cerebrovascular disease. cerebrovascular disease “stroke” macrovascular disease microvascular...
TRANSCRIPT
CEREBROVASCULARDISEASE
CEREBROVASCULARDISEASE
“STROKE”• Macrovascular disease• Microvascular disease• Emboli• Venous thrombosis
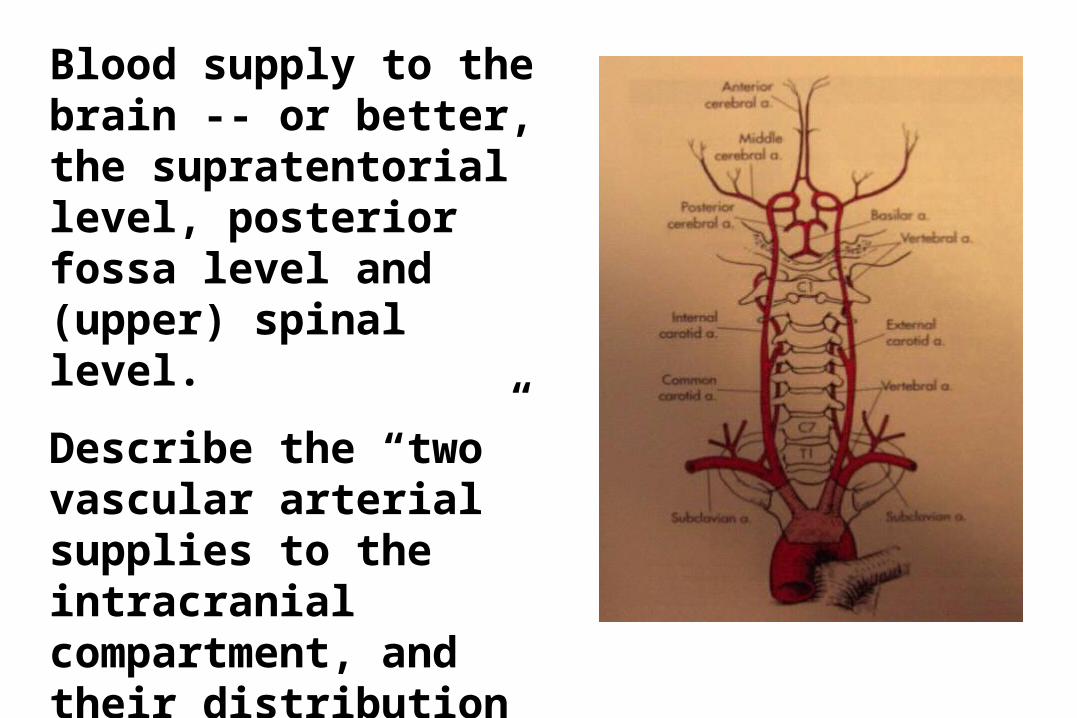
Blood supply to the brain -- or better, the supratentorial level, posterior fossa level and (upper) spinal level.
Describe the “two” vascular arterial supplies to the intracranial compartment, and their distribution to the portions of the neuraxis
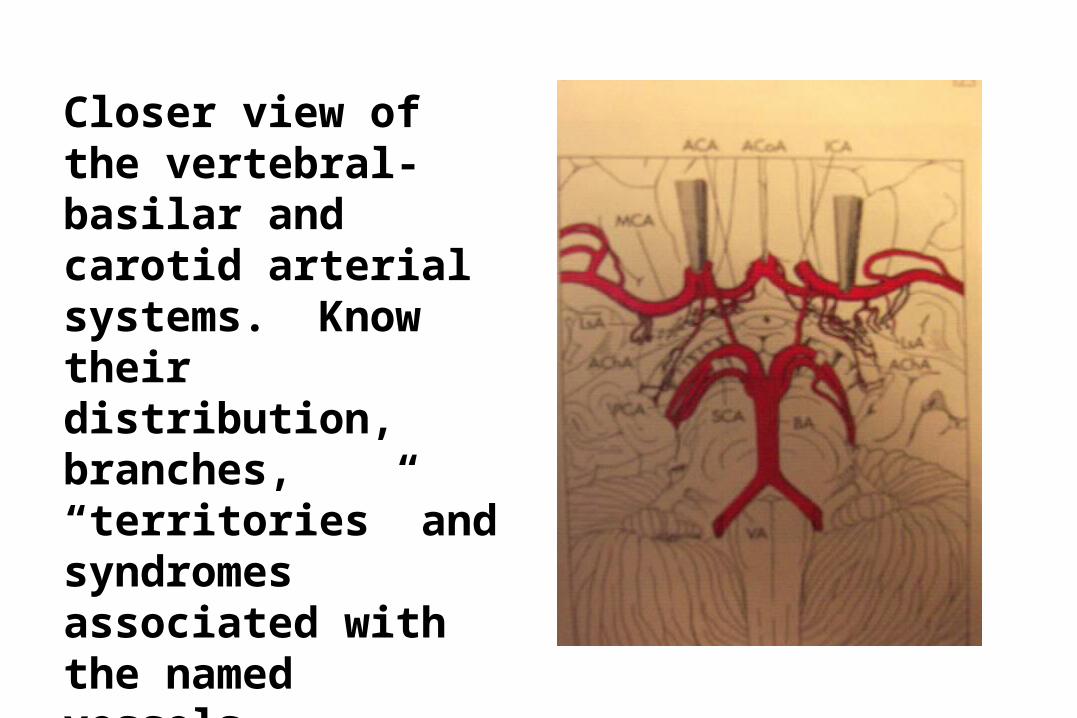
Closer view of the vertebral-basilar and carotid arterial systems. Know their distribution, branches, “territories” and syndromes associated with the named vessels.
