centrally acting analgesics opioids biomedicine spring 08 year 2 no 2 frågor till [email protected]
Post on 19-Dec-2015
216 views
TRANSCRIPT

Centrally acting analgesicsCentrally acting analgesicsOpioidsOpioids
Biomedicine spring 08Biomedicine spring 08Year 2 no 2Year 2 no 2
Frågor till [email protected]ågor till [email protected]
Pain medicationPain medication
ParacetamolParacetamol
NSAIDsNSAIDs
OpioidsOpioids
Steroids, radiation, TENS, acupuncture Steroids, radiation, TENS, acupuncture
PhysiologyPhysiology
Afferent, peripheral nerves C and AAfferent, peripheral nerves C and A
C-fibresC-fibres 0,5-1,5 0,5-1,5 m, <1 m/s, m, <1 m/s, unmyelinatedunmyelinated
AA-fibrer-fibrer1-5 1-5 m, 5-35 m/s, myelinatedm, 5-35 m/s, myelinated
(larger A(larger Atouch, vibration, proprioception)touch, vibration, proprioception)



Pain pathwaysPain pathways
Tissue damage releases bradykinin, serotonin, histamin, Tissue damage releases bradykinin, serotonin, histamin, lactate, ATP, ADP, potassium (among others) lactate, ATP, ADP, potassium (among others)
Glutamate (excitatory) transmittor in dorsal horn synapseGlutamate (excitatory) transmittor in dorsal horn synapse
GABA (inhibitory) transmittor interneuronGABA (inhibitory) transmittor interneuron

Pain, pathwaysPain, pathways
Nociceptive neurons in dorsal root ganglionNociceptive neurons in dorsal root ganglion Relays via tractus spinothalamicus, Relays via tractus spinothalamicus,
spinomesencephalicus and spinoreticularisspinomesencephalicus and spinoreticularis Reaches thalamus and ponsReaches thalamus and pons Connects to cortexConnects to cortex Inhibitory neuronsInhibitory neurons Inhibitory mechanoreceptorsInhibitory mechanoreceptors

Pain, pathwaysPain, pathways
Brain - upwards probably glutamat main Brain - upwards probably glutamat main transmittortransmittor
Downwards neurons GABA, ACh, Downwards neurons GABA, ACh, monoamines (serotonin, NA, DA).monoamines (serotonin, NA, DA).

Endogenous opioidsEndogenous opioids
Endorphin, enkephalin, dynorphinEndorphin, enkephalin, dynorphin
Spinal tract dynorphin interneuron, Spinal tract dynorphin interneuron, enkephalin downward inhibitory neurons.enkephalin downward inhibitory neurons.
In brain around ”pain centre” but also in In brain around ”pain centre” but also in areas not involved in nociception and non-areas not involved in nociception and non-neuronal tissuesneuronal tissues

Opioid receptorOpioid receptor
Receptors in brain and spinal cordReceptors in brain and spinal cord4 subtypes: 4 subtypes: (my)(my)and NOP (ORL-1)and NOP (ORL-1)

Opioid receptorOpioid receptor
G-proteinG-protein Intra/extracellular, intramembranousIntra/extracellular, intramembranousPre- and postsynaptic membranesPre- and postsynaptic membranes

NMDA-receptorNMDA-receptorN-metyl-D-AspartateN-metyl-D-AspartateLearningLearningActivation makes spinal neurons more Activation makes spinal neurons more
sensitive to pain stimulussensitive to pain stimulusLong-term C-fiberstimulation activates Long-term C-fiberstimulation activates
NMDA NMDA central sensitisation central sensitisationNMDA-antagonistsNMDA-antagonists

GlutamatGlutamat
Presynaptic ion channel calcium influx Presynaptic ion channel calcium influx glutamat releaseglutamat release
Crosses synapse and binds to NMDA-Crosses synapse and binds to NMDA-receptors postsynapticly receptors postsynapticly depolarisation depolarisation hyperexcitability in nociceptive neurons hyperexcitability in nociceptive neurons


Pre- and postsynaptic bindingPre- and postsynaptic binding
G-protein inhibits adenylate cyclaseG-protein inhibits adenylate cyclase
Lower content intracellular cAMPLower content intracellular cAMP
Opens KOpens K++, inhibits Ca, inhibits Ca2+2+
Inhibits pre-synaptic release of glutamatInhibits pre-synaptic release of glutamat

