changing directions in diabetes
TRANSCRIPT

CHANGING DIRECTIONS IN DIABETES
Mark Thomas, Dept of Nephrology, RPH

The size of the problem

Micro and macrovascular disease

Oral Rx Insulin Rx
Too tight vs too loose control: oral Rx vs insulin
Currie, Lancet 2010
UK GP database 1986-2008: patients > 50yrs intensified from monotherapy to either oral combination (n= 28,000) or regimen inc insulin (n = 20,000)

Avoiding disaster

Multifactorial Rx in T2DM & legacy effect
Cumulative incidence of
any CV event (%)
STENO 2 TRIAL N Engl J Med 2008;358:580–591.
80
70
60
40
30
10
50
20
0
Conventional therapy
Intensive therapy
Years
0 1 2 3 4 5 6 7 8 9 10 12 1311
Trial: intensive vs conventional Post-trial: all intensive
53% reduction in CVD
N=160 T2DM microalbuminuria
Hazard ratio = 0.47 (95% CI, 0.24–0.73; p = 0.008)

CV events prevented by different interventions per 1000 patient yrs of treatment
Preiss D , and Ray K K BMJ 2011;343:bmj.d4243
Individualise and prioritise therapy targets
Individualise targets
� Tight targets: for young motivated compliant patients, short duration of DM, no micro/macrovascular disease, few co-morbidities
� Gentle targets : treat the elderly with respect
– E.g. Systolic BP 110 vs 140, HbA1c 6 vs 8%
Prioritise targets
1. BP and lipids: easier to achieve, bigger mortality benefit
2. Glucose control and weight loss
Deeper analysis
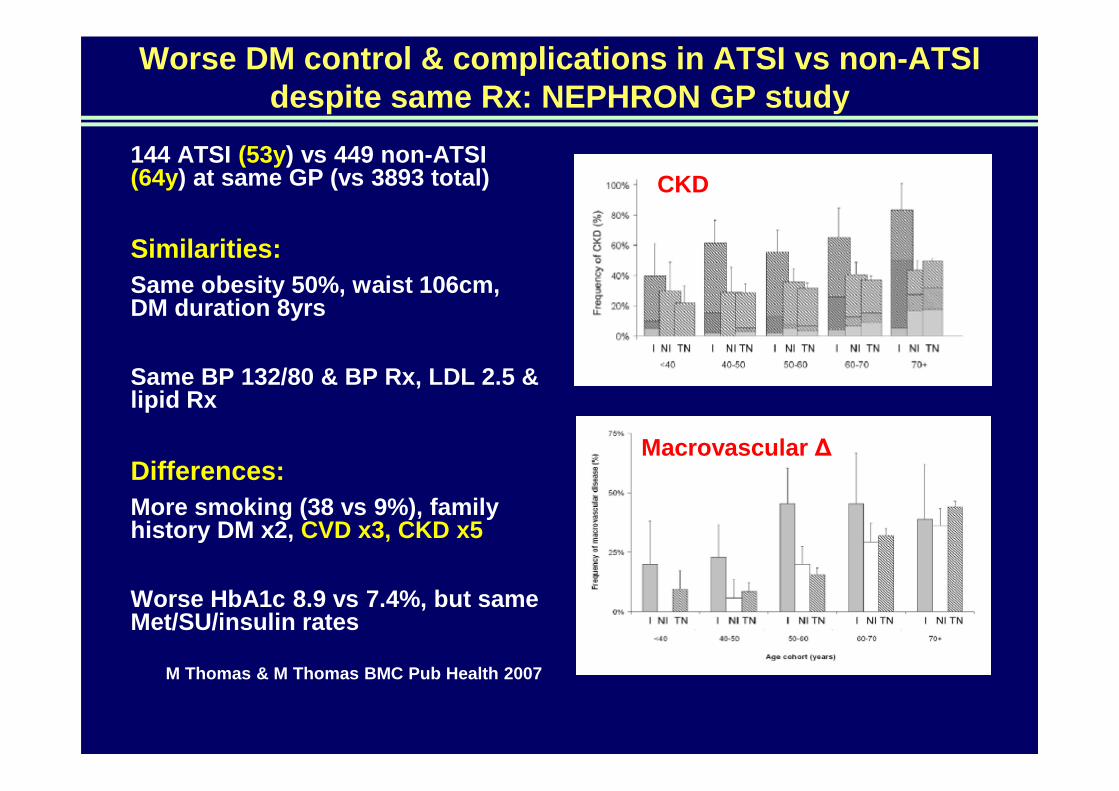
Worse DM control & complications in ATSI vs non-ATS I despite same Rx: NEPHRON GP study
144 ATSI (53y) vs 449 non-ATSI (64y) at same GP (vs 3893 total)
Similarities:Same obesity 50%, waist 106cm, DM duration 8yrs
Same BP 132/80 & BP Rx, LDL 2.5 & lipid Rx
Differences:More smoking (38 vs 9%), family history DM x2, CVD x3, CKD x5
Worse HbA1c 8.9 vs 7.4%, but same Met/SU/insulin rates
M Thomas & M Thomas BMC Pub Health 2007
CKD
Macrovascular ∆


