cfit online learning center - vanderbilt...
TRANSCRIPT

Introduction to this PDF Document
CFIT Online Learning Center
© Vanderbilt University, All rights reserved
CFIT
Dear Providence Staff Member:
In response to your requests, this PDF* version of the Common Factor module has been made available for you to print and share with staff within your region/office only. Before you continue, please take a moment to read this cover page.
You’ll still need to go through the online version of the module in E-learning in order for your completion status to appear and be updated, and to have access to the self-test and module evaluation. Your completion status can be viewed within the E-learning system.
Most importantly, please remember that only some regions across the country were randomly assigned to receive this additional training on common factors. During the evaluation of CFIT, only staff within those select regions will have access to these modules in E-learning. To preserve the integrity of the evaluation, under no circumstances should you share this PDF, either in paper or electronic form, with anyone outside your office. Similarly, you should not share access to the online modules in E-learning.
This is a large document and may take a while to print.
Providence, and our Vanderbilt consultants, greatly appreciate your support for this important quality enhancement initiative. If you have any questions or comments, please do not hesitate to contact us at [email protected]
* To view this document, you’ll need Adobe® Reader®. Adobe® Reader® allows you to view documents which have been created in the Portable Document Format (PDF). Adobe® Reader® is freely available. If you do not have a version of it already on your computer, you can download it at: http://www.adobe.com/products/acrobat/readstep2.html. If you do not know whether you have the appropriate software to operate CFIT, please contact the technical support of your office or any person in your office that may know.

4/12/06 SDK/SC/SD 1
CFIT Online Learning Center:Collaborative Treatment Planning
Version 1.1
Robert King, Ph.D., Susan E. Casey, M.S.W., & Susan Douglas Kelley, Ph.D.
Editors: Susan Douglas Kelley, Ph.D. and Susan E. Casey, M.S.W.
Acknowledgements
The development of this training module was made possible with the collaborative efforts of Vanderbilt University and Providence Service Corporation. We would also like to thank the following for their contributions:
Expert Reviewers: Scott D. Miller, Ph.D., Institute for the Study of Therapeutic Change, IL
Clinical Scenarios: Insoo Kim Berg, M.S.W., Brief Family Therapy Center, WI
Web Design: Sitening
Partially supported by NIMH Grant R01-MH068589, Leonard Bickman, Ph.D. (Principal Investigator)
Welcome
COLLABORATIVE TREATMENT PLANNING
© Vanderbilt University, All rights reserved
CFIT
Page 1
4/12/06 SDK/SC/SD 2
You are entering the first section.
It should take approximately 5 minutes to complete, with a total of 9 pages.
© Vanderbilt University, All rights reserved
Welcome
COLLABORATIVE TREATMENT PLANNINGCFIT
Page 2

4/12/06 SDK/SC/SD 3
• What should I expect?
• What is the point of collaborative treatment planning?
• What am I going to take away from this learning experience?
© Vanderbilt University, All rights reserved
Welcome
COLLABORATIVE TREATMENT PLANNINGCFIT
Page 3

4/12/06 SDK/SC/SD 4
What should I expect?
• There are five sections to this module and a total of 96 pages.
• This module takes approximately 2 hours to complete. Keep in mind that this is only an estimate. Time to complete will vary, based on your pace and utilization of hyperlinks. Thus, it may take anywhere between an hour and a half to 3 hours to complete this module.
• If you do not have 2 hours, don’t worry. We have designed it so you can complete one section at a time.
Now sit back and enjoy!
© Vanderbilt University, All rights reserved
Welcome
COLLABORATIVE TREATMENT PLANNINGCFIT
Page 4
4/12/06 SDK/SC/SD 5
WelcomeA brief introduction to the module and how it is relevant to your clinical practice
Clinical PracticeThis section includes two parts. The first is General Applications, which reviews identifying,
negotiating, and clarifying goals, negotiating treatment tasks, and measuring achievement, including how to apply these concepts in practice. The second is Specific Scenarios, which presents five clinical situations you may encounter with tips for activities and dialogue for collaborative treatment planning.
Bridging ConceptsThis section reviews the theoretical foundations and evidence base for collaborative treatment
planning. We also review the role of collaborative treatment planning in the therapeutic alliance and how it relates to PSC core values.
ResourcesSeveral additional sources for further information are provided for your continued learning.
Module EvaluationIn the final section, you will find a brief evaluation of the module. Your responses provide us with
valuable feedback for continued improvement.
Don’t forget to take the Self-Test (on the CFIT Training page in Qualifacts system) to finish this module.
Welcome
COLLABORATIVE TREATMENT PLANNING
This module includes five sections:
© Vanderbilt University, All rights reserved
CFIT
Page 5

4/12/06 SDK/SC/SD 6
What is the point of collaborative treatment planning?
• Provides a purposeful and systematic approach to working with clients and caregivers
• Promotes a strengths-based approach to collaboration between counselor, client, and caregiver
• Establishes how counseling will proceed, which contributes to building a positive therapeutic alliance
© Vanderbilt University, All rights reserved
Welcome
COLLABORATIVE TREATMENT PLANNINGCFIT
Page 6

4/12/06 SDK/SC/SD 7
• How to develop collaborative treatment plans in practice
• How collaborative treatment planning is related to other areas of clients’ treatment
• Tools and exercises to use for practice, reflection, and supervision
• Powerful questions and activities to help you deal with challenging situations
• Additional resources to further your understanding of client and caregiver expectancies
What am I going to take away from this learning experience?Key information, tools, and resources
© Vanderbilt University, All rights reserved
Welcome
COLLABORATIVE TREATMENT PLANNINGCFIT
Page 7

4/12/06 SDK/SC/SD 8
1. Use collaborative treatment planning processes to help clients identify, develop and clarify specific goals that are congruent with their aspirations.
2. Help clients identify a full range of resources, including caregivers and others in their support network, that can help them achieve goals.
3. Use collaborative planning processes, especially lifework assignments, to help clients implement activities that help them achieve goals.
4. Apply collaborative planning processes with caregivers and/or other key people in the client’s life.
5. Explain how collaborative planning activates the common factors that contribute positively to counseling outcome.
6. Be able to explain how collaborative treatment planning is related to the therapeutic alliance.
7. Be able to describe the foundations of evidence and theory underlying collaborative treatment planning and its relation to treatment outcomes.
8. Be able to access resources to learn more about skills in goal clarification and collaborative treatment planning.
Learning Objectives
© Vanderbilt University, All rights reserved
Welcome
COLLABORATIVE TREATMENT PLANNINGCFIT
Page 8

4/12/06 SDK/SC/SD 9
Congratulations! You have completed this section.
If you are pressed for time, return at a later date to continue the module.
First of five sections complete
© Vanderbilt University, All rights reserved
Welcome
COLLABORATIVE TREATMENT PLANNINGCFIT
Page 9

4/12/06 SDK/SC/SD 10
You are entering the second section (Part I of II).
It should take approximately 35 minutes complete, with a total of 38 pages.
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 10

4/12/06 SDK/SC/SD 11
• What is collaborative treatment planning?
• Multiple functions of collaborative treatment planning
• Five primary steps1. Identify and clarify goals2. Identify and develop strategies that are likely to result in each goal being achieved3. Negotiate and set ‘lifework’ assignments4. Set a time frame for implementation of each strategy5. Record and review the plan
• Working with caregivers around collaborative treatment planning
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 11
4/12/06 SDK/SC/SD 12
What is collaborative treatment planning?
Collaborative treatment planning is the process by which client and counselor work together to identify and clarify goals and strategies for achieving goals. They are collaborative because both goals and strategies are negotiated and shared together rather than imposed by the counselor. Plans are regularly reviewed and revised as goals develop, are achieved, or as strategies change.
The key to effective counseling is to be an active participant without taking over. It is a client centered process, in that client goals provide the starting point. However, the counselor is an active participant, assisting the client in operationalizing and sequencing goals, identifying strategies, setting targets and time frames for achievement, and identifying resources.
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 12
4/12/06 SDK/SC/SD 13
Functions of collaborative planning
Function 1: To identify and clarify goals and strategies
Function 2: To help both the counselor and client work purposefully and systematically
Function 3: To support the strengths-based approach
Function 4: To contribute to building a positive therapeutic alliance
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General Applications
CFIT
Page 13

4/12/06 SDK/SC/SD 14
Collaborative plans provide both a focus and framework for the counseling process and extend beyond the immediate counseling experience by including strategies that can be implemented outside of the counseling session.
Functions of collaborative treatment planning
1. To identify and clarify goals and strategies
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 14

4/12/06 SDK/SC/SD 15
A collaborative plan requires clearly specified targets and time frames that help the counselor and the client determine whether or not the agreed upon strategies are advancing counseling goals.
Functions of collaborative treatment planning2. To help both the counselor and client work purposefully and systematically
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 15

4/12/06 SDK/SC/SD 16
At the core of strengths-based counseling is the collaborative relationship between the counselor and the client.
Once the basic relationship is established through the assessment of client strengths, it will be possible to assist the client with identifying major goals for counseling.
Functions of collaborative treatment planning3. To support the strengths-based approach
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 16

4/12/06 SDK/SC/SD 17
The client will experience and report a strong alliance when he or she believes that goals and strategies are shared in common with the counselor.
Functions of collaborative treatment planning4. To contribute to building a positive therapeutic alliance
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 17
4/12/06 SDK/SC/SD 18
Step 1. Identify and clarify goals
Step 2. Identify and develop strategies that are likely to result in each goal being achieved
Step 3. Negotiate and set lifework assignments
Step 4. Set a time frame for implementing of each strategy
Step 5. Record and review the plan
There are five primary steps to collaborative treatmentplanning
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 18

4/12/06 SDK/SC/SD 19
Five primary steps
Step 1. Identify and clarify goals that are achievable within the counseling time frame
Collaborative planning starts with the identification of clear goals with the following characteristics:
• They are relevant to the long term goals of the client• When achieved, the goals will be useful in helping the client achieve long terms goals• They are concrete and set benchmarks for achievement• There is a medium to high probability of successful achievement within the counseling time frame• Both client and counselor endorse the goals• Family members and caregivers (preferably) endorse the goals
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 19

4/12/06 SDK/SC/SD 20
Clients often start out with goals that are quite vague or quite distant – e.g., ‘I just want to be happy’ or ‘I want people to like me.’
When this happens, the counselor should try to understand what the client means and help the client create a practical set of steps that achieve the larger goal.
It is very important to know what the larger goals are, and the counseling plan must be based on sub-goals that are specific and achievable in the short or medium term.
Five primary steps
Step 1. Identify and clarify goals
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 20
4/12/06 SDK/SC/SD 21
When goal aspirations are either vague, such as happiness, or distant, such as being liked, the counselor might respond by helping the client specify what it means to be happy or what it means to be liked. The counselor could then negotiate dimensions of being happy or being liked that might be achievable within the time frame of the counseling.
The order of questions is important. Concrete questions can stimulate the client to think more specifically and to be able to respond appropriately to more abstract, and therefore more difficult, questions.
Click here for sample dialogue relevant to when the aspiration is vague, such as happiness. Click here for sample dialogue relevant to when the aspiration is distant, such as being liked.
Five primary steps
Step 1. Identify and clarify goals
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 21

How would your life be different if you were happy?
How would people be treating you differently?
When the aspiration is vague such as happinessStep 1: Identify and clarify goals that are achievable within the counseling time frame
What kinds of things would you be doing that you are not doing now?
In what ways would you be feeling different from the way you are feeling now?
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General Applications
Page 22

How would you know if someone liked you?
How about if one person who doesn’t like you right now or maybe doesn’t even know you got to like you?
When the aspiration is distant such as being liked
Step 1: Identify and clarify goals that are achievable within the counseling time frame
What kinds of things would they say or do?
Is there someone in particular you want to like you more?
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General Applications
Page 23

