chapter 1shodhganga.inflibnet.ac.in/bitstream/10603/34633/7/07_chapter1.pdf1.1 fluoroquinolone: an...
TRANSCRIPT

Department of Chemistry (SPU)
Chapter 1
Introduction
Chapter 1
Department of Chemistry (SPU) Page 1
1 Introduction 1.1 Fluoroquinolone: An antibacterial agent
1.1.1 Introduction of fluoroquinolone Quinolones were discovered in 1962 as a result of alterations to a compound
isolated from production of the antimalarial drug chloroquine [1]. The first drug in this class was nalidixic acid, which approved for clinical use in 1965. Nalidixic acid was poorly absorbed in the gastrointestinal tract and had a narrow spectrum of activity. Its use was limited to treating urinary tract infection caused by Enterobacteriaceae. The structure of nalidixic acid was modified in the 1980s, improving its absorption, bioavailability and broadcasting it efficacy to include Pseudomonas aeruginosa and certain Gram(+ve) bacteria cooci [2]. These changes included the addition of a fluorine molecule to the basic quinolone structure, resulting in what is now termed a fluoroquinolone.
The quinolones have evolved from antibacterial agents with a limited spectrum of predominantly Gram(–ve) antimicrobial activity and a restricted number of indications to a class of widely used oral (in some cases, intravenous) antibiotics with extensive indications for infections caused by many bacterial pathogens in most body tissues and fluids. This evolutionary pattern has arisen through the development of new core and side-chain structures, with associated improvements in activity, pharmacokinetics and tolerability, and through the selection of molecules that remain useful and well tolerated.
The molecular structures of the quinolones have been adapted over time in association with clinical need. The naphthyridone nucleus of nalidixic acid became the basis of a series of more active compounds; piperazine substitution at the 7-position led to compounds with significant activity against P. aeruginosa, e.g. pipemidic acid and, fluorination at the 6-position (giving the fluoroquinolones) and modification of other side chains led to enhanced anti-Gram(+ve) activity, including improved potency against the pneumococcus, pharmacokinetic profiles and longer serum half-lives [3,4]. These compounds, which are suitable for once-daily administration and are clinically effective in pneumococcal respiratory and other Gram(+ve) infections, have differing adverse drug reaction profiles. In some cases, there are relationships between structure and adverse reaction, notably in terms of phototoxicity, which is more commonly associated with additional fluorine (lomefloxacin, sparfloxacin) or chlorine (clinafloxacin and sitafloxacin) substitution at the 8-position, and central nervous system (CNS) effects, which are more commonly associated with unsubstituted 7-piperazine derivatives [5,6].
However, more serious reactions, such as the temafloxacin-associated haemolytic–uraemic syndrome [7] and the recent serious, unpredictable hepatic reactions associated with trovafloxacin did not seem to have any specific structural relationship. There were also no obvious structural associations, either nuclear or substituent, with QT (Q and T wave) interval prolongation, a recently recognized class effect [8]. Nevertheless, the known adverse reaction profiles and improving broad-spectrum activity have led to the evolution of safer, more clinically efficacious molecules by a process akin to the Darwinian principles of fitness of the surviving molecular ‘mutations’ and attrition of the defective ones [9,10]. Thus today, newer compounds can be designed that maintain or enhance activity whilst minimizing the risk of use-limiting adverse effects.

Chapter 1
Department of Chemistry (SPU) Page 2
There are two aspects to the evolution of the quinolones. Firstly, there is the natural history, characterized by the development of novel structures with better activity, pharmacokinetics and tolerability than previous members of the class. Secondly, there is ‘natural selection’ by prescribers and registration/licensing authorities of those agents and molecular configurations that remain useful and deselection of those that do not. 1.1.2 History of fluoroquinolone
The evolution of quinolones actually emanated from discovery of nalidixic acid [10]. As a by-product of antimalarial research, the first respectative of the quinolones which was found effective against some Gram(–ve) organisms.
Nalidixic acid became the lead compound [11] for medicinal chemist for structural modification to get many newer fluoroquinolone in order to get rid of its three major shortcomings i. Narrow spectrum covering Gram(–ve) organisms only ii. Achieves inadequate tissue level for systematic infection iii. Bacterial resistance development.
This opened for flood gate for synthesising newer and more interesting fluoroquinolones. Out of more than 8000 analogues of fluoroquinolones synthesised [12-15] bearing variety of ring system, a few dozen have been established in the market, and more were in the horizon to be introduced. Such an explosive growth of this group of compound occurred mainly due to three factor; firstly, unprecedented mode of action depending on inhibition ability of susceptible microorganisms to shape their DNA for storage or replication; secondly their potency and antimicrobial spectrum being equally comparative to the desired fermentation based semi-synthetic antibiotic; and finally, their chemical structure being simple, a large number of analogues could be prepared following simple synthetic sequence in cheaper way from readily available intermediates or chemicals.
Further, rapid progress has been made towards broadening their spectrum of activity based on structure-activity relationship (SAR) to treat various systematic infection other than urinary tract infection [16], improving their pharmacokinetic properties [17], and to reduce adverse reaction, especially central nervous system side effect, which is common among these groups of compounds. 1.1.3 Generation of fluoroquinolones on the basis of microbiological activity microbiological activity microbiological activity microbiological activity First generation
The first-generation agents include cinoxacin and nalidixic acid, which are the oldest and least often used quinolones. Because minimal serum levels are achieved, use of these drugs has been restricted to the treatment of uncomplicated urinary tract infections.
Cinoxacin and nalidixic acid require more frequent dosing than the newer quinolones, and they are more susceptible to the development of bacterial resistance. These agents are not recommended for use in patients with poor renal function because of significantly decreased urine concentrations.

Chapter 1
Department of Chemistry (SPU) Page 3
Second generation Second-generation agents include ciprofloxacin, enoxacin, lomefloxacin,
norfloxacin and ofloxacin. The second-generation quinolones have increased Gram(–ve) activity, as well as some Gram(+ve) and atypical pathogen coverage. Compared with first-generation drugs and considered as a group, these agents have broader clinical applications in the treatment of complicated urinary tract infections, pyelonephritis, sexually transmitted diseases, selected pneumonias and skin infections. Ciprofloxacin is the most potent fluoroquinolone against P. aeruginosa. Because of its good penetration into bone, orally administered ciprofloxacin is a useful alternative to parenterally administered antibiotics for the treatment of osteomyelitis caused by susceptible organisms.
Although the FDA (Food and Drug Administration) has labeled some second-generation quinolones for the treatment of lower respiratory tract infections and acute sinusitis, it should be stressed that Staphylococcus pneumoniae is frequently resistant to agents in this class. Consequently, second-generation quinolones are not the drugs of first choice for lower respiratory tract infections and acute sinusitis.
Of the second-generation agents, ofloxacin has the greatest activity against Chlamydia trachomatis. Ciprofloxacin and ofloxacin are the most widely used second-generation quinolones because of their availability in oral and intravenous formulations and their broad set of FDA-labeled indications. Third generation
The third-generation quinolones include levofloxacin, gatifloxacin, moxifloxacin and sparfloxacin. These agents are separated into a third class because of their expanded activity against Gram(+ve) organisms, particularly penicillin-sensitive and penicillin-resistant S. pneumoniae, and atypical pathogens such as Mycoplasma pneumoniae and Chlamydia pneumoniae [18-20]. Although the third-generation quinolones retain broad Gram(–ve) coverage, they are less active than ciprofloxacin against Pseudomonas species.
Because of their expanded antimicrobial spectrum, third-generation quinolones are useful in the treatment of community-acquired pneumonia, acute sinusitis and acute exacerbations of chronic bronchitis, which are their primary FDA-labeled indications. Gatifloxacin also has FDA-labeled indications for urinary tract infections and gonorrhoea. Levofloxacin (the more active component of the ofloxacin racemic mixture [19,21] and gatifloxacin are available in oral and intravenous formulations.
Sparfloxacin carries a significant risk of phototoxicity [21,22]. Grepafloxacin, sparfloxacin and moxifloxacin have been reported to cause prolongation of the QT interval; gatifloxacin has not. However, the FDA recommends that all of these drugs should be avoided in patients who are taking drugs that are known to prolong the QT interval, such as tricyclic antidepressants, phenothiazines and class I antiarrhythmics [23]. In contrast, levofloxacin does not affect the QT interval. Fourth generation
Clinafloxacin, gemifloxacin, sitafloxacin, trovafloxacin and prulifloxacin, currently the member of the fourth-generation class, adds significant antimicrobial activity against anaerobes while maintaining the Gram(+ve) activity of the third-generation

Chapter 1
Department of Chemistry (SPU) Page 4
quinolones. It also retains activity against Pseudomonas species comparable to that of ciprofloxacin [24,25].
Trovafloxacin is available in an oral tablet and as the prodrug alatrofloxacin (Trovan IV) in an intravenous formulation. Although the findings of few clinical trials on trovafloxacin have been published, the drug is originally labeled by the FDA for the treatment of a wide spectrum of infectious diseases [24]. Because of concern about hepatotoxicity, trovafloxacin therapy should be reserved for life- or limb-threatening infections requiring inpatient treatment (hospital or long-term care facility), and the drug should be taken for no longer than 14 days [26]. 1.1.4 Generation of fluoroquinolone on basis of spectrum of activity
As a group, the fluoroquinolones have excellent in-vitro activity against a wide range of both Gram(+ve) and Gram(–ve) bacteria. The newest fluoroquinolones have enhanced activity against gram(+ve) bacteria with only a minimal decrease in activity against Gram(–ve) bacteria. Generation of quinolones on the basis of spectrum of activity is shown below:
Quinolone generation
Agents Antimicrobial spectrum
General clinical indications
First generation
Cinoxacin Flumequine Nalidixic acid Oxolinic acid Piromidic acid Pipemidic acid Rosoxacin
Gram(–ve) organisms (but not Pseudomonas species)
Uncomplicated urinary tract infections
Second generation
Ciprofloxacin Enoxacin Fleroxacin Lomefloxacin Nadifloxacin Norfloxacin Ofloxacin Pefloxacin Rufloxacin
Gram(–ve) organisms (including Pseudomonas species), some Gram(+ve) organisms (including Staphylococcus aureus
but not S. pneumoniae) and some atypical pathogens
Uncomplicated and complicated urinary tract infections and pyelonephritis, sexually transmitted diseases, prostatitis, skin and soft tissue infections
Third generation
Balofloxacin Gatifloxacin Grepafloxacin Levofloxacin Moxifloxacin Pazufloxacin Sparfloxacin Temafloxacin Tosufloxacin
Same as for second-generation agents plus expanded Gram(+ve) coverage (penicillin-sensitive and penicillin-resistant S. pneumoniae) and expanded activity against atypical pathogens
Acute exacerbations of chronic bronchitis, community-acquired pneumonia

