function. Thus, increasing evidence suggeststhat mitochondrial Ca2� sequestration has a key role in modu-lating the tone of synaptic plasticity in a variety of neuronalcircuits and that that regulation of mitochondrial function is likelyto play important roles in regulating synaptic strength of neuro-nal circuitry mediating complex behaviors. Indeed, it is possiblethat lithium’s ability to upregulate Bcl-2 robustly may play a rolein its antidepressant potentiating effects. It is also noteworthythat pramipexole also upregulates Bcl-2 in several brain areas(Takata et al 2000) and has been shown to exert antidepressanteffects in double-blind, placebo-controlled trial in patients withbipolar II depression (Zarate et al 2004b). Although the dopa-mine agonistic effects of pramipexole clearly may also contributeto its purported antidepressant effects, its robust neurotrophiceffects suggest that it may have broader utility as an antidepres-sant potentiator. In this context, ongoing longitudinal studies atthe National Institute of Mental Health are investigatingpramipexole’s antidepressant and neurotrophic effects with theuse of serial magnetic resonance spectroscopy (MRS) measure-ments of N-acetyl-aspartate (NAA), and volumetric MRIs.
Conclusions
In conclusion, emerging results from a variety of clinical andpreclinical experimental studies suggest that a reconceptualiza-tion about the pathophysiology, course, and optimal long-termtreatment of recurrent mood disorders may be warranted. Un-derstanding the biochemical targets of the most effective medi-cations used in bipolar disorder as well as understanding thepresumed pathophysiology of the illness will provide us with thegreatest opportunity to develop next generation therapies. Drugsthat inhibit the direct targets of lithium and valproate (e.g., GSK-3and HDAC) and drugs that act on the shared downstreambiochemical targets of lithium and valproate (e.g., PKC) offerconsiderable promise in drug development for bipolar disorder.Less evidence exists to support the other direct targets of lithiumand valproate for the development of novel therapeutics forbipolar disorder. In terms of the presumed pathophysiology ofbipolar disorder and other severe recurring mood disorders,increasing evidence supports the idea that regional reductions inbrain volume are most likely a consequence of impairments ofstructure plasticity and resilience. Thus, optimal acute and long-term treatment for these severe illnesses will require bothneurochemical and neurotrophic support. As reviewed, there area number of pharmacologic “plasticity-enhancing” strategies thatmay be of considerable utility in the treatment of mood disorders(see Table 1 and Figure 5). Among the most immediate candi-
dates are glutamate-release-reducing agents, NMDA antagonists,
Aacni
iafsaicftmhfa
gMAla
FwlapeAeel4auepwC
C.A. Zarate, Jr. et al BIOL PSYCHIATRY 2006;59:1006–1020 1017
MPA potentiators, cAMP phosphodiesterase inhibitors, and GRntagonists. Some of these compounds are in early phases oflinical testing (e.g., corticotropin releasing factor [CRF] antago-ists, riluzole), and as such, the results will need to be confirmedn larger controlled studies.
Furthermore, an increasing number of strategies are beingnvestigated to develop small molecule agents to regulate thectivity of growth factors, MAP kinases cascades, and the Bcl-2amily of proteins. Finally, in addition to treating the coreymptoms of bipolar disorder, next generation drugs might beble to target other important aspects of the illness (e.g., enhanc-ng cognition independent of whether mood symptoms signifi-antly improve; GR antagonists), prevent or reverse epigeneticactors that may have long-term negative impact on the course ofhe illness (e.g., histone deacetylase inhibitors), or reduce certainedical comorbidities (e.g., diabetes; GSK-inhibitors). This progressolds much promise for the development of novel therapeuticsor the long-term treatment of severe, refractory mood disordersnd for improving the lives of millions.
This study was supported by the Intramural Research Pro-ram of the National Institute of Mental Heath, the Stanleyedical Research Institute, and NARSAD. The authors thanklex Noury for outstanding editorial assistance. Because of space
imitations, we often cited review papers and apologize to those
igure 5. Plasticity regulators as targets for the development of novel agenthich neuroplasticity and cellular resilience can be increased in mood disor
ikely elevations of glucocorticoids), and illness progression may all contribund atrophy observed in mood disorders. Bcl-2 attenuates apoptosis by sreventing the release of mitochondrial apoptogenic factors such as calciunhancing mitochondrial calcium uptake. Antidepressants regulate the exprand TrkB utilize the PI-3-kiase/Akt and ERK MAP kinase pathways to bring
xpression of Bcl-2 via its effects on CREB. (1) Phosphodiesterase inhibxpression of the major neurotrophic protein, Bcl-2. (3) Metabotropic g
evels of glutamate. (4) Drugs such as lamotrigine and riluzole act on Na�-isoxazole propionic acid potentiators (AMPAs) upregulate the expressnd memantine enhance plasticity and cell survival. (7) Novel drugs to entility for the treatment of depressive disorders. (8) Corticotropin releffects of hypercortisolemia, and CRH antagonists may exert other benefiituitary–adrenal) mechanisms. (10) Agents that upregulate Bcl-2 (e.g. pould be postulated to have considerable utility in the treatment of depharney and Manji (2004): Sci STKE 225:re5.
uthors whose original data could not be included. None of the
investigators in this study have a possible conflict of interest,financial or otherwise.
