chapter 24 head and facial traumas -...
TRANSCRIPT

1
Chapter 24Chapter 24Head and Facial TraumaHead and Facial Trauma
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
ObjectivesObjectivesDescribe mechanism of injury, assessment, Describe mechanism of injury, assessment, and management of:and management of:
Maxillofacial injuriesMaxillofacial injuriesEar, eye, and dental injuriesEar, eye, and dental injuriesAnterior neck traumaAnterior neck traumaInjuries to the scalp, cranial vault, or cranial Injuries to the scalp, cranial vault, or cranial nervesnerves
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
ObjectivesObjectivesDistinguish between types of traumatic brain Distinguish between types of traumatic brain injuryinjury
Outline the prehospital management of patients Outline the prehospital management of patients with cerebral injurywith cerebral injury
Calculate a Glasgow Coma Scale, trauma Calculate a Glasgow Coma Scale, trauma score, revised trauma score, and pediatric score, revised trauma score, and pediatric trauma score for a given scenariotrauma score for a given scenario
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Sanders: Mosby's Paramedic Textbook, Revised 3rd Edition PowerPoint Lecture Notes
Chapter 24: Head and Facial Traumas

2
ScenarioScenarioA10A10--yearyear--old boy is carried into your station, his arms old boy is carried into your station, his arms and legs draped limply over his frantic fatherand legs draped limply over his frantic father’’s arms. He s arms. He fell off an ATV about an hour ago, was knocked out fell off an ATV about an hour ago, was knocked out briefly, then seemed fine until he suddenly had a briefly, then seemed fine until he suddenly had a seizure and seizure and ““passed out.passed out.”” Your crew carefully Your crew carefully immobilizes him while you determine the following: his immobilizes him while you determine the following: his airway is noisy, and he has no gag reflex; he is airway is noisy, and he has no gag reflex; he is breathing irregularly about 10 times/min; BP 72/50 mm breathing irregularly about 10 times/min; BP 72/50 mm Hg; P 68/min; right pupil 2 mm and reacts to light, left Hg; P 68/min; right pupil 2 mm and reacts to light, left pupil 5 mm and unreactive; flaccid response to pain; wt pupil 5 mm and unreactive; flaccid response to pain; wt 35 kg. 35 kg.
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
DiscussionDiscussionWhat are your immediate priorities for his care?What are your immediate priorities for his care?
Calculate his GCS, RTS, and PTSCalculate his GCS, RTS, and PTS
What type of brain injury is likely in this child?What type of brain injury is likely in this child?
Explain the significance of his pupillary findingsExplain the significance of his pupillary findings
Why might his blood pressure be low?Why might his blood pressure be low?
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Maxillofacial InjuryMaxillofacial Injury
ArteriesArteriesNervesNerves
5th cranial nerve (trigeminal)5th cranial nerve (trigeminal)7th cranial nerve (facial)7th cranial nerve (facial)
Frontal boneFrontal boneNasal bonesNasal bonesMaxillaMaxillaZygomatic boneZygomatic boneMandibleMandible
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

3
Maxillofacial InjuryMaxillofacial InjuryCausesCauses
Motor vehicle crashesMotor vehicle crashesHome accidentsHome accidentsAthletic injuriesAthletic injuriesAnimal bitesAnimal bitesIntentional violent actsIntentional violent actsIndustrial injuriesIndustrial injuries
Maxillofacial trauma classified as:Maxillofacial trauma classified as:Soft tissue injuriesSoft tissue injuriesFacial fracturesFacial fractures
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Soft Tissue InjuriesSoft Tissue InjuriesFacial soft tissue injuries often appear seriousFacial soft tissue injuries often appear serious
Seldom life threateningSeldom life threateningExceptionsExceptions
•• Compromised upper airwayCompromised upper airway•• Potential for significant bleedingPotential for significant bleeding
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Soft Tissue InjurySoft Tissue InjuryAppearance of patient after being attacked and after cleansing
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

4
HistoryHistoryMechanism of injuryMechanism of injury
Events leading up to injuryEvents leading up to injury
Time of injuryTime of injury
Associated medical problemsAssociated medical problems
AllergiesAllergies
MedicationsMedications
Last oral intakeLast oral intake
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
ManagementManagementSpinal precautionsSpinal precautions
Assess for airway obstruction Assess for airway obstruction Apply suction as neededApply suction as needed
Secure and maintain airway Secure and maintain airway
Ensure ventilation and oxygenationEnsure ventilation and oxygenation
Control bleedingControl bleedingDirect pressure and pressure bandagesDirect pressure and pressure bandages
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Facial FracturesFacial FracturesCommon after blunt traumaCommon after blunt trauma
Signs and symptoms Signs and symptoms
Fractures of the mandibleFractures of the mandible
Dislocations of the mandibleDislocations of the mandible
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

