cerebral palsy
TRANSCRIPT

CEREBRAL PALSY
Dr Alpana KondekarAssistant Professor, Pediatric Neurodevlopmental Clinic
Faculty –Autism screening and CertificationDepartment of PediatricsT.N.M.C & B.Y.L.Nair Hospital
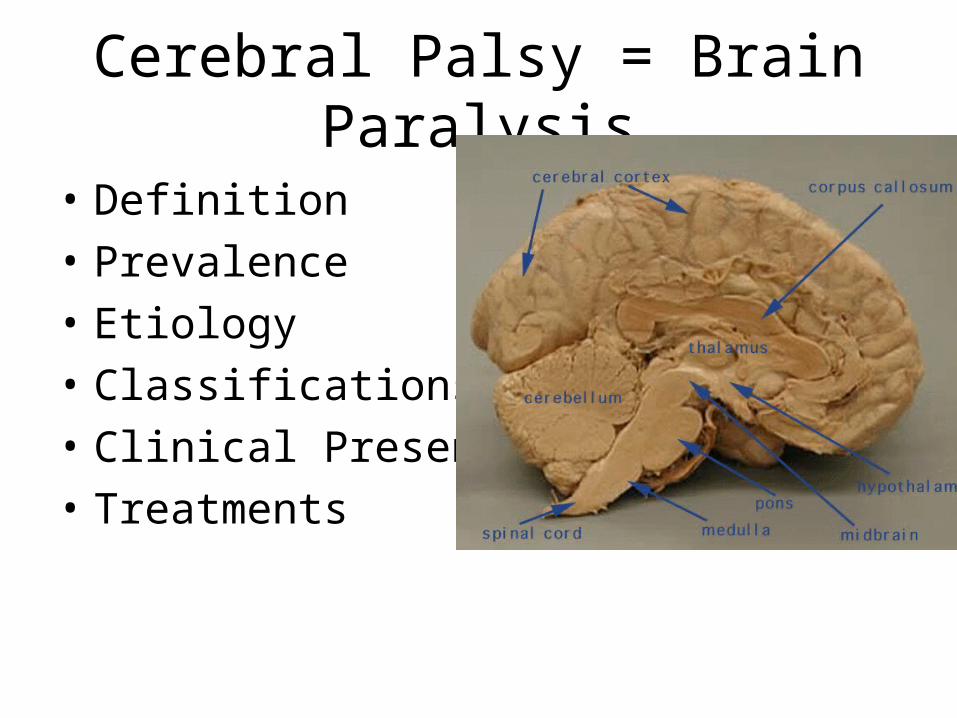
Cerebral Palsy = Brain Paralysis
• Definition• Prevalence• Etiology• Classifications• Clinical Presentation• Treatments

Cerebral Palsy: Definition• Cerebral palsy is a static encephalopathy that is non-progressive disorder
of posture and movement of Variable etiologies• Often associated with epilepsy, speech problems, vision compromise, &
cognitive dysfunction
• In all cases the following must be true…• Cerebral palsy is the result of a brain lesion. Therefore, the spinal cord and
muscles are structurally and biochemically normal.• The brain lesion must be fixed and non progressive. Thus, all of the
progressive neuro degenerative disorders are excluded from the definition.
• The abnormality of the brain result in motor impairment.
Cerebral Palsy: Prevalence
• 2-4/1000; 7-10,000 new babies each yr• 150 years ago described by Dr. Little an
orthopedic surgeon and known as Little’s Disease
• During past 3 decades considerable advances made in obstetric & neonatal care, but unfortunately there has been virtually no change in incident of CP

Cerebral Palsy: Etiologic
• Prenatal (70%)Infection, anoxia, toxic, vascular, Rh disease, genetic, congenital malformation of brain
• Perinatal (5-10%)Anoxia, traumatic delivery, metabolic,Fetal distress,Premature delivery,
• Post natalTrauma, infection, Sepsis in neonatal period,Bronchopulmonary dysplasia and prolonged ventilation in preterm infants.
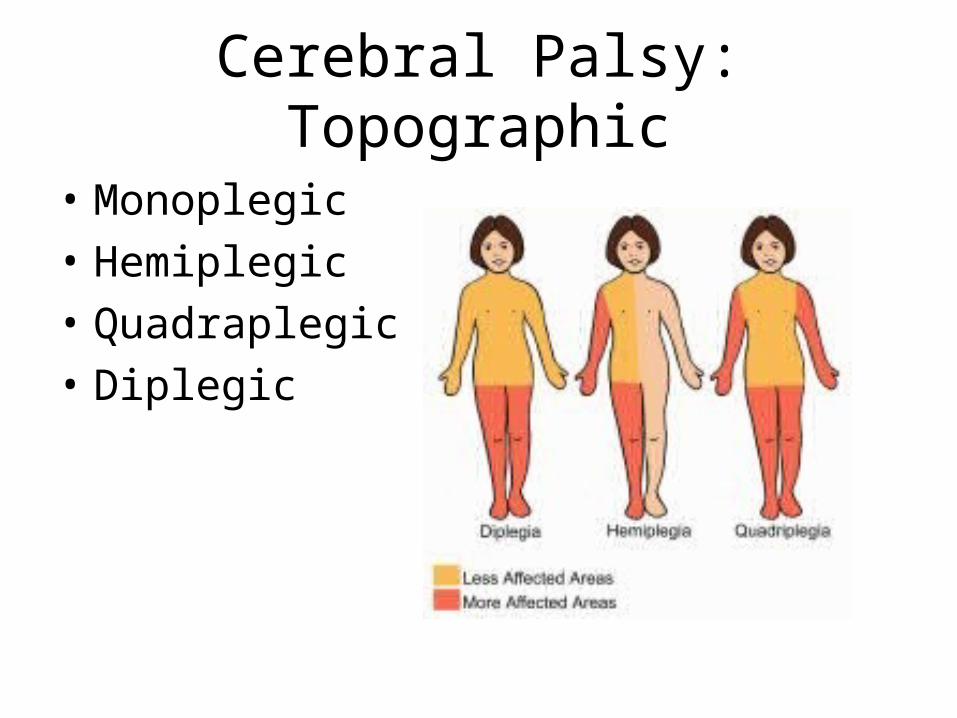
Cerebral Palsy: Topographic
• Monoplegic• Hemiplegic• Quadraplegic• Diplegic