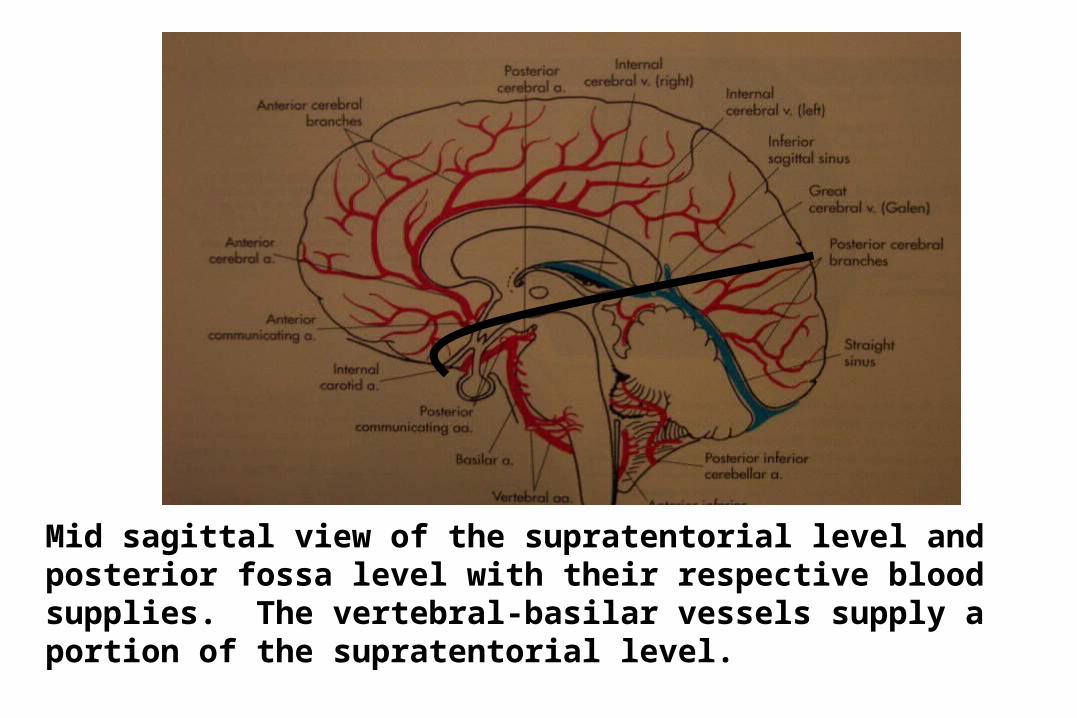
Mid sagittal view of the supratentorial level and posterior fossa level with their respective blood supplies. The vertebral-basilar vessels supply a portion of the supratentorial level.
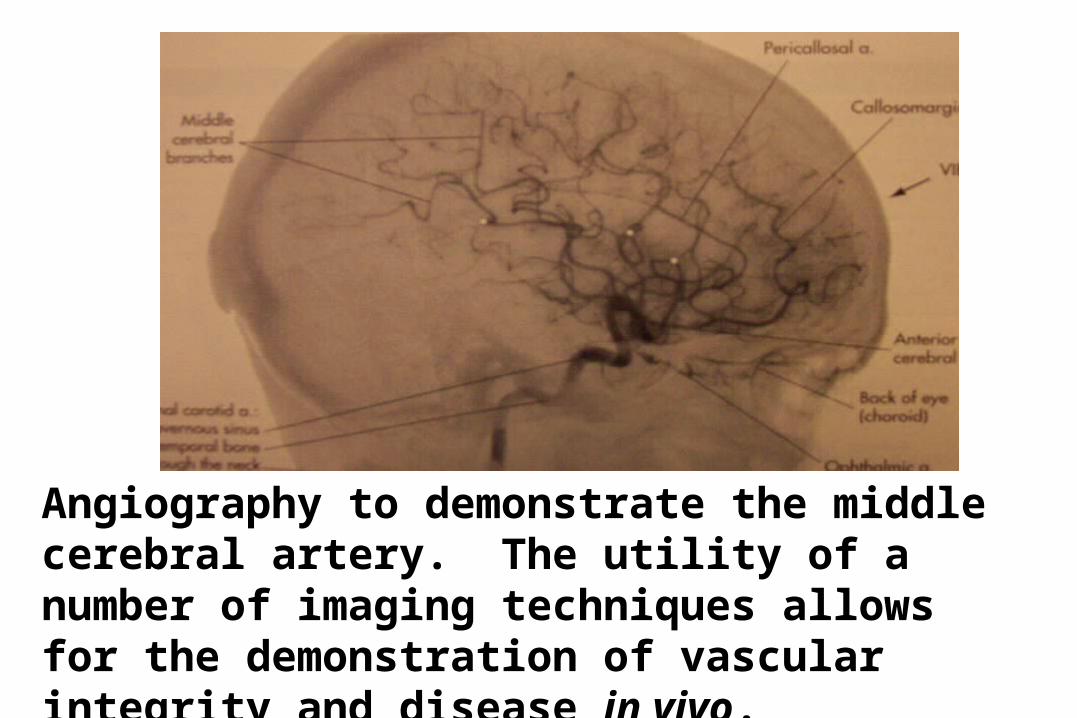
Angiography to demonstrate the middle cerebral artery. The utility of a number of imaging techniques allows for the demonstration of vascular integrity and disease in vivo.
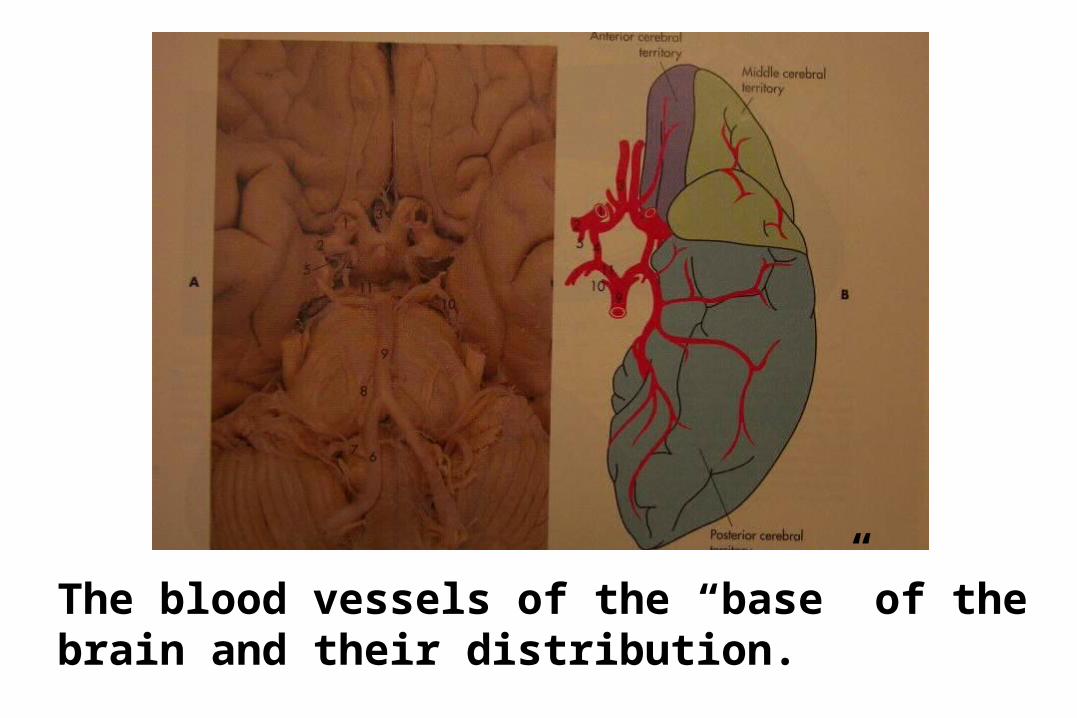
The blood vessels of the “base” of the brain and their distribution.
