challenging scenarios in pv - normal” pregnancies successful pregnancies (surviving...
TRANSCRIPT

Jean-Jacques Kiladjian, MD, PhD Clinical Investigations Center
Saint-Louis Hospital – Paris Diderot University Paris, France
Challenging scenarios in PV
Disclosures for Jean-Jacques Kiladjian, MD, PhD
Royalty N/A
Receipt of intellectual property/ Patent holder
N/A
Consulting fee Novartis, Shire, AOP Orphan
Speakers bureau N/A
Fees for non-CME services N/A
Contracted research Novartis, AOP Orphan
Ownership interest (stocks, stock options)
N/A
Other N/A
N/A = Not Applicable (no conflicts listed) Presentation includes discussion of off-label or unapproved use of a drug or medical device

PREGNANCY IN PV

Clinical case
• 26-year-old woman
• Referred for thrombocytosis discovered during first pregnancy
• Severe complication during pregnancy: pre-eclampsia, IUGR, placental abruption, emergency cesarean delivery @ 6 months, baby died at D2
• No other significant medical or surgical history
• Asymptomatic, palpable splenomegaly 3 cm
• CBC: • WBC 17 G/L, 82% PMN
• Hemoglobin 16.2 g/dL, Ht 47%, MCV 86 fl
• Plt 818 G/L

Case n°1
• BCR-ABL1 negative; JAK2V617F positive
• Red cell mass: + 150%
• Erythropoietin: 2 U/L (low)
• Polycythemia Vera
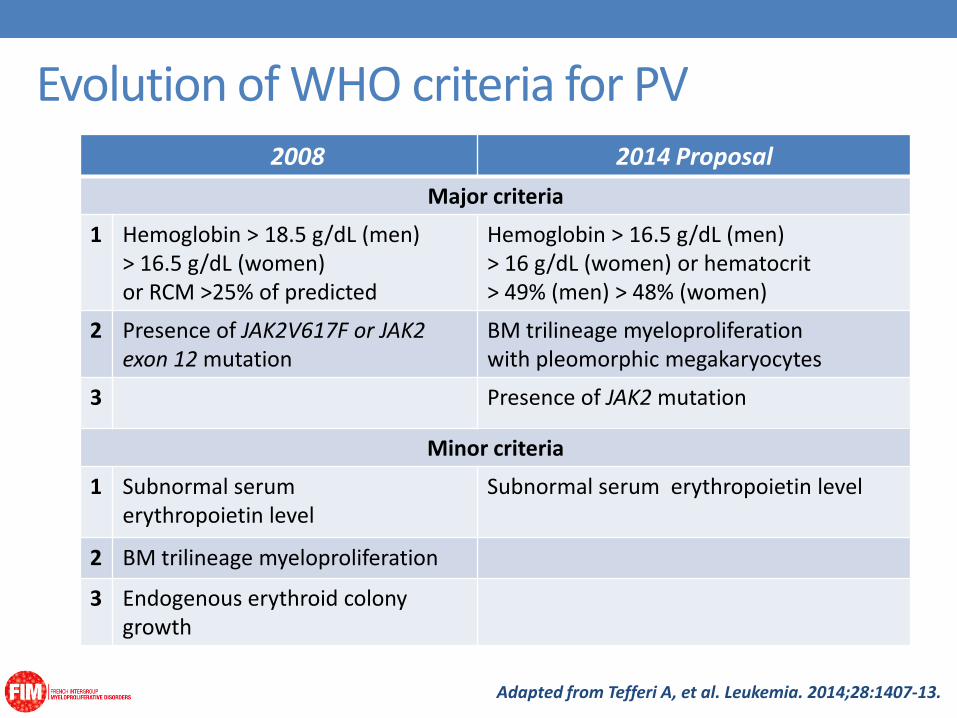
Evolution of WHO criteria for PV 2008 2014 Proposal
Major criteria
1 Hemoglobin > 18.5 g/dL (men) > 16.5 g/dL (women) or RCM >25% of predicted
Hemoglobin > 16.5 g/dL (men) > 16 g/dL (women) or hematocrit > 49% (men) > 48% (women)
2 Presence of JAK2V617F or JAK2 exon 12 mutation
BM trilineage myeloproliferation with pleomorphic megakaryocytes
3 Presence of JAK2 mutation
Minor criteria
1 Subnormal serum erythropoietin level
Subnormal serum erythropoietin level
2 BM trilineage myeloproliferation
3 Endogenous erythroid colony growth
Adapted from Tefferi A, et al. Leukemia. 2014;28:1407-13.
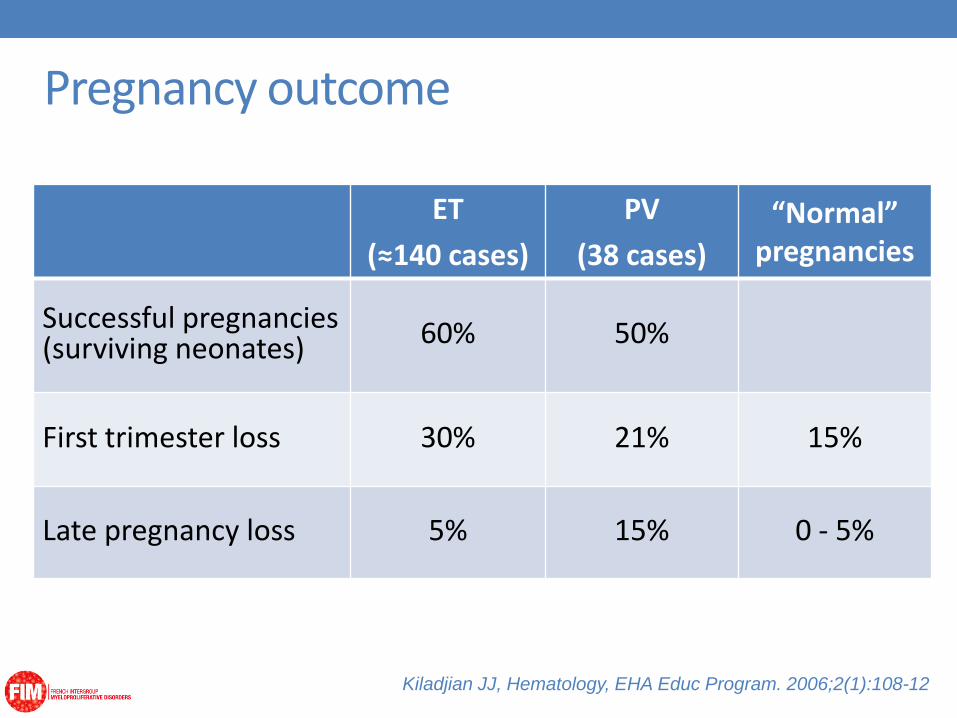
Pregnancy outcome
ET
(≈140 cases)
PV
(38 cases)
“Normal” pregnancies
Successful pregnancies (surviving neonates) 60% 50%
First trimester loss 30% 21% 15%
Late pregnancy loss 5% 15% 0 - 5%
Kiladjian JJ, Hematology, EHA Educ Program. 2006;2(1):108-12