The opioid receptorThe opioid receptor
The opioid receptorThe opioid receptor
, , , , identical around 70%identical around 70% G-protein binds to 3rd receptor loopG-protein binds to 3rd receptor loop

The opioid receptor The opioid receptor (mu)(mu)
Mainly analgesic effectsMainly analgesic effects Respiratory depressionRespiratory depression Nausea / vomitingNausea / vomiting ConstipationConstipation Cough reflexCough reflex EuphoriaEuphoria AddictionAddiction SedationSedation Most analgesic opioids are Most analgesic opioids are -agonists-agonists

The opioid receptor The opioid receptor (delta) (delta)
Probably effects outside the CNSProbably effects outside the CNS
Some analgetic effektsSome analgetic effekts
Seizures?Seizures?
Least knowledgeLeast knowledge
The opioid receptor The opioid receptor (kappa) (kappa)
Analgesia on mainly spinal cord levelAnalgesia on mainly spinal cord level
Nausea and dysphoria Nausea and dysphoria
Psychotomimetic effects – limits abuse Psychotomimetic effects – limits abuse potentialpotential


Side effects - mechanismsSide effects - mechanisms
Respiratory depressionRespiratory depressionRespiratory centre (medulla oblongata) Respiratory centre (medulla oblongata)
Less COLess CO2 2 stimulationstimulation
Decreased respiratory rateDecreased respiratory rate Nausea / vomitingNausea / vomiting
Area postrema (medulla oblongata) Area postrema (medulla oblongata) (triggerzone vomiting reflex)(triggerzone vomiting reflex)
Stimulation of DA-receptorsStimulation of DA-receptorsStimulation mechano/chemoreceptors GI Stimulation mechano/chemoreceptors GI tracttract
Side effects - mechanismsSide effects - mechanisms
ConstipationConstipationperipheral and central affection peripheral and central affection less GI movement and increased less GI movement and increased
tonus tonus No toleransNo toleransLaxatives necessaryLaxatives necessaryPeroral naloxone possiblePeroral naloxone possible
ItchingItchingHistamine release or centrally Histamine release or centrally
mediatedmediated

Side effects - MechanismsSide effects - Mechanisms
SedationSedationOverdoseOverdose
Wrong strategyWrong strategy
Sleep deptSleep dept


DrugsDrugs
Agonists (Agonists (-receptors)-receptors)morphine, metadon, fentanyl, heroin morphine, metadon, fentanyl, heroin
Partial agonistsPartial agonistsbuprenorfin, kodein, tramadolbuprenorfin, kodein, tramadol
AntagonistAntagonistnaloxone naloxone

What is an opioid?What is an opioid?
Alkaloid (plant) or syntheticAlkaloid (plant) or synthetic
Morphine like effekts, inhibited by naloxonMorphine like effekts, inhibited by naloxon
OpiumOpium
Narcotic resin from opium poppies:Narcotic resin from opium poppies:morphine 10%, noskapin 6%, papaverin 1%, kodein morphine 10%, noskapin 6%, papaverin 1%, kodein 0,5% 0,5%

HistoryHistory
3400 BC3400 BCOpium puppies grown in Mesopotamia Opium puppies grown in Mesopotamia
460 BC460 BCHippocrates medicine (psychiatric disease Hippocrates medicine (psychiatric disease and epidemies)and epidemies)

HistoryHistory 330 BC330 BC
Alexander the Great introduces opium to Persia Alexander the Great introduces opium to Persia and Indiaand India
400 AD400 ADOpium with traders to ChinaOpium with traders to China
Parcelsus (1490-1541) opium as medicineParcelsus (1490-1541) opium as medicine
Laudanum (opium, sherry, cinnamon, clove bud Laudanum (opium, sherry, cinnamon, clove bud oil, saffron) 17th centuryoil, saffron) 17th century
HistoryHistory
Morphin 1806Morphin 1806Kodein 1832Kodein 1832Heroin 1832Heroin 1832


