challenges in surgery of cutaneous melanoma: indications ... f064... · risk factor odds ratio ......
TRANSCRIPT

Challenges in Surgery of
Cutaneous Melanoma:
Indications for Margin Control
Prior to Reconstruction
Christopher J. Miller, MDDirector of Dermatologic Surgery
Assistant Professor of Dermatology
I have no conflicts of interest
or relevant ties with industry.
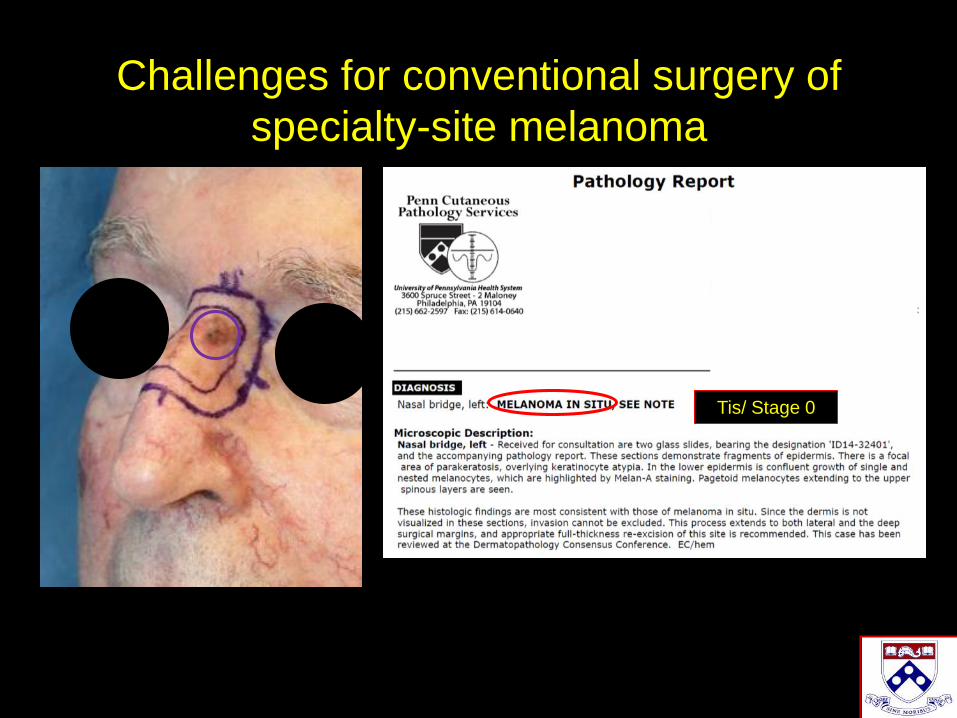
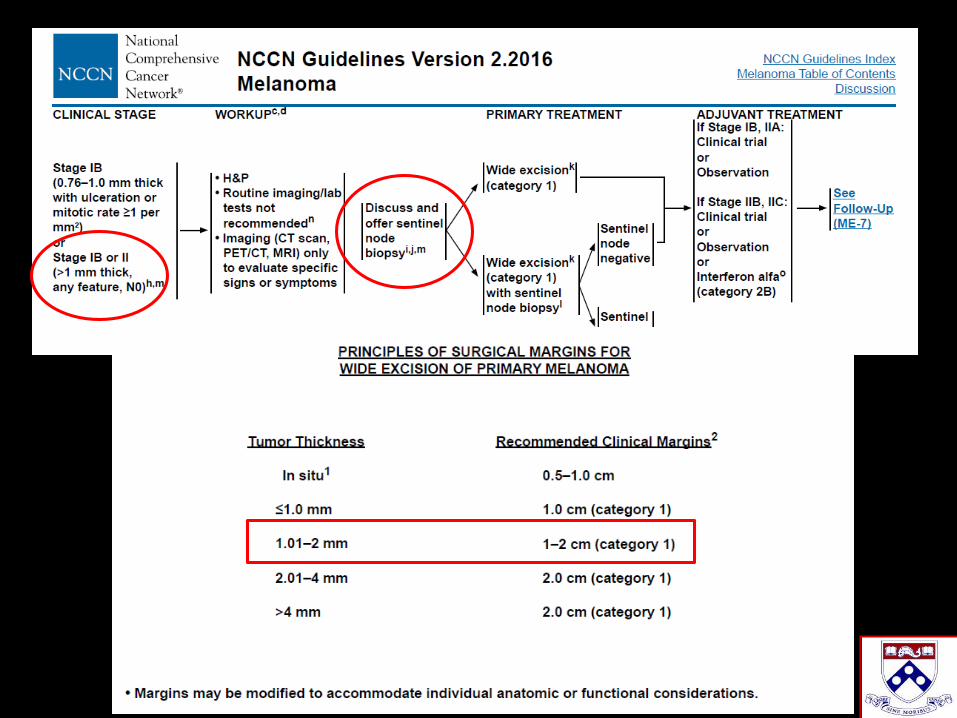
Challenges for conventional surgery of
specialty-site melanoma
Tis/ Stage 0
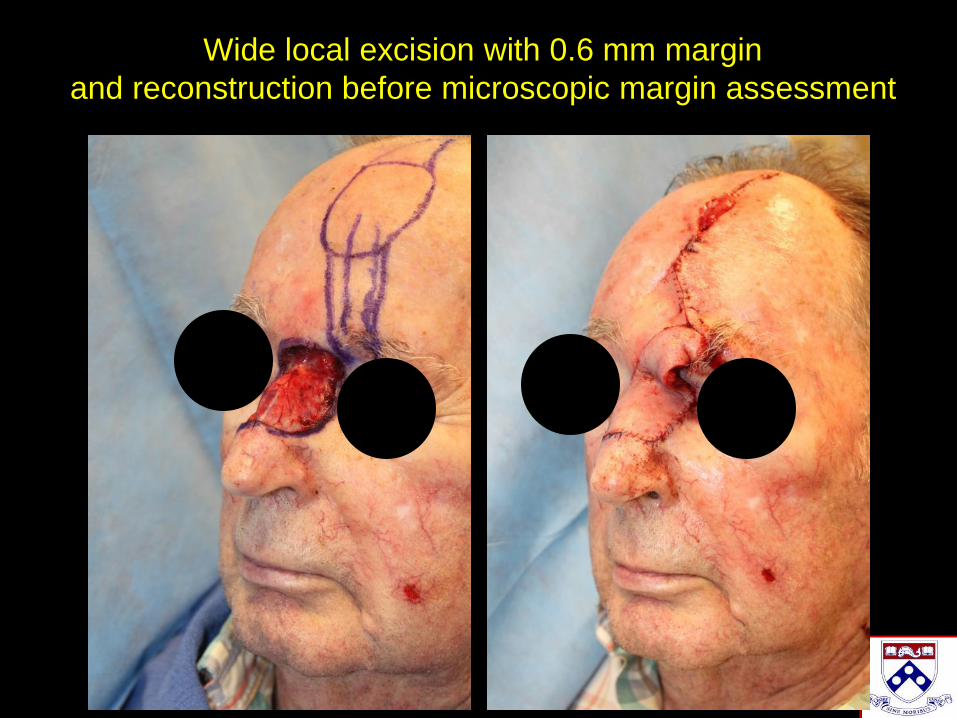
Wide local excision with 0.6 mm margin
and reconstruction before microscopic margin assessment