Maternal complications
ET
(≈150 cases)
PV
(36 cases)
Major thrombosis 5% 8%
Major hemorrhage 3% 3%
Kiladjian JJ, Hematology, EHA Educ Program. 2006;2(1):108-12

Cytoreductive drugs & pregnancy
• None of the cytoreductive agents has product license for
use in pregnancy
• Risk factors used to decide cytoreduction in ET and PV are
modified or controversial during pregnancy
• Impact of cytoreductive treatment on pregnancy
outcome is controversial
• No evidence-based strategy

Cytoreductive drugs & pregnancy
Fertility Teratogenicity (animals)
Fetal toxicity in reported pregnancies
Hydroxyurea Reduced spermatogenesis yes
55 pregnancies 42 live births (4 IUD, 9 abortions) 1 malformation* Perez-Encinas, 1994 Harrison, 2005
Anagrelide Disrupted implantation
? (may cross placenta)
Interferon Reduced
spermatogenesis Decreased libido
no
23 pregnancies 1 malformation* Barbui, 2004
Robinson, 2005
*same pregnancy: HU at conception, IFN after 4 months

Aspirin • Low-dose aspirin is beneficial in PV (ECLAP)
• Low-dose aspirin is safe during pregnancy (CLASP)
• Is low-dose aspirin useful during pregnancy in MPN?
• No advantage: Wright & Tefferi, 2001 (43 cases)
• Advantage: Barbui, 2004 (245 cases)
Griesshammer, 2003 (155 cases)
Passamonti, 2009 (129 cases)
Low-dose aspirin should be used during MPN
pregnancy (unless contraindication or acquired vWD)
Landolfi R et al., N Engl J Med 2004; 350:114-24
CLASP, Lancet 1994; 343:619-29