Cerebral Palsy: Classification• 1. Spastic (70-80% of cases). Further classified by the following
descriptions of extremity involvement: a) Quadriplegia (10-15%): All 4 extremities are
affected equally along with the trunk b) Diplegia (30-40%): Lower extremities are affected
to a greater degree than the upper extremities c) Hemiplegia (20-30%): Involvement is observed on 1
side of the body, including an arm and a leg d) Monoplegia (rare): Involvement is noted in 1 limb,
either an arm or a leg • 2. Dyskinetic (10-15% of cases). Characterized by abnormal
movements• 3. Ataxic (<5% of cases). Characterized by unsteadiness

Spastic hemiplegic CP
• One-sided upper motor neuron deficit • Arm generally affected more than leg; possible early hand
preference or relative weakness on one side; gait possibly characterized by circumduction of lower extremity on affected side
• Specific learning disabilities • Oromotor dysfunction • Possible unilateral sensory deficits • Visual-field deficits (eg, homonymous hemianopsia) and
strabismus • Seizures


Spastic diplegic CP
• Upper motor neuron findings in the legs more than the arms
• Scissoring gait pattern with hips flexed and adducted, knees flexed with valgus, and ankles in equinus, resulting in toe walking
• Learning disabilities and seizures less commonly than in spastic hemiplegia


Spastic quadriplegic CP
• All limbs affected, either full-body hypertonia or truncal hypotonia with extremity hypertonia
• Oromotor dysfunction • Increased risk of cognitive difficulties • Multiple medical complications Seizures • Legs generally affected equally or more than arms • Categorized as double hemiplegic if arms more
involved than legs
Dyskinetic (extrapyramidal) CP• Early hypotonia with movement disorder emerging
at age 1-3 years • Arms more affected than legs • Deep tendon reflexes usually normal to slightly
increased • Some spasticity • Oromotor dysfunction • Gait difficulties • Truncal instability • Risk of deafness in those affected by kernicterus
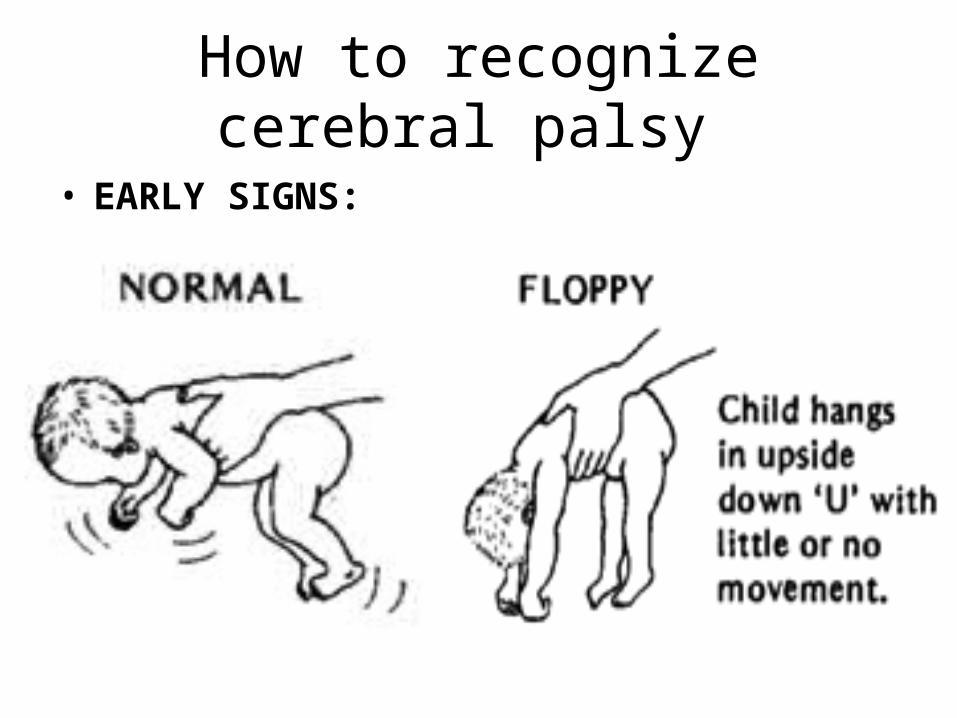
How to recognize cerebral palsy
• EARLY SIGNS:

• Slow development • Hand preference

• Feeding problems • Difficulty in putting the diaper

• Communication difficulties
• Hearing difficulties
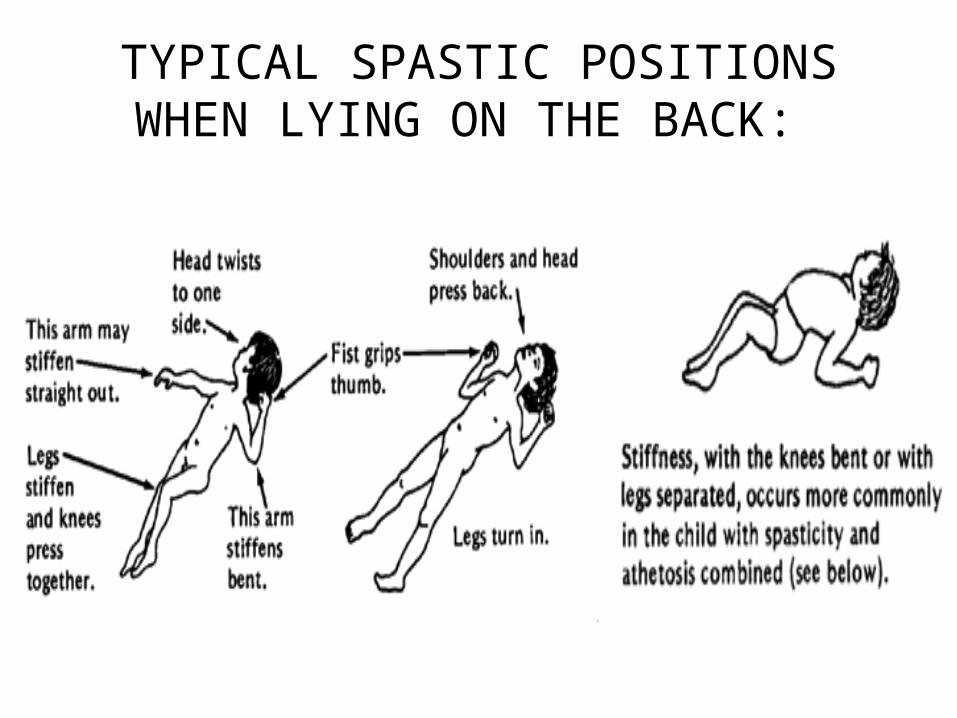
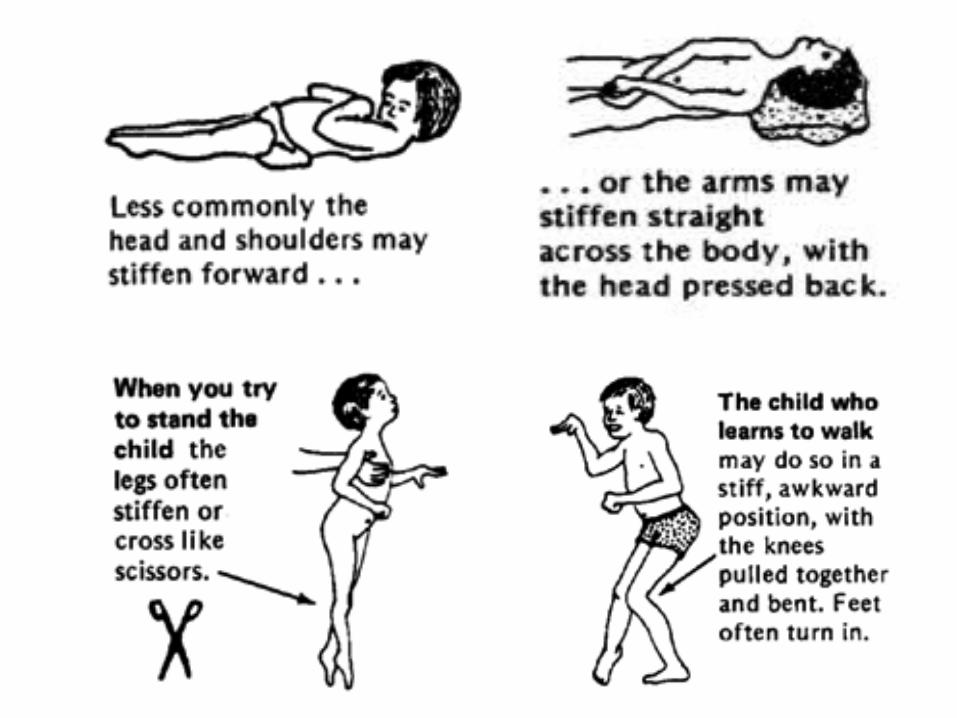
TYPICAL SPASTIC POSITIONS WHEN LYING ON THE BACK:

Cerebral Palsy: Complications
• Spasticity• Weakness• Increase reflexes• Clonus• Seizures• Articulation &
Swallowing difficulty
• Visual compromise• Deformation• Hip dislocation• Kyphoscoliosis• Constipation• Urinary tract infection
What is not a cerebral palsy ?

Mimics of Cerebral Palsy:Conditions• presenting with true muscle weakness
– Muscular dystrophies: Duchenne and Becker types– Infantile neuro-axonal dystrophy– Mitochondrial cytopathies– Cerebral white matter diseases may present in the first year with hypotonia and
developmental delay, with spasticity and metal retardation occurring later.• Conditions with significant dystonia or involuntary movements:
– DOPA responsive dystonia– Hallervordan Spatz Disease– Pyruvate dehydrogenase deficiency– Glutaric aciduria type I– Leigh syndrome– Juvenile neuronal ceroid lipofuscinosis– Rett syndrome– Pelizaeus-Merzbacher disease– Lesch Nyhan Syndrome
Mimics of Cerebral Palsy:Conditions
Conditions with predominant diplegia or quadriplegia:AdrenoleukodystrophyAdrenomyeloneuropathyArginase deficiencyMetachromatic leukodystrophyHereditary progressive spastic paraplegiaHolocarboxylase synthetase deficiencyPrenatal iodine deficiency ("neurological cretinism")
Conditions with ataxia (Ataxic CP is Rare)Angelman syndromeNiemann-Pick disease type CAtaxia-telangiectasia (Louis-Barr syndrome)Ponto-cerebellar hypoplasia or atrophyChronic/adult GM2 gangliosidosisMitochondrial cytopathy (NARP mutation)Posterior fossa tumoursX-linked spino-cerebellar ataxia

Evaluation Detailed history, including birth, family, developmental history, and physical examDeveopmental evaluationScreening for sensory deficit
Neuroimaging? CT scan (77% abnormal yield) –useful if abnormal, potentially treatable lesion (e.g. Hydrocephalus, AVM) MRI (89% abnormal yield)—higher abnormal yield that CT, useful to pinpoint timing of brain injury (pre/peri/postnatal), often suggests etiology.
Metabolic and genetic testing? (Hyperarginemia, glutaric acidurea, and homocystinurea are among common treatable metabolic causes of cerebral palsy). Coagulation studies? hemiplegic CP

Cerebral Palsy
• Mobility• Communication• Learning• Self Care• Self Direction• Independent Living• Economic Sufficiency
Current scenario in India
The usual medical advice currently given to parents of children with CP is one of the following:
• CP is incurable: so don't waste money on treatment. • Unsubstantiated but well publicised alternative
modalities claiming to "cure the brain without side-effects", e.g., homeopathy, herbal or biochemic pills, oil massges or biofeedback
• Refer to physiotherapist for further management and physicians take no further active role in treatment