Upstaged from MIS to IIA
Positive margins
1.62 mm, 1 mit/mm2, no ulceration
T2b/Stage IIA
*Upstaged to SLNB candidacy
Outline
• Define the problem:
–Rule of 10s
• Define the solution:
–Microscopic margin-controlled
surgery before reconstruction
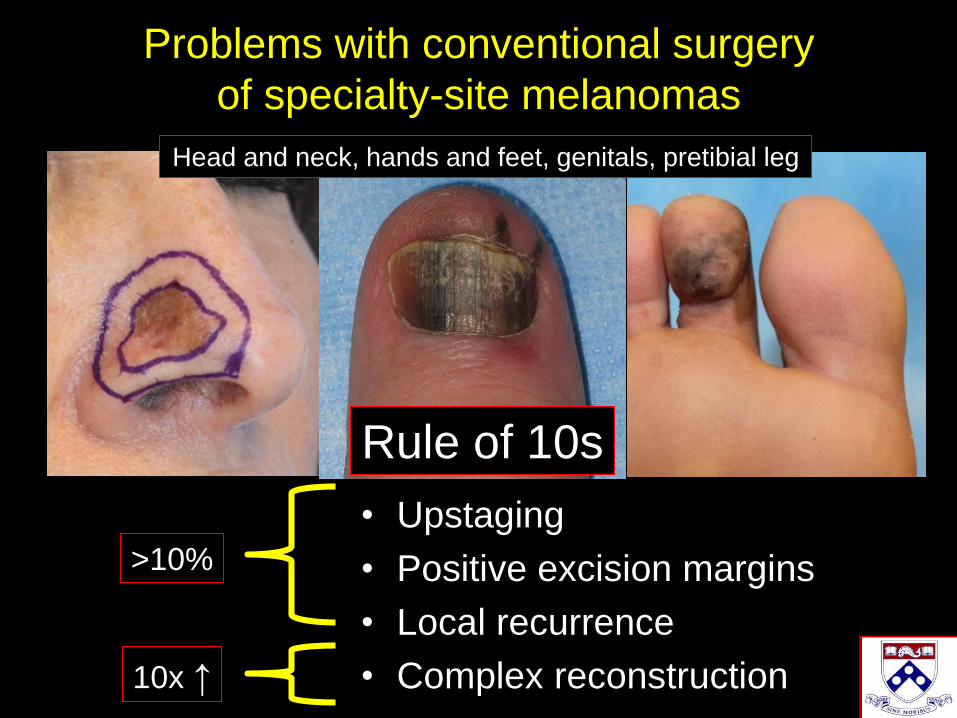
Problems with conventional surgery
of specialty-site melanomas
Head and neck, hands and feet, genitals, pretibial leg
• Upstaging
• Positive excision margins
• Local recurrence
• Complex reconstruction
>10%
10x ↑
Rule of 10s

Conventional Surgery
Rule of 10s
>10% risk of
upstaging after
reconstruction

1332 melanomas treated with
conventional WLE at Penn
Primary outcome: upstaging
(defined as increase in the AJCC T stage
after excision)
J Am Acad Dermatol 2017;77:341-8
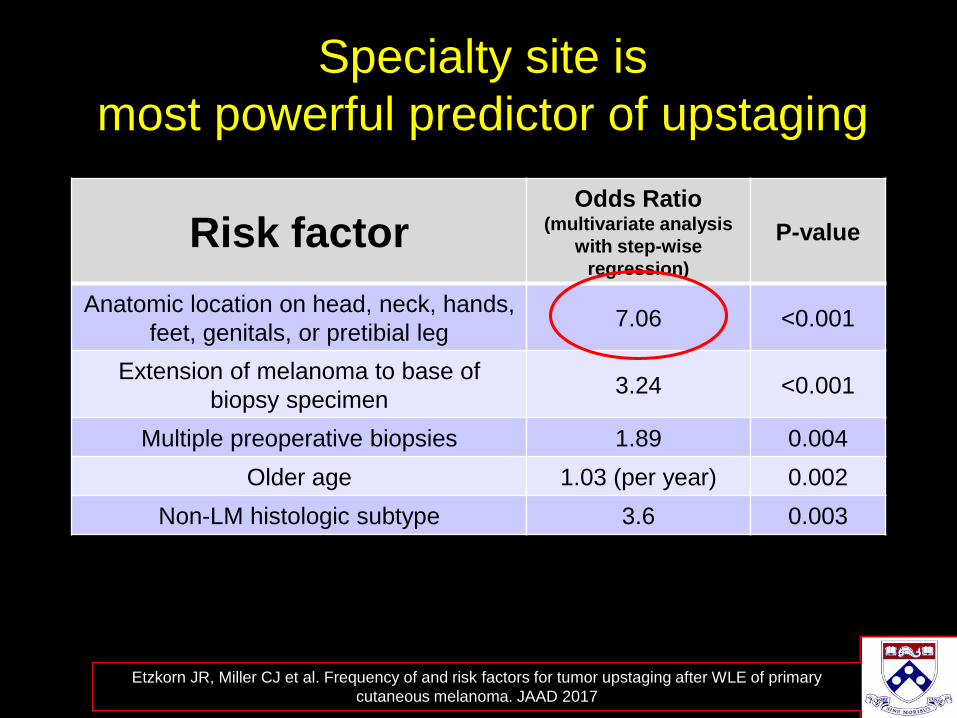
Specialty site is
most powerful predictor of upstaging
Risk factorOdds Ratio
(multivariate analysis
with step-wise
regression)
P-value
Anatomic location on head, neck, hands,
feet, genitals, or pretibial leg7.06 <0.001
Extension of melanoma to base of
biopsy specimen3.24 <0.001
Multiple preoperative biopsies 1.89 0.004
Older age 1.03 (per year) 0.002
Non-LM histologic subtype 3.6 0.003
Etzkorn JR, Miller CJ et al. Frequency of and risk factors for tumor upstaging after WLE of primary
cutaneous melanoma. JAAD 2017
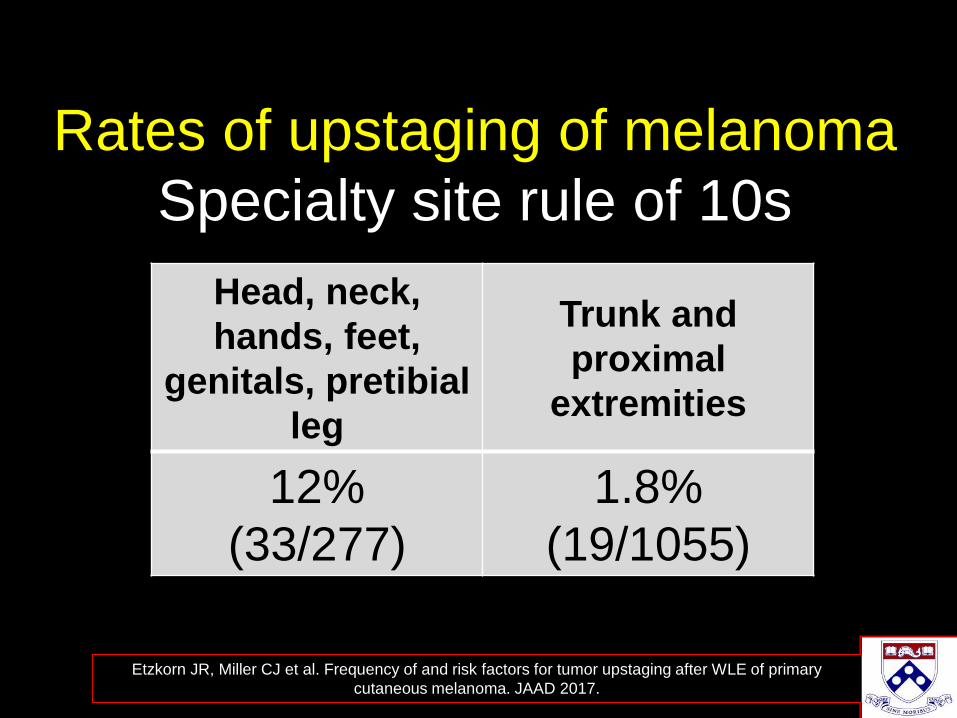
Rates of upstaging of melanoma
Specialty site rule of 10s
Head, neck,
hands, feet,
genitals, pretibial
leg
Trunk and
proximal
extremities
12%
(33/277)
1.8%
(19/1055)
Etzkorn JR, Miller CJ et al. Frequency of and risk factors for tumor upstaging after WLE of primary
cutaneous melanoma. JAAD 2017.
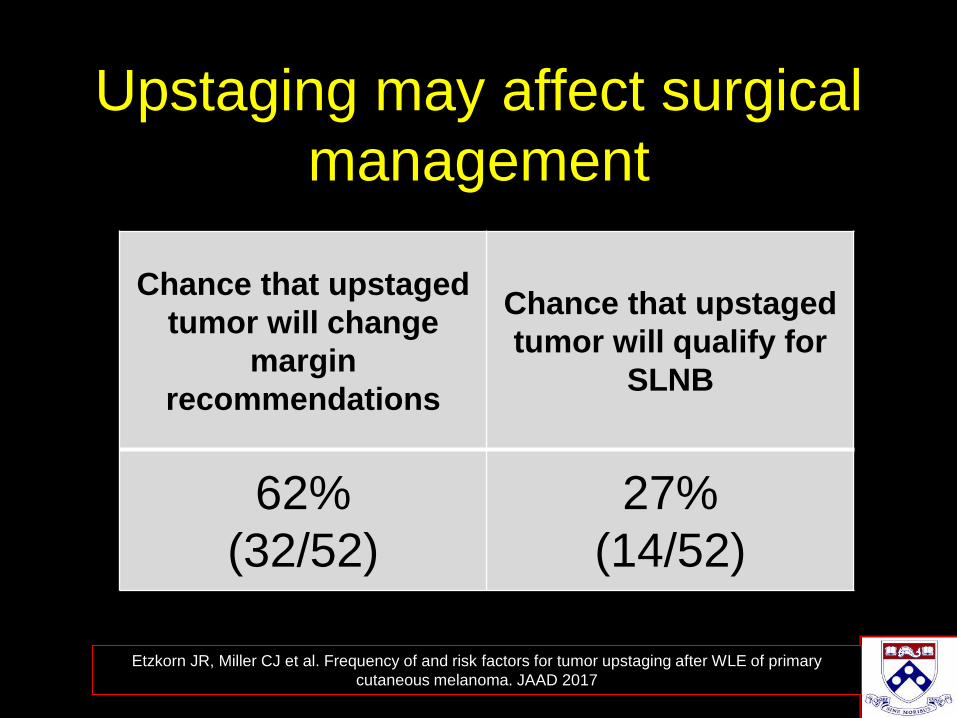
Upstaging may affect surgical
management
Chance that upstaged
tumor will change
margin
recommendations
Chance that upstaged
tumor will qualify for
SLNB
62%
(32/52)
27%
(14/52)
Etzkorn JR, Miller CJ et al. Frequency of and risk factors for tumor upstaging after WLE of primary
cutaneous melanoma. JAAD 2017
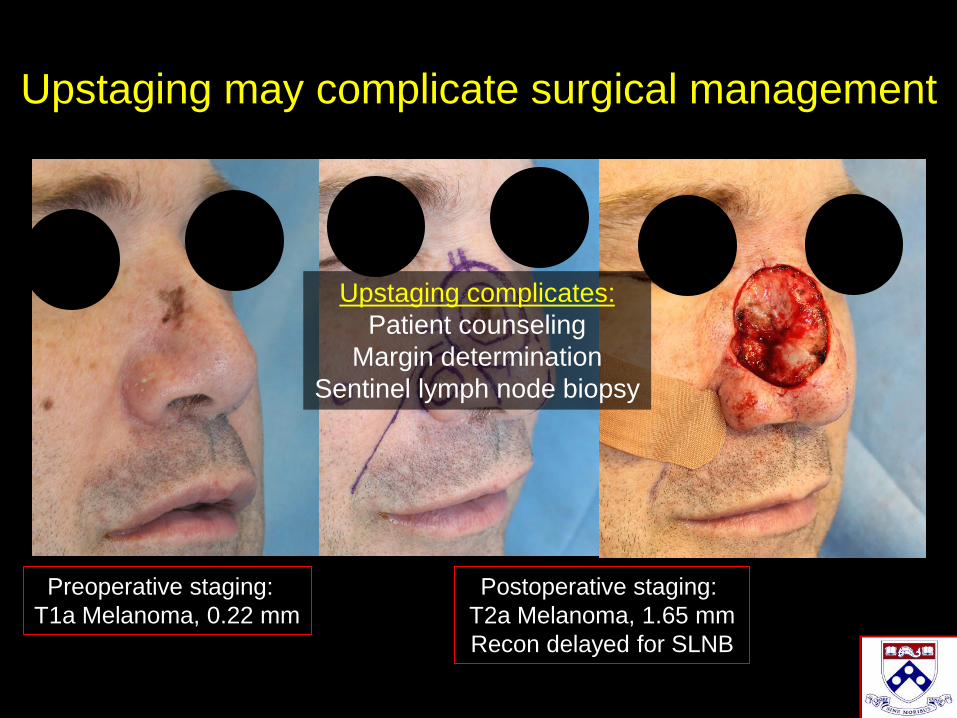
Upstaging may complicate surgical management
Preoperative staging:
T1a Melanoma, 0.22 mm
Postoperative staging:
T2a Melanoma, 1.65 mm
Recon delayed for SLNB
Upstaging complicates:
Patient counseling
Margin determination
Sentinel lymph node biopsy

