certification of consumer, youth, family and parent peer ... · certification of consumer, youth,...
TRANSCRIPT

Certification of Consumer, Youth, Family and Parent Peer Providers A Summary of Regional Stakeholder Meeting Findings
June
2012
Funded by Proposition 63 Submitted to the Office of Statewide Health Planning and Development (OSHPD) by Working Well Together www.workingwelltogether.org

1
THIS PAGE IS INTENTIONALLY BLANK.
2
The views expressed in this publication do not necessarily reflect the views of the Office of Statewide
Health Planning and Development.
Table of Contents
Acknowledgements ......................................................................................................................... 4
Executive Summary ........................................................................................................................ 5
Introduction ..................................................................................................................................... 6
Focus Group Findings ..................................................................................................................... 8
Purpose of Certification .............................................................................................................. 9
Training Peer Providers ............................................................................................................ 11
Qualifications of Training Organizations ................................................................................. 12
Maintaining Peerness ................................................................................................................ 14
Qualifications of Supervisors .................................................................................................... 15
Additional Comments and Suggestions .................................................................................... 18
Survey Data Information............................................................................................................... 19
Curriculum Type ....................................................................................................................... 19
Curriculum Topics .................................................................................................................... 20
Number of Training Hours in Curriculum ................................................................................ 21
Number of Work/Volunteer Hours Required ........................................................................... 21
Examination Requirements ....................................................................................................... 22
Continuing Education Requirements (CEUs) ........................................................................... 23
Certification Renewal ............................................................................................................... 23
Certifying Body ........................................................................................................................ 24
Funding for Certification .......................................................................................................... 25
“Grandfathering in” Recommendations .................................................................................... 26
Mechanism for Billing Medi-Cal .............................................................................................. 27
Wrap Up of Stakeholder Meeting ................................................................................................. 28
Barriers and Challenges ............................................................................................................ 28
Solutions ................................................................................................................................... 29
Critical Decisions for Implementation Planning........................................................................... 31
Stakeholder Input Regarding Critical Decisions for Implementation Planning ....................... 31
Question and Answer Sessions ..................................................................................................... 34
Recommendations ......................................................................................................................... 35

3
Conclusion .................................................................................................................................... 37
Addendum I .................................................................................................................................. 38
Questions and Comments Central Region ................................................................................ 38
Questions and Comments Greater Bay Area Region ................................................................ 40
Questions and Comments Southern Region ............................................................................. 42
Question and Comments Los Angeles Region ......................................................................... 44
Questions and Comments Superior Region .............................................................................. 47

4
Acknowledgements
Working Well Together (WWT) would like to thank the many people who have been involved in
the work regarding peer certification. While we cannot name all of them individually, we are
grateful to the participants on the monthly Consumer, Youth, Family and Parent (CYFP)
Certification teleconferences. We want to acknowledge and appreciate Karin Lettau, MS, CRC
for her dedication and diligent work in organizing all of the stakeholder meetings. We want to
extend our appreciation to all of the individuals who participated in the stakeholder meetings
across the state, giving of their time and energy to read the research and spend a day in
thoughtful discussion of this important subject.
WWT is a collaborative project comprised of the California Network of Mental Health Clients,
NAMI California, United Advocates for Children and Families, and the California Institute for
Mental Health. Funded by the Mental Health Services Act and the Office of Statewide Health
Planning and Development (OSHPD), the WWT Training and Technical Assistance Center
supports the vision of the MHSA Act to transform systems to be client and family-driven. As such,
WWT supports the sustained development of client, family member and parent/caregiver peer
employment within every level of the public mental health workforce.
www.workingwelltogether.org
This report was produced by Debra Brasher, MS, CPRP, and Lucinda Dei Rossi, MPAC, CPRP,
of Inspired at Work. www.inspiredatwork.net [email protected]

5
Executive Summary
The Working Well Together Collaborative undertook a year-long process of gathering data and
information from stakeholders throughout the state on the development of a statewide
Certification for Consumers, Youth, Family and Parent Peer Support Providers. This process
was based on the principles and values of the Mental Health Services Act (MHSA) which
stipulates that individuals with lived experience of a mental health challenge and their family
members should be primary drivers in the development and provision of mental health services.
MHSA also specifies the importance of the inclusion of family members and persons with lived
experience in the mental health workforce to ensure transformation to a recovery and resiliency-
oriented approach to services. This report summarizes the input from five regional meetings
held throughout the state and provides specific recommendations on Peer Support Certification.
Stakeholders included people with lived experience, youth, family members, parents, county
mental health administrators, peer organizations, community colleges and community-based
organizations, each offering their unique and important voice to the process. Identified benefits
of certification include: the standardization of training of peer providers resulting in improved
consistency and quality of services throughout the state, the development of a clear scope of
practice for peer providers and validation of peer support as an integral part of recovery-oriented
service provision.
All stakeholders received the Certification of Consumer, Youth, Family and Parent Providers: A
Review of the Research Report as key background information for participation. This report
summarizes national efforts regarding certification as well as the current training and
employment efforts taking place across California. Feedback was gathered through a written
survey, focus groups and question/comment opportunities during the stakeholder meetings.
Stakeholders across the state were particularly interested and concerned with the role of peer
providers under the Affordable Care Act (ACA). One of the critical decisions needed for
implementation addressed Health Care Reform and proposed two recommendations: 1) ensure
the inclusion of whole health curriculum content into the core curriculum and 2) ensure that
people with lived experience and family member stakeholders are present during the state-level
discussions regarding implementation of the ACA. In total, 18 recommendations were
developed. A few examples include:
Development of standards for a core curriculum with additional specialized curriculum
resulting in specific certifications for family members, parents, transition-age youth,
older adults, forensics and whole health
A qualified statewide entity should become the certifying body
Development of a code of ethics and scope of practice for peer providers
Inclusion of peer providers and peer services in the state plan amendment for specialty
mental health services

6
Introduction
Peer support is a long established and increasingly used practice that offers hope, inspires
positive growth and promotes recovery and resiliency for individuals and their family members,
parents and caregivers who are living with the challenges of a mental health issue. In California,
the Mental Health Services Act (MHSA), passed by voters in 2004, stipulates that individuals
receiving services for a mental health diagnosis, as well as their family members, must be
actively involved in the development and provision of services to ensure system transformation
toward a recovery and resiliency orientation. A significant strategy for system transformation is
peer support. The MHSA has created increased demand and opportunities for individuals to
receive and provide peer support services.
Nationally, the research conducted indicates that there are anywhere from twenty-three (23) to
thirty-five (35) states currently providing certification for Peer Support Specialists and four or
five states providing Family Support Specialist certification. Raw data from the Pillars of Peer
Support Summit Report (2009) indicate that twenty-three (23) states are currently providing
certification. As this data was collected from attendees at the conference, it is limited to the
number of states represented at the Summit. Data from an OptumHealth report draft entitled,
State Handbook for Peer and Family Support Services (2010) reports data for thirty (30) states
that are providing certification. When these two reports are combined there is a great degree of
overlap, however there are five states that have data that appear in one data set but not the other.
Most state mental health programs have opted to develop and fund peer support services through
the federally funded Medicaid program. Most states have included peer support under the
Rehabilitation Option within their state plans. Medicaid allows for a number of different ways to
fund this service, including billing by service type and/or service provider, billing through stand-
alone peer support organizations and billing under a capitated rate in a managed care system.
States that bill Medicaid for identified peer support services have followed the recommended
guidelines developed by the Centers for Medicare and Medicaid Services. These
recommendations include the development of a certification program for peer support specialists
as defined by the state.
Working Well Together, a collaborative of the California Network of Mental Health Clients
(CNMHC), NAMI California, United Advocates for Children and Families and the California
Institute for Mental Health, under California Department of Mental Health contract agreement
#11-71041-000, was tasked with conducting five regional meetings with local stakeholders
across the State of California to gather feedback and input regarding state-wide certification
standards for Peer Support Specialists working in the public mental health field. Inspired at
Work, through a contract with Working Well Together, was engaged to conduct five regional
Peer Certification Stakeholder Meetings during the months of March and April of 2012 in
Redding (Superior/Northern California Region), Sacramento (Central Region), San Jose (Greater
Bay Area Region), Los Angeles (Los Angeles Region) and San Diego (Southern California
Region).
A total of 165 people attended these meetings. The survey that was used for data collection
contained a list of 14 categories of stakeholder/constituency groups. Each attendee chose to
identify with one or more stakeholder groups. Consumer/Peer Providers were the largest

7
category of attendees, followed by individuals representing Community-Based Organizations
(CBOs), and Family Member Peer Providers. County mental health administration
representatives were also well represented.
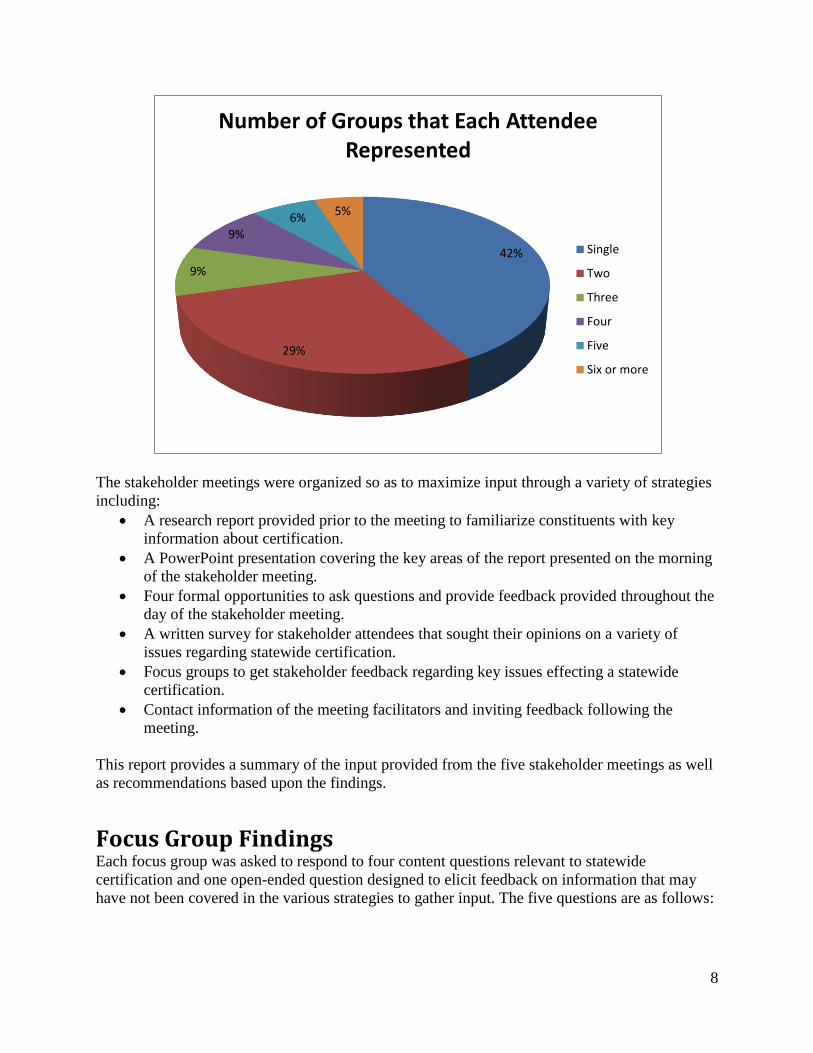
While 42 percent of attendees selected only one group as their primary affiliation, a number of
attendees selected more than one group/constituency. A number of individuals were wearing
more than one hat as stakeholders.
48
40 35
26 21 19 19
16 14 10 10 9 9
4
0
10
20
30
40
50
60
Representation of Attendees
8
The stakeholder meetings were organized so as to maximize input through a variety of strategies
including:
A research report provided prior to the meeting to familiarize constituents with key
information about certification.
A PowerPoint presentation covering the key areas of the report presented on the morning
of the stakeholder meeting.
Four formal opportunities to ask questions and provide feedback provided throughout the
day of the stakeholder meeting.
A written survey for stakeholder attendees that sought their opinions on a variety of
issues regarding statewide certification.
Focus groups to get stakeholder feedback regarding key issues effecting a statewide
certification.
Contact information of the meeting facilitators and inviting feedback following the
meeting.
This report provides a summary of the input provided from the five stakeholder meetings as well
as recommendations based upon the findings.
Focus Group Findings Each focus group was asked to respond to four content questions relevant to statewide
certification and one open-ended question designed to elicit feedback on information that may
have not been covered in the various strategies to gather input. The five questions are as follows:
42%
29%
9%
9%
6% 5%
Number of Groups that Each Attendee Represented
Single
Two
Three
Four
Five
Six or more
9
Purpose of Certification
1. Which purpose for certification would you support and why? a. Formal validation alone. b. Formal validation and the ability to bill. c. Neither - I do not support certification.
2. Who do you think should be authorized to train peer providers and why? Please consider qualifications of the training organization. a. Should there be one training entity or more than one?
3. How should a training and certification process ensure that peer specialists are able to maintain their peerness?
4. In addition to standard supervisory excellence, what additional qualifications/training/experience do you think is needed for a supervisor of peer support staff?
5. Any additional comments/suggestions? 5. Additional comments/suggestions/questions.