Heparin
• LMW Heparin is safe and beneficial in pregnancies at high risk of
thrombosis
• LMWH was superior to aspirin in patients with thrombophilia
• Role of LMWH in MPN not clearly established
Hunt BJ et al., Thromb Haemost, 1997;77:39-43
Gris JC et al., Blood, 2004; 103:3695-9

Management - Before pregnancy
• Information of female patients of childbearing age
• Screening for thrombophilia recommended
• Start low-dose aspirin
• Patients on HU / anagrelide: gradually stop, > 3 months
wash-out period before conception
• Phlebotomy
• IFN if cytoreductive treatment is required
Management - During pregnancy
• Low-dose aspirin throughout pregnancy
• Consider IFN and prophylactic LMWH if:
• Previous major thrombosis or hemorrhage (pregnant or not)
• Platelet count > 1000 x 109/L
• Severe complication during previous pregnancy

Management - Delivery
• Stop aspirin 2 weeks before delivery, replaced
by prophylactic LMWH
• Stop LMWH 12 to 24 hours before delivery

Management - Puerperium
• Restart LMWH continued for at least 6 weeks
• Close monitoring of maternal blood counts (rebound)
• If cytoreduction is required, breastfeeding is
contraindicated

Conclusion - Pregnancy in PV
• Pregnancy is possible in PV patients
• But it should be considered and managed as a “high-
risk” pregnancy, like in other prothrombotic states
• Close collaboration between hematologists and
obstetricians is crucial
• Information of all MPD patients is essential to avoid
unanticipated pregnancy

SPLANCHNIC VEIN THROMBOSIS
Clinical case
• 25-year-old woman
• Admitted for abdominal pain
• Ascites, jaundice, hepatomegaly + 8 cm, splenomegaly + 10 cm
• Ultrasonography, then CT-scan: Budd-Chiari Syndrome
• CBC: • WBC 14 G/L, 82% PMN
• Hemoglobin 12 g/dL, MCV 72 fl
• Plt 390 G/L
• JAK2V617F positive
Diagnosed with MPN

Splanchnic vein thromboses
Hepatic veins Primary Budd-Chiari syndrome
Portal vein Acute: Pylephlebitis, Pylethrombosis Chronic: Portal cavernoma

BCS: Improved survival over 3 decades
Valla D-C. Gut 2008;57:1469-1478
Copyrighted material

Valla D-C. Gut 2008;57:1469-1478
Therapeutic strategy

Splanchnic vein thromboses
Hepatic veins/ Terminal IVC Primary Budd-Chiari syndrome
Portal vein Acute: Pylephlebitis, Pylethrombosis
Chronic: Portal cavernoma

Portal vein thrombosis
Bleeding Ascites MOF
Intestinal Ischemia
Uncomplicated Acute PVT
Abdominal Pain SIRS
Chronic PVT
Bleeding Encephalopathy
Collateral veins (cavernoma)
Portal hypertension

Prothrombotic diseases in BCS & PVT
Myeloproliferative neoplasms %
Antiphospholipid syndrome %
Inherited disorders %
Others (PNH, Behcet, IBD, …) %
Any of the above %
50 35
15 15
35 35
10 10
65 65
BCS PVT
From Janssen HL, et al. Blood 2000;96:2364-2368. Denninger MH, et al. Hepatology 2000;31:587-91.
Primignani M, et al Hepatology 2006;44:1528-34

V617F JAK2 + BMB +
V617F JAK2 - BMB +
V617F JAK2 - BMB -
V617F JAK2 + BMB -
25%
7%
12% 44%
(n=241) 0
%
100
56%
87%
Myeloproliferative neoplasms in SVT
No MPL515 No JAK2 exon 12

Myeloproliferative neoplasms in SVT
Smalberg J H et al. Blood 2012;120:4921-4928
MPL515: 3/305 tested cases (meta-analysis)
JAK2 exon 12: 0/268 tested cases (meta-analysis)
1 case report (Colaizzo, Blood 2007)
CALR: 4/209 (Turon et al., J Hepatol. 2014)
6/308 (French cohort, unpublished)

Myeloproliferative neoplasms in SVT
241 patients with SVT
JAK2V617F positive (n= 94)
JAK2V617F negative (n= 147)
P
Females 62% 48% 0.048
Splenomegaly (cm) 5 [0-11] 0 [0-2] <.001
Kiladjian JJ et al. Blood 2008; 111(10):4922-9