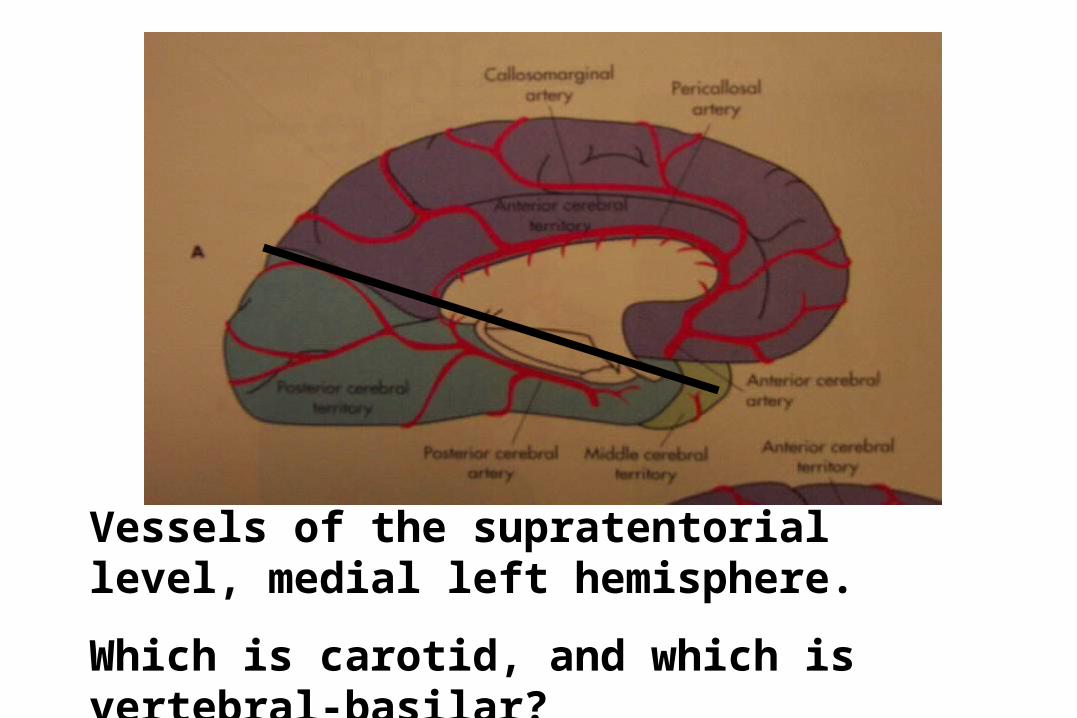
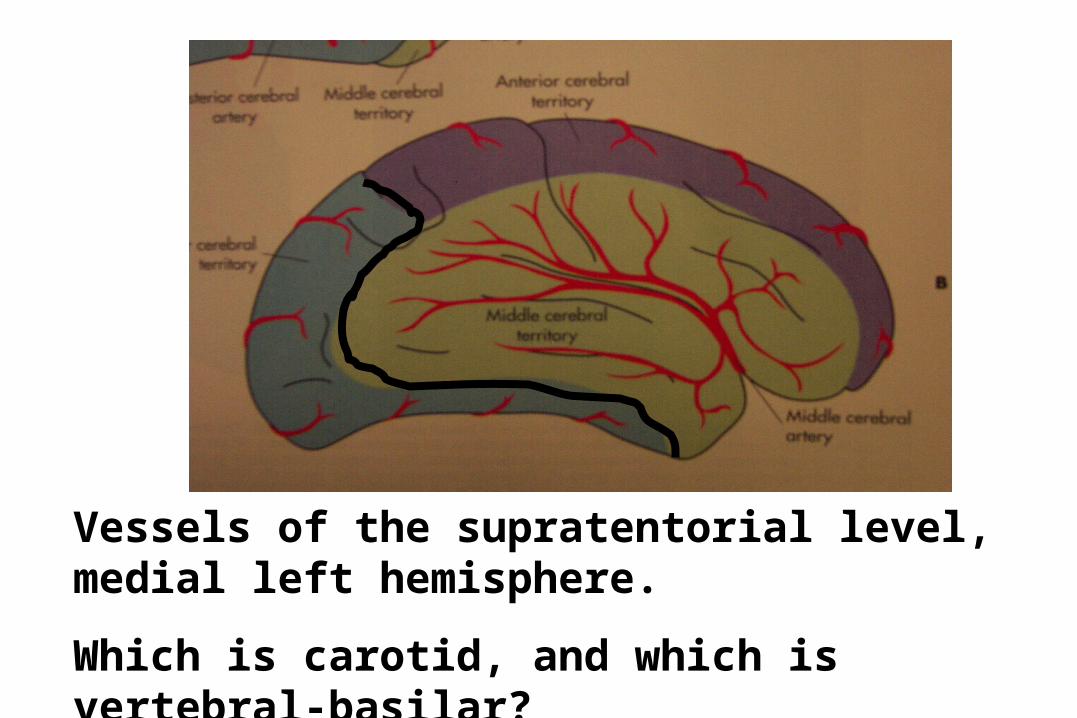
Vessels of the supratentorial level, medial left hemisphere.
Which is carotid, and which is vertebral-basilar?
Vessels of the supratentorial level, medial left hemisphere.
Which is carotid, and which is vertebral-basilar?