10
There were a total of 237 responses to this question. The responses were grouped into the three
options listed above. Responses that did not reflect a direct answer to this question were
categorized based on similarities. A total of 119 of the responses were directly responsive to the
question. An additional 69 comments were about billing and certification. The remaining 49
responses could not be categorized as clearly responsive. Of the 119 responses, the vast majority
were supportive of option b, “formal validation and the ability to bill” with a total of 87
responses. Twenty-six responses supported option a, “formal validation alone” and six responses
supported option c, “not supportive of certification”.
Focus group respondents identified a number of reasons for pursuing certification of peer support
specialists. These include:
It legitimizes the role by establishing recognized standards of practice and a code of
ethics.
It may lead to professional advancement and salary increases.
It may reduce some of the barriers to creating specific coded positions for peer support
within civil service systems.
It establishes a standard of practice.
It will provide peer support workers with a professional voice.
It may help to reduce stigma and discrimination.
22%
73%
5%
Purpose of Certification
Formal Validation Only
Formal Validation andAbility to Bill
No Certification
1. Which purpose for certification would you support and why?
a. Formal validation alone
b. Formal validation and the ability to bill.
c. Neither - I do not support certification
11
It will provide education to existing system of care employees on the role and value of
peer support.
It allows for portability from one county to another.
While most people were supportive of certification and the ability to bill Medi-Cal, there were a
number of responses that indicated a significant concern about billing. Nineteen responses were
supportive of billing with caution and another 20 were simply concerns about billing. These
concerns group into the following categories:
Billing Medi-Cal will force peers into a “medical model” role that will require them to
use language in a billable note that is deficit based and not person-centered.
The ability to bill will lead to a requirement to bill with productivity standards that may
erode the ability to provide important peer support that is not currently billable.
Becoming part of the billable system may co-opt peers into system values at the expense
of peer values.
The current system of billing is onerous and takes a significant amount of time away
from direct services.
Respondents expressed some hopes and opportunities that could result from certification that
includes the ability to bill Medi-Cal, including:
Awareness that a state plan amendment to include peer services could result in billing
standards and language that are more supportive of recovery and resiliency oriented work
throughout the system of care.
An acknowledgment that in the Children’s System of Care, there is a barrier to providing
services to family members in support of the minor receiving services. It is hoped that the
inclusion of peer support could result in a billing code that is more expansive and directly
tied to the provision of services to the family member or parent as a “peer”.
An interest in the potential ability to create stand- alone peer operated centers that could
bill for peer services.
An opportunity to bill for “peer support” as well as the ability to bill to existing codes
where appropriate both within a clinic system or a peer operated service.
Training Peer Providers
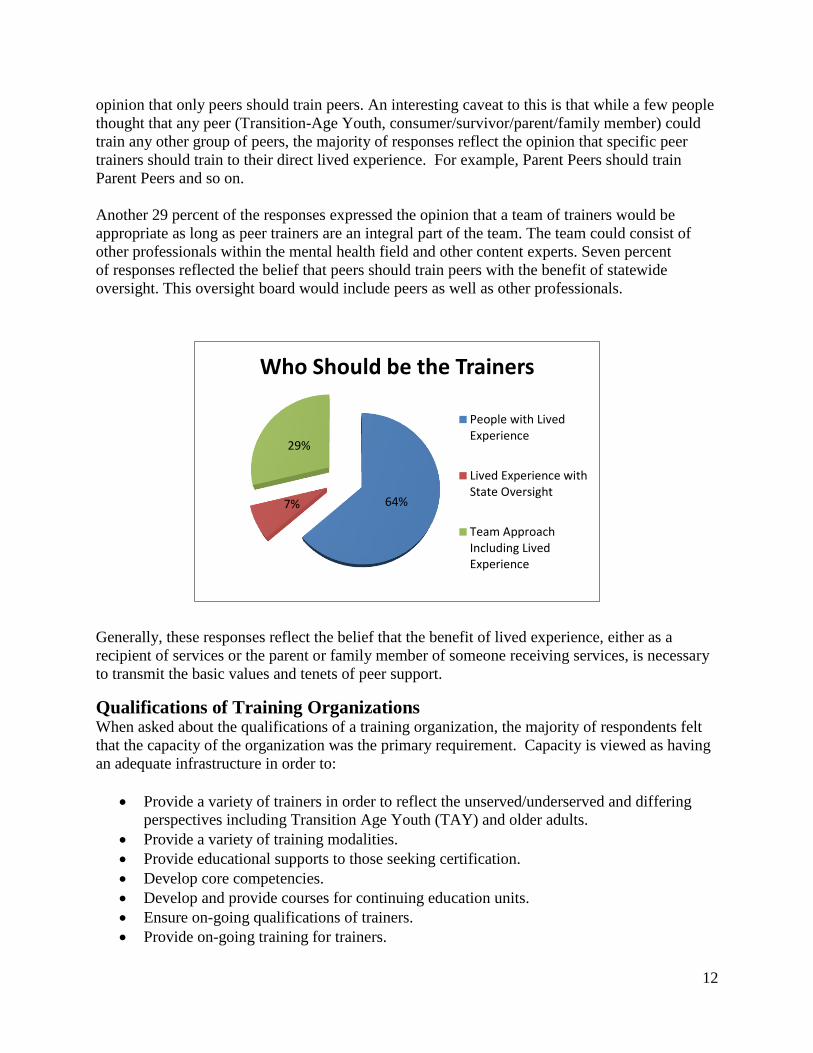
Overwhelmingly, stakeholders believe that Peer Support Specialists should be trained by other
peers or qualified persons with lived experience. Sixty-four percent of the responses reflect the
2. Who do you think should be authorized to train peer providers and why?
Should there be one training entity or more than one?
12
opinion that only peers should train peers. An interesting caveat to this is that while a few people
thought that any peer (Transition-Age Youth, consumer/survivor/parent/family member) could
train any other group of peers, the majority of responses reflect the opinion that specific peer
trainers should train to their direct lived experience. For example, Parent Peers should train
Parent Peers and so on.
Another 29 percent of the responses expressed the opinion that a team of trainers would be
appropriate as long as peer trainers are an integral part of the team. The team could consist of
other professionals within the mental health field and other content experts. Seven percent
of responses reflected the belief that peers should train peers with the benefit of statewide
oversight. This oversight board would include peers as well as other professionals.
Generally, these responses reflect the belief that the benefit of lived experience, either as a
recipient of services or the parent or family member of someone receiving services, is necessary
to transmit the basic values and tenets of peer support.
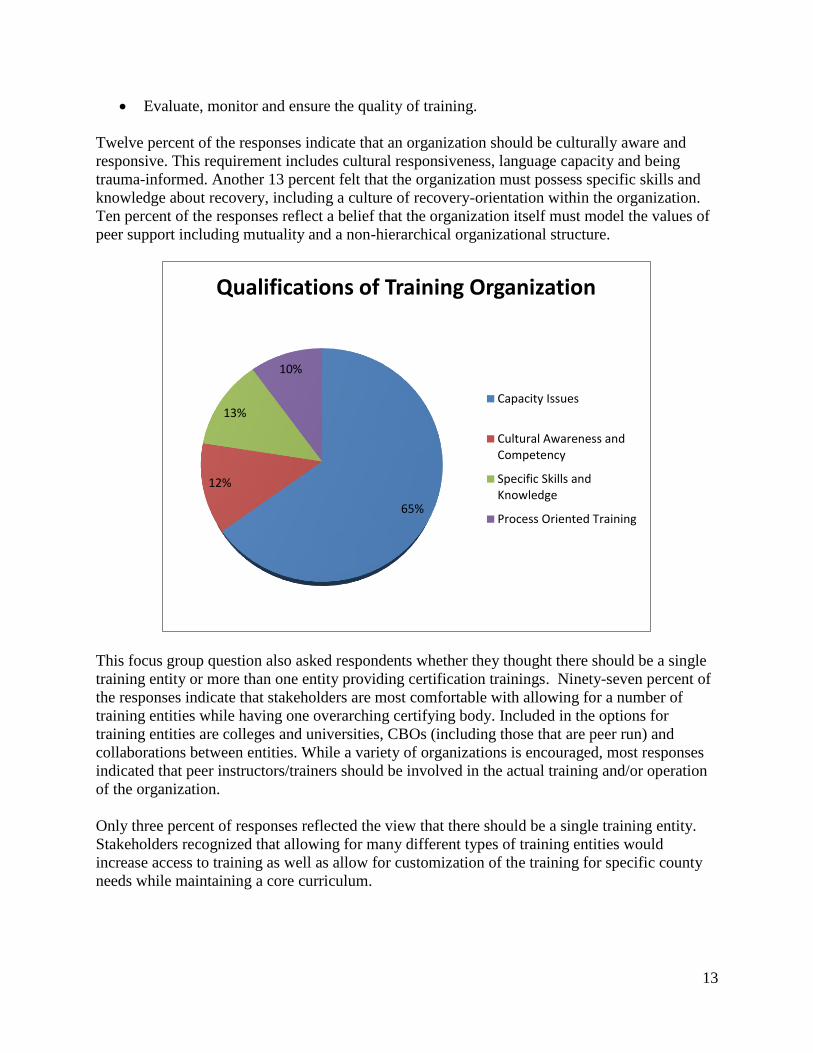
Qualifications of Training Organizations When asked about the qualifications of a training organization, the majority of respondents felt
that the capacity of the organization was the primary requirement. Capacity is viewed as having
an adequate infrastructure in order to:
Provide a variety of trainers in order to reflect the unserved/underserved and differing
perspectives including Transition Age Youth (TAY) and older adults.
Provide a variety of training modalities.
Provide educational supports to those seeking certification.
Develop core competencies.
Develop and provide courses for continuing education units.
Ensure on-going qualifications of trainers.
Provide on-going training for trainers.
64% 7%
29%
Who Should be the Trainers
People with LivedExperience
Lived Experience withState Oversight
Team ApproachIncluding LivedExperience
13
Evaluate, monitor and ensure the quality of training.
Twelve percent of the responses indicate that an organization should be culturally aware and
responsive. This requirement includes cultural responsiveness, language capacity and being
trauma-informed. Another 13 percent felt that the organization must possess specific skills and
knowledge about recovery, including a culture of recovery-orientation within the organization.
Ten percent of the responses reflect a belief that the organization itself must model the values of
peer support including mutuality and a non-hierarchical organizational structure.
This focus group question also asked respondents whether they thought there should be a single
training entity or more than one entity providing certification trainings. Ninety-seven percent of
the responses indicate that stakeholders are most comfortable with allowing for a number of
training entities while having one overarching certifying body. Included in the options for
training entities are colleges and universities, CBOs (including those that are peer run) and
collaborations between entities. While a variety of organizations is encouraged, most responses
indicated that peer instructors/trainers should be involved in the actual training and/or operation
of the organization.
Only three percent of responses reflected the view that there should be a single training entity.
Stakeholders recognized that allowing for many different types of training entities would
increase access to training as well as allow for customization of the training for specific county
needs while maintaining a core curriculum.
65%
12%
13%
10%
Qualifications of Training Organization
Capacity Issues
Cultural Awareness andCompetency
Specific Skills andKnowledge
Process Oriented Training