Myeloproliferative neoplasms in SVT
241 patients with SVT
JAK2V617F positive (n= 94)
JAK2V617F negative (n= 147)
P
Hemoglobin, g/dL 13.4 12.8 0.012
Hematocrit, % 43% 39% <.001
Neutrophils 5.2 3.7 <.001
Platelets 333 159 <.001
Kiladjian JJ et al. Blood 2008; 111(10):4922-9
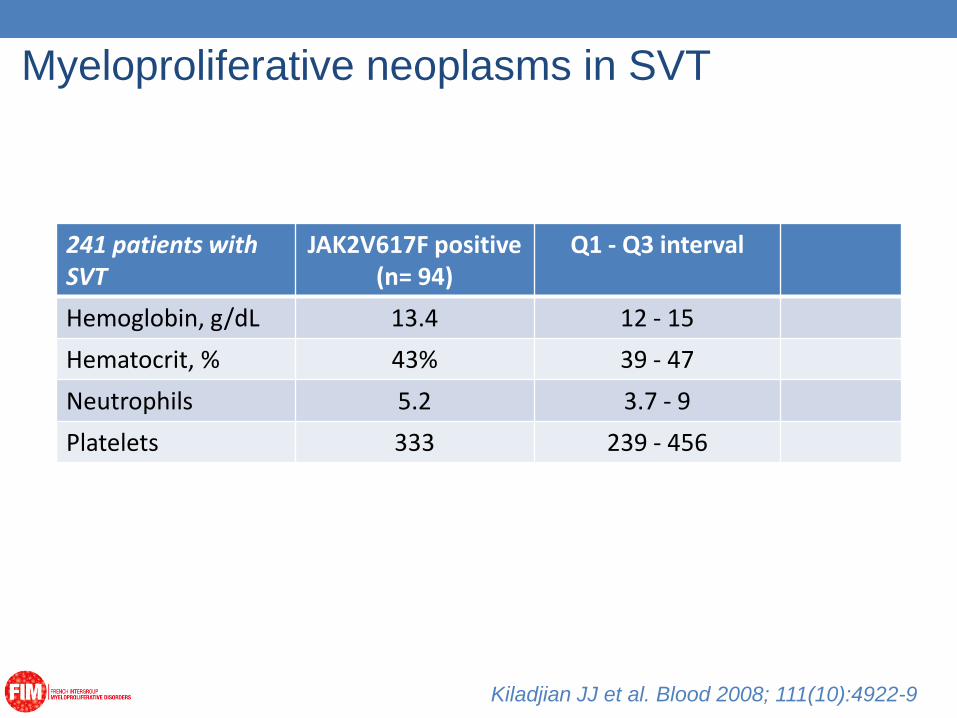
Myeloproliferative neoplasms in SVT
241 patients with SVT
JAK2V617F positive (n= 94)
Q1 - Q3 interval
Hemoglobin, g/dL 13.4 12 - 15
Hematocrit, % 43% 39 - 47
Neutrophils 5.2 3.7 - 9
Platelets 333 239 - 456
Kiladjian JJ et al. Blood 2008; 111(10):4922-9

Myeloproliferative neoplasms in SVT
241 patients with SVT
JAK2V617F positive (n= 94)
Q1 - Q3 interval
Hemoglobin, g/dL 13.4 12 - 15
Hematocrit, % 43% 39 - 47
Neutrophils 5.2 3.7 - 9
Platelets 333 239 - 456
RCM > 125% 61.3%
KiladjianJJ et al. Blood 2008; 111(10):4922-9

Myeloproliferative neoplasms in SVT
241 patients with SVT
JAK2V617F positive (n= 94)
JAK2V617F negative (n= 147)
P
APLS 14% 17% NS
F.V or F.II mutations 9.6% 11% NS
PC, PS, AT deficiency
10.5% 9.5% NS
Kiladjian JJ et al. Blood 2008; 111(10):4922-9

Myeloproliferative neoplasms in SVT:
Cytoreduction or Not?
• MPN with a history of thrombosis: high risk, indication for cytoreductive therapy
• But, the majority of patients have blood counts within the normal range…
• No definitive evidence for, or against, cytoreductive therapy in MPNs with SVT

Conclusion - MPN and SVT
• MPNs are the first cause of “idiopathic” SVT
• Additional prothrombotic states are found in 15%-30% of patients
• 80%-90% of these MPN are JAK2V617F positive, about 2% are CALR mutated and less than 1% display an MPL mutation
• The favorable impact of specific MPN therapy on overall outcome has not been demonstrated
INTOLERANCE TO HYDROXYUREA

Clinical case
• 64-year-old man diagnosed with PV at age 52
• Managed with phlebotomy alone for 8 years
• HU initiated due to increasing symptoms (pruritus) and frequency of phlebotomy to maintain Hct <45%
• Titrated HU to 1.5 g
• After 4 years, patient experienced leg ulcers
• HU discontinued following 8 months with problematic leg ulcer requiring visits to wound care
• How would you manage this patient’s PV?