Conventional Surgery
Rule of 10s>10% risk of positive
margins after
reconstructionExcision with positive margins
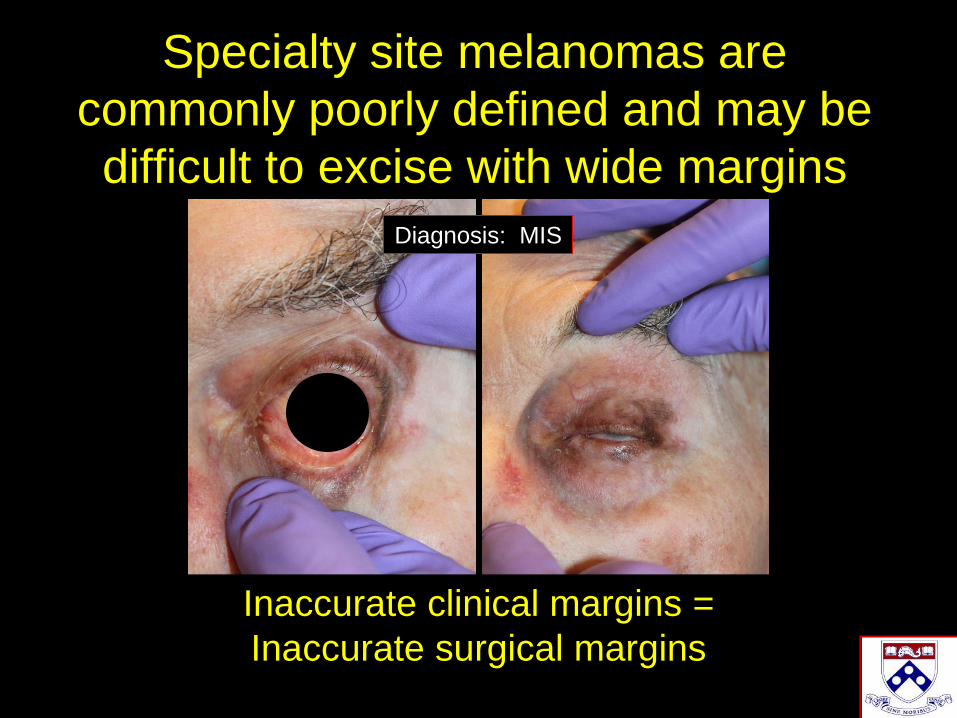
Specialty site melanomas are
commonly poorly defined and may be
difficult to excise with wide margins
Diagnosis: MIS
Inaccurate clinical margins =
Inaccurate surgical margins
1345 melanomas treated with
conventional WLE at Penn
Primary outcome:
Frequency of positive or equivocal margins
Miller CJ, Etzkorn JR et al. JAAD 2017;77:333-40

Predictors of positive margins on
conventional WLE
Risk factorOdds Ratio
(multivariate analysis
with step-wise
regression)
P-value
Non-compliance with recommended
margins5.57 0.002
Anatomic location on head, neck, hands,
feet, genitals, or pretibial leg5.07 <0.001
Histologic regression 2.78 0.007
Melanoma in situ 2.27 0.011
Multiple preoperative biopsies 1.92 (per biopsy) 0.004
Older age 1.049 (per year) <0.001
Miller CJ, Etzkorn JR et al. Risk factors for positive or equivocal margins after WLE of 1345 cutaneous
melanomas. JAAD 2017. Provisional acceptance 2/2017