5
Fractures of the MidfaceFractures of the MidfaceMiddle third of faceMiddle third of face
MaxillaMaxillaZygomaZygomaFloor of the orbitFloor of the orbitNoseNose
Fracture of middle 1/3 of face
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Le Fort FracturesLe Fort Fractures
I II III
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Fractures of the ZygomaFractures of the ZygomaZygoma articulates with Zygoma articulates with frontal, maxillary, and frontal, maxillary, and temporal bonestemporal bones
Associated with orbital Associated with orbital fractures and has fractures and has similar clinical signssimilar clinical signs
Signs and symptomsSigns and symptoms
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

6
Fractures of the OrbitFractures of the OrbitBlowout fractures to orbitBlowout fractures to orbit
Periorbital edema, Periorbital edema, subconjunctival ecchymosis, subconjunctival ecchymosis, diplopia, enopthalmos, diplopia, enopthalmos, epistaxis, anesthesia, epistaxis, anesthesia, impaired EOMimpaired EOM
Suspect injury to orbital Suspect injury to orbital contents with any facial contents with any facial fracturefracture
Blowout fracture caused by ball’s impact
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Fractures of the NoseFractures of the NoseMost often fractured structureMost often fractured structure
Injuries mayInjuries mayDepress dorsum of noseDepress dorsum of noseDisplace it to one sideDisplace it to one sideResult in epistaxis and swelling (without skeletal Result in epistaxis and swelling (without skeletal deformity)deformity)
Orbital fractures may also be presentOrbital fractures may also be present
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
EpistaxisEpistaxisApply external pressure to anterior naresApply external pressure to anterior nares
Conscious patientConscious patientSeated upright or leaning forward while paramedic compresses Seated upright or leaning forward while paramedic compresses naresnares
Unconscious patientUnconscious patientPositioned on side (if no spinal injury is suspected)Positioned on side (if no spinal injury is suspected)
Treat for shock if bleeding is severeTreat for shock if bleeding is severe
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

7
Management of Facial FracturesManagement of Facial FracturesAssume spine is injuredAssume spine is injured
Use spinal precautionsUse spinal precautions
Assess airway for obstructionAssess airway for obstructionApply suction as needed Apply suction as needed
Ensure adequate ventilation and oxygenationEnsure adequate ventilation and oxygenation
Control bleeding through direct pressure and Control bleeding through direct pressure and pressure bandagespressure bandages
Control epistaxis by external direct pressure Control epistaxis by external direct pressure
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Nasal and Ear Foreign BodiesNasal and Ear Foreign BodiesForeign bodies in nose or ear common in childrenForeign bodies in nose or ear common in children
May need transport for physician evaluationMay need transport for physician evaluation
Remove foreign body in ear if easily retrievedRemove foreign body in ear if easily retrieved
Do not remove nasal foreign body in field unless Do not remove nasal foreign body in field unless it:it:
Compromises airway Compromises airway Can be easily removed without equipmentCan be easily removed without equipment
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Ear TraumaEar TraumaLacerations and contusionsLacerations and contusions
Usually blunt traumaUsually blunt traumaTreated by direct pressure to control bleeding and Treated by direct pressure to control bleeding and ice or cold compresses ice or cold compresses
•• To decrease swellingTo decrease swelling
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

8
Ear TraumaEar TraumaRetrieve avulsed tissue if possibleRetrieve avulsed tissue if possible
Wrap in moist gauzeWrap in moist gauzeSeal in plasticSeal in plasticPlace on icePlace on iceTransport with patient for surgical repairTransport with patient for surgical repair
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Ear TraumaEar TraumaPartially detached pinna Loss of rim
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Ear TraumaEar TraumaThermal injuriesThermal injuries
Chemical injuriesChemical injuries
Traumatic perforationsTraumatic perforationsImpaled objectsImpaled objects
BarotitisBarotitis
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

