chapter 25 pleural diseases. mosby items and derived items © 2009 by mosby, inc., an affiliate of...
TRANSCRIPT
Chapter 25Chapter 25
Pleural DiseasesPleural Diseases
Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 2
ObjectivesObjectives Describe important anatomic features and physiologic Describe important anatomic features and physiologic
function of the visceral and parietal pleural membranes.function of the visceral and parietal pleural membranes.
Describe how pleural effusions occur and the difference Describe how pleural effusions occur and the difference between transudative and exudative effusions.between transudative and exudative effusions.
Identify common causes of transudative and exudative Identify common causes of transudative and exudative pleural effusions.pleural effusions.
Write definitions of “chylothorax,” “hemothorax,” and Write definitions of “chylothorax,” “hemothorax,” and “pneumothorax.”“pneumothorax.”
Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 3
Objectives (cont.)Objectives (cont.)
Describe the impact of moderate to large Describe the impact of moderate to large pleural effusions on lung function.pleural effusions on lung function.
State the role of the chest radiograph in State the role of the chest radiograph in recognizing pleural effusions.recognizing pleural effusions.
State the purpose of thoracentesis and the State the purpose of thoracentesis and the potential complications.potential complications.

Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 4
Objectives (cont.)Objectives (cont.)
Identify the definitions of Identify the definitions of spontaneousspontaneous, , secondarysecondary, and , and tension pneumothoraxtension pneumothorax..
Describe the diagnosis and treatment of Describe the diagnosis and treatment of pneumothorax.pneumothorax.
Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 5
The Pleural SpaceThe Pleural Space
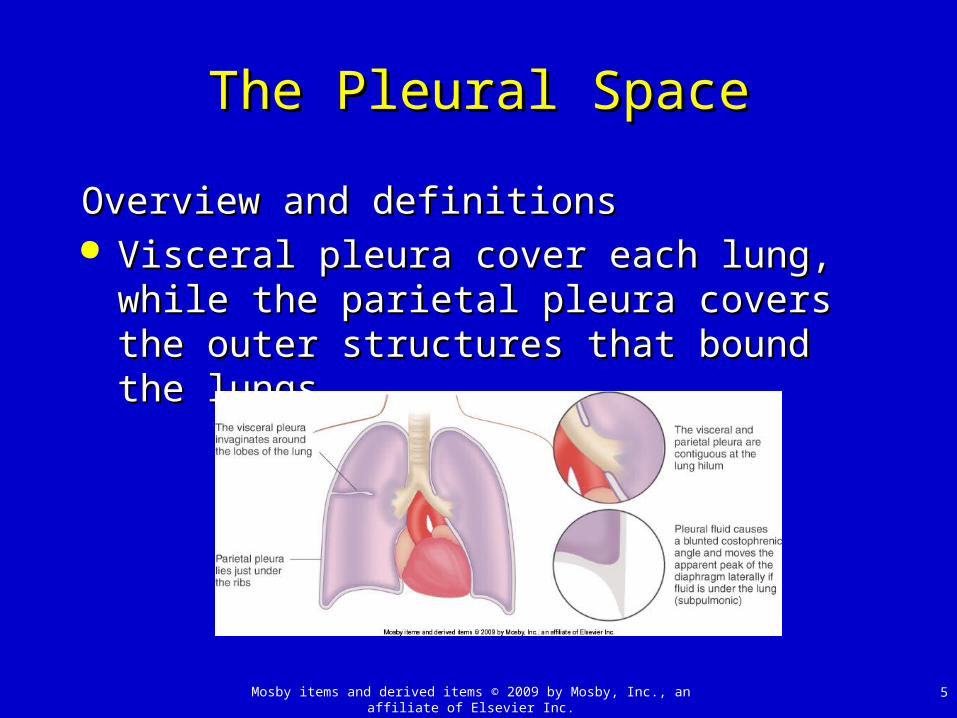
Overview and definitionsOverview and definitions Visceral pleura cover each lung, while the Visceral pleura cover each lung, while the
parietal pleura covers the outer structures parietal pleura covers the outer structures that bound the lungs.that bound the lungs.

Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 6
The Pleural Space (cont.)The Pleural Space (cont.)
Overview and definitions (cont.)Overview and definitions (cont.) Pleural fluid about 10 to 20 mm thick separates the Pleural fluid about 10 to 20 mm thick separates the
visceral from parietal pleura.visceral from parietal pleura. There is ~8 ml of fluid per hemithorax.There is ~8 ml of fluid per hemithorax. Pleural fluid is very similar to interstitial fluid.Pleural fluid is very similar to interstitial fluid. This fluid minimizes the friction caused by the lungs to This fluid minimizes the friction caused by the lungs to
expanding in the thorax during inspiration.expanding in the thorax during inspiration.
Pleural pressure is typically negative due to outward Pleural pressure is typically negative due to outward
thoracic recoil and inward recoil of lung.thoracic recoil and inward recoil of lung.

Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 7
Pleural EffusionsPleural Effusions
Any abnormal accumulation of fluid in the Any abnormal accumulation of fluid in the pleura is considered a pleural effusion.pleura is considered a pleural effusion.
Fluid enters the pleural space from visceral Fluid enters the pleural space from visceral and parietal pleurae, particularly in face of and parietal pleurae, particularly in face of increased pressure.increased pressure. Stomata that connect to lymphatic system remove Stomata that connect to lymphatic system remove
fluid from this space.fluid from this space. Either increased fluid production or blockage of Either increased fluid production or blockage of
drainage can result in pleural effusions.drainage can result in pleural effusions.
Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 8
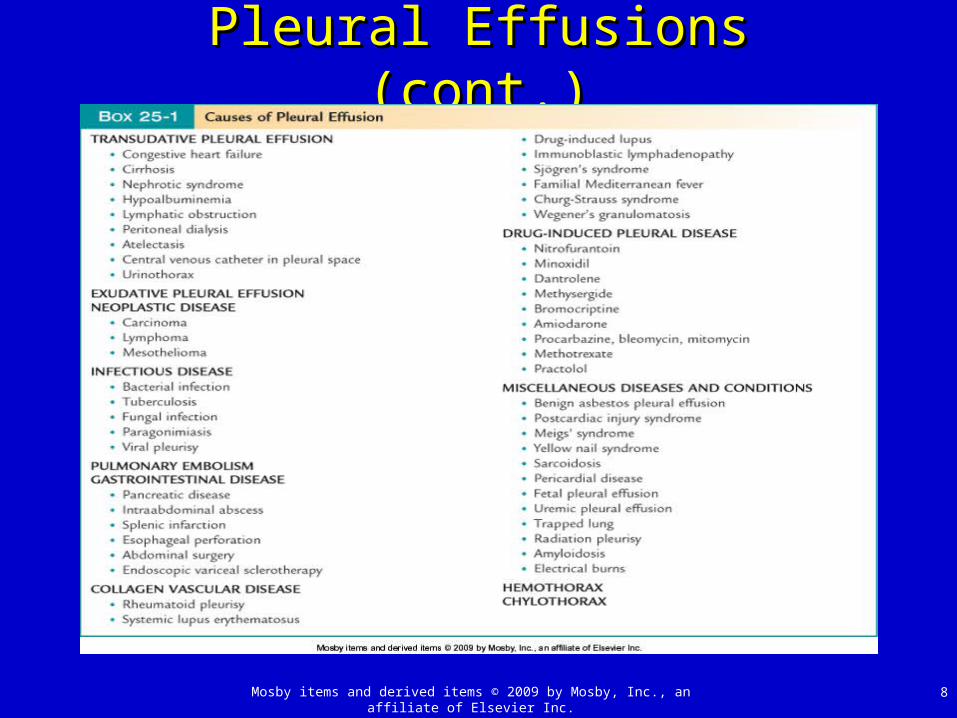
Pleural Effusions (cont.)Pleural Effusions (cont.)
Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 9
Pleural Effusions (cont.)Pleural Effusions (cont.)
Transudative effusionsTransudative effusions Any effusion that forms while pleural space is Any effusion that forms while pleural space is
undamaged will have [protein] <50% of serum level undamaged will have [protein] <50% of serum level and LDH <60% of serum leveland LDH <60% of serum level
Specific causes of transudative effusionsSpecific causes of transudative effusions CHF: high hydrostatic pressure increases pleura fluid CHF: high hydrostatic pressure increases pleura fluid
production, most common cause of effusionsproduction, most common cause of effusions
Nephrotic syndrome: protein loss in urine results in Nephrotic syndrome: protein loss in urine results in low capillary oncotic pressure and fluid third spacinglow capillary oncotic pressure and fluid third spacing

Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 10
Pleural Effusions (cont.)Pleural Effusions (cont.)Specific causes of transudative effusions (cont.)Specific causes of transudative effusions (cont.) Hypoalbuminemia: different cause but mimics aboveHypoalbuminemia: different cause but mimics above
Liver disease: ascites fluid moves through small holes Liver disease: ascites fluid moves through small holes in diaphragm, almost always on right sidein diaphragm, almost always on right side
Atelectasis: cause pleural pressures to become more Atelectasis: cause pleural pressures to become more negative resulting in small effusionsnegative resulting in small effusions
Lymphatic obstruction: blockage prevents drainage Lymphatic obstruction: blockage prevents drainage and results in accumulationand results in accumulation

Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 11
Pleural Effusions (cont.)Pleural Effusions (cont.)
Exudative effusionsExudative effusions Occur due to inflammation of lung or pleura and will Occur due to inflammation of lung or pleura and will
have a higher protein and inflammatory cell contenthave a higher protein and inflammatory cell content
Thoracentesis may be performed to determine type.Thoracentesis may be performed to determine type.Specific causes of exudative effusionsSpecific causes of exudative effusions Parapneumonic: secondary to lung inflammation Parapneumonic: secondary to lung inflammation
associated with pneumoniaassociated with pneumonia Complicated if clots form and loculate fluidComplicated if clots form and loculate fluid Persistent fever may signal an empyema, which must be Persistent fever may signal an empyema, which must be
drained for recoverydrained for recovery
Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 12
Pleural Effusions (cont.)Pleural Effusions (cont.)
Specific causes of exudative effusions (cont.)Specific causes of exudative effusions (cont.) Viral pleurisy: presents with inflammation and painViral pleurisy: presents with inflammation and pain
Pain may result in atelectasis and hypoxemia.Pain may result in atelectasis and hypoxemia.
Tuberculous pleurisy: occurs when caseous Tuberculous pleurisy: occurs when caseous granulomas rupture viscera pleura and drain into granulomas rupture viscera pleura and drain into pleural spacepleural space Patients need to be isolated.Patients need to be isolated.
Malignancy: most common cause of large unilateral Malignancy: most common cause of large unilateral
effusions, most require pleurodesis to treateffusions, most require pleurodesis to treat

Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 13
Pleural Effusions (cont.)Pleural Effusions (cont.)
Specific causes of exudative effusions (cont.)Specific causes of exudative effusions (cont.) Postoperative: common following abdominal or Postoperative: common following abdominal or
thoracic surgerythoracic surgery
Chylothorax: caused by rupture of thoracic duct, 50% Chylothorax: caused by rupture of thoracic duct, 50% malignant, 20% surgicalmalignant, 20% surgical Fluid may be white or yellow, sometimes bloodyFluid may be white or yellow, sometimes bloody
Hemothorax: trauma or blood vessel hemorrhage into Hemothorax: trauma or blood vessel hemorrhage into pleura spacepleura space Hematocrit > 50% of serum levelHematocrit > 50% of serum level

Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 14
Physiological Importance of Physiological Importance of Pleural EffusionsPleural Effusions
Mechanics of ventilationMechanics of ventilation Effusions cause atelectasis due to limited thoracic Effusions cause atelectasis due to limited thoracic
space resulting in restrictive pattern on PFTs.space resulting in restrictive pattern on PFTs.
Patients commonly dyspneic even with small effusionsPatients commonly dyspneic even with small effusions
Rarely cause fibrothorax with true restrictive impairmentRarely cause fibrothorax with true restrictive impairment
HypoxemiaHypoxemia Most effusions cause increased P(A – a)OMost effusions cause increased P(A – a)O22, which may , which may
worsen following thoracentesis.worsen following thoracentesis.
Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 15
Diagnostic Tests for Diagnostic Tests for Pleural EffusionsPleural Effusions
Chest radiographyChest radiography Most common method of detecting effusionsMost common method of detecting effusions
Upright PA and lateral decubitus are useful.Upright PA and lateral decubitus are useful. 1-cm meniscus lung to rib allows for thoracentesis1-cm meniscus lung to rib allows for thoracentesis
Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 16
Diagnostic Tests for Pleural Diagnostic Tests for Pleural Effusions (cont.)Effusions (cont.)
Ultrasonography and computed tomographyUltrasonography and computed tomography Ultrasound is very sensitive to pleural Ultrasound is very sensitive to pleural
effusions.effusions. May use to localize and direct for thoracentesisMay use to localize and direct for thoracentesis
Contrast-enhanced CT is most sensitive Contrast-enhanced CT is most sensitive study for effusions.study for effusions.
Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 17
Diagnostic Tests for Pleural Diagnostic Tests for Pleural Effusions (cont.)Effusions (cont.)
ThoracentesisThoracentesis Percutaneous needle aspiration of effusion samplePercutaneous needle aspiration of effusion sample
Drainage for lung reexpansion involves placement of Drainage for lung reexpansion involves placement of a chest tubea chest tube
Risks includeRisks include Artery lacerationArtery laceration InfectionInfection PneumothoraxPneumothorax

Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 18
Diagnostic Tests for Pleural Diagnostic Tests for Pleural Effusions (cont.)Effusions (cont.)

Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 19
Diagnostic Tests for Pleural Diagnostic Tests for Pleural Effusions (cont.)Effusions (cont.)
Thoracoscopy (video-assisted)Thoracoscopy (video-assisted) Ideally designed for diagnostic and Ideally designed for diagnostic and
therapeutic pleural procedurestherapeutic pleural procedures
Allows visualization of surfaces, drainage of Allows visualization of surfaces, drainage of effusion, biopsy, and pleurodesis if neededeffusion, biopsy, and pleurodesis if needed

Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 20
Management for Pleural Management for Pleural EffusionsEffusions
Chest thoracotomy tubesChest thoracotomy tubes Designed for tight fit in tissues to avoid leaks Designed for tight fit in tissues to avoid leaks
and allow drainage of effusion and subsequent and allow drainage of effusion and subsequent lung reexpansionlung reexpansion
Tube is attached to chest drainage unit.Tube is attached to chest drainage unit.

Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 21
Management for Pleural Management for Pleural Effusions (cont.) Effusions (cont.)
Pleurodesis Pleurodesis Process fusing parietal and visceral pleurae, Process fusing parietal and visceral pleurae,
which prevents further formation of effusionswhich prevents further formation of effusions
Can be performed by surgical abrasion or Can be performed by surgical abrasion or introduction of chemical irritant, most commonly introduction of chemical irritant, most commonly talctalc
Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 22
Management for Pleural Management for Pleural Effusions (cont.)Effusions (cont.)
Pleuroperitoneal shunt and Pleurex catheterPleuroperitoneal shunt and Pleurex catheter For effusions refractory to all other treatment For effusions refractory to all other treatment
optionsoptions
Small pump moves fluid from pleura to Small pump moves fluid from pleura to peritoneal cavity.peritoneal cavity.
Pleurex catheter connects to suction at home Pleurex catheter connects to suction at home to drain persistent effusions.to drain persistent effusions.

Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 23
PneumothoraxPneumothorax Defined as air in the pleural space which can occur Defined as air in the pleural space which can occur
through a number of mechanismsthrough a number of mechanisms
Traumatic pneumothoraxTraumatic pneumothorax Penetrating chest traumaPenetrating chest trauma
Common secondary to bullet or knife penetrationCommon secondary to bullet or knife penetration Chest tube is usually adequate to treat.Chest tube is usually adequate to treat. May require surgery if bleeding is severeMay require surgery if bleeding is severe
Blunt traumaBlunt trauma Broken ribs puncture lung with air escape into pleura.Broken ribs puncture lung with air escape into pleura. Chest tube is all that is generally required.Chest tube is all that is generally required.

Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 24
Pneumothorax (cont.)Pneumothorax (cont.)
Blunt trauma (cont.)Blunt trauma (cont.) Tracheal fracture and esophageal ruptureTracheal fracture and esophageal rupture
• These are two special causes of pneumothorax that These are two special causes of pneumothorax that require surgical repair.require surgical repair.
IatrogenicIatrogenic Most common cause of traumatic pneumothoraxMost common cause of traumatic pneumothorax Common iatrogenic causes areCommon iatrogenic causes are
• Needle aspiration lung biopsyNeedle aspiration lung biopsy
• ThoracentesisThoracentesis
• Central venous catheter placementCentral venous catheter placement

Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 25
Pneumothorax (cont.)Pneumothorax (cont.)Neonatal Neonatal Spontaneous pneumothorax occurs in 1–2% of infantsSpontaneous pneumothorax occurs in 1–2% of infants
Likely caused by high transpulmonary pressures and Likely caused by high transpulmonary pressures and transient bronchial blockage (i.e. meconium)transient bronchial blockage (i.e. meconium)
Recognition is difficultRecognition is difficult Contralateral heart sounds may be a clue.Contralateral heart sounds may be a clue. Transillumination of thorax may be useful. Transillumination of thorax may be useful.
Most neonates with this condition require chest tubes.Most neonates with this condition require chest tubes.

Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 26
Pneumothorax (cont.)Pneumothorax (cont.)
SpontaneousSpontaneous Pneumothorax with no obvious causePneumothorax with no obvious cause
Primary spontaneous pneumothoraxPrimary spontaneous pneumothorax Occurs with no underlying lung diseaseOccurs with no underlying lung disease Most (80%) have small subpleural blebsMost (80%) have small subpleural blebs Typically happens in tall, thin, young adultsTypically happens in tall, thin, young adults >90% have had short-term smoking history>90% have had short-term smoking history
• Smoking cessation recommendedSmoking cessation recommended
Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 27
Pneumothorax (cont.)Pneumothorax (cont.)
Secondary spontaneous pneumothoraxSecondary spontaneous pneumothorax Occurs with underlying lung diseaseOccurs with underlying lung disease
• Most common associated disease is COPDMost common associated disease is COPD
• Also seen during exacerbations of asthma and CFAlso seen during exacerbations of asthma and CF
• Interstitial lung diseases with normal lung volumesInterstitial lung diseases with normal lung volumes Sarcoidosis, BOOPSarcoidosis, BOOP
Depending on extent of disease, pneumothorax Depending on extent of disease, pneumothorax can be devastatingcan be devastating• 43% 5-year mortality43% 5-year mortality
Evacuation, not observation, should be the Evacuation, not observation, should be the standard of care with these patients.standard of care with these patients.
Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 28
Pneumothorax (cont.)Pneumothorax (cont.)ComplicationsComplications Tension pneumothoraxTension pneumothorax
Pleural air pressure exceeds atmospheric pressurePleural air pressure exceeds atmospheric pressure Radiographic appearanceRadiographic appearance
• Mediastinal shift, diaphragmatic depression, flattened ribsMediastinal shift, diaphragmatic depression, flattened ribs
Clinical presentationClinical presentation• Venous return and cardiac output decrease with Venous return and cardiac output decrease with
hypotension and tachycardiahypotension and tachycardia
• Hypoxemia due to alveolar collapseHypoxemia due to alveolar collapse
Treatment: emergency needle decompression Treatment: emergency needle decompression
Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 29
Pneumothorax (cont.)Pneumothorax (cont.)
ComplicationsComplications Reexpansion pulmonary edemaReexpansion pulmonary edema
Occurs following rapid lung reexpansion Occurs following rapid lung reexpansion particularly:particularly:• From low lung volumesFrom low lung volumes
• Long duration pneumothorax Long duration pneumothorax
• High pressure gradient across lungHigh pressure gradient across lung
May be related to reperfusion injuryMay be related to reperfusion injury Lung reexpansion should be slowLung reexpansion should be slow
• First, just waterseal, no suctionFirst, just waterseal, no suction
• If lung fails to reexpand, then apply suctionIf lung fails to reexpand, then apply suction

Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 30
Pneumothorax (cont.)Pneumothorax (cont.)
DiagnosisDiagnosis Chest radiographyChest radiography
Requires good quality film Requires good quality film In ICU, 30% of pneumothoraces are missed due In ICU, 30% of pneumothoraces are missed due
to:to:• Low-quality filmLow-quality film
• Supine position of patient on AP filmSupine position of patient on AP film• Air hidden behind thoracic or mediastinal structuresAir hidden behind thoracic or mediastinal structures
CT may be used to confirm size and CT may be used to confirm size and presence of pneumothorax.presence of pneumothorax.
Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 31
Pneumothorax (cont.)Pneumothorax (cont.)
TherapyTherapy OxygenOxygen
Should be administered to all patientsShould be administered to all patients Supplemental OSupplemental O22 speeds absorption of air from speeds absorption of air from
pleural spacepleural space
Observation of stable patientsObservation of stable patients Primary: observe 4 hours, if no enlargement: homePrimary: observe 4 hours, if no enlargement: home Secondary and iatrogenic: hospitalize and observe Secondary and iatrogenic: hospitalize and observe
carefully, carefully, • If there is any deterioration (SpOIf there is any deterioration (SpO22, RR, etc) - drain , RR, etc) - drain
Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 32
Pneumothorax (cont.)Pneumothorax (cont.)
TherapyTherapy Simple aspirationSimple aspiration
Small catheter placed in pleural spaceSmall catheter placed in pleural space Connect to three-way stopcockConnect to three-way stopcock Slowly evacuate until no more air can be removedSlowly evacuate until no more air can be removed This works as many leaks heal between time of This works as many leaks heal between time of
leak and its drainage.leak and its drainage.
If 4 L air is removed without resistance, chest If 4 L air is removed without resistance, chest tube placement is requiredtube placement is required

Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 33
Pneumothorax (cont.)Pneumothorax (cont.)TherapyTherapy Chest tubes buy timeChest tubes buy time
Resolution is mostly determined by lung healing Resolution is mostly determined by lung healing Small bore: placed via small incision in second Small bore: placed via small incision in second
intercostal space (ICS), midclavicular line or intercostal space (ICS), midclavicular line or laterally, fifth–seventh ICSlaterally, fifth–seventh ICS• Connected to underwater seal or Heimlich valveConnected to underwater seal or Heimlich valve
Large bore: placed via blunt dissection, usually Large bore: placed via blunt dissection, usually connected to “three-bottle” chest drainage systemconnected to “three-bottle” chest drainage system
Chest tubes are sutured in placeChest tubes are sutured in place
Pleurodesis: consider with recurrent pneumothoracesPleurodesis: consider with recurrent pneumothoraces
Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 34
Pneumothorax (cont.)Pneumothorax (cont.)
Bronchopleural fistulaBronchopleural fistula Usually used to refer to large, persistent air leaksUsually used to refer to large, persistent air leaks
Most are on MVMost are on MV PPV perpetuates the leakPPV perpetuates the leak
May require more than one chest tubeMay require more than one chest tube Aids restoring lung proximity to chest wall and promotes Aids restoring lung proximity to chest wall and promotes
healinghealing
Avoid auto-PEEP, consider bronchoscopic closure or Avoid auto-PEEP, consider bronchoscopic closure or thoracoscopic surgerythoracoscopic surgery