Rates of positive margins after WLE
Non-compliant
surgical margins
Compliant
surgical margins
22.6%
(7/31)
3.2%
(41/1282)
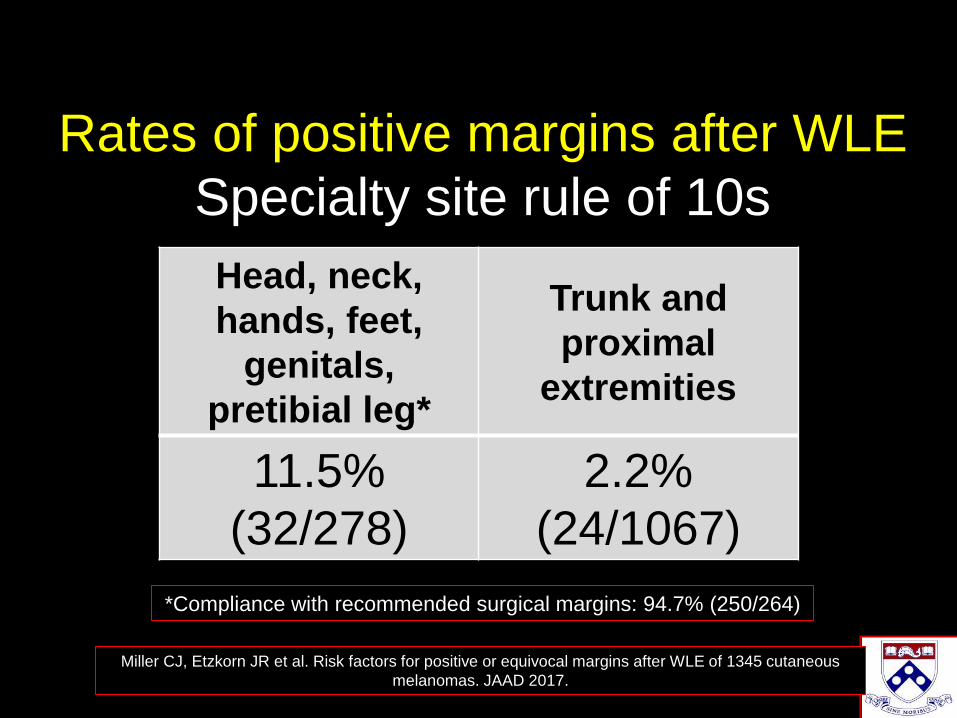
Rates of positive margins after WLE
Specialty site rule of 10s
Head, neck,
hands, feet,
genitals,
pretibial leg*
Trunk and
proximal
extremities
11.5%
(32/278)
2.2%
(24/1067)
Miller CJ, Etzkorn JR et al. Risk factors for positive or equivocal margins after WLE of 1345 cutaneous
melanomas. JAAD 2017.
*Compliance with recommended surgical margins: 94.7% (250/264)

Conventional Surgery
Rule of 10s>10% risk of
local recurrence
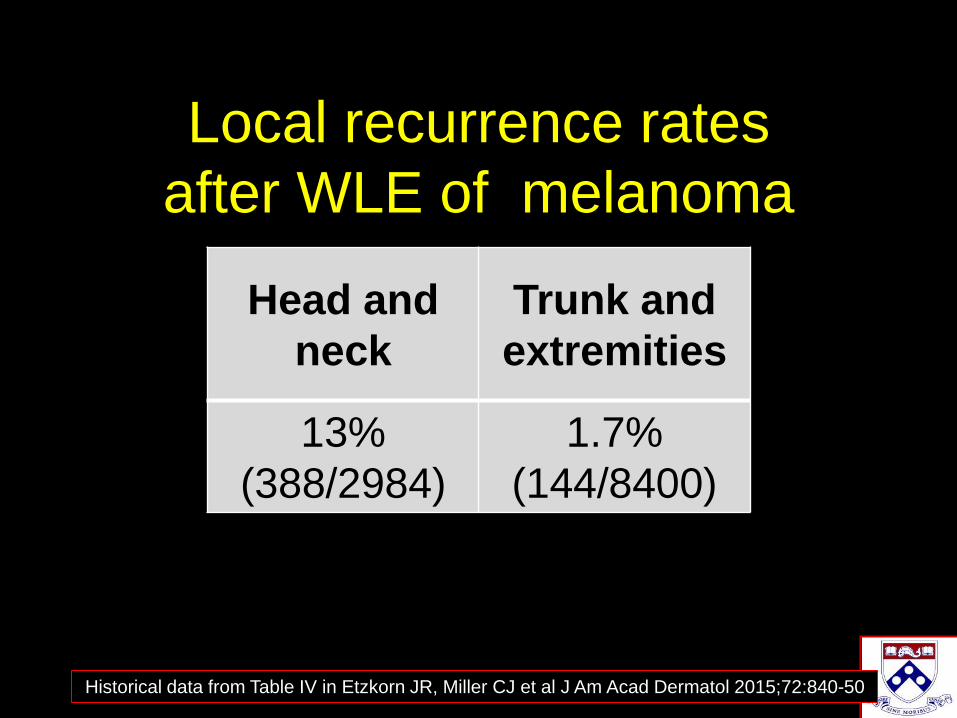
Local recurrence rates
after WLE of melanoma
Head and
neck
Trunk and
extremities
13%
(388/2984)
1.7%
(144/8400)
Historical data from Table IV in Etzkorn JR, Miller CJ et al J Am Acad Dermatol 2015;72:840-50
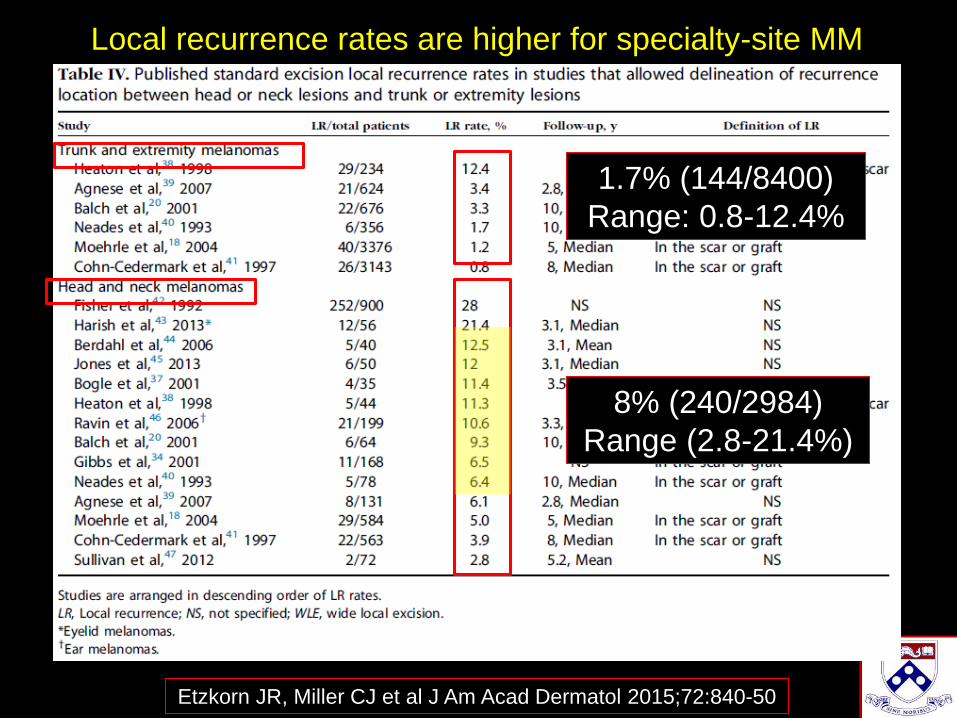
1.7% (144/8400)
Range: 0.8-12.4%
8% (240/2984)
Range (2.8-21.4%)
Etzkorn JR, Miller CJ et al J Am Acad Dermatol 2015;72:840-50
Local recurrence rates are higher for specialty-site MM

Rule of 10s10x increased likelihood of
complex reconstruction

10x greater likelihood of complex reconstruction
for specialty site melanomas
Anatomic
location
Frequency of
flap or graft
reconstruction
Odds Ratio
(95% CI)P-value
Specialty site 53.7% (275/512) 10.3 (4.86-21.8) 0.0001
Trunk and
proximal
extremity
10.1% (8/79) 1 (reference)
Etzkorn JR, Miller CJ et al. Dermatol Surg 2016;42:471-476