Anwyl R (1999): Metabotropic glutamate receptors: Electrophysiologicalproperties and role in plasticity. Brain Res Brain Res Rev 29:83–120.
Arana GW, Forbes RA (1991): Dexamethasone for the treatment of depres-sion: A preliminary report. J Clin Psychiatry 52:304 –306.
Arana GW, Santos AB, Laraia MT, et al (1995): Dexamethasone for the treat-ment of depression: A randomized, placebo-controlled, double-blindtrial. Am J Psychiatry 152:265–267.
Areosa SA, Sherriff F (2003): Memantine for dementia. Cochrane DatabaseSyst Rev July 20 (3):CD003154.
Bai F, Bergeron M, Nelson DL (2003): Chronic AMPA receptor potentiator(LY451646) treatment increases cell proliferation in adult rat hippocam-pus. Neuropharmacology 44:1013–1021.
Bannerman DM, Good MA, Butcher SP, Ramsay M, Morris RG (1995): Distinctcomponents of spatial learning revealed by prior training and NMDAreceptor blockade. Nature 378:182–186.
Baskys A, Bernstein NK, Barolet AW, Carlen PL (1990): NMDA and quisqualatereduce a Ca-dependent K� current by a protein kinase-mediated mech-anism. Neurosci Lett 112:76 – 81.
Bates TE, Strangward M, Keelan J, Davey GP, Munro PM, Clark JB (1996):Inhibition of N-acetylaspartate production: Implications for 1H MRSstudies in vivo. Neuroreport 7:1397–1400.
Bebchuk JM, Arfken CL, Dolan-Manji S, Murphy J, Hasanat K, Manji HK (2000):A preliminary investigation of a protein kinase C inhibitor in the treat-ment of acute mania. Arch Gen Psychiatry 57:95–97.
Belanoff JK, Rothschild A, Cassidy F, DeBattista C, Baulieu EE, Schold C,Schatzberg AF (2002): An open label trial of C–1073 (mifepristone) for
he treatment of mood disorders. This figure depicts the multiple targets byGenetic and neurodevelopmental factors, repeated affective episodes (andthe impairments of cellular resilience, volumetric reductions, and cell deathstering proforms of death-driving cysteine proteases (called caspases) bytochrome c, and apoptosis-inducing factor (AIF) into the cytoplasm and byn of brain-derived neurotrophic factor (BDNF) and its receptor TrkB. Both Trkt their neurotrophic effects. The ERK MAP kinase cascade also increases theincrease the levels of pCREB. (2) MAP kinase modulators increase theate receptors (mGluRs) II/III agonists modulate the release of excessivennels to attenuate glutamate release. (5) �-amino-3-hydroxy-5-methyl-
f BDNF. (6) N-methyl-D-aspartate (NMDA) antagonists such as ketaminee glial release of trophic factors and clear excessive glutamate may havefactor (CRF). (9) Glucocorticoid antagonists attenuate the deleteriousffects in the treatment of depression through non-HPA (hypothalamic–
pexole, shown to be effective in bipolar depression; Zarate et al 2004 b)n and other stress-related disorders. Reproduced with permission from
s for tders.te toequem, cyessioabou
itorslutam
chaion ohanc
asingcial eramiressio
psychotic major depression. Biol Psychiatry 52:386 –392.
www.sobp.org/journal

B
B
B
B
B
B
B
B
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
D
D
1018 BIOL PSYCHIATRY 2006;59:1006–1020 C.A. Zarate, Jr. et al
w
erman RM, Cappiello A, Anand A, Oren DA, Heninger GR, Charney DS,Krystal JH (2000): Antidepressant effects of ketamine in depressed pa-tients. Biol Psychiatry 47:351–354.
eyer JL, Kuchibhatla M, Payne ME, et al (2004): Hippocampal volume mea-surement in older adults with bipolar disorder. Am J Geriatr Psychiatry12:613– 620.
irnbaum SG, Yuan PX, Wang M, Moo-Young M, Cassidy F, Macfall J, Krish-nan KR (2004): Protein kinase C overactivity impairs prefrontal corticalregulation of working memory. Science 306:882– 884.
lack MD (2005): Therapeutic potential of positive AMPA modulators andtheir relationship to AMPA receptor subunits. A review of preclinicaldata. Psychopharmacology (Berl) 179:154 –163.
leakman D, Lodge D (1998): Neuropharmacology of AMPA and kainatereceptors. Neuropharmacology 37:1187–1204.
orges K, Dingledine R (1998): AMPA receptors: Molecular and functionaldiversity. Prog Brain Res 116:153–170.