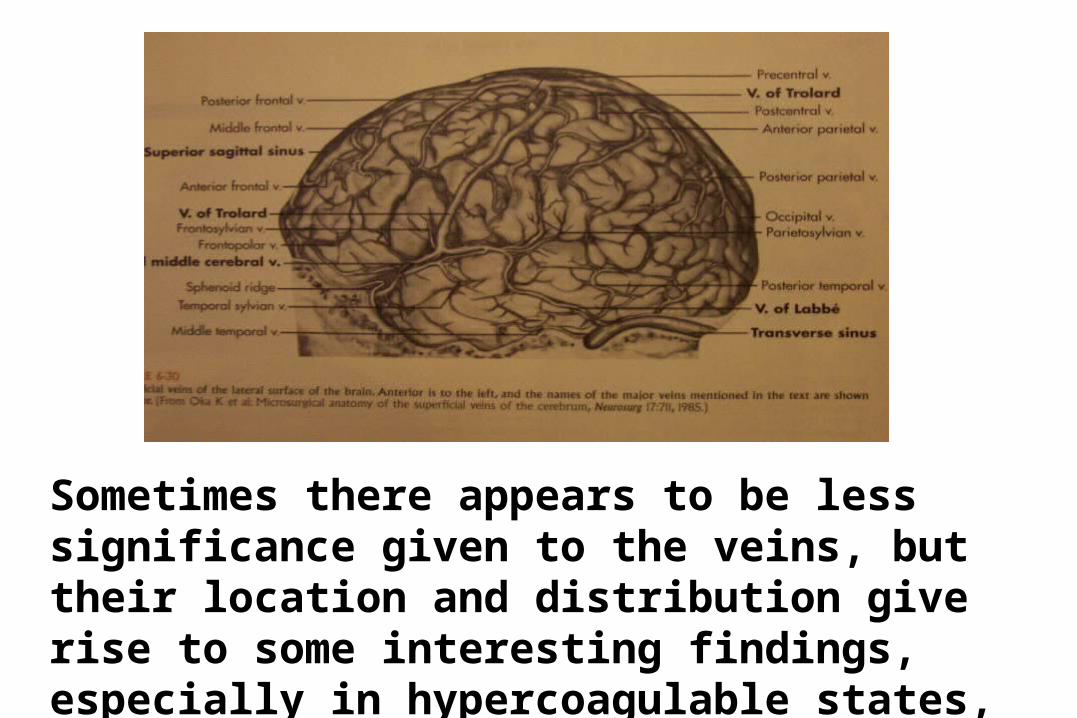
Sometimes there appears to be less significance given to the veins, but their location and distribution give rise to some interesting findings, especially in hypercoagulable states, and trauma.
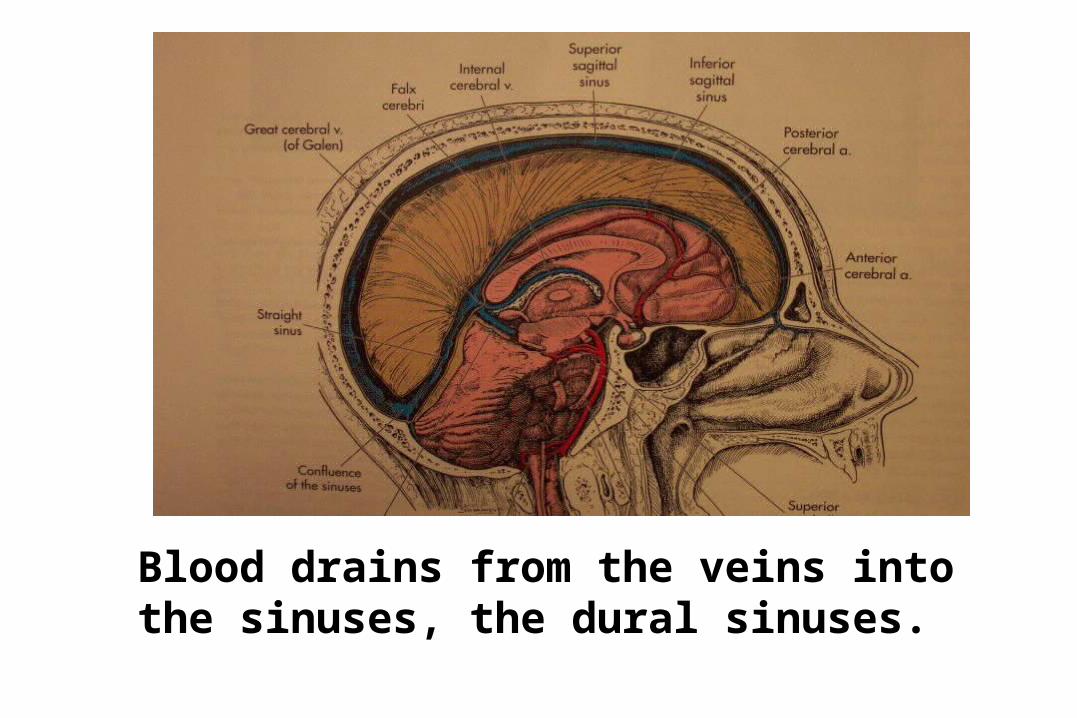
Blood drains from the veins into the sinuses, the dural sinuses.
Define and differentiate hypoxia, ischemia and infarction
Discuss the etiology and pathogenesis of ischemic encephalopathy
Define and differentiate hypoxia, ischemia and infarction
STRAIGHT FROM ROBBINS
Discuss the etiology and pathogenesis of ischemic encephalopathy
Ischemic (hypoxic) Encephalopathy
Vulnerability to ischemia
Neurons
Glial cells
Tissue necrosis
First to die
Prolonged ischemia
Mechanism of neuron cell death
Excitotoxin release
Persistent opening of NMDA receptor channels
Influx of Ca++
NO toxicity
Why is this important? NO synthase inhibitors protect against effects of ischemia in some model systems!!!! Treatment for ischemia?
Define and differentiate hypoxia, ischemia and infarction
Discuss the etiology and pathogenesis of ischemic encephalopathy
STRAIGHT FROM ROBBINS
Ischemic encephalopathy
Episodes of hypotension
Transient (if mild)
Severe global ischemia
Survivor = persistent vegetative state
Isoelectric (flat) EEG
Respirator brain
Morphology
Brain swollen
Flat surface
Poor gray-white distinction
Acute neuronal changes (12 - 24 hours)
Glial cell death
Vulnerability factor
Necrosis, macrophages, vascular proliferation, gliosis
What is a watershed infarct, and how does it relate to the discussion of ischemic encephalopathy?