Previously treated melanomas are significantly
more likely to require more complex reconstruction
10/11/2011
Linear scar previous surgery
Final Mohs defect
4 stages
Etzkorn JR, Miller CJ et al. Dermatol Surg 2016;42:471-476
3 conditions for optimal surgery
of melanomas
• Accurate pathologic staging
prior to reconstruction
• Clear microscopic margins
• Reconstruction in tumor-free
skin
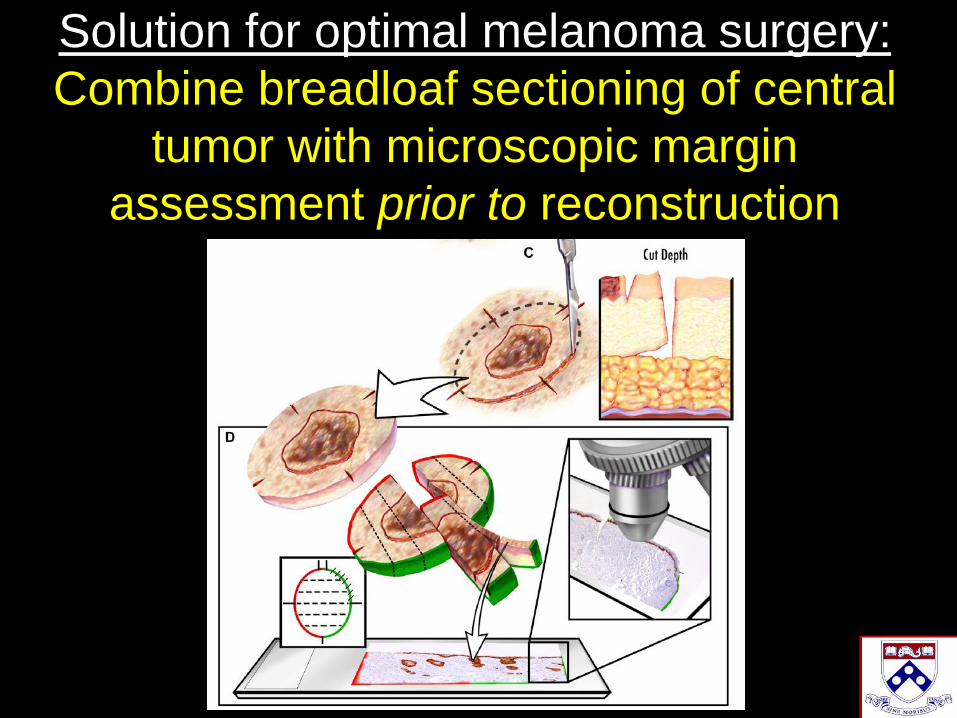
Solution for optimal melanoma surgery:
Combine breadloaf sectioning of central
tumor with microscopic margin
assessment prior to reconstruction
Numerous methods of margin control improve
surgical management of melanoma
• Mohs surgery
• Slow Mohs
• Square procedure
• Spaghetti technique
• Mapped serial excision
• Staged excision with radial sections
Table from Mayo K et al. Chapter 6. Staged Excision Techniques. In LMM. Springer 2016. Eds Nehal and Busam
Thank you to Drs. Zitelli and Brodland for
their pioneering work in Mohs for melanoma
J Am Acad Dermatol 2005;52:92-100
Dermatol Surg 2004;30:403-408