ormann J (1989): Memantine is a potent blocker of N-methyl-D-aspartate(NMDA) receptor channels. Eur J Pharmacol 166:591–592.
rown ES, Rush AJ, McEwen BS (1999): Hippocampal remodeling and dam-age by corticosteroids: Implications for mood disorders. Neuropsychop-harmacology 21:474 – 484.
alabrese JR, Bowden CL, Sachs GS, Ascher JA, Monaghan E, Rudd GD (1999):A double-blind placebo-controlled study of lamotrigine monotherapy inoutpatients with bipolar I depression. Lamictal 602 Study Group. J ClinPsychiatry 60:79 – 88.
alabresi P, Siniscalchi A, Pisani A, Stefani A, Mercuri NB, Bernardi G (1996): Afield potential analysis on the effects of lamotrigine, GP 47779, andfelbamate in neocortical slices. Neurology 47:557–562.
ameron HA, McEwen BS, Gould E (1995): Regulation of adult neurogenesisby excitatory input and NMDA receptor activation in the dentate gyrus.J Neurosci 15:4687– 4692.
havez-Blanco A, Segura-Pacheco B, Perez-Cardenas E, Taja-Chayeb L,Cetina L, Candelaria M, et al (2005): Histone acetylation and histonedeacetylase activity of magnesium valproate in tumor and peripheralblood of patients with cervical cancer. A phase I study. Mol Cancer 4:22.
hen G, Rajkowska G, Du F, Seraji-Bozorgzad N, Manji HK (2000): Enhance-ment of hippocampal neurogenesis by lithium. J Neurochem 75:1729 –1734.
hen G, Zeng WZ, Yuan PX, Huang LD, Jiang YM, Zhao ZH, Manji HK (1999):The mood-stabilizing agents lithium and valproate robustly increase thelevels of the neuroprotective protein bcl-2 in the CNS. J Neurochem72:879 – 882.
hen HS, Lipton SA (1997): Mechanism of memantine block of NMDA-activated channels in rat retinal ganglion cells: Uncompetitive antago-nism. J Physiol 499 (Pt 1):27– 46.
hen HS, Wang YF, Rayudu PV, Edgecomb P, Neill JC, Segal MM, et al (1998):Neuroprotective concentrations of the N-methyl-D-aspartate open-channel blocker memantine are effective without cytoplasmic vacu-olation following post-ischemic administration and do not blockmaze learning or long-term potentiation. Neuroscience 86:1121–1132.
hen RW, Chuang DM (1999): Long term lithium treatment suppresses p53and Bax expression but increases Bcl–2 expression. A prominent role inneuroprotection against excitotoxicity. J Biol Chem 274:6039 – 6042.
hojnacka-Wojcik E, Klodzinska A, Pilc A (2001): Glutamate receptor ligandsas anxiolytics. Curr Opin Investig Drugs 2:1112–1119.
ollingridge GL (1994): Long-term potentiation. A question of reliability.Nature 371:652– 653.
ollingridge GL, Bliss TV (1995): Memories of NMDA receptors and LTP.Trends Neurosci 18:54 –56.
otter D, Mackay D, Landau S, Kerwin R, Everall I (2001): Reduced glial celldensity and neuronal size in the anterior cingulate cortex in major de-pressive disorder. Arch Gen Psychiatry 58:545–553.
oyle JT, Duman RS (2003): Finding the intracellular signaling pathwaysaffected by mood disorder treatments. Neuron 38:157–160.
oyle JT, Schwarcz R (2000): Mind glue: Implications of glial cell biology forpsychiatry. Arch Gen Psychiatry 57:90 –93.
’Sa C, Duman RS (2002): Antidepressants and neuroplasticity. Bipolar Dis-ord 4:183–194.
avis LL, Bartolucci A, Petty F (2005): Divalproex in the treatment ofbipolar depression: A placebo-controlled study. J Affect Disord 85:
259 –266.ww.sobp.org/journal
De Sarro G, Siniscalchi A, Ferreri G, Gallelli L, De Sarro A (2000): NMDA andAMPA/kainate receptors are involved in the anticonvulsant activity ofriluzole in DBA/2 mice. Eur J Pharmacol 408:25–34.
Devries AC, Joh HD, Bernard O, Hattori K, Hurn PD, Traystman RJ, Alkayed NJ(2001): Social stress exacerbates stroke outcome by suppressing Bcl–2expression. Proc Natl Acad Sci USA 98:11824 –11828.
Doble BW, Woodgett JR (2003): GSK-3: tricks of the trade for a multi-taskingkinase. J Cell Sci 116:1175–1186.
Dorronsoro I, Castro A, Martinez A (2002): Inhibitors of glycogen synthasekinase-3: Future therapy for unmet medical needs. Expert Opin TherPatents 12:1527–1536.
Drevets WC (2001): Neuroimaging and neuropathological studies of depres-sion: Implications for the cognitive– emotional features of mood disor-ders. Curr Opin Neurobiol 11:240 –249.