The team of medical professionals who are going to treat a child with CP must have:
• Knowledge of normal anatomy and physiology, particularly with respect to ambulation
• A good understanding of the functional pathology present in CP
• Realistic goals / objectives for treatment that are shared commonly by the patient, family, and others concerned with the child's welfare
• Knowledge and ability to carry out any of the treatments that are required
• A facility with the resources to carry out the necessary evaluations / treatments
Cerebral Palsy: Management
• Neurologic and Physiatric• OT and PT• Speech• Adaptive equipment• Surgical• Rhizotomy, Baclofen pumps, Botoxin

Multidisciplinary CP clinics
centers that provide a dedicated, trained and qualified multidisciplinary team comprising of,
1. Developmental Pediatrician, 2. Pediatric Orthopedic Surgeon,3. Pediatric Neurologist4. Neurosurgeon,5. Physiotherapist, 6. Occupational Therapist and Orthotist.
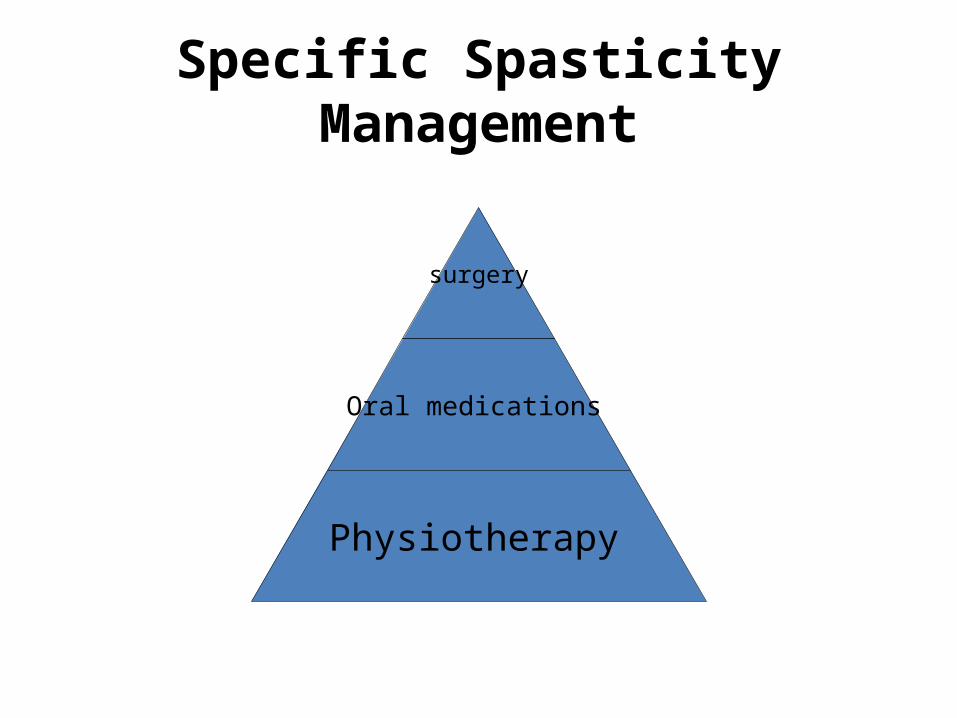
Specific Spasticity Management
surgery
Oral medications
Physiotherapy

Cerebral palsy
Clinical AssessmentHip Adductors
Hip abduction / knees extended Hip abduction / knees flexedThe Gracilis
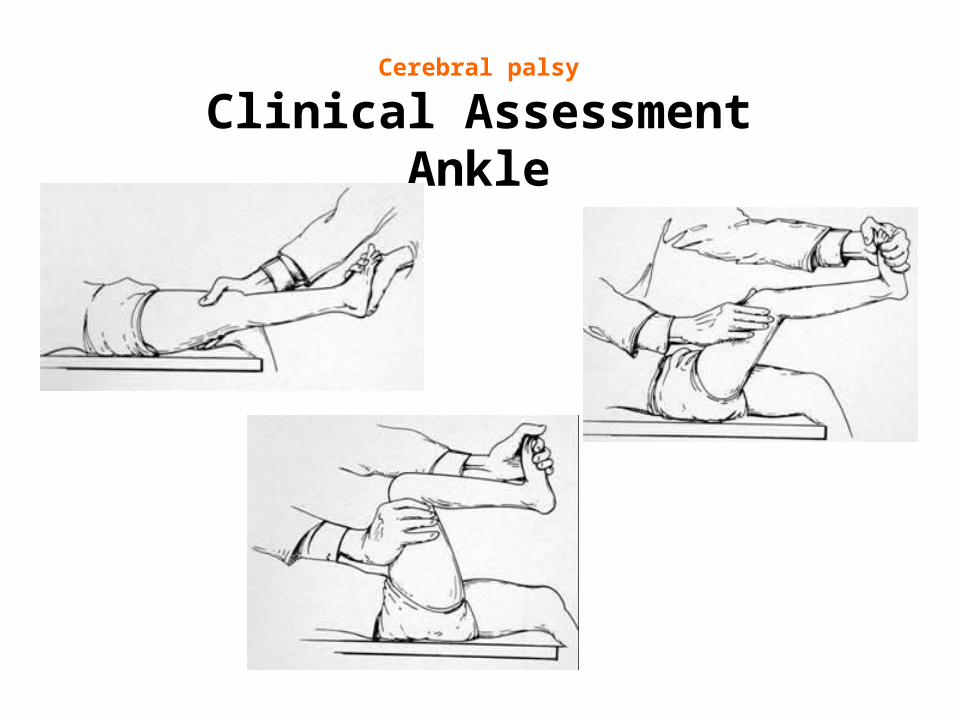
Cerebral palsy
Clinical AssessmentAnkle

Modified ashworth scale00 No increase in muscle toneNo increase in muscle tone
11 Slight increase in muscle tone, manifested by a catch and Slight increase in muscle tone, manifested by a catch and release or by minimal resistance at the end range of motion release or by minimal resistance at the end range of motion when the part is moved in flexion or extension/abduction or when the part is moved in flexion or extension/abduction or adduction, etc.adduction, etc.
1+1+ Slight increase in muscle tone, manifested by a catch, followed Slight increase in muscle tone, manifested by a catch, followed by minimal resistance throughout the remainder (less than by minimal resistance throughout the remainder (less than half) of the ROMhalf) of the ROM
22 More marked increase in muscle tone through most of the More marked increase in muscle tone through most of the ROM, but the affected part is easily movedROM, but the affected part is easily moved
33 Considerable increase in muscle tone, passive movement is Considerable increase in muscle tone, passive movement is difficultdifficult
44 Affected part is rigid in flexion or extension (abduction or Affected part is rigid in flexion or extension (abduction or adduction, etc.)adduction, etc.)

