chapter 3 laws and ethics.pdf
TRANSCRIPT

Laws and Ethics
3c h a p t e r
administrative lawsadvance directiveallocation of scarce
resourcesanecdotal recordassaultbatteryboard of nursingcivil lawscode of ethicscode statuscommon lawconfidentialitycriminal lawsdefamationdefendantdeontologydurable power of
attorney for healthcaredutyethical dilemmaethicsfalse imprisonmentfelony
Good Samaritan lawsincident reportintentional tortinvasion of privacylawsliability insurancelibelliving willmalpracticemisdemeanornegligencenurse practice actplaintiffreciprocityrestraintsrisk managementslanderstatute of limitationsstatutory lawsteleologytorttruth tellingunintentional tortwhistle-blowing
Learning Objectives
On completion of this chapter, the reader will:
● Name six types of laws.● Discuss the purpose of nurse practice acts and the role of the state board
of nursing.● Explain the difference between intentional and unintentional torts.● Describe the difference between negligence and malpractice.● Identify three reasons it is advantageous for a nurse to obtain profes-
sional liability insurance.● List five ways that a nurse’s professional liability can be mitigated in the
case of a lawsuit.● Define the term ethics.● Explain the purpose for a code of ethics.● Describe two types of ethical theories.● List five ethical issues common in nursing practice.
Words to Know
Laws, ethics, client rights, and nursing duties affectnurses throughout their careers. This chapter introducesbasic legal and ethical concepts and issues that affect thepractice of nursing.
LAWS●
Laws (rules of conduct established and enforced by thegovernment of a society) are intended to protect both thegeneral public and each person. There are six categories
of laws: constitutional, statutory, administrative, com-mon, criminal, and civil (Table 3-1).
Constitutional Law
The founders of the United States wrote the country’sfirst set of formal laws within the framework of the Con-stitution. This document, which has endured with fewamendments, divides power among three branches ofgovernment and establishes the process of checks and
Unit 2 Integrating Basic Concepts

balances, protecting the entire nation. It also identifiesthe rights and privileges to which all U.S. citizens areentitled. Two examples of rights protected by constitu-tional law are free speech and privacy.
Statutory Laws
Statutory laws (laws enacted by federal, state, or locallegislatures) sometimes are identified as public acts, codes,or ordinances. For example, the legislative branch of stategovernments assumes responsibility for enacting statutesthat ensure the competence of those who provide healthcare. A nurse practice act (statute that legally defines theunique role of the nurse and differentiates it from thatof other health care practitioners, such as physicians) isone example of a statutory law (Box 3-1). Although eachstate’s nurse practice act is unique, all generally containcommon elements:
• They define the scope of nursing practice.• They establish the limits to that practice.• They identify the titles that nurses may use, such as
licensed practical nurse (LPN), licensed vocationalnurse (LVN), or registered nurse (RN).
• They authorize a board of nursing to oversee nurs-ing practice.
• They determine what constitutes grounds for disci-plinary action.
Administrative Laws
Administrative laws (legal provisions through whichfederal, state, and local agencies maintain self-regulation)affect the power to manage governmental agencies. Someadministrative laws give federal and state governmentsthe legal authority to ensure the health and safety of theircitizens. The state board of nursing is an example of anadministrative agency that enforces administrative law.
30 UNIT 2 ● Integrating Basic Concepts
TABLE 3.1 TYPES OF LAWS
CATEGORY PURPOSE EXAMPLES
Constitutional Law
Statutory Law
Administrative Law
Common Law
Criminal Law
Civil Law
Protects fundamental rights and freedoms ofU.S. citizens
Defines the duties and limitations of theexecutive, legislative, and judicial branchesof government
Identifies local, state, or federal rulesnecessary for the public’s welfare
Develops regulations by which to carry outthe mission of a public agency
Interprets legal issues based on previouscourt decisions in similar cases (legalprecedents)
Determines the nature of criminal acts thatendanger all society
Determines the circumstances and manner inwhich a person may be compensated forbeing the victim of another person’s actionor omission of an action
Bill of Rights, freedom of speech
Public health ordinances, tax laws, nursepractice acts
State boards of nursing, which enact andenforce rules as they relate to nursepractice acts
Tarasoff vs. Board of Regents of Universityof California [1976], which justifiesbreaching a client’s confidentiality if he orshe reveals the identity of a potentialvictim of crime
Identifies the differences in first-degree andsecond-degree murder, manslaughter, etc.
Dereliction of duty, negligence
The practice of nursing means the performance of services provided for pur-poses of nursing diagnosis and treatment of human responses to actual orpotential health problems consistent with educational preparation. Knowl-edge and skill are the basis for assessment, analysis, planning, intervention,and evaluation used in the promotion and maintenance of health and nurs-ing management of illness, injury, infirmity, restoration of optional function,or death with dignity. Practice is based on understanding the human condi-tion across the human lifespan and understanding the relationship of theindividual within the environment. This practice includes execution of themedical regime including the administration of medications and treatmentsprescribed by any person authorized by state law to so prescribe.