4/12/06 SDK/SC/SD 22
Five primary steps
Step 1: Identify and Clarify Goals
At the beginning of counseling, it is important to identify goals that can be achieved quickly. This builds confidence in the counseling process. It is preferable to set a goal that is easily achieved rather than one that is likely to result in failure and discouragement.
Although it is difficult early in the counseling to know exactly how much capacity a client has, ideally a goal is slightly challenging.
Early goals should not stress the client. As the client builds a history of successful achievement he/she will become more tolerant of frustration and challenge so goals can be more demanding.
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 24

4/12/06 SDK/SC/SD 23
Five primary steps
Step 1: Identify and Clarify Goals
Sometimes clients identify a goal that is really a strategy to achieve a goal. The goal itself has not yet been specified and the client may not have really thought about it. The role of the counselor here is to help the client to work out what is behind the strategy.
The collaborative part of the planning process requires that both the client and counselor endorse the goals. This is partly achieved through the process of negotiating specificity, but there will also be occasions when client goals are unacceptable to the counselor.
In these circumstances, it is recommended that the counselor make use of techniques based on motivational interviewing to find goals that are acceptable to both parties. Resources on motivational interviewing are provided in the Resources section of this module.
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 25
4/12/06 SDK/SC/SD 24
Goal Clarification
Click on the Practice Tool for a suggested activity you can complete with your client and family to identify, clarify and negotiate goals. This is a more systematic and structured exercise that can be particularly helpful when the client has identified goals or values that are in conflict with other key people in the client’s life.
ToolboxTimes3
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Practice Tool
Page 26

1
CFIT Online Learning Center Collaborative Treatment Planning Practice Tool: Goal Clarification Exercise You can complete this exercise with your client and family to identify, clarify and negotiate goals.
Background Goals: Realizable intermediate steps that can be attained along the way toward achieving
major goals. Goal clarification can often be achieved by:
• Inquiring about the goals of your client • Differentiating longer and shorter term goals • Prioritizing goals • Identifying goals that are in conflict with the goals or values of other key people • A more systematic and structured manner using specifically designed exercises, such
as the one that follows Purpose This exercise provides the starting point for: 1. Identifying specific client goals 2. Identifying conflicting goals, which may be targeted with motivational interviewing
strategies It will often be important to achieve goal clarification with caregivers or other key people in the client’s life so that everyone with a stake in the counseling is clear about what each party is seeking to achieve.
• This can be done completing this as a family exercise, or by doing the exercise with only the caregivers
Indications Use this goal clarification exercise when:
• Client goals are unclear • Expectations for counseling are low • There is evidence of conflict between the goals of different stakeholders • CFIT measures indicate:
• Low client and caregiver expectations • Discrepancy between client and family expectations
Contraindications This exercise is not recommended when:
• There is a very clear focal problem • CFIT measures indicate that client expectations remain very low
• In this case, it is better to work on building alliance to develop rapport and more positive expectations before proceeding to this goal clarification exercise
Page 27

2
Preparation for Exercise The following steps should be taken before doing this exercise:
1. Review client and caregiver expectations based on the ETQ • Note total score (high, medium, low) of ETQ • Note whether there are differences in outcome expectations between the youth
and caregiver • Examine item-level information about role and process expectations for signs
of low expectations
2. Gather necessary materials: • 6 sets of ‘post-it’ pads – each a different color • Fine point marker • 6 sheets of poster paper
Overview of Exercise This following goal clarification exercise has five phases:
1. Orienting the client to the exercise 2. Identifying the stakeholders of counseling 3. Describing the goals of each stakeholder 4. Ranking stakeholder goals 5. Identifying shared goals, unshared goals, and mutually exclusive goals
Procedure 1. Explain the purpose of the exercise:
Example: “I want to get a clear picture of what different people are hoping to achieve from the counseling. I have looked at the survey you completed about your expectations for counseling and also the survey your caregiver completed so I have some general ideas – but now I want to get really clear so I can help you achieve the things you want. Is that OK?”
If client is happy to proceed, go to the next step.
If the client is uncertain or unwilling, check for concerns and discuss until she or he is ready to proceed.
2. Identify the stakeholders of counseling:
Example: “The first thing I would like you to do is to think about the people who want or hope for something good to come out of the counseling – who comes to mind?”
When the client names a person or category give him/her a colored post-it pad and have her/him write the person’s name or category on the top post-it – e.g., mom, teacher, parole officer, best friend, sibling etc.
If ‘me’ has not come up within the first people or categories, prompt – “What about you?” Be prepared to prompt for other categories until you are sure you have all the important stakeholders.
Page 28
3
Continue until all stakeholders have been identified, putting each person’s name on the top post-it of a pad.
3. Describe the goals of each stakeholder:
Example: “I would like to get your ideas about all the kinds of good things that you and the people you listed think might come from the counseling.”
Once the client identifies an outcome, ask the client to write it down on the next post-it in that stakeholder’s pad.
Identify any other stakeholders that would share the same wish and write the wish post-its in their pads.
Ask if the client also shares that wish. If so, have him/her add it to his/her post-it pad.
There should be only one wish per post-it for each stakeholder.
When the process is exhausted get the client to review the wishes they have recorded on the ‘me’ post-it pad and ask if any of her or his own wishes have been overlooked.
4. Rank the goals of each stakeholder:
Have the client write the name of each stakeholder on the top of a sheet of poster paper. Put each stakeholder on a separate sheet of paper.
Stick the post-its for each person in the order of importance that the client thinks this person would have for the various wishes, with the most important ones at the top and the least important at the bottom.
5. Identify shared goals, unshared goals, and mutually exclusive goals:
Ask the client to review her/his own wish list and to identify any wishes that are incompatible with another person’s wish.
You may end the exercise with something like: “Thank you for helping me get a better understanding of what different people are hoping to achieve from your counseling. This will help me in helping you achieve some of the things you want.”
Page 29

4/12/06 SDK/SC/SD 25
Once goals are established, the primary task of both client and counselor is to work out strategies that will be effective in achieving goals.
Strategies should have the following qualities:
•High self-efficacyThe client really believes he/she can do what is required.
•High ownershipThe client feels it is something he/she really wants to do and not just something the counselor thinks will work.
Five primary steps
Step 2. Developing strategies to achieve goals
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 30

4/12/06 SDK/SC/SD 26
Strategies should also have these qualities:
• Consistency with client strengthsUtilizes those client capacities and attributes that are well developed and have been successfully used in the past
•Consistency with current resourcesDoes not require cognitive, personality, social or material resources that the client lacks
•Feasible according to the counselorIt is important that the counselor also thinks the strategy has a high probability of success
•Acceptable to family or caregivers
Five primary steps
Step 2. Developing strategies to achieve goals
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 31

4/12/06 SDK/SC/SD 27
Brainstorming is a useful procedure for generating strategies. The counselor can ask the client to come up with all the ways of achieving the goal he/she can imagine. There are three phases of brainstorming:
1. No reality testing. ‘Tell me anything you can think of – we will work it out later if it is practical.’
2. Reality testing, where the ideas are sorted into three categories: ‘won’t work,’ ‘may work’ ‘should work’ (or something similar).
3. Prioritizing. The focus is on the ‘should work’ category.
The aim is to find the strategy or strategies that the client prefers which will yield results quickly and can be implemented without difficulty.
Five primary steps
Step 2. Developing strategies to achieve goals
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 32

4/12/06 SDK/SC/SD 28
Brainstorming Strategy
For more details about brainstorming, click on the Practice Tool for a suggested activity you can complete with your clients to generate strategies for identified goals.
This exercise helps stimulate the creative process, so both the counselor and client can have some fun while brainstorming all the ways clients can achieve their goals.
ToolboxTimes3
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Practice Tool
Page 33

CFIT Online Learning Center Collaborative Treatment Planning Practice Tool: Brainstorming Exercise You can do this activity you with your clients to generate strategies for identified goals. This exercise helps to stimulate the creative process so both the counselor and client can have some fun while brainstorming all the ways in which clients can achieve their goals. Brainstorming Strategy Brainstorming is a useful procedure for generating strategies. The counselor asks the client to come up with all the ways of achieving the goal s/he can imagine. A white board or something similar is helpful with brainstorming because it enables both client and counselor to keep track of the work that is taking place. PHASE 1: Free Thinking In the first phase of brainstorming there is no reality testing- ‘Tell me anything you can think of – we will work out later if it is practical’. After the client has exhausted ideas, the counselor can throw in a few as well. If the counselor has some very practical suggestions that might work, it is a good idea to include a few ‘wild’ ideas as well. The reason for this is that when it comes to reality testing, both client and counselor will get some suggestions thrown out quickly – this ensures that it is not a split between the counselor with good ideas and the client with dumb ideas. It also models for the inhibited client that it is OK to think laterally. When the counselor is done the client gets another opportunity to suggest some ideas. PHASE 2: Reality Testing The second phase is reality testing, the ideas are sorted into 3 categories: 1.) ‘won’t work’ 2.) ‘might work’ 3.) ‘should work’ or something similar. The client takes the lead on the sort with the counselor acting mainly as recorder. The sort can be done using 3 columns on a white board or using cards or pieces of paper if there is no white board. When the client dismisses an idea that the counselor thinks has merit, the counselor can ask: ‘what about this do you think won’t work/’ or ‘could it work if …?’
1
Page 34

If the client has something in the ‘should work’ category that the counselor thinks improbable, the counselor can say: ‘I don’t understand that one – tell me how it would work’. Ideas can be shifted from one column to the next until both counselor and client are happy with the assignment. PHASE 3: Prioritizing The third phase is prioritizing. The focus is on the ‘should work’ category. The aim is to find the strategy or strategies that the client prefers which will yield results quickly and can be implemented without difficulty.
• Strategies can be cognitive such as practicing positive self statements, actions such as practicing ball handling drills or interactions such as saying ‘Hi’ to a new student in class
• A time frame for implementing each strategy should be discussed
• These strategies provide the basis for the ‘lifework’ that the client will
undertake
2
Page 35
4/12/06 SDK/SC/SD 29
‘Lifework’ is a term that can be used to describe the tasks that the client agrees to undertake before to the next counseling session. Lifework signifies a different meaning from homework—that this is work related to the client or caregiver’s everyday life. Ask the client to choose their own special word for lifework to foster collaboration.
Lifework assignments involve implementing the agreed upon strategies in the client’s own environment.
Five primary steps
Step 3. Negotiating and setting lifework assignments
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 36

4/12/06 SDK/SC/SD 30
The role of the counselor is to:
• Negotiate lifework assignments
• Help the client formulate the lifework assignment
• Provide opportunities to prepare for lifework assignment through rehearsal in the session or work out solutions to obstacles likely to prevent completion of the assignment
• Motivate the client to undertake and complete assignments
• Ensure the client is clear about the expectations of the counselor
Five primary steps
Step 3. Lifework assignments
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 37
4/12/06 SDK/SC/SD 31
Lifework assignments should be sufficiently simple that they can be successfully completed by the next counseling session.
When assignments involve cognitive or interactional processes, the counselor can encourage the client to rehearse during the counseling session.
Motivating the client is partially achieved when the client understands the link between the assignment and achievement of personal goals.
It is useful for the counselor to explain the relationship between practice and the development of new skills, and also to explain to the client that research indicates there is a positive relationship between completing lifework assignments and achieving counseling goals.
Five primary steps
Step 3. Lifework assignments
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 38

4/12/06 SDK/SC/SD 32
It is important the client knows and understands exactly what the counselor would like the client to do before the next session. This is best achieved by writing down the lifework assignment.
When e-mail is available, sending the client an e-mail message containing the lifework assignment serves both as a written record of the agreed upon assignment and a prompt.
If the client does not follow through with agreed upon assignment, the counselor can renegotiate for the client to complete the lifework assignment for the following session.
Five primary steps
Step 3. Lifework assignments
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 39