9
Eye TraumaEye TraumaCommon causes of eye injuryCommon causes of eye injury
Motor vehicle crashesMotor vehicle crashesSports and recreational activitiesSports and recreational activitiesViolent altercationsViolent altercationsChemical exposure Chemical exposure Foreign bodiesForeign bodiesAnimal bites and scratchesAnimal bites and scratches
EvaluationEvaluation
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Eye Trauma Evaluation Eye Trauma Evaluation HistoryHistory
Exact mode of injuryExact mode of injuryUse of corrective glasses or contact lensesUse of corrective glasses or contact lenses
Visual acuityVisual acuityTest injured eye first; compare to uninjured eyeTest injured eye first; compare to uninjured eye
Pupillary reactionPupillary reaction
Extraocular movementExtraocular movement
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Specific Eye InjuriesSpecific Eye InjuriesOcular trauma should be evaluated by physicianOcular trauma should be evaluated by physicianForeign bodiesForeign bodiesCorneal abrasionCorneal abrasionBlunt traumaBlunt traumaPenetrating injuryPenetrating injuryProtruding intraocular foreign bodiesProtruding intraocular foreign bodiesChemical injuries to the eyeChemical injuries to the eye
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
10
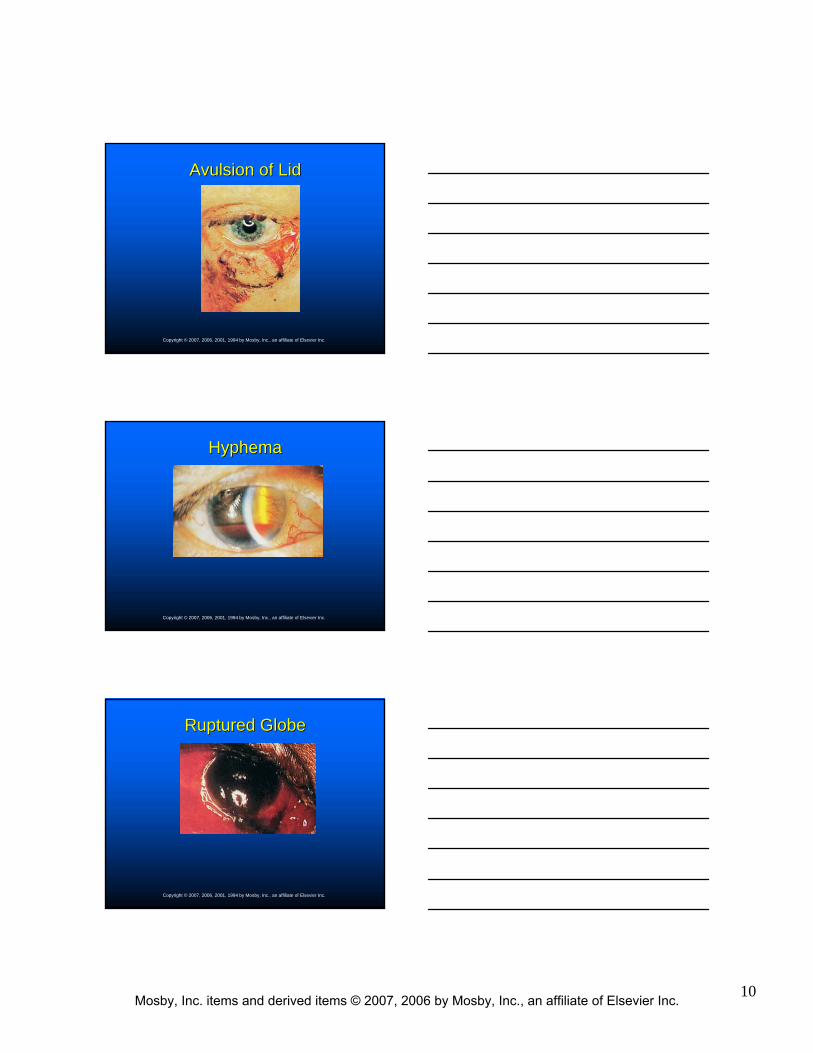
Avulsion of LidAvulsion of Lid
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
HyphemaHyphema
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Ruptured GlobeRuptured Globe
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

11
Acid BurnAcid Burn
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Alkali BurnAlkali Burn
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Corneal Abrasion CareCorneal Abrasion Care
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

12
Contact LensesContact LensesHard lensesHard lenses
Soft hydrophilic lensesSoft hydrophilic lenses
Rigid gasRigid gas--permeable lensespermeable lenses
As a rule, EMS personnel should not attempt As a rule, EMS personnel should not attempt to remove contact lenses in patients with eye to remove contact lenses in patients with eye injuriesinjuries
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Dental TraumaDental Trauma32 teeth in adult32 teeth in adultSectionsSections
CrownCrownRootRoot
Hard tissues of teeth Hard tissues of teeth Soft tissues of teeth Soft tissues of teeth Tooth fracture Tooth fracture Tooth avulsionTooth avulsion
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anterior Neck TraumaAnterior Neck Trauma
Blunt and Blunt and penetrating traumapenetrating trauma
Can damage:Can damage:Skeletal structuresSkeletal structuresVascular structuresVascular structuresNerves, muscles, Nerves, muscles, and glands of neck and glands of neck Self-inflicted stab wound that had entered pharynx
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

13
Common Mechanisms of InjuryCommon Mechanisms of Injury
Motor vehicle crashesMotor vehicle crashes
Sports and recreational activitiesSports and recreational activities
Industrial accidentsIndustrial accidents
Violent altercationsViolent altercations
HangingsHangings
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Evaluation of the NeckEvaluation of the NeckZone IZone I
Injuries carry highest mortality Injuries carry highest mortality
Zone IIZone IIMost common injuries but Most common injuries but lower mortality than zone I lower mortality than zone I injuriesinjuries
Zone IIIZone IIIGreatest risk of injury to distal Greatest risk of injury to distal carotid artery, salivary glands, carotid artery, salivary glands, and pharynxand pharynx
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Hematomas and EdemaHematomas and EdemaEdema of pharynx, larynx, trachea, epiglottis, Edema of pharynx, larynx, trachea, epiglottis, and vocal cords may obstruct airway and vocal cords may obstruct airway completelycompletely
Consider oral or nasal intubation with spinal Consider oral or nasal intubation with spinal precautions in patients with airway precautions in patients with airway compromisecompromise
Smaller ET tube may be neededSmaller ET tube may be needed
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