Hoy e al. Nephrol 2016
ATSI ESKD: esp women in remote Qld

Missing factors in ATSI T2DM: chronic stress
Cause: Chronic stress
• Socio-economic
• Family health
Consequence: Cortisol
• Insomnia
• Constant hunger with central obesity
• Insulin resistance with acanthosis
• Resistant hypertension with relatively low K+
• Muscle weakness and fatigue
• Recurrent infectionsSchmitt & Spargo Bio Soc Sci 1995
Sweeter options
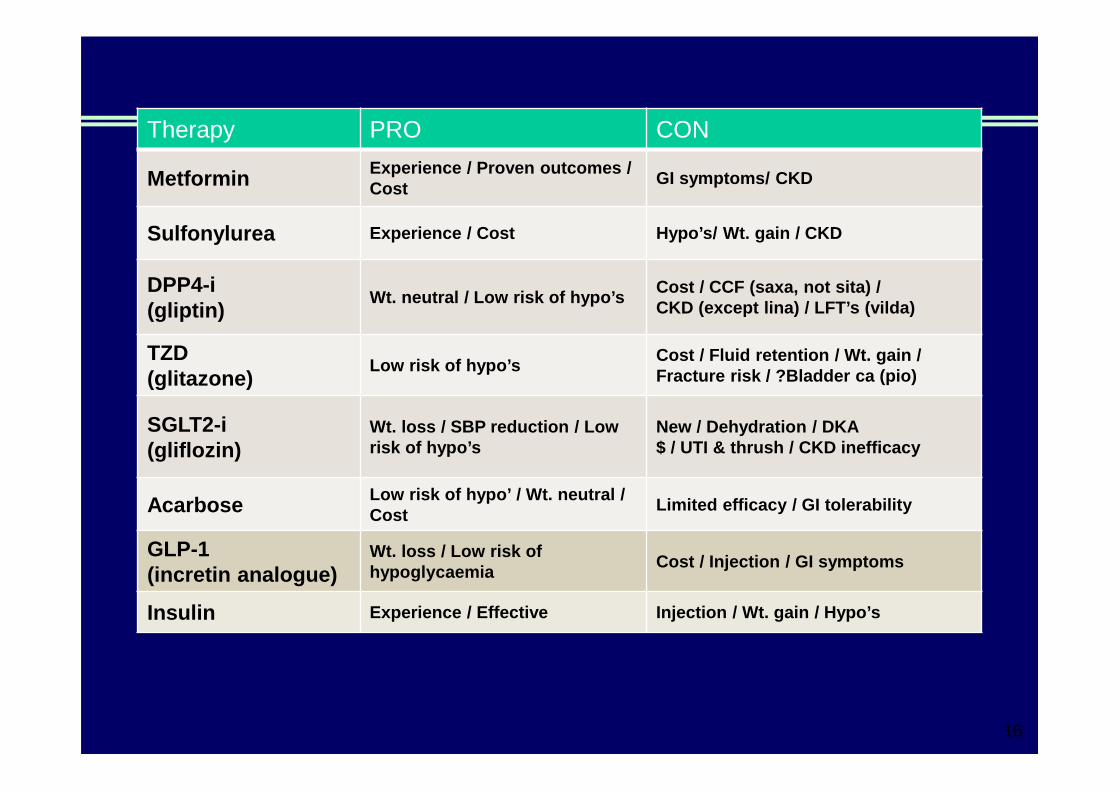
Therapy PRO CON
Metformin Experience / Proven outcomes / Cost
GI symptoms/ CKD
Sulfonylurea Experience / Cost Hypo’s/ Wt. gain / CKD
DPP4-i (gliptin)
Wt. neutral / Low risk of hypo’sCost / CCF (saxa, not sita) / CKD (except lina) / LFT’s (vilda)
TZD (glitazone)
Low risk of hypo’sCost / Fluid retention / Wt. gain / Fracture risk / ?Bladder ca (pio)
SGLT2-i (gliflozin)
Wt. loss / SBP reduction / Low risk of hypo’s
New / Dehydration / DKA$ / UTI & thrush / CKD inefficacy
Acarbose Low risk of hypo’ / Wt. neutral / Cost
Limited efficacy / GI tolerability
GLP-1 (incretin analogue)
Wt. loss / Low risk of hypoglycaemia
Cost / Injection / GI symptoms
Insulin Experience / Effective Injection / Wt. gain / Hypo’ s
16

Pathophysiology of Hyperglycaemia: missing 3?
Adapted from DeFronzo RA. Diabetes. 2009;58:773-795 .
Gut
Pancreas
Hyperglycaemia
Decreased Insulin SecretionIncreased Glucagon Secretion
DecreasedIncretin Effect
Muscle
DecreasedGlucose Uptake
17
Kidney
IncreasedGlucoseReabsorption
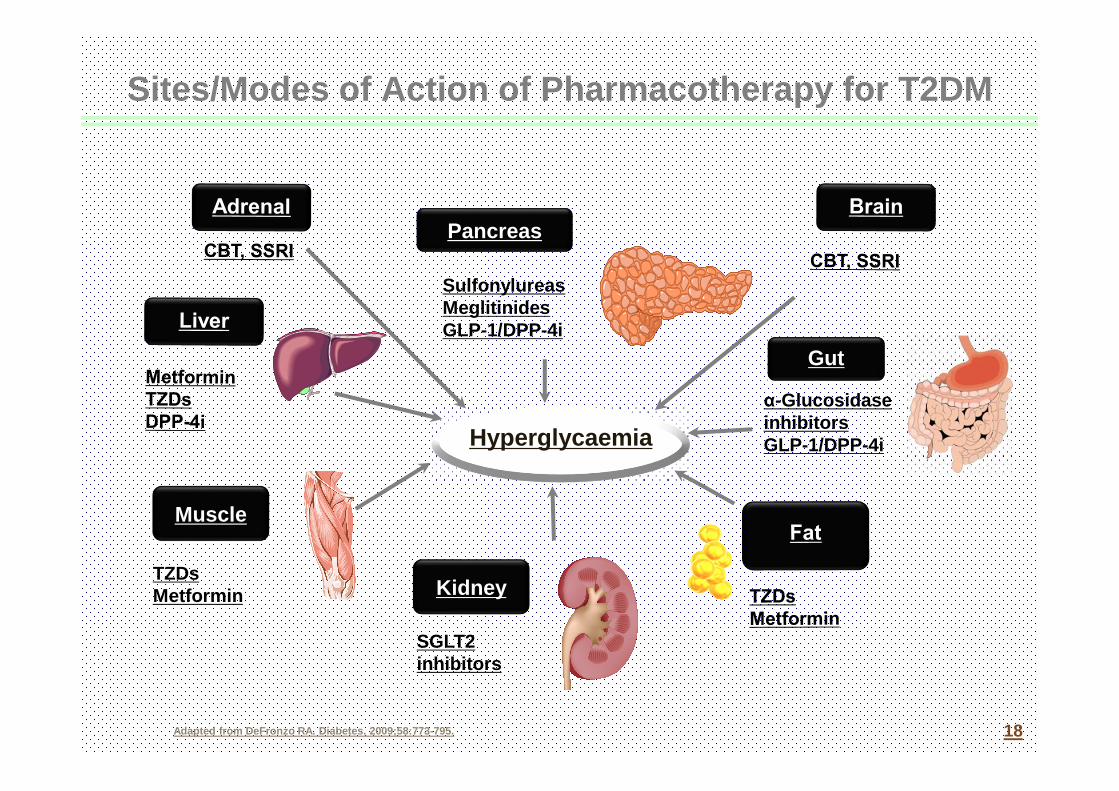
Sites/Modes of Action of Pharmacotherapy for T2DM
Adapted from DeFronzo RA. Diabetes. 2009;58:773-795 .
Gut
Pancreas
Hyperglycaemia
Muscle
TZDsMetformin
18
Kidney
SulfonylureasMeglitinidesGLP-1/DPP-4i
α-Glucosidase inhibitorsGLP-1/DPP-4i
SGLT2 inhibitors

Don’t beat up your beta-cells
Maintain beta-cell mass
� Avoid pancreatitis
� Tight BSL control
� Statins: ↓lipotoxicity
� Incretins: ↑proliferation, ↓apoptosis
� Glitazones: ↑proliferation, ↓apoptosis
� ACE-I/ARB: ↓ fibrosis
� ?Immunotherapy for Type I (rituximab 2009; anti IL-1 2013)
Reduce insulin demand
� Small meals with low glycaemic index
� Tight control
� Avoid high-dose SU’s
� Early insulin
Increase insulin sensitivity
� Increase exercise & muscle
� Reduce body fat mass & stress
� Use metformin +/- ?glitazones

50% of Australian Type 2 diabetics have CKD
10% GFR < 60 & normal uACR
25% ↑↑↑↑uACR & normal GFR
50% Either or both
NEPHRON study
MJA 2006; 185 (3): 140-144
uACR = spot urine albumin: creatinine ratio