Drummond D, Noble C, Kirpotin D, Guo Z, Scott G, Benz C (2005): Clinicaldevelopment of histone deacetylase inhibitors as anticancer agents.Annu Rev Pharmacol Toxicol 45:495–528.
Ducottet C, Griebel G, Belzung C (2003): Effects of the selective nonpeptidecorticotropin-releasing factor receptor 1 antagonist antalarmin in thechronic mild stress model of depression in mice. Prog Neuropsychophar-macol Biol Psychiatry 27:625– 631.
Duman RS, Heninger GR, Nestler EJ (1997): A molecular and cellular theory ofdepression. Arch Gen Psychiatry 54:597– 606.
Dyke HJ, Montana JG (2002): Update on the therapeutic potential of PDE4inhibitors. Expert Opin Investig Drugs 11:1–13.
Einat H, Manji HK, (in press): Cellular plasticity cascades: Genes-to-behaviorpathways in animal models of bipolar disorder. Biol Psychiatry.
Evans SJ, Choudary PV, Neal CR, Li JZ, Vawter MP, Tomita H, et al (2004):Dysregulation of the fibroblast growth factor system in major depres-sion. Proc Natl Acad Sci U S A 101:15506 –15511.
Fagiolini A, Kupfer DJ, Masalehdan A, Scott JA, Houck PR, Frank E (2005):Functional impairment in the remission phase of bipolar disorder. Bipo-lar Disord 7:281–285.
Ferrante RJ, Kubilus JK, Lee J, et al (2003): Histone deacetylase inhibition bysodium butyrate chemotherapy ameliorates the neurodegenerativephenotype in Huntington’s disease mice. J Neurosci 23:9418 –9427.
Finkbeiner S, Tavazoie SF, Maloratsky A, Jacobs KM, Harris KM, GreenbergME (1997): CREB: A major mediator of neuronal neurotrophin responses.Neuron 19:1031–1047.
Frank RN (2002): Potential new medical therapies for diabetic retinopathy:Protein kinase C inhibitors. Am J Ophthalmol 133:693– 698.
Frizzo ME, Dall’Onder LP, Dalcin KB, Souza DO (2004): Riluzole enhancesglutamate uptake in rat astrocyte cultures. Cell Mol Neurobiol 24:123–128.
Gallagher P, Watson S, Smith MS, Ferrier IN, Young AH (2005): Effects ofadjunctive mifepristone (RU-486) administration on neurocognitivefunction and symptoms in schizophrenia. Biol Psychiatry 57:155–161.
Gould TD, Chen G, Manji HK (2004): In vivo evidence in the brain for lithiuminhibition of glycogen synthase kinase-3. Neuropsychopharmacology 29:32–38.
Gould TD, Gray NA, Manji HK (2003): Effects of a glycogen synthase kinase-3inhibitor, lithium, in adenomatous polyposis coli mutant mice. Pharma-col Res 48:49 –53.
Gould TD, Manji HK (2002): The Wnt signaling pathway in bipolar disorder.Neuroscientist 8:497–511.
Gould TD, Manji HK (2005): Glycogen synthase kinase-3: A putative molecu-lar target for lithium mimetic drugs. Neuropsychopharmacology 30:1223–1237.
Gould TD, Quiroz JA, Singh J, Zarate CA, Manji HK (2004): Emerging experi-mental therapeutics for bipolar disorder: Insights from the molecularand cellular actions of current mood stabilizers. Mol Psychiatry 9:734 –755.
Gould TD, Zarate CA, Manji HK (2004): Glycogen synthase kinase-3: A targetfor novel bipolar disorder treatments. J Clin Psychiatry 65:10 –21.
Griebel G, Simiand J, Steinberg R, et al (2002): 4-(2-Chloro-4-methoxy-5-methylphenyl)-N-[(1S)-2-cyclopropyl-1-(3-fluoro-4-methylphenyl)ethyl]5-methyl-N-(2-propynyl)-1, 3-thiazol-2-amine Hydrochloride (SSR125543A),a potent and selective corticotrophin-releasing factor1 receptor antag-onist. II. Characterization in rodent models of stress-related disorders.J Pharmacol Exp Ther 301:333–345.
Gurvich N, Berman MG, Wittner BS, Gentleman RC, Klein PS, Green JB (2005):Association of valproate-induced teratogenesis with histone deacety-
lase inhibition in vivo. FASEB J 19:1166 –1168.