14
Hematomas and EdemaHematomas and EdemaOther measures to treat edematous airwaysOther measures to treat edematous airways
Cool, humidified oxygenCool, humidified oxygenSlight elevation of patient's head (if not Slight elevation of patient's head (if not contraindicated)contraindicated)
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Lacerations and Puncture WoundsLacerations and Puncture Wounds
Superficial injuriesSuperficial injuriesUsually managed by covering wound Usually managed by covering wound
Deep penetrating woundsDeep penetrating woundsSerious injuries may require:Serious injuries may require:
•• Aggressive airway therapy and ventilatory supportAggressive airway therapy and ventilatory support•• SuctionSuction•• Hemorrhage control by direct pressureHemorrhage control by direct pressure•• Fluid replacementFluid replacement
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Lacerations and Puncture WoundsLacerations and Puncture Wounds
Signs and symptoms of significant penetrating neck traumaSigns and symptoms of significant penetrating neck traumaShockShockActive bleedingActive bleedingTenderness on palpationTenderness on palpationMobility and crepitusMobility and crepitusLarge or expanding hematomaLarge or expanding hematomaPulse deficitPulse deficitNeurological deficit Neurological deficit
DyspneaDyspneaHoarsenessHoarsenessStridorStridorSubcutaneous emphysemaSubcutaneous emphysemaHemoptysisHemoptysisDysphagiaDysphagiaHematemesisHematemesis
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

15
Vascular InjuryVascular InjuryBlood vessels are most commonly injured structures Blood vessels are most commonly injured structures in the neckin the neck
Blunt or penetrating traumaBlunt or penetrating trauma
Vessels at risk of injuryVessels at risk of injuryCarotidCarotidVertebralVertebralSubclavianSubclavianInnominateInnominateInternal mammary arteriesInternal mammary arteriesJugular and subclavian veinsJugular and subclavian veins
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Vascular InjuryVascular Injury——ManagementManagementSecure airway with spinal precautionsSecure airway with spinal precautions
Adequate ventilatory supportAdequate ventilatory support
Control hemorrhage by direct pressureControl hemorrhage by direct pressure
Fluid replacement for hypovolemia guided by Fluid replacement for hypovolemia guided by medical direction medical direction
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Laryngeal or Tracheal InjuryLaryngeal or Tracheal InjuryBlunt or penetrating trauma to anterior neck Blunt or penetrating trauma to anterior neck may cause:may cause:
Fracture or dislocation of the laryngeal and Fracture or dislocation of the laryngeal and tracheal cartilagestracheal cartilagesHemorrhageHemorrhageSwelling of air passagesSwelling of air passages
Rapid airway control can save patient Rapid airway control can save patient
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

16
Laryngeal or Tracheal InjuryLaryngeal or Tracheal InjuryHigh degree of suspicion for:High degree of suspicion for:
Vascular disruptionVascular disruptionEsophageal, chest, and abdominal injuryEsophageal, chest, and abdominal injury
Emergency airway management in these Emergency airway management in these injuries is controversial injuries is controversial
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Esophageal InjuryEsophageal InjurySuspect in patients with trauma to neck or Suspect in patients with trauma to neck or chestchest
Specific injuries that require a high degree of Specific injuries that require a high degree of suspicion for associated esophageal injury suspicion for associated esophageal injury include:include:
Tracheal fracturesTracheal fracturesPenetrating trauma from stab or gunshot woundsPenetrating trauma from stab or gunshot woundsIngestion of caustic substancesIngestion of caustic substances
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Esophageal Injury Esophageal Injury Signs and symptoms may include:Signs and symptoms may include:
Subcutaneous emphysemaSubcutaneous emphysemaNeck hematomaNeck hematomaOropharyngeal or nasogastric blood (indicating Oropharyngeal or nasogastric blood (indicating esophageal perforation)esophageal perforation)
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

17
Head TraumaHead TraumaAnatomical components of skullAnatomical components of skull
ScalpScalpCranial vaultCranial vault
•• Dural membraneDural membrane•• Arachnoid membraneArachnoid membrane•• PiaPia•• Brain substancesBrain substances
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
ScalpScalpHairHair
Subcutaneous tissueSubcutaneous tissueMajor scalp veins bleed profuselyMajor scalp veins bleed profusely
MuscleMuscleAttached above eyebrows and at base of occiputAttached above eyebrows and at base of occiput
GaleaGaleaFreely movable sheet of connective tissueFreely movable sheet of connective tissueHelps deflect blowsHelps deflect blows
Loose connective tissueLoose connective tissueContains emissary veins that drain intracraniallyContains emissary veins that drain intracranially
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Soft Tissue Injuries to the ScalpSoft Tissue Injuries to the Scalp
Irregular linear laceration Irregular linear laceration common common
May lead to profuse May lead to profuse bleeding and hypovolemiableeding and hypovolemia
Particularly in infants and Particularly in infants and childrenchildren
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