Chapter 1
Department of Chemistry (SPU) Page 5
Fourth generation
Clinafloxacin Gemifloxacin Sitafloxacin Trovafloxacin Prulifloxacin
Same as for third-generation agents plus broad anaerobic coverage
Same as for first, second and third generation agents (urinary tract infections and pyelonephritis), intraabdominal infections, nosocomial pneumonia, pelvic infections
1.1.5 Classification of quinolone antibiotics
Figure 1.1.1: Development of quinolones since the early 1960s as an “evolutionary” tree
Chapter 1
Department of Chemistry (SPU) Page 6
1.1.6 Broadened antimicrobial activity The original fluoroquinolone agents were introduced in the late 1980s. Shortly
thereafter, ciprofloxacin became the most frequently used antibiotic throughout the world [27]. The first fluoroquinolones were widely used because they were the only orally administered agents available for the treatment of serious infections caused by Gram(–ve) organisms, including Pseudomonas species. Some infectious disease specialists have become concerned about the overuse of fluoroquinolones. Because of the broad spectrum and oral availability of these agents, overuse is quite easy. Family physicians should always follow the principle of using the drug with the narrowest spectrum and the least toxicity.
Six new fluoroquinolones have been introduced in the United States during the past years. Levofloxacin and sparfloxacin became available in 1996, and grepafloxacin and trovafloxacin were introduced in 1997. Gatifloxacin and moxifloxacin became available in early 2000. In December 1999, grepafloxacin was voluntarily withdrawn. Compared with ciprofloxacin (the prototypical agent of the original fluoroquinolones), the newest fluoroquinolones have enhanced activity against Gram(+ve) bacteria with only a minimal decrease in activity against Gram(–ve) bacteria [28,29] Their expanded Gram(+ve) activity is especially important because it includes significant activity against S.
pneumonia [30,31]. Levofloxacin has enhanced activity against S. pneumoniae, S. aureus and
Enterococcus species, as well as good activity against Mycoplasma and Chlamydia species [32,33]. Sparfloxacin has a further expanded spectrum of activity that includes some activity against anaerobes. Sparfloxacin has even greater activity against Mycoplasma
species. Trovafloxacin is the fluoroquinolone with the most potent anaerobic activity, including activity against bacteroides species. As a result, this agent has the broadest spectrum of activity of the currently available quinolones, as well as a wide range of indications [28,34]. 1.1.7 Mechanism of action
Fluoroquinolones inhibit two enzymes of DNA metabolism in bacteria, Topoisomerase II and IV, the first one also being known as DNA gyrase. Depending on the type of bacterium, these enzymes represent either the primary or secondary target of antimicrobial action. In Gram(–ve) bacteria, such as E. coli, fluoroquinolones predominantly inhibit DNA gyrase, whereas for Gram(+ve) organisms like S. aureus, Topoisomerase IV was recently found to be the principle target. DNA gyrase and Topoisomerase IV have a very similar protein structure, each composed of two subunits (Gyr-A and Gyr-B).
DNA gyrase introduces negative supercoils into the linear DNA double helix, which results in the highly condensed three-dimensional structure of the genetic material usually present inside the cell. This mechanism is necessary to condense the bacterial chromosome. For example in E. coli, a DNA strand of around 1.300 µm length must fit into a cell which is only 2 µm long. The function of Topoisomerase IV is barely understood. However, it is known that this enzyme is involved in the separation process of the DNA daughter chains after chromosome duplication. Models to explain the
Chapter 1
Department of Chemistry (SPU) Page 7
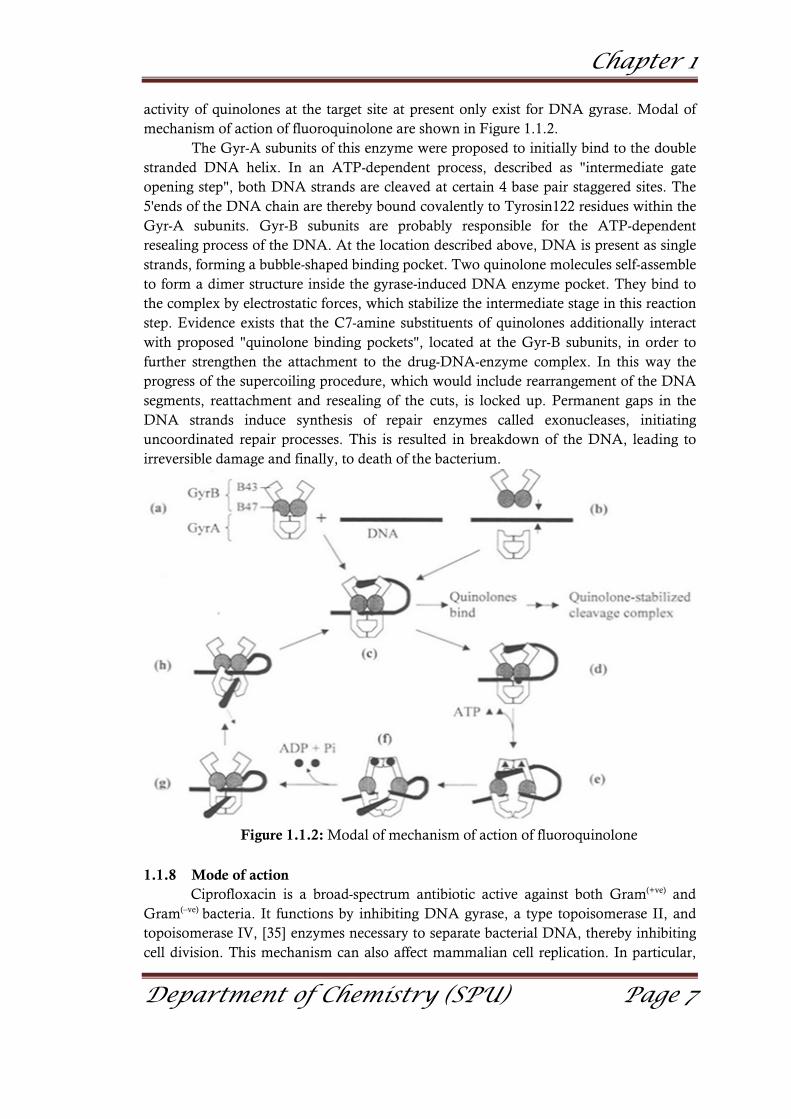
activity of quinolones at the target site at present only exist for DNA gyrase. Modal of mechanism of action of fluoroquinolone are shown in Figure 1.1.2.
The Gyr-A subunits of this enzyme were proposed to initially bind to the double stranded DNA helix. In an ATP-dependent process, described as "intermediate gate opening step", both DNA strands are cleaved at certain 4 base pair staggered sites. The 5'ends of the DNA chain are thereby bound covalently to Tyrosin122 residues within the Gyr-A subunits. Gyr-B subunits are probably responsible for the ATP-dependent resealing process of the DNA. At the location described above, DNA is present as single strands, forming a bubble-shaped binding pocket. Two quinolone molecules self-assemble to form a dimer structure inside the gyrase-induced DNA enzyme pocket. They bind to the complex by electrostatic forces, which stabilize the intermediate stage in this reaction step. Evidence exists that the C7-amine substituents of quinolones additionally interact with proposed "quinolone binding pockets", located at the Gyr-B subunits, in order to further strengthen the attachment to the drug-DNA-enzyme complex. In this way the progress of the supercoiling procedure, which would include rearrangement of the DNA segments, reattachment and resealing of the cuts, is locked up. Permanent gaps in the DNA strands induce synthesis of repair enzymes called exonucleases, initiating uncoordinated repair processes. This is resulted in breakdown of the DNA, leading to irreversible damage and finally, to death of the bacterium.
Figure 1.1.2: Modal of mechanism of action of fluoroquinolone
1.1.8 Mode of action Ciprofloxacin is a broad-spectrum antibiotic active against both Gram(+ve) and
Gram(–ve) bacteria. It functions by inhibiting DNA gyrase, a type topoisomerase II, and topoisomerase IV, [35] enzymes necessary to separate bacterial DNA, thereby inhibiting cell division. This mechanism can also affect mammalian cell replication. In particular,

Chapter 1
Department of Chemistry (SPU) Page 8
some congeners of this drug family (for example those that contain the C-8 fluorine) [36] display high activity not only against bacterial topoisomerase but also against eukaryotic topoisomerase and are toxic to cultured mammalian cells and in-vivo tumour models [37]. Although quinolones are highly toxic to mammalian cells in culture, its mechanism of cytotoxic action is not known. Quinolone-induced DNA damage was first reported in 1986 [38].
Recent studies have demonstrated a correlation between mammalian cell cytotoxicity of the quinolones and the induction of micronuclei [39-43]. As such, some fluoroquinolones may cause injury to the chromosome of eukaryotic cells [44-49]. There continues to be debate as to whether or not this DNA damage is to be considered one of the mechanisms of action concerning the severe adverse reactions experienced by some patients following fluoroquinolone therapy [50]. 1.1.9 Bacterial resistance of fluoroquinolone
Gram(+ve) and Gram(–ve) bacteria have been reported to be resistant to quinolones [51,52]. This resistance appears to be the result of one of three mechanisms: alterations in the quinolone enzymatic targets (DNA gyrase), decreased outer membrane permeability or the development of efflux mechanisms. The accumulation of several bacterial mutations (DNA gyrase and bacterial permeability) has been associated with the development of very high minimum inhibitory concentrations to ciprofloxacin in isolates of S. aureus, Enterobacteriaceae species and P. aeruginosa [51]. Resistance to fluoroquinolones can also develop because of alterations in bacterial permeability and the development of efflux pumps. This resistance mechanism is shared with antimicrobial agents structurally unrelated to the fluoroquinolones, such as the β-lactams, tetracyclines and chloramphenicol (chloromycetin). Cross-resistance among the quinolones is expected, but the extent to which the minimum inhibitory concentration is affected varies from agent to agent. Therefore, the bacterial susceptibility and pharmacokinetic profiles of each fluoroquinolones should be considered in determining the effectiveness of specific agents [52,53]. 1.1.10 Uses of fluoroquinolones
� Urinary tract infections (norfloxacin, lomefloxacin, enoxacin, ofloxacin, ciprofloxacin, levofloxacin, gatifloxacin and trovafloxacin)
� Lower respiratory tract infections (lomefloxacin, ofloxacin, ciprofloxacin and trovafloxacin)
� Skin and skin-structure infections (ofloxacin, ciprofloxacin, levofloxacin and trovafloxacin)
� Urethral and cervical gonococcal infections (norfloxacin, enoxacin, ofloxacin, ciprofloxacin, gatifloxacin and trovafloxacin)
� Prostatitis (norfloxacin, ofloxacin and trovafloxacin) � Acute sinusitis (ciprofloxacin, levofloxacin, gatifloxacin, moxifloxacin (Avelox)
and trovafloxacin) � Acute exacerbations of chronic bronchitis (levofloxacin, sparfloxacin (Zagam),
gatifloxacin, moxifloxacin and trovafloxacin)

Chapter 1
Department of Chemistry (SPU) Page 9
� Community-acquired pneumonia (levofloxacin, sparfloxacin, gatifloxacin, moxifloxacin and trovafloxacin)
1.1.11 Ciprofloxacin
Bayer introduced ciprofloxacin in 1987 and was later approved by the FDA on 22nd October 1987 for use in the United States to treat specific bacterial infections. In 1991, the intravenous formulation was introduced. The current United States patent appears to be held by Bayer, being the assignee [54]. The United States patent was applied in January 1987, but was not approved until 1996 according to the patent history.
Ciprofloxacin is a synthetic chemotherapeutic antibiotic of the fluoroquinolone [55,56]. It is a second-generation fluoroquinolone antibacterial. It kills bacteria by interfering with the enzymes that cause DNA to rewind after being copied, which stops synthesis of DNA and of protein. Ciprofloxacin is marketed worldwide with over three hundred different brand names. In the United States, Canada, and the UK, it is marketed as Baycip, Ciloxan, Ciflox, Cipro, Cipro XR, Cipro XL, Ciproxin, Prociflor, and most recently, Proquin. In addition, ciprofloxacin is available as a generic drug under a variety of different brand names and is also available for limited use in veterinary medicine. Ciprofloxacin interacts with other drugs, herbal and natural supplements, and thyroid medications [57].
Ciprofloxacin has been shown to be more effective than trimethoprim-sulfamethoxazole and aminoglycosides in 7-10 days courses for the treatment of complicated urinary tract infections. However, few patients maintain sterile urine six weeks after any antibiotic therapy [58,59]. Bacterial resistance and Candida super infection often limit treatment in complicated urinary tract infections, with an estimated failure rate of at least 2 percent [60,61]. Failure rates as high as 20 percent may be encountered with infections caused by pathogens such as P. aeruginosa.
Chemistry of ciprofloxacin The IUPAC name of ciprofloxacin is 1-cyclopropyl-6-fluoro-1,4-dihydro-4-oxo-7-
(1-piperazinyl)-3-quinolinecarboxylic acid. Its empirical formula is C17H18FN3O3 and its molecular weight is 331.4 g/mol. It is a faintly yellowish to light yellow crystalline substance [62]. Clinical uses of ciprofloxacin
Ciprofloxacin is effective against many aerobic Gram(–ve) organisms including several Streptococcus and Staphylococcus strains. It is also active against several Gram(+ve) organisms including E. coli. It has been also recently used for both prophylaxis and treatment of Bacillus anthracis infection. Since the quinolones have a different mechanism of action from many other antibacterial classes, there is little incidence of cross-resistance between the classes. Therefore, ciprofloxacin and other quinolones can be used in cases of resistance to other antibiotics.
Chapter 1
Department of Chemistry (SPU) Page 10
Adverse effects of ciprofloxacin Ciprofloxacin may have central nervous system (CNS) effects such as dizziness, hallucinations, tremors and depression. It may also cause convulsions and toxic psychosis. As a result of these possible effects, patients already at increased risk for seizures or CNS problems should be closely monitored when taking quinolones. Anaphylactic reactions are also possible, so patients should be advised to look for symptoms such as itching, dyspnoea and pharyngeal or facial edema, and to seek medical help if these symptoms appear. Pseudomembranous colitis can be caused by almost all antibiotics, including quinolones, so if patients present with diarrhoea during or after treatment with ciprofloxacin, proper treatment including fluid and electrolyte replenishment may be required. There have also been reports of rare cases of peripheral neuropathy or tendon weakening ciprofloxacin treatment. 1.2 Chemistry and biochemistry of copper
1.2.1 Chemistry of copper metal Copper is a chemical element with the symbol Cu (Latin: cuprum) and atomic
number 29. Copper(II) ions (Cu2+) are soluble in water, where they function at low concentration as bacteriostatic substances, fungicides, and wood preservatives. In sufficient amounts, copper salts can be poisonous to higher organisms as well [63-65]. However, despite universal toxicity at high concentrations, the Cu2+ ion at lower concentrations is an essential trace nutrient to all higher plant and animal life. In animals, including humans, it is found widely in tissues, with concentration in liver, muscle, and bone. It functions as a co-factor in various enzymes and in copper-based pigments.
1.2.2 Biochemistry of copper Copper is known to be an essential element in human metabolism. However,
copper does not exist in the body in measurable amounts in ionic form. All measurable amounts of copper in the body exist in tissues as complexes with the organic compounds of proteins and enzymes. Therefore, it has been concluded that copper as involved in body processes. Some copper complexes serve to store copper, others to transport it, and yet others play important roles in key cellular and metabolic processes.
The key to the effective use of copper-based pharmaceuticals is not the use of inorganic compounds of copper, as used by the ancients, but rather the use of metallo-organic complexes or chelates of copper. The process of chelating metals allows them to be smuggled in the transport process across the intestinal wall and thereby enter into the mainstream of nutrient flow and usage in the body [66].
Copper is incorporated into a number of metalloenzymes involved in haemoglobin formation, drug/xenobiotic metabolism, carbohydrate metabolism, catecholamine biosynthesis and the cross-linking of collagen as well as in the antioxidant defense mechanism. Moreover, copper-dependent enzymes, such as cytochrome c oxidase, superoxide dismutase, ferroxidases, monoamine oxidase, and dopamine β-monooxygenase function to reduce reactive oxygen species (ROS) or molecular oxygen [67]. Symptoms associated with copper deficiency in humans include normocytic,

Chapter 1
Department of Chemistry (SPU) Page 11
hypochromic anaemia, leucopoenia, and osteoporosis. Copper deficiency is rarely observed in the general population [68]. 1.2.3 Biomedical applications
Copper doorknobs are used by hospitals to reduce the transfer of disease, and Legionnaires disease is suppressed by copper tubing in air-conditioning systems. Copper(II) sulphate is used as a fungicide and as algae control in domestic lakes and ponds. It is used in gardening powders and sprays to kill mildew [69]. Copper complex containing radioactive copper-62, is used as a positron emission tomography radiotracer for heart blood flow measurements. Copper-64 can be used as a positron emission tomography radiotracer for medical imaging. When it from complex with a chelating agents, it can be used to treat cancer through radiation therapy. 1.2.4 Biological role Copper essentiality
Copper is an essential trace element that is vital to the health of all living things (humans, plants, animals, and microorganisms). The human body normally contains copper at a level of about 1.4 to 2.1 mg for each kg of body mass [70]. Copper is distributed widely in the body and occurs in liver, muscle and bone. Copper is transported in the bloodstream on a plasma protein called ceruloplasmin. When copper is first absorbed in the gut, it is transported to the liver bound to albumin. Daily dietary standards for copper have been set by various health agencies around the world. Researchers specializing in the fields of microbiology, toxicology, nutrition, and health risk assessments are working together to define precise copper levels required for essentiality while avoiding deficient or excess copper intakes. Excess and deficiency of copper
It is believed that zinc and copper compete for absorption in the digestive tract so that a diet that is excessive in one of these minerals may result in a deficiency in the other. The RDA for copper in normal healthy adults is 0.9 mg/day. On the other hand, professional research on the subject recommends 3.0 mg/day [71]. Because of its role in facilitating iron uptake, copper deficiency can often produce anaemia-like symptoms. Conversely, accumulations of copper in body tissues are believed to cause the symptoms of Wilson's disease in humans. Copper deficiency is also associated with neutropenia, bone abnormalities, hypopigmentation, impaired growth, increased incidence of infections, and abnormalities in glucose and cholesterol metabolism. Severe deficiency can be found by testing for low plasma or serum copper levels, low ceruloplasmin, and low red blood cell superoxide dismutase (SOD) levels. However, these tests are not sensitive to marginal but not severe copper status. The "cytochrome c oxidase activity of leucocytes and platelets" is another sign of deficiency, but the results have not been confirmed by replication [72]. Chronic copper depletion leads to abnormalities in metabolism of fats, high triglycerides, non-alcoholic steatohepatitis (NASH), fatty liver disease and poor melanin and dopamine synthesis causing depression and sunburn.