Metformin in CKD
Dose-related GI side-effects
Renal excretion:
� Dose-adjust to GFR
Idiosyncratic lactic acidosis
Blocks liver glucose release & lactic acid uptake:
� Stop if unwell
Rates of lactic acidosis/10^5 patient-years:
� 57 (12-168) on metformin (n = 3)
� 28 (3-100) off metformin (n = 2), p = nsKamber, Davis et al. MJA 2008;188:446
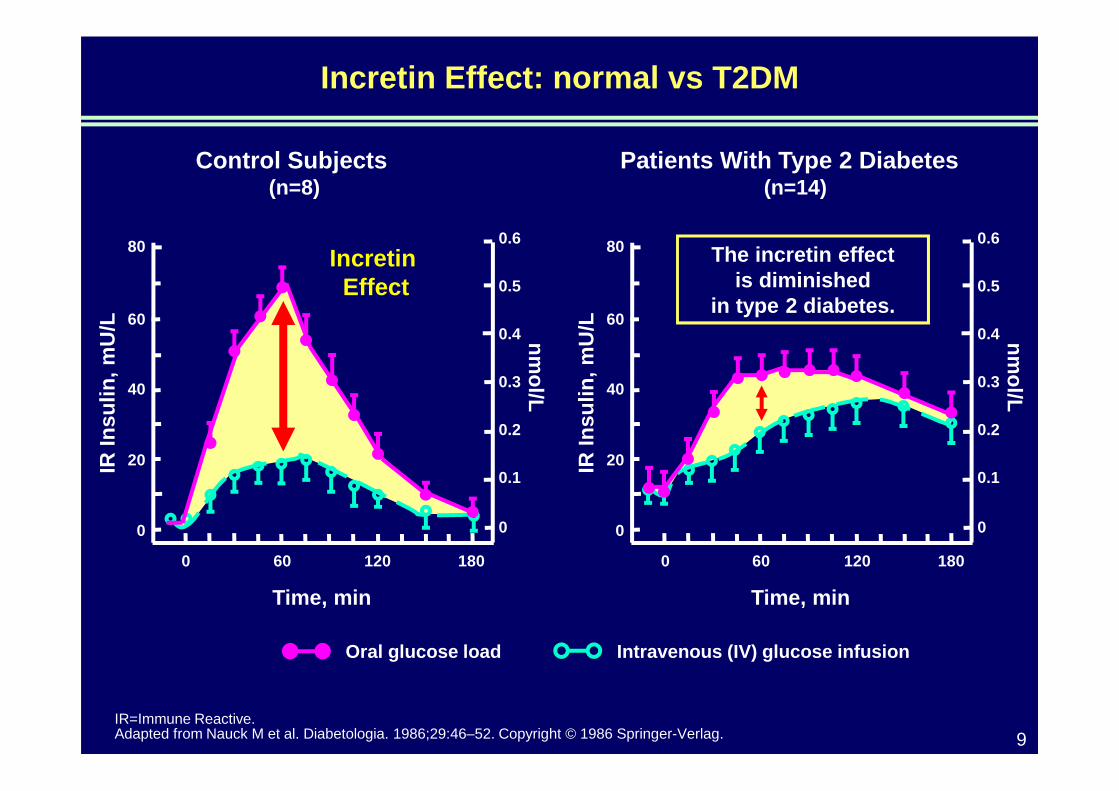
Incretin Effect: normal vs T2DM
IR=Immune Reactive.Adapted from Nauck M et al. Diabetologia. 1986;29:46–52. Copyright © 1986 Springer-Verlag. 9
Time, minIR
Insu
lin, m
U/L nm
ol/L
0.6
0.5
0.4
0.3
0.2
0.1
0
80
60
40
20
0
18060 1200
Control Subjects(n=8)
Patients With Type 2 Diabetes(n=14)
Time, min
IR In
sulin
, mU
/L nmol/L
0.6
0.5
0.4
0.3
0.2
0.1
0
80
60
40
20
0
18060 1200
Oral glucose load Intravenous (IV) glucose infusion
Incretin Effect
The incretin effect is diminished
in type 2 diabetes.

Effects of incretins and incretin-based therapy1
Adapted from DeFronzo RA, 20091
Reference 1. DeFronzo RA, Diabetes 2009; 58: 773-95.
Incretin effects are
enhanced by GLP-1
agonists and DPP-4
inhibitorsAlpha cells:
Reduction ofpostprandialglucagon secretion
Beta cells: Increase of glucose-dependent insulinsecretion
Liver: GlucagonReduceshepatic glucoseproduction
Stomach:Slowing of gastricemptying
GLP-1 secretion occurs after food intake

1yr Gliptin vs SU in CKD & ESKD
CKD ESKD
Number 426 129
HbA1c ∆ -0.8 v -0.6 -0.7 v -0.9
Hypo’s 6 v 17% 6 v 11%
Wt ∆ -0.6 v +1.2 -0.2 v +0.8
Other All equivCellulitis/headache
Ferreira et al Diabetes Care 2012 Am J Kidney Dis 2013

DPP4i safety – watch the BNP , not the lipase

BYDUREON Pen: Microsphere technology enables once-
weekly dosing1,2
Proven microsphere technology provides a continuous level of exenatide
� Biodegradable polymer that dissipates into CO2 and water
� Technology used in extended-release products, e.g. risperidone & naltrexone
Adapted from 1. DeYoung MB et al. 20111
Reference 1. DeYoung MB et al. Diabetes Technol Ther 2011;13:1145–54. 2. BYDUREON Approved Product Information.
Subcutaneous
injection of
microsphere
suspension of
exenatide
Individual
microspheres
aggregate and
initial release of
exenatide
Microsphere
degradation and
continued release of
exenatide
Further degradation
and metabolism of
microsphere polymer
provide sustained
level of exenatide

Exenatide QW Pharmacokinetics*
Pla
sma
Exe
natid
e C
once
ntra
tion
1 Steady state maintainedwith subsequent doses
• 2 mg single dose releases exenatide over 9-11 weeks 1
• Steady state concentrations reached by week 6-7 2
• Exenatide not detectable approximately10 weeks after last dose 1,2
0 2 4 6 8 10 12 14 16 18 20 22 24Weeks
PK/PD data does not necessarily predict clinical effect* Graphical representation of ExQW pharmacokinetics.Reference 1. Fineman, M et al. Clin Pharmacokinet. 2011;50(1):65-74; 2. BYDUREON Approved Product Information.

Effective FPG and PPG reduction1
Exenatide BID Week 14
Exenatide BID Baseline
Exenatide QW Week 14
Exenatide QW Baseline
-1 0 1 2 3 4 5
100
150
200
250
300
Time (h)
Glu
cose
(mg/
dL)
-1 0 1 2 3 4 5
100
150
200
250
300
Time (h)
Glu
cose
(mg/
dL)
Exenatide QW 2 mg1 Exenatide BID 10 µg1
*
Mean data;
*P = 0.0124 vs. exenatide QW
Reference 1. Drucker DJ, et al. Lancet 2008;372:1240-1250;
17
14
11
8
5