14
Maintaining Peerness
Meeting participants clearly felt that in order for Peer Support Specialists (PSS) to maintain their
identity and job role as a peer, they must be collegially engaged with other peer providers. Forty-
two percent of all responses reflected the belief that networking with and supporting other peer
providers is essential for maintaining the values and philosophy of peer support. Networking
activities ranged from formal conferences to informal support groups. Respondents also
expressed the need to be engaged with other peer staff in a manner that is consistent with the
peer support value of a process orientation that allows people to share and receive feedback. The
value of mutuality and respect is repeated throughout the responses within this question and
throughout all of the focus group questions.
Nineteen percent of the responses indicated that the topic of “maintaining peerness” should be
included in the certification curriculum as well as offered as Continuing Education Units
(CEUs). Sixteen percent of the responses reflected the need to develop a consensus definition of
peer support. It is felt that such a definition can not only assist Peer Specialists in maintaining
their unique role but will also assist the system and colleagues in understanding and supporting
their role. Other responses to this question should help to inform the system on how to
incorporate the peer role into the workforce while maintaining the integrity of the role. These
21 19 18
14
9
4 4 3
0
5
10
15
20
25M
ult
iple
Tra
inin
g
Org
aniz
atio
ns
wit
h a
sin
gle
Cer
tify
ing
Bo
dy
Com
mu
nit
y C
oll
ege
and
Un
iver
sity
CB
O a
nd
Pee
r
Org
aniz
atio
n
Mu
ltip
le T
rain
ing
Org
aniz
atio
ns
incl
ud
ing
Pee
r O
rgan
izat
ion
s
Mu
ltip
le O
rgan
izat
ion
s
wit
h a
Sta
nd
ard
ized
Curr
icu
lum
CC
Pri
vat
e//C
oun
ty
Coll
abo
rati
on
CC
an
d P
eer
Run
Org
aniz
atio
n
Sin
gle
Enti
ty
One or More Training Entities
3. How should a training and certification process ensure that peer specialists are
able to maintain their “peerness”?

15
include: educating existing mental health staff on the role and value of peer support, ensuring
that recovery and wellness values are integrated into the workplace, addressing stigma within the
mental health workplace, supporting the advancement of Peer Support Specialists into leadership
roles, creating buy-in among county administration, developing a standardized code of ethics and
ensuring that there is always more than one peer support specialist on a team.
Qualifications of Supervisors
Responses to this question required that they be placed into five general categories and then an
analysis of the two categories that received the highest number of responses was conducted.
Below are the six general categories of responses from the stakeholder meetings. The majority of
these responses involved specific trainings that supervisors of Peer Support Specialists should
receive. Close behind is a list of general positive qualities that any supervisor should have. Forty-
six responses, or 23 percent, support lived experience as a requirement for supervising Peer
Support Specialists. Other qualifications include knowledge of the Peer Support Specialist role,
78
35 29
14 10 7
3 3 3 3
0
10
20
30
40
50
60
70
80
90
PSP
to
PSP
Net
wo
rkin
g/Su
pp
ort
Incl
ud
e in
th
e C
urr
icu
lum
an
dC
EU C
on
ten
t
Cre
ate
a D
efi
nit
ion
of
"Pe
ern
ess
"
Edu
cate
Co
lleag
ues
ab
ou
t th
eR
ole
an
d V
alu
e
Ensu
re R
eco
very
an
d W
elln
ess
Val
ue
s in
th
e W
ork
pla
ce
Ad
dre
ss S
tigm
a W
ith
in t
he
Me
nta
l He
alth
Sys
tem
Pe
er S
up
po
rt E
mp
loye
es in
Lead
ers
hip
Ro
les
Cre
ate
Ad
min
istr
ativ
e B
uy-
In
De
velo
p a
Co
de
of
Eth
ics
Ensu
re M
ore
Th
an O
ne
PSP
on
Team
How to Maintain Peerness
4. In addition to standard supervisory excellence, what additional
qualifications/training/experience do you think is needed for a supervisor of
peer support staff?

16
the ability to manage issues of inclusion and the ability to participate in a supervisors support
group.
Specific Supervisor Training Requirements
Stakeholders reported that supervisors of Peer Support Specialists should receive specialized
training in order to facilitate a good supervisory relationship. The majority of responses, thirty-
seven percent, reflect the need for supervisors to develop a management style that will create a
relationship with Peer Support Specialists that is reflective of the values of Peer Support.
These values include mutuality, a flattened hierarchical structure that prioritizes relationships
over the exertion of power, mutual respect and circular feedback and evaluation. The supervisor
in this type of environment takes on the role of mentor and facilitates a workplace where process
and teamwork are valued.
The next highest response, at twenty-one percent, is similar to the first. This training involves the
ability to create an environment reflective of wellness, resiliency and recovery values for
staff. This then would ideally be transferred to the relationship between staff and persons
receiving services. Other training requirements include: receiving the Peer Certification training
required for Peer Support Specialists, specific training on supervising Peer Support staff, training
to dispel the myths that peer support staff breach confidentiality more frequently and have more
severe boundary problems than do other staff, knowledge of the consumer/family movements,
knowledge of billing for Peer Support services and cultural competence, including
consumer/family member culture.
65
57
46
23
6 4
0
10
20
30
40
50
60
70
Require
Specific
Training
General
Postitive
Qualities
Require Lived
Experience
Clear
Knowledge of
Peer Role
Ability to
Manage
Inclusion and
Integration
Provide a
Support Group
for Supervisors
Qualifications of Supervisors

17
The most frequently stated qualification in the category of General Positive Qualities of
Supervisors identifies personal characteristics of the supervisor, (30 percent). These include
qualities that would ideally be present in all supervisors and are listed below.
Personal Characteristics of Supervisors
Uses authority well Able to tolerate multiple perspectives
Models awareness of personal growth and self-
care Equanimity
Non-stigmatizing Understanding
Willingness to not always be the expert Flexibility
Strengths based Knowledge of differences in learning curves
Belief in Recovery/Resiliency Good advocate
Welcoming Values honesty
Other qualities desirable in a supervisor of Peer Support Specialist include the ability to provide
support, good communication skills and empathy, encouragement of growth and advancement,
knowledge and effective use of accommodations and the ability to tolerate risk.
21
12
8 7
3 2 2 2
0
5
10
15
20
25M
anag
emen
t S
tyle
Ref
lect
ive
of
Pee
r S
upp
ort
Val
ues
Ab
ilit
y t
o C
reat
e a
Wel
lnes
s an
d R
eco
ver
y
En
vir
on
men
t fo
r C
lien
ts
and S
taff
Rec
eive
the
Pee
r
Cer
tifi
cati
on T
rain
ing
Sp
ecif
ic T
rain
ing
on
Su
per
vis
ing P
eer
Sp
ecia
list
s
Un
der
stan
d t
he
Myth
s an
d
Fac
ts A
bou
t
Con
fid
enti
alit
y a
nd
Bou
ndar
ies
Kn
ow
led
ge
of
Con
sum
er/F
amil
y
Mo
vem
ents
Kn
ow
led
ge
of
Bil
ling
fo
r
Pee
r S
up
po
rt S
ervic
es
Cult
ura
l C
om
pet
ence
Specific Training Areas

18
Additional Comments and Suggestions
This question provided each focus group with the opportunity to include feedback not already
captured by the stakeholder survey, the four focus group questions or questions asked during the
informational presentation. It was purposely left open to allow for maximum participation and
broad inclusion of issues or concerns.
Fifty two percent of the responses represent concerns associated with integration issues, career
ladder and workforce issues and certification curriculum. Integration issues refer to concerns that
Peer Support Specialists are stigmatized within the mental health workforce. Peer Support
Specialists want their role to be valued and understood by existing mental health staff. They see
their role as complementary to, not in competition with, other staff roles in the clinical setting.
Existing Peer Support Specialists often feel isolated, unwelcomed and misunderstood by the
traditional mental health professionals.
Career ladder and workforce issues are of vital importance to PSS staff. Generally, stakeholders
expressed a strong need to have a career ladder that would include non-certified peer support
staff. A concern exists that certification may become a barrier to employment for those
individuals who do not seek certification. This would ensure an entry level avenue for
employment for those not wishing become certified. A career ladder should also support
advancement beyond a Certified Peer Support Specialist or even a Peer Support job role. It was
expressed that many people would like to have a career ladder that includes lateral as well as
upward movement into leadership roles and non-peer roles such as Mental Health Rehabilitation
Specialist and Licensed Clinical Social Worker. Additionally, concern was expressed that
people with lived experience are tracked into Peer Support Specialist roles versus being given
more employment options beyond working in the mental health system.
Stakeholders also expressed concern that individuals at the entry level of the career ladder have
the opportunity to work in part-time positions with benefits as well as full-time positions. It was
also stated that certification should lead to career advancement with salary increases and other
financial benefits.
Another expressed concern is that Certified PSS’s could become perceived as a cheaper form of
labor for general clinical activities, thereby losing their unique role as Peer Support. Another
economic concern is that the cost of the bureaucracy to implement certification could result in
fewer jobs available. However, this concern is countered by the reality that there are not enough
job opportunities currently and it is hoped that certification will encourage the hiring of PSS
staff.
Curriculum issue concerns fell into three broad categories. First, participants expressed a strong
desire to have a process for vetting curriculum that would include stakeholder input. Secondly, a
number of content areas were suggested and these have been captured in the curriculum section
under the Stakeholder Survey. Third, meeting participants expressed a need for technology to
5. Additional comments/suggestions/questions?

19
include on-line courses and videoconferencing for networking purposes for those counties that
are either too small to create a critical mass for training or too rural to have ready access. The
remaining items addressed in this section are listed below. Most have been captured elsewhere in
this summary.
Survey Data Information The survey was completed by 129 stakeholders, or 78 percent of attendees. Below are the survey
responses.
Curriculum Type
1. In terms of training curriculum, which
do you prefer?
Survey respondents were asked whether or
not they preferred a core curriculum, with
specializations for particular training needs,
such as adult system of care, child/youth
system of care, whole health, etc. or a
separate training curriculum for each group.
22 21 21
9 8 8 8
7 5 5
4 4 3
0
5
10
15
20
25
Inte
gra
tio
n I
ssu
es
Car
eer
Lad
der
and
Work
forc
e Is
sues
Curr
icu
lum
Mai
nta
in P
eer
Val
ues
Mee
tin
g L
og
isti
cs
Job
Avai
labil
ity
Ad
voca
cy
Gra
ndfa
ther
ing
Pro
cess
Sm
all
and
Ru
ral
Co
un
ties
Cult
ura
l C
om
pet
ence
Nee
d t
o C
reat
e W
ork
pla
ce
Wel
lnes
s
Pai
rin
g w
ith
Oth
er
Cer
tifi
cati
on P
roce
sses
Tra
nsi
tio
n A
ged
Yo
uth
Issu
es
Other Comments
76%
24%
Type of Curriculum
One Core withSpecializations
SeparateSpecializedCurriculum