Gross motor functional classification score
Level-ILevel-I Minimal restriction of activityMinimal restriction of activity
Level-IILevel-II Activities carried out with minimal assistance Activities carried out with minimal assistance or supportor support
Level-IIILevel-III Activities carried out with the help of assisted Activities carried out with the help of assisted mobility devices.mobility devices.
Level-IVLevel-IV Can function in sitting, but require extensive Can function in sitting, but require extensive use of mobility devices-limited independence.use of mobility devices-limited independence.
Level-VLevel-V Lack of independence even in basic Lack of independence even in basic antigravity postural control.antigravity postural control.

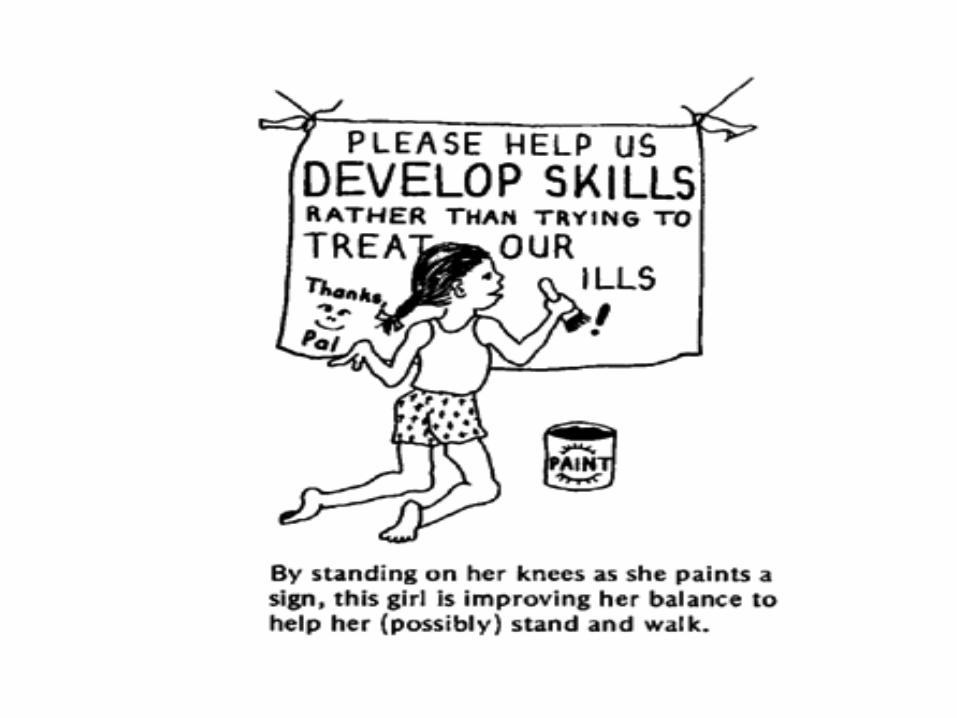
Physical therapyAim
• To help child reach his or her maximum potential for functional independence through a variety of approaches including, exercise, mobility training ,orthotics or braces, and use of other equipment.
• Muscle training and exercises may help child's strength, flexibility, balance, motor development and mobility, as well as ease caregiving.
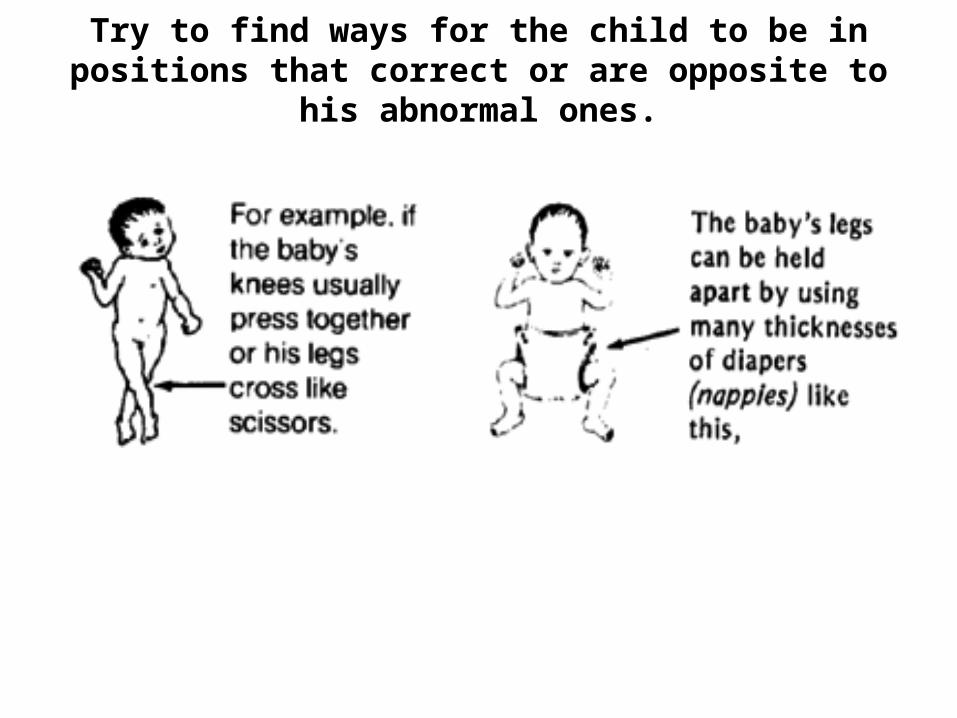
Try to find ways for the child to be in positions that correct or are opposite to his abnormal ones.