Chapter 1
Department of Chemistry (SPU) Page 12
Antibacterial properties Copper is antibacterial/germicidal, via the oligodynamic effect. For example,
brass door knobs disinfect themselves of many bacteria within a period of eight hour [73]. Antimicrobial properties of copper are effective against MRSA,[74] Escherichia coli [75] and other pathogens [76-78]. Colder temperatures and longer times are required to kill bacteria. Copper kills a variety of potentially harmful pathogens. On February 29, 2008, the United States Environmental Protection Agency (USEPA) registered 275 alloys, containing greater than 65% nominal copper content, as antimicrobial materials [79]. Registered alloys include pure copper, an assortment of brasses and bronzes, and additional alloys. EPA-sanctioned tests using good laboratory practices were conducted in order to obtain several antimicrobial claims valid against: methicillin-resistant S. aureus (MRSA), Enterobacter aerogenes, E. coli O157: H7 and P. aeruginosa. The EPA registration allows the manufacturers of these copper alloys to legally make public health claims as to the health effects of these materials. Several of the aforementioned bacteria are responsible for a large portion of the nearly two million hospital-acquired infections contracted each year in the United States [80]. Frequently touched surfaces in hospitals and public facilities harbour bacteria and increase the risk for contracting infections. Covering touch surfaces with copper alloys can help reduce microbial contamination associated with hospital-acquired infections on these surfaces. 1.3 Chemistry and biochemistry of palladium
1.3.1 Chemistry of palladium Palladium was discovered by William Hyde Wollaston in 1803 [81,82]. It was
named by Wollaston in 1804 after the asteroid Pallas, which had been discovered two years earlier [83]. Wollaston found palladium in crude platinum ore by dissolving the ore in aqua regia, neutralizing the solution with sodium hydroxide, and precipitating platinum as ammonium chloroplatinate with ammonium chloride. He added mercuric cyanide to form the compound palladium cyanide, which was heated to extract palladium metal. 1.3.2 Biochemistry of palladium
The low anti-tumour activity of palladium complexes has been attributed to rapid hydrolysis leading to easy dissociation (in solution) of leaving groups and to the formation of very reactive species unable to reach their pharmacological targets [84].
Based on the structural analogy between Pt(II) and Pd(II) complexes, some studies on Pd(II) compounds as suitable drugs have been carried out. However, advances in this area have been scarce probably due to kinetic reasons; it is well known that comparable Pt(II) compounds always react more slowly by a factor of 105 than corresponding Pd(II) complexes. Relatively few palladium(II) and palladium(IV) complexes have been investigated for their cytotoxic anti-tumour activity [85]. 1.3.3 Applications of palladium in biology
Palladium complexes are the most frequently used as anticancer drugs. It is one of the most active agents against testicular, lung, cervical, bladder and head and neck cancers. It is used as a single agent and in combination regimens to treat a variety of solid tumours [86,87]. Palladium complexes are also used to treat Hodgkin's and non-

Chapter 1
Department of Chemistry (SPU) Page 13
Hodgkin's lymphomas, neuroblastoma, sarcomas, multiple myeloma, melanoma, and mesothelioma. Due to its successful contribution, testicular cancer has become a model for curable neoplasm. 1.4 Metal in medicine 1.4.1 General
When one discusses "drugs", one open thing only of organic molecule [88]. This belies the fact that metal complexes too, play an important role in chemotherapy. Approximately one third of proteins and enzymes require at least one metal ion to function properly, perhaps it is not surprising that metal complexes have a role to play in medicine as well. The interactions of heavy metals such as platinum, palladium and gold with N,S-donor atoms have been recognised for their anti-carcinogenic properties with the potential to develop metal-based drugs [89]. Metal ions and metal coordination compounds are known to affect cellular processes in a dramatic way [90]. This metal effect influences not only natural processes, such as cell division and gene expression, but also non-natural processes, such as toxicity, carcinogenicity, and anti-tumour chemistry [91].
Medicinal inorganic chemistry is a discipline of growing significance in both therapeutic and diagnostic medicine [92]. Inorganic compounds have been used in medicine for many centuries, but often only in an empirical way with little attempt to design the compounds to be used, and with little or no understanding of the molecular basis of their mechanism of action. Progress in the design of metal-based inorganic drugs has been slow due to problems relating to substitution and hydrolytic equilibria, redox and polymerisation reactions [93]. The interactions of heavy metals such as platinum and gold with N,S-donor atoms have been recognised for their anti-cancer properties with the potential to develop metal-based drugs [94]. The successful use of metal complexes as therapeutic and diagnostic agents depends on the control of their kinetic and thermodynamic properties through appropriate choice of oxidation state, numbers of bound ligands, and coordination geometry [95]. In this way, it is possible to achieve specificity of biological activity and most importantly, to minimise toxic side-effects. However, before rational drug design can be pursued, a detailed knowledge of the mechanism of action is required [96].
Equally, if one is to "design out" toxic side effects, it is important to know that drug/target interactions are responsible for the toxicity. Broad interest in the pharmacological properties of metal compounds first arose with the pioneering work of Barnett Rosenberg, who in the late 1960s by chance discovered the cytostatic effects of cisplatin and related compounds [97]. It seemed that biological activity (anti-tumour activity) had to be unique among heavy metal compounds [98]. It was seen as a result of the specific kinetic and structural properties of Pt2+ centre making possible the specific impact on genomic DNA. It was shown later that in addition to platinum(II) complexes, numerous planar and octahedral platinum complexes as well as compounds of other platinum-group metals exhibited anti-tumour properties. Anti-tumour activity has been reported for a variety of compounds involving metals such as titanium, vanadium, iron, gold, silver, copper, palladium, ruthenium, germanium and tin [99].
Chapter 1
Department of Chemistry (SPU) Page 14
In 1991, Peter Sadler noted that most elements of the periodic table, up to atomic number 83, have potential used as drugs or diagnostic agents [100-102]. The platinum compounds as anticancer agents, vanadium compounds as insulin substitutes for diabetics, 99m-technetium reagents used in diagnostic and treatment capabilities, and MRI contrast reagents containing gadolinium are interested in medicinal chemistry [103]. Inorganic compounds have found usage in chemotherapeutic agents such as: � Anticancer agents like [Pd(bpy)Cl2] � The gold-containing antiarthritic drug auranofin � Metal-mediated antibiotics like bleomycin, which requires iron or other metals for
activity � Technetium-99m and other short-lived isotopes used as radiopharmaceuticals in
disease diagnosis and treatment � Magnetic resonance imaging (MRI)-enhancing gadolinium compounds � Antibacterial, antiviral, antiparasitic, and radiosensitizing agents
1.4.2 Copper in medicinal chemistry
Since 1934, it has been known that individuals suffering from such diseases as scarlet fever, diphtheria, tuberculosis, arthritis, malignant tumours and lymphogranulomas exhibit an elevation of copper in their blood plasma. Since then, the list of maladies bringing about such elevation has been extended to fever, wounds, ulcers, pain, seizures, cancers, carcinogenesis, diabetes, cerebrovascular, cardiovascular, irradiation and tissue stresses, including restricted blood flow. This suggests that redistribution of copper in the body has a general role in responding to physiological, disease, or injury stress.
Copper is known to be an essential element in human metabolism. However, copper does not exist in the body in measurable amounts in ionic form. All measurable amounts of copper in the body exist in tissues as complexes with the organic compounds of proteins and enzymes. Therefore, it has been concluded that copper becomes and remains intimately involved in body processes. Some copper complexes serve to store copper, others to transport it, and yet others play important roles in key cellular and metabolic processes. Studies into the roles that these copper complexes play and the mechanisms of these roles have further confirmed that copper enters into the prevention and control of a number of disease states in the body. The key to the effective use of copper-based pharmaceuticals is not the use of inorganic compounds of copper, as used by the ancients, but rather the use of metallo-organic complexes or chelates of copper. The process of chelating metals allows them to be smuggled in the transport process across the intestinal wall and thereby enter into the mainstream of nutrient flow and usage in the body. Ulcer and wound-healing activities of copper complexes
It has been demonstrated that copper complexes such as copper aspirinate and copper tryptophanate, markedly increase healing rate of ulcers and wounds. For example, copper complexes heal gastric ulcers five days sooner than other reagents. Further, it has been shown that, whereas non-steroidal anti-inflammatory drugs, such as

Chapter 1
Department of Chemistry (SPU) Page 15
ibuprofen and enefenamic acid suppress wound healing, copper complexes of these drugs promote normal wound healing while at the same time retaining anti-inflammatory activity. Anticonvulsant activities of copper complexes
The brain contains more copper than any other organ of the body except the liver, where copper is stored for use elsewhere. This fact suggests that copper plays a role in brain functions. With reports of seizures in animals and humans following the protracted consumption of copper-deficient diets, it is reasoned that copper has a role to play in the prevention of seizures. It is subsequently discovered that organic compounds that are not themselves anti-convulsants, exhibit anticonvulsant activity when complexed with copper. Further, it was found that copper complexes of all anti-epileptic drugs are more effective and less toxic than their parent drugs. Anticancer activities of copper complexes
As early as 1912, patients in Germany were treated for facial epithelioma with a mixture of copper chloride and lecithin. Success of such treatment suggested that copper compounds have anticancer activity. Work at the University of Liverpool in 1913 demonstrated that subcutaneous and intravenous injections of a copper salt or colloidal copper softened and degenerated carcinomas transplanted into mice. In 1930, work in France indicated that injections of colloidal copper mobilized and expelled tumour tissue. Recent work with mice in the USA has shown that, indeed, treatment of solid tumors with non-toxic doses of various organic complexes of copper markedly decreased tumour growth and metastasis and thus increased survival rate. These copper complexes did not kill cancer cells but caused them to revert to normal cells. Radiation protection and radiation recovery of copper complexes
Ionizing radiation, such as that used in the treatment of cancer, has been shown to induce massive systemic inflammation. Ideally, such radiation-induced injury might be prevented or ameliorated by chemical repair mechanisms in the body. Thus, pharmacological approaches to the repair of radiation-damaged tissue are needed. As early as 1984, copper complexes have been shown to have radiation protection and radiation recovery activities. They are capable of causing rapid recovery of immune competence and recovery from radiation induced tissue changes. The mechanism of this activity appears to be tied to the ability of certain copper complexes to deactivate the superoxide, or free radicals liberated by ionizing radiation. In addition, since radiation has the capability of breaking the bonds of natural copper enzymes in the body, supplementing these with non-toxic doses of pharmaceutical copper complexes restores the lost tissue-repair capability. Since these complexes may also have anticarcinogenic activity, it is suggested that there would be merit in using copper complexes in the treatment of cancer and in particular, treating patients undergoing ionizing radiation therapy for their cancer, accidental exposure to radiation, and astronauts undertaking space travel.

Chapter 1
Department of Chemistry (SPU) Page 16
Heart disease and copper complexes Numerous studies have drawn attention to the relationship between copper
deficiency and heart disease. Dr. L.M. Klevay at the U.S. Department of Agriculture, Human Nutrition Research Center in 1973 has led to the postulation that copper has a direct effect on the control of cholesterol. In continuing work published in 1975, he theorized that a metabolic imbalance between zinc and copper with more emphasis on copper deficiency than zinc excess is a major contributing factor to the aetiology of coronary heart disease. Subsequent work by other investigators has shown that copper complexes also can have a valuable role in the minimization of damage to the aorta and heart muscle as oxygenated blood into tissues myocardial infarction. This action is based on the anti-inflammatory action of copper complexes. These studies suggest the use of copper dietary supplements as a means of preventing and controlling such diseases as atherosclerosis (a form of arteriosclerosis), coronary heart disease, aortic aneurysms and myocardial infarction. It has been speculated that the reason that the heart attack rate in France is lower than in the rest of Europe is because of the French practice of drinking red wine. Red wine has a higher copper content than white wine because it is prepared with the skin of the grape intact. The copper originates in the wine from the copper fungicides used on the grapes in the field.
1.4.3 Toxicity of cooper
In human body, copper is maintained in homeostasis [104]. If the intake of copper exceeds the range of the human tolerance, it would cause toxic effects such as hemolysis, jaundice and even death. Most recently, the study indicates that the overload of common copper in-vivo can induce a set of toxicological activities such as hepatocirrhosis [105], changes in lipid profile, oxidative stress, renal dysfunction [106] and stimulation of mucous membrane of elementary canal, etc. However, recent toxicological investigations of manufactured nanoparticles revealed such a nature that compared with the larger particles of the same chemical composition (on the identical mass basis), nanoparticles tends to exhibit quite different toxicological effects in-vivo [107-109]. Copper is actively excreted by the normal body, chronic copper toxicities in humans without a genetic defect in copper handling has not been demonstrated [110,111]. However, large amounts of copper salts taken in suicide attempts have produced acute copper toxicity in normal humans. Equivalent amounts of copper salts (30 mg/kg) are toxic in animals [112]. 1.4.4 Palladium in medicinal chemistry
The palladium(II) and palladium(IV) complexes with neutral amine ligands, such as ethylenediamine, diaminocyclohexane, ammonia, pyridine and pyrimidine derivatives, alkylaminophosphine, oxides, mercepto-imidazoles, and pyrimidines. have been investigated for their cytotoxic anti-tumour activity [113,114]. The promising anti-proliferative activity was found in Pd-complexes with chelating ligands or alkyl- or aryl-thiosemicarbazones.
The synthesis and evaluation of the biological activity of the new metal-based compounds is the field of growing interest. Numerous complexes based on palladium(II) ion have been synthesized and their different biological activities have been documented