MorphinMorphin
CC1717HH1919NONO33
Greek. Morpheus (God of dreams)Greek. Morpheus (God of dreams) 1806 from opium1806 from opium 1956 chemical structure1956 chemical structure
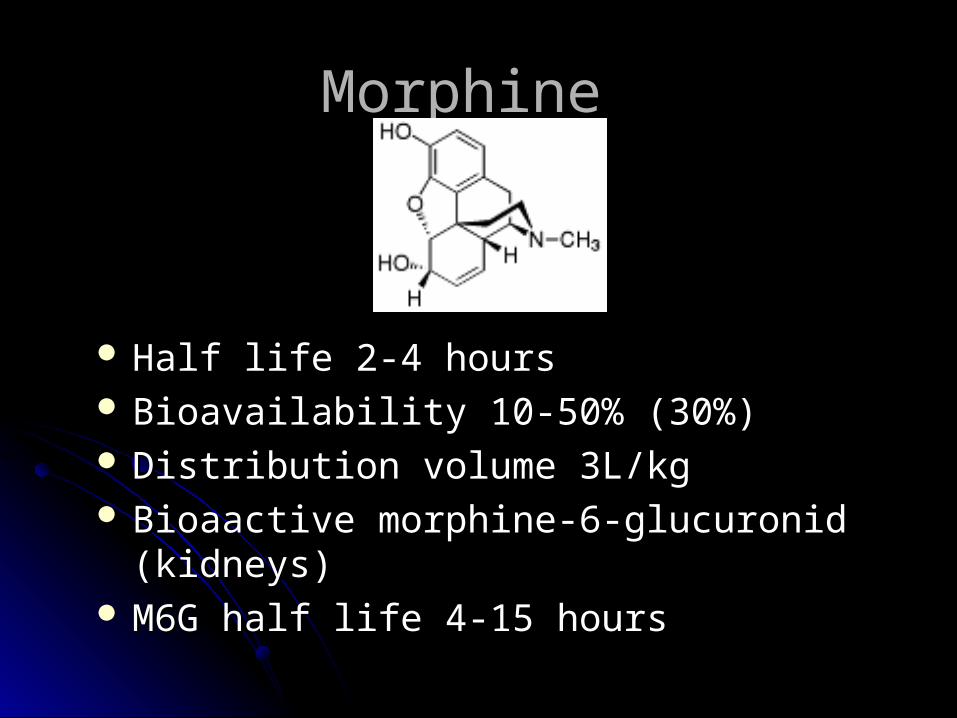
Morphine Morphine
Half life 2-4 hoursHalf life 2-4 hours Bioavailability 10-50% (30%)Bioavailability 10-50% (30%) Distribution volume 3L/kgDistribution volume 3L/kg Bioaactive morphine-6-glucuronid (kidneys)Bioaactive morphine-6-glucuronid (kidneys) M6G half life 4-15 hoursM6G half life 4-15 hours

HeroinHeroin CC2121HH2323NONO5 5 (morphin (morphin
CC1717HH1919NONO33)) Higher fat solubilityHigher fat solubility Produced 1874Produced 1874 Bayer 1899 Bayer 1899 Drug Sweden until Drug Sweden until
1964 1964 Half life 30 minutesHalf life 30 minutes MorphineMorphine

KodeinKodein
CC1818HH2121NONO3 3 (morfin C(morfin C1717HH1919NONO33))Produced 1832Produced 1832Low receptor affinityLow receptor affinity10% into morphine 10% into morphine M6G M6G7-10% non-responders 7-10% non-responders Half life 2-4 hours.Half life 2-4 hours.10 mg morfin 10 mg morfin Kodein 60mg Kodein 60mg

DextropropoxifenDextropropoxifen
Half time 8-18 (90) hoursHalf time 8-18 (90) hoursActive metabolite norpropoxyfenActive metabolite norpropoxyfenMetabolite half life 30-45 (100) hoursMetabolite half life 30-45 (100) hoursAlcohol enhances respiratory inhibitionAlcohol enhances respiratory inhibition10mg morfin 10mg morfin 100mg Dextropropoxifen 100mg Dextropropoxifen