18
Soft Tissue Injuries to the ScalpSoft Tissue Injuries to the Scalp
ManagementManagementPrevent contamination of open woundsPrevent contamination of open woundsDirect pressure or pressure dressings to decrease Direct pressure or pressure dressings to decrease blood lossblood lossIV fluid replacement if neededIV fluid replacement if neededConsider potential for underlying skull fracture and Consider potential for underlying skull fracture and brain and spinal trauma brain and spinal trauma
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
SkullSkullFacial bonesFacial bones
Cranial bonesCranial bonesDouble layer of solid bone surrounds spongy middle layerDouble layer of solid bone surrounds spongy middle layerFrontal, occipital, temporal, parietal, and mastoidFrontal, occipital, temporal, parietal, and mastoid
Middle meningeal arteryMiddle meningeal arteryUnder temporal boneUnder temporal boneCan tear artery if fracturedCan tear artery if fractured
Skull floorSkull floor——many ridgesmany ridges
Foramen magnumForamen magnumOpening at base of skull for spinal cordOpening at base of skull for spinal cord
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Classification of Skull FracturesClassification of Skull Fractures
Linear fracturesLinear fractures
Basilar fracturesBasilar fractures
Depressed fracturesDepressed fractures
Open vault fracturesOpen vault fractures
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

19
Linear FracturesLinear Fractures80% of all skull fractures80% of all skull fractures
Not usually depressedNot usually depressed
May occur without an May occur without an overlying scalp lacerationoverlying scalp laceration
Generally low Generally low complication rate (if complication rate (if isolated injury)isolated injury)
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Basilar Skull FractureBasilar Skull Fracture
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Basilar Skull FractureBasilar Skull Fracture——Signs and SymptomsSigns and Symptoms
Ecchymosis over mastoid Ecchymosis over mastoid processprocess
Temporal bone fractureTemporal bone fractureBattle's signBattle's sign
Blood behind tympanic Blood behind tympanic membranemembrane
Fractures of temporal boneFractures of temporal boneHemotympanumHemotympanum
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

20
Basilar Skull FractureBasilar Skull Fracture——Signs and SymptomsSigns and Symptoms
Ecchymosis of one or Ecchymosis of one or both orbitsboth orbits
Fracture of base of Fracture of base of sphenoid sinussphenoid sinusRaccoon's eyesRaccoon's eyes
CSF leakageCSF leakageCan result in bacterial Can result in bacterial meningitismeningitis
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Depressed Skull FracturesDepressed Skull Fractures
Relatively small object Relatively small object strikes head at high speedstrikes head at high speed
Often scalp lacerationsOften scalp lacerations
Frontal and parietal bones Frontal and parietal bones most often affectedmost often affected
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Open Vault FracturesOpen Vault Fractures
Direct communication Direct communication between a scalp laceration between a scalp laceration and cerebral substanceand cerebral substance
Often occur with multisystem Often occur with multisystem traumatraumaHigh mortality rateHigh mortality rateMay lead to infection May lead to infection (meningitis)(meningitis)
Prehospital managementPrehospital management
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

21
Severe Fracture of Base of SkullSevere Fracture of Base of Skull
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Skull FracturesSkull Fractures——ComplicationsComplicationsCranial nerve injuryCranial nerve injury
Vascular involvementVascular involvementMeningeal arteryMeningeal arteryDural sinusesDural sinuses
InfectionInfection
Underlying brain injuryUnderlying brain injury
Dural defects caused by depressed bone fragmentsDural defects caused by depressed bone fragments
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Cranial Nerve InjuriesCranial Nerve InjuriesUsually associated with skull fracturesUsually associated with skull fractures
Cranial nerve I (olfactory nerve)Cranial nerve I (olfactory nerve)Loss of smellLoss of smellImpairment of taste (dependent on food aroma)Impairment of taste (dependent on food aroma)Sign of basilar skull fractureSign of basilar skull fracture
Cranial nerve II (optic nerve)Cranial nerve II (optic nerve)Blindness in one or both eyesBlindness in one or both eyesVisual field defectsVisual field defects
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

22
Cranial NervesCranial NervesCranial nerve III (oculomotor)Cranial nerve III (oculomotor)
Origin from midbrainOrigin from midbrainControls pupil sizeControls pupil sizePressure on nerve paralyzes nervePressure on nerve paralyzes nerve
•• Pupil nonreactivePupil nonreactive
Cranial nerve X (vagus)Cranial nerve X (vagus)Origin in medullaOrigin in medullaNerves that supply SA and AV node, stomach, and GI tractNerves that supply SA and AV node, stomach, and GI tractPressure on nerve stimulates bradycardiaPressure on nerve stimulates bradycardia
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Cranial Nerve InjuriesCranial Nerve InjuriesCranial nerve III (oculomotor nerve)Cranial nerve III (oculomotor nerve)
Ipsilateral, dilated, fixed pupilIpsilateral, dilated, fixed pupilVulnerable to compression by temporal lobeVulnerable to compression by temporal lobeMimic direct ocular traumaMimic direct ocular trauma
Cranial nerve VII (facial nerve)Cranial nerve VII (facial nerve)Immediate or delayed facial paralysisImmediate or delayed facial paralysisBasilar skull fractureBasilar skull fracture
Cranial nerve VIII (auditory nerve)Cranial nerve VIII (auditory nerve)DeafnessDeafnessBasilar skull fracture Basilar skull fracture
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Brain TraumaBrain TraumaTraumatic insult to the brain is capable of Traumatic insult to the brain is capable of producing physical, intellectual, emotional, producing physical, intellectual, emotional, social, and vocational changesocial, and vocational change
Primary brain injuryPrimary brain injury
Secondary brain injurySecondary brain injury
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