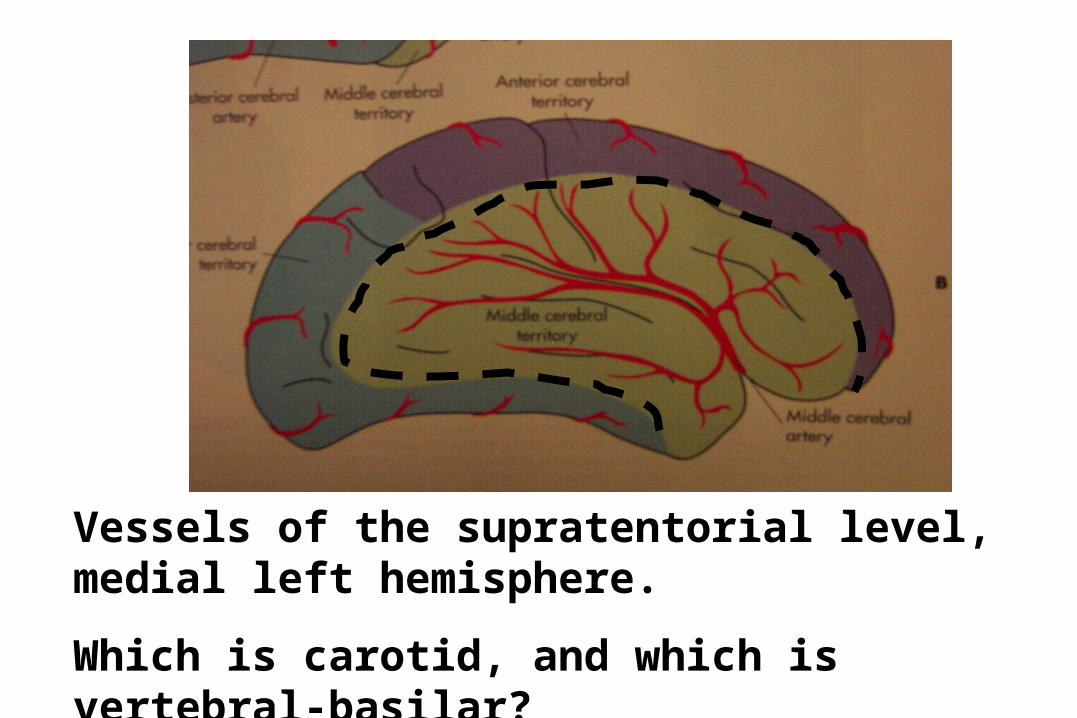
Vessels of the supratentorial level, medial left hemisphere.
Which is carotid, and which is vertebral-basilar?
Differentiate between ischemic and hemorrhagic (white
vs. red) infarcts, and define the most likely causes of each
AB
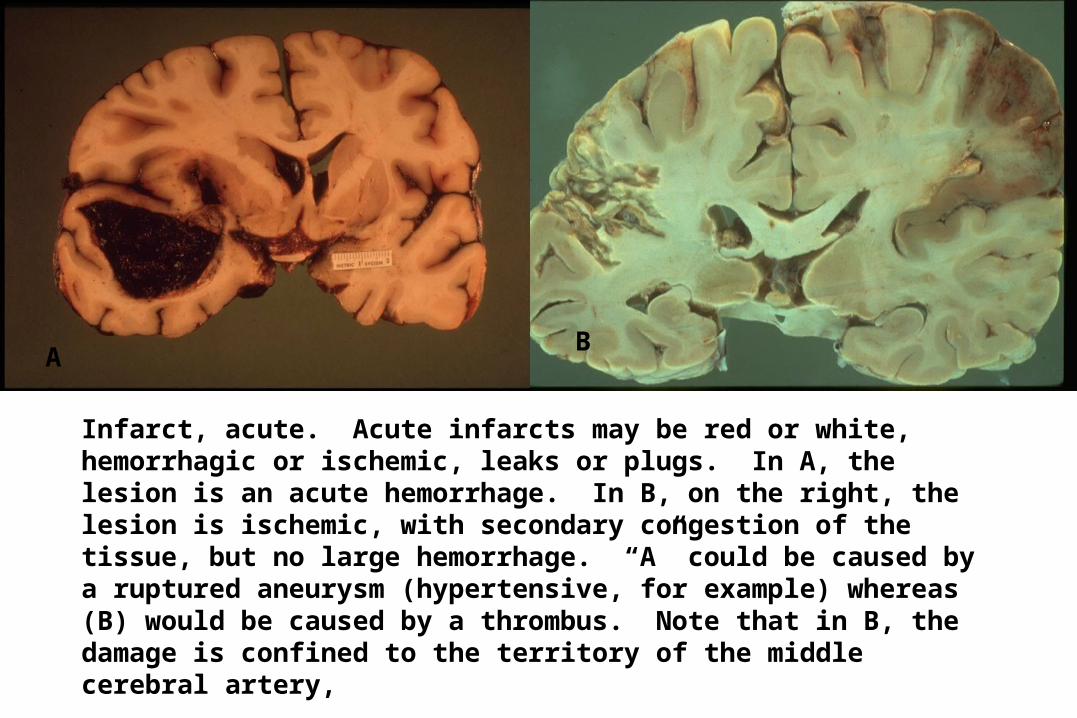
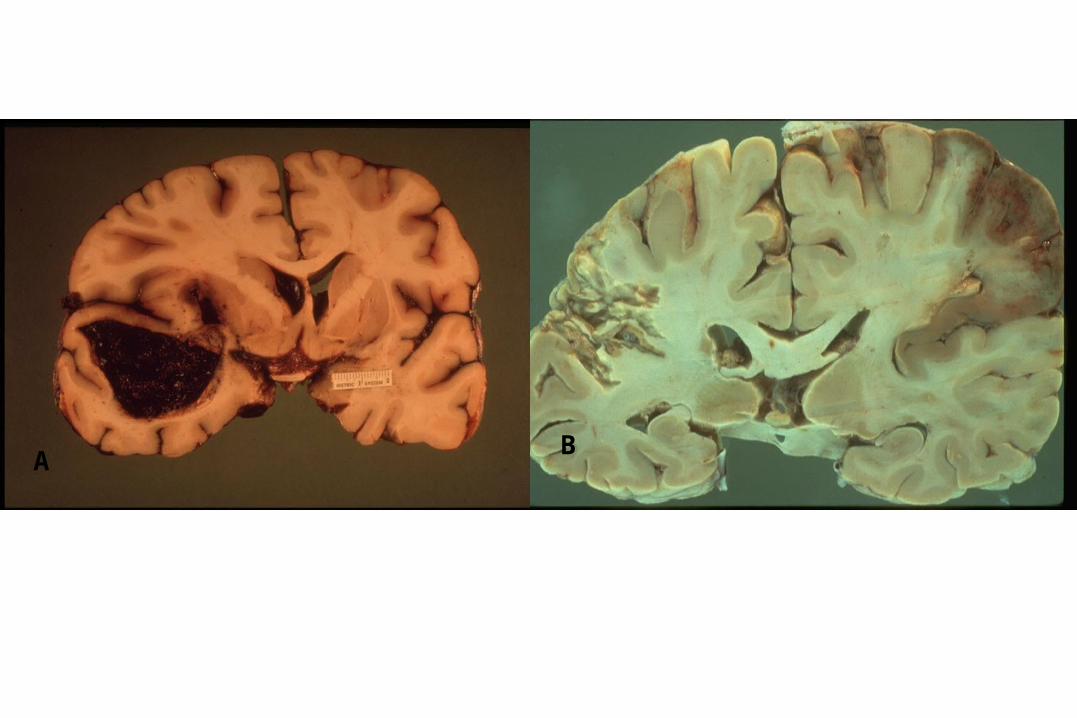
Infarct, acute. Acute infarcts may be red or white, hemorrhagic or ischemic, leaks or plugs. In A, the lesion is an acute hemorrhage. In B, on the right, the lesion is ischemic, with secondary congestion of the tissue, but no large hemorrhage. “A” could be caused by a ruptured aneurysm (hypertensive, for example) whereas (B) would be caused by a thrombus. Note that in B, the damage is confined to the territory of the middle cerebral artery,
What is the lesion on the left side of picture B?
AB
Differentiate between thrombotic and embolic infarction, and given a gross or microscopic picture, be able to recognize the difference between the two
CEREBROVASCULARDISEASE