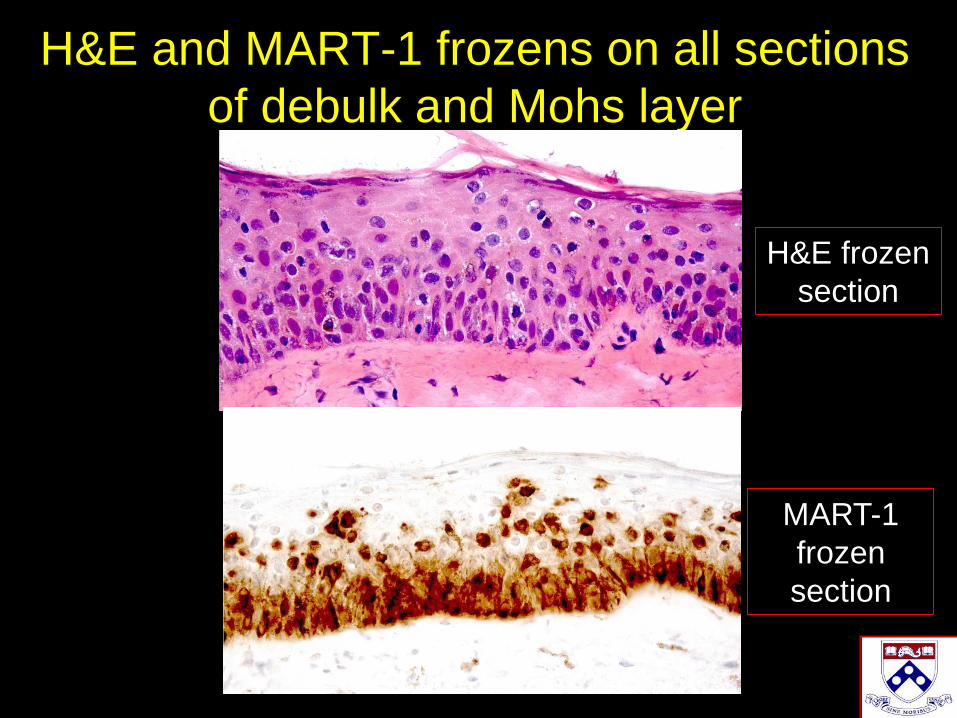
H&E and MART-1 frozens on all sections
of debulk and Mohs layer
H&E frozen
section
MART-1
frozen
section
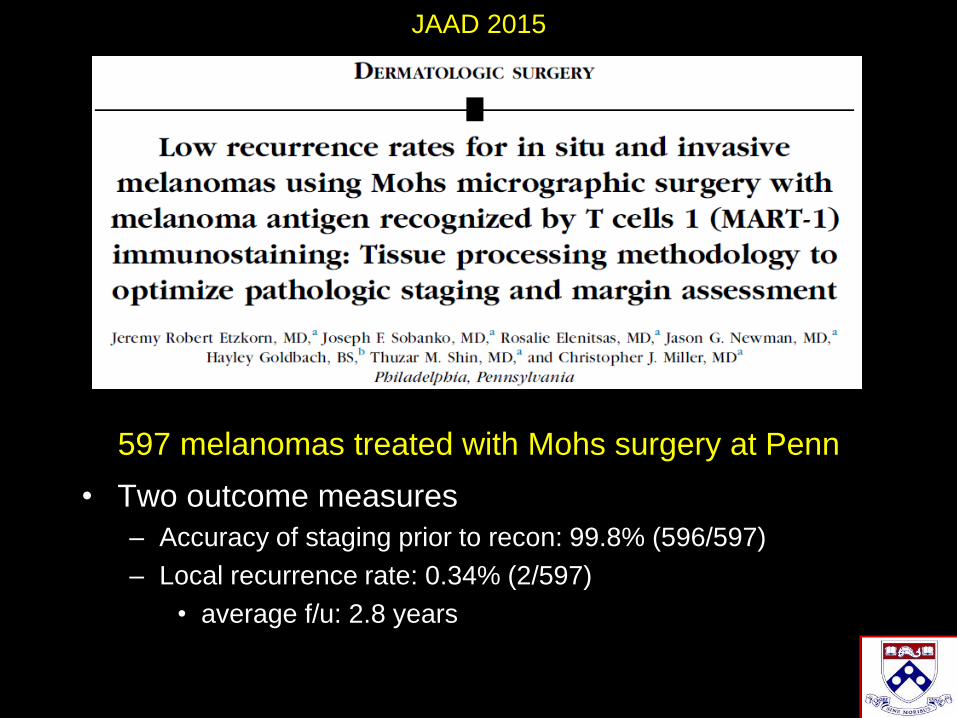
597 melanomas treated with Mohs surgery at Penn
• Two outcome measures
– Accuracy of staging prior to recon: 99.8% (596/597)
– Local recurrence rate: 0.34% (2/597)
• average f/u: 2.8 years
JAAD 2015
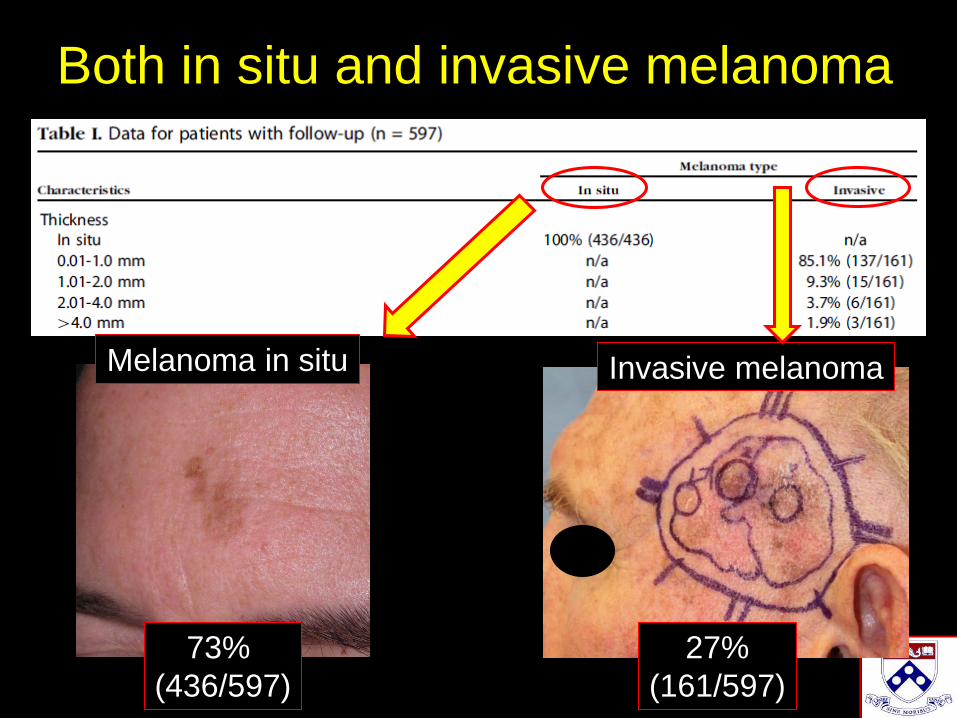
Both in situ and invasive melanoma
Melanoma in situ
73%
(436/597)
Invasive melanoma
27%
(161/597)
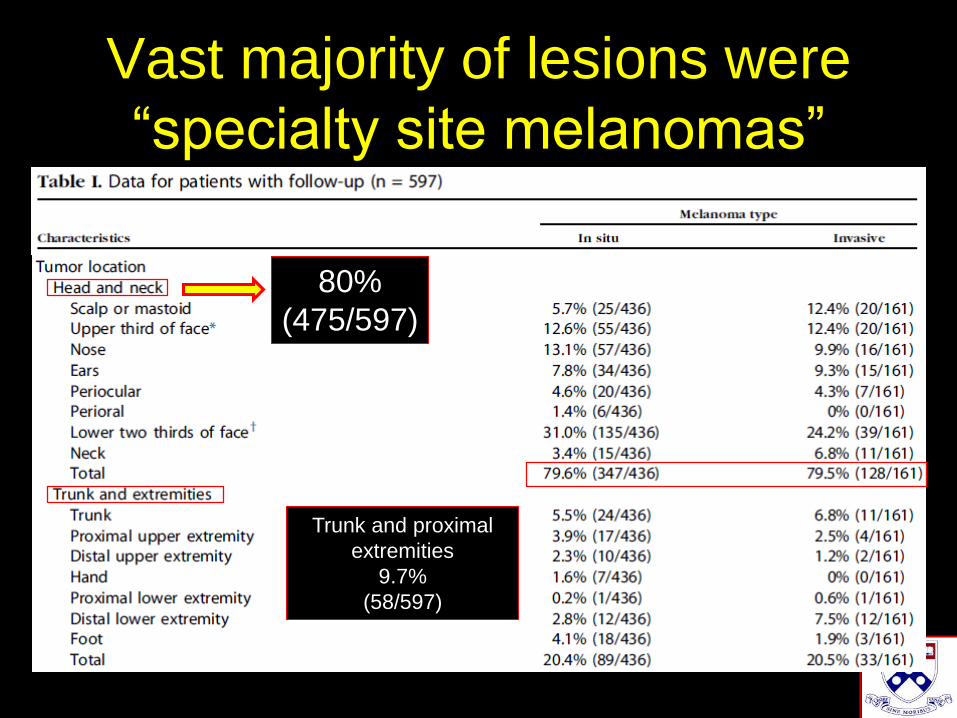
80%
(475/597)
Vast majority of lesions were
“specialty site melanomas”
Trunk and proximal
extremities
9.7%
(58/597)
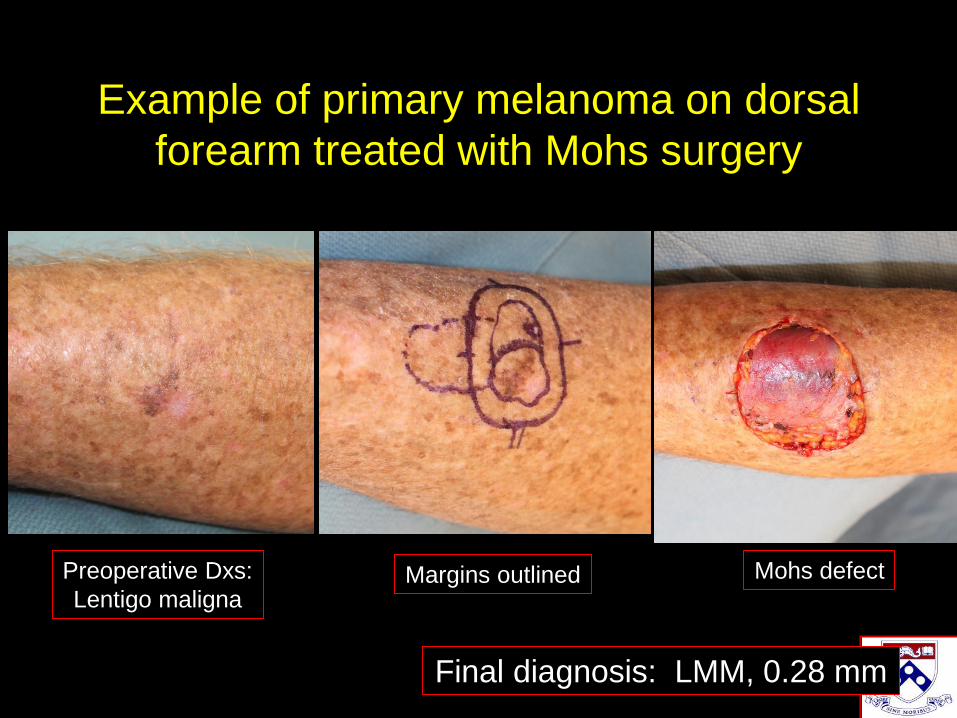
Example of primary melanoma on dorsal
forearm treated with Mohs surgery
Preoperative Dxs:
Lentigo malignaMargins outlined Mohs defect
Final diagnosis: LMM, 0.28 mm
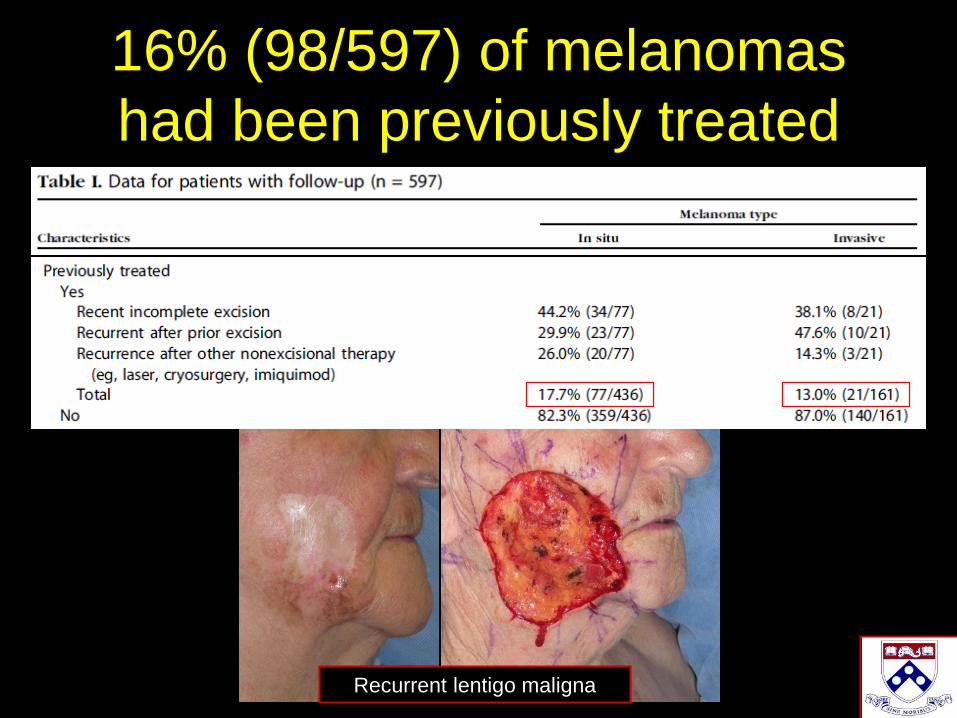
16% (98/597) of melanomas
had been previously treated
Recurrent lentigo maligna