20
A majority of attendees thought that a single, core curriculum with specializations would be
preferable.
Curriculum Topics
2. In a core curriculum, which topics do you think should be included?
The survey listed 35 topics for consideration in a training curriculum for peer providers.
In addition, the survey included an “other” category where individuals could add topic areas
as needed.
There were 30 additional topic areas identified under “other”. Of these, three topics received
multiple recommendations: “self-care” was identified seven times, conflict resolution was
identified three times and Intentional Peer Support was identified twice.
0
20
40
60
80
100
120Curriculum Topics
21
Additional Curriculum Topic Areas Identified under “Other”
Self-care (7) Political aspects of mental illness
Wraparound principles
Conflict resolution(3) Social aspects of mental illness
Domestic violence
Intentional Peer Support (2) Values of peer support English course
Resiliency Peer leadership Typing/computer course
Local resources Disabilities Grief and Trauma training
Homelessness Forensic specialty History of mental health care
Special Education Creative process Health Navigator
Emerging research literature
Maintaining peerness Professionalism in the workplace
Alternative models of philosophy
Time management Non-violent crisis intervention
Manage up (manage your job skills)
Budgeting Medication education
Number of Training Hours in Curriculum
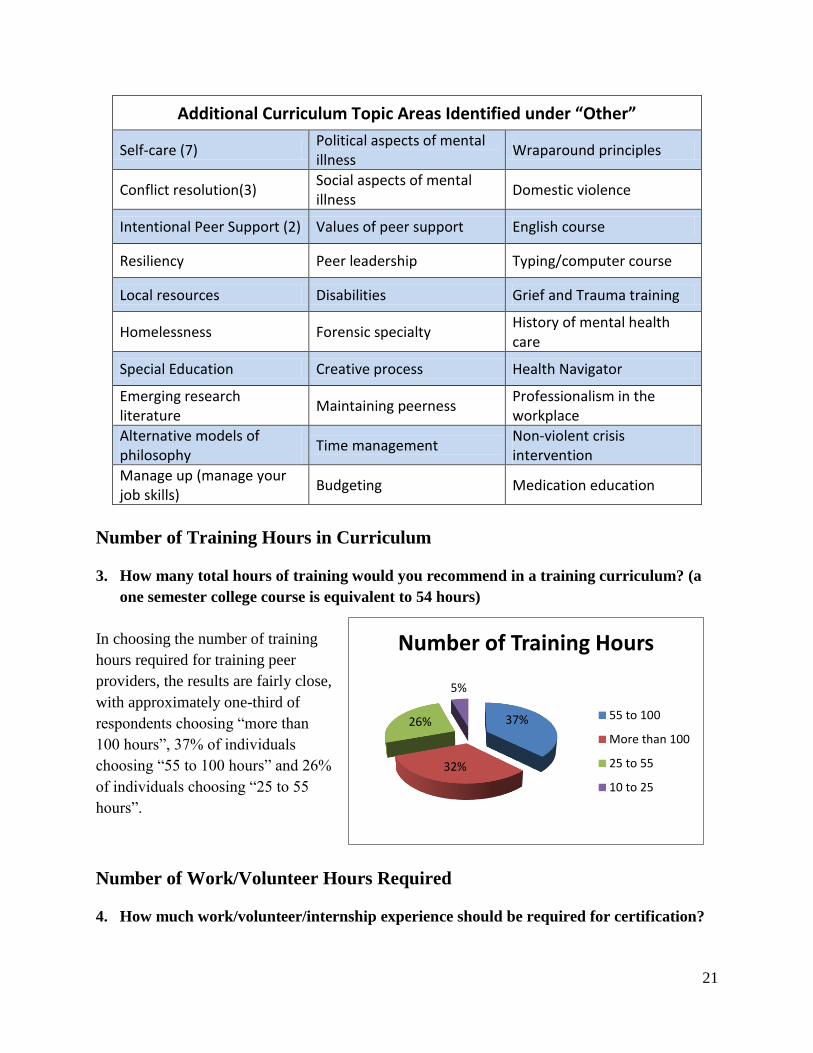
3. How many total hours of training would you recommend in a training curriculum? (a
one semester college course is equivalent to 54 hours)
In choosing the number of training
hours required for training peer
providers, the results are fairly close,
with approximately one-third of
respondents choosing “more than
100 hours”, 37% of individuals
choosing “55 to 100 hours” and 26%
of individuals choosing “25 to 55
hours”.
Number of Work/Volunteer Hours Required
4. How much work/volunteer/internship experience should be required for certification?
37%
32%
26%
5%
Number of Training Hours
55 to 100
More than 100
25 to 55
10 to 25
22
Certification programs often require
a number of work or volunteer
hours be completed prior to
receiving certification. Almost one-
third of survey respondents chose
“3-6 months” of work/volunteering
experience and 24 percent chose
”six months – one year” of
work/volunteer as the minimum
qualification in this area. The
remaining options were all tied at
11 percent: no requirement, 20-40
hours, 40-80 hours and more than
one year of work/volunteering.
Examination Requirements
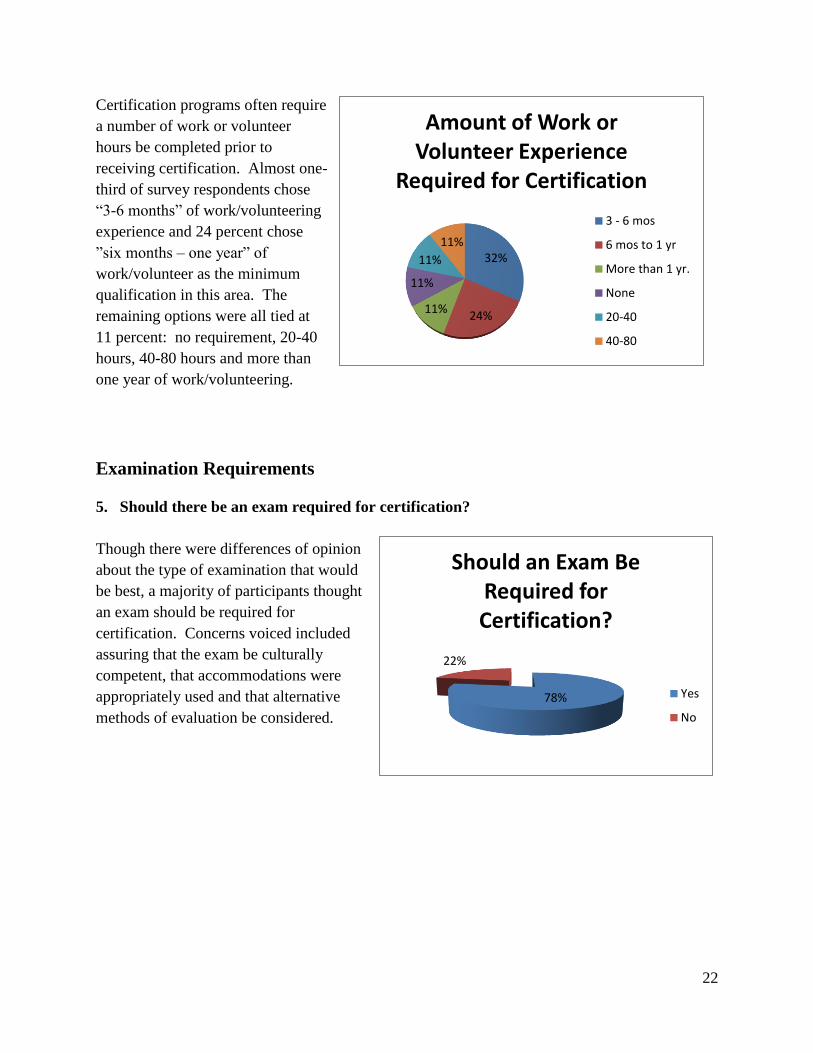
5. Should there be an exam required for certification?
Though there were differences of opinion
about the type of examination that would
be best, a majority of participants thought
an exam should be required for
certification. Concerns voiced included
assuring that the exam be culturally
competent, that accommodations were
appropriately used and that alternative
methods of evaluation be considered.
78%
22%
Should an Exam Be Required for Certification?
Yes
No
32%
24% 11%
11%
11%
11%
Amount of Work or Volunteer Experience
Required for Certification
3 - 6 mos
6 mos to 1 yr
More than 1 yr.
None
20-40
40-80

23
Continuing Education Requirements (CEUs)
6. How many Continuing Education Units should be required per year to maintain
certification?
Stakeholders were asked to consider how
many continuing education units would be
appropriate to maintain certification.
Almost half of the survey respondents chose
“10-15 hours per year”. Another 26%
thought that “15-20 hours” of CEU training
would be best.
Certification Renewal
7. How frequently should the certification be renewed?
Stakeholders were asked to respond to the issue of renewal of certification and determine the
time period appropriate for re-certification. In this question, 43 percent of survey respondents
opted for “every two years” and 30 percent chose “every three years”.
Seventeen percent of respondents opted for annual
re-certification and ten percent thought there should
not be any re-certification requirements.
46%
26%
17%
11%
CEU's Required to Maintain Certification
10 to 15
15 to 20
20 to 30
None
43%
30%
17%
10%
Re-Certification Requirements
Every twoyears
Every threeyears
Annually
Not at all
24
Certifying Body
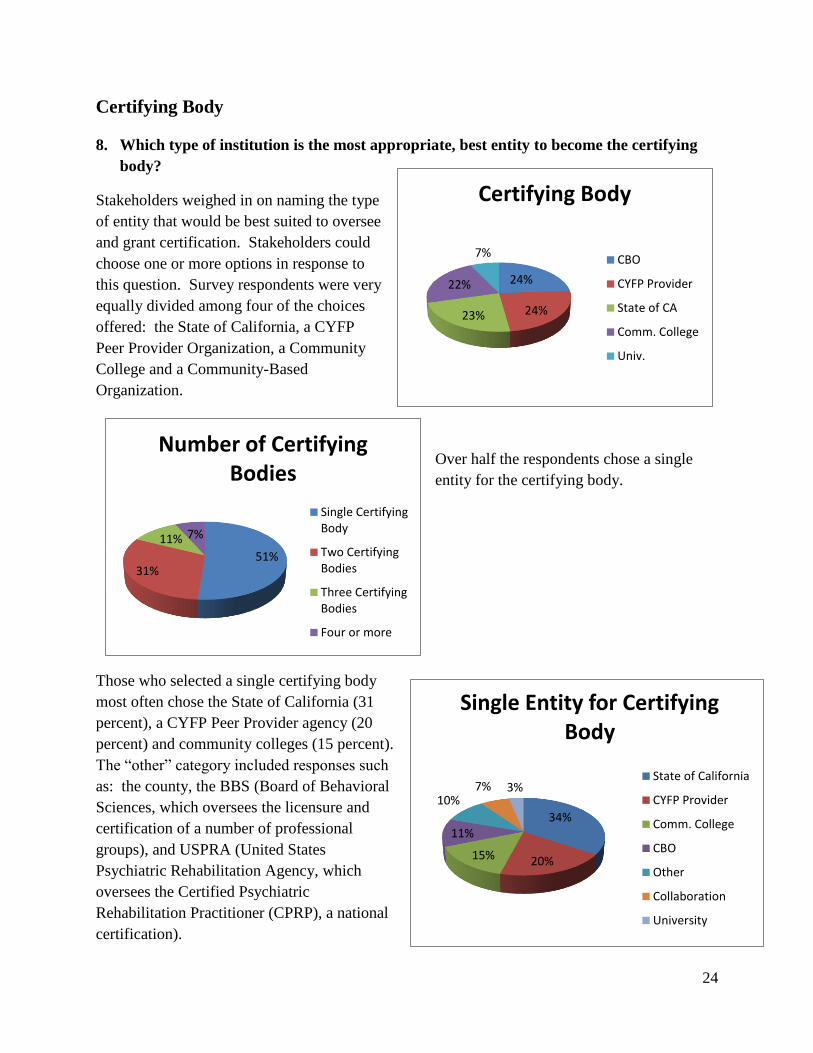
8. Which type of institution is the most appropriate, best entity to become the certifying
body?
Stakeholders weighed in on naming the type
of entity that would be best suited to oversee
and grant certification. Stakeholders could
choose one or more options in response to
this question. Survey respondents were very
equally divided among four of the choices
offered: the State of California, a CYFP
Peer Provider Organization, a Community
College and a Community-Based
Organization.
Over half the respondents chose a single
entity for the certifying body.
Those who selected a single certifying body
most often chose the State of California (31
percent), a CYFP Peer Provider agency (20
percent) and community colleges (15 percent).
The “other” category included responses such
as: the county, the BBS (Board of Behavioral
Sciences, which oversees the licensure and
certification of a number of professional
groups), and USPRA (United States
Psychiatric Rehabilitation Agency, which
oversees the Certified Psychiatric
Rehabilitation Practitioner (CPRP), a national
certification).
51% 31%
11% 7%
Number of Certifying Bodies
Single CertifyingBody
Two CertifyingBodies
Three CertifyingBodies
Four or more
34%
20% 15%
11%
10% 7% 3%
Single Entity for Certifying Body
State of California
CYFP Provider
Comm. College
CBO
Other
Collaboration
University
24%
24% 23%
22%
7%
Certifying Body
CBO
CYFP Provider
State of CA
Comm. College
Univ.