23
Brain TraumaBrain TraumaBrain occupies 80% of intracranial spaceBrain occupies 80% of intracranial space
ComponentsComponentsBrain stemBrain stemDiencephalonDiencephalonCerebrumCerebrumCerebellumCerebellum
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Brain TraumaBrain TraumaCategoriesCategories
Mild diffuse injuryMild diffuse injuryModerate diffuse injuryModerate diffuse injuryDiffuse axonal injuryDiffuse axonal injuryFocal injuryFocal injury
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mild Diffuse Injury (Concussion)Mild Diffuse Injury (Concussion)
Fully reversible brain injuryFully reversible brain injury
No structural damage to brainNo structural damage to brain
CausesCauses
Signs and symptomsSigns and symptoms
ManagementManagement
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

24
Moderate Diffuse InjuryModerate Diffuse InjuryMinute petechial bruising of brain tissueMinute petechial bruising of brain tissue
Brain stem and reticular activating system Brain stem and reticular activating system involvement lead to unconsciousnessinvolvement lead to unconsciousness
Signs and symptomsSigns and symptoms
ManagementManagement
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Diffuse Axonal Injury (DAI)Diffuse Axonal Injury (DAI)Most severe brain injuryMost severe brain injury
Brain movement within skull secondary to Brain movement within skull secondary to acceleration or deceleration forcesacceleration or deceleration forces
DAI may be classified as mild, moderate, or DAI may be classified as mild, moderate, or severesevere
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Diffuse Axonal InjuryDiffuse Axonal InjuryMild DAIMild DAI
Coma of 6Coma of 6-- 24 hrs24 hrs
Moderate DAIModerate DAIMore commonMore commonComa >24 hrs and abnormal posturingComa >24 hrs and abnormal posturing
Severe DAISevere DAIFormerly known as brainstem injuryFormerly known as brainstem injurySevere shearing of axons in both cerebral hemispheres Severe shearing of axons in both cerebral hemispheres extending to brain stemextending to brain stem
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

25
Focal InjuryFocal InjurySpecific, grossly observable brain lesionsSpecific, grossly observable brain lesions
Result from:Result from:Skull fractureSkull fractureContusionContusionEdema with associated increased ICPEdema with associated increased ICPIschemiaIschemiaHemorrhageHemorrhage
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Intracranial ContentsIntracranial ContentsBrain water: 58%Brain water: 58%
Brain solids: 25%Brain solids: 25%
Cerebrospinal fluid: 7%Cerebrospinal fluid: 7%
Intracranial blood: 10%Intracranial blood: 10%
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Cerebral ContusionCerebral ContusionBruising of brain around cortex or deeper within Bruising of brain around cortex or deeper within frontal, temporal, or occipital lobesfrontal, temporal, or occipital lobes
Structural change in brain tissueStructural change in brain tissueGreater neurological deficits and abnormalities than Greater neurological deficits and abnormalities than with concussionwith concussionCoup injuriesCoup injuriesContrecoup injuriesContrecoup injuries
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
26
EdemaEdemaSignificant brain injuries may result in Significant brain injuries may result in swelling of brain tissue swelling of brain tissue
With or without associated hemorrhageWith or without associated hemorrhage
Swelling results from humoral and metabolic Swelling results from humoral and metabolic responses to injuryresponses to injury
Increase in intracranial pressureIncrease in intracranial pressureMay be decreased cerebral perfusion or herniationMay be decreased cerebral perfusion or herniation
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
IschemiaIschemiaCan result from:Can result from:
Vascular injuriesVascular injuriesSecondary vascular spasmSecondary vascular spasmIncreased intracranial pressureIncreased intracranial pressureFocal or more global infarcts can resultFocal or more global infarcts can result
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
HemorrhageHemorrhageInto or around brain tissueInto or around brain tissue
Epidural or subdural hematomas can compress Epidural or subdural hematomas can compress underlying brain tissue or intraparenchymal underlying brain tissue or intraparenchymal hemorrhagehemorrhage
Often associated with:Often associated with:Cerebral contusionsCerebral contusionsSkull fracturesSkull fractures
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
27
Cerebral Blood FlowCerebral Blood Flow
Oxygen and glucose delivery are controlled by Oxygen and glucose delivery are controlled by cerebral blood flowcerebral blood flow
A function of cerebral perfusion pressure (CPP) and A function of cerebral perfusion pressure (CPP) and resistance of the cerebral vascular bedresistance of the cerebral vascular bedCPP = MAP CPP = MAP -- ICPICP
•• MAP = Diastolic pressure + 1/3 Pulse pressureMAP = Diastolic pressure + 1/3 Pulse pressure
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Cerebral Blood FlowCerebral Blood FlowAs ICP approaches MAP:As ICP approaches MAP:
Gradient for flow decreasesGradient for flow decreasesCerebral blood flow is restrictedCerebral blood flow is restricted
When ICP increases, CPP decreasesWhen ICP increases, CPP decreasesCerebral vasodilation occursCerebral vasodilation occursIncreased cerebral blood volume (increasing ICP)Increased cerebral blood volume (increasing ICP)
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Cerebral Blood FlowCerebral Blood FlowVascular tone in brain regulated by:Vascular tone in brain regulated by:
Carbon dioxide pressure (PCOCarbon dioxide pressure (PCO22))Oxygen pressure (POOxygen pressure (PO22))Autonomic and neurohumoral controlAutonomic and neurohumoral control
PCOPCO22 has greatest effect on intracerebral has greatest effect on intracerebral vascular diameter and subsequent resistancevascular diameter and subsequent resistance
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