From Oklahoma Nursing Practice Act, 2001. Oklahoma Statutes, Title 59, Chapter 12,Section 567.1 et seq. http://www.ncsbn.org/public/regulation/nursing_practice_acts.htm.
BOX 3-1 ● Scope of Nursing Practice as Defined in Sample Nurse Practice Act

Each state’s board of nursing (regulatory agency formanaging the provisions of a state’s nurse practice act) hasa primary responsibility to protect the public receivingnursing care within the state. Some activities of the state’sboard of nursing include (1) reviewing and approvingnursing education programs in the state, (2) establishingcriteria for licensing nurses, (3) overseeing procedures fornurse licensing examinations, (4) issuing and transferringnursing licenses, (5) investigating allegations such assubstance abuse against nurses licensed in that state,and (6) disciplining nurses who violate legal and ethicalstandards.
The state’s board of nursing is responsible for sus-pending and revoking licenses and reviewing applicationsasking for reciprocity (licensure based on evidence ofhaving met licensing criteria in another state). A licensein one state does not give a person a right to automaticlicensure in another. Reciprocity is important for nurseswho live in one state and work in another, those who wishto practice in more than one state, or those who movefrom one state to another. Reciprocity has been abused: inthe past, a nurse whose license had been revoked as apunitive measure in one state could move to another andobtain a license there. Legislation has been enacted, how-ever, to track incompetent practitioners. Since 1989, thenames of licensed health care workers who have been dis-ciplined by hospitals, courts, licensing boards, profes-sional associations, insurers, and peer review committeesare submitted to a National Practitioner Data Bank, acomputerized resource sponsored by the Office of QualityAssurance, a branch of the Department of Health andHuman Services. The information is made available tolicensing boards and health care facilities that hire nursesthroughout the nation.
Common Law
Common law (decisions based on prior cases of a simi-lar nature) is also known as judicial law. It is based on aprinciple referred to as stare decisis (“let the decisionstand”), in which prior outcomes serve as guidelines fordecisions in other jurisdictions dealing with comparablecircumstances. Common law refers to litigation that fallsoutside the realm of constitutional, statutory, and admin-istrative laws.
Criminal Laws
Criminal laws (penal codes that protect the safety of allcitizens from people who pose a threat to the public good)are used to prosecute those who commit crimes. The staterepresents “the people” when prosecuting those accusedof crimes. Crimes are either misdemeanors or felonies.
A misdemeanor is a minor criminal offense. An exam-ple is shoplifting. If a person is convicted of a mis-demeanor, a small fine, a short period of incarceration, orboth may be levied. The fine is paid to the state.
A felony is a serious criminal offense. Examplesinclude murder, falsifying medical records, insurancefraud, and stealing narcotics. Conviction is punishableby a lengthy prison term or even execution. The stategenerally prohibits felons from obtaining an occupa-tional license, and the state will revoke such a license ifits holder is convicted of a felony.
Civil Laws
Civil laws (statutes that protect personal freedoms andrights) apply to disputes that arise between individual cit-izens. Some examples include laws that protect the rightto be left alone, freedom from threats of injury, freedomfrom offensive contact, and freedom from characterattacks. In civil cases, the plaintiff (person claiminginjury) brings charges against the defendant (personcharged with violating the law). The case is referred to asa tort (litigation in which one person asserts that aninjury, which may be physical, emotional, or financial,occurred as a consequence of another person’s actions orfailure to act). A tort implies that a person breached hisor her duty to another person. A duty is an expectedaction based on moral or legal obligations.
It does not take the same quality or quantity of evi-dence to be convicted in a civil lawsuit as in a criminalcase. If a defendant is found guilty of a tort, he or she isrequired to pay the plaintiff restitution for damages.Torts are classified as intentional or unintentional.
Intentional Torts
Intentional torts are lawsuits in which a plaintiffcharges that a defendant committed a deliberately aggres-sive act. Examples include assault, battery, false impris-onment, invasion of privacy, and defamation.
ASSAULT. Assault is an act in which there is a threat oran attempt to do bodily harm. Such harm may be in theform of physical intimidation, remarks, or gestures. Theplaintiff interprets the threat to mean that force may beforthcoming. A nurse may be accused of assault if he orshe verbally threatens to restrain a client unnecessarily(e.g., to curtail the use of the signal light).
BATTERY. Battery (unauthorized physical contact) caninclude touching a person’s body, clothing, chair, or bed.A plaintiff can claim battery even if the contact does notactually cause him or her physical harm. The criterion isthat the contact took place without the plaintiff’s consent.
CHAPTER 3 ● Laws and Ethics 31

Sometimes nonconsensual physical contact can be jus-tified. For example, health professionals can use physicalforce to subdue clients with mental illness or those underthe influence of alcohol or drugs if their actions endangertheir own safety or that of others. Documentation mustshow, however, that the situation required the degree ofrestraint used. Excessive force is never appropriate whenless would have been effective. When recording infor-mation about such situations, nurses must describe thebehavior and the client’s response when lesser forms ofrestraint were used first.