“STROKE”• Macrovascular disease• Microvascular disease• Emboli• Venous thrombosis
STROKE: EPIDEMOLOGICFACTORS
• 0.5 million / year• 3 X 106 ‘survivors’• 150,000 deaths / year• Incidence 100 / 100,000 ages 45-54 1800 / 100,000 ages 85+• Risk factors• Infarction 10 X > Hemorrhage
STR0KE: RISK FACTORS
MAJOR FACTORS• Age• Family history• Diabetes Mellitus• Cigarette smoking• Hypertension• Lipid Metabolism• Truncal obesity
OTHER FACTORS• Oral contraceptives• Hematologic Sickle cell Polycythemia• Coagulation disorders• Cardiac disease• Vascular disease
ATHEROSCLEROSIS & STROKE
• Documented risk factors• TIA -- common presentation• TIA -- high risk• Embolization• Occlusive thrombosis Extracranial -- common Intracranial -- less often
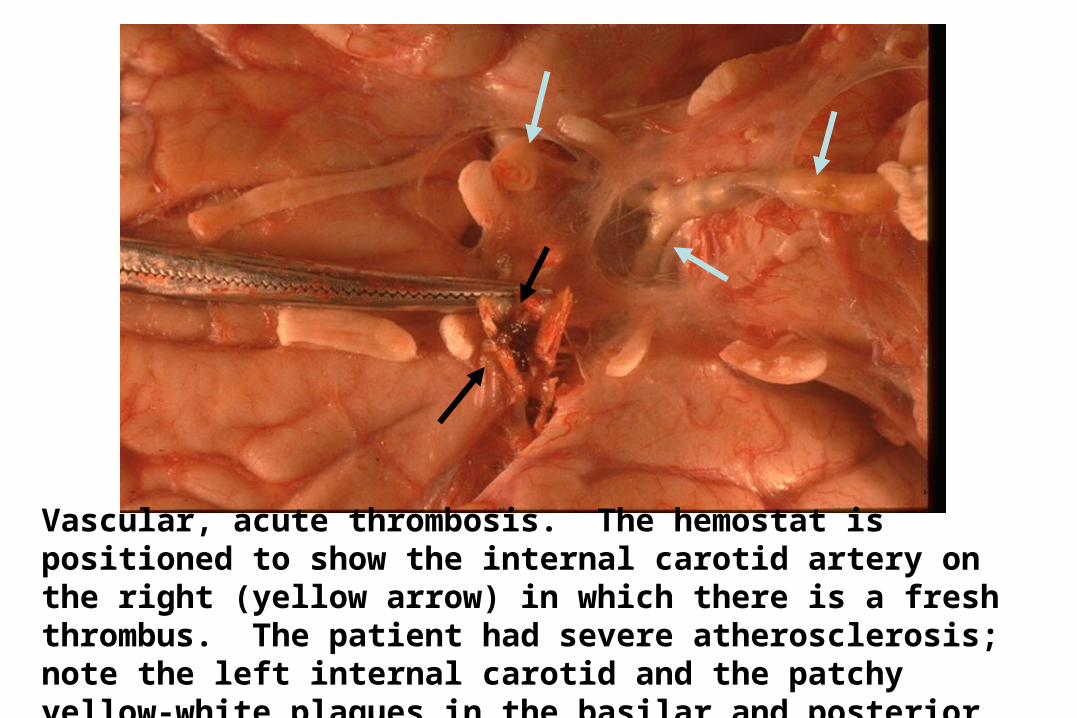
Vascular, acute thrombosis. The hemostat is positioned to show the internal carotid artery on the right (yellow arrow) in which there is a fresh thrombus. The patient had severe atherosclerosis; note the left internal carotid and the patchy yellow-white plaques in the basilar and posterior cerebral arteries (blue arrows).