25
Funding for Certification
9. How should certification be paid for?
121 survey respondents chose one or more of
four options for funding the certification
process: state MHSA dollars, the county,
individual fees and other. Overall, 53 percent
of responses reflect a preference for using
statewide MHSA dollars for funding, 22
percent preferred using individual fees and 12
percent preferred using county funding. In
addition, 13 percent identified other options,
which include scholarships and grants,
Department of Rehabilitation, federal
workforce monies and CBO’s employing peer
providers.
Overall, 48 percent of the respondents chose
a single funding source while 32 percent
chose two funding sources, 12 percent chose
three and two percent chose four funding
sources.
Further evaluation showed that of the
respondents who chose a single funding
source, 78 percent of chose MHSA monies,
10 percent chose individual fees, nine
percent chose county funding and three
percent chose other. When responses from
individuals choosing two funding sources
were evaluated, 40 percent chose MHSA
monies, 27 percent chose county funding, 23
percent chose individual fees and 10 percent
chose other options.
53% 22%
12%
13%
Recommended Funding for Certification
StatewideMHSA
Individual Fees
Per County
Other
48%
38%
12% 2%
Number of Funding Sources Selected
Single FundingSource
Two fundingsources
Three fundingsources
Four or more

26
The most common pairing was the MHSA and county funding, chosen by 46 percent of
respondents. Next most common combination was the MHSA and individual fees, chosen by 26
percent. The third most common combination was the MHSA and other sources, chosen by
eight percent of respondents.
“Grandfathering in” Recommendations
10. What should be the policy regarding certification for all those who are currently
working as Peer Specialists within the mental health system?
There are many peer providers currently employed within the county mental health system,
community-based organizations and peer provider organizations. Stakeholders were asked to
weigh in on the concept of grandfathering people in regarding certification.
Survey respondents were
fairly equally divided
among the top two choices:
“ a minimum of one year’s
experience” and “having a
set number of years of
experience plus three letters
of recommendation” (39
percent and 36 percent
respectively) and equally
divided among the other
two choices: “no
experience requirement”
and “a minimum of five
years of experience” (13 percent and 12 percent).
39%
36%
13%
12%
Grandfathering In Requirements
Minimum of 1 year ofexperience
Set number of years,plus 3 letters ofrecommendation
No experiencerequirement
Minimum of 5 years ofexperience
78%
10% 9% 3%
Single Funding Source
StatewideMHSAIndividualFeesCounty
Other
40%
27%
23% 10%
Two Funding Sources StatewideMHSA
Per county
Individual
Other
27
Mechanism for Billing Medi-Cal
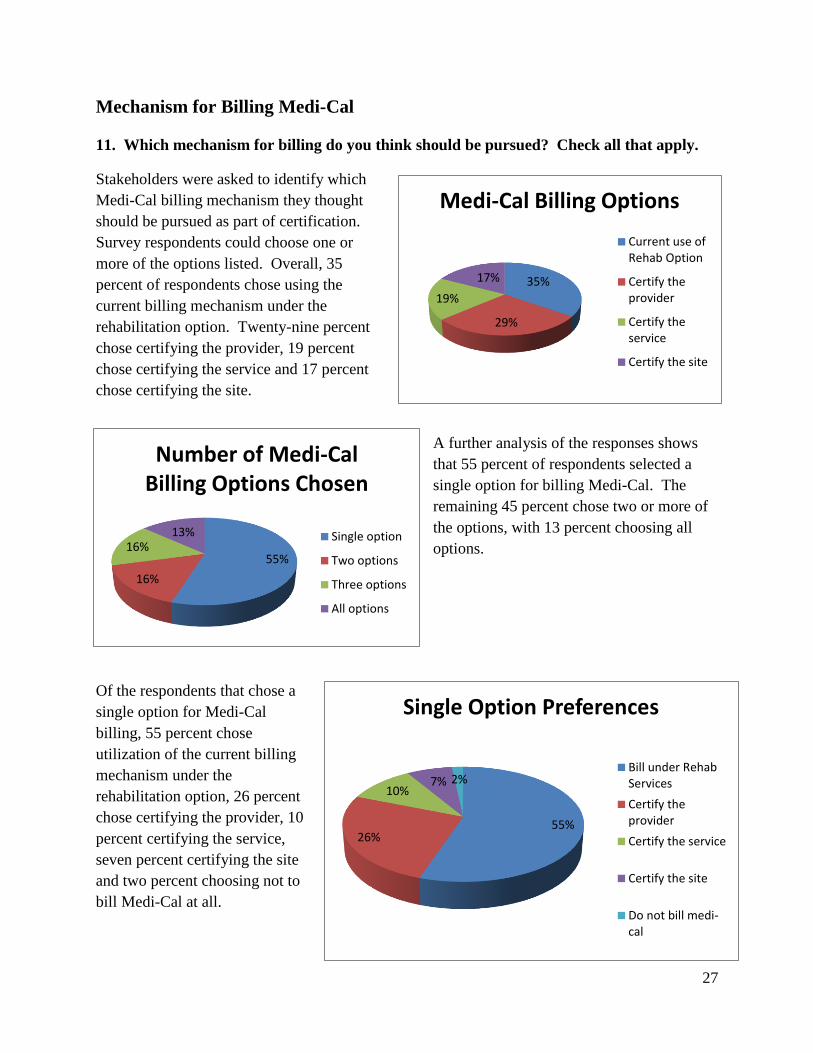
11. Which mechanism for billing do you think should be pursued? Check all that apply.
Stakeholders were asked to identify which
Medi-Cal billing mechanism they thought
should be pursued as part of certification.
Survey respondents could choose one or
more of the options listed. Overall, 35
percent of respondents chose using the
current billing mechanism under the
rehabilitation option. Twenty-nine percent
chose certifying the provider, 19 percent
chose certifying the service and 17 percent
chose certifying the site.
A further analysis of the responses shows
that 55 percent of respondents selected a
single option for billing Medi-Cal. The
remaining 45 percent chose two or more of
the options, with 13 percent choosing all
options.
Of the respondents that chose a
single option for Medi-Cal
billing, 55 percent chose
utilization of the current billing
mechanism under the
rehabilitation option, 26 percent
chose certifying the provider, 10
percent certifying the service,
seven percent certifying the site
and two percent choosing not to
bill Medi-Cal at all.
35%
29%
19%
17%
Medi-Cal Billing Options
Current use ofRehab Option
Certify theprovider
Certify theservice
Certify the site
55%
16%
16% 13%
Number of Medi-Cal Billing Options Chosen
Single option
Two options
Three options
All options
55% 26%
10% 7% 2%
Single Option Preferences
Bill under RehabServices
Certify theprovider
Certify the service
Certify the site
Do not bill medi-cal
28
The analysis of the responses to this question reveals a very mixed picture. There is a need for
further stakeholder information and discussion as pointed out in the recommendations.
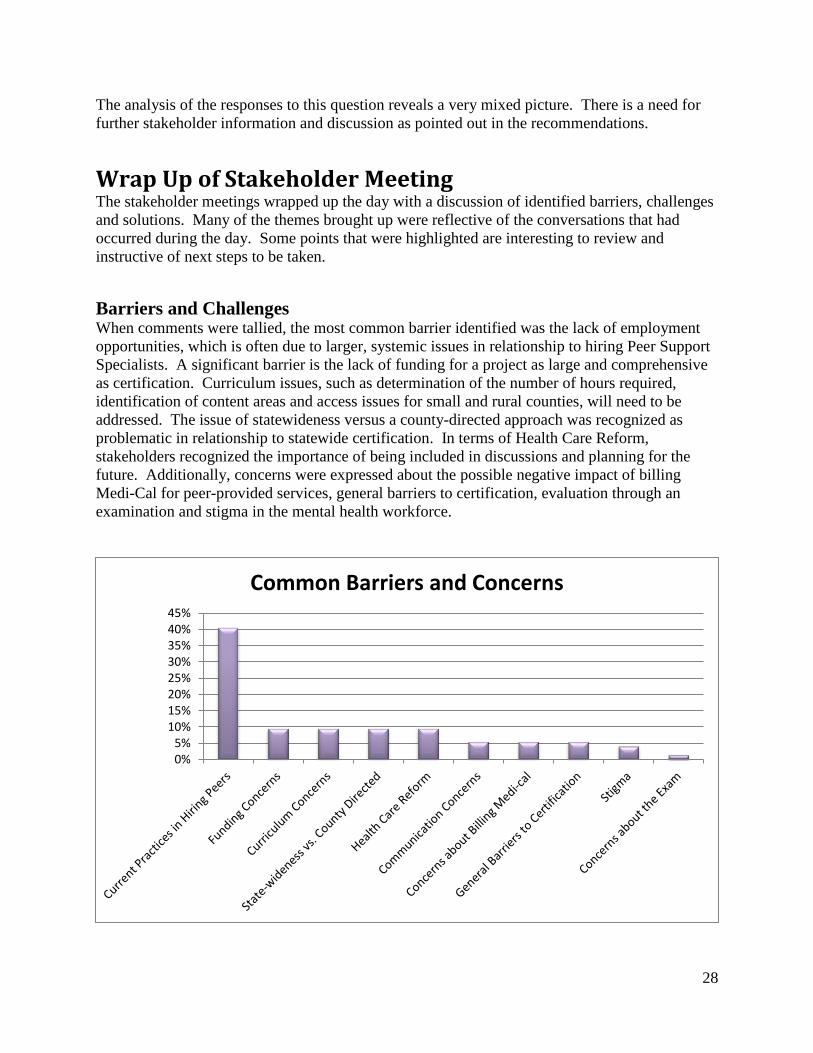
Wrap Up of Stakeholder Meeting The stakeholder meetings wrapped up the day with a discussion of identified barriers, challenges
and solutions. Many of the themes brought up were reflective of the conversations that had
occurred during the day. Some points that were highlighted are interesting to review and
instructive of next steps to be taken.
Barriers and Challenges When comments were tallied, the most common barrier identified was the lack of employment
opportunities, which is often due to larger, systemic issues in relationship to hiring Peer Support
Specialists. A significant barrier is the lack of funding for a project as large and comprehensive
as certification. Curriculum issues, such as determination of the number of hours required,
identification of content areas and access issues for small and rural counties, will need to be
addressed. The issue of statewideness versus a county-directed approach was recognized as
problematic in relationship to statewide certification. In terms of Health Care Reform,
stakeholders recognized the importance of being included in discussions and planning for the
future. Additionally, concerns were expressed about the possible negative impact of billing
Medi-Cal for peer-provided services, general barriers to certification, evaluation through an
examination and stigma in the mental health workforce.
0%5%
10%15%20%25%30%35%40%45%
Common Barriers and Concerns
29
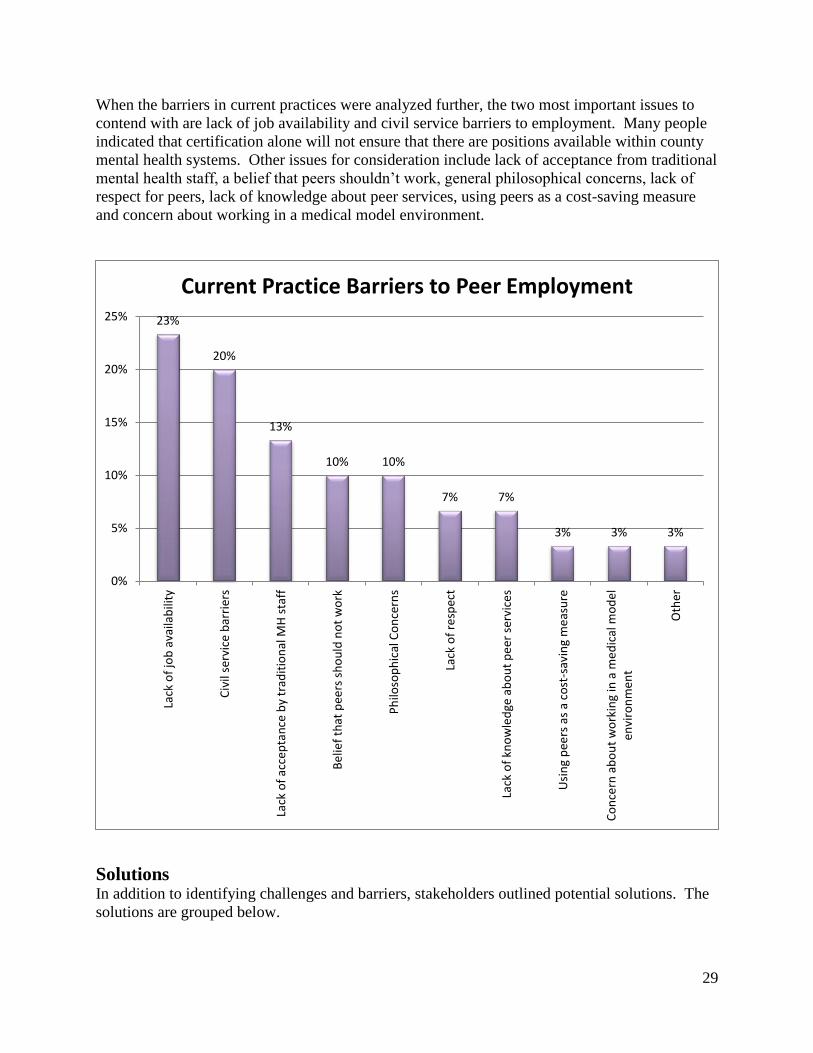
When the barriers in current practices were analyzed further, the two most important issues to
contend with are lack of job availability and civil service barriers to employment. Many people
indicated that certification alone will not ensure that there are positions available within county
mental health systems. Other issues for consideration include lack of acceptance from traditional
mental health staff, a belief that peers shouldn’t work, general philosophical concerns, lack of
respect for peers, lack of knowledge about peer services, using peers as a cost-saving measure
and concern about working in a medical model environment.
Solutions In addition to identifying challenges and barriers, stakeholders outlined potential solutions. The
solutions are grouped below.
23%
20%
13%
10% 10%
7% 7%
3% 3% 3%
0%
5%
10%
15%
20%
25%
Lack
of
job
ava
ilab
ility
Civ
il se
rvic
e b
arri
ers
Lack
of
acce
pta
nce
by
trad
itio
nal
MH
sta
ff
Be
lief
that
pee
rs s
ho
uld
no
t w
ork
Ph
iloso
ph
ical
Co
nce
rns
Lack
of
resp
ect
Lack
of
kno
wle
dge
ab
ou
t p
eer
ser
vice
s
Usi
ng
pee
rs a
s a
cost
-sav
ing
me
asu
re
Co
nce
rn a
bo
ut
wo
rkin
g in
a m
ed
ical
mo
de
len
viro
nm
en
t
Oth
er
Current Practice Barriers to Peer Employment
30
Job Availability Solutions
Require that county contracts with the state include a set number/percentage of Peer
Support positions.
Financial Solutions
Utilize MHSA/Workforce Education and Training monies
Redirect some of the millions of dollars currently allocated to other guilds, such as social
workers, to fund certification
Utilize revenue generated from billing for peer services
Provide scholarships
Medi-Cal Billing Solutions
Incorporate Quality Improvement Departments in the discussion of Peer Support.
Educate mental health providers about recovery and resiliency oriented treatment
planning to assure that treatment plans are strengths-based and compatible with recovery
and resiliency.
Integrate peer services into the treatment plan.
General Certification Solutions
Look to the state and nationally for organizations with existing infrastructure that can
take on the issue of peer provider certification.
Statewideness Solutions
Use the opportunity of this coming year to prepare for creation of a state plan amendment
that would outline the essentials of peer certification.
Educate mental health directors about certification and employment of peers.
Use templates regarding job descriptions and policies that have been created successfully
in other similar fields.
Create curricula standards broad enough to allow multiple curricula to be vetted for
certification of peers.
Create an authorizing body that prepares trainers.
Stigma Solutions
Join in on events that celebrate disclosure of lived experience, such as National Coming
Out Day or the Up to Us Campaign.
Create safe environments for mental health professionals to disclose lived experience.
Train the workforce to welcome and value peer providers.
Share recovery stories.
Exam Solutions
Create alternative evaluation methods such as oral exams.
Utilize accommodations to enhance success in taking the exam.