4/12/06 SDK/SC/SD 33
Values Compass
Click on the Practice Tool for a suggested activity you can complete with your clients to help them identify important values in their lives that they would like to focus on and strengthen. Once the client has identified important values, you can work together to create lifework assignments that the client can do between sessions.
ToolboxTimes3
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Practice Tool
Page 40

Adapted from: Hayes, S.C., Strosahl, K.D. & Wilson, K.G. (2003). Acceptance and commitment therapy: An experiential approach to behavior change. NY: Guilford.
1
CFIT Online Learning Center Collaborative Treatment Planning Practice Tool: Values Compass Exercise You can complete this activity with your clients to help them identify important values in their life that they would like to focus on and strengthen. Once the client has identified important values, you can work together to create lifework assignments that the client can do between sessions. Directions: Use this diagram as a guide. Have the youth draw a circle in the center of the page and have him write “The Me I Want to Be” or a version of this using his own words. Next, ask the youth to identify the most important areas/values in his life. Offer a few examples like those listed in the diagram to get the creative process started. Draw lines from the center of the circle and create smaller circles for each “value” he/she identifies. Once the youth has an exhaustive list, work with the youth to prioritize them in order of importance. After the youth has prioritized the list, ask the youth to write in the middle of the circle what he values about _______. So, for example, if the youth identified Friendship as one of his top priorities, ask him what he values about friendship and have him write it in the middle of the circle. What characteristics are important to him in a friend? What kind of friend is he? Is he the kind of friend to others that he wants a friend to be to him? The idea is to help the youth identify values that are important to him and things that he can do to strengthen the areas that matter most to him. Use the Values Assessment Worksheet to record identified goals for the values, action steps toward achieving goals, and potential barriers.
Page 41

Values Compass
Values: These are the “big picture” or “longer-term” things you want to do- values are like our life’s journey
Some areas that values may be about are:
Dating Education Family Friendships Health Recreation/Fun Work So, the question is…where do you want to go?
Adapted from: Hayes, S.C., Strosahl, K.D. & Wilson, K.G. (2003). Acceptance and commitment therapy: An experiential approach to behavior change. NY: Guilford.
2
Page 42

4/12/06 SDK/SC/SD 34
Values Assessment Worksheet
Click on the Practice Tool for a suggested activity you can complete with your clients, or have them work on independently. This blank worksheet can be used to record the values the youth identified in the previous practice tool (Values Compass Exercise). It provides clients with a structure to list goals, action steps, and potential barriers to achieving goals.
ToolboxTimes3
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Practice Tool
Page 43

CFIT Online Learning Center Collaborative Treatment Planning Practice Tool: Values Assessment Worksheet
Adapted from: Hayes, S.C., Strosahl, K.D. & Wilson, K.G. (2003). Acceptance and commitment therapy: An experiential approach to behavior change. NY: Guilford.
1
The blank worksheet on the following page can be used to record the values the youth identified in the Values Compass Exercise. It provides clients with a structure to list goals, action steps, and potential barriers to achieving goals.
Page 44

Adapted from: Hayes, S.C., Strosahl, K.D. & Wilson, K.G. (2003). Acceptance and commitment therapy: An experiential approach to behavior change. NY: Guilford.
2
Values, Goals, Actions, and Barriers
Values: These are the “big picture” or “long-term” things you want to do- values are like our life’s journey Goals: These are the specific, short term things you want to do- goals are like specific stops along the way Actions: These are the very specific steps you take toward your goals and values- actions are like the steps in
your journey Value Statement: _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ _____________________________________________________________________________________________________
Goals
Actions
Barriers
Page 45

4/12/06 SDK/SC/SD 35
Targets are the means by which both client and counselor can determine whether the agreed strategies are effective in helping the client achieve goals.
Targets must be clearly linked to goals and sufficiently clear and concrete for them to provide a meaningful benchmark.
Vague targets make it much more difficult to determine whether or not the plan is working.
Five primary steps
Step 4. Setting counseling targets
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 46

4/12/06 SDK/SC/SD 36
Targets usually have both a quantitative dimension and time dimension. For example, a client who has a long term goal of making new friends and a short term goal of getting to know Jarred might be stated like this: The client will talk to Jarred during the lunch break, a target might be spending at least ten minutes talking to Jarred during one lunch break over the next two weeks.
A target like this is modest and can easily be achieved, even exceeded. Even minimal achievement is a step on the way to achieving larger goals.
Five primary steps
Step 4. Setting counseling targets
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 47

4/12/06 SDK/SC/SD 37
If the target is not achieved, it is a clear indication that either the strategies are not working, or the goal is no longer a priority.
The time frame for achieving the target should be sufficiently short to enable adjustment of strategies if it is not working, but sufficiently long to enable a succession of strategies to be implemented.
Five primary steps
Step 4. Setting counseling targets
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 48
4/12/06 SDK/SC/SD 38
The plan is a living document that provides both the client and counselor with a map of the agreed upon goals, strategies, lifework assignments and targets.
It provides a reference point that allows the client and counselor to review the progress and impact of counseling.
It also documents evolving goals and changes in counseling focus.
The counselor takes responsibility for reviewing the plan and helps the client reformulate goals and strategies if the plan is not working.
Five primary steps
Step 5. Recording the plan
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 49

4/12/06 SDK/SC/SD 39
An example of a plan structure is as follows:
Five primary steps
Step 5. Recording the plan
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 50

4/12/06 SDK/SC/SD 40
Whose language do you use when you write treatment plans and documentation notes?
Click on the Reflection Tool for reflective questions intended to help you think about how you use language in the work you do with your clients and families.
ToolboxTimes3
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Reflection Tool
Page 51

CFIT Online Learning Center Collaborative Treatment Planning Reflection: Whose language do you use when you write treatment plans and documentation notes? DIRECTIONS: The reflections and reflective exercises are intended to give you some thoughts/questions to think about when you have some quiet time. Take a moment to think about the questions and write out the answers. Reflection:
A shift in [the client’s] experience takes place when [they] find the right word to describe it. When [they] are called by [their] correct name, or [their] experience is correctly named, [they] relax and breathe easier from being understood (Johanson & Kurtz, 1991, p. 2).
Reflective Exercise: When you are working with your clients, do you use their words when writing out their goals, objectives and strategies…or do you use your language? Pull out a treatment plan and try reading it from the client’s perspective. Whose words are they? What was your experience when you read it from the client’s perspective? Do your client and family understand everything that is on the client’s treatment plan? Do they understand you when you are talking with them during their session? If they read your documentation notes, would they understand and agree with what you have written? Would they feel understood? Would they feel respected and heard? How do you know? What do they say or do that tells you they feel respected and heard?
Johanson, G. & Kurtz, R. (1991). Grace unfolding: Psychotherapy in the spirit of the Tao-te ching. New York: Bell Tower.
Page 52

4/12/06 SDK/SC/SD 41
Working with caregivers around collaborative treatment planning
Because caregivers are integral to any treatment their children receive, including them in planning is particularly important.
There are three ways by which family members, school counselors or other people actively engaged with the client can be involved in the collaborative planning process:
1. Ensuring that system resources and characteristics are taken into account in developing the plan—especially when developing strategies for achieving goals.
2. Sharing the plan with members of the wider system.
3. Including caregivers in the actual planning process.
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 53
4/12/06 SDK/SC/SD 42
The inclusion of system resources and characteristics is best achieved by prompting the client when it comes to identifying strategies to achieve goals. For example, the counselor could ask, ‘Can you think of anyone in your family who could help you achieve this?’ or ‘Is there some way the school could help?’
Sometimes it is also important to identify and plan for potential obstacles in the wider system by asking questions such as, ‘What do you think your mom or dad would think about that?’
Working with caregivers around collaborative treatment planning1. Including system resources in the plan
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 54

4/12/06 SDK/SC/SD 43
Sharing the plan can often be helpful both to the client and to people in his or her wider system.
The plan helps caregivers understand what the client is trying to achieve and provides them with the opportunity to provide support or at least not unintentionally obstruct his or her goals. It also fosters a more general alliance between caregivers and the counseling process.
The plan helps caregivers understand what is happening and why, and may help them overcome fears or apprehensions. It helps them have realistic expectations about the impact of counseling.
Not only should caregivers be involved in planning, but they should have tasks to work toward on the plan.
Working with caregivers around collaborative treatment planning2. Sharing the plan
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 55

4/12/06 SDK/SC/SD 44
While there are many good reasons to share plans, it is essential that the client is comfortable with this and is not simply complying with a request in a passive way or to appease the counselor and caregivers.
It is useful to discuss sharing prior to writing it because the client may want to express parts of the plan differently if he/she knows that others will be reading it.
Working with caregivers around collaborative treatment planning2. Sharing the plan
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 56

4/12/06 SDK/SC/SD 45
Caregivers can be active participants. When counseling includes a parent or other family member, this person (or persons) will be part of the planning process. In these circumstances, the counselor and the client need to be clear about whose plan it is. If it is the client’s plan it must be based on the client’s goals. Caregivers can assist with identifying strategies but the counselor must ensure that they do not take over the process.
If it is a family plan, goals will relate to the wider system rather than any one individual and strategies will be negotiated within the system.
Sometimes counseling will include counseling for one or more caregivers as well as for the client. In these circumstances, there will be more than one plan, as each person will have specific objectives. The same basic procedures for collaborative planning that have been recommended for use with young clients can also be applied in counseling with adults.
Working with caregivers around collaborative treatment planning3. Including caregivers in the process
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 57

4/12/06 SDK/SC/SD 46
What are you doing to create a level playing field with your client?
Click on the Supervision Tool for questions to bring into supervision. The questions are intended to help you think about how to create a collaborative process with your client while understanding that a power differential does exist between you.
ToolboxTimes3
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Supervision Tool
Page 58

CFIT Online Learning Center Collaborative Treatment Planning Supervision: What are you doing to create a level playing field with your client? DIRECTIONS: The supervision exercises and questions are intended to give you some guided questions to think about and bring to your supervision session and talk over with your clinical supervisor. Questions for Supervision: In understanding that while we are trying to create a respectful collaborative process, there remains a power differential between you and your client, because counselors are being paid to provide a service. Therefore, the questions to bring to supervision are: What is it that I need to do in my sessions to level the playing field? And what have I done up to this point to facilitate that? What has worked? What has not worked? What can I try that I have not tried yet?
Page 59
4/12/06 SDK/SC/SD 47
Congratulations! You have completed the first part of this section.
If you are pressed for time, return at a later date to continue the module.
Second of five sections partially complete
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part I: General ApplicationsCFIT
Page 60

4/12/06 SDK/SC/SD 48
You are entering the second section (Part II of II).
It should take approximately 35 minutes to complete, with a total of 25 pages.
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 61

4/12/06 SDK/SC/SD 49
In part I, we discussed the general concepts of collaborative treatment plans and how to operationalize those concepts in practice.
Here in part II, we will be looking at five specific scenarios.
Scenarios 1-3 will demonstrate how to negotiate and clarify goals.
Scenarios 4-5 will demonstrate how to negotiate treatment tasks and measure achievements.
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 62

4/12/06 SDK/SC/SD 50
What are you getting from and contributing to your supervision?
Click on the Supervision Tool for questions to bring into supervision. These questions will help you think about how to create a collaborative process with your supervisor, while being mindful of the power differential inherent to supervision.
ToolboxTimes3
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Supervision Tool
Page 63