Oral Pharmacotherapy:Trihexyphenidyl
Can be useful in children with dystonia Suppresses an overactivity of central cholinergic
effects in dystonia Dosage: start at a low dosage and work up every
two weeks (0.5 mg bid - work up to tid and increase until effect noted) - can get up to doses of 40 mg
Side Effects: constipation, urinary retention
Botulinum toxin injection
• 2-8 years of age with relatively mild global spasticity• lower extremity spasticity that causes difficulty with
walking.• Children > approximately 4 years of age who have
severe spasticity in a localized area.• Rated I or II on GMFCS** if difficulty is in lower
extremities.• Rated I to V on GMFCS** if difficulty is in upper
extremities.

Dosing Guideline RecommendationsBiceps: 1U/kgBrachioradialis: 0.75U/kgFinger/Wrist Flexors: 1.5U/kgPronator teres: 0.75U/kgThumb adductor: 0.3U/kg (max 10U)Thumb opponens: 0.3U/kg (max 10U)

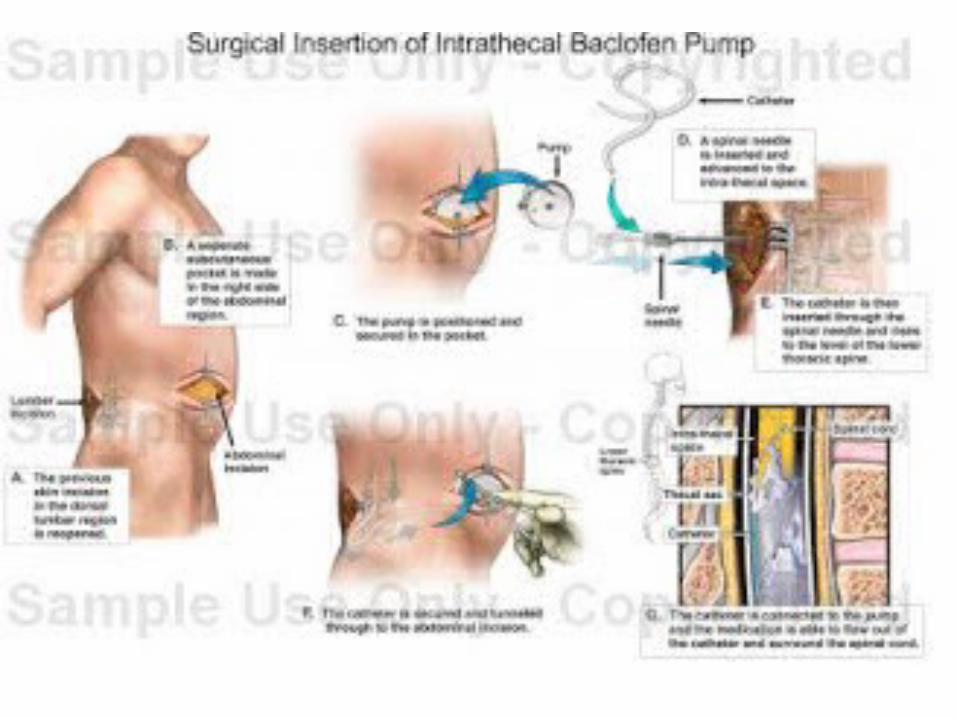
Baclofen pump
• Children approximately 3 years of age and older who are large enough to accommodate an abdominal implant.
• Severe spasticity that causes pain or major positioning or care problems.
• Children with spasticity that is greater in lower extremities or who have a
• combination of other movement disorders and spasticity.
• • Rated Level IV or V on GMFCS.**

Occupational therapy.
• Focus on the development of fine motor skills and self-care skills. Using exercises, facilitated practice, alternative strategies and adaptive equipment.
• To promote child's independent participation in daily activities and routines in the home, school and community.
• Also address difficulties with feeding and swallowing.

Speech therapy.• A speech therapist works with child on both the
receptive (understanding) part of speech and language as well as the expressive part (talking).
• Speech therapists help improve child's ability to speak clearly or communicate using alternative means such as an augmentative communication device or sign language.
• Speech therapists may also help with difficulties related to feeding and swallowing.

Hearing Problems
• Hearing impairment is very common in children with CP; (sensorineural loss or secretory otitis media or both ).
• A complete evaluation by an audiologist and speech pathologist is needed in all children with CP.
• Brain stem evoked responses may help in children who are too young or are unable to co-operate for audiometry.
• Early use of hearing aids and speech stimulation techniques can help prevent or minimize speech and language problems. Appropriate speech therapy is needed for children with speech problems

Orthopedic Surgery.Deformity Commonly done procedure Hip flexion (Fixed flexion deformity > 15 degrees)
Lengthening of Ilio-psoas tendon at insertion to lesser trochanter
Hip adduction (Passive hip abduction after Medial Hamstring lengthening of < 30 degrees)
Adductor tenotomy and Obturator neurectomy
Knee flexion (Popliteal angle > 40 degrees under anaesthesia)
Eggers procedure (transfer of Hamstrings to femoral condyle)
Increased femoral anteversion (Internal rotation gait and external rotation in extension < 30 degrees, with excessive internal rotation of hip)
Adductor tenotomy and Obturator neurectomy (for a presumed scissoring gait)