Video of Mohs for Melanoma

Data show that we met 3 conditions for
optimal surgery of melanoma
• Accurate pathologic staging
prior to reconstruction
• Clear microscopic margins
• Reconstruction in tumor-free
skin
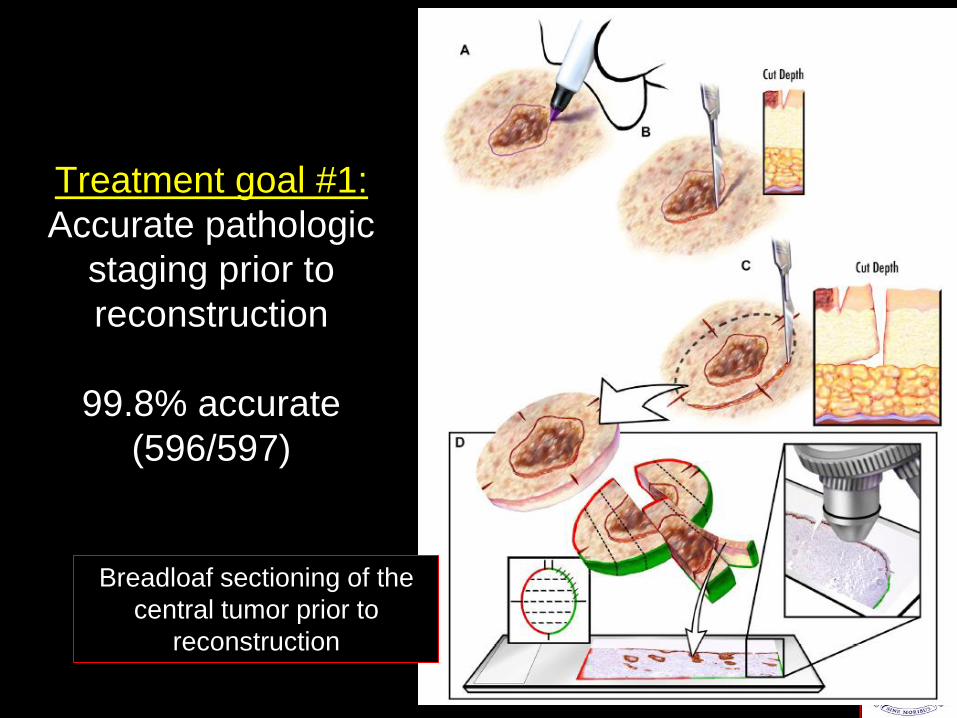
Treatment goal #1:
Accurate pathologic
staging prior to
reconstruction
99.8% accurate
(596/597)
Breadloaf sectioning of the
central tumor prior to
reconstruction

34/614 (5.5%) patients
upstaged AJCC T category
8
97% (33/34) detected by Mohs surgeon prior to reconstruction
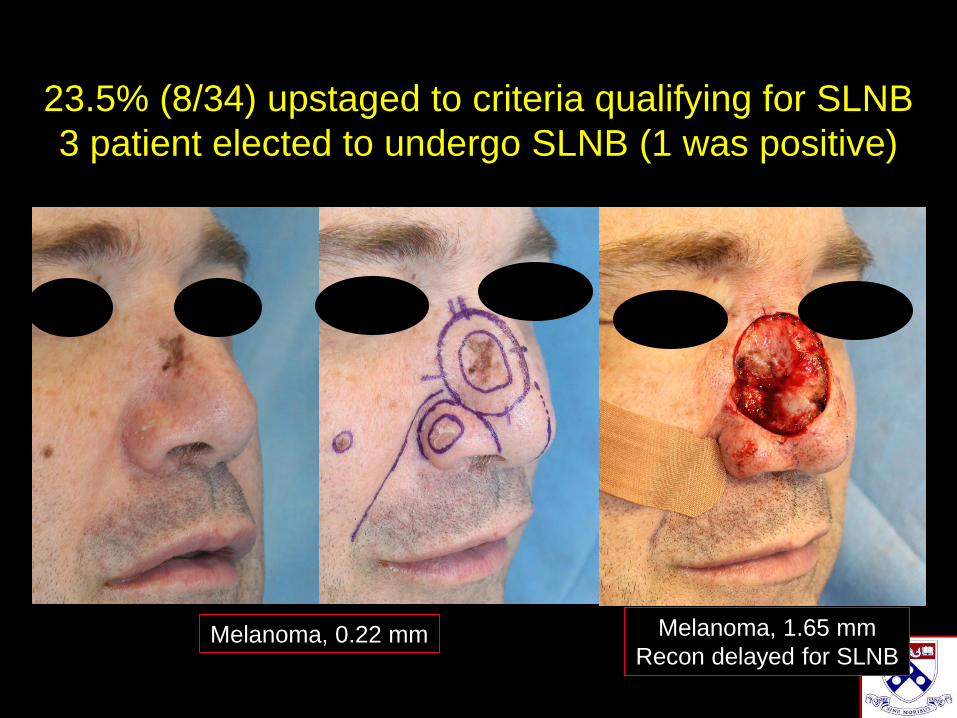
23.5% (8/34) upstaged to criteria qualifying for SLNB
3 patient elected to undergo SLNB (1 was positive)
Melanoma, 0.22 mm Melanoma, 1.65 mm
Recon delayed for SLNB
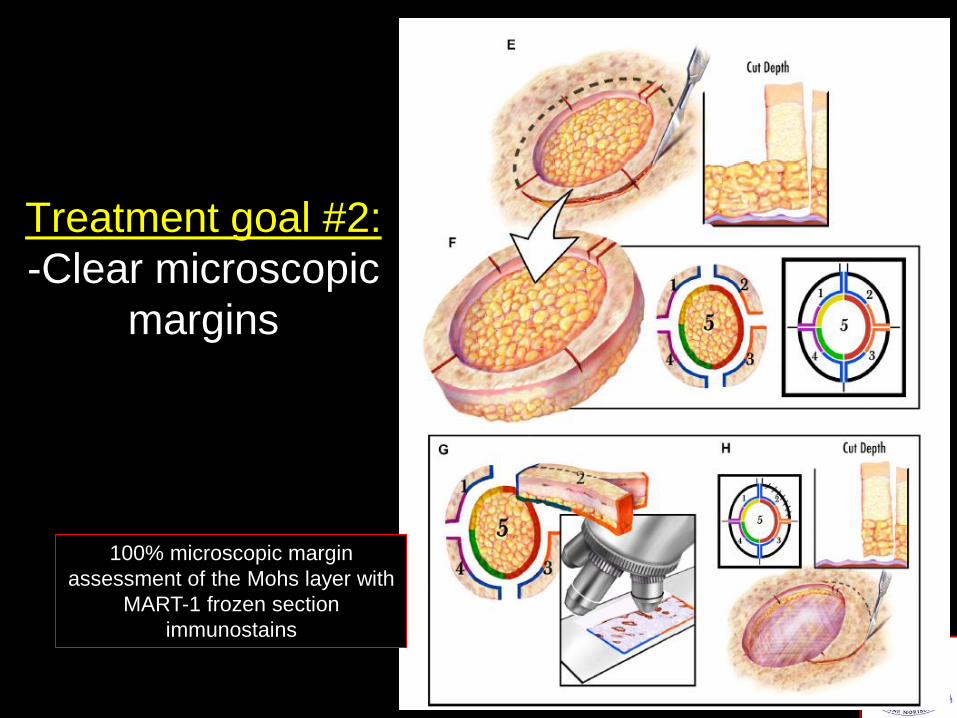
Treatment goal #2:
-Clear microscopic
margins
100% microscopic margin
assessment of the Mohs layer with
MART-1 frozen section
immunostains