To protect health care workers from being chargedwith battery, adult clients are asked to sign a general per-mission for care and treatment at the time of admission(Fig. 3-1) and additional written consent forms for tests,procedures, or surgery. The physician must provide thefollowing information when seeking consent for specifictypes of treatment:
• Description of the proposed intervention• Potential benefits• Risks involved• Expected outcome• Available alternatives• Consequences if the intervention is not performed
Health care personnel obtain consent from a parentor guardian if the client is a minor, mentally retarded,or mentally incompetent. In an emergency, consent canbe implied. In other words, it is assumed that in life-threatening circumstances, a client would give consent fortreatment if he or she were able to understand the risks. Inmost cases, another physician must concur that the emer-gency procedure is essential (Marquis & Huston, 2003).
FALSE IMPRISONMENT. A plaintiff can allege false impris-onment (interference with a person’s freedom to moveabout at will without legal authority to do so) if a nursedetains a competent client from leaving the hospital orother health care agency. If a client wants to leave withoutbeing medically discharged, it is customary for him or herto sign a form indicating personal responsibility for leav-ing against medical advice (AMA) (Fig. 3-2). If the clientrefuses to sign the paper, however, health care personnelcannot bar him or her from leaving.
Forced confinement is legal under two conditions: ifthere is a judicial restraining order (e.g., a prisoneradmitted for medical care) or if there is a court-orderedcommitment (e.g., a client with mental illness who is dan-gerous to self or others).
Restraints are devices or chemicals that restrictmovement. They are used with the intention to subdue aclient’s activity. Types of restraints include cloth limbrestraints, bedrails, chairs with locking lap trays, and seda-tive drugs. Unnecessary or unprescribed restraints canlead to charges of false imprisonment, battery, or both.
The Nursing Home Reform Act of the Omnibus Bud-get Reconciliation Act (OBRA) passed in 1987 and imple-
mented in 1990 states that residents in nursing homeshave “the right to be free of, and the facility must ensurefreedom from, any restraints imposed or psychoactivedrug administered for purposes of discipline or conve-nience, and not required to treat the residents’ medicalsymptoms.” This is not to say that restraints cannot beused; rather, that they should be used as a last resortrather than the initial intervention. Their use must bejustified and accompanied by informed consent from theclient or a responsible relative.
Before using restraints, the best legal advice is to tryalternative measures for protecting wandering clients,reducing the potential for falls (see Chap. 18), and ensur-ing that clients do not jeopardize medical treatment bypulling out feeding tubes or other therapeutic devices. Ifless restrictive alternatives are unsuccessful, nurses mustobtain a medical order before each and every instance inwhich they use restraints. In acute care hospitals, medicalorders for restraints are renewed every 24 hours. Oncerestraints are applied, charting must indicate regularclient assessment; provisions for fluids, nourishment, andbowel and bladder elimination; and attempts to releasethe client from the restraints for a trial period. Once theclient is no longer a danger to self or others, nurses mustremove the restraints.
INVASION OF PRIVACY. Civil law protects individuals frominvasion of privacy (failure to leave people and theirproperty alone). Nonmedical examples include trespass-ing, illegal search and seizure, wiretapping, and revealingpersonal information about someone, even if true. Exam-ples of privacy violations in health care include photo-graphing a client without consent, revealing a client’sname in a public report, or allowing an unauthorized per-son to observe the client’s care. To ensure and protectclients’ rights to privacy, medical records and informationare kept confidential. Personal names and identities areconcealed or obliterated in case studies or research. Pri-vacy curtains are used during care, and permission isobtained if a nursing or medical student will be present asan observer during a procedure.
DEFAMATION. Defamation (an act in which untrue infor-mation harms a person’s reputation) is unlawful. Exam-ples include slander (character attack uttered orally inthe presence of others) and libel (damaging statementswritten and read by others). Injury is considered to occurbecause the derogatory remarks attack a person’s charac-ter and good name.
If a client accuses a nurse of defamation of character,the client must prove that there was malice, misuse ofprivileged information, and spoken or written untruths.Nurses are at risk for defamation of character suits if theymake negative comments in public areas like elevators orcafeteria, or assert opinions regarding a client’s characterin the medical record. To avoid accusations of defama-tion, nurses must avoid making or writing negative com-ments about clients, physicians, or other coworkers.
32 UNIT 2 ● Integrating Basic Concepts

CHAPTER 3 ● Laws and Ethics 33
FIGURE 3.1 Consent for treatment form. (From Timby, B. K., & Smith, N. E. [2003]. Introductory medical-surgical nursing [8th ed.]. Philadelphia: Lippincott Williams & Wilkins, p. 34.)

Unintentional Torts
Unintentional torts are situations that result in aninjury, although the person responsible did not mean tocause harm. The two types of unintentional torts involveallegations of negligence and malpractice.