CFIT Online Learning Center Collaborative Treatment Planning Supervision: What are you getting and contributing to your supervision? DIRECTIONS: The supervision exercises and questions are intended to give you some guided questions to think about and bring to your supervision session and talk over with your clinical supervisor. Questions for Supervision: In understanding that while your supervisor is trying to create a respectful collaborative process, there remains a power differential between you and your supervisor due to your supervisor’s position and authority in the agency. Supervision is only effective if the supervisee feels safe, respected, and heard. Therefore, the question to bring to supervision is: What do I need from my supervision to feel safe? Am I getting this? What do I need from my supervisor to feel respected? Am I getting this? How will I know if I have been heard? Is this happening? What can I do to contribute to create a respectful environment? Am I doing this? Do I “hear” my supervisor? Can I share this exercise with my supervisor? If the answer is no…and you do not have safety in your supervision…is there another person in a supervisory role to whom you can go to and share your struggle?
Page 64

4/12/06 SDK/SC/SD 51
Before we get started, there are three important points to remember about goal negotiation and clarification:
1. Goals must target early steps towards a solution, not the absence of problems.
2. Goals must involve observable social interactions; that is, there are social components to goals- goals do not just describe desired thoughts like “I will be happier some day.”
3. Caregivers and/or youth may not know what we are asking them when we use words like “goals,” since setting goals and taking steps toward achieving them may be unfamiliar life experiences.
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 65
4/12/06 SDK/SC/SD 52
The first three scenarios demonstrate working collaboratively with clients and caregivers to negotiate, clarify and shape goals. The three scenarios are:
Scenario 1: Caregiver states goals in broad terms
Scenario 2: Client refuses to identify goals to work on
Scenario 3: Counselor has a difficult time asking follow–up questions when client and caregiver stonewall the process
Negotiate, clarify, and shape goals
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 66
4/12/06 SDK/SC/SD 53
Scenario 1: Caregiver talks about goals in broad termsFor example, “I want my child to listen to me when I tell him to do something!”
While a general goal is a starting point for developing goals, a concrete, behavioral indicator of change is needed. Such behavioral indicators show the parent that their child is changing. Small, focused goals should be utilized, since goals mark progress towards change, rather than the end of change. Using small, simpler, achievable goals makes it easier to see success immediately. This instills hope that change is possible. In addition, change may become more desirable by both the youth and caregiver when success is attained.
Click here for a sample dialogue about how to simplify the goal.
Negotiate, clarify, and shape goals
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 67
Counselor: So suppose he goes to school, what difference would it make your relationship with him?
Parent: Well, then I don’t have to yell at him all the time. He hates it when I harp on him like that about school.
Counselor: So, this is a lot of work for you also, harping on him as you say.
Parent: I don’t like to yell at him all the time either and I know he doesn’t like it either.
Counselor: I’m sure that’s true. So, suppose he goes to school and stays there, I’m not sure how he is going to do that, but just suppose he does. . . what would the two of you do then that you are not doing right now?
Parent: Oh, we’ll get along, talk more, have dinner together once in a while, instead of getting mad at each other all the time.
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific Scenarios
Scenario 1: Caregiver talks about goals in broad terms
“I want my child to stop acting like a brat!”
Working collaboratively to negotiate, clarify, and shape goals
Page 68

4/12/06 SDK/SC/SD 54
Scenario 2: Client is not able to or refuses to identify any goals that he/she is interested in working on.
One major reason this may happen is that clients are often mandated to seek counseling. These clients often feel forced to do something they do not perceive as important or beneficial. Clients may even believe that counseling could be harmful.
Most likely, such clients will show their objections to counseling in many different ways.
For these clients, expecting major changes is unreasonable and not likely to be successful or rewarding. Therefore, it is best to have very modest goals when beginning work.
Engagement with the client is the key in this scenario. Rather than pushing the client to engage in the relationship or in goal negotiation at your pace, proceed slowly, allowing the client to come to his/her own terms with counseling.
Negotiate, clarify, and shape goals
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 69

4/12/06 SDK/SC/SD 55
What to do? • Give the youth lots of praise about being there physically, even though he/she does
not want to be there.
• Acknowledge the youth’s decision to be there when he/she could have run away, not shown up, or forgotten about his/her counseling session.
• Appreciate when the youth has a moderate to high level of cooperation and see it as a sign that he/she wants to do what is good for himself/herself.
• Ask the youth about his/her talents, interests, hobbies, and special skills. Show interest rather than judgment.
• Ask the youth about his/her social life, what kinds of things he/she does with friends. Again show curiosity, rather than a mission to enact changes.
Scenario 2: Client is not interested in working on goalsNegotiate, clarify, and shape goals
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 70

4/12/06 SDK/SC/SD 56
How do you help your clients discover their own inner wisdom?
Click on the Reflection Tool for reflective questions intended to help you think about what you have done with your clients to help them discover their inner wisdom.
ToolboxTimes3
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Reflection Tool
Page 71

CFIT Online Learning Center Collaborative Treatment Planning Reflection: How do you help your clients discover their own inner wisdom? DIRECTIONS: The reflections and reflective exercises are intended to give you some thoughts/questions to think about when you have some quiet time. Take a moment to think about the questions and write out the answers Reflection:
The work of therapists is not analogous to that of engineers or artists. Therapists do not create something they can stand back from, look at, and claim as their own. Mindful, nonviolent therapy simply helps [clients] discover and affirm the wisdom of [their] inner experience (Johanson & Kurtz, 1991, p. 38).
Exercise: What specifically did you do in previous sessions with clients (think of at least 3 clients you are currently working with) that: Helped them discover the wisdom of their inner experience? Helped them to discover new insights about their experiences? Make a list of questions you asked that initiated reflection and insight. Make a list of exercises, or activities you did that seemed to generate movement in the client. Do you have a client or clients that “feel” stuck? Try some of these things from your list and notice what happens…
Johanson, G. & Kurtz, R. (1991). Grace unfolding: Psychotherapy in the spirit of the Tao-te ching. New York: Bell Tower.
Page 72

4/12/06 SDK/SC/SD 57
Scenario 3: Counselor has a difficult time asking follow–upquestions when client and caregiver stonewall the process.
What is “resistance”? Steve de Shazer (1984) proposed that what therapists call client resistance is actually the client’s way of cooperating by showing us how to work with them.
We can learn from this idea and look at the client’s and family’s reluctance to engage with us and refusal to respond to our questions—behaviors that others might call “resistance”—in a different light.
Negotiate, clarify, and shape goals
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 73

4/12/06 SDK/SC/SD 58
Imagine what would happen if a counselor viewed the client’s refusal to answer questions in this light. Rather than “resistance” in the traditional sense, the counselor could view this refusal to talk as the client’s way of ensuring that it is safe to respond, protecting his/her family from “prying” eyes, making sure his/her parents do not look bad to those outside of the family, or keeping his/her family’s troubles concealed.
Based on this perspective, it may be much more useful to support a youth’s decisions about sharing with you.
Scenario 3: Counselor has a difficult time following-up
Negotiate, clarify, and shape goals
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 74

4/12/06 SDK/SC/SD 59
Many clients may feel that life just happens to them; they do not necessarily feel they control or shape their own lives. Therefore, many clients and caregivers need help understanding what it means to negotiate. The counselor’s task is to translate this idea into understandable language that conveys that the caregivers’ and client’s input matters and is necessary.
In addition, youth may have been told many times by many adults what is wrong with them. This type of feedback is both negative and unsolicited. Imagine you were in their place: how would you feel sitting with yet another adult you think is about to pick you apart and tell you what’s wrong with you?
Scenario 3: Counselor has a difficult time following-up
Negotiate, clarify, and shape goals
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 75

4/12/06 SDK/SC/SD 60
Transition into discussing the youth’s interests and strengths. Perhaps he plays an instrument. She may be an amazing basketball player. The youth may demonstrate passion and dedication about these areas.
Ask about clients’ passion(s) and acknowledge them as experts in these areas. As the counselor, be open to being educated about their areas of expertise. Respect and work with those areas of expertise, rather than trying to change them.
Scenario 3: Counselor has a difficult time following-up
Negotiate, clarify, and shape goals
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 76

4/12/06 SDK/SC/SD 61
Even without discussing it, clients likely have some understanding about why they are in counseling.
We cannot change other people. We can only change our own responses to them. This can help reshape interaction patterns to become more positive and cooperative. While counselors may be the experts at the process of finding solutions, caregivers, clients and their families will take care of the details of how to get from “here” to “there.” Remember that “there” is defined by the clients and caregivers.
By embracing this approach, you can avoid attempts to force clients and families to think exactly like you do.
Scenario 3: Counselor has a difficult time following-up
Negotiate, clarify, and shape goals
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 77
4/12/06 SDK/SC/SD 62
Scenarios 4-5 will demonstrate how to negotiate treatment tasks and measure achievement. Scenarios 4-5 include:
Scenario 4: Caregiver responds to suggestions for possible treatment tasks with “I’ve already tried that and it didn’t work.” But she is not able to come up with other suggestions.
Scenario 5: Client helps create goals and agrees to weekly tasks, but then never follows through with agreed upon tasks.
Negotiating treatment tasks and measuring achievement
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 78

4/12/06 SDK/SC/SD 63
Scenario 4: Caregiver responds to suggestions for possible treatment tasks with “I’ve already tried that and it didn’t work.” But, she is not able to come up with other suggestions.
When a caregiver responds in this way, it usually indicates that the counselor either missed cues from the caregiver or offered suggestions before the caregiver was ready to hear them.
Everything we do in counseling has to do with timing. Even the best suggestion offered at the wrong time will not be heard and carried out. Recognizing this helps us be sensitive to the timing and method of offering suggestions.
Negotiating treatment tasks and measuring achievement
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 79

4/12/06 SDK/SC/SD 64
Scenario 4: “I’ve already tried that and it didn’t work.”
It is also possible that the caregiver really thinks that, “I’ve tried everything under the sun” and “you are not telling me anything I don’t know.” Therefore, it is always better only offer suggestions when asked.
Offering suggestions is an art. As counselors, we do not want to be dismissed by the caregiver or the youth. Some good ways of offering suggestions while minimizing being dismissed are discussed on the next few pages.
Negotiating treatment tasks and measuring achievement
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 80

4/12/06 SDK/SC/SD 65
Scenario 4: “I’ve already tried that and it didn’t work.”
Good ways to be heard, rather than dismissed:
• Do not offer suggestions easily or provide quick solutions. When you do this, caregivers may feel like you are not taking their problems seriously, or don’t really appreciate the seriousness of their problem (i.e., they may believe you are being dismissive of them).
• Make a thorough list of what the caregiver tried and how effective each strategy was.• After each strategy is described, the counselor should ask, “How well did
that work?” After getting a response, the counselor can follow-up with, “What else have you tried?” (repeat this up to four or five times).
• Remember that the items on the list were ineffective, so unless you suspect poor implementation of strategies, do not suggest trying these strategies again.
Negotiating treatment tasks and measuring achievement
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 81

4/12/06 SDK/SC/SD 66
Good ways to be heard, rather than dismissed:
• When a counselor feels pressured to offer suggestions simply because the situation seems so dire, it is likely that any suggestions offered will be unsuccessful.
• Be aware of strategies the caregiver is using that are effective or have potential to be effective- encourage him/her to do more of the things that do work.
• Remember to praise and express enthusiasm about the caregiver’s efforts to help the youth.
Scenario 4: “I’ve already tried that and it didn’t work.”
Negotiating treatment tasks and measuring achievement
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 82

4/12/06 SDK/SC/SD 67
Good ways to be heard, rather than dismissed:
• Be aware that some situations call for the caregiver to do something entirely different from what he/she has been doing, rather than doing more of the same.• Suggest that he/she thinks about “doing something entirely different.”
• Remember that the solution must fit with the client’s frame of reference and the family’s way of doing things. Offering the suggestion to “do something different” opens up options for the family, rather than narrowing them. • If caregivers respond to this by asking, “So, what do you think we should do?”
a counselor may respond honestly, by saying, “I don’t know yet. But it seems like it may be the last thing your son would expect you to do.”
Scenario 4: “I’ve already tried that and it didn’t work.”
Negotiating treatment tasks and measuring achievement
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 83