TramadolTramadol
Halflife 4-6 hoursHalflife 4-6 hoursActive metabolite D-desmetyltramadolActive metabolite D-desmetyltramadolHalflife metabolite 9-12 hoursHalflife metabolite 9-12 hours5-10% non-responders5-10% non-responders Inhibits reuptake NA / 5-HTInhibits reuptake NA / 5-HT


FentanylFentanyl
””Complicated kinetics” Complicated kinetics” Halflife 1 min, 8 min, 8 timHalflife 1 min, 8 min, 8 timActive metabolites unknownActive metabolites unknown10mg morfin 10mg morfin 0,05 mg fentanyl (iv) 0,05 mg fentanyl (iv)
PethidinePethidine
synthetic opioidsynthetic opioid
Most histamine release. Seizures.Most histamine release. Seizures.
100mg 100mg 10mg morphine 10mg morphine
Shivering Shivering

KetoganKetogan
Ketobemidon(hydroklorid)Ketobemidon(hydroklorid)NMDA – receptor antagonist?NMDA – receptor antagonist?Halflife 2-4 hoursHalflife 2-4 hoursUnknown metabolite activityUnknown metabolite activityAbuse riskAbuse risk ””Less documented morphine alternative”Less documented morphine alternative” ””only” indication only” indication renal failure (+NMDA?) renal failure (+NMDA?)10mg morphine 10mg morphine 10mg ketobemidon 10mg ketobemidon

OxicodonOxicodon
Halflife 2-4 timmarHalflife 2-4 timmarProbably inaktiva metaboliterProbably inaktiva metaboliter10mg morfin 10mg morfin 5mg oxikodon 5mg oxikodon


MetadonMetadon
NMDA-receptor antagonist ?NMDA-receptor antagonist ?Halflife 15-40 hoursHalflife 15-40 hours ””Bad reputation” Bad reputation” Advanced pain treatmentAdvanced pain treatment

Clinical useClinical use
Cancer painCancer painPostoperative painPostoperative painLong-term pain ?Long-term pain ?Neurogenic pain?Neurogenic pain? ””Always” in combination with paracetamol Always” in combination with paracetamol
and NSAIDand NSAIDElderly ?Elderly ?Try not to mix different opioidsTry not to mix different opioids
IntoxicationIntoxication
Mios (small pupils)Mios (small pupils)Lower conscienceLower conscienceBreathingBreathing

Antidote – Naloxone (Narcanti)Antidote – Naloxone (Narcanti)
opioid antagonistopioid antagonist reverses endogenous and exogenous reverses endogenous and exogenous
substanses and acupuncturesubstanses and acupunctureeffect within 2 minuteseffect within 2 minutes IteratedIterated iv + im when abuse overdoseiv + im when abuse overdose

AbstinenceAbstinence
sweating, fever (”cold turkey”), shakings, sweating, fever (”cold turkey”), shakings, muscular cramps, itching, diarrhea, muscular cramps, itching, diarrhea, nausea, vomiting (the flu)nausea, vomiting (the flu)
At pain treatment because of to quick At pain treatment because of to quick withdrawal withdrawal re-medicate! re-medicate!

Cold CaseCold Case
CancerCancerCurrent medication:Current medication:
Tb. Dolcontin (longacting morphine) Tb. Dolcontin (longacting morphine) 60mgx260mgx2Tb. Morphine (shortacting) 20mg as req.Tb. Morphine (shortacting) 20mg as req.inj. Ketogan 5mgvbinj. Ketogan 5mgvbTb. Tramadol 100mgx2Tb. Tramadol 100mgx2
Pain. What to do?Pain. What to do?
PatientfallPatientfall
Patient insatt på Ketogan tablett 5mgx6 Patient insatt på Ketogan tablett 5mgx6 med god effekt. Översatt till Dolcontin med god effekt. Översatt till Dolcontin 20mgx2. Inkommer efter 1 vecka till 20mgx2. Inkommer efter 1 vecka till akuten: illamående, kräkningakuten: illamående, kräkning
Diffdiagnos (opioidrelaterat) ?Diffdiagnos (opioidrelaterat) ?Ytterligare status etc?Ytterligare status etc?Vad göra?Vad göra?


Afterlife …..Afterlife …..
Morphina is currently Golden StandardMorphina is currently Golden Standard
Renal failureRenal failure
Treat pain! Treat pain!