NEGLIGENCE. Negligence (harm that results because aperson did not act reasonably) implies that a personacted carelessly. In cases of negligence, a jury decideswhether any other prudent person would have acted dif-ferently than the defendant, given the same set of cir-cumstances. For example, a person’s car breaks down onthe highway, and the driver pulls off to the side of theroad, raises the hood, and activates the emergency flash-ing lights. If another vehicle strikes the disabled car andthe driver of the second car sues, the guilt or innocenceof the driver of the disabled car hinges on whether thejury believes the driver’s action was reasonable. Reason-ableness is based on the jury’s opinion of what constitutesgood common sense.
MALPRACTICE. Malpractice is professional negligence,which differs from simple negligence. It holds profession-als to a higher standard of accountability. Rather thanbeing held accountable for acting as an ordinary, reason-
able lay person, in a malpractice case the court determineswhether a nurse or other health care worker acted in amanner comparable to that of his or her peers. The plain-tiff must prove four elements to win a malpractice lawsuit:duty, breach of duty, causation, and injury (Box 3-2).
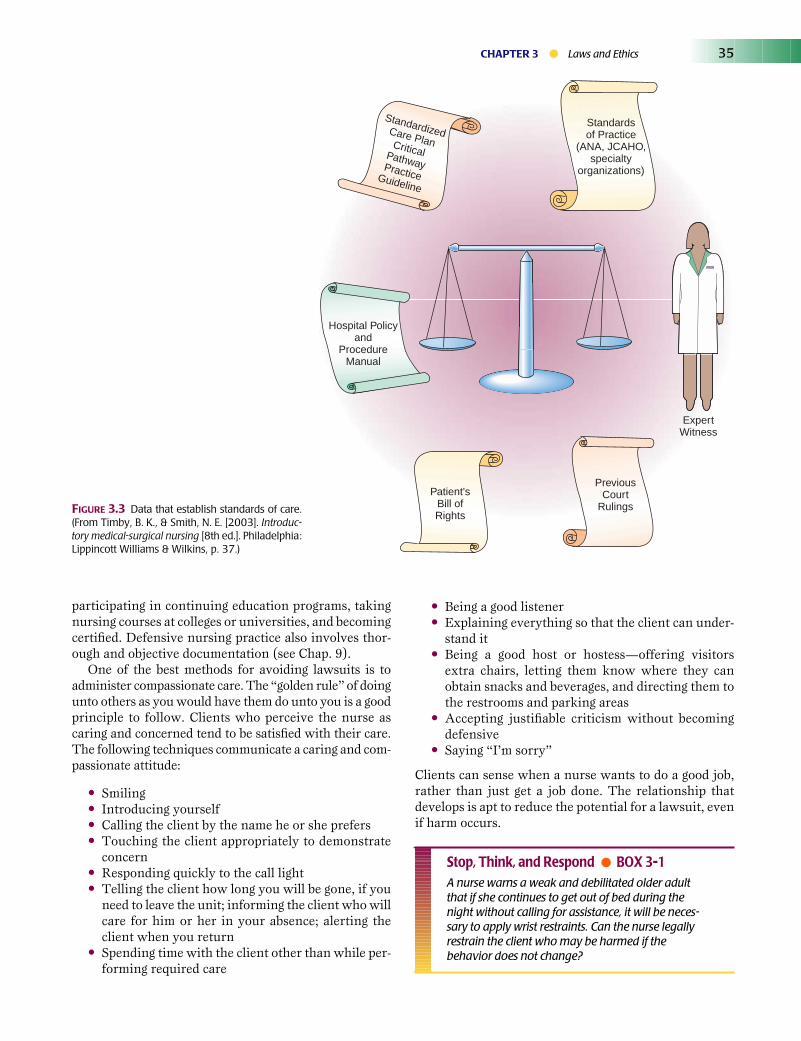
Because the jury may be unfamiliar with the scope ofnursing practice, the plaintiff may present other resourcesin court to prove breach of duty. Some examples includethe employing agency’s standards for care, written policiesand procedures, care plans or clinical pathways, and thetestimony of expert witnesses (Fig. 3-3).
The best protection against malpractice lawsuits iscompetent nursing. Nurses demonstrate competency by
34 UNIT 2 ● Integrating Basic Concepts
Duty—An obligation existed to provide care for the person who claims tohave been injured or harmed.Breach of Duty—The nurse failed to provide appropriate care, or the care pro-vided was given negligently; that is, in a way that conflicts with how others withsimilar education would have acted given the same set of circumstances.Causation—The professional’s action, or lack of it, caused the plaintiff harm.Injury—Physical, psychological, or financial harm occurred.
BOX 3-2 ● Elements in a Malpractice Case
FIGURE 3.2 Release form for discharging oneself against medical advice.
participating in continuing education programs, takingnursing courses at colleges or universities, and becomingcertified. Defensive nursing practice also involves thor-ough and objective documentation (see Chap. 9).