4/12/06 SDK/SC/SD 68
How do you encourage growth?
Click on the Reflection Tool for reflective questions intended to help you think about what happens, what can happen, and what you are doing to encourage your client’s discovery, healing and growth.
ToolboxTimes3
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Reflection Tool
Page 84

CFIT Online Learning Center Collaborative Treatment Planning Reflection: How do you encourage growth? DIRECTIONS: The reflections and reflective exercises are intended to give you some thoughts/questions to think about when you have some quiet time. Take a moment to think about the questions and write out the answers Reflection:
The compassion of the therapist, sometimes expressed through laughter, can affirm the presence of [the client’s] buried resourcefulness, whereas a response of pity would be an affirmation that [the client] does not have what it takes, that [the client] need[s] a white knight to save [her] (Johanson & Kurtz, 1991, p. 26).
Exercise: Counselors are present in different ways at different times for different people. However, they are constantly making careful judgments about what is happening or can happen to encourage [the client’s] growth in human-beingness. This is the counselor’s main criterion for acting: In your next session, ask yourself these questions: Will what you do or not do in the moment be helpful in [the client’s] study and discovery of themselves? Will it support the client’s healing and growth? How will it support the client’s healing and growth?
Johanson, G. & Kurtz, R. (1991). Grace unfolding: Psychotherapy in the spirit of the Tao-te ching. New York: Bell Tower.
Page 85

4/12/06 SDK/SC/SD 69
Scenario 5: Client helps create goals and agrees to weekly tasks, but then never follows through with agreed upon tasks.
Remember a few slides back when we referenced the 1984 article published by Steve de Shazer entitled “The Death of Resistance”? de Shazer called resistance the client’s way of cooperating with us by showing us how to work with them.
When a client “agrees” to goals and tasks and continuously does not do them, he/she is trying to show you something. The question is what! The next few pages have some things to consider.
Negotiating treatment tasks and measuring achievement
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 86

4/12/06 SDK/SC/SD 70
• Make sure the process of negotiating goals and tasks is truly collaborative. When a client appears to be very agreeable to all goals and tasks and seems to be going through the motions, it may be a sign that he/she is not engaged in collaboration.
• When the client repeatedly does not do tasks, the counselor may become upset with the client, causing an impasse that leaves both sides feeling frustrated.
• Rather than getting stuck in such an impasse, the counselor can open the discussion with the assumption that the client has “good reasons” for not having done the task.• “Bobby, it sounds like you must have had good reason for not having filled out the
job applications last week. I’d like to hear about these reasons.”• By saying this, the counselor implies that the client is a reasonable person, and
since reasonable people do things with ‘good reasons,” you’re interested in understanding where he/she is coming from.
Scenario 5: Client never follows through.
Negotiating treatment tasks and measuring achievement
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 87

4/12/06 SDK/SC/SD 71
Do you allow for spontaneity in your sessions?
Click on the Reflection Tool for reflective questions intended to help you think about times when your agenda for the therapeutic session is incongruent with your clients’ own needs and plans.
ToolboxTimes3
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Reflection Tool
Page 88

CFIT LEARNING COLLABORATIVE TREATMENT PLANNING REFLECTION TOOL: Do you allow for spontaneity in your sessions? DIRECTIONS: The reflections and reflective exercises are intended to give you some thoughts/questions to think about when you have some quiet time. Take a moment to think about the questions and write out the answers Reflection: Another prerequisite for good therapists is being comfortable with not being in control. The whole process depends on using the spontaneous as a beginning and continuing point of departure. To do this requires the ability to give up not only personal agendas but also therapeutic agendas. (pg. 83) Exercise: In your next session with your client, make a conscious effort to observe yourself throughout the session… Are there times when you feel frustrated with how the session is going? Do you feel that your client is being resistant? Do you feel tired? Annoyed? Disinterested? Distracted? What triggered these feelings? What did you say? How did your client respond? Write it down. When these feeling arise, you are most likely working on an agenda that is incongruent with your clients. When this happens, we tend to be “in our heads” and unable to “hear” our client and therefore no longer able to allow for the spontaneous words and actions to flow in the moment. What do you need to allow for spontaneity?
Page 89

4/12/06 SDK/SC/SD 72
Congratulations! You have completed this section.
If you are pressed for time, return at a later date to continue the module.
Second of five sections complete
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Clinical Practice Part II: Specific ScenariosCFIT
Page 90

4/12/06 SDK/SC/SD 73
You are entering the third section.
It should take approximately 20 minutes to complete, with a total of 10 pages.
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Bridging ConceptsCFIT
Page 91

4/12/06 SDK/SC/SD 74
•What is the evidence for using collaborative treatment planning in counseling?
•How does collaborative treatment planning relate to therapeutic alliance?
•How does collaborative treatment planning correspond to PSC’s core values?
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Bridging ConceptsCFIT
Page 92

4/12/06 SDK/SC/SD 75
What is the evidence?
In your role as a counselor, it’s important to know that the interventions you use are based on evidence of what works.
Theoretical Foundation
There are several theories that inform our understanding of collaborative treatment planning, including learning theory (specifically self-efficacy), empowerment theory, and cueing theory. In addition, goal clarification is informed by systems theory.
Click here on theoretical frameworks to access a comprehensive review.
Coll. Planning
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Bridging ConceptsCFIT
Page 93

THEORETICAL FOUNDATIONS OF COLLABORATIVE PLANNING Three theoretical frameworks inform this approach: Empowerment theory proposes that a person’s ownership of a planned strategy for solving a problem is as important as the objective quality of the strategy. A strategy with high objective quality but weak ownership will not be implemented. Collaborative planning ensures that goals and strategies are owned by the client and are not simply imposed by the counselor. Self-efficacy theory proposes that a person’s capacity to successfully undertake a task or realize a goal is enhanced through cognitive rehearsal and development of a positive expectancy as a result of thinking through the various processes required. A plan provides a map that supports the development of self-efficacy. The development of the plan provides a structure for the rehearsal process and the plan itself provides a continuing reference point that sustains self-efficacy. Cueing theory proposes that behavior change can be facilitated by external reminders that signal a specific response that is required in a specific circumstance. In the absence of such external cues, it is more likely that pre-existing internally directed responses will dominate. As new behaviors are applied and reinforced through positive outcomes, external cueing is less important. However, in the early stages of behavior change, cueing is vital. A plan is a set of cues and therefore assists a person seeking to change behavior by providing external reminders of the new behavior.
Page 94

THEORETICAL FOUNDATIONS OF GOAL CLARIFICATION Three theoretical frameworks provide information for this approach: Learning theory (self-efficacy) proposes that people are more likely to undertake a novel series of actions if they have developed a cognitive schema or belief that they are able to complete these actions. The development of goals is the first stage in the process of mapping out such a cognitive schema. Major goals include identifying the end-point, a series of intermediate goals and strategies to achieve these goals, and the means to achieve the end-point. When a client can identify goals for therapy that she can achieve, it increases his/her self-efficacy. Empowerment theory proposes that a person’s ownership of a solution to a problem is as important as the quality of the solution. A good solution with weak ownership will not be implemented. When a client works out a solution it not only addresses the specific need but also affirms his/her capacity to find solutions in general and therefore reduces his/her long-term dependence on professional assistance. Systems theory proposes that individual goals and goal focused behavior is not autonomous but rather occurs in the context of and in response to other system components such as family members, peers etc. Functioning within the system is, in part, determined by perception of the values and goals of key components within the system and effective change requires explicit attention to the wider system and not just individual goals.
Page 95

4/12/06 SDK/SC/SD 76
Evidence Base
Collaborative treatment planning appears to be a useful area for intervention, with an evidence rating of Four Stars. Research shows that collaboration is associated with increased confidence and decreased need for specialized services. In addition, setting goals and homework are both associated with positive treatment outcomes. In particular, collaboration during goal setting and the specificity—not the content—of goals seem to be key. In addition, both setting and compliance with homework are associated with more positive outcomes.
Click here on evidence base to access a comprehensive review.
What is the evidence?
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Bridging ConceptsCFIT
Page 96

EVIDENCE BASE Collaborative treatment planning: what works? Evidence rating: what does it mean? The 4 star evidence rating indicates findings from two or more randomized controlled trials with related but not equivalent client groups. These studies likely have adequate methodological rigor.
Both collaborative treatment planning and goal clarification (a specific method for doing collaborative treatment planning) achieved the 4 star evidence rating
What does the research on collaborative treatment planning suggest? Collaboration—particularly when the focus is on making decisions, specifying goals, and setting homework—is associated with positive therapy outcomes and decreased need for specialized services. • Specificity of goals but not content of goals is a predictor of counseling outcome
(Schwenn, 2002). • Homework setting and homework compliance [which can follow from collaborative
treatment plans] predict positive therapy outcome (Kazantzis, Deane, & Ronan, 2000; Kazantzis & Lampropoulos, 2002).
• Client experience of collaboration in decision making is associated with increased level of met need (Roth & Crane-Ross, 2002).
• Self management plans that promote client choice and decision making in chronic illness promoted confidence and reduced need for specialist services (Kennedy et al., 2004).
Page 97
EVIDENCE BASE Goal clarification: What works? What does the research on goal clarification suggest? Note: Goal clarification is a component of Problem Solving therapy (PST). The
evidence base presented here is partly derived from studies of problem solving therapy as a whole as well as goal clarification specifically.
Problem solving therapy, which can be used with adolescents, is associated with decreases in symptoms, family burden and readmissions. • Depressed clients in problem solving therapy enjoy symptom reduction to the same
extent and at the same rate as clients on medication (Mynors-Wallis, Gath, Lloyd-Thomas, & Tomlinson, 1995).
• PST, whether delivered by doctors or nurses, achieves the same outcomes and with approximately half the client contact time than is standard for cognitive-behavioral therapy (CBT; Mynors-Wallis, Gath, Day, & Baker, 2000). Note that this comparison is based on comparative effect sizes and standard treatment duration, not a randomized control trial comparing PST with CBT.
• Problem solving therapy is effective in reducing family burden and in reducing the rate of readmissions for adults with major mental illness (McFarlane, Dixon, Lukens, & Lucksted, 2003).
• Problem solving has been applied successfully with adolescent populations (Cleary & Zimmerman, 2004).
Collaborative goal setting is associated with positive outcomes. • Therapists, clients and caregivers do not start out with shared goals – these goals
need to be negotiated (Hawley & Weisz, 2003). • Collaborative goal setting predicts positive outcome in psychotherapy (Tryon &
Winograd, 2002). Goal commitment and goal attainment predict treatment-related improvements. • Progress in goal attainment predicts improvement in both role circumstances and
role satisfaction for adolescents (Sheldon & Elliot, 2000). • Clients with high commitment to treatment goals respond better to treatment of
bulimia than clients with low commitment (Mussell, et al. 2000).
Page 98