DURATION-2: BYDUREON vs sitagliptin or pioglitazone, on background metforminBYDUREON effective as first medication added to metformin1,2
Graph adapted from Wysham C, et al. 2011, showing data for the evaluable population as least squares mean ±
standard error.2
BL=baseline; CI=confidence interval.
Reference 1. Bergenstal RM, et al. Lancet 2010;376:431–9; 2. Wysham C, et al. Diabet Med 2011;28:705–14.
At the primary endpoint of 26 weeks, HbA1c changes from baseline were –1.5% with BYDUREON, –0.9%
with sitagliptin and –1.2% with pioglitazone (p<0.05 for BYDUREON vs both comparators)1
HbA1c reductions were sustained to week 52 throughout continued treatment with BYDUREON, or after
switching from sitagliptin or pioglitazone to BYDUREON at week 262
HbA1c Change from Week 26 to Week 52:Sitagliptin ����BYDUREON –0.31% (95 % CI, –0.50 to –0.13), P<0.05BYDUREON���� BYDUREON 0.06% (95 % CI, –0.13 to 0.25), P value not reportedPioglitazone ���� BYDUREON –0.10% (95 % CI, –0.29 to 0.09), P value not reported
Ch
an
ge
in
Hb
A1
c(%
)
Ch
an
ge
in H
bA
1c
from
ba
selin
e (m
mo
l/mo
l)
-0.5
-1.0
-1.5
-2.0
0
-5
-10
-15
-20
0.0
0 4 6 1
0
1
4
1
8
2
2
2
6
3
0
3
4
4
0
4
6
5
2Time (weeks) BYDUREON, BL=8.6% (70.5 mmol/mol)
Sitagliptin ���� BYDUREON, BL=8.5% (69.4 mmol/mol)
Pioglitazone ���� BYDUREON, BL=8.5% (69.4 mmol/mol)

DURATION-3: BYDUREON vs insulin glargine
HbA1c improvement with BYDUREON vs insulin sustained for 3 years1
Modified from Diamant M, et al. 2014.1
*The daily dose of insulin glargine was based on the INITIATE algorithm (Initiate Insulin by Aggressive Titration and Education) and was individually
adjusted to achieve fasting glucose values of 4.0–5.5 mmol/l.
In the Insulin glargine arm, from a starting daily insulin dose of 10IU/day, mean dose increased to approximately 31 IU/day at 26 weeks.
Background therapy: Metformin with or without sulfonylurea.
Reference 1. Diamant M, et al. Lancet Diabetes Endocrinol 2014; 2:464-73.
8.5
8.0
7.5
7.0
6.5
Hb
A1
c(%
)
Insulin glargine (n=220)Once daily, variable dose based on treat-to-target algorithm*
Exenatide QW (n=228)2 mg once weekly
Time (weeks)
0 3
6
8 13
2
1
8
2
6
4
8
6
0
7
2
8
4
9
6
1
0
8
12
0
14
4
15
6
Δ -0.20 %
p=0.03

Weight in DURATION studies: Overview*1–5
Modified from Bergenstal RM, et al 20101.
Reference 1. Bergenstal RM, et al. Lancet 2010; 376:431-9; 2. Drucker DJ, et al. Lancet 2008; 372:1240-50; 3. Blevins T, et al. J Clin Endocrinol Metab 2011; 96:1301-10;
4. Buse JB, et al. Lancet 2013; 381:117-24; 5. Diamant M, et al. Lancet 2010; 375:2234-43.
††BYDUREON did not meet primary endpoint of non-inf eriority vs 1.8mg liraglutide (upper limit of CI <0.25%) in DURATION-6. 4
æBYDUREON is not indicated for use in combination wi th TZDs
*BYDUREON is not indicated for weight loss.

DURATION-3: BYDUREON vs insulin glargine
Weight change over 3 years1,2
Graph adapted from Diamant M, et al. 2014, showing data for the modified intent-to-treat population as least squares mean ± standard
error.1 *p<0.001.
BL=baseline.
Reference 1. Diamant M, et al. Lancet Diabetes Endocrinol 2014;2:464–73; 2. BYDUREON Approved Product Information.
Treatment with Bydureon resulted in significant weight reduction compared to
weight gain with insulin glargine over 3 years1*
4
2
0
-2
-4
Ch
an
ge
in
bo
dy
we
igh
t (k
g)
Insulin glargine, BL=90.6 kg (n=222)
Bydureon, BL=91.2 kg (n=233)
Time (weeks)
0 3
6
8 13
2
1
8
2
6
4
8
6
0
7
2
8
4
9
6
1
0
8
12
0
14
4
15
6
Change from BL:+2.01 ± 0.28 kg
–2.49 ± 0.28 kg*
*BYDUREON is not indicated for weight loss. 2
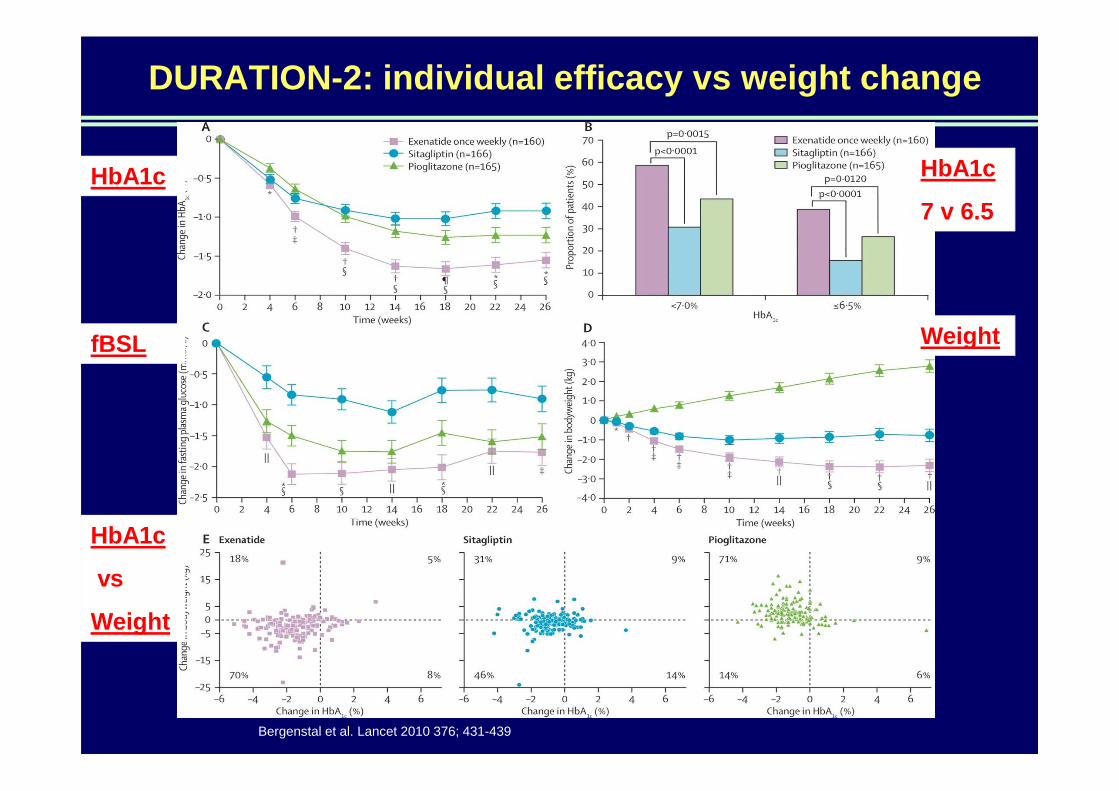
DURATION-2: individual efficacy vs weight change
Bergenstal et al. Lancet 2010 376; 431-439
HbA1c HbA1c
7 v 6.5
WeightfBSL
HbA1c
vs
Weight

Less nausea with BYDUREON vs. exenatide bdæ1–3
Patients administered exenatide or liraglutide with background therapy.
Adapted from BYDUREON Approved Product Information1 and Buse et al. 2013.4
Reference 1. BYDUREON Approved Product Information. 2. Drucker DJ et al. Lancet 2006; 368:1696–1705. 3. Blevins T
et al. DURATION-5. J Clin Endocrinol Metab 2011; 96:1301–1310. 4. Buse JB et al. DURATION-6. Lancet 2013;
381(9861):117–124.
� Withdrawal due to nausea or vomiting each occurred in ≈1% of BYDUREON-treated patients1
� Most episodes of nausea were mild to moderate1
BYDUREN associated with less nausea compared to exenatide BD or 1.8mg liraglutideæ‡1–4
‡BYDUREON did not meet primary endpoint of non-infer iority vs 1.8mg liraglutide (upper limit of CI <0.25%) in DURATION-6. 4
æStatistical significance not tested.