COAGULATION DEFECTS &BRAIN INFARCTS
• Protein C deficiency• Factor V Leiden mutation
(Arg506Gln)• Protein S deficiency• Antithrombin III abnormalities• Carbohydrate-deficient
glycoprotein synthase type I
MICROANGIOPATHY• Angitis and vasculitis• Primary angitis of CNS• Vasculitides
Polyarteritis nodosaAllergic angitis and granulomatosisWegener’s granulomatosisLymphomatoid granulomatosis
• Microvasculopathy associated with dementiaBinswanger’sAutosomal dominant arteriopathy
BINSWANGER’S SUBCORTICALARTERIOSCLEROTIC
LEUKOENCEPHALOPATHY
• Slowly progressive, but “stairstep”• 6th to 7th decade• Memory, mood, cognition• Pseudobulbar: gait and sphincter control
EMBOLIC DISEASES
Embolic stroke results when solid material:forms in the arterial circulationis introduced into arterial circulationshifts from venous to arterial circulation
Resultant infarct is:abrupthemorrhagic (reperfusion
Differential diagnosis is:ischemic infarctcerebral hemorrhage
SOURCES OF BRAIN &SPINAL CORD EMBOLI
• Atheroma• Cardiogenic• Fat• Neoplasms and parasites• Iatrogenic• Miscellaneous
SOURCES OF BRAIN &SPINAL CORD EMBOLI
• AtheromaComplicated atherosclerosis
• CardiogenicLeft atrium (noncontractile)Mural thrombiEndocarditisValve lesions
CNS INFARCTION• Acute
5-8 hours undetectable12-36 hours blurring gray/white
interface, dusky, softeningterritorial
• Subacute2-4 days softening, blurring, dusky, EDEMA
• ChronicStage I: liquefactive necrosis to cavitationStage II: (months) cavitary
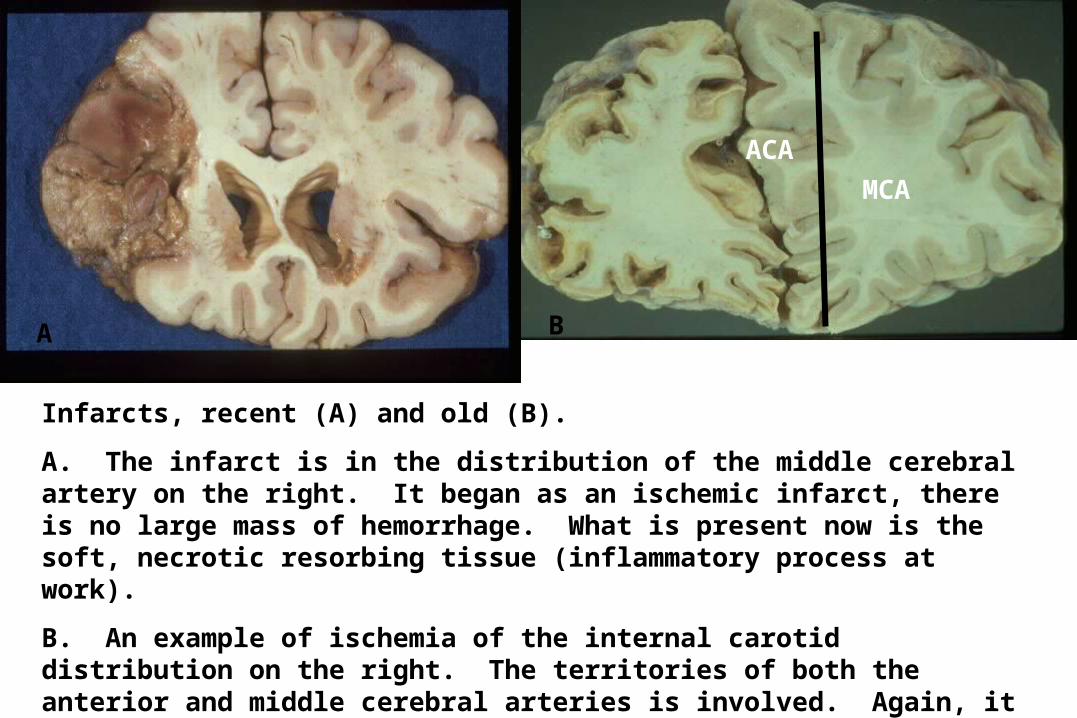
Infarcts, recent (A) and old (B).
A. The infarct is in the distribution of the middle cerebral artery on the right. It began as an ischemic infarct, there is no large mass of hemorrhage. What is present now is the soft, necrotic resorbing tissue (inflammatory process at work).
B. An example of ischemia of the internal carotid distribution on the right. The territories of both the anterior and middle cerebral arteries is involved. Again, it was an ischemic, there is no large mass of blood as in a ruptured aneurysm. Vessel territories are demonstrated on the left of B.
A B
ACA
MCA
CNS INFARCTION
• Acute (hours)eosinophilia with pyknosisvacuolation of neurophil
• Subacute (days)PMN infiltrationnecrotic microvesselsfoamy macrophages
• Chronic (weeks to months)foamy macrophages, hemosiderinreactive astrocytes
CORTICAL DYSFUNCTION:TERRITORIAL
MCA hemipariesis aphasia hemisensory deficit
ACA hemipariesis transcortical aphasia abulia
PCA thalamic syndrome hemianopia alexia
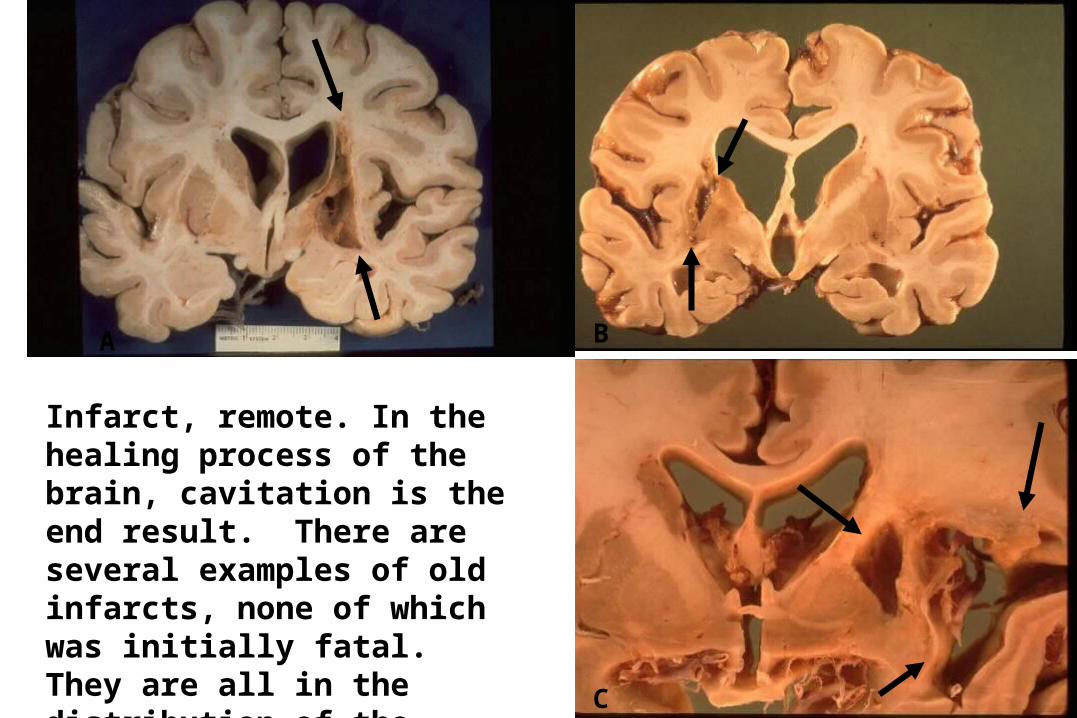
Infarct, remote. In the healing process of the brain, cavitation is the end result. There are several examples of old infarcts, none of which was initially fatal. They are all in the distribution of the ____________ artery?