References
Cleary, T. J., & Zimmerman, B. J. (2004). Self-regulation empowerment program: A school-based program to enhance self-regulated and self-motivated cycles of student learning. Psychology in the Schools, 41, 537-550.
Hawley, K. M., & Weisz, J. R. (2003). Child, parent and therapist (dis)agreement on
target problems in outpatient therapy: The therapist's dilemma and its implications. Journal of Consulting and Clinical Psychology, 71, 62-70.
Kazantzis, N., Deane, F. P., & Ronan, K. R. (2000). Homework assignments in
cognitive and behavioral therapy: A meta-analysis. Clinical Psychology: Science and Practice, 7, 189-202.
Kazantzis, N., & Lampropoulos, G. K. (2002). Reflecting on homework in
psychotherapy: What can we conclude from research and experience? Journal of Clinical Psychology, 58, 577-585.
Kennedy, A. P., Nelson, E., Reeves, D., Richardson, G., Roberts, C., Robinson, A., et
al. (2004). A randomised controlled trial to assess the effectiveness and cost of a patient orientated self management approach to chronic inflammatory bowel disease. Gut, 53, 1639-1645.
McFarlane, W. R., Dixon, L., Lukens, E., & Lucksted, A. (2003). Family
psychoeducation and schizophrenia: A review of the literature. Journal of Marital and Family Therapy, 29, 223-245.
Mussell, M. P., Mitchell, J. E., Crosby, R. D., Fulkerson, J. A., Hoberman, H. M., &
Romano, J. L. (2000). Commitment to treatment goals in prediction of group cognitive-behavioral therapy treatment outcome for women with bulimia nervosa. Journal of Consulting and Clinical Psychology, 68, 432-437.
Mynors-Wallis, L. M., Gath, D. H., Day, A., & Baker, F. (2000). Randomised controlled
trial of problem solving treatment, antidepressant medication, and combined treatment for major depression in primary care. British Medical Journal, 320, 26-30.
Mynors-Wallis, L. M., Gath, D. H., Lloyd-Thomas, A. R., & Tomlinson, D. (1995).
Randomised controlled trial comparing problem solving treatment with amitriptyline and placebo for major depression in primary care. British Medical Journal, 310, 441-445.
Roth, D., & Crane-Ross, D. (2002). Impact of services, met needs, and service
empowerment on consumer outcomes. Mental Health Services Research, 4, 43-56.
Page 99

Schwenn, H. H. T. (2002). The relationship between client-established goals and outcome in counseling. Dissertation Abstracts International: Section B: The Sciences and Engineering, 63(5-B), 2603.
Sheldon, K. M., & Elliot, A. J. (2000). Personal goals in social roles: Divergences and
convergences across roles and levels of analysis. Journal of Personality, 68, 51-84.
Tryon, G. S., & Winograd, G. (2002). Goal consensus and collaboration. In J. C.
Norcross (Ed.), Psychotherapy Relationships That Work: Therapist Contributions and Responsiveness to Patients (pp. 109-125). London: Oxford University Press.
Page 100

CFIT Online Learning Center EVIDENCE RATING SYSTEM All evidence informing evidence-based practice is not equal. To help you evaluate the strength of the evidence cited, we use a star rating system with a maximum of seven stars for the highest rating of evidence, and one star for the lowest acceptable rating of evidence. The number of stars reflects two factors: evidence quality (the number and quality of studies that provide the evidence) and relevance (the extent to which the evidence relates to similar population and similar problems to those you are likely to be working with. The star rating system is at best a rough guide and you are invited to evaluate the quality and relevance of evidence cited by following up on the references provided. As new studies are being published each week, it is also important to attempt to keep abreast of emerging evidence by using databases such as Medline, Psych Info and Social Work Abstracts. Interpretation of Star Ratings ******* Findings from one or more meta-analyses with equivalent client groups
****** Findings from one or more meta-analyses with related but not equivalent client groups
***** Findings from two or more randomized controlled trials (RCTs) with equivalent client groups
**** Findings from two or more randomized controlled trials with related but not equivalent client groups
*** Findings from one randomized controlled trial or two or more controlled studies with equivalent client groups
** Findings from one randomized controlled trial or two or more controlled studies with related but not equivalent client groups
* Expert consensus or results of uncontrolled studies
Page 101

4/12/06 SDK/SC/SD 77
Collaborative plans are a key component of therapeutic alliance. Agreement on goals and tasks is central to alliance. The development of a collaborative plan is a process by which the counselor, the client and the caregiver negotiate agreed goals and strategies to achieve them.
In this process, the counselor acts as a coach, helping the client shape vague or general goals into specific and achievable goals. The counselor provides expertise about strategies that may be effective if agreed upon by the client.
A well designed collaborative plan also promotes positive treatment expectancy. Goals that are both important to the client and realizable set a framework for achievement. Realistic strategies and appropriate lifework assignments build confidence in the client that goals can and will be achieved.
How does collaborative treatment planning relate to therapeutic alliance?
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Bridging ConceptsCFIT
Page 102

4/12/06 SDK/SC/SD 78
Successful collaborative planning will result in mutual commitment to both treatment goals and to tasks that are designed to achieve these goals.
The counselor’s willingness to be direct and clear about third-party goals will help to reduce the clients suspicion that the counselor is an agent of the school, parents, etc. and provides a foundation for addressing goal conflict.
Collaborative planning is important in the management of therapeutic rupture. When a collaborative plan does not result in the expected outcomes, the alliance will be under strain.
Regular review of goals and strategies in the context of achievement of targets helps keep the alliance positive. Furthermore, it provides early evidence of divergences on goals and tasks that are indications of the development of an alliance rupture.
How does collaborative treatment planning relate to therapeutic alliance?
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Bridging ConceptsCFIT
Page 103

4/12/06 SDK/SC/SD 79
The training modules included in the CFIT Learning Center support all six of the core values of Providence Service Corporation.
Community- based & multi-
systemic services
Identifying and building on strengths
Respectful organizational
culture
Local viability that is
nationally supported
Best practice models
Cultural diversity
How does collaborative treatment planning correspond to PSC’s core values?
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Bridging ConceptsCFIT
Page 104
4/12/06 SDK/SC/SD 80
In the introductory module, you learned about how ‘common factors’correspond generally to PSC’s core values. Here, we relate collaborative treatment planning specifically to the six core values:
Community based and multi-systemic services. A key component of collaborative planning is identification of resources, including the support network that can help the client meet personal goals. This places the client and the counseling process in the context of the community and the wider system of care and ensures that the counseling maintains a multi-systemic focus.
Identifying and building on strengths. Collaborative planning is a way to empower clients and ensure that their goals are central to the counseling process. Client strengths are identified and utilized as essential resources in achieving goals.
How does collaborative treatment planning correspond to PSC’s core values?
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Bridging ConceptsCFIT
Page 105

4/12/06 SDK/SC/SD 81
Local viability that is nationally supported. Collaborative Planning is a core counseling process that can be readily utilized within a generic counseling framework and does not rely on highly specialized expertise, intensive training or additional resources. It can be utilized regardless of wealth or resources of a specific region.
Respectful organizational culture. The use of Collaborative Planning promotes positive relationships between counselors and supervisors. Collaborative plans provide a clear point of reference that help counselors and supervisors talk about progress in counseling and identify positive directions.
Best practice models. Collaborative Planning maps out a clear, concrete direction for counseling. Client strengths are mobilized in the process, while lifework assignments implement these directions to achieve best practice outcomes.
Cultural diversity. The emphasis on collaboration and engagement with the client and caregiver demonstrate sensitivity and respect for cultural differences.
How does collaborative treatment planning correspond to PSC’s core values?
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Bridging ConceptsCFIT
Page 106
4/12/06 SDK/SC/SD 82
Congratulations! You have completed this section.
If you are pressed for time, return at a later date to continue the module.
Third of five sections complete
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Bridging ConceptsCFIT
Page 107

4/12/06 SDK/SC/SD 83
You are entering the fourth section.
It should take approximately 10 minutes to complete, with a total of 11 pages.
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
ResourcesCFIT
Page 108
4/12/06 SDK/SC/SD 84
We have listed a variety of resources for continued learning including:• Toolbox Times Three (these are the same practice, reflection, and
supervision tools that appeared throughout the module summarized for your convenience)
• Books and articles (these are great sources of further information on topics related to the module, including clinical manuals where available)
• Websites (these are resources available on the internet, including both topic specific sites and sites related to more general clinical content)
• Cited References (these are references cited throughout the module, including the linked pages)
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
ResourcesCFIT
Page 109

4/12/06 SDK/SC/SD 85
A Work in ProgressYour opinions and experience are vital to the continued improvement of the CFIT Learning Center. Do you know of a resource not listed here? Do you have a practice, reflection, or supervision tool we might add to the Toolbox Times Three? Or, come back and tell us about your experience using the tools and resources we have listed. Please email us at [email protected].
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
ResourcesCFIT
Page 110

4/12/06 SDK/SC/SD 86
Practice ToolsGoal ClarificationBrainstorming StrategyValues CompassValues Assessment Worksheet
Supervision Tools
Reflection Tools
ToolboxTimes3
Whose language do you use when you write treatment plans and documentation notes?How do you help your clients discover their own inner language?How do you encourage growth?Do you allow for spontaneity in your sessions?
What are you doing to create a level playing field with your client?What are you getting from and contributing to your supervision?
Click here to open up all the tools in one document for easy printing.
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
ResourcesCFIT
Page 111

1
CFIT Online Learning Center Collaborative Treatment Planning Practice Tool: Goal Clarification Exercise You can complete this exercise with your client and family to identify, clarify and negotiate goals.
Background Goals: Realizable intermediate steps that can be attained along the way toward achieving
major goals. Goal clarification can often be achieved by:
• Inquiring about the goals of your client • Differentiating longer and shorter term goals • Prioritizing goals • Identifying goals that are in conflict with the goals or values of other key people • A more systematic and structured manner using specifically designed exercises, such
as the one that follows Purpose This exercise provides the starting point for: 1. Identifying specific client goals 2. Identifying conflicting goals, which may be targeted with motivational interviewing
strategies It will often be important to achieve goal clarification with caregivers or other key people in the client’s life so that everyone with a stake in the counseling is clear about what each party is seeking to achieve.
• This can be done completing this as a family exercise, or by doing the exercise with only the caregivers
Indications Use this goal clarification exercise when:
• Client goals are unclear • Expectations for counseling are low • There is evidence of conflict between the goals of different stakeholders • CFIT measures indicate:
• Low client and caregiver expectations • Discrepancy between client and family expectations
Contraindications This exercise is not recommended when:
• There is a very clear focal problem • CFIT measures indicate that client expectations remain very low
• In this case, it is better to work on building alliance to develop rapport and more positive expectations before proceeding to this goal clarification exercise
Page 112

2
Preparation for Exercise The following steps should be taken before doing this exercise:
1. Review client and caregiver expectations based on the ETQ • Note total score (high, medium, low) of ETQ • Note whether there are differences in outcome expectations between the youth
and caregiver • Examine item-level information about role and process expectations for signs
of low expectations
2. Gather necessary materials: • 6 sets of ‘post-it’ pads – each a different color • Fine point marker • 6 sheets of poster paper
Overview of Exercise This following goal clarification exercise has five phases:
1. Orienting the client to the exercise 2. Identifying the stakeholders of counseling 3. Describing the goals of each stakeholder 4. Ranking stakeholder goals 5. Identifying shared goals, unshared goals, and mutually exclusive goals
Procedure 1. Explain the purpose of the exercise:
Example: “I want to get a clear picture of what different people are hoping to achieve from the counseling. I have looked at the survey you completed about your expectations for counseling and also the survey your caregiver completed so I have some general ideas – but now I want to get really clear so I can help you achieve the things you want. Is that OK?”
If client is happy to proceed, go to the next step.
If the client is uncertain or unwilling, check for concerns and discuss until she or he is ready to proceed.
2. Identify the stakeholders of counseling:
Example: “The first thing I would like you to do is to think about the people who want or hope for something good to come out of the counseling – who comes to mind?”
When the client names a person or category give him/her a colored post-it pad and have her/him write the person’s name or category on the top post-it – e.g., mom, teacher, parole officer, best friend, sibling etc.
If ‘me’ has not come up within the first people or categories, prompt – “What about you?” Be prepared to prompt for other categories until you are sure you have all the important stakeholders.
Page 113