� Mostly mild to moderate
� Usually did not lead to withdrawal from
studies
� Injection site reactions were higher in
exenatide once weekly treated patients (16%)
compared exenatide BD treated patients (2%-
7%): pruritus (8%), erythema (4%),
induration (4%) and nodule (3%).
� Asymptomatic nodule formation (up to 77%).
Approximately 73% of the first incidence of
treatment emergent injection site reactions
resolved within 60 days.
Injection-site
Reference 1. BYDUREON Approved Product Information. 2. DeYoung MB et al. Diabetes Technol Ther 2011; 13: 1145-54.
� Small, raised nodules very frequently occur at
the injection site
– Consistent with known properties of
poly (D,L-lactide co-glycolide) polymer
microsphere technology
� Most individual nodules were asymptomatic
and resolved over 4-8 weeks
Injection-site reactions Injection-site bumps
Size of bump
Bump
BYDUREON: Summary of safety and tolerability profile
As with other GLP-1 receptor agonists,1–4 the most frequent adverse drug
reactions (≥5% of patients treated with BYDUREON) were mainly gastrointestinal-
related (nausea, vomiting, diarrhoea and constipation)
In addition, injection-site reactions (pruritus, nodules, erythema, induration),
hypoglycaemia (with a SU) and headache occurred1
Most adverse reactions associated with BYDUREON were mild to moderate in
intensity1
There have been rare, spontaneously reported events of acute pancreatitis and
renal failure. If pancreatitis is suspected, BYDUREON should be discontinued1
Data source comprises 5 trials comparing 2 mg exenatide once weekly to either 10 μg exenatide twice daily (a 30 week study), sitagliptin
and pioglitazone (a 26 week study), and insulin glargine (a 26 week study). Background therapies included diet and exercise and oral anti-
diabetic agents.
BD=twice daily; SU=sulphonylurea; TZD=thiazolidinedione.
Reference 1. BYDUREON Approved product Information. 2. BYETTA Approved product Information. 3. VICTOZA Approved product
Information. 4. LYXUMIA Approved product Information.

PBS listing
Dual combination therapy with
metformin OR a sulfonylurea
Authority Required (STREAMLINED) 6354
Clinical Criteria:
The treatment must be in combination with metformin; OR
the treatment must be in combination with a sulfonylurea
AND
Patient must have a contraindication to a combination of
metformin and a sulfonylurea; OR patient must not have
tolerated a combination of metformin and a sulfonylurea
AND
Patient must have, or have had, a HbA1c measurement
greater than 7% prior to the initiation of a dipeptidyl
peptidase 4 inhibitor (gliptin), a thiazolidinedione
(glitazone), a glucagon-like-peptide-1 or a sodium-glucose
co-transporter 2 (SGLT2) inhibitor despite treatment with
either metformin or a sulfonylurea.
Triple combination therapy with
metformin AND a sulfonylurea
Authority Required (STREAMLINED) 6339
Clinical Criteria:
The treatment must be in combination with metformin
AND
The treatment must be in combination with a sulfonylurea
AND
Patient must have, or have had, a HbA1c measurement greater
than 7% prior to the initiation of a dipeptidyl peptidase 4
inhibitor (gliptin), a thiazolidinedione (glitazone), a glucagon-
like-peptide-1 or a sodium-glucose co- transporter 2 (SGLT2)
inhibitor despite treatment with maximally tolerated doses of
metformin and a sulfonylurea.

BYDUREON PEN: SUMMARY
� BYDUREON is the first approved once weekly GLP-1 re ceptor agonist
� HbA 1c reductions are sustained for up to 6 years vs basel ine †2
� Potential for weight reduction over 6 years vs base line * and low risk of hypoglycaemia ††1,2
� Most common adverse events: gastrointestinal (nause a, diarrhoea, vomiting, constipation), nasopharyngitis, hypoglycae mia, injection site reactions (pruritus, nodules, erythema, indurat ion) 1
†Open-label, uncontrolled extension study in patients administered BYDUREON with background therapy. 43% of patients
remained in the study at Year 6.
*BYDUREON is not indicated for weight loss.1
††SUs are associated with an increased risk of hypoglycaemia. When BYDUREON is added to SU therapy, a reduction in the dose
of SU should be considered to reduce the risk of hypoglycaemia.1
Reference 1. BYDUREON Approved Product Information. 2. Henry RH, et al. Poster presented at ADA 2014. 964-P
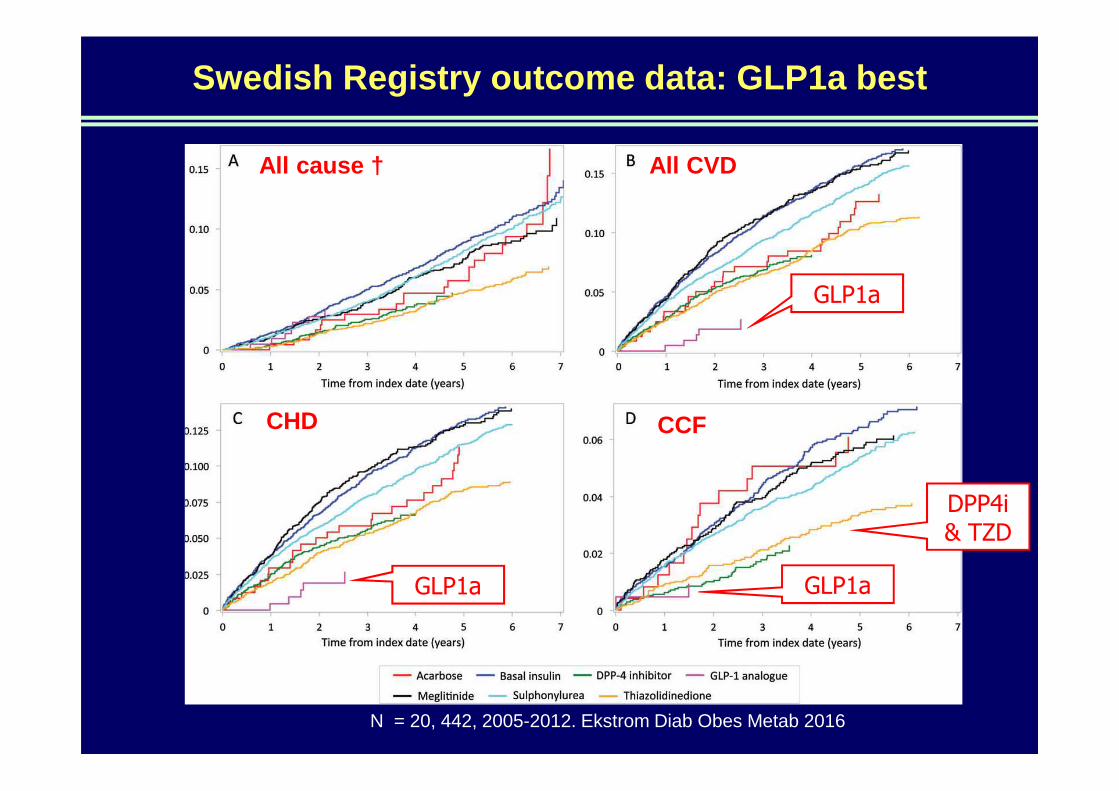
Swedish Registry outcome data: GLP1a best
All cause † All CVD
CHD CCF
GLP1a
GLP1a GLP1a
DPP4i & TZD
N = 20, 442, 2005-2012. Ekstrom Diab Obes Metab 2016