H
H
H
H
H
H
I
J
J
K
K
K
K
K
K
K
K
L
L
L
L
L
L
L
C.A. Zarate, Jr. et al BIOL PSYCHIATRY 2006;59:1006–1020 1019
abib KE, Weld KP, Rice KC, Pushkas J, Champoux M, Listwak S, et al (2000):Oral administration of a corticotropin-releasing hormone receptor an-tagonist significantly attenuates behavioral, neuroendocrine, and auto-nomic responses to stress in primates. Proc Natl Acad Sci U S A 97:6079 –6084.
arro J, Tonissaar M, Eller M (2001): The effects of CRA 1000, a non-peptideantagonist of corticotropin-releasing factor receptor type 1, on adaptivebehaviour in the rat. Neuropeptides 35:100 –109.
aydon PG (2001): GLIA: Listening and talking to the synapse. Nat RevNeurosci 2:185–193.
ockly E, Richon VM, Woodman B, et al (2003): Suberoylanilide hydroxamicacid, a histone deacetylase inhibitor, ameliorates motor deficits in amouse model of Huntington’s disease. Proc Natl Acad Sci USA 100:2041–2046.
olmes A, Heilig M, Rupniak NM, Steckler T, Griebel G (2003): Neuropeptidesystem as novel therapeutic targets for depression and anxiety disor-ders. Trends Pharmacol Sci 24:580 –588.
uang Z, Ducharme Y, Macdonald D, Robichaud A (2001): The next genera-tion of PDE4 inhibitors. Curr Opin Chem Biol 5:432– 438.
keda SR, Lovinger DM, McCool BA, Lewis DL (1995): Heterologous expres-sion of metabotropic glutamate receptors in adult rat sympathetic neu-rons: Subtype-specific coupling to ion channels. Neuron 14:1029 –1038.
ahn H, Schick M, Kiefer F, Kellner M, Yassouridis A, Wiedemann K (2004):Metyrapone as additive treatment in major depression: a double-blindand placebo-controlled trial. Arch Gen Psychiatry 61:1235–1244.
ope RS, Bijur GN (2002): Mood stabilizers, glycogen synthase kinase-3betaand cell survival. Mol Psychiatry 7(suppl 1):S35–S45.
ato T, Iwamoto K, Kakiuchi C, Kuratomi G, Okazaki Y (2005): Genetic orepigenetic difference causing discordance between monozygotic twinsas a clue to the molecular basis of mental disorders. Mol Psychiatry10:622– 630.
eck PE, Jr., Manji HK (2002): Current and Emerging Treatments for AcuteMania and Long-Term Prophylaxis for Bipolar Disorder. Philadelphia: Lip-pincott Williams & Wilkins.
etter TA, Wang PW (2003): The emerging differential roles of GABAergicand antiglutamatergic agents in bipolar disorders. J Clin Psychiatry64(suppl 3):15–20.
lein PS, Melton DA (1996): A molecular mechanism for the effect of lithiumon development. Proc Natl Acad Sci U S A 93:8455– 8459.
napp RJ, Goldenberg R, Shuck C, Cecil A, Watkins J, Miller C, Crites G,Malatynska E (2002): Antidepressant activity of memory-enhancingdrugs in the reduction of submissive behavior model. Eur J Pharmacol440:27–35.
orzus E, Rosenfield MG, Mayford M (2004): CBP histone acetyltransferaseactivity is a critical component of memory consolidation. Neuron 42:961–972.
unzel HE, Zobel AW, Nickel T, Nickel T, Ackl N, Sonntag A, Holsboer F, Uhr M(2003): Treatment of depression with the CRH-1-receptor antagonistR121919: Endocrine changes and side effects. J Psychiatr Res 37:525–533.
upfer DJ (2005): The increasing medical burden in bipolar disorder. JAMA293:2528 –2530.
angley B, Gensert J, Beal F, Ratan R (2005): Remodeling chromatin andstress resistance in the central nervous system: Histone deacetylaseinhibitors as novel and broadly effective neuroprotective agents. CurrDrug Targets CNS Neurol Disord 4:41–50.
auterborn J, Lynch G, Vanderklish P, Arai A, Gall CM (2000): Positive modu-lation of AMPA receptors increases neurotrophin expression by hip-pocampal and cortical neurons. J Neurosci 20:8 –21.
auterborn J, Truong G, Baudry M, Bi X, Lynch G, Gall C (2003): Chronicelevation of brain-derived neurotrophic factor by ampakines. J Pharma-col Exp Ther 307:297–305.
each MJ, Marden CM, Miller AA (1986): Pharmacological studies on lam-otrigine, a novel potential antiepileptic drug: II. Neurochemical studieson the mechanism of action. Epilepsia 27:490 – 497.
everich GS, McElroy SL, Suppes T, Keck PE Jr, Denicoff KD, Nolen WA, et al(2003): Factors associated with suicide attempts in 648 patients withbipolar disorder in the Stanley Foundation Bipolar Network. J Clin Psychi-atry 64:506 –515.
i X, Tizzano JP, Griffey K, Clay M, Lindstrom T, Skolnick P (2001): Antidepres-sant-like actions of an AMPA receptor potentiator (LY392098). Neuro-pharmacology 40:1028 –1033.
i YW, Hill G, Wong H, Kelly N, Ward K, Pierdomenico M, et al (2003): Receptor
occupancy of nonpeptide corticotropin-releasing factor 1 antagonistDMP696: Correlation with drug exposure and anxiolytic efficacy.J Pharmacol Exp Ther 305:86 –96.