3
Continue until all stakeholders have been identified, putting each person’s name on the top post-it of a pad.
3. Describe the goals of each stakeholder:
Example: “I would like to get your ideas about all the kinds of good things that you and the people you listed think might come from the counseling.”
Once the client identifies an outcome, ask the client to write it down on the next post-it in that stakeholder’s pad.
Identify any other stakeholders that would share the same wish and write the wish post-its in their pads.
Ask if the client also shares that wish. If so, have him/her add it to his/her post-it pad.
There should be only one wish per post-it for each stakeholder.
When the process is exhausted get the client to review the wishes they have recorded on the ‘me’ post-it pad and ask if any of her or his own wishes have been overlooked.
4. Rank the goals of each stakeholder:
Have the client write the name of each stakeholder on the top of a sheet of poster paper. Put each stakeholder on a separate sheet of paper.
Stick the post-its for each person in the order of importance that the client thinks this person would have for the various wishes, with the most important ones at the top and the least important at the bottom.
5. Identify shared goals, unshared goals, and mutually exclusive goals:
Ask the client to review her/his own wish list and to identify any wishes that are incompatible with another person’s wish.
You may end the exercise with something like: “Thank you for helping me get a better understanding of what different people are hoping to achieve from your counseling. This will help me in helping you achieve some of the things you want.”
Page 114

CFIT Online Learning Center Collaborative Treatment Planning Practice Tool: Brainstorming Exercise You can do this activity you with your clients to generate strategies for identified goals. This exercise helps to stimulate the creative process so both the counselor and client can have some fun while brainstorming all the ways in which clients can achieve their goals. Brainstorming Strategy Brainstorming is a useful procedure for generating strategies. The counselor asks the client to come up with all the ways of achieving the goal s/he can imagine. A white board or something similar is helpful with brainstorming because it enables both client and counselor to keep track of the work that is taking place. PHASE 1: Free Thinking In the first phase of brainstorming there is no reality testing- ‘Tell me anything you can think of – we will work out later if it is practical’. After the client has exhausted ideas, the counselor can throw in a few as well. If the counselor has some very practical suggestions that might work, it is a good idea to include a few ‘wild’ ideas as well. The reason for this is that when it comes to reality testing, both client and counselor will get some suggestions thrown out quickly – this ensures that it is not a split between the counselor with good ideas and the client with dumb ideas. It also models for the inhibited client that it is OK to think laterally. When the counselor is done the client gets another opportunity to suggest some ideas. PHASE 2: Reality Testing The second phase is reality testing, the ideas are sorted into 3 categories: 1.) ‘won’t work’ 2.) ‘might work’ 3.) ‘should work’ or something similar. The client takes the lead on the sort with the counselor acting mainly as recorder. The sort can be done using 3 columns on a white board or using cards or pieces of paper if there is no white board. When the client dismisses an idea that the counselor thinks has merit, the counselor can ask: ‘what about this do you think won’t work/’ or ‘could it work if …?’
1
Page 115

If the client has something in the ‘should work’ category that the counselor thinks improbable, the counselor can say: ‘I don’t understand that one – tell me how it would work’. Ideas can be shifted from one column to the next until both counselor and client are happy with the assignment. PHASE 3: Prioritizing The third phase is prioritizing. The focus is on the ‘should work’ category. The aim is to find the strategy or strategies that the client prefers which will yield results quickly and can be implemented without difficulty.
• Strategies can be cognitive such as practicing positive self statements, actions such as practicing ball handling drills or interactions such as saying ‘Hi’ to a new student in class
• A time frame for implementing each strategy should be discussed
• These strategies provide the basis for the ‘lifework’ that the client will
undertake
2
Page 116

Adapted from: Hayes, S.C., Strosahl, K.D. & Wilson, K.G. (2003). Acceptance and commitment therapy: An experiential approach to behavior change. NY: Guilford.
1
CFIT Online Learning Center Collaborative Treatment Planning Practice Tool: Values Compass Exercise You can complete this activity with your clients to help them identify important values in their life that they would like to focus on and strengthen. Once the client has identified important values, you can work together to create lifework assignments that the client can do between sessions. Directions: Use this diagram as a guide. Have the youth draw a circle in the center of the page and have him write “The Me I Want to Be” or a version of this using his own words. Next, ask the youth to identify the most important areas/values in his life. Offer a few examples like those listed in the diagram to get the creative process started. Draw lines from the center of the circle and create smaller circles for each “value” he/she identifies. Once the youth has an exhaustive list, work with the youth to prioritize them in order of importance. After the youth has prioritized the list, ask the youth to write in the middle of the circle what he values about _______. So, for example, if the youth identified Friendship as one of his top priorities, ask him what he values about friendship and have him write it in the middle of the circle. What characteristics are important to him in a friend? What kind of friend is he? Is he the kind of friend to others that he wants a friend to be to him? The idea is to help the youth identify values that are important to him and things that he can do to strengthen the areas that matter most to him. Use the Values Assessment Worksheet to record identified goals for the values, action steps toward achieving goals, and potential barriers.
Page 117

Values Compass
Values: These are the “big picture” or “longer-term” things you want to do- values are like our life’s journey
Some areas that values may be about are:
Dating Education Family Friendships Health Recreation/Fun Work So, the question is…where do you want to go?
Adapted from: Hayes, S.C., Strosahl, K.D. & Wilson, K.G. (2003). Acceptance and commitment therapy: An experiential approach to behavior change. NY: Guilford.
2
Page 118

CFIT Online Learning Center Collaborative Treatment Planning Practice Tool: Values Assessment Worksheet
Adapted from: Hayes, S.C., Strosahl, K.D. & Wilson, K.G. (2003). Acceptance and commitment therapy: An experiential approach to behavior change. NY: Guilford.
1
The blank worksheet on the following page can be used to record the values the youth identified in the Values Compass Exercise. It provides clients with a structure to list goals, action steps, and potential barriers to achieving goals.
Page 119
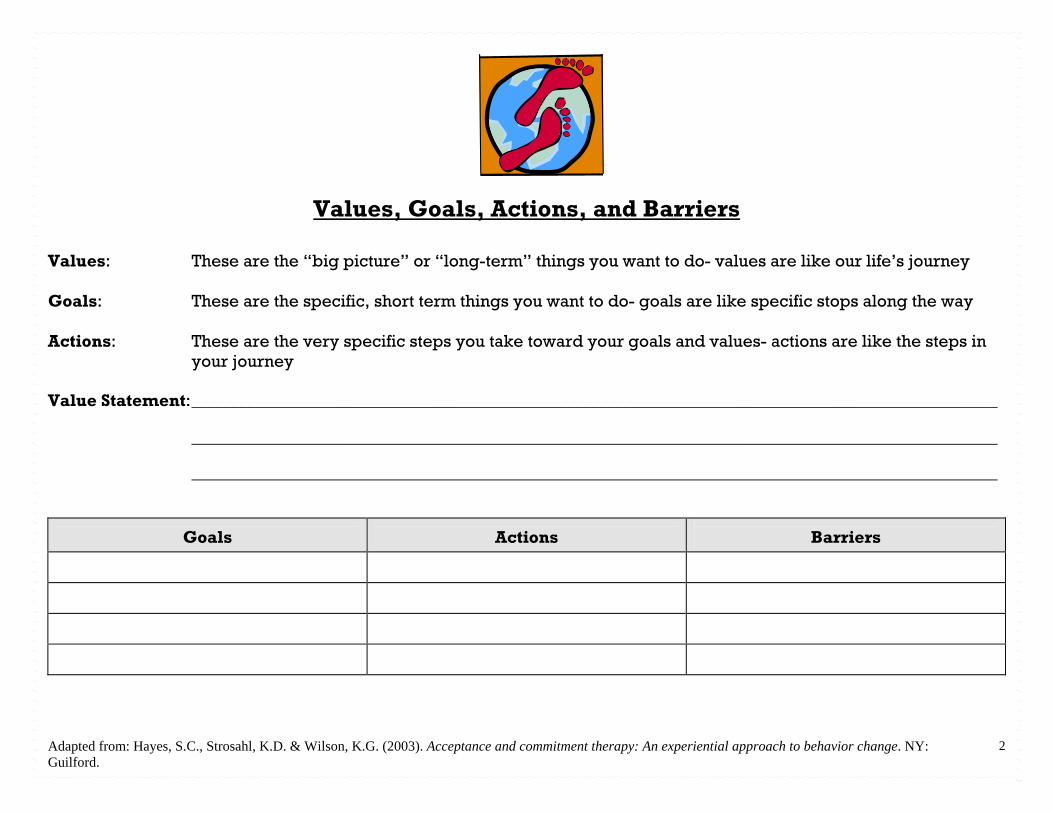
Adapted from: Hayes, S.C., Strosahl, K.D. & Wilson, K.G. (2003). Acceptance and commitment therapy: An experiential approach to behavior change. NY: Guilford.
2
Values, Goals, Actions, and Barriers
Values: These are the “big picture” or “long-term” things you want to do- values are like our life’s journey Goals: These are the specific, short term things you want to do- goals are like specific stops along the way Actions: These are the very specific steps you take toward your goals and values- actions are like the steps in
your journey Value Statement: _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ _____________________________________________________________________________________________________
Goals
Actions
Barriers
Page 120

CFIT Online Learning Center Collaborative Treatment Planning Reflection: Whose language do you use when you write treatment plans and documentation notes? DIRECTIONS: The reflections and reflective exercises are intended to give you some thoughts/questions to think about when you have some quiet time. Take a moment to think about the questions and write out the answers. Reflection:
A shift in [the client’s] experience takes place when [they] find the right word to describe it. When [they] are called by [their] correct name, or [their] experience is correctly named, [they] relax and breathe easier from being understood (Johanson & Kurtz, 1991, p. 2).
Reflective Exercise: When you are working with your clients, do you use their words when writing out their goals, objectives and strategies…or do you use your language? Pull out a treatment plan and try reading it from the client’s perspective. Whose words are they? What was your experience when you read it from the client’s perspective? Do your client and family understand everything that is on the client’s treatment plan? Do they understand you when you are talking with them during their session? If they read your documentation notes, would they understand and agree with what you have written? Would they feel understood? Would they feel respected and heard? How do you know? What do they say or do that tells you they feel respected and heard?
Johanson, G. & Kurtz, R. (1991). Grace unfolding: Psychotherapy in the spirit of the Tao-te ching. New York: Bell Tower.
Page 121

CFIT Online Learning Center Collaborative Treatment Planning Reflection: How do you help your clients discover their own inner wisdom? DIRECTIONS: The reflections and reflective exercises are intended to give you some thoughts/questions to think about when you have some quiet time. Take a moment to think about the questions and write out the answers Reflection:
The work of therapists is not analogous to that of engineers or artists. Therapists do not create something they can stand back from, look at, and claim as their own. Mindful, nonviolent therapy simply helps [clients] discover and affirm the wisdom of [their] inner experience (Johanson & Kurtz, 1991, p. 38).
Exercise: What specifically did you do in previous sessions with clients (think of at least 3 clients you are currently working with) that: Helped them discover the wisdom of their inner experience? Helped them to discover new insights about their experiences? Make a list of questions you asked that initiated reflection and insight. Make a list of exercises, or activities you did that seemed to generate movement in the client. Do you have a client or clients that “feel” stuck? Try some of these things from your list and notice what happens…
Johanson, G. & Kurtz, R. (1991). Grace unfolding: Psychotherapy in the spirit of the Tao-te ching. New York: Bell Tower.
Page 122