One of the best methods for avoiding lawsuits is toadminister compassionate care. The “golden rule” of doingunto others as you would have them do unto you is a goodprinciple to follow. Clients who perceive the nurse ascaring and concerned tend to be satisfied with their care.The following techniques communicate a caring and com-passionate attitude:
• Smiling• Introducing yourself• Calling the client by the name he or she prefers• Touching the client appropriately to demonstrate
concern• Responding quickly to the call light• Telling the client how long you will be gone, if you
need to leave the unit; informing the client who willcare for him or her in your absence; alerting theclient when you return
• Spending time with the client other than while per-forming required care
• Being a good listener• Explaining everything so that the client can under-
stand it• Being a good host or hostess—offering visitors
extra chairs, letting them know where they canobtain snacks and beverages, and directing them tothe restrooms and parking areas
• Accepting justifiable criticism without becomingdefensive
• Saying “I’m sorry”
Clients can sense when a nurse wants to do a good job,rather than just get a job done. The relationship thatdevelops is apt to reduce the potential for a lawsuit, evenif harm occurs.
Stop, Think, and Respond ● BOX 3-1A nurse warns a weak and debilitated older adultthat if she continues to get out of bed during thenight without calling for assistance, it will be neces-sary to apply wrist restraints. Can the nurse legallyrestrain the client who may be harmed if thebehavior does not change?
CHAPTER 3 ● Laws and Ethics 35
Standardsof Practice
(ANA, JCAHO,specialty
organizations)
Hospital Policyand
ProcedureManual
PreviousCourt
RulingsPatient's
Bill ofRights
StandardizedCare PlanCriticalPathwayPracticeGuideline
ExpertWitness
FIGURE 3.3 Data that establish standards of care.(From Timby, B. K., & Smith, N. E. [2003]. Introduc-tory medical-surgical nursing [8th ed.]. Philadelphia:Lippincott Williams & Wilkins, p. 37.)

PROFESSIONAL LIABILITY●
All professionals, including nurses, are held responsibleand accountable for providing safe, appropriate care.Because nurses have specialized knowledge and proxim-ity to clients, they have a primary role in protecting clientsfrom preventable or reversible complications.
The number of lawsuits involving nurses is increasing.Therefore, it is to every nurse’s advantage to obtain liabil-ity insurance and to become familiar with legal mecha-nisms, such as Good Samaritan laws and statutes oflimitations, that may prevent or relieve culpability, as wellas with strategies for providing a sound legal defense, suchas written incident reports and anecdotal records.
Liability Insurance
Liability insurance (a contract between a person or cor-poration and a company willing to provide legal servicesand financial assistance when the policyholder is involvedin a malpractice lawsuit) is a necessity for all nurses.Although many agencies that employ nurses have liabil-ity insurance with an umbrella clause that includes itsemployees, nurses should obtain their own personal lia-bility insurance. The advantage is that the nurse involvedin a lawsuit will have a separate attorney working on hisor her sole behalf. Because the damages sought in mal-practice lawsuits are so costly, attorneys hired by healthcare facilities sometimes are more committed to defendingthe facility against liability and negative publicity, ratherthan defending an employed nurse whom they also arebeing paid to represent.
Student nurses are held accountable for their actionsduring clinical practice and should also carry liabilityinsurance. Liability insurance is available through theNational Federation for Licensed Practical Nurses, theNational Student Nurses’ Association, the AmericanNurses Association (ANA), and other private insurancecompanies.
Reducing Liability
It is unrealistic to think that lawsuits can be avoided com-pletely, but some avenues protect nurses and other healthcare workers from being sued or provide a foundation fora sound legal defense. Examples include Good Samaritanlaws, statutes of limitations, principles regarding assump-tion of risk, appropriate documentation, risk manage-ment, incident reports, and anecdotal records.
Good Samaritan Laws
Most states have enacted Good Samaritan laws, or lawsthat provide legal immunity to passersby who provideemergency first aid to victims of accidents. The legislationis based on the Biblical story of the person who gave aid
to a beaten stranger along a roadside. The law defines anemergency as one occurring outside a hospital, not in anemergency department.
Although laws of this nature are helpful, no GoodSamaritan law provides absolute exemption from prose-cution in the event of injury. Paramedics, ambulancepersonnel, physicians, and nurses who stop to provideassistance are still held to a higher standard of carebecause they have training above and beyond that of aver-age lay persons. In cases of gross negligence (total dis-regard for another’s safety), health care workers may becharged with a criminal offense.
Statute of Limitations
Each state establishes a statute of limitations (desig-nated time within which a person can file a lawsuit). Thelength of time varies among states and generally is calcu-lated from when the incident occurred. When the injuredparty is a minor, however, the statute of limitations some-times does not commence until the victim reaches adult-hood. Once the time period expires, an injured party canno longer sue, even if his or her claim is legitimate.
Assumption of Risk
If a client is forewarned of a potential hazard to his or hersafety and chooses to ignore the warning, the court mayhold the client responsible. For example, if a hospitalizedclient objects to having the side rails up or lowers therails independently, the nurse or healthcare facility maynot be held fully accountable if an injury occurs. It isessential that the nurse document that he or she warnedthe client and that the client disregarded the warning.The same recommendation applies when nurses cautionclients about ambulating only with assistance.