31
Critical Decisions for Implementation Planning The stakeholder process included an analysis of existing national certification efforts as well as a
description of current practices in California regarding the hiring and training of Peer Support
Specialists. These findings were included in a report entitled, Certification of Consumer, TAY,
Family and Parent Peer Providers, A Review of the Research. This report included a summary
of critical decision points necessary for implementation planning. The stakeholder meetings
provided some key information on values as well as clear direction for future planning. In an
effort to contextualize and expand upon relevant information from the stakeholder meetings in
relationship to the indicators included in the research report we have included the outline from
the report here. Together, these underscore the critical nature of the findings. Where information
gathered from the stakeholder meetings intersects with these decision points, it has been included
within the outline.
Stakeholder Input Regarding Critical Decisions for Implementation Planning
1. Identification of a Certifying Body
While the information from the survey appears mixed on who should be the certifying
body, an analysis of those restricting themselves to one response shows that choosing the
state through an existing entity such as the Board of Behavioral Sciences (BBS) or the
Department of Health Care Services would be an acceptable choice.
2. Infrastructure Needs
The stakeholders clearly felt that the capacity to manage the various functions of a
certification process was a key priority in choosing a certifying body. These functions
include the ability to manage the multiple functions of certification including, but not
limited to, authorizing training entities/trainers, establishing eligibility and granting
certification, auditing Continuing Education requirements, managing complaints and
possible ethical violations and certification renewal. The cost of such an infrastructure
was a major concern and it was felt that utilizing an existing state body with existing
capacity would be the wisest choice.
3. Training
Stakeholders provided information on a variety of issues related to training.
A minimum of 55 hours of training should be required. Thirty two percent of
stakeholders felt that 100 hours or more of training should be required.
A variety of training organizations qualified to provide training is supported by
stakeholders. Additionally, partnership between educational entities and CBO’s is
encouraged. Generally, stakeholders reported that variety of training entities
should be encouraged to allow for ease of access as well as meeting the needs of
individual counties.
Training entities should meet a number of qualifications (see Qualifications for
Training Entities) in order to best serve certificate recipients as well as those
receiving services.
Trainers with lived experience themselves is highly valued and should be a
deciding factor in choosing training entities.

32
4. Core Curriculum
Stakeholders believe that there should be a core curriculum for all Peer Support
Specialists with specialized curricula tracks for the type of peer provider as well as
specific areas of specialization including health care, trauma informed care and forensic
services. Stakeholders also reported that peers themselves should be involved in
determining content areas for curricula. It was also felt that multiple curricula could be
utilized if core content areas are established and each curriculum is reviewed to assure
that these content requirements are met. This allows existing curricula to be used and
allows each county to individualize training to their specific needs.
5. Core Competencies
Stakeholders felt that the development of standardized core competencies for Peer
Support Specialists is critical. Peers should be integrally involved in the development of
these core competencies. Additionally, a code of ethics should be developed or an
existing code adopted.
6. Measurement
Stakeholders strongly believe that an exam-based certification is appropriate. However, it
will be important to include alternative forms of testing beyond that of a written exam.
Oral testing should be an option and educational supports and accommodations should be
provided.
7. CEUs
The majority of stakeholders stated that Certified Peer Specialists should receive between
10-15 hours per year of continuing education units to maintain their certification.
Meeting participants stressed the importance of including the topic of “maintaining
peerness” in course offerings.
8. Meeting Centers for Medi-Care and Medicaid Services (CMS) Guidelines
Stakeholder comments regarding care coordination indicate a concern that current
treatment planning practices may not be consistent with the philosophy of person-
centered and parent/family driven care. Stakeholders are hopeful that current efforts to
train existing mental health staff in implementing wellness and recovery and resiliency
oriented treatment plans will create an environment where peer services can be easily
incorporated within a holistic service plan. Additionally, it is felt that certified Peer
Specialists should be included as providers able to work with clients and family members
in developing treatment plans.
With regard to supervision, meeting attendees stressed that individuals who supervise
Peer Support Specialists should be able to develop a working relationship that is based
upon the values of peer support and wellness and recovery principles. These are
discussed in this paper under Qualifications of Supervisors. Additionally supervisors
should have specific training geared toward developing a good knowledge of the peer
role and how to supervise peer support specialists. Having lived experience is also highly
valued in a supervisor.
33
9. Options for Medi-Cal billing
Based upon responses to the survey, most stakeholders felt that utilizing the current
rehabilitation option for Peer Support Specialists to bill Medi-Cal was preferable.
However, verbal responses during the stakeholder meetings indicated that stakeholders
generally supported the use of at least four options: certifying the provider, certifying the
service, certifying the site and utilizing existing ability to bill under the rehabilitation
option. There were expressed concerns that certifying the provider or service could result
in lower billing rates. Stakeholders felt that a lower billing rate would be a disincentive to
counties and therefore counties would not favor these options.
The results may also reflect the complexity of the issue. A key factor that could have
affected stakeholders’ opinions is the lack of knowledge about the options themselves,
the nuances related to choosing more than one option and the intended and unintended
consequences of choosing one option over another. Going forward it would be necessary
to utilize content experts to delve more fully into these issues to allow for a more
informed decision.
10. Funding and Sustainability
Stakeholders strongly support the use of MHSA money to support the administration of a
certification program as well as to pay for individual fees through stipends and grants.
State level MHSA monies are currently used to fund a variety of financial incentive
programs targeting graduate level degrees related to mental health.
11. Partnering with Statewide Organizations
Stakeholders agreed that creating partnerships with key state entities is essential to
forward progress on the path of certification. Decision-makers at the state level are
important to include in discussions. Stakeholders felt that regular communication with
groups such as the California Mental Health Directors Association, the Department of
Health Care Services and California Center for Medicaid Services would enhance the
buy-in and ease the process considerably.
12. Employability
Stakeholders expressed concern about the lack of availability of jobs. Certification
without employment opportunities creates disincentives to embark on the rigorous
process of becoming certified. Several factors mentioned by stakeholders relate to the
need to prepare the current workforce for the inclusion of peer providers: lack of
understanding about the role of peer providers, lack of belief that peers should be
working, philosophical concerns and a lack of acceptance from traditional mental health
staff.
Stakeholders ranked civil service barriers second among the top two barriers to
employment of peer providers. This will require ongoing attention and problem-solving
to address issues such as a lack of appropriate coded positions to accommodate these new
employees, restrictive hiring practices and union concerns about practices such as
“bumping”, where seniority plays a significant role in determining lay-offs.

34
Partnering with Human Resources was also mentioned as an important way to address the
problems related to hiring practices, the creation of job descriptions and clear policies and
procedures related to the employment of peers.
13. Career Ladder
Stakeholders discussed the need for career ladder opportunities and suggested creating
step levels within the Peer Support Specialist classification as well as articulating the
career ladder moves laterally and upward through other classifications. Stakeholders also
suggested that opportunities for advancement may be increased through assuring that
Peer Support Specialists can produce revenue through the ability to bill Medi-Cal for
services. Generating revenue for the system is a potential factor that could influence the
value placed on these positions.
14. Portability
In order to have portability across county lines, county mental health directors must buy
in to the certification standards that are developed and vet the training as able to produce
qualified individuals for work in the mental health system. Some stakeholders have
mixed feelings about a statewide certification. In order to have portability, the county
mental health directors need to come to an agreement about this issue.
15. Rural and Small County Issues
Representatives from small and rural counties expressed concern that statewide
certification may be problematic if there isn’t good participation and input received from
their constituency. Stakeholders confirmed the importance of issues such as difficulty
accessing trainings. Small and rural counties often do not have a critical mass of peers to
be trained. Transportation is a difficulty as well. Concern was also expressed by small
counties who had invested considerable time and attention in development of their own
peer provider trainings and whether their work would be vetted in a statewide process.
16. Health Care Reform
Stakeholder recognized that Health Care Reform offers great opportunities for Peer
Support Specialists going forward and see the need to include healthcare content into the
core curriculum and/or develop specialty curricula to prepare Peer Support Specialists for
these new positions. A key concern is that stakeholders are included in the discussions
happening at the state level with regard to the upcoming implementation of Health Care
Reform.
Question and Answer Sessions During each stakeholder meeting, there were three opportunities scattered throughout the
PowerPoint presentation to ask questions, seek clarification and provide input. Each of these
sessions was transcribed and is presented by stakeholder meeting in Addendum I.