Chapter 1
Department of Chemistry (SPU) Page 17
[115–117]. The impact of different palladium complexes on the growth and metabolism of various groups of microorganisms has been studied. Garoufis et al., [118] reviewed numerous scientific papers on anti-viral, antibacterial and antifungal activity of palladium(II) complexes with different types of ligands (sulphur and nitrogen donor ligands, Schiff base ligands and drugs as ligands). Guerra et al., [119] synthesized three palladium complexes with antibiotics of the tetracycline family and they tested their effects on tetracycline sensitive and resistant bacterial strains. The palladium complex with tetracycline was 16 times stronger than the tetracycline itself against resistant strain. Vieira et al., [120] prepared new palladium(II) and platinum(II) complexes with fluoroquinolones which showed activity to mycobacterium tuberculosis. There are other papers in the literature showing different intensity of palladium complexes activity on various species of bacteria and fungi [121–125].
The Pd(II) chelates with inert ligands (e.g. sulphur or nitrogen) were suggested by Das and Livingstone [126] to be more effective anti-tumour agents than those of other metals, they possess the proper liability to bring the metal to the target (DNA) and allow it to interact with it. In this respect, Pt(II) chelates are very inert kinetically, while those of other metals like Ni(II), Zn(II), Cu(II), etc. do not have sufficient thermodynamic stability. The N,S-donor ligands used to prepare anti-tumour and antimicrobial Pd(II) complexes were mostly thiosemicarbazones and dithiocarbazates. These ligands possess anti-viral, malarial, fungal, microbial and tumour activity and their mechanism of action, most probably involves the inhibition of ribonucleotide reductase, converting ribonucleotides to deoxyribonucleotides [127,128]. 1.4.5 Toxicity of palladium
It has become important to clarify the potential toxic properties of palladium. In the past, little effort has been spent on the toxicology of palladium compounds. Two separate studies have shown rapid death following intravenous injection of palladium chloride solution [129,130]. Although damage to the heart was indicated, the mechanisms underlying the effect were poorly understood. Moreover, a number of reports also suggest that palladium may be a health hazard. Shishniashvili et al., [131] reported that incubation of calf thymus (CT) DNA with palladium ions resulted in the degradation of DNA molecules. Schroeder [132] has shown that palladium is carcinogenic in an animal study. However, the mode of action of this heavy metal in producing these toxic effects remains unclear. Rapaka et al., [133] reported that palladium ions not only affected the incorporation of radioactive proline into non-dialyzable fraction in l0-day chick embryo cartilage explants, but also markedly inhibited the hydroxylation of proline in collagen precursor molecules.
Like mercury, palladium is cytotoxic which kills or damages cells [134-136]. Palladium also causes considerable damage and degradation of DNA and exacerbates hydroxyl radical damage. Palladium also damages cell mitochondria and inhibits enzyme activity and function [137-139]. Palladium also causes significant numbers of allergic reactions as well as contact dermatitis, stomatitis, lichinoid reactions, and periodontal gum disease [140-142]. Because of its toxicity and high mobility, many cases of palladium poisoning have resulted and palladium in dental alloys has been banned in

Chapter 1
Department of Chemistry (SPU) Page 18
Switzerland. Likewise the German Health Ministry has been warning dentists since 1993 not to use palladium-copper alloys.
Late symptoms of palladium poisoning include: Dying of the teeth, granulomas, puss pockets with dead tissue, swollen tongue, nerve pain in the face, paralysis of face, muscle cramps of tongue, lips, around eyes, sinus infection, bronchitis and lung ailments without clear reason; difficulty breathing at night, problems with stomach, intestines, liver, bladder, kidneys, weight loss, joint and muscle pain, muscle cramps and weakness, earnoise, visual disturbance, depression, insomnia, outbreaks of sweat, palpitations, difficulty concentrating.
Palladium is toxic in nature but due to chelation of palladium and N,N or N,S- donor ligand the toxicity is reduced. Considerably higher reactivity of palladium complexes implies that if an antitumor palladium drug is to be developed, it must somehow be stabilized by a strongly coordinated nitrogen donor ligand and a suitable leaving group. If this group is reasonably non-labile, the drug may maintain its structural integrity in-vivo long enough to show antitumor activity. A series of mononuclear and dinuclear palladium complexes has been investigated by different researchers including their cytotoxicity against a number of cancer cell lines. Some of the palladium compounds showed anticancer activities same as platinum compounds. 1.5 Nitrogen donor ligand 1.5.1 Terpyridines
Terpyridine was first synthesized by G. Morgan and F. H. Burstall in 1932 by the oxidative coupling of pyridines. This method, however, proceeded in low yields. In 1991, a more efficient synthesis was described that involves the condensation of 2-acetylpyridine and enaminone, which was prepared by the reaction of 2-acetylpyridine with N,N-dimethylformamide dimethylacetal. Alternatively, the base-catalyzed reaction of 2-acetylpyridine with carbon disulfide followed by alkylation with methyl iodide gave C5H4NCOCH=C(SMe)2. Condensation of this species with 2-acetylpyridine forms the related 1,5-diketone, which condensed with ammonium acetate to form a terpyridine [143]. Treatment of this derivative with Raney nickel removes the thioether group [144].
2,2':6',2''-Terpyridines are among the N-heterocycles, which have very high binding affinity towards transition metal ions due to d̟- p̟* back bonding of the metal to the pyridine ring and the chelate effect [145,146]. Complexation of one or two 2,2':6',2''-terpyridine a ligands can lead to a formation of metal-complexes [147]. These complexes possess distinct photophysical, electrochemical and magnetic properties [148].
Terpyridines, which form metal complexes with a variety of transition metal ions, [149-151] have many potential applications in fields such as macromolecular chemistry, nanoscience, biochemistry and photophysics. 1.5.2 Properties of terpyridines
Terpyridine is a tridentate ligand that binds metals at three meridional sites giving two adjacent 5-membered MN2C2 chelate rings [152]. Terpyridine forms complexes with most transition metal ion as do other polypyridine compounds, such as 2,2'-bipyridine and 1,10-phenanthroline. Complexes containing two terpyridine complexes, i.e. [M(terpy)2]n+ are common. They differ structurally from the related [M(bipy)3]n+

Chapter 1
Department of Chemistry (SPU) Page 19
complexes in being achiral. Terpyridine complexes, like other polypyridine complexes, exhibit characteristic optical and electrochemical properties: metal-to-ligand charge transfer (MLCT) in the visible region, reversible reduction and oxidation, and fairly intense luminescence. Because they are ̟-acceptors, terpy and bipyridine to stabilize metals in lower oxidation states. For instance in acetonitrile solution, it is possible to generate the [M(terpy)2] (M = Ni, Co). 1.5.3 Imidazo[4,5-f]-1,10-phenanthrolines
Phenanthroline is a heterocyclic organic compound. As a bidentate ligand, it forms strong complexes with most metal ions. In terms of its coordination properties, phen is similar to 2,2'-bipyridine. The imidazo[4,5-f]-1,10-phenanthrolines may be prepared by a reaction of 1,10-phenanthroline-5,6-dione with aldehydes in the presence of ammonium acetate in acetic acid [153]. Aromatic ligands such as 1,10-phenanthroline, which is one of the most used ligands in coordination chemistry, has been utilized in the field of antitumour-transition metal chemistry. Its planar geometry enables its participation as a DNA intercalator. Several derivatives of 1,10-phenanthroline were prepared and used as tetradentate ligands. 1.5.4 Properties and application of imidazo[4,5-f]-1,10-phenanthrolines
The chelating ligands 1,10-phenanthroline and their substituted derivatives have played an important role in the development of coordination chemistry [154]. Phenanthrolines are of interest because of the occurrence of their saturated and partially saturated derivatives in biologically active compounds and natural products such as nucleotide of NAD, pyridoxol (vitamin B6), and pyridine alkaloids [155]. Due to their ̟-stacking ability, some phenanthrolines are used in supramolecular chemistry [156]. Some compounds are used in pharmaceutics (as antimalarial, vasodilator, anaesthetic, anticonvulsant and antiepileptic), dyes, additives (as antioxidant), agrochemicals (as fungicidal, pesticidal, and herbicidal), veterinary (as anthelmintic, antibacterial and antiparasitic), and also in qualitative and quantitative analysis [157]. 1.6 Deoxyribose nucleic acids – DNA 1.6.1 History of DNA research
The history of DNA begins with the Greeks. Pythagoras the philosopher speculated around 500 BC that human life begins with a blend of male and female fluids, or semens, each originating from a part of the body. Later, Aristotle postulated that the semens were purified blood, therefore, was the element of heredity. Due to little advancements in science and though for over two thousand years, this concept persisted in the western world and was demonstrated by such common phrases as blue blood, blood-will-tell, blood relative, bad blood, and royal blood. In the 1860s, a monk named Gregor Mendel discovered that the differences between organisms such as colours of pea flowers were distributed among the offspring’s of a mating between two organisms in a regular way that can be understood only if the trait was determined as discrete entities, later called genes.
DNA was first isolated by the Swiss physician Friedrich Miescher who, in 1869, discovered a microscopic substance in the pus of discarded surgical bandages. It resided

Chapter 1
Department of Chemistry (SPU) Page 20
in the nuclei of cells called nuclein [158]. In 1919, Phoebus Levene identified the base, sugar and phosphate nucleotide unit [159]. Levene suggested that DNA consisted of a string of nucleotide units linked together through the phosphate groups. However, Levene thought the chain was short and the bases repeated in a fixed order. In 1937 William Astbury produced the first X-ray diffraction patterns, which showed that DNA had a regular structure [160].
In 1953, James D. Watson and Francis Crick suggested what is now accepted as the first correct double-helix model of DNA structure in the journal Nature [161]. Their double-helix, molecular model of DNA was then based on a single X-ray diffraction image [162] taken by Rosalind Franklin and Raymond Gosling in May 1952, as well as the information that the DNA bases are paired also obtained through private communications from Erwin Chargaff in the previous years. Chargaff's rules played a very important role in establishing double-helix configurations for B-DNA as well as A-DNA.
DNA's role in heredity was confirmed in 1952, when Alfred Hershey and Martha Chase in the Hershey–Chase experiment showed that DNA is the genetic material of the T2 phage [163]. This team of biologists grew a particular type of phage, known as T2, in the presence of two different radioactive labels so that the phage DNA incorporated radioactive phosphorus (32P), while the protein incorporated radioactive sulphur (35S). They allowed the labeled phage particles to infect non-radioactive bacteria and asked a very simple question: which label would they find associated with the infected cell? Their analysis showed that most of the 32P-label was found inside of the cell, while most of the 35S was found outside. This suggested to them that the proteins of the T2 phage remained outside of the newly infected bacterium while the phage-derived DNA was injected into the cell. They then showed that the phage derived DNA caused the infected cells to produce new phage particles. 1.6.2 The structure of DNA
The unit of a DNA molecule is the deoxyribose sugar, with a phosphate group, linked to one of the four bases. The bases are two pyrimidines; thymine (T) and cytosine (C) and two purines; adenine (A) and guanine (G). This unit is called a nucleotide. Minus the phosphate it is called a nucleoside. Levene’s model showed that the links between nucleotides were phosphodiesters from the 5’ carbon of one nucleotide to the 3’ carbon of the next nucleotide and that the bases were bound to the sugar through the 1’ carbon (Figure 1.6.1).
Figure 1.6.1: 3' and 5' units of DNA
OP O
O
O -
H 2 C
O-
O -
OH
OH
H
H
HH
H 2 C
H 2 C
HH
H
H
OHH
O
O
P OO
O
OPO H
H
H
H
OHH
O
HO

Chapter 1
Department of Chemistry (SPU) Page 21
1.6.3 Groove of DNA Twin helical strands form the DNA backbone. Another double helix may be
found by tracing the spaces, or grooves, between the strands. These voids are adjacent to the base pairs and may provide a binding site. As the strands are not directly opposite to each other, the grooves are unequally sized. The major groove, is 22 Å wide and the minor groove, is 12 Å wide [164]. The narrowness of the minor groove means that the edges of the bases are more accessible in the major groove. As a result, proteins like transcription factors that can bind to specific sequences in double-stranded DNA usually make contacts to the sides of the bases exposed in the major groove [165]. This situation varies in unusual conformations of DNA within the cell, but the major and minor grooves are always named to reflect the differences in size that would be seen if the DNA is twisted back into the ordinary B form.
Major and minor grooves
The strand backbones are closer together on one side of the helix than on the other. The major groove occurs where the backbones are far apart, the minor groove occurs where they are close together (Figure 1.6.2). The grooves twist around the molecule on opposite sides. Certain proteins bind to DNA to alter its structure or to regulate transcription (copying DNA to RNA) or replication (copying DNA to DNA). It is easier for these DNA binding proteins to interact with the bases (the internal parts of the DNA molecule) on the major groove side because the backbones are not in the way.
Figure 1.6.2: Minor groove and major groove of DNA
1.7 Binding modes of DNA
There are four different types of binding modes by which DNA can interact to metal complexes: i. Electrostatic binding: Electrostatic or external binding occurs when cations or cationic molecules are attracted to the anionic surface of DNA. Ions and charged metal complexes such as Na+ associate electrostatically with DNA by forming ionic or hydrogen bonds along the outside of the DNA double helix [166]. Although divalent cations would normally be expected to stabilize the DNA double helix by screening electrostatic repulsions, instead those high concentrations of transition metal cations

Chapter 1
Department of Chemistry (SPU) Page 22
destabilized the double helix, causing base unpairing, unstacking and backbone disorder at lower temperatures than observed with monovalent cations, or divalent alkaline earths. ii. Groove binding: It occurs when the shape of groove on DNA and Van der Waals force of interaction between the base pair and complex or a segment of complex are complementary fit to each other. Generally it occurs for the case of complexes having planar ligands. Some of the most commonly studied minor groove-binding compounds, such as distamycin A, netropsin, bisbenzimidazole dyes (Hoechst dyes), [Ru(phen)3]2+
[phen = phenanthroline], netropsin, berenil and DAPI (4',6-diamidino-2-phenylindole) are known to bind to the minor groove of DNA with A+T specificity and to cause widening of the minor grooves. Some major groove binders can be summarized as enantiomeric complexes Λ- and ∆-[Ru(bpy)2(pqx)](PF6)2 [pqx =2-(2’-pyridyl)quinoxaline] [167]. iii. Covalent binding and coordinate covalent binding: It occurs via replacement of the labile ligands by covalent binding to nitrogen base of the DNA. Such type of binding is observed for the case of complex when easily replaceable ligands like halides, aqua etc are present. Covalent binding in DNA is irreversible and invariably leads to complete inhibition of DNA processes and subsequently cell death. The widely used anticancer drug cis-platin obtains its cytotoxicity by forming coordinate covalent DNA intrastrand and interstrand cross-links as well as protein-DNA cross links in the cellular genome [168-172] iv. Intercalation: The complexes having planar aromatic portion which favour their insertion between the two base pairs resulting in the formation of sandwich like model can bind to DNA via intercalation mode [173]. It can be a partial intercalation and/or classical intercalation. Most of the metal based anticancer drugs interact with DNA via inter–strand coordinate covalent cross–linking as well as protein–DNA cross linking [174–177]. Intercalating molecules generally contain charged groups or metal ions, which make intercalation more favourable through electrostatic interactions between the intercalating molecule and the DNA [178]. 1.8 Superoxide dismutase
Although the enzymatic disproportionation of superoxide radical was discovered over last four decades, [179] the question can still be asked: what is superoxide dismutase? To begin with superoxide dismutase is typically an enzyme of organisms which utilize oxygen as the major electron acceptor. Univalent reduction of oxygen, with production of superoxide, is a biological reality [180] which appears to have led to the evolution of multiple superoxide dismutases as a safeguard against aberrant oxygen metabolism.
Superoxide dismutases (SODs) are a class of closely related enzymes that catalyze the breakdown of the superoxide anion into oxygen and hydrogen peroxide. SOD enzymes are present in almost all aerobic cells and in extracellular fluids. Superoxide dismutase enzymes contain metal ion cofactors that, depending on the