Documentation
A major component to limiting liability is accurate, thor-ough documentation. Nurses are held responsible or liablefor information that they either include or exclude inreports and documentation. Each healthcare setting re-quires accurate and complete documentation. The med-ical record is a legal document and is used as evidence incourt. Records must be timely, objective, accurate, com-plete, and legible (see Chapter 9). The quality of the docu-mentation, including neatness and spelling, can influencea jury’s decision.
Risk Management
Risk management (process of identifying and reducingthe costs of anticipated losses) is a concept originallydeveloped by insurance companies. Health care institu-tions have now adopted risk management as well. In doingso, they employ risk managers to review all the problemsthat occur in the workplace, identify common elements,and then develop methods to reduce their risk. A primarytool of risk management is the incident report.
36 UNIT 2 ● Integrating Basic Concepts

Incident Reports
An incident report is a written account of an unusualevent involving a client, employee, or visitor that has thepotential for being injurious (Fig. 3-4). It is kept separatefrom the medical record. Incident reports serve two pur-poses: to determine how to prevent hazardous situations,and to serve as a reference in case of future litigation.Incident reports must include five important pieces:
• When the incident occurred• Where it took place• Who was involved• What happened• What actions were taken at the time
All witnesses are identified by name. Any pertinentstatements made by the injured person, before or after theincident, are quoted. Accurate and detailed documenta-tion often helps to prove that the nurse acted reasonablyor appropriately in the circumstances.
Anecdotal Records
An anecdotal record (personal, handwritten account ofan incident) is not recorded on any official form, nor isit filed with administrative records. The information isretained by the nurse. The notation is safeguarded andmay be used later to refresh the nurse’s memory if a law-suit develops. Anecdotal notes can be used in court onadvice of an attorney.
Malpractice Litigation
A successful outcome in a malpractice lawsuit depends onmany variables, such as the physical evidence and theexpertise of one’s lawyer. The appearance, demeanor, andconduct of the nurse defendant inside and outside thecourtroom, however, can help or damage the case. Thesuggestions in Box 3-3 may be helpful if a nurse becomesinvolved in malpractice litigation.
ETHICS●
The word ethics comes from the Greek word ethos,meaning customs or modes of conduct. Ethics (moral orphilosophical principles) direct actions as being eitherright or wrong. Various organizations, such as those rep-resenting nurses, have identified standards for ethicalpractice, known as a code of ethics, for members withintheir discipline.
Codes of Ethics
A code of ethics (a list of written statements describingideal behavior) serves as a model for personal conduct.The National Association for Practical Nurse Education
and Services, the National Federation for Licensed Prac-tical Nurses, and the International Council of Nursesare examples of organizations that have composed codesof ethics. Box 3-4 is the ANA’s current code of ethics.Because of rapidly changing technology, no code of ethicsis ever specific enough to provide guidelines for each andevery dilemma that nurses may face.
Ethical Dilemmas
An ethical dilemma (choice between two undesirablealternatives) occurs when individual values and lawsconflict. This is especially true in relation to health care.Occasionally, nurses find themselves in situations thatmay be considered legal but are personally unethical, orare ethical but illegal. For instance, abortion is legal, butsome believe it is unethical. Assisted suicide is illegal(except in Oregon), but some believe it is ethical.
Ethical Theories
Nurses generally use one of two ethical problem-solvingtheories, either teleology or deontology, to guide them insolving ethical dilemmas.
Teleologic Theory
Teleology is ethical theory based on final outcomes. It isalso known as utilitarianism, because the ultimate ethi-cal test for any decision is based on what is best for themost people. Stated from a different perspective, teleolo-gists believe “the end justifies the means.” Therefore, thechoice that benefits many people justifies the harm thatmay come to a few. A teleologist would argue that selec-tive abortion (destroying some fetuses in a multiple preg-nancy) is ethically correct because it is done to ensurethe full-term birth of the remaining healthy fetuses. Inother words, terminating the life of a fetus is justified insome situations but may not be justified in all cases.
Teleologists analyze ethical dilemmas on a case-by-case basis. They propose that an action is not good or badin and of itself. Instead, the consequences determine ifthe action is good or bad. The primary consideration is adesirable outcome for those most affected.
Deontologic Theory
Deontology is ethical study based on duty or moral obli-gations. It proposes that the outcome is not the primaryissue—rather, decisions must be based on the ultimatemorality of the act itself. In other words, certain actionsare always right or wrong regardless of extenuating cir-cumstances. Deontologists would argue that destroyingany fetus is wrong, whether it is done to save others or not,because killing is always immoral. Deontology proposesthat health care providers have a moral duty to maintainand preserve life. Therefore, it is immoral for a nurse to
CHAPTER 3 ● Laws and Ethics 37

38 UNIT 2 ● Integrating Basic Concepts
FIGURE 3.4 An incident report form.

assist with abortion, to assist a terminally ill person withsuicide, or to support the execution of a convicted prisoner.
Deontology also proposes that moral duty to others isequally as important as consequences. A duty is an oblig-ation to perform or to avoid an action to which others areentitled. For example, deontologists believe that lyingis never acceptable because it violates the duty to tellthe truth to those who are entitled to honest informa-tion. Nurses ultimately have a professional duty to theirclients, and clients have rights to which they are entitled(Box 3-5).