Maiese K, Vincent A, Lin SH, Shaw T (2000): Group I and group III metabo-tropic glutamate receptor subtypes provide enhanced neuroprotection.J Neurosci Res 62:257–272.
Manji H, Duman R (2001): Impairments of neuroplasticity and cellular resil-ience in severe mood disorder: Implications for the development ofnovel therapeutics. Psychopharmacol Bull 35:5– 49.
Manji HK, Lenox RH (1999): Ziskind-Somerfeld Research Award. Protein ki-nase C signaling in the brain: Molecular transduction of mood stabiliza-tion in the treatment of manic-depressive illness. Biol Psychiatry 46:1328 –1351.
Manji HK, Moore GJ, Rajkowska G, Chen G (2000): Neuroplasticity and cellu-lar resilience in mood disorders. Millennium Article. Mol Psychiatry5:578 –593.
Manji HK, Quiroz JA, Sporn J, Payne JL, Denicoff K, A Gray N, et al (2003):Enhancing neuronal plasticity and cellular resilience to develop novel,improved therapeutics for difficult-to-treat depression. Biol Psychiatry53:707–742.
Mansbach RS, Brooks EN, Chen YL (1997): Antidepressant-like effects ofCP–154,526, a selective CRF1 receptor antagonist. Eur J Pharmacol 323:21–26.
Martinez A, Castro A, Dorronsoro I, Alonso M (2002): Glycogen synthasekinase 3 (GSK-3) inhibitors as new promising drugs for diabetes, neuro-degeneration, cancer, and inflammation. Med Res Rev 22:373–384.
McEwen BS (1999): Stress and hippocampal plasticity. Annu Rev Neurosci22:105–122.
Mesulam MM (1999): Neuroplasticity failure in Alzheimer’s disease: Bridgingthe gap between plaques and tangles. Neuron 24:521–529.
Mizuta I, Ohta M, Ohta K, Nishimura M, Mizuta E, Kuno S (2001): Riluzolestimulates nerve growth factor, brain-derived neurotrophic factor andglial cell line-derived neurotrophic factor synthesis in cultured mouseastrocytes. Neurosci Lett 310:117–120.
Monneret C (2005): Histone deacetylase inhibitors. Eur J Med Chemistry 40:1–13.
Moore GJ, Bebchuk JM, Hasanat K, Chen G, Seraji-Bozorgzad N, Wilds IB, et al(2000): Lithium increases N-acetyl-aspartate in the human brain: In vivoevidence in support of bcl–2’s neurotrophic effects? Biol Psychiatry48:1–8.
Moore GJ, Bebchuk JM, Wilds IB, Chen G, Manji HK (2000): Lithium-inducedincrease in human brain gray matter. Lancet 356:1241–1242.
Moryl E, Danysz W, Quack G (1993): Potential antidepressive properties of aman-tadine, memantine and bifemelane. Pharmacol Toxicol 72:394–397.
Nestler EJ, Barrot M, DiLeone RJ, Eisch AJ, Gold SJ, Monteggia LM (2002):Neurobiology of depression. Neuron 34:13–25.
Nibuya M, Nestler EJ, Duman RS (1996): Chronic antidepressant administra-tion increases the expression of cAMP response element binding protein(CREB) in rat hippocampus. J Neurosci 16:2365–2372.
Nicoletti F, Bruno V, Copani A, Casabona G, Knopfel T (1996): Metabotropicglutamate receptors: A new target for the therapy of neurodegenerativedisorders? Trends Neurosci 19:267–271.
Ochs G, Penn RD, York M, Giess R, Beck M, Tonn J, et al (2000): A phase I/II trialof recombinant methionyl human brain derived neurotrophic factoradministered by intrathecal infusion to patients with amyotrophic lat-eral sclerosis. Amyotroph Lateral Scler Other Motor Neuron Disord 1:201–206.
Okuyama S, Chaki S, Kawashima N, Suzuki Y, Ogawa S, Nakazato A, et al(1999): Receptor binding, behavioral, and electrophysiological pro-files of nonpeptide corticotropin-releasing factor subtype 1 receptorantagonists CRA1000 and CRA1001. J Pharmacol Exp Ther 289:926 –935.
Ongur D, Drevets WC, Price JL (1998): Glial reduction in the subgenualprefrontal cortex in mood disorders. Proc Natl Acad Sci U S A 95:13290 –13295.
Orgogozo JM, Rigaud AS, Stoffler A, Mobius HJ, Forette F (2002): Efficacy andsafety of memantine in patients with mild to moderate vascular demen-tia: A randomized, placebo-controlled trial (MMM 300). Stroke 33:1834 –1839.