Chapter 1
Department of Chemistry (SPU) Page 23
isoenzyme, can be copper, zinc, manganese or iron. In humans, the copper/zinc SOD is present in the cytosol, while manganese SOD is present in the mitochondrion. There also exists a third form of SOD in extracellular fluids, which contains copper and zinc in its active sites. The mitochondrial isozyme seems to be the most biologically important of these three, since mice lacking this enzyme die soon after birth. In contrast, the mice lacking copper/zinc SOD are viable but have numerous pathologies and a reduced lifespan, while mice without the extracellular SOD have minimal defects (sensitive to hyperoxia). In plants, SOD isoenzymes are present in the cytosol and mitochondria, with an iron SOD found in chloroplasts that is absent from vertebrates and yeast [181,182]. 1.8.1 Copper-zinc SOD
Eukaryotic and prokaryotic cells accumulate essential first row transition metals for various cellular functions. Copper for instance, is maintained at a total intracellular concentration in the 1024 -1025 M range. Despite this abundance, it has been shown that copper ions are typically unavailable in the cytoplasm for direct substitution into metalloenzymes. In fact, the steady state concentration of the free or labile form of copper ion in the cytoplasm of yeast is far less than one ion per cell.
Cu2Zn2SOD is a well known homodimeric enzyme of 32000 Da that catalyzes the dismutation of the superoxide radical to hydrogen peroxide and oxygen through a two step reaction [183-185]: Cu2+ + O2
–• Cu+ + O2 Cu+ + O2
–• Cu2+ (O22–) 2H+ Cu2+ + H2O2
The active site of each subunit contains both zinc and copper ion. Copper occurs in the oxidized and in the reduced state, both of which are necessary for the function. The X-ray structure of the oxidized form has been available since 1982 for the bovine enzyme [186] and several other structures have become available [187-189]. Reduced state structures are also available although the picture is less clear-cut around the copper-binding site [190,191]. 1.9 Literature survey
The history of the fluoroquinolones is directly related to nalidixic acid, (1-ethyl-7-methyl-4-oxo-1,8-naphthyridine-3-carboxylic acid), the first quinolone to present anti-bacterial activity, was synthesized and patented in 1962 by Lescher et al [192]. De Souza et al., studied the fluoroquinolones constitute an important class of synthetic antimicrobial agents, which had been the objects of intensive study [193]. Norfloxacin, which patented in 1978, can be cited as the first fluoroquinolone to present potent anti-bacterial activity [194]. Macias et al., reported the numerous studies regarding the interaction between various quinolones with metallic cations [195]. Anacona research groups reported the antibacterial properties of metal complexes with fluoroquinolones [196]. Vieira et al., studied the platinum(II) complexes with fluoroquinolones [197]. Chen et al., reported the two molecules of the norfloxacin coordinate via the ketonic and carboxylic oxygen atoms and two other molecules coordinate by way of the terminal nitrogen of the piperazine [198]. Lomaestro and Bailie reported the detrimental effects of metal ions on absorption of drugs and proposed that the reduction in bioavailability is a consequence of complex formation in the gastric system [199]. Broad spectrum
Chapter 1
Department of Chemistry (SPU) Page 24
antibacterial activity of the fluoroquinolone family drugs is well–known, but Smith et al., reported that the divalent metal ion might affect the susceptibility of quinolones [200].
Mendoza-Diaz and Pannell studied the copper(II) complexes of nalidixic acid and oxolinic acid and suggested that the binding of copper(II) to nalidixic acid depends on the nature of other ligands present in solution [201]. Valisena et al., reported that the presence of Na+ or K+ ions does not affect the uptake and effectiveness of norfloxacin appreciably, but divalent ions causes a dramatic decrease in uptake and effectiveness of norfloxacin [202]. Mersch–Sundermann et al., reported that quinolone antibacterial drugs commonly used to treat urinary tract infections because of Gram(–ve) bacteria can cause severe damages to host DNA in the absence of exogenous metabolizing system [203].
Mitscher proposed that the quinolones target the bacterial enzyme gyrase–DNA complex, which is responsible for the supercoiling of bacterial DNA [204]. The interactions between metal ions and quinolones were extensively studied by Turel [205]. Ruíz et al., studied nuclease properties of several binary and ternary complexes of copper(II) with norfloxacin and 1,10-phenanthroline [206]. Jimenez-Garrido et al., established the ability of Cu(CPF)2(NO3)2.6H2O to cleave DNA. Their results not only showed that the complex behaves as an efficient chemical nuclease with ascorbate/hydrogen peroxide activation, but their mechanistic studies with different inhibiting reagents also reveal that hydroxyl radicals involved in the DNA scission process [207]. Sigman et al., documented the DNAase activity of copper phenanthroline complexes [208]. Ramirez-Ramirez et al., studied the [Cu(phen)(nal)]+ compound as a powerful nuclease capable of degrading plasmid DNA under reductive conditions, with an even stronger activity than that of the chemical nuclease copper phenanthroline [Cu(phen)2]2+ [209].
Deitz et al., studied the mechanism action of nalidixic acid on E. coli [210]. The studies indicated that nalidixic acid acts directly on the replication of DNA rather than on the "initiator" of DNA synthesis. Mechanism of norfloxacin involved inhibition of bacterial DNA gyrase, which was essential for DNA replication studies [211]. Morissey et al., explored that stereochemistry affects significantly the antibacterial activity since the S(-) ofloxacin isomer (levofloxacin) is 8–128 times more potent than R(+) ofloxacin [212]. The fluoroquinolones are used to treat infections such as urinary tract infections, lower respiratory tract infections, skin and skin-structure infections, soft tissue infections, urethral and cervical gonococcal infections, typhoid fever, prostatitis, acute sinusitis, bone-joint infections and community-acquired pneumonia [213]. Mixed ligands neutral mononuclear copper(II) complexes of phenanthroline with nalidixic acid, cinoxacin and ciprofloxacin were reported by Drevensek et al., [214], as well as ionic copper(II) complexes of protonated norfloxacin were reported by Turel et al [215]. The binding of ciprofloxacin to natural and synthetic polymeric DNA was investigated at different solvent conditions using a combination of spectroscopic and hydrodynamic techniques [216].
King et al., studied the modifications of nalidixic acid based on structure–activity relationships [217]. The structure and activity of certain quinolones and the interaction of their Cu(II) complexes on a DNA model were studied by Robles et al., and suggested that the intercalation of the quinolone complex to DNA was an important step in the

Chapter 1
Department of Chemistry (SPU) Page 25
processes [218]. Ruíz et al., studied the structure and chemical behaviour of several complexes of cinoxacin and ciprofloxacin, as well as the antimicrobial activity of some of their compounds [219]. The synthesis and physico-chemical properties of several fluoroquinolone compounds with their biological activity were reported by Macías et al [220]. The participation of intracellular metals in the activity of quinolones is strongly influenced by the metal environment, which can give rise to dramatic effects on their physicochemical properties [221]. DNA-gyrase or an interaction with the DNA molecule via a metal complex intermediate was studied by Crumpiin et al. They proposed that copper or iron complex could be involved in the interactions [222]. Crystal structures of mixed-ligand complexes of metal ions, quinolones, and N,N-donors were reported by Diaz et al [223]. Drevenšek et al., studied the mixed-valence Cu(II)/Cu(I) complex of quinolone ciprofloxacin isolated by a hydrothermal reaction in the presence of L-histidine and comparison of biological activities of various copper–ciprofloxacin compounds [224]. Song et al., pointed out that quinolone–Cu2+ binary complex can interact with DNA by intercalative binding mode, and Cu2+ plays an intermediary role [225]. Low molecular weight copper complexes were proven beneficial against several diseases such as tuberculosis, rheumatoid, gastric ulcers, and cancers [226]. Quinolones react with several metal ions and the crystal structures of boron, cadmium, calcium, cerium, cobalt, copper, iron, magnesium, nickel, silver and zinc complexes were reported by Turel [227].
From theoretical and experimental studies on the structural activity of certain quinolones, and the interaction of their Cu2+ complexes on a DNA model, suggested that the intercalation of the quinolone complex to DNA was an important step in the processes [228]. Liu et al., carried out synthesis, characterization and DNA-binding properties of Ln(III) complexes with gatifloxacin and indicated that the complexes and ligand bind to DNA via groove binding mode [229]. Pansuriya and Patel prepared the Fe(III) and Cu(II) mixed ligand complexes with ciprofloxacin and some neutral bidentate Schiff’s bases; and performed the antibacterial activity and DNA-binding studies [230,231]. The mononuclear metal complexes with ciprofloxacin have been prepared by Psomas (M= Mn2+, Fe3+, Co2+, Ni2+ and MoO2
2+) and evaluated DNA-binding properties [232]. Synthesis of fluoroquinolone metal complexes were carried out as an attempt to clarify their physico-chemical properties where as some antibacterial activity studies showed that the complexes allowed the alteration of the potency and specificity of fluoroquinolones [233]. Complexation equilibria of ciprofloxacin with proton and metal ions in aqueous-organic mixtures were studied by Sekhon et al [234]. Hydrothermal reactions of ciprofloxacin with Cu(ClO4)2�6H2O, and ofloxacin with Cu(CH3COO)2�4H2O have been carried out and the crystal structure and antibacterial activities of novel [Cu(H-Cip)2]�(ClO4)2�6H2O and [Cu(Ofl)2�H2O]�2H2O complexes were reported by Yu et al [235]. The role of transition metals, how they exert their action on biological systems and the coordinative behavior of quinolone drugs in complexes of the type [Cu(phen)(antib)]+ (where antib is a quinolone or fluoroquinolone) were explored by Mendoza-Díaz et al [236]. Pansuriya et al., synthesized and studied the biological aspects of Fe(II), Fe(III) and Cu(II) complexes with ciprofloxacin [237,238]. Refat carried out the synthesis and characterization of norfloxacin-Ag(I), Cu(II) and Au(III) complexes
Chapter 1
Department of Chemistry (SPU) Page 26
and showed moderate activity against the Gram (+ve) and Gram(–ve) bacteria as well as against fungi [239]. Chattah et al., characterized the aluminum complexes of norfloxacin and ciprofloxacin by NMR and IR spectroscopy [240,241]. Tan et al., studied the binding characteristics of gatifloxacin and human serum albumin by fluorescence spectroscopy in aqueous solution, and the interaction influenced by copper(II) ion [242]. Skrzypek et al., reported the synthesis and spectroscopic studies of iron(III) complex with pipemidic acid [243]. Overgaard et al., studied experimental electron density of a complex between copper(II) and ciprofloxacin [244]. Campbell et al., reported the interactions of norfloxacin with antacids and minerals, and concluded that the efficacy of norfloxacin may be compromised when it is taken concurrently with preparations containing ferrous sulphate, zinc sulphate, aluminum hydroxide and magnesium hydroxide ions [245]. Macias et al., reported the complexes of Ni(II), Cu(II), Co(II) and Zn(II) with ofloxacin [246,247]. Sissi et al., reported that “ciprofloxacin affects conformational equilibria of DNA gyrase A in the presence of magnesium ions” [248]. Alteration in activity of fluoroquinolone was proved by the wide spectrum of antimicrobial activity shown against Gram(+ve) and Gram(–ve) bacteria as well as against protozoans [249]. Lopez-Gresa et al., studied the interactions of metal ions (Cd2+, Co2+, Zn2+, Ni2+) with two quinolone antimicrobial agents (cinoxacin and ciprofloxacin) [250].
Tercera et al., studied the synthesis, characterization, solution equilibria and DNA binding of some mixed-ligand palladium(II) complexes. They also described the thermodynamic models for carboplatin drug and analogous compounds [251]. Häring et
al., studied the reactivity of palladium(II) complexes [252]. Rau et al., illustrated the reactions of the dichloroethylenediaminepalladium(II) with different ligands of biological interest were frequently used as models of those of the antitumor drug cis-diamminedichloroplatinum(II) [253]. Tercero-Moreno et al., simulated the behavior of [Pd(en)Cl2] in a variety of aqueous systems of biological interest. The simulations provide the information about the thermodynamically stable species that cis-DDP may produce under these conditions [254]. Nadeem et al., studied the synthesis, crystal structures, antibacterial and antiproliferative activities of palladium(II) complexes of triphenylphosphine and thioamides [255]. Rauterkus et al., studied cisplatin analogues with 2,2'-dipyridylamine ligands, their reactions with DNA model nucleobases and the hydrophobicity around the drug/DNA binding site [256]. Nyarko et al., studied the fluorescence and phosphorescence spectra of Au(III), Pt(II) and Pd(II) porphyrins with DNA at room temperature [257]. Vanderkooi et al., studied the palladium(II) complexes of porphyrins and related tetrapyrrolic pigments. [258]. Müller et al., studied the interaction of Pt(II) and Pd(II) complexes of terpyridine with 1-methylazoles [259]. Müller et al., studied the metal-binding behavior of four azole-based nucleobases surrogates as potential building blocks for metal-mediated base pairs [260]. Ternary complexes of palladium(II) with ethylenediamine and dicarboxylate ligands were studied by Tercero et al., and performed DNA binding activity [261]. Antibacterial and antiproliferative activities of palladium(II) complexes were studied by Nadeem et al., and illustrated that complexes showed significant activities in most of the cases against the tested bacteria as compared to that of a standard drug and no cytotoxic effects in brine shrimps lethality bioassay study [262]. The fluorescence and phosphorescence studies on