GLP1 analogue & CV outcome RCT
N = 9340, >50yr & CV factor, 3.8yr f/up, no DPP4i Primary EP = 3-pt MACE: 13.0 vs 14.9%, HR 0.87, p<0.001
Marso, NEJM 2016

New arrivals
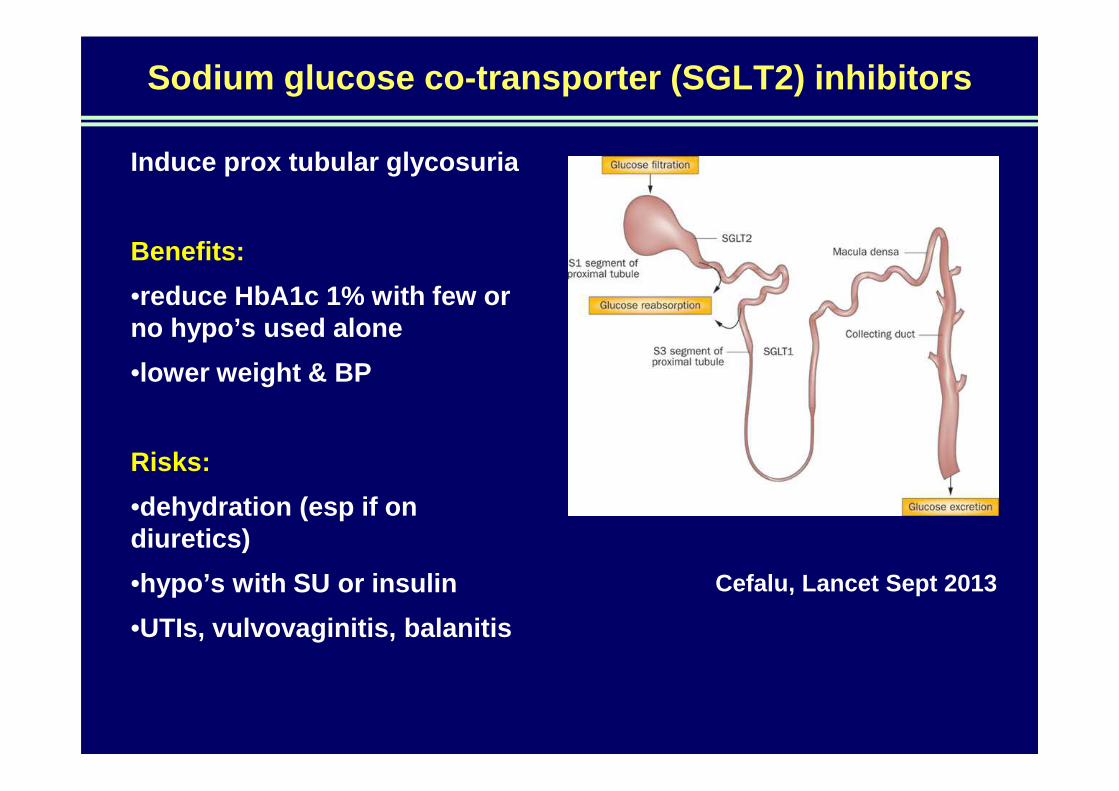
Sodium glucose co-transporter (SGLT2) inhibitors
Induce prox tubular glycosuria
Benefits:
•reduce HbA1c 1% with few or no hypo’s used alone
•lower weight & BP
Risks:
•dehydration (esp if on diuretics)
•hypo’s with SU or insulin
•UTIs, vulvovaginitis, balanitis
Cefalu, Lancet Sept 2013