Deformity Commonly done procedure
Tibial torsion, usually external (tibial rotation deformity > 20 degrees, measured with knee in 90 degree flexion)
Tibial derotational osteotomy
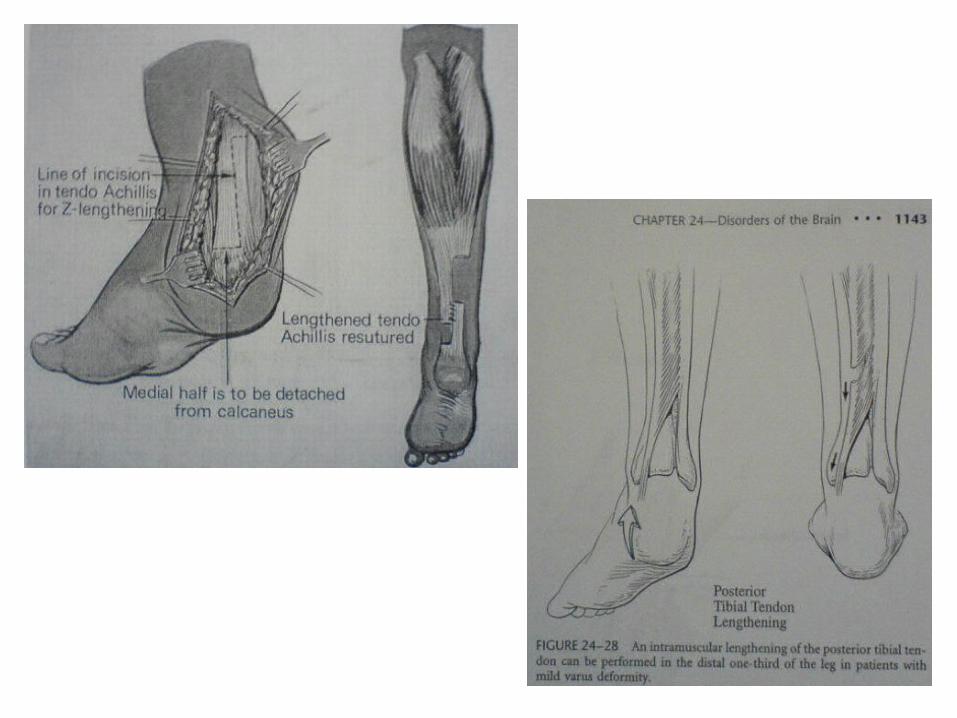
Ankle plantarflexion (equines not correctable to neutral under anaesthesia)
Open z-lengthening of Tendoachilles
Talipes Equinovalgus Grice procedure (Extra-articular fusion of subtalar joint)
Talipes Equinovarus Transfer of Tibialis Anterior or Posterior
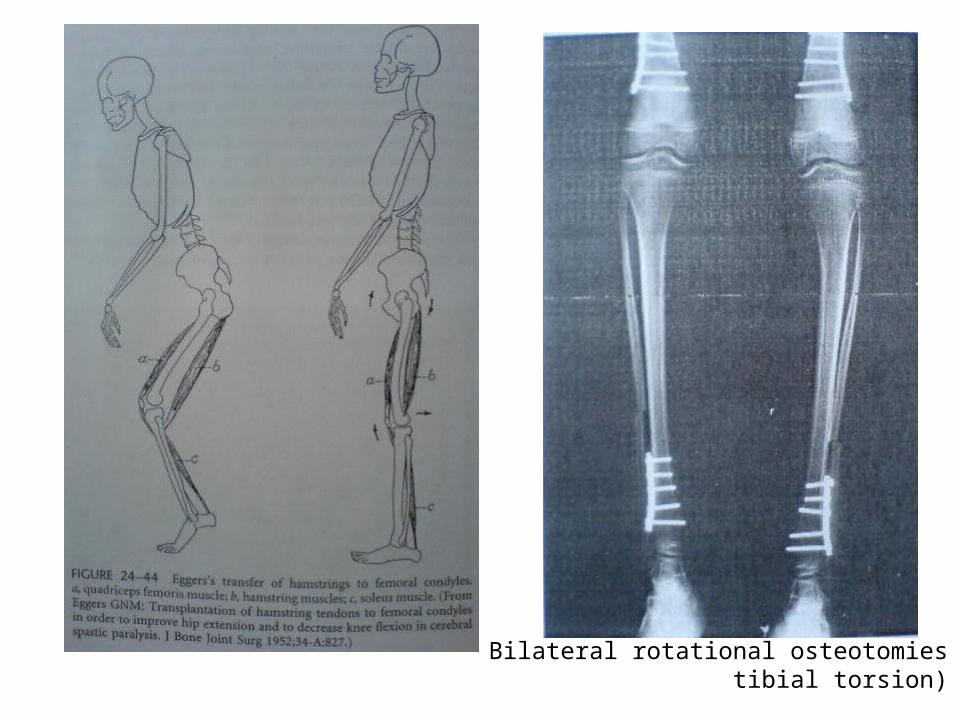
Bilateral rotational osteotomies(tibial torsion
Neurosurgery –Selective Dorsal Rhizotomy (SDR)
• This neurosurgical operation involves a laminoplasty from L1 to S1 and section of 20% to 40% of the dorsal nerve rootlets.
• The selection criteria includes pure spasticity, good selective motor control, adequate underlying muscle strength, age 4 years to 7 years, and diagnosis of spastic diplegia due to prematurity
• Long-term effects (scoliosis, lordosis, hip dislocations and foot deformities)
Assistive technology
• A range of devices and gadgets can help with communication, mobility and daily tasks.
• Assistive technology includes such small things as rails, grab bars, magnifiers, and Velcro grips attached to forks and pens to make them easier to grasp.
• It also includes more expensive, high-tech tools, such as customized wheelchairs, voice communication devices, computer software programs, and positioning equipment that puts a child in the correct posture to sit or stand with other kids or family members.
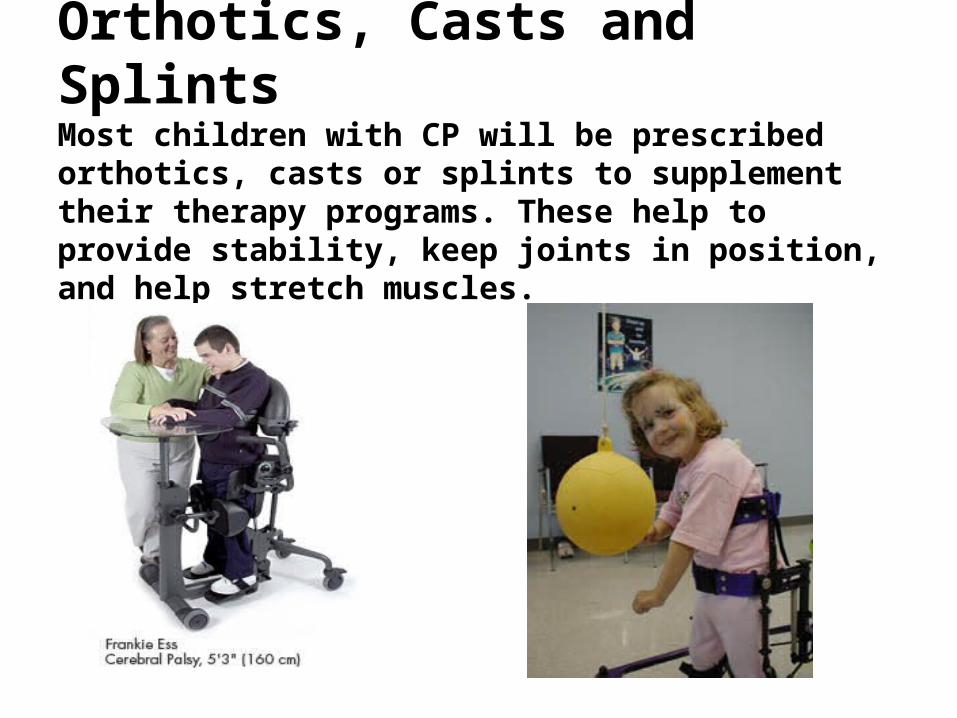
Orthotics, Casts and Splints Most children with CP will be prescribed orthotics, casts or splints to supplement their therapy programs. These help to provide stability, keep joints in position, and help stretch muscles.
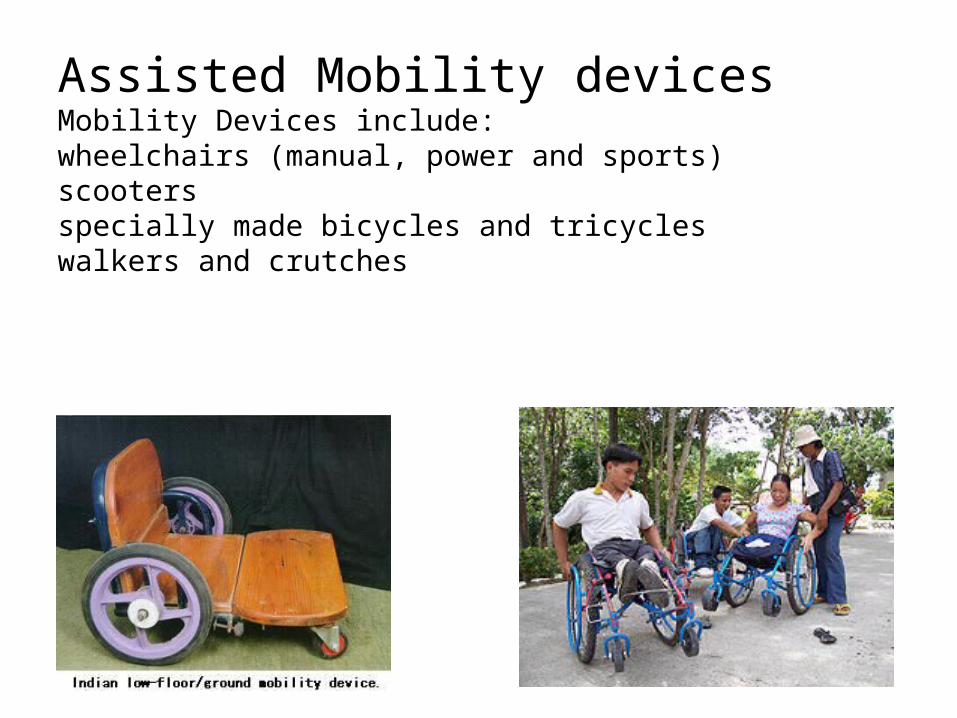
Assisted Mobility devicesMobility Devices include:wheelchairs (manual, power and sports)scootersspecially made bicycles and tricycleswalkers and crutches