Chapter 1
Department of Chemistry (SPU) Page 27
the interactions of Au(III), Pt(II) and Pd(II) derivatives were studied by Nyarko et al., and reported the partial intercalation binding mode of DNA at high concentrations [263]. Mock et al., studied the reactions with nucleobases and cytotoxicity of palladium complexes and reported that the biological studies on the three novel compounds indicate the highest cytotoxicity for the most hydrophobic compound [264]. 1.10 Rationalization of research work
The rational drug design requires knowledge of the mechanism of action. To achieve specificity of biological activity and minimum toxic side-effects of drug, it is important to measure its effect on nucleic acid. Many microorganisms, nowadays, have developed resistance to common drugs. This resistance appears to be the result of one of three mechanisms: alterations in the quinolone enzymatic targets (DNA gyrase), decrease outer membrane permeability and the development of efflux mechanisms. The accumulation of several bacterial mutations (DNA gyrase and bacterial permeability) has been associated with the development of very high minimum inhibitory concentrations to the drugs. However, recent research has drawn our attention towards metal incorporation in rational drug design.
Approximately one third of proteins and enzymes require at least one metal ion to function properly, perhaps it is not surprising that metal complexes have a role to play in medicine as well. Medicinal inorganic chemistry is a discipline of growing significance in both therapeutic and diagnostic medicine. The successful use of metal complexes as therapeutic and diagnostic agents depends on the control of their kinetic and thermodynamic properties through appropriate choice of oxidation state, types and numbers of bound ligands, and coordination geometry. Metallo-organic complexes or chelates of copper have antibacterial/germicidal action, via the oligodynamic effect. Copper is known to be a natural antibiotic and used in prevention and control of a number of disease states in the body. Due to structural analogy between Pt(II) and Pd(II) complexes, the Pd(II) complexes of diaminocyclohexane, ammonia, pyridine and pyrimidines derivatives, alkylaminophosphine oxide, mercapto-imidazoles and pyrimidines have promising anti-proliferative, cytotoxic and anti-tumour activity.
Mixed-ligand complexes represent a novel set of highly active antibacterial agents. There is no enough literature available on metal complexes of quinolone family drugs and their interaction with DNA, although the problem of antibiotic resistance prompted much research in the design of novel antimicrobial agents. There is considerable interest in the DNA binding of metal complexes because of their application as DNA probes and as possible antitumor agents. Chemotherapy is an important approach in management of human cancer. So due to above biological role of metal complexes, some studies on copper(II) and palladium(II) complexes have been carried out to develop their chemistry towards artificial metallonucleases and DNA probes. 1.11 Outline of the thesis
This thesis deals with synthesis, characterization antimicrobial, DNA interaction and superoxide dismutase studies of mixed ligand copper(II) complexes with ciprofloxacin and neutral bidentate/tridentate ligands, as well as square planar

Chapter 1
Department of Chemistry (SPU) Page 28
palladium(II) complexes with neutral bidentate ligands. The entire work of the thesis is divided into five chapters. Chapter-1 deals with introduction, includes fluoroquinolone: an antibacterial agent, chemistry and biochemistry of copper and palladium, metal in medicine, nitrogen donor ligands, deoxyribose nucleic acids, binding modes of DNA, superoxide dismutase, literature survey and rationalization of work. Chapter-2 deals with the synthesis and characterization of ligands. The ligands have been characterized using elemental analysis, infrared spectroscopy, 1H NMR and 13C NMR spectroscopy. Chapter-3 contains the synthesis of copper(II) with terpyridines/phenanthrolines derivatives and ciprofloxacin, and palladium(II) complexes with bidentate ligands. Complexes have been characterised using elemental analysis, magnetic moment measurements, electronic/reflectance spectra, IR and mass spectroscopy. Chapter-4 deals with biological interphase of the synthesized Cu(II) complexes. It is divided into seven sections: 4.1 In-vitro antibacterial activity: This section deals with antibacterial activity of copper(II) complexes against three Gram(–ve) and two Gram(+ve) microorganisms in terms of minimum inhibitory concentration (MIC). 4.2 Bactericidal activity: This section includes the bactericidal activity of copper(II) complexes against three Gram(–ve) and two Gram(+ve) microorganisms in terms of colony forming unit. 4.3 Absorption titration technique: This section deals with the DNA binding activity of the copper(II) complexes with CT DNA. The results show that the complexes bind to DNA through intercalation mode and their intrinsic binding constants (Kb) are in the range of 104 M–1. 4.4 Viscosity measurements: This section concerns the viscosity measurements of DNA with the copper(II) complexes. It has been found that the viscosity of DNA increases steadily with the increase of the concentration of the complex, which suggests classical intercalation mode of binding. 4.5 DNA thermal denaturation: This section deals with thermal denaturation study of copper(II) complexes with CT DNA. 4.6 Gel electrophoresis technique: This section contains the DNA cleavage activity of copper(II) complexes towards pUC19 DNA. All the complexes show higher nuclease activity compare to ciprofloxacin and metal salt. 4.7 SOD-like activity: This section deals with the superoxide dismutase like activity of copper(II) complexes. The activity was performed using nonenzymatic NBT/NADH/PMS system in terms of IC50 value.
Chapter-5 deals with biological interphase of the synthesized Pd(II) complexes. It is divided into five sections:

Chapter 1
Department of Chemistry (SPU) Page 29
5.1 In-vitro antibacterial activity: This section deals with bacteriostatic activity (MIC) of palladium(II) complexes against three Gram(–ve) and two Gram(+ve) microorganisms. 5.2 Absorption titration technique: This section concerns with UV-Vis. absorption spectra of CT DNA in presence of palladium(II) complexes for determining their binding strength (Kb). The results show that the complexes bind to DNA by intercalation mode. 5.3 Viscosity measurements: This section deals with effect on viscosity of DNA in presence of palladium(II) complexes for determining their exact mode of binding. It has been found that the viscosity of DNA increases steadily with increasing the concentration of the complex. 5.4 DNA thermal denaturation: This section includes thermal denaturation study of palladium(II) complexes with CT DNA. 5.5 Gel electrophoresis technique: This section contains the DNA cleavage activity of palladium(II) complexes towards plasmid pUC19 DNA. All the complexes show higher nuclease activity compare to metal salt.
Chapter 1
Department of Chemistry (SPU) Page 30
1.12 References [1] G.Y. Lescher, E.D. Froelich, M.D. Gruet, J.H. Bailey, R.P. Brundage, J. Med.
Pharmaceut. Chem. 5 (1962) 1063. [2] D.C. Hooper, Biochim. et Biophys. Acta 1400 (1998) 45. [3] P. Ball, (1998). The quinolones: history and overview. In The Quinolones, 2nd
edn, (Andriole, V. T., Ed.), pp. 1–28. Academic Press, London. [4] P. Ball, A. Fernald, G. Tillotson, Expert. Opin. Invest. Drugs 7 (1998), 761. [5] P. Ball, L. Mandell, Y. Niki, G. Tillotson, Drug Safety 21 (1999) 407. [6] J.M. Domagala, J. Antimicrob. Chemother. 33 (1994) 685. [7] M.D. Blum, D.J. Graham, C.A. McCloskey, Clinical Infectious Disease 18 (1994)
946. [8] P. Ball, J. Antimicrob. Chemother. 45 (2000) 557. [9] G.S. Tillotson, J. Med. Microbio. 44 (1996) 320. [10] C.G. Dave, H.M. Joshipura India,n. J. Chem. 41 (2002) 650. [11] E.M. Scholar, Am. J. Pharm. Educ. 66 (2003) 165. [12] Y.-L. Chen, K.-C. Fang , J.-Y. Sheu, S.-L. Hsu, C.-C. Tzeng, J. Med. Chem, 44
(2001) 2374. [13] J.-H. Liu, H.-Y. Guo, J. Med. Chem. 35 (1992) 3469. [14] H. Kondo, M. Taguchi, Y. Inoue, F. Sakamato, G. Tsukamoto, J. Med. Chem. 33
(1990) 2012. [15] L.E. Nicolle, "Use of quinolones in urinary tract infection and prostatitis," in The
Quinolones, Academic Press, New York NY, pp. 183-202, 1998. [16] G.Y. Lesher, E.J. Foelich, M.D. Garnett, J.H. Baily, P.R. Brundage, J. Med. Chem.
5 (1962) 259. [17] P. Ball, J. Antimicrob. Chemother. 46 (2000) 17. [18] G.E. Stein, Clin. Infect. Dis. 23 (1996) 19. [19] G.E. Stein, D.H. Havlichek, Postgrad. Med. 103 (1998) 67. [20] D.E. King, M.D.R. Malone, D. Pharm. S.H. Lilley, Med. Lett. Drugs Ther.
(2000) 15. [21] Sparfloxacin and levofloxacin. Med Lett Drugs Ther 1997;39:41-4. [22] P.S. Lietman, Drugs 49 (1995) 159. [23] Zagam (sparfloxacin). Collegeville, Rhône-Poulenc Rorer Pharmaceuticals Inc.,
1997. [24] K.E. Brighty, T.D. Gootz, J. Antimicrob. Chemother. 39 (1997) 1. [25] Trovan (trovafloxacin). New York, N.Y.: Pfizer Inc., 1998. [26] http://www.fda.gov/cder/ news/trovan/trovan-advisory.htm. [27] S.R. Norrby, P.S. Lietman, Drugs 45 (1993) 59. [28] G.E. Stein, Clin. Infect. Dis. 23 (1996) 19. [29] G. Milkovich, J.F. Reitan, Med. Pharm. Forum (1998) 17. [30] P.G. Ambrose, R.C. Owens, R. Quintiliani, C.H. Nightingale, Conn. Med. 61
(1997) 269. [31] J.F. Acar, F.W. Goldstein, Clin. Infect. Dis. 24 (1997) 67. [32] M.E. Ernst, E.J. Ernst, M.E. Klepser, Am. J. Health Syst. Pharm. 54 (1997) 2569. [33] P.C. Appelbaum, Drugs 49 (1995) 76.
Chapter 1
Department of Chemistry (SPU) Page 31
[34] D.W. Hecht, H.M. Wexler, Clin. Infect. Dis. 23 (1996) 2. [35] K. Drlica, X. Zhao, Microbiol. Mol. Biol. Rev. 61 (1997) 377. [36] M.J. Robinson, B.A. Martin, T.D. Gootz, P.R. McGuirk, N. Osheroff,
Antimicrob. Agents Chemother. 36 (1992) 751. [37] C. Sissi, M. Palumbo, Curr. Med. Chem. Anticancer Agents 3 (2003) 439. [38] P. Hussy, G. Maass, B. Tümmler, F. Grosse, U.P. Schomburg, Antimicrob.
Agents Chemother. 29 (1986) 1073. [39] http://www.jstor.org/pss/4454399. [40] A. Forsgren, A. Bredberg, A.B. Pardee, S.F. Schlossman, T.F. Tedder,
Antimicrob. Agents Chemother. 31 (1987) 774. [41] T.D. Gootz, J.F. Barrett, J.A. Sutcliffe, Antimicrob. Agents Chemother. 34 (1990)
8. [42] J.W. Lawrence, S. Darkin-Rattray, F. Xie, A.H. Neims, T.C. Rowe, J. Cell.
Biochem. 51 (1993) 165. [43] S.H. Elsea, N. Osheroff, J.L. Nitiss, J. Biol. Chem. 267 (1992) 13150. [44] M.J. Suto, J.M. Domagala, G.E. Roland, G.B. Mailloux, M.A. Cohen, J. Med.
Chem. 35 (1992) 4745. [45] H. Enzmann, C. Wiemann, H.J. Ahr, G. Schlüter,. Mutat. Res. 425 (1999) 213. [46] Y. Kashida, Y.F. Sasaki, K. Ohsawa, Toxicol. Sci. 69 (2002) 317. [47] A. Thomas, J. Tocher, D.I. Edwards,. J. Antimicrob. Chemother. 25 (1990) 733. [48] http://www.academy.org.uk/pharmacy/fluoroq.htm. [49] Y.A. Al-Soud, N.A. Al-Masoudi, J. Braz. Chem. Soc. 14 (2003). (Page number) [50] Y.A. Al-Soud, N.A. Al-Masoudi, J. Braz. Chem. Soc. 14 (2003) 790. [51] J.F. Acar, F.W. Goldstein, Clin. Infect. Dis. 24 (1997) 67. [52] G.E. Stein, D.H. Havlichek Postgrad. Med. 103 (1998) 67. [53] J.S. Wolfson, D.C. Hooper, Clin. Microbiol. Rev. 2 (1989) 378. [54] W.G. Streuff, S.G. Bovine, United States Patent 5, 286, 754. [55] J.M. Nelson, T.M. Chiller, J.H. Powers, F.J. Angulo, Clin. Infect. Dis. 44 (2007)
977. [56] S. Kawahara, Nippon Rinsho 56 (1998) 3096. [57] J.G. Cooper, K. Harboe, S.K. Frost, J.G. Skadberg, Bio. Med. J. 330 (2005) 1002. [58] Hooper D. Quinolones. In: Mandell GL, Bennett JE, Dolin R. Mandell, Douglas,
and Bennett's Principles and practice of infectious diseases. 5th ed. Philadelphia: Churchill Livingstone, 2000:404–23.
[59] D.C. Hooper, Clin. Infect. Dis. 30 (2000) 243. [60] D.C. Hooper, J.S. Wolfson, Engl. J. Med. 324 (1991) 384. [61] G.D. Fang, C. Brennen, M. Wagener, D. Swanson, M. Hilf, L. Zadecky,
Antimicrob. Agents Chemother. 35 (1991) 1849. [62] http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/019537s073
020780s030lbl.pdf. [63] http://books.google.de/books?id=cItuoO9zSjkC&pg=PA623. [64] http://www.csa.com/discoveryguides/copper/overview.php. Retrieved 2008-09-
12. [65] R.W. Hesse. Greenwood Publishing Group (2007) 56. [66] H.H.A. Dollwet, J.R.J. Sorenson, Trace Elements in Medicine 2 (1985) 80.
Chapter 1
Department of Chemistry (SPU) Page 32
[67] G.J. Brewer, J. Am. College Nutrit. 28 (2009) 238. [68] H. Tapiero, D.M. Townsend, K.D. Tew, Biomed. & Pharmacother. 57 (2003) 386. [69] http://books.google.de/books?id=cItuoO9zSjkC&pg=PA623. [70] http://www.copper.org/consumers/health/papers/cu_health_uk/cu_healthuk.ht
ml. [71] D.C. Washington, Copper. In: Recommended Dietary Allowances.: National
Research Council, Food Nutrition Board, NRC/NAS. 1980. pp. 151–154. [72] M. Bonham, J.M. O’Connor, B.M. Hannigan, British J. Nutrition. 87 (2002) 393. [73] J.O. Noyce, H. Michels, C.W. Keevil, J. Hosp. Infect. 63 (2006) 289. [74] J.O. Noyce, H. Michels, C.W. Keevil, Appl. Environ. Microbiol. 72 (2006) 4239. [75] S. Mehtar, I. Wiid, S.D. Todorov, J. Hosp. Infect. 68 (2008) 45. [76] V.A. Gant, M.W. Wren, M.S. Rollins, A. Jeanes, S.S. Hickok, T.J. Hall, J.
Antimicrob. Chemother. 60 (2007) 294. [77] J.O. Noyce, H. Michels, C.W. Keevil, Appl. Environ. Microbiol. 73 (2007) 2748. [78] http://www.epa.gov/pesticides/factsheets/copper-alloy-products.html. [79] A. Venturini, J. Gonzalez, J. Org. Chem. 67 (2002) 9089. [80] C.M.L. Delpiccolo, E.G. Mata, Tetrahedron: Asymmetry 13 (2002) 905. [81] W.P. Griffith. Platinum Metals Review 47 (2003) 175. [82] W.H. Wollaston, Royal Society of London 94 (1804) 419. [83] C.R. Hammond (2004). The Elements, in Handbook of Chemistry and Physics
81st edition. CRC press. ISBN 0849304857. [84] K. Akdi, R. Vilaplana, S. Kamah, J. Navarro, J. Salas, F. Gonzalez-Vilchez, J.
Inorg. Biochem. 90 (2002) 51. [85] J. Kuduk-Jaworska, A. Puszko, M. Kubiak, M. Pelczynska, J. Inorg. Biochem. 98
(2004) 1447. [86] M.E. Cooley, L.E. Davis, , M. DeStefano, J. Abrahm, Cancer Nursing 17 (1994)
173. [87] A.H. Calvert, D.R. Newell, L.A. Gumbrell, S. O'Reilly, M. Burnell, F.E. Boxall,
Z.H. Siddik, I.R. Judson, M.E. Gore, E. Wiltshaw, J. Clinical Oncology 7 (1989) 1748.
[88] E. Tiekink (2003). Gold derivatives for the treatment of cancer. World Gold Council. [89] T.S. Lobana, R. Verma, G. Hundal, A. Castineiras. Polyhedron 19 (2000) 899. [90] J . Reedijk, Proc. Natl. Acad.Sci. USA 100 (2003) 3611. [91] M.A. Jakupec, M. Galanski, B.K. Keppler, Revs. Physiol. Biochem. Pharmacol.
146 (2003) 1. [92] L. Ronconi, P.J. Sadler, Cood. Chem. Revs. 251 (2007) 1633. [93] S.J. Berners-Price, R. Norman, P.J. Sadler J. Inorg. Biochem 31 (1987) 197. [94] O.H. Amin, L.J. Al-Hayaly, S.A. Al-Jibori, T.A.K. Al-allaf Polyhedron 23 (2004)
2013. [95] P. Sadler, J. Inorg. Biochem. 67 (1997) 1. [96] T. Hambley, Coord. Chem. Revs. 166 (1997) 181. [97] M.A. Jakupec, M. Galanski, B.K. Keppler, Revs. Physio. Biochem. Pharmacol.
146 (2003) 1. [98] J. Kuduk-Jaworska, A. Puszko, M. Kubiak, M. Pelczynska, J. Inorg. Biochem. 98
(2004) 1447.