↓GFR →↑retention but ↓efficacy
Kasichayanulaet al, Dapagliflozin
pharmacokinetics in moderate and
severe CKD, BJCP 2012
50mg stat
20mg 1 week
AUC
20mg 1 week
uGluc
loss
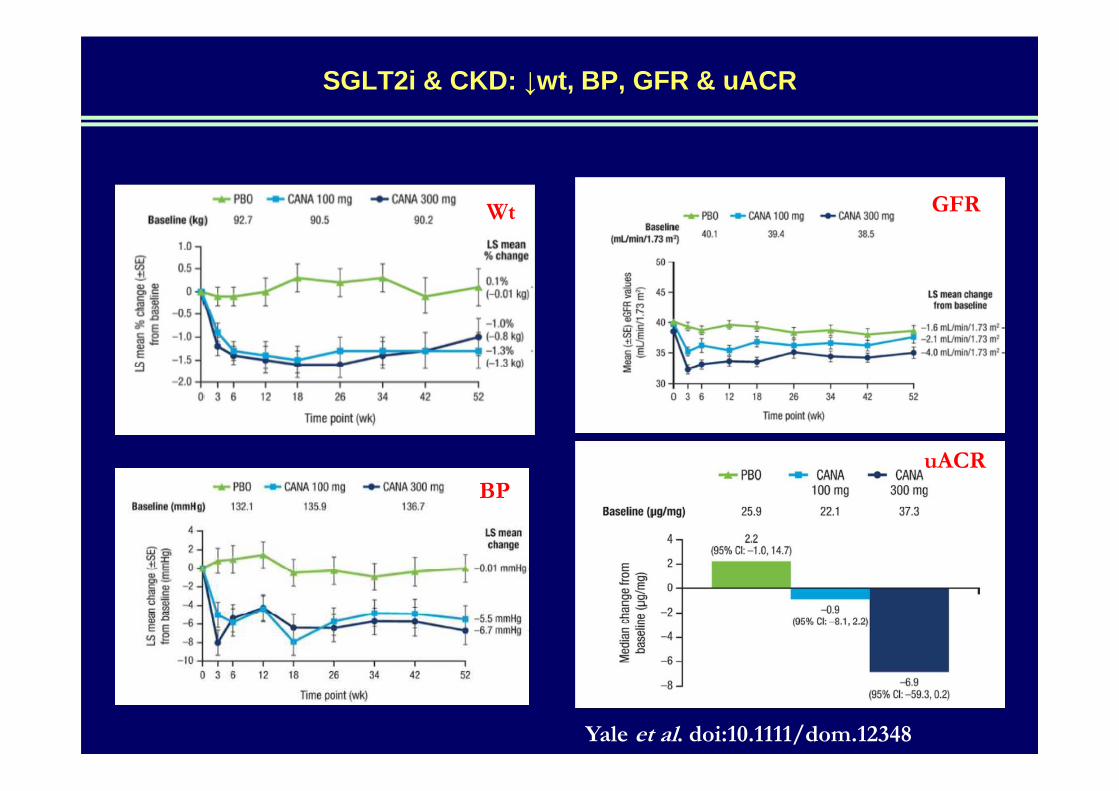
SGLT2i & CKD: ↓wt, BP, GFR & uACR
Yale et al. doi:10.1111/dom.12348
Wt
BP
GFR
uACR
Gliflozin guidelines
20% reduction in insulin/ SU if tight control
50% reduction in BP Rx/diuretic if tight control
Daily BP, weight, BSL
Daily groin/apron wash, dry, baby powder
Zinc/castor oil if red, clotrimazole if thrush
MSU pot & cephalexin, pre-emptive Rx if dysuria
Hold SGLT2i if too symptomatic, try alternate daily
Watch for DKA in long-standing T2DM
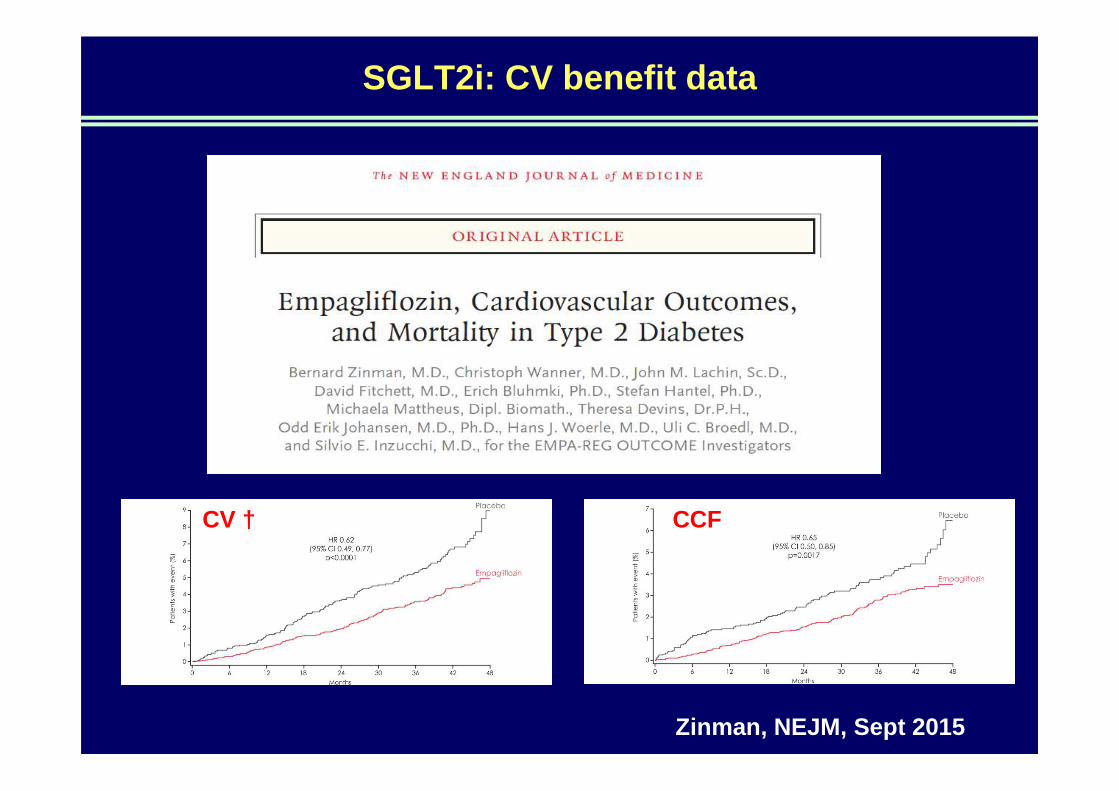
SGLT2i: CV benefit data
CV † CCF
Zinman, NEJM, Sept 2015

SGLT2i: CKD benefit data
Wanner, NEJM, June 2016
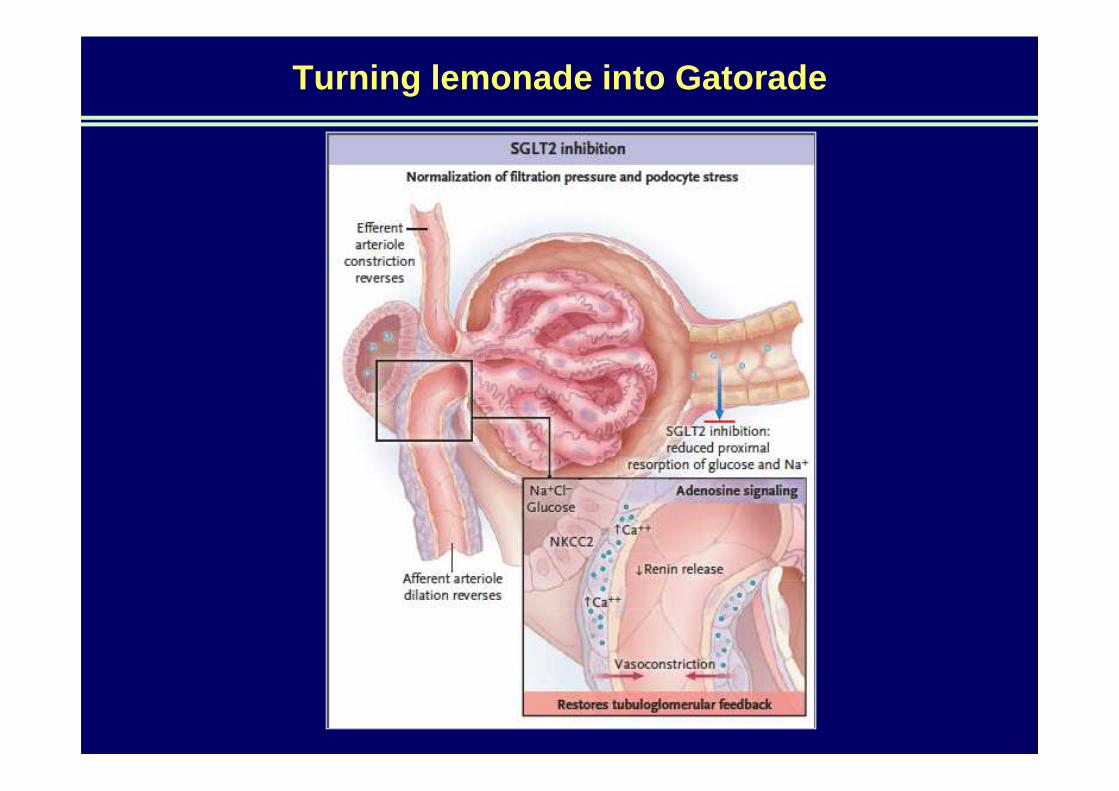
Turning lemonade into Gatorade

SGLT2i class efficacy & safety
More stroke
Less CV †
Less CCF
N= 37,525, 6 regulatory submissions, 7 drugs
Wu, Lancet Diab Endocrin 2016