CHAPTER 3 ● Laws and Ethics 39
1. The nurse, in all professional relationships, practices with compassionand respect for the inherent dignity, worth and uniqueness of every indi-vidual, unrestricted by considerations of social or economic status, personal attributes, or the nature of health problems.
2. The nurse’s primary commitment is to the patient, whether an individual,family, group or community.
3. The nurse promotes, advocates for, and strives to protect the health,safety, and rights of the patient.
4. The nurse is responsible and accountable for individual nursing practiceand determines the appropriate delegation of tasks consistent with thenurse’s obligation to provide optimum patient care.
5. The nurse owes the same duties to self as to others, including theresponsibility to preserve integrity and safety, to maintain competence,and to continue personal and professional growth.
6. The nurse participates in establishing, maintaining, and improvinghealthcare environments and conditions of employment conducive tothe provision of quality health care and consistent with the values of theprofession through individual and collective action.
7. The nurse participates in the advancement of the profession throughcontributions to practice, education, administration, and knowledgedevelopment.
8. The nurse collaborates with other health professionals and the publicin promoting community, national, and international efforts to meethealth needs.
9. The profession of nursing, as represented by associations and their mem-bers, is responsible for articulating nursing values, for maintaining theintegrity of the profession and its practice, and for shaping social policy.
Reprinted with permission from American Nurses Association. (2001). Code of ethicsfor nurses with interpretive statements. Washington, DC: American Nurses Publishing.
BOX 3-4 ● Code for Nurses
1. Notify the claims agent of your professional liability insurance company.2. Contact the National Nurses Claims Data Base through the ANA. This
confidential service provides information that supports nurses involvedin litigation.
3. Discuss the particulars of the case only with your attorney.4. Tell your attorney everything.5. Avoid giving public statements.6. Reread the client’s record, incident sheet, and your anecdotal notes
before testifying.7. Ask to reread information again in court if it will help to refresh your
memory.8. Dress conservatively, in a businesslike manner. Avoid excesses in
makeup, hairstyle, or jewelry.9. Look directly at whomever asks a question.
10. Speak in a modulated but audible voice that the jury and others in thecourt can hear easily.
11. Tell the truth.12. Use language with which you are comfortable. Do not try to impress
the court with legal or medical terms.13. Say as little as possible in court under cross-examination.14. Answer the prosecuting lawyer’s questions with “Yes” or “No”; limit
answers to only the questions asked.15. If you do not know or cannot remember information, say so.16. Wait to expand on information if asked by your defense attorney.17. Remain calm, objective, and cooperative.
BOX 3-3 ● Legal Advice
1. The patient has the right to considerate and respectful care.2. The patient has the right to and is encouraged to obtain from physi-
cians and other direct caregivers relevant, current, and understandableinformation concerning diagnosis, treatment, and prognosis.
3. The patient has the right to make decisions about the plan of care priorto and during the course of treatment and to refuse a recommendedtreatment or plan of care to the extent permitted by law and hospitalpolicy and to be informed of the medical consequences of this action.
4. The patient has the right to have an advance directive (such as a livingwill, health care proxy, or durable power of attorney for health care)concerning treatment or designating a surrogate decision maker withthe expectation that the hospital will honor the intent of that directiveto the extent permitted by law and hospital policy.
5. The patient has the right to every consideration of privacy. Case discus-sion, consultation, examination, and treatment should be conducted soas to protect each patient’s privacy.
6. The patient has the right to expect that all communications andrecords pertaining to his or her care will be treated as confidential bythe hospital, except in cases such as suspected abuse and public healthhazards when reporting is permitted or required by law.
7. The patient has the right to review the records pertaining to his or hermedical care and to have the information explained or interpreted asnecessary, except when restricted by law.
8. The patient has the right to expect that, within its capacity and policies,a hospital will make reasonable response to the request of a patient forappropriate and medically indicated care and services. The hospitalmust provide evaluation, service, and/or referral as indicated by theurgency of the case.
9. The patient has the right to ask and be informed of the existence ofbusiness relationships among the hospital, educational institutions,other health care providers, or payers that may influence the patient’streatment and care.
10. The patient has the right to consent to or decline to participate in pro-posed research studies or human experimentation affecting care andtreatment or requiring direct patient involvement, and to have thosestudies fully explained prior to consent.
11. The patient has the right to expect reasonable continuity of care whenappropriate and to be informed by physicians and other caregivers ofavailable and realistic patient care options when hospital care is nolonger appropriate.
12. The patient has the right to be informed of hospital policies and practicesthat relate to patient care, treatment, and responsibilities. The patient hasthe right to be informed of available resources for resolving disputes,grievances, and conflicts. The patient has the right to be informed of thehospital’s charges for services and available payment methods.
© 1992 with permission of the American Hospital Association.
BOX 3-5 ● A Patient’s Bill of Rights

Stop, Think, and Respond ● BOX 3-2How might a teleologist and a deontologistapproach an ethical dilemma such as managingthe care of an infant with microcephaly (smallbrain and severe mental retardation) who develops a very high fever as a result of infection?