Chapter 1
Department of Chemistry (SPU) Page 33
[99] J. Schurig, H. Meinema, K. Timmer, B. Long, A. Casazza, Prog. Clin. Biochem. Med. 10 (1989) 205.
[100] J.R.R. da Silva, R.J.P. Williams, The Biological Chemistry of the Elements: The Inorganic Chemistry of Life. Clarendon Press, New York, 1991.
[101] P.J. Sadler, Adv. Inorg. Chem. 36 (1991) 1. [102] S. Budavari, ed., The Merck Index, 13th ed., Merck & Co., Rahway, NJ, 2001. [103] C.A. Claussen, E.C. Long, Chem. Rev. 99 (1999) 2797. [104] B. Jesse, R.L. Mary, J. Nutr. Biochem. 15 (2004) 316. [105] P.Z. Björn, H.D. Hermann, L. Max, S. Heide, K.G. Barabara, D. Hartmut, Sci.
Total Environ. 302 (2003) 127. [106] C.M. Galhardi, Y.S. Diniz, L.A. Faine, H.G. Rodrigues, R. C. Burneiko, B.O.
Ribas, E.L. Novelli, Food Chem. Toxicol. 42 (2004) 2053. [107] G. Oberdörster, E. Oberdörster, J. Oberdörster, Nanotoxicology 113 (2005) 823. [108] K. Donaldson, X.Y. Li, N.W. Mac, J. Aerosol Sci. 29 (1998) 553. [109] A. Whitehead, N. Stallard, Altern. Lab. Anim. 32 (2004) 73. [110] http://www.merck.com/mmpe/sec01/ch005/ch005c.html?qt=copper%
20and%20milk&alt=sh. Retrieved 2008. [111] http://pmep.cce.cornell.edu/profiles/extoxnet/carbaryl-dicrotophos/copper-
sulfate-ext.html. [112] http://members.vol.at/schmiede/MsgverSSt.html. Retrieved 2007-08-15. [113] U.K. Häring, R.B. Martin, Inorg. Chim. Acta 78 (1983) 25. [114] T. Rau, R. van Eldik, in: H. Sigel, A. Sigel (Eds.), Metal Ions in Biological Systems,
vol. 31, Marcel Dekker, New York, 1996, p. 339. [115] B.T. Khan, J. Bhatt, K. Najmoddin, S. Shamsuddin, K. Annapoorna, J. Inorg.
Biochem. 44 (1991) 55. [116] C. Navarro-Eanninger, J.M. Perez, F. Zamora, V.M. Gonzales, J.M. Masaguer,
C. Alonso, J. Inorg. Biochem. 52 (1993) 37. [117] I. Brudzinska, Y. Mikata, M. Obata, C. Ohtsuki, S. Yano, Bioorg. Med. Chem.
Lett. 14 (2004) 2533. [118] A. Garoufis, S.K. Hadjikakou, N. Hadjiliadis, Coord. Chem. Rev. 253 (2009)
1384. [119] W. Guerra, E.A. Azevedo, A.R. de Souza Monteiro, M. Bucciarelli- Rodriguez, E.
Chartone-Souza, A.M.A. Nascimento, A.P. Soares Fontes, L. Le Moyec, E.C. Pereira- Maia, J. Inorg. Biochem. 99 (2005) 2348.
[120] L.M.M. Vieira, M.V. de Almeida, M.C.S. Lourenco, F.A.F.M. Bezerra, A.P.S. Fontes, Eur. J. Med. Chem. 44 (2009) 4107.
[121] D. Kovala-Demertzi, M.A. Demertzis, J.R. Miller, C. Papadopoulou, C. Dodorou, G. Filousis, J. Inorg. Biochem. 86 (2001) 555.
[122] R.R. Coombs, M.K. Ringer, J.M. Blacquiere, J.C. Smith, J.S. Neilsen, Y.-S. Uh, J.B. Gilbert, L.J. Leger, H. Zhang, A.M. Irving, S.L. Wheaton, C.M. Vogels, S.A. Westcott, A. Decken, F.J. Baerlocher, Trans. Met. Chem. 30 (2005) 411.
[123] M.A. Ali, A.H. Mirza, R.J. Butcher, K.A. Crouse, Trans Met Chem 31 (2006) 79. [124] N.M. Aghatabay, M. Somer, M. Senel, B. Dulger, F. Gucin, Eur. J. Med. Chem.
42 (2007) 1069.
Chapter 1
Department of Chemistry (SPU) Page 34
[125] M.K. Biyala, K. Sharma, M. Swami, N. Fahmi, R. Vir Singh, Transition Met. Chem. 33 (2008) 377.
[126] M. Das, S.E. Livingstone, Br. J. Cancer 37 (1978) 466. [127] E. Bermejo, R. Carballa, A. Castineiras, R. Dominguez, A.E. Liberta, C.
Maichelle-Mössmer, M.M. Salberg, D.X. West, Eur. J. Inorg. Chem. (1999) 965. [128] A.G. Quiroga, J.M. Perez, I. Lopez-Solera, J.R. Masaguer, A. Luque, P. Roman,
A. Edwaeds, C. Alonso, C. Navarro-Ranninger, J. Med. Chem. 41 (1998) 1399. [129] S.F. Meek, G.C. Harrold and C.P. McCord, Indust. Med. Surg. 12 (1943) 447. [130] G. Orestano, Bull. Sot. Ital. Biol. Spec. 8 (1933) 1154. [131] D.M. Shishniashvili, V.N. Lystaov and Y.U. Moshkovskii, Chem. Abstr., 77
(1972) 149. [132] H.A. Schroeder, U.S. Govt. Res. Develop. Reports 70 (1970) 57. [133] S.S.R. Rapaka, K. Sorensen, S.D. Lee and R.S. Bhatnagar, Biochim. Biophys.
Acta 429 (1976) 63. [134] Y. Kawata, M. Shiota, , H. Tsutsui, , Y. Yoshida, , H. Sasaki, , and Y. Kinouchi, J.
Dent. Res. 60 (1981) 1403. [135] T.Z. Liu, Free Radic. Biol. Med. 23 (1997)155. [136] C.K. Pillai, Biochem. Biophys. Acta 474 (1977) 11. [137] G.M. Kolesova, Vopr. Med. Khim. 25 (1979) 537. [138] J.D. Spikes, C.F. Hodgson, Biochem. Biophys. Res. Commun. 35 (1969) 420. [139] M.D. Shultz, J.P. Lassig, M.G. Gooch, B.R. Evans, J. Woodward, Biochem.
Biophys. Res. Commun. 209 (1995) 1046. [140] A.M. Al-roubaie, Fogorv Sz 79 (1986) 207. [141] D. Downey, Contact Dermatitis, 21 (1989)54. [142] J.A. Marcusson, Contact Dermatitis, 34 (1996) 320. [143] Lide, David R. (1998), Handbook of Chemistry and Physics (87 ed.), Boca Raton,
FL: CRC Press, pp. 3–510 [144] K.T. Potts, P. Ralli, G. Theodoridis, P. Winslow, Colloids 7 (1990) 476. [145] J.-M. Lehn, Supramolecular Chemistry, Concepts and Perspectives, VCH,
Weinheim, 1995. [146] F. Vögtle, Editor, Supramolecular Chemistry: An Introduction, J. Wiley and Sons,
1993. [147] E.C. Constable, Adv. Inorg. Chem. Radiochem. 30 (1986) 69. [148] J.P. Sauvage, J.P. Collin, J.C. Chambron, S. Guillerez, C. Coudret, V. Balzani, F.
Barigelletti, L. De Cola, L. Flamigni, Chem. Rev. 94 (1994) 993. [149] E.C. Constable, Adv. Inorg. Chem. Radiochem. 30 (1986) 69. [150] J.P. Sauvage, J.P. Collin, J.C. Chambron, S. Guillerez, C. Coudret, V. Balzani, F.
Barigelletti, L. De Cola, L. Flamigni, Chem. Rev. 94 (1994) 993. [151] U.S. Schubert, C. Eschbaumer, P. Andres, H. Hofmeier, C.H. Weidl, E.
Herdtweck, E. Dulkeith, A. Morteani, N.E. Hecker, J. Feldmann, Synth. Met. 121 (2001) 1249.
[152] A.L. Gavrilova, B. Bosnich, Chem. Rev. 104 (2004) 349. [153] B.E. Halcrow, W.O. Kermack J. Chem. Soc. 43 (1946) 155. [154] K. Warnmark, J.A. Thomas, O. Heyke, J.-M. Lehn, Chem. Commun. (1996) 701.

Chapter 1
Department of Chemistry (SPU) Page 35
[155] M. Adib, H. Tahermansouri, S.A. Koloogani, B. Mohammadia, H.R. Bijanzadeh, Tetrahedron Lett. 47 (2006) 5957.
[156] Z.C. Watson, N. Bampos, J.K.M. Sanders, New J. Chem. (1998) 1135. [157] B.Y. Kim, J.B. Ahn, H.W. Lee, S.K. Kang, J.H. Lee, J.S. Shin, S.K. Ahn, C.I.
Hong, S.S. Yoon, Eur. J. Med. Chem. 39 (2004) 433. [158] A. Sayre (1975) Rosalind Franklin and DNA. New York: WW Norton & Co. [159] P. Levene, J. Biol. Chem. 40 (1919) 415. [160] A. Hershey, M. Chase, J. Gen. Physiol. 36 (1952) 39. [161] J.D. Watson, F.H.C. Crick, Nature 171 (1953) 737. [162] F. Rosalind, G. Raymond, Nature 171 (1953) 740. [163] A. Hershey, M. Chase, J. Gen. Physiol. 36 (1952) 39. [164] R. Wing, H. Drew, T. Takano, C. Broka, S. Tanaka, K. Itakura, R. Dickerson,
Nature 287 (1980) 755. [165] C. Pabo, R. Sauer, Annu. Rev. Biochem. 53 (1984) 293. [166] R.V. Gessner, G.J. Quigley, A.H.J. Wang, G.A. Van der Marel, J.H. Van Boom,
A. Rich, Biochemistry 24 (1985) 237. [167] A. Garoufis, G. Malandrinos, N. Hadjiliadis, Eur. J. Inorg. Chem. 16 (2004) 3326. [168] P. Nagababu, S. Satyanarayana, Polyhedron 26 (2007) 1686. [169] Q.-L. Zhang, J.-G. Liu, H. Xu, H. Li, J.-Z. Liu, H. Zhou, L.-H. Qu, L.-N. Ji,
Polyhedron 20 (2001) 3049. [170] R. Rao, A.K. Patra, P.R. Chetana, Polyhedron 26 (2007) 5331. [171] S. Banerjee, S. Mondal, W. Chakraborty, S. Sen, R. Gachhui, R.J. Butcher,
A.M.Z. Slawin, C. Mandal, S. Mitra, Polyhedron 28 (2009) 2785. [172] Q. Wang, W. Li, F. Gao, S. Li, J. Ni, Z. Zheng, Polyhedron 29 (2010) 539. [173] K.W. Jennette, S.J. Lippard, G.A. Vassiliades, W.R. Bauer, Pro. Nat. Acad. Sci.
USA 71 (1974) 3839. [174] P. Perego, L. Gatti, C. Caserini, R. Supino, D. Colangelo, R. Leone, S. Spinelli,
N. Farrell, F. Zunino, J. Inorg. Biochem. 77 (1999) 59. [175] H. Rauter, R.D. Di, E. Menta, A. Oliva, Y. Qu, N. Farrell, Inorg. Chem. 36
(1997) 3919. [176] P.K. Wu, Y. Qu, B. van Houten, N. Farrell, J. Inorg. Biochem. 54 (1994) 207. [177] A. Eastman, Chem. Biol. Int. 61 (1987) 241. [178] D.Y. Sun, M. Hansen, J.J. Clement, L.H. Hurley, Biochemistry 32 (1993) 8068. [179] J.M. McCord I. Fridovich, J. Biol. Chem. 244 (1969) 6049. [180] A. Boveris, Adz. Expd. Med. Biol. 78 (1977) 67. [181] K. Puget, A.M. Michehon, Biochem. Biephys. Res. Commun. 58 (1974) 830. [182] P.M. Vignais, M.-F. Henry, A. Terech, J. Chabert, Arch. Biochem. Biophys. 4
(1980) 154. [183] I. Fridovich, Adv. Enzymol. Relat. Areas Mol. Biol. 58 (1986) 61. [184] B. Halliwell, & J.M. Gutteridge, (1989) Free Radicals in Biology and Medicine.
Clarendon Press, Oxford pp. 22-408. [185] J.A. Fee, B.P. Gaber, J. Biol. Chem. 247 (1972) 60. [186] J.A. Tainer, E.D. Getzoff, J.S. Richardson, D.C. Richardson, Nature 306 (1983)
284.