35
Recommendations The recommendations that follow are based upon the input from participants in the Stakeholder
process and are not listed in order of priority. This should not be considered a comprehensive
list as new information and input from other interested parties and experts will necessitate on-
going revision of plans and recommendations.
1. Develop a statewide certification for Peer Support Specialists that will legitimize peer
support as an effective and necessary service to clients and family members.
a. Training should consist of a minimum of 55 hours.
b. Develop a standardized set of core content areas for curricula for all PSS’s with
specialty modules to meet the specific needs of the consumer/survivor, TAY, family
and parent specialists, as well as specialized content areas.
c. An exam should be required with adequate educational supports including alternative
evaluation techniques including a verbal exam.
d. Establish a work/volunteer experience requirement of three months to one year.
e. Establish a CEU requirement of 10-15 hours per year to maintain certification.
f. Re-certification should be done every two years.
g. Allow for a grandfathering process to include at least one year of full-time equivalent
work and three letters of recommendation.
2. Include PSS as a provider type within the State Plan for Specialty Mental Health. Allow for
maximum flexibility in what PSSs can bill for including, but not limited to, peer support,
rehabilitation services including group and individual, collaterals, recovery planning,
strengths based assessments and targeted case management.
3. Include in the State Plan an option for peer-operated agencies to provide an array of mental
health services, including peer support, which can be billed under Medicaid. An option to
allow stand-alone peer operated agencies to specialize in and provide only peer support
services should be included as well.
4. Request that the county mental health directors adopt whatever statewide requirements are
developed for certification and billing practices to avoid individual counties adding
requirements beyond those specified by the Centers for Medicaid and Medicare and the
Department of Health Care Services.
5. Develop a statewide definition and code of ethics for PSSs.
6. Evaluate the possibility of broadening the definition of “service recipient” to include parents
and family members of individuals receiving services so that peer support services can be
documented and billed more directly and clearly.
7. Develop a plan for funding a certification process utilizing Workforce, Education and
Training monies from the MHSA.

36
8. Address the concern that current practice of documentation for billing may not be aligned
with the values and principles of peer support and a wellness, recovery and resiliency
orientation.
9. Provide extensive and expansive training on the values, philosophy and efficacy of peer
support to mental health administration and clinic staff.
10. Develop a policy statement regarding the importance of maintaining the integrity of peer
support as a mechanism for avoiding the potential incentive to drift from peer support to
providing services in a more traditional manner as well as utilizing PSSs as less expensive
labor for other clinical duties.
11. Develop a statewide solution to deal with civil service barriers to the employment of PSSs
into specified coded positions.
12. Address the problem of lack of employment opportunities for PSSs by establishing a
statewide workforce minimum to comply with the intent of the MHSA.
13. Develop career ladders for PSSs that begin with non-certified PSSs and create lateral as well
as upward mobility including leadership positions. Develop statewide models that can inform
county leadership.
14. Create welcoming environments that embrace the use of multidisciplinary teams that can
incorporate PSSs fully onto mental health teams.
15. Select a single certifying body to implement and manage the certification of PSS’s. The
certifying body would preferably be an existing state body or a statewide agency that
represents Peer Support Specialists.
16. Develop standards and oversight for training providers. Trainers must either be individuals
with lived experience or a team of individuals that includes people with lived experience.
Ensure that a number of training organizations and/or collaborations of training entities
would be eligible. Ensure that these organizations have existing infrastructure to support the
considerations expressed by stakeholders in the “Qualifications of Training Organizations”.
17. Develop a policy to establish qualifications for who may supervise Peer Support Specialists.
Stakeholders clearly prefer that people with lived experienced provide supervision. However,
due to capacity issues the remaining qualifications may have to suffice. These include
specific training for supervisors as well as the presence of personal characteristics that align
with peer support values and philosophy.
18. Develop a policy that supports the importance of PSSs maintaining their “peer” role. This
will involve creating networking opportunities, both formal and informal to allow for the
profession itself to grow as well as to allow PSSs to maintain and hone their professional
values and principles.

37
Conclusion
Stakeholders across the state weighed in on the complicated issues concerning the certification of
peer providers and articulated a set of recommendations to further the process. A majority of
participants believed the purpose of certification would be both a formal validation of their role
in the mental health system and the ability to bill to Medi-Cal. Similarly, a large majority
believed certified peer providers should be trained by other peers or qualified persons with lived
experience. Stakeholders suggested certified peer providers could maintain their identity and job
role through networking with and supporting other peer providers as well as including this topic
in both the certification curriculum and continuing education. Additionally, supervisors of peer
providers should receive specialized training to facilitate a good supervisory relationship.
Additional concerns and comments in the regional focus groups included integration issues
within mental health, a career ladder for both certified and non-certified peer providers, and input
into the curriculum required for certification. Finally, stakeholders identified the two biggest
barriers to current peer employment were the lack of job availability and civil service barriers.
Overall, the participants agreed certification must be driven by people with lived experience,
family members and parents modeling what has been successfully done in many states across the
country.
The stakeholder process included reviewing the report on existing national certification efforts
and current practices in California and soliciting input regarding critical decisions for
implementation planning. For example, stakeholders believe continuing education should be
required as well as use of MHSA funds to support the administration of a certification program.
The recommendations from these stakeholder meetings will be presented in a final statewide
summit to gather additional feedback and finalize the recommendations to the State of California
regarding certification of peer providers.

38
Addendum I
Regional Forum on State Certification for Consumer/Youth/Family Parent Peer Support
Services - Central Region 3.23.12
Questions and Comments Central Region Section I
1. Grandfathering in? What will happen?
2. Legitimacy word is offending – feels that people are past that. Be careful of language used
when discussing it. Really what we want to assure is the quality of service and expertise.
3. Supervision – would qualifications be written in the amendment?
4. Peers can bill now for services under the Rehab Option.
5. Job descriptions
6. Why is the TAY certification separate from a consumer certification? There is a felt need for
youth-generated, youth culture-oriented services and skills.
7. How will people who are coming out of the legal system be able to be used? Howie the Harp
organization offers a Forensic Peer Specialist Certification. May be used as an example of
how to do it.
8. The system of amendments and waivers has been going on a long time. How long do they
take to take effect? Once approved, a date is set. Not sure how long it takes to get an
amendment through the process. Been told that a window of opportunity in California will
be within the next year or two. Time to start the work is now.
9. Look for a better way to describe Forensic peer specialist.
10. The county has flexibility about who bills. One example, Community Action Marin is peer-
run and contracted with Marin County, and bills under rehab services.
11. Eleven counties (that we are aware of) currently bill Medi-Cal for peer services
12. Do peer providers need a National Provider Identification (NPI)?
13. Overmatch situations – needs additional scrutiny.
14. Providers (CBO’s) may also choose not to bill for peer services.
Section II
1. Licensed/unlicensed
2. Are the peers that are doing billing working directly for the county or CBO’s? Both are true.
3. Are peers who bill doing this under a clinician? Treatment plan is the basis for billing for
any provider.
4. Other qualified provider must meet the minimum qualifications of being 18 and having a
high school diploma.
5. Why certify? Might be able to assure that peer services are provided in a recovery-resiliency
oriented way.
6. You could create a peer provider that does not require a high school diploma.
7. May raise the bar for all services to be more recovery and resiliency-oriented services.
39
8. MH directors can set the standards for the county. If you set the competencies and standards
and create a whole package for directors to be able to mitigate the risk, this can help. They
do not HAVE to accept certification, but it will help.
9. Is there a plan they can be forced to accept? No, and probably it is best that people do have
choice and a good working relationship.
10. In California, there is no Medi-Cal definition of peer provider. Counties however are hiring
people as peer providers.
11. Changes will be happening as we change to the Department of Health Care Services. They
need to be at the table and have been invited to be partnering in these discussions.
12. Be willing to update language and use language in a sensitive manner, respectful.
Section III
1. List of reported job requirements is on pg. 23 of the research paper. Lived experience plus
recovery is one example of a job requirement – what does this mean? One county only
stipulated the need for demonstrated recovery plus lived experience.
2. Some counties do want to see documentation that you have received mental health services
as a job requirement.
3. Pillars of Peer support reports can be found at pillarsofpeersupport.org or use Network of
Care, which has a link to the report.
4. Why include the MHSOAC? Aren’t they just MHSA? Their role is broadening and can be a
helpful advocacy group in this effort.
5. Include California Office of Statewide Health Planning and Development (OSHPD)
6. Could Health Care Reform dismantle what we have?
7. Are Primary Care Providers (PCP) going to be retrained? It’s required that they receive
mental health and substance abuse training.
8. Health care reform is being implemented in Fresno. They did a survey of Peer Providers to
find out what they need for training.
9. Health care reform needs to be on people’s minds as we approach the task of certification.
May need training to work in physical health care settings. May need a specialty curriculum
for this kind of employment.
10. Not sure how the funding for training is being drawn down.
11. What is the availability of jobs? Can certification ensure that people will have jobs? We
need to find out about the need for peer providers. Need to educate employers about the
benefits and competencies of peers to increase peer provider positions – this might be done
through a guild organization.
12. Coordination of health care – a morbidity study that consumers are dying ten years younger
than their non-consumer peers. Wants to reduce the morbidity rate and increase of health of
consumers. (Mortality and Morbidity Study).

40
Regional Forum on State Certification for Consumer/Youth/Family Parent Peer Support
Services – Greater Bay Area Region 4-16-2012
Questions and Comments Greater Bay Area Region
Section I
1. Would the payment of peer provided services be less than other rehab services? Yes, it is
likely that peer services would be paid at a lower rate.
2. The lower rate is a push and pull. One of the things we wanted is to have peer services
legitimized. Peer support services are different, based on connecting, vs. traditional services
which are assessing and objectifying.
3. Essential to have peer provided services called out to provide validity for the wider range of
services than falls under Rehab Option.
4. Creation of a distinct service is different from creation of a distinct provider type.
5. Sites can bill for services as well as do non-billable services.
6. If health care reform goes through, more managed care entities will come in to be the
provider of mental health services. OptumHealth is an example, working in San Diego.
7. If you are not certified as a Medi-Cal provider (as an agency for example), you can’t bill.
8. Potential issue with acting as a peer provider and other qualified provider at the same time.
9. Provider sites can be defined as having peer providers and peer services – can be creative due
to the flexibility in the negotiation.
10. Could peers bill as private practitioners? Any group that wants to practice privately has to be
done through legislative action.
11. Can we look at the satisfaction level of people who went through the different types of
training before deciding on what’s best here?
12. Has there been any research on the success of different types of certification programs?
13. We can have a problem with the need for CEU’s when what’s available is not recovery-
oriented, more clinically focused. Potentially losing peerness.
14. How can we mold designations like MHRS, to be more peer-friendly? Definition of Other
Qualified Provider is what peers currently fit under. The only qualifications that it requires
are 18 years of age and a high school diploma.
15. How would malpractice insurance be handled with peer providers? If you are employed
under an agency, they hold the insurance.
Section II
1. Alameda is billing Medi-Cal with peers as well through Fred Finch.
2. Some groups in Alameda do not bill.
3. Contra Costa, Solano, San Francisco, Sacramento CBOs do bill Medi-Cal
4. There was a time when co-signatures were required for Other Qualified Providers. These do
not exist from [the state] at this time. Counties may require it.
5. “Supervision” does not mean the supervisor has to sign off on every note.
6. Rehab services are listed in the research paper, pg. 16. All services are listed.
7. If we set it up in Medi-Cal, private insurance may follow suit.