• Therapy
“The choice of second-line myelosuppressive drugs for PV
should be carefully evaluated because some drugs
administered after hydroxyurea may enhance the risk of
acute leukemia”
Age, Vascular events Low risk High risk
Low dose aspirin
Age > 60 and/or
Vascular event
Cytoreduction
1st line: HU or IFNα
Management: 2011 ELN Recommendations
Barbui T, J Clin Oncol. 2011 Feb 20;29(6):761-70

• Second-line therapy
• Busulphan, and 32P are second-line therapies reserved for
patients with short life expectancy
• IFN alpha (off label)
Management: 2011 ELN Recommendations
Barbui T, J Clin Oncol. 2011 Feb 20;29(6):761-70

Advantages of IFNα in PV
Reduction of the MPN clone
Kiladjian JJ, Hematology Am Soc Hematol Educ Program. 2012;2012:561-6
M0 M12 M24 M36 M48 M60 M72
50%
100%
0
%V
61
7F

Reduction of the MPN clone
Clinical remissions without cytoreductive therapy
• 27% of patients in hematological CR off-therapy after
IFN discontinuation
Advantages of IFNα in PV
26% stopped for toxicity immune disorder (n=2, auto-Abs) allergy (n=2) neutropenia (n=1) after 9 months depression, fatigue (n=1) after 14 months peripheral neuropathy (n=1) after 12 months liver enzyme elevation (n=1) after 12 months arthralgia (n=1) after 27 months
Kiladjian JJ, Hematology Am Soc Hematol Educ Program. 2012;2012:561-6

Reduction of the MPN clone
Clinical remissions without cytoreductive therapy
Reduce incidence of vascular events?
Alter natural history of MPN?
clinical-hematological CR
molecular CR
histopathological CR
Advantages of IFNα in PV

peg-IFN-2a
Phase 2 (MPD-RC 111) ongoing
Phase 3 (MPD-RC 112) ongoing
Phase 3 in DK (DALIAH)
peg-IFN -2b (AOP 2014)
Phase 2 completed (PEGINVERA)
Phase 3 ongoing (PROUD-PV)
Ongoing studies of IFNα in PV

Ruxolitinib Proves Superior to Best Available Therapy in a Prospective, Randomized, Phase 3 Study (RESPONSE) in
Patients with Polycythemia Vera Resistant to or Intolerant Of Hydroxyurea
Alessandro M. Vannucchi,1 Jean-Jacques Kiladjian,2 Martin Griesshammer,3 Tamas Masszi,4 Simon Durrant,5 Francesco Passamonti,6 Claire N. Harrison,7 Fabrizio Pane,8 Pierre Zachee,9 Ruben Mesa,10 Shui He,11 Mark M.Jones,11 William
Garrett,11 Jingjin Li,12 Nathalie Francillard,13 Dany Habr,12 Srdan Verstovsek14
1University of Florence, Florence, Italy; 2Hôpital Saint-Louis et Université Paris Diderot, Paris, France; 3Johannes Wesling Clinic, Minden, Germany; 4St. István and St. László Hospital, Budapest, Hungary; 5Royal Brisbane & Women’s Hospital, Brisbane, Australia; 6Ospedale di Circolo e Fondazione Macchi,
Varese, Italy; 7Guy’s and St Thomas’ NHS Foundation Trust, London, UK; 8University of Naples Federico II, Naples, Italy; 9ZNA Stuivenberg, Antwerp, Belgium
10Mayo Clinic Cancer Center, Scottsdale, AZ, USA; 11Incyte Corporation, Wilmington, DE, USA; 12Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA; 13Novartis Pharma S.A.S., Rueil-Malmaison, France;
14The University of Texas MD Anderson Cancer Center, Houston, TX, USA
Vannucchi AM et al., EHA 2014 abst. LB2436

Conclusion – Second-line therapy
• There is no approved drug for second-line therapy in PV
• A concern for second-line therapy after HU is the cumulative
risk of leukemia with a second chemotherapy
• In patients intolerant or resistant to hydroxyurea, current
guidelines suggest the use of IFN-alpha
• However, there are some contra-indications and about 20% of
patients develop intolerance to IFN
• There is a need for new therapies, and ruxolitinib may be an
alternative second line therapy in selected patients