Local recurrence rate
0.34% (2/597)
(Mean follow time: 2.8 years)
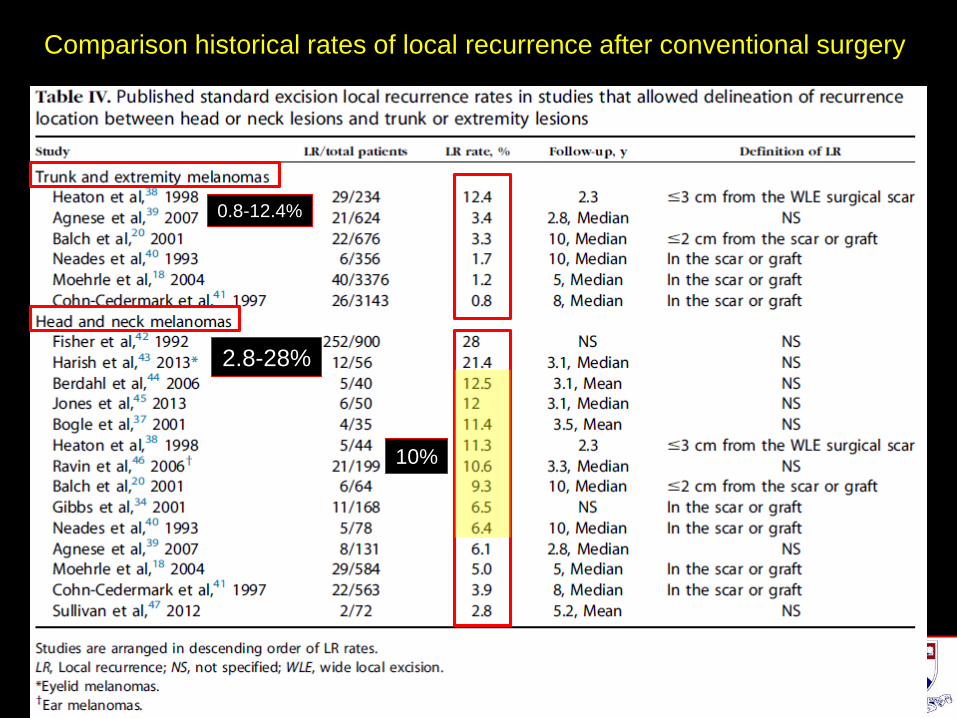
0.8-12.4%
2.8-28%
10%
Comparison historical rates of local recurrence after conventional surgery

Penn local recurrence rate
(published Penn data)
Estimated local
recurrence rate after
conventional surgery
(historical published data)
2/597 (0.34%) 60/597 (10%)

Treatment goal #3:
-Reconstruction in
tumor-free field
100% microscopic margin
assessment of the Mohs layer with
MART-1 frozen section
immunostains
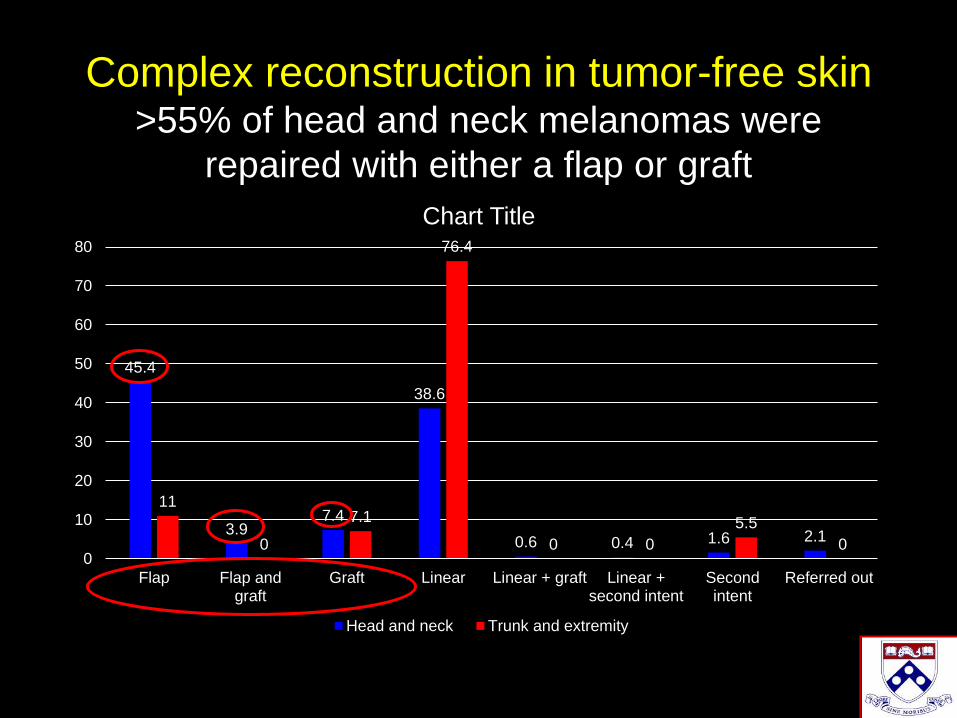
Complex reconstruction in tumor-free skin>55% of head and neck melanomas were
repaired with either a flap or graft
45.4
3.97.4
38.6
0.6 0.4 1.6 2.1
11
0
7.1
76.4
0 0
5.5
00
10
20
30
40
50
60
70
80
Flap Flap andgraft
Graft Linear Linear + graft Linear +second intent
Secondintent
Referred out
Chart Title
Head and neck Trunk and extremity
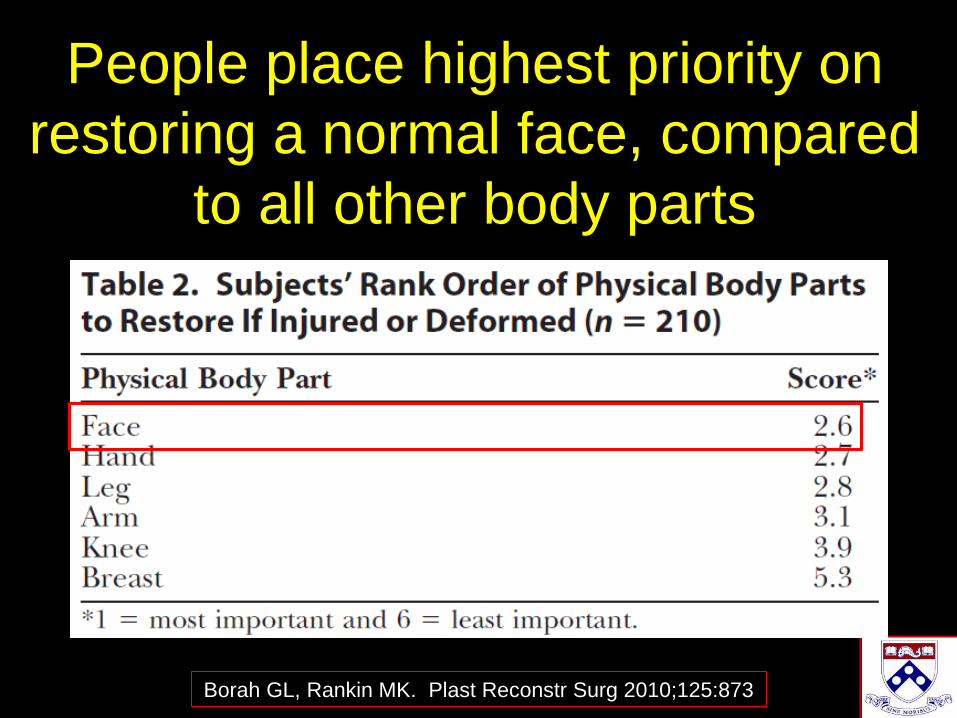
People place highest priority on
restoring a normal face, compared
to all other body parts
Borah GL, Rankin MK. Plast Reconstr Surg 2010;125:873
Outline
• Define the problem:
–Rule of 10s
• Define the solution:
–Microscopic margin-controlled
surgery before reconstruction