28
Intracranial Pressure (ICP)Intracranial Pressure (ICP)Normal range is 0Normal range is 0--15 torr15 torr
When ICP rises above this levelWhen ICP rises above this levelCerebral blood flow decreasesCerebral blood flow decreases
Body tries to compensate for decline in CPP by a rise in Body tries to compensate for decline in CPP by a rise in MAP: MAP:
Further elevates ICP, and CSF is displaced to compensate for Further elevates ICP, and CSF is displaced to compensate for the expansionthe expansion
If unresolved, brain substance herniates If unresolved, brain substance herniates
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Effects of Increased Intracranial PressureEffects of Increased Intracranial Pressure
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Increased Intracranial PressureIncreased Intracranial PressureEarlyEarly
HeadacheHeadacheNausea and vomitingNausea and vomitingAltered level of consciousnessAltered level of consciousness
Eventually, CushingEventually, Cushing’’s triads triadIncreased systolic pressure (widened pulse pressure)Increased systolic pressure (widened pulse pressure)Decreased pulse rate Decreased pulse rate Irregular respiratory patternIrregular respiratory pattern
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

29
Increased Intracranial PressureIncreased Intracranial Pressure
Herniation through temporal lobe causes Herniation through temporal lobe causes compression of cranial nerve III (oculomotor)compression of cranial nerve III (oculomotor)
Patient rapidly unresponsive to verbal and Patient rapidly unresponsive to verbal and painful stimulipainful stimuli
Exhibits decorticate posturing or decerebrate Exhibits decorticate posturing or decerebrate posturingposturing
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
PosturingPosturing
Abnormal extension (decerebrate posturing)
Abnormal flexion (decorticate posturing)
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Critical Signs of HerniationCritical Signs of HerniationUnresponsive patient with:Unresponsive patient with:
Bilateral, dilated, unresponsive pupils Bilateral, dilated, unresponsive pupils OROR
Asymmetric pupils (>1 mm)Asymmetric pupils (>1 mm)ANDAND
Abnormal extension (decerebrate) posturing Abnormal extension (decerebrate) posturing OROR
No motor response to painful stimulusNo motor response to painful stimulus
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

30
Respiratory PatternsRespiratory Patterns
Associated with increased intracranial pressure Associated with increased intracranial pressure and brain stem injury:and brain stem injury:
HypoventilationHypoventilationCheyneCheyne--Stokes breathingStokes breathing
•• May accompany decorticate posturingMay accompany decorticate posturing
Central neurogenic hyperventilationCentral neurogenic hyperventilation•• May accompany decerebrate posturingMay accompany decerebrate posturing
Ataxic breathingAtaxic breathing
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory PatternsRespiratory Patterns
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Types of Brain HemorrhageTypes of Brain Hemorrhage
Classified according to Classified according to location:location:
EpiduralEpiduralSubduralSubduralSubarachnoidSubarachnoidCerebral (intraparenchymal)Cerebral (intraparenchymal)
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

31
Epidural HematomaEpidural HematomaCollection of blood between Collection of blood between cranium and dura in cranium and dura in epidural spaceepidural space
Rapidly developing lesion Rapidly developing lesion from laceration of middle from laceration of middle meningeal arterymeningeal artery
Common causes Common causes
Signs and symptomsSigns and symptoms
ManagementManagement
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Subdural HematomaSubdural Hematoma
Blood between dura Blood between dura and surface of brain and surface of brain in subdural spacein subdural space
Usually bleeding from Usually bleeding from veins that bridge veins that bridge subdural spacesubdural space
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Subdural HematomaSubdural HematomaClassifications Classifications
AcuteAcute—— symptoms symptoms <<24 hours24 hoursSubacuteSubacute——symptoms 2symptoms 2--10 days10 daysChronicChronic——symptoms >2 weekssymptoms >2 weeks
Signs and symptomsSigns and symptoms
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