41
8. Can we take some political action to help this process? The CA Association of MH Directors
has invited WWT to come in to begin the discussion. This includes CM
Section III
1. Think about using the training from the department of developmental services training that
exists for direct service workers.
2. Where did WRAP go in the categories? It falls under specific practices.
3. Accessibility of training needs to be considered especially related to cross disabilities and
people below the poverty level.
4. Transgendered people need to be included in training and curriculum.
5. We need to foster the process of becoming a “peer” by experiencing the process through
groups and owning your own journey and be able to model it. Not so much a knowledge base
but an experience base.
6. Need to maintain the value of peer leadership and peer run training. It is about the process of
recovery perhaps that can be built into the CEU process or on-going support.
7. Important to be able to include dual diagnosis population for drug and alcohol.
8. Which counties require training before hire?
9. How do the three terms of individual, group and crisis terms of scope of practice relate to
current regulations and/or definition of peer support.
10. How many counties are using existing codes as this is dangerous because peers get bumped
out of jobs.
11. Sometimes creating new codes can result in creating lesser paid jobs for similar work.
12. Tests should be given with options for oral, written, literacy level etc.
13. Want to evaluate how to develop a testing system to accommodate inclusiveness.
14. Can certification be set up to guarantee employment with county services? It is an advocacy
effort. The certification needs to be something people can trust.
15. Working in primary care is going to happen even without healthcare reform. Training
programs are already being researched. Integration of primary care and mental health will
happen. Good to be prepared.
16. TAY perspective: Understand culture changes and gender gaps. Important also to have an
adult ally as a mentor.
17. It’s co-mentoring, because TAY experience is also important to value.
18. Diversity in California can be inclusive of the community experience. Part of our learning
experience should be shared. Young people don’t have to go through the hardships that we
did. Need to make supported employment available early. Be inclusive of the community
need when considering certification.
19. Possibility of waiving elements in the certification process, due to lived experience,
challenging the requirements, etc.
42
Regional Forum on State Certification for Consumer/Youth/Family Parent Peer Support
Services - Southern Region 4.13.12
Questions and Comments Southern Region
Section I
1. Clarification needed between provider type and service type. Provider certification is related
to the individual. Service type means that Peer services are defined and then the state
decides who can provide these services.
2. Family support is provided to the parent. The service recipient is the child. Billing collateral
services gets convoluted. If Peer Support is defined, then it could have a code for providing
these services (not having to relate the note to the child). Complications of what gets written
in the child’s file (parent issues, for example).
3. Certification standards: supervision is related to post-certification.
4. In county mental health systems, the MH Director is the ultimate supervisor of all staff.
5. Who does the supervision? They use “Qualified MH Provider” – defined differently,
includes Peers who are trained to be supervisors.
6. In California, does the state require supervision by a licensed staff person – no.
7. In other states, supervisors are licensed but required to go through the Peer Training.
8. The timing is very good for this process. Don Kingdon, thinks a window of opportunity will
be about one year.
9. Comment – it is very important to have a peer supervisor. Someone who knows the services
provided by peers.
10. There should be a statewide system. Many counties have done a lot a good work on this.
States don’t like to open up the state plan too much. Seems important to “strike while the
iron’s hot”. MH Directors have signed off on the general issue. Not sure what exactly they
would be willing to do.
11. If you create a new service called peer support services, you will need to go through a rate
setting process – likely to be paid less than other services.
12. You can do more than one option: peer provider, peer services and peer sites.
Section II
1. Which counties have higher qualifications for “Other Qualified Provider”? Some counties do
not use OQP. Used to be that notes have to be co-signed. Not required by the state, but
some counties still do this.
2. How is a warm line billed? Could be done, but the county is currently paying for the service
out of another pot of money.
3. Not all good services are billable. Medi-Cal is an insurance program. There are services that
can be billed and this provides revenue.
4. If the county is integrating physical care and mental health care, they should find a way to
bill it. Physical health care is very familiar with and supportive of peer services.
5. Social skills are already billable.
43
6. Concern about screening re: certification so people don’t get screened out. Barrier for
employment is civil service rules. Each county has different regulations. The state has to
deal with these issues, potentially through legislation.
7. Concern that the state would be the one to provide regulation of the above issue. San Diego
has worked it out successfully on their own. Whoever works on this issue needs to be skillful
and inclusive of forensic backgrounds. For example, might suggest that the employer may
not look back more than three years.
8. County Council may be involved in the decision to hire.
9. Inclusion of people with forensic backgrounds needs to be done. So important for peers on
these backgrounds.
Section III
1. Did all of the counties have experience as a requirement? No - some had no experience at all.
We will need to adjust the PowerPoint.
2. NAMI has a training program for people in the adult system.
3. Recovery Innovations (RI) has done a training for TAY.
Section IV
1. Riverside County has a monthly peer support meeting. Uses Keeping Recovery Alive, 52
topics. Allows people to connect and bring up questions/issues.
2. Recovery Innovations, CA (RICA) does a monthly meeting for all peer providers, run by
peer providers.
3. Certification can create professional stigma, about what your “level” of peer is.
4. Certification has allowed me to use a language that reinforces being a peer.
5. Language is very powerful in maintaining peerness.
6. Are we looking at educating the system – understanding peer support. This is an important
aspect of what’s needed.
7. People need to be educated about being in a still traditional mental health system.
8. Remembering who we are – and official statement that reinforces peerness.
9. Make sure that wherever I go, I can take any position and still maintain my peerness.
10. Family members want to see growth, and the higher you go, it is a good role model.
11. You can speak both languages – system and peer. Reality is that they have to speak the
system’s language for promotion within the system.
12. County supporting two people in masters’ programs through 20/20.
13. Never met a consumer/family member who weren’t supportive of the services provided by
peers. More issues with colleagues in the system. Educate the staff.
14. Hardest part of job as a family member supervisor is the attitude of other staff.
15. NAMI Provider to Provider course educates the providers.
16. Ensure that peer providers learn and value the other providers too.
17. Knowing each other’s roles, teamwork and conflict resolution.
18. Team-building within each organization is needed.

44
Regional Forum on State Certification for Consumer/Youth/Family Parent Peer Support
Services - Los Angeles Region 4.20.12
Question and Comments Los Angeles Region
Section I
1. This movement is seeking a statewide standard. Certification that is defined as including the
ability to bill. The issue is that in California, the MH Director will still have the authority to
determine what happens in his/her county. Important to get the MH Directors on board.
2. There is no state requirement that the state requires that notes by peers be signed off. MH
Directors may still require it as a risk management measure.
3. Peer providers are not more likely to bill inaccurately for services than other providers.
4. Have there been people who have opposed peer certification? Yes, some are concerned
about the requirements of billing and that this will degrade the provision of peer support
services.
5. Concerns about how to do billing for peer services in the child/youth system.
6. Community colleges are also an option for a certifying body.
7. Who should be a training body? Will be a focus group question.
8. Will all peer services have to be billed for? Could other services be added to the definition of
peer services? This could be defined in the state plan.
9. Many states have created stand-alone peer sites billing. In LA, currently only sites that have
ALL services can bill for peer services as well.
10. What about people working with clients who are not involved with the rest of the system?
What would care coordination mean?
Section II
1. Is there resistance to billing for peer support? What is it? Mostly seems to be a lack of
knowledge and risk management.
2. Some administrators have created mechanisms to support billing by peers.
3. Felt sense is that professionals devalue peer services. Devalue unlicensed people working in
the field.
4. Education of the workforce regarding the role of peers. Education regarding the value of
peers. Not in competition with professional workforce.
5. Concern about the word “recovery”. It is a long road. Concern about the lack of
opportunities. Certification needs to look at the career ladder possibilities.
6. Have clinicians or doctors been against certification? Not in these meetings, but most likely
it does exist in some places.
7. The question about billing implies stigma about the capability of people with lived
experience.
8. One example: Clinicians were positive about peers doing welcoming in the clinic.
9. Riverside County has a very strong peer support network. Struggling with licensed staff who
are worried that peers will take jobs. Supporting certification to legitimize the important
work that peers are doing.

45
10. A lot of peers are being trained to get licensed. This will be another way to change the
system.
11. Need for more research to provide additional validity of peer services. Yale is doing some
work. Michigan has done some great work.
12. Important to remember that lived experience is the basic reason we are here today.
13. What about getting away from use of the word peer, which creates barriers.
Section III
1. Disclosure of lived experience can be a barrier due to HIPPA requirements.
2. A problem can occur when hiring partners if they don’t really have lived experience.
3. How were people being hired? Part-time/full-time and living wage. This should be a
consideration when developing codes and jobs.
4. There are some places that are requiring volunteer work before hire. Is this a general
practice? (Riverside) There are people being hired and then are in training for a year before
being hired into real positions. This is not being done with any other codes in the County
(Riverside).
5. How is lived experience defined across the State? Does it require public system experience?
Or some other requirement.
6. For a lot of peers they have not worked for a long time but people are now being hired. Peer
training should include things like how to do interviews, self-care, how to deal with stressful
situations, how to work co-workers and supervisors etc.
7. National Council for Community Behavioral Health Care Consumers in the Mental Health
Work Force: A handbook for community providers.
8. Have to address stand-alone peer sites.
9. Medical groups are focused on education and insist that doctors in the group. Groups that
have the best outcomes do not have professionals in the group.
10. Important to look at how peer services are being delivered in CBO’s and peer operated
centers. Peers being used in non-peer ways. Some mechanism of oversight is necessary.
11. Peer hired in a contract agency that was told not to get her coffee at the staff coffee pot.
Additional questions/comments
1. Once the certified peer specialist curriculum topics/competencies have been finalized for CA,
will there be an open bid process for organizations to be selected as contractors to provide the
state certification training? If not, who will provide the state training and what will happen
to our many peer organizations throughout the state that currently provide peer trainings
within and required by their counties?
2. Will ALL peer services provided in CA have to be billed to Medi-Cal? For example, some
peer services may compromise the very essence of peer provision if the service is based on
Medi-Cal’s definition of medical necessity. I’d hate to have only Medi-Cal billable peer
services and /or endanger MHSA funds which allow for more flexibility to some of our peer
services (endanger because all peer services become Medi-Cal billable and MHSA funds
currently used for peer services are freed up for other non-peer services/programs.
3. How will we ensure cultural and linguistic diversity within some of the certification
requirements such as testing and training diversity?

46
4. What will happen if certified peer specialist’s certification becomes national vs. state-driven?
This has been in discussion for over three years and there is still movement at the national
level to adopt national certification standards – can the presenters comment on how what we
are doing on CA is aligned with or can contribute to this national certification movement?

47
Regional Forum on State Certification for Consumer/Youth/Family Parent Peer Support
Services - Superior Region 4.27.12
Questions and Comments Superior Region
Section I
1. Movement towards integrated care re: alcohol/drug services – some things cannot be billed in
alcohol/drug services. How will this be dealt with? Important to deal with the billing issues.
2. The integration of alcohol/drug services is uneven. Documentation and tracking continues to
be separate and distinct. Have a ways to go with complete integration.
3. Can this be in the discussion in this next go round on state plan amendment?
4. Alcohol/drug has much more stringent requirements on confidentiality which must also be
dealt with.
5. What would training/credentialing look like? What accommodations might be put in place?
6. Requirement for CEU’s – considered a best practice for certification.
7. Certifying bodies: what about community college certificates? Certificates are not an AA.
Need to work with community colleges to make sure that the certificates that articulate to
further education. Make sure the credits are transferrable.
8. Community college option is a lot more relevant for rural areas.
9. How long in remission/recovery does a person have to have in order to be a peer provider?
There was not a clear definition. People tended to show “being in recovery” as having a
WRAP and/or, disclosing and using your story, finishing a training program, as adequate
demonstration of recovery.
10. You can provide peer services if you have other credentialing – must be willing to share your
story.
Section II
1. Is being able to bill really “peerness?” Does billing for services change the relationship
because documentation is required? Definition is very important – mutuality that creates
change for both recipient and provider. Important to have different requirements that allow
this uniqueness to be reflected in documentation.
2. Hire for peer support and then have peers bill for standardized mental health services. Not
really validating pure peer support without a peer service type definition.
3. Is a better model to have people with lived experience join the mental health workforce or
contractors that do not fall under the umbrella of county services.
a. A false choice as peers need to be infused in the county system
b. More peer organizations are needed
4. Each peer provider’s experience is unique. Important not to have a power relationship by
billing.
Section III
1. Integration of primary care and mental health: while it looks on paper that primary care has
adopted peer support, it is only in the support group arena. It’s not direct services.
48
2. Solano is training receptionists, waiting room personnel, to be welcoming.
3. Another challenge with integration is that the medical providers are medical model driven vs.
rehab and recovery. A lot of resistance among medical practitioners to integrating with
mental health.

49
THIS PAGE IS INTENTIONALLY BLANK.