Palucha A, Tatarczynska E, Branski P, Szewczyk B, Wieronska JM, Klak K, et al(2004): Group III mGlu receptor agonists produce anxiolytic- and antide-pressant-like effects after central administration in rats. Neuropharma-
cology 46:151–159.www.sobp.org/journal

P
P
Q
R
R
R
R
R
R
R
R
S
S
S
S
S
S
S
S
S
T
T
T
1020 BIOL PSYCHIATRY 2006;59:1006–1020 C.A. Zarate, Jr. et al
w
etronis A (2004): The origin of schizophrenia: genetic thesis, epigeneticantithesis, and resolving synthesis. Biol Psychiatry 55:965–970.
hiel CJ, Wilson CA, Lee VM, Klein PS (2003): GSK-3 alpha regulates produc-tion of Alzheimer’s disease amyloid-beta peptides. Nature 423:435– 439.
uiroz JA, Singh J, Gould TD, Denicoff KD, Zarate CA, Manji HK (2004):Emerging experimental therapeutics for bipolar disorder: Clues from themolecular pathophysiology. Mol Psychiatry 9:756 –776.
ajkowska G (2000): Postmortem studies in mood disorders indicatealtered numbers of neurons and glial cells. Biol Psychiatry 48:766 –77.
ajkowska G (2002): Cell pathology in bipolar disorder. Bipolar Disord4:105–116.
ajkowska G, Miguel-Hidalgo JJ, Wei J, Dilley G, Pittman SD, Meltzer HY, et al(1999): Morphometric evidence for neuronal and glial prefrontal cellpathology in major depression. Biol Psychiatry 45:1085–1098.
eisberg B, Doody R, Stoffer A, Schmitt F, Ferris S, Mobius HJ (2003): Meman-tine in moderate-to-severe Alzheimer’s disease. N Engl J Med 348:1333–1341.
evicki DA, Matza LS, Flood E, Lloyd A (2005): Bipolar disorder and health-related quality of life:Review of burden of disease and clinical trials.Pharmacoeconomics 23:583–594.
iedel G, Platt B, Micheau J (2003): Glutamate receptor function in learning andmemory. Behav Brain Res 140:1–47.
ogoz Z, Skuza G, Maj J, Danysz W (2002): Synergistic effect of uncompetitiveNMDA receptor antagonists and antidepressant drugs in the forced swim-ming test in rats. Neuropharmacology 42:1024–1030.
ouaux C, Jokic N, Mbebi C, Boutillier S, Loeffler JP, Bouillier AL (2003):Critical loss of CBP/p300 histone deacetylase activity by caspase-6 dur-ing neurodegeneration. EMBO J 22:6537– 6549.
alinska E, Stafiej A (2003): Metabotropic glutamate receptors (mGluRs) areinvolved in early phase of memory formation: Possible role of modula-tion of glutamate release. Neurochem Int 43:469 – 474.
apolsky RM (2000): Glucocorticoids and hippocampal atrophy in neuropsy-chiatric disorders. Arch Gen Psychiatry 57:925–935.
apolsky RM (2004): Is impaired neurogenesis relevant to the affectivesymptoms of depression? Biol Psychiatry 56:137–139.
aunders J, Williams J (2003): Antagonists of the corticotropin releasingfactor receptor. Prog Med Chem 41:195–247.
chmidt PJ, Daly RC, Bloch M, Smith MJ, Danaceau MA, St Clair LS, et al(2005): Dehydroepiandrosterone monotherapy in midlife-onset majorand minor depression. Arch Gen Psychiatry 62:154 –162.
choepp DD (2001): Unveiling the functions of presynaptic metabotropicglutamate receptors in the central nervous system. J Pharmacol Exp Ther299:12–20.
eymour PA, Schmidt AW, Schulz DW (2003): The pharmacology of CP-154,526, a non-peptide antagonist of the CRH1 receptor: A review. CNSDrug Rev 9:57–96.
kolnick P, Legutko B, Li X, Bymaster FP (2001): Current perspectives on thedevelopment of non-biogenic amine-based antidepressants. PharmacolRes 43:411– 423.
pooren WP, Vassout A, Neijt HC, Kuhn R, Gasparini F, Roux S, et al (2000):Anxiolytic-like effects of the prototypical metabotropic glutamate re-ceptor 5 antagonist 2-methyl-6-(phenylethynyl)pyridine in rodents.J Pharmacol Exp Ther 295:1267–1275.
akahashi M, Terwilliger R, Lane C, Mezes PS, Conti M, Duman RS (1999): Chronicantidepressant administration increases the expression of cAMP-specificphosphodiesterase 4A and 4B isoforms. J Neurosci 19:610–618.
akata K, Kitamura Y, Kakimura J, Kohno Y, Taniguchi T (2000): Increase ofbcl-2 protein in neuronal dendritic processes of cerebral cortex and hip-pocampus by the antiparkinsonian drugs, talipexole and pramipexole.Brain Res 872:236–241.
an Y, Hori N, Carpenter DO (2003): The mechanism of presynaptic long-term depression mediated by group I metabotropic glutamate recep-
tors. Cell Mol Neurobiol 23:187–203.ww.sobp.org/journal
Tao X, Finkbeiner S, Arnold DB, Shaywitz AJ, Greenberg ME (1998): Ca2�influx regulates BDNF transcription by a CREB family transcription factor-dependent mechanism. Neuron 20:709 –726.