Ankle Foot Orthoses(AFO)

Epilepsy
• Seizures occur in about a third of children with C.P. • it was found that epilepsy was seen in 35% cases,
most often in children with spastic hemiplegia (66%) followed by quadriplegia (43%) and diplegia (16%).
• Seizures were difficult to control and polytherapy was required in 38%.
• Most children with CP had onset of seizures in the first or second year of life.
• A significant correlation was found between mental retardation, microcephaly and frequency of seizures.

Visual Problems.
• Almost half of children with CP have visual problems. The commonest are strabismus and refractory errors. Early corrective intervention by an Ophthalmologist is essential.

Behaviour problems & Sleep Problems
• Some children with CP may have problematic aggression and at times hyperactivity and destructive behaviour.
• Behaviour modification techniques and parental counselling are helpful.
• Drugs methylphenidate, antipsychotics like haloperidol and other pharmacological agents.
• A number of children with CP have difficulty in sleeping and irregular sleep rhythms. Use of night sedatives, like chloral hydrate for a few days may help. Melatonin 2 mg half an hour before sleep can also be tried.
Feeding and Nutrition • Bulbar palsy, involuntary movements, tone problems, handling
and seating difficulties• They may ' spit out' food because of tongue thrust and difficulty
in swallowing.• Chewing may be difficult and a number of them have gastro-
oesophageal reflux leading to repeated aspirations.• Special feeding techniques and prokinetics may be required.
gastrostomy may be needed to provide nutrition to the child. • Principles of providing a balanced diet, alongwith an adequate
supply of vitamins and iron remain the same as for a normal child.
• Lack of mobility and gut hypotonia may lead to constipation in some children. Dietary modification with a high fibre diet and plenty of fluids are helpful.
• Excessive Salivation: Oral exercises are taught to the child. Atropine and benztropine have been used occasionally for temporary relief.

Education and Training• Education, prevocational and vocational training are
important aspects of rehabilitation.• These need to be individualized according to the
child's abilities, as determined by detailed assessment.
• Currently there is considerable emphasis on inclusive education. While it may be Guidance should be provided to the parents regarding availability of appropriate schools and training institutions.
• The ultimate aim of management in C.P is to help the child achieve his optimal developmental potential and to integrate him as a useful member in the society.

Parent Counselling • An honest appraisal of the child's condition is
essential. • The clinician should endeavour to provide a balanced
account of the child's problem but simultaneously emphasize the child's abilities so as to help channelize the parents' thought process towards positive goals.
• Parents must learn that 'treatment' is a continuous process; however it can be broken down into a number of short term constructive goals- attainment of these brings a sense of achievement and a hope of progress.





Thank you