CFIT Online Learning Center Collaborative Treatment Planning Reflection: How do you encourage growth? DIRECTIONS: The reflections and reflective exercises are intended to give you some thoughts/questions to think about when you have some quiet time. Take a moment to think about the questions and write out the answers Reflection:
The compassion of the therapist, sometimes expressed through laughter, can affirm the presence of [the client’s] buried resourcefulness, whereas a response of pity would be an affirmation that [the client] does not have what it takes, that [the client] need[s] a white knight to save [her] (Johanson & Kurtz, 1991, p. 26).
Exercise: Counselors are present in different ways at different times for different people. However, they are constantly making careful judgments about what is happening or can happen to encourage [the client’s] growth in human-beingness. This is the counselor’s main criterion for acting: In your next session, ask yourself these questions: Will what you do or not do in the moment be helpful in [the client’s] study and discovery of themselves? Will it support the client’s healing and growth? How will it support the client’s healing and growth?
Johanson, G. & Kurtz, R. (1991). Grace unfolding: Psychotherapy in the spirit of the Tao-te ching. New York: Bell Tower.
Page 123

CFIT Online Learning Center Collaborative Treatment Planning Supervision: What are you doing to create a level playing field with your client? DIRECTIONS: The supervision exercises and questions are intended to give you some guided questions to think about and bring to your supervision session and talk over with your clinical supervisor. Questions for Supervision: In understanding that while we are trying to create a respectful collaborative process, there remains a power differential between you and your client, because counselors are being paid to provide a service. Therefore, the questions to bring to supervision are: What is it that I need to do in my sessions to level the playing field? And what have I done up to this point to facilitate that? What has worked? What has not worked? What can I try that I have not tried yet?
Page 124

CFIT Online Learning Center Collaborative Treatment Planning Supervision: What are you getting and contributing to your supervision? DIRECTIONS: The supervision exercises and questions are intended to give you some guided questions to think about and bring to your supervision session and talk over with your clinical supervisor. Questions for Supervision: In understanding that while your supervisor is trying to create a respectful collaborative process, there remains a power differential between you and your supervisor due to your supervisor’s position and authority in the agency. Supervision is only effective if the supervisee feels safe, respected, and heard. Therefore, the question to bring to supervision is: What do I need from my supervision to feel safe? Am I getting this? What do I need from my supervisor to feel respected? Am I getting this? How will I know if I have been heard? Is this happening? What can I do to contribute to create a respectful environment? Am I doing this? Do I “hear” my supervisor? Can I share this exercise with my supervisor? If the answer is no…and you do not have safety in your supervision…is there another person in a supervisory role to whom you can go to and share your struggle?
Page 125
4/12/06 SDK/SC/SD 87
de Shazer, S. (1984). The death of resistance. Family Process, 23, 79-93.
King, R., Bambling, M., & Shea, S. (In Draft). Problem solving therapy: Treatment manual for individual and group therapy.
Nezu, A. M., Nezu, C. M., & Lombardo, E. (2004). Cognitive-behavioral case formulation and treatment design: A problem-solving approach. New York: Springer Publishing Co.
Nezu, A. M., Nezu, C. M., & Perri, M. G. (1989). Problem-solving therapy for depression: Theory, research, and clinical guidelines. New York: Wiley.
Books and Articles
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
ResourcesCFIT
Page 126

4/12/06 SDK/SC/SD 88
Motivational interviewing: Resources for clinicians, researchers and trainers (n.d.). Retrieved May 18, 2006, from: http://www.motivationalinterview.org/
Websites
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
ResourcesCFIT
Page 127

4/12/06 SDK/SC/SD 89
Cited References
Cleary, T. J., & Zimmerman, B. J. (2004). Self-regulation empowerment program: A school- based program to enhance self-regulated and self-motivated cycles of student learning. Psychology in the Schools, 41, 537-550.
de Shazer, S. (1984). The death of resistance. Family Process, 23, 79-93.
Hawley, K. M., & Weisz, J. R. (2003). Child, parent and therapist (dis)agreement on target problems in outpatient therapy: The therapist's dilemma and its implications. Journal of Consulting and Clinical Psychology, 71, 62-70.
Hayes, S.C., Strosahl, K., & Wilson, K.G. (1999). Acceptance and Commitment Therapy: An experiential approach to behavior change. NY: Guilford.
Johanson, G., & Kurtz, R. (1991). Grace unfolding: Psychotherapy in the spirit of the Tao-te ching. NY: Bell Tower.
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
ResourcesCFIT
Page 128
4/12/06 SDK/SC/SD 90
Cited References
Kazantzis, N., Deane, F. P., & Ronan, K. R. (2000). Homework assignments in cognitive and behavioral therapy: A meta-analysis. Clinical Psychology: Science and Practice, 7, 189-202.
Kazantzis, N., & Lampropoulos, G. K. (2002). Reflecting on homework in psychotherapy: What can we conclude from research and experience? Journal of Clinical Psychology, 58, 577-585.
Kennedy, A. P., Nelson, E., Reeves, D., Richardson, G., Roberts, C., Robinson, A., et al. (2004). A randomised controlled trial to assess the effectiveness and cost of a patient orientated self management approach to chronic inflammatory bowel disease. Gut, 53, 1639- 1645.
Lambert, M. J. & Ogles, B. M. (2004). The efficacy and effectiveness of psychotherapy. In M. J. Lambert (Ed.). Bergin & Garfield’s Handbook of psychotherapy and behavior change (5th Ed., pp. 139-193). New York: Wiley.
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
ResourcesCFIT
Page 129

4/12/06 SDK/SC/SD 91
Cited References
McFarlane, W. R., Dixon, L., Lukens, E., & Lucksted, A. (2003). Family psychoeducation and schizophrenia: A review of the literature. Journal of Marital and Family Therapy, 29, 223- 245.
Mussell, M. P., Mitchell, J. E., Crosby, R. D., Fulkerson, J. A., Hoberman, H. M., & Romano, J. L. (2000). Commitment to treatment goals in prediction of group cognitive-behavioral therapy treatment outcome for women with bulimia nervosa. Journal of Consulting and Clinical Psychology, 68, 432-437.
Mynors-Wallis, L. M., Gath, D. H., Day, A., & Baker, F. (2000). Randomised controlled trial of problem solving treatment, antidepressant medication, and combined treatment for major depression in primary care. British Medical Journal, 320, 26-30.
Mynors-Wallis, L. M., Gath, D. H., Lloyd-Thomas, A. R., & Tomlinson, D. (1995). Randomised controlled trial comparing problem solving treatment with amitriptyline and placebo for major depression in primary care. British Medical Journal, 310, 441-445.
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
ResourcesCFIT
Page 130

4/12/06 SDK/SC/SD 92
Cited References
Roth, D., & Crane-Ross, D. (2002). Impact of services, met needs, and service empowerment on consumer outcomes. Mental Health Services Research, 4, 43-56.
Safran, J.D. & Muran, J.C. (2000). Negotiating the therapeutic alliance: A relational treatment guide. NY: Guilford.
Schwenn, H. H. T. (2002). The relationship between client-established goals and outcome in counseling. Dissertation Abstracts International: Section B: The Sciences and Engineering, 63(5-B), 2603.
Sheldon, K. M., & Elliot, A. J. (2000). Personal goals in social roles: Divergences and convergences across roles and levels of analysis. Journal of Personality, 68, 51-84.
Tryon, G. S., & Winograd, G. (2002). Goal consensus and collaboration. In J. C. Norcross (Ed.), Psychotherapy Relationships That Work: Therapist Contributions and Responsiveness to Patients (pp. 109-125). London: Oxford University Press.
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
ResourcesCFIT
Page 131

4/12/06 SDK/SC/SD 93
Congratulations! You have completed this section.
If you are pressed for time, return at a later date to continue the module.
Fourth of five sections complete
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
ResourcesCFIT
Page 132

4/12/06 SDK/SC/SD 94
You are entering the final section.
It should take approximately five minutes to complete.
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Module EvaluationCFIT
Page 133

4/12/06 SDK/SC/SD 95
Your evaluation of this CFIT learning module is vital to continued improvement. Your responses to this brief survey are completely anonymous. Your name and ID number are not linked in any way, so please feel free to answer as completely and honestly as possible.
Click on the link below to complete the survey. Once you’re done, you’ll return to this page.
Module Evaluation
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Module EvaluationCFIT
Page 134

4/12/06 SDK/SC/SD 96
Congratulations!
You have almost completed this module. When you leave this page and return to the CFIT Training section of the CareLogic system, don’t forget to take the self-test (only seven questions long) to finish this module.
Last of five sections complete
© Vanderbilt University, All rights reserved
COLLABORATIVE TREATMENT PLANNING
Module EvaluationCFIT
Page 135
CFIT Online Learning Center Glossary Cognitive Dissonance: Cognitive dissonance is a psychological phenomenon that occurs when a person realizes the incompatibility or inconsistency between two or more of their attitudes, beliefs or behaviors. For example, if a person states a belief yet his/her behavior is inconsistent with that statement, he/she may experience this type of psychological conflict. Cognitive dissonance may be resolved by either modifying the belief or the behavior. Common Factors: Lambert and Ogles (2004, p. 151) define common factors as “those dimensions of the treatment setting (therapist, therapy, client) that are not specific to any particular technique.” The broad categories that common factors may fall into are: client characteristics, therapist characteristics, change processes, treatment structure and therapeutic relationship. Disembedding: Disembedding refers to the process of disengaging from a communication pattern (e.g., therapeutic alliance rupture). This process includes both the therapist recognizing his or her participation and contribution to this process, and then actively stopping the rupture cycle, often through the technique of metacommunication (see definition below). Goals: Goals represent short-term things that individuals want to achieve. In the context of values, goals are like stops along the way or places you want to visit during life’s journey (Hayes, Strosahl & Wilson, 1999). Goals are things that can be achieved or accomplished- they can be checked off of a list. Goals might be directed toward pursuing life values or may be based on desired counseling outcomes. Lifework: While clients often work with their counselors on developing goals and learning new skills to help achieve these goals, often clients need to practice or work on these counseling-related goals and skills in their everyday lives. Thus, lifework represents tasks and goals set by the counselor and client that will help enhance or facilitate the work that happens in session. Thus, these are tasks the client agrees to undertake between sessions. Metacommunication: Metacommunication is the skill of disengaging from an alliance rupture by talking with the client about the current interaction (Safran & Muran, 2000). This is done by moving the conversation toward a discussion of the rupture interaction in the here-and-now experience. Therapeutic Alliance (TA): TA is commonly regarded as having three components:
a bond between the counselor and the client based on mutual linking, respect, and trust
a set of common goals that provides the framework for the counseling work that is done together
1
Page 136

agreement about the kinds of tasks that will result in these goals being achieved
Therapeutic Rupture: The three components of TA are closely interlinked and a failure in one will usually result in a failure in the others. Even though the counselor and client might have common goals, if the client does not think the counselor is understanding or respectful, she or he will be reluctant to work with the counselor to achieve these goals. These kinds of problems constitute ‘alliance rupture,’ which is sometimes unavoidable in counseling. It is important to recognize and repair it at the earliest opportunity. Values: As described in Hayes, Strosahl & Wilson (1999), values represent desired long-term life directions. Values are like the life’s journey. While people may take steps toward or away from their values, they never achieve or fail at them. In this way, values are like a life path or direction. Different people may place different value on different areas of life and may want different things from those life areas. Common areas of life that people may value include: dating/marriage, education, family, friendships, health, parenting, recreation/fun, and work. References Hayes, S.C., Strosahl, K., & Wilson, K.G. (1999). Acceptance and Commitment Therapy: An experiential approach to behavior change. NY: Guilford. Lambert, M. J. & Ogles, B. M. (2004). The efficacy and effectiveness of psychotherapy. In M. J. Lambert (Ed.). Bergin & Garfield’s Handbook of psychotherapy and behavior change (5th Ed., pp. 139-193). New York: Wiley. Safran, J.D. & Muran, J.C. (2000). Negotiating the therapeutic alliance: A relational treatment guide. NY: Guilford.
2
Page 137