32
Subarachnoid BleedingSubarachnoid Bleeding
Intracranial bleeding Intracranial bleeding into CSF, resulting in into CSF, resulting in bloody CSF and bloody CSF and meningeal irritationmeningeal irritation
Signs and symptomsSigns and symptoms
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Intracerebral HematomaIntracerebral Hematoma> 5 mL blood somewhere within brain> 5 mL blood somewhere within brain
Commonly frontal or temporal lobeCommonly frontal or temporal lobe
CausesCauses
Signs and symptomsSigns and symptoms
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Penetrating InjuryPenetrating InjuryMissiles fired from handgunsMissiles fired from handguns
Stab woundsStab woundsFallsFallsHighHigh--velocity motor vehicle crashesvelocity motor vehicle crashes
Associated injuriesAssociated injuries
ComplicationsComplications
Definitive careDefinitive care
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

33
Assessment and EvaluationAssessment and EvaluationConsider:Consider:
Mechanism and severity of injuryMechanism and severity of injuryLevel of consciousnessLevel of consciousnessAssociated injuriesAssociated injuries
Assess GCS every 5 minAssess GCS every 5 min
Determine pupilDetermine pupilSizeSizeReactivityReactivity
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Assessment and ManagementAssessment and ManagementMaintain airwayMaintain airway
Maintain SaOMaintain SaO22 >90%>90%
NS or LR fluid bolus if adult BP <90 mm HgNS or LR fluid bolus if adult BP <90 mm Hg
Hyperventilate only when critical signs of herniation Hyperventilate only when critical signs of herniation are presentare present
Neurological examNeurological exam
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Assessment and ManagementAssessment and ManagementDrug therapyDrug therapy
Medical direction may prescribe drugs for head Medical direction may prescribe drugs for head injuries (considered controversial)injuries (considered controversial)
•• Mannitol for cerebral edemaMannitol for cerebral edema•• Lorazepam and diazepam for seizure activityLorazepam and diazepam for seizure activity
Rarely used in prehospital setting in HI due to sedationRarely used in prehospital setting in HI due to sedation•• Lidocaine to control ICP that occurs with ET intubationLidocaine to control ICP that occurs with ET intubation•• Sedatives and paralytics for airway managementSedatives and paralytics for airway management
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

34
Glasgow Coma Scale (GCS)Glasgow Coma Scale (GCS)Evaluates:Evaluates:
Eye openingEye openingVerbal responsesVerbal responsesBrain stem reflex functionBrain stem reflex function
Evaluate at least every 5 minEvaluate at least every 5 minMild head injury: GCS 13Mild head injury: GCS 13--1515Moderate head injury: GCS 9Moderate head injury: GCS 9--1212Severe head injury: GCS Severe head injury: GCS <<88
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Trauma Score (TS)Trauma Score (TS)Predicts outcome of patients with blunt or Predicts outcome of patients with blunt or penetrating injuriespenetrating injuries
Modified trauma index to include systolic Modified trauma index to include systolic blood pressure, respiratory rate, and the GCSblood pressure, respiratory rate, and the GCS
Limited use in prehospital settingLimited use in prehospital setting
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Revised Trauma Score (RTS)Revised Trauma Score (RTS)GCS with systolic blood pressure and respiratory GCS with systolic blood pressure and respiratory rate rate
RTS essentially same as TS except for RTS essentially same as TS except for consideration of capillary refillconsideration of capillary refill
Patients with RTS of Patients with RTS of <<11 should be transferred 11 should be transferred to a level I trauma center to a level I trauma center
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

35
Pediatric Trauma Score (PTS)Pediatric Trauma Score (PTS)Evaluates:Evaluates:
Size (weight)Size (weight)AirwayAirwayCentral nervous systemCentral nervous systemSystolic blood pressureSystolic blood pressureOpen woundOpen woundSkeletal injurySkeletal injury
Pediatric trauma patient with PTS <8 should be Pediatric trauma patient with PTS <8 should be transported to a level I trauma centertransported to a level I trauma center
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Other MethodsOther Methods
CUPS systemCUPS systemAssigns patients to one of four categoriesAssigns patients to one of four categories
Constant monitoring of patient is crucialConstant monitoring of patient is crucial
Changes in patientChanges in patient’’s status may alter the s status may alter the course of a treatment plancourse of a treatment plan
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
ConclusionConclusionHead injuries affect nearly 4 million people each Head injuries affect nearly 4 million people each year in the United States. Approximately 50,000 year in the United States. Approximately 50,000 patients with severe head trauma die each year patients with severe head trauma die each year
before reaching the emergency department. before reaching the emergency department. Accurate assessment and appropriate Accurate assessment and appropriate
prehospital intervention can improve survival and prehospital intervention can improve survival and brain function for patients with these injuries.brain function for patients with these injuries.
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

36
Questions?Questions?
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.