Chapter 1
Department of Chemistry (SPU) Page 36
[187] I. Bertini, S. Mangani, M.S. Viezzoli, (1998) Structure and properties of copper/zinc superoxide dismutases. In Advanced Inorganic Chemistry (Sykes, A.G., ed.), pp. 127-250. Academic Press, San Diego, CA, USA.
[188] A. Battistoni, S. Folcarelli, G. Rotilio, C. Capasso, A. Pesce, M. Bolognesi, A. Desideri, Protein Sci. 5 (1996) 2125.
[189] C.K. Djinovic, A. Battistoni, M. Carrõ, F. Polticelli, A. Desideri, G. Rotilio, A. Coda, K.Wilson, M. Bolognesi, Acta Cryst. 52 (1996) 176.
[190] W.R. Rypniewski, S. Mangani, B. Bruni, P.L. Orioli, M. Casati, K.S. Wilson, J. Mol. Biol. 251 (1995) 282.
[191] N.L. Ogihara, H.E. Parge, J.P. Hart, M.S. Weiss, J.J. Goto, B.R. Crane, J. Tsang, K. Slater, J.A. Roe, J.S. Valentine, D. Eisenberg, J.A. Tainer, Biochemistry 35 (1996) 2316.
[192] G.Y. Lescher, E.D. Froelich, M.D. Gruet, J.H. Bailey, R.P. Brundage, J. Med. Pharm. Chem. 5 (1962) 1063.
[193] M.V.N. de Souza, M.V. de Almeida, A.D. da Silva, M.R.C. Couri, Curr. Med. Chem. 10 (2003) 21.
[194] P.C. Appelbaum, P.A. Hunter, Int. J. Antimicrob. Agents 16 (2000) 5. [195] B. Macias, M.V. Villa, M. Sastre, A. Castiñeiras, J. Borrás, J. Pharm. Sci. 91
(2002) 2416. [196] J.R. Anacona, C. Toledo, Trans. Met. Chem. 26 (2001) 228. [197] L.M.M. Vieira, M.V. de Almeida, H.A. de Abreu, H.A. Duarte, R.M. Grazul,
A.P.S. Fontes, Inorg. Chim. Acta 362 (2009) 2060. [198] Z.F. Chen, R.G. Xiong, J. Zhang, X.T. Chen, Z.L. Xue, X.Z. You, Inorg. Chem.
40 (2001) 4075. [199] B.M. Lomaestro, G.R. Bailie, Ann. Pharmacother. 25 (1991) 1249. [200] S.M. Smith, R.H. Eng, C.E. Cherubin, Chemotherapy 34 (1988) 308. [201] G. Mendoza-Diaz, K.H. Pannell, Inorg. Chim. Acta 152 (1988) 77. [202] S. Valisena, M. Palumbo, C. Parolin, G. Palu, G.A. Meloni, Biochem. Pharmacol
1990, 40, 431. [203] V. Mersch–Sundermann, K.H. Hauff, P. Braun, W. Lu, Int. J. Oncol. 5 (1994)
855. [204] L.A. Mitscher, Chem. Rev. 105 (2005) 559. [205] I. Turel, Coord. Chem. Rev. 232 (2002) 27. [206] P. Ruíz, R. Ortiz, L. Perelló, G. Alzuet, M. González-Á lvarez, M. Liu-González,
F. Sanz-Ruíz, J. Inorg. Biochem. 101 (2007) 831. [207] N. Jiménez-Garrido, L. Perelló , R. Ortiz, G. Alzuet, M. González- Álvarez, E.
Cantón, M. Liu-González, S. García-Granda, M. Pérez- Priede, J. Inorg. Biochem. 99 (2005) 677.
[208] D.S. Sigman, A. Mazumder, D.M. Perrin, Chem. Rev. 93 (1993) 2295. [209] N. Ramirez-Ramirez, G. Mendoza-Díaz, F. Gutiérrez-Corona, M. Pedraza-Reyes,
J. Biol. Inorg. Chem. 3 (1998) 188. [210] W.H. Deitz, T.M. Cook, W.A. Goss, J. Bacteriol. 91 (1966) 768. [211] L.L. Shen, J. Biol. Chem. 264 (1989) 2973. [212] I. Morrissey, K. Hoshino, K. Sato, A. Yoshida, I. Hayakawa, M.G. Bures, L.L.
Shen, Antimicrob. Agents Chemother. 40 (1996) 1775.

Chapter 1
Department of Chemistry (SPU) Page 37
[213] D.T.W. Chu, P.B. Fernandes, In Advances in Drug Research; Testa B (Ed), Academic: London, 1991, Vol. 21, pp 39–144.
[214] P. Drevensek, I. Leban, I. Turel, G. Giester, E. Tillmanns, Acta Crystallogr., Sect. C 59 (2003) 376.
[215] I. Turel, K. Gruber, I. Leban, N. Bukovec, J. Inorg. Biochem. 61 (1996) 197. [216] I.D. Vilfan, P. Drevenšek, I. Turel, N.P. Ulrih, Biochim. Biophys. Acta 1628
(2003) 111. [217] D.E. King, R. Malone, S.H. Lilley, Am. Fam. Physician 61 (2000) 2741. [218] J. Robles, J. Martin Polo, L.Á. Valtierra, L. Hinojosa, G. Mendoza-Díaz, Metal
Based Drugs 7 (2000) 301. [219] M. Ruíz, R. Ortiz, L. Perelló, A. Castiñeiras, Acta Cryst. C 55 (1999) 878. [220] B. Macías, M.V. Villa, M. Sastre, A. Castiñeiras, J. Borrás J. Pharm. Sci. 91 (2002)
2416. [221] G. Mendoza-Díaz, R. Pérez-Alonso, R. Moreno-Esparza, J. Inorg. Biochem. 64
(1996) 207. [222] G.C. Crumpiin, J.M. Midgley, J.T. Smith, Top. Antibiot. Chem. 8 (1980) 9. [223] G.M. Diaz, L.M.R. Martinez-Aguilera, R.M. Esparza, K.H. Panell, F.C. Lee, J.
Inorg. Biochem. 50 (1993) 65. [224] P. Drevenšek, T. Zupancic, B. Pihlar, R. Jerala, U. Kolitsch, A. Plaper, I. Turel, J.
Inorg. Biochem. 99 (2005) 432. [225] G.W. Song, Y. He, Z.X. Cai, J. Fluoresc. 14 (2004) 705. [226] D.H. Brown, A.E. Lewis, W.E. Smith, J.W. Teape, J. Med. Chem. 23 (1980) 729. [227] I . Turel, Coord. Chem. Rev. 232 (2002) 27. [228] J. Robles, J. Martin-polo, L. Alvarez-Valtierra, L. Hinojosa, J. Mendoza-diaz,
Metal Based Drugs 7 (2000) 301. [229] T. Liu, H. Lu, P. Xi, X. Liu, Z. Xu, F. Chen, Z. Zeng, J. Biomol. Struct. Dyn. 26
(2008) 293. [230] P.B. Pansuriya, M.N. Patel, J. Enzyme Inhib. Med. Chem. 23 (2008) 230. [231] P.B. Pansuriya, M.N. Patel, J. Enzyme Inhib. Med. Chem. 23 (2008) 108. [232] G. Psomas, J. Inorg. Biochem. 102 (2008) 1798. [233] L.D. Ross, M.C. Riley, J Pharm Biomed Anal, 12 (1994) 1325. [234] B.S. Sekhon, J. Srivastava, S. Kaur, S.K. Randhawa, J. Indian Chem. Soc. 85
(2008) 200. [235] L.C. Yu, Z.L. Tang, P.G. Yi, S.L. Liu, X. Li, J. Coord. Chem. 61 (2008) 2961. [236] G. Mendoza-Díaz, L.M.R. Martínez-Aguilera, R. Pérez-Alonso, X. Solans, R.
Moreno-Esparza, Inorg. Chim. Acta 138 (1987) 41. [237] P.B. Pansuriya, M.N. Patel, Appl. Organomet. Chem. 21 (2007) 926. [238] P.B. Pansuriya, M.N. Patel, Appl. Organomet. Chem. 21 (2007) 739. [239] M.S. Refat, Spectrochim. Acta Part A 68 (2007) 1393. [240] P. Ruiz, R. Ortiz, L. Perello, G. Alzuet, M. Gonzalez-Alvarez, M. Liu-Gonzalez,
F. Sanz-Ruiz, J. Inorg. Biochem. 101 (2007) 831. [241] A.K. Chattah, Y.G. Linck, G.A. Monti, P.R. Levstein, S.A. Breda, R.H. Manzo,
M.E. Olivera, Magn. Reson. Chem. 45 (2007) 850. [242] F. Tan, M. Guo, Q.S. Yu, Spectrochim. Acta Part A 61 (2005) 3006.
Chapter 1
Department of Chemistry (SPU) Page 38
[243] D. Skrzypek, B. Szymanska, D. Kovala-Demertzi, J. Wiecek, E. Talik, M.A. Demertzis, J. Phys. Chem. Solids 67 (2006) 2550.
[244] J. Overgaard, I. Turel, D.E. Hibbs, Dalton Trans. 21 (2007) 2171. [245] N.R. Campbell, M. Kara, B.B. Hasinoff, W.M. Haddara, D.W. McKay, Br. J.
Clin. Pharmacol. 33 (1992) 115. [246] B. Macias, M.V. Villa, I. Rubio, A. Castineiras, J. Borras, J. Inorg. Biochem. 84
(2001) 163. [247] B. Macias, M.V. Villa, M. Sastre, A. Castineiras, J. Borras, J. Pharm. Sci. 91
(2002) 2416. [248] C. Sissi, E. Perdona, E. Domenici, A. Feriani, A.J. Howells, A. Maxwell, M.
Palumbo, J. Mol. Biol. 311 (2001) 195. [249] S. Arias-Negrete, M. Nieto-Gómez, F. Anaya-Velázquez, R.M. García-Nieto, G.
Mendozaíaz Díaz, Rev. Soc. Quim. 37 (1993) 3. [250] M.P. López-Gresa, R. Ortiz, L. Perelló, J. Latorre, M. Liu-González, S. García-
Granda, M. Pérez-Priede, E. Cantón, J. Inorg. Biochem. 92 (2002) 65. [251] J.M. Tercero, A. Matilla, M.A. Sanjuán, C.F. Moreno, J.D. Martín, J.A.
Walmsley, Inorg. Chim. Acta 342 (2003) 77. [252] U.K. Häring, R.B. Martin, Inorg. Chim. Acta 78 (1983) 25. [253] T. Rau, R. van Eldik, in: H. Sigel, A. Sigel (Eds.), Metal Ions in Biological
Systems, vol. 31, Marcel Dekker, New York, 1996, p. 339. [254] J.M. Tercero-Moreno, A. Matilla-Hernández, S. González-García, J. Niclós-
Gutiérrez, Inorg. Chim. Acta 253 (1996) 23. [255] S. Nadeem, M. Bolte, S. Ahmad, T. Fazeelat, S.A. Tirmizi, M.K. Rauf, S.A.
Sattar, S. Siddiq, A. Hameed, S.Z. Haider, Inorg. Chim. Acta 363 (2010) 3261. [256] M.J. Rauterkus, S. Fakih, C. Mock, I. Puscasu, B. Krebs, Inorg. Chim. Acta 350
(2003) 355. [257] E. Nyarko, N. Hanada, A. Habib, M. Tabata, Inorg. Chim. Acta 357 (2004) 739. [258] J.M. Vanderkooi, D.F. Wilson, Adv. Exp. Med. 200 (1986) 189. [259] J. Müller, E. Freisinger, P. Lax, D.A. Megger, F.-A. Polonius, Inorg. Chim. Acta
360 (2007) 255. [260] J. Müller, F.-A. Polonius, M. Roitzsch, Inorg. Chim. Acta 358 (2005) 1225. [261] J.M. Tercero, A. Matilla, M.A. Sanjuán, C.F. Moreno, J.D. Martín, J.A.
Walmsley Inorg. Chim. Acta 342 (2003) 77. [262] S. Nadeem, M. Bolte, S. Ahmad, T. Fazeelat, S.A. Tirmizi, M.K. Rauf, S.A.
Sattar, S. Siddiq, A. Hameed, S.Z. Haider, Inorg. Chim. Acta 363 (2010) 3261. [263] M.J. Rauterkus, S. Fakih, C. Mock, I. Puscasu, B. Krebs, Inorg. Chim. Acta 350
(2003) 355. [264] C. Mock, I. Puscasu, M.J. Rauterkus, G. Tallen, J.E.A. Wolff, B. Krebs, Inorg.
Chim. Acta 319 (2001) 109.