A B
C
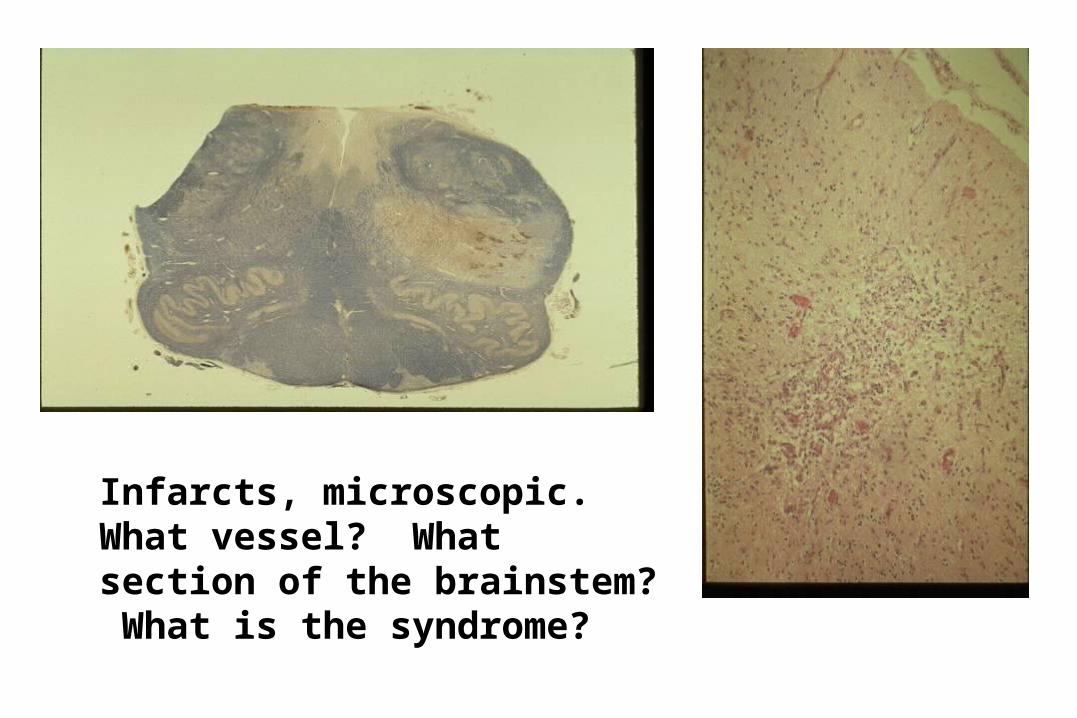
Infarcts, microscopic. What vessel? What section of the brainstem? What is the syndrome?
INTRACRANIAL HEMORRHAGE
• Extradural• Subdural• Subarachnoid• Parenchymal
CerebralCerebellarBrain stem
Define the etiology and pathogenesis of hypertensive vascular disease including hemorrhage and lacunar infarcts
HYPERTENSIVE PARENCHYMALHEMORRHAGES
Pathogenesisrupture of weakened arterioles replacement of muscle by fibrous tissue fragmentation of elastic tissue focal microaneurysms
Associated systemic hypertension
PARENCHYMAL HEMORRHAGES
• Hypertension• Trauma• Cerebral amyloid angiopathy• Saccular aneurysms• Vascular malformations• Bleeding diathesis (anticoagulants)• Vasculitis• Neoplasms• Infections
HYPERTENSIVE HEMORRHAGES
• Putamen hemiparesis hemisensory loss visual field defects
• Thalamus hemiparesis hemisensory loss gaze abnormalities
• Cerebellumvomiting & headacheataxiacranial nerve abnormalities
• Large pontinecomaquadriparesis or quadraplegiasmall reactive pupils
• Small pontinegaze paresisataxiasensorimotor deficit
Symptoms and Signs
HYPERTENSIVE HEMORRHAGES
• Gross findingsacute hematomaintraventricular extensionswelling, herniationresorb, cavitationdoes not respect vascular territorysecondary Wallerian degeneration
HYPERTENSIVE HEMORRHAGES
Microscopic featuresfresh bloodinflammatory cells, macrophageshemosiderin, hematoidin
Small vessels“onion-skinning”lipohyalinosismicroaneurysmsfibrinoid necrosis
ARTERIOSCLEROTIC CHANGE
HYPERTENSIVE HEMORRHAGES
Thickening of the mediaAdventitial fibrosisFragmentation / reduplication
of elasticaIntimal thickeningAccumulation of macrophages
Charcot - Bouchard microaneurysm
Cerebral Autosomal DominantArteriopathy With
Subcortical Infarcts &Leukoencephalopathy
(CADASIL)
Binswanger’S SubcorticalArteriosclerotic
Leukoencephalopathy
Cerebral Amyloid Angiopathy
MICROVASCULAR DEMENTIA