Tatarczynska E, Klodzinska A, Chojnacka-Wojcik E, Palucha A, Gasparini F,Kuhn R, Pilc A (2001): Potential anxiolytic- and antidepressant-like ef-fects of MPEP, a potent, selective and systemically active mGlu5 receptorantagonist. Br J Pharmacol 132:1423–1430.
Tatarczynska E, Klodzinska A, Kroczka B, Chojnacka-Wojcik E, Pilc A (2001):The antianxiety-like effects of antagonists of group I and agonists ofgroup II and III metabotropic glutamate receptors after intrahippocam-pal administration. Psychopharmacology (Berl) 158:94 –99.
Tohen M, Zarate CA Jr, Hennen J, Khalsa HM, Strakowski SM, Gebre-MedhinP, et al (2003): The McLean-Harvard First-Episode Mania Study: Predic-tion of recovery and first recurrence. Am J Psychiatry 160:2099 –2107.
Tremolizzo L, Doueiri MS, Dong E, Grayson DR, Davis J, Pinna G, et al (2005):Valproate corrects the schizophrenia-like epigenetic behavioral modifi-cations induced by methionine in mice. Biol Psychiatry 57:500 –509.
Tsai G, Coyle JT (1995): N-acetylaspartate in neuropsychiatric disorders. ProgNeurobiol 46:531–540.
Ullian EM, Sapperstein SK, Christopherson KS, Barres BA (2001): Control ofsynapse number by glia. Science 291:657– 661.
Wachtel H, Schneider HH (1986): Rolipram, a novel antidepressant drug,reverses the hypothermia and hypokinesia of monoamine-depletedmice by an action beyond postsynaptic monoamine receptors. Neuro-pharmacology 25:1119 –1126.
Wang SJ, Huang CC, Hsu KS, Tsai JJ, Gean PW (1996): Presynaptic inhibitionof excitatory neurotransmission by lamotrigine in the rat amygdalarneurons. Synapse 24:248 –255.
Watkins J, Collingridge G (1994): Phenylglycine derivatives as antagonists ofmetabotropic glutamate receptors. Trends Pharmacol Sci 15:333–342.
Watson S, Gallagher P, Ritchie JC, Ferrier IN, Young AH (2004): Hypothalamic-pituitary-adrenal axis function in patients with bipolar disorder. Br JPsychiatry 184:496 –502.
Weaver IC, Cervoni N, Champagne FA, D’Alessio AC, Sharma S, Seckl JR, et al(2004): Epigenetic programming by maternal behavior. Nat Neurosci7:847– 854.
Wheeler GD (2003): Ruboxistaurin (Eli Lilly). IDrugs 6:159 –163.Wilson BE, Mochon E, Boxer LM (1996): Induction of bcl–2 expression by
phosphorylated CREB proteins during B-cell activation and rescue formapoptosis. Mol Cell Biol 16:5546 –5556.
Young AH, Gallagher P, Watson S, Del-Estal D, Owen BM, Nicol Ferrier I(2004): Improvements in neurocognitive function and mood followingadjunctive treatment with mifepristone (RU-486) in bipolar disorder.Neuropsychopharmacology 29:1538 –1545.
Young LT (2002): Neuroprotective effects of antidepressant and mood sta-bilizing drugs. J Psychiatry Neurosci 27:8 –9.
Young LT, Wang JF, Woods CM, Robb JC (1999): Platelet protein kinase Calpha levels in drug-free and lithium-treated subjects with bipolar disor-der. Neuropsychobiology 40:63– 66.
Zarate CA Jr, Payne JL, Quiroz J, Sporn J, Denicoff KK, Luckenbaugh D, et al(2004a): An open-label trial of riluzole in patients with treatment-resis-tant major depression. Am J Psychiatry 161:171–174.
Zarate CA Jr, Payne JL, Singh J, Quiroz JA, Luckenbaugh DA, Denicoff KD,et al (2004b): Pramipexole for bipolar II depression: A placebo-controlledproof of concept study. Biol Psychiatry 56:54 – 60.
Zarate CA, Quiroz J, Payne J, Manji HK (2002): Modulators of the glutamater-gic system: Implications for the development of improved therapeuticsin mood disorders. Psychopharmacol Bull 36:35– 83.
Zarate CAJ, Singh J, Quiroz J, Denicoff KD, De Jesus G, Luckenbaugh D, et al(2006): Memantine in major depression: a double-blind placebo-con-trolled study. Am J Psychiatry 163:153–155.
Zobel AW, Nickel T, Kunzel HE, Ackl N, Sonntag A, Ising M, Holsboer F (2000):Effects of the high-affinity corticotropin-releasing hormone receptor 1
antagonist R121919 in major depression: The first 20 patients treated.J Psychiatr Res 34:171–181.