Therapy PRO CON
Metformin Experience / Proven outcomes / Cost
GI symptoms/ CKD
Sulfonylurea Experience / Cost Hypo’s/ Wt. gain / CKD
DPP4-i (gliptin)
Wt. neutral / Low risk of hypo’sCost / CCF (saxa, not sita) / CKD (except lina) / LFT’s (vilda)
TZD (glitazone)
Low risk of hypo’sCost / Fluid retention / Wt. gain / Fracture risk / ?Bladder ca (pio)
SGLT2-i (gliflozin)
Wt. loss / SBP reduction / Low risk of hypo’s
New / Dehydration / DKA$ / UTI & thrush / CKD inefficacy
Acarbose Low risk of hypo’ / Wt. neutral / Cost
Limited efficacy / GI tolerability
GLP-1 (incretin analogue)
Wt. loss / Low risk of hypoglycaemia
Cost / Injection / GI symptoms
Insulin Experience / Effective Injection / Wt. gain / Hypo’ s
50

Therapy PRO CON
Metformin Experience / Proven outcomes / Cost
GI symptoms/ CKD
Sulfonylurea Experience / Cost Hypo’s/ Wt. gain / CKD
DPP4-i (gliptin)
Wt. neutral / Low risk of hypo’sCost / CCF (saxa, not sita) / CKD (except lina) / LFT’s (vilda)
TZD (glitazone)
Low risk of hypo’sFluid retention / Wt. gain / Fracture risk / ?Bladder ca (pio)
SGLT2-i (gliflozin)
Wt. loss / SBP reduction / Low risk of hypo’
New / Dehydration / DKA$ / UTI & thrush / CKD inefficacy
Acarbose Low risk of hypo’ / Wt. neutral / Cost
Limited efficacy / GI tolerability
GLP-1 (incretin analogue)
Wt. loss / Low risk of hypoglycaemia
Cost / Injection / GI symptoms
Insulin Experience / Effective Injection / Wt. gain / Hypo’ s
51
TOO RISKY
TOO WEAK
BASELINE
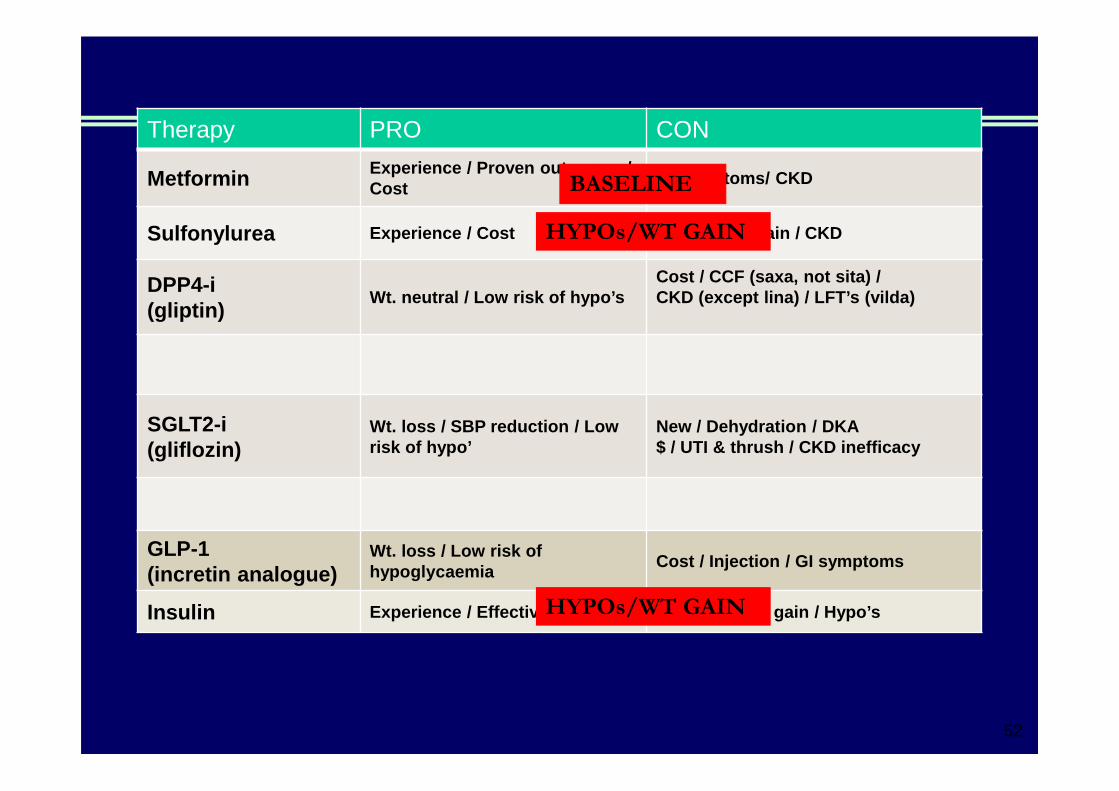
Therapy PRO CON
Metformin Experience / Proven outcomes / Cost
GI symptoms/ CKD
Sulfonylurea Experience / Cost Hypo’s/ Wt. gain / CKD
DPP4-i (gliptin)
Wt. neutral / Low risk of hypo’sCost / CCF (saxa, not sita) / CKD (except lina) / LFT’s (vilda)
SGLT2-i (gliflozin)
Wt. loss / SBP reduction / Low risk of hypo’
New / Dehydration / DKA$ / UTI & thrush / CKD inefficacy
GLP-1 (incretin analogue)
Wt. loss / Low risk of hypoglycaemia
Cost / Injection / GI symptoms
Insulin Experience / Effective Injection / Wt. gain / Hypo’ s
52
HYPOs/WT GAIN
HYPOs/WT GAIN
BASELINE

Homeward bound

Organ-specific effects of obesity
CVA, dementia, carpal tunnel, benign intracranial HTN
Depression, fatigue, isolation, low self-esteem
Dyspnoea, asthma, sleep apnoea, PE
HTN, angina, CCF, varicose veins
Insulin resistance, ↑ lipids & BSL
Gallstones, gastric reflux, fatty liver,
cirrhosis , pancreatitis
Glomerulosclerosis, renal calculi, urine
incontinence
Osteoarthritis, gout, flat feet, plantar fasciitis
Cancer: breast, uterus, cervix, oesophagus,
colon, pancreas, kidney, prostate Male: erectile dysfn.
Female: irregular periods, polycystic ovary, infertility
Skin Candida, acanthosis, hirsutism, stretch,
Healthy lifestyle
Mediterranean diet
Alcohol moderation
Physical activity
Non-smoking
→ Reduced all-cause mortality by 65%Koops, JAMA 2004

Lean Weight: Rule of Thumb
Max lean weight (kg) = Ht (cm) - 100
Height (cm)
155 165 175 185
Weight (kg)
BMI = 25
60 68 76 85

Praise the positive

Eat right
Quantity, quality & value
Pre-meal vinegar as anorectic
Eat like a hippie, not like a truckie
Make food crunchy and colourful
Traffic light detox drink
Move well
Motivation: age 20 vs 50 vs 80
Purpose: fit, strong, flexible, stable
Bird-rocket half-squats
“Seven”

Stay calm
Friends & family
Pets & plants
Movement, music & massage
CRUfAD.org
“This Way Up”

Stay connected