Ethical Decision-Making
It is sometimes impossible or impractical to analyze ethi-cal issues from a teleologic or deontologic point of view.Most nurses do not exclusively use the principles fromone ethical theory. Rather, ethical decisions are often theresult of the nurse’s values. Values are a person’s mostmeaningful beliefs and the basis on which he or she makesmost decisions about right or wrong. Values have commoncharacteristics. They are:
• Acquired from parental models, life experiences,and religious tenets
• Reinforced by a person’s world view• Modeled in personal behavior• Consistent over time• Defended when challenged
Most nurses possess values that pertain to autonomy,facilitating a person’s right to make choices for himself orherself without intimidation or influence; justice, beingfair to all regardless of age, gender, race, religion, or sex-ual orientation; fidelity, maintaining commitments towork-related obligations and responsibilities; and verac-ity, being honest.
The following serve as guidelines to ethical decision-making:
• Make sure that whatever is done is in the client’sbest interest.
• Preserve and support the Patient’s Bill of Rights.• Work cooperatively with the client and other health
practitioners.• Follow written policies, codes of ethics, and laws.• Follow your conscience.
Ethics Committees
Ethical decisions are complex, especially when theyaffect the lives of clients. Because making a judgment foranother is a weighty responsibility, many health careagencies have established ethics committees. These com-mittees are composed of professionals and nonprofession-als representing a broad cross-section of people within thecommunity with varying viewpoints. Their diversityencourages healthy debate about ethics issues. Ethics com-
mittees are best used in a policy-making capacity beforeany specific dilemma occurs. Ethics committees are alsocalled on to offer advice, however, to protect clients’ bestinterests and to avoid legal battles.
Common Ethical Issues
Several ethical issues recur in nursing practice. Commonexamples include telling the truth, maintaining confi-dentiality, withholding or withdrawing medical treat-ment, advocating for the most ethical allocation of scarceresources, and protecting vulnerable people from unsafepractices or practitioners.
Truth Telling
Truth telling proposes that all clients have the right tocomplete and accurate information. It implies that physi-cians and nurses have a duty to tell clients the truth aboutmatters concerning their health. Health care personneldemonstrate respect for this right by explaining to theclient the status of his or her health problem, benefits andrisks of treatment, alternative forms of treatment, andconsequences if the treatment is not administered.
It is the physician’s duty to inform clients. Conflictoccurs when the client has not been given full informa-tion, when the facts have been misrepresented, or whenthe client misunderstands the information. In some cases,physicians are reluctant to talk honestly with clients orpresent the proposed treatment in a biased manner. Oftenthe nurse is forced to choose between remaining silent inallegiance to the physician or providing truthful infor-mation to the client. Either action may have frustratingconsequences.
Confidentiality
Confidentiality, or safeguarding a person’s health infor-mation from public disclosure, is the foundation for devel-oping trust. Nurses must not divulge health informationto unauthorized individuals without the client’s writtenpermission. Even giving medical information to a client’shealth insurance company requires a signed release.
Consequently, nurses must use discretion when shar-ing information verbally so that others do not hear itindiscriminately. Now that vast information about clientsis stored on computers, the duty to protect confidentialityextends to safeguarding written and electronic data.
Withholding and Withdrawing Treatment
Technology often is used to prolong life at all costs, beyondjustifying its benefits. Decisions involving life and deathmay in some cases continue to circumvent clients, a clearviolation of ethical principles. Completing advance direc-tives and determining a client’s code status ensures that
40 UNIT 2 ● Integrating Basic Concepts

a person’s health care is in accordance with his or herwishes.
ADVANCE DIRECTIVES. Legislation now makes it manda-tory to discuss the issue of terminal care with clients.Since Congress approved the Patient Self-DeterminationAct in 1990, health care agencies reimbursed throughMedicare must ask clients whether they have executedan advance directive (written statement identifying a
competent person’s wishes concerning terminal care).The two types of advance directives are a living will anda durable power of attorney for healthcare.
A living will is an instructive form of an advancedirective; that is, it is a written document that identifiesa person’s preferences regarding medical interventionsto use—or not to use—in the case of a terminal condition,irreversible coma, or persistent vegetative state with nohope of recovery (Fig. 3-5). Clients must share advance
CHAPTER 3 ● Laws and Ethics 41
FIGURE 3.5 Living will.
T/C

directives with health care providers to ensure that theyare implemented. Refer to Client and Family Teaching 3-1for information to make available to those who have orwish to complete an advance directive.
A durable power of attorney for health care des-ignates a proxy for making medical decisions when theclient becomes incompetent or incapacitated to such anextent that he or she cannot make decisions indepen-dently. The person designated with power of attorneyfor health care can give or withhold permission fortreatment procedures on the client’s behalf in end-of-lifecircumstances and also when the client is temporarilyunconscious.
Living will and durable power of attorney for healthcare are not measures reserved for older adults; any com-petent adult can initiate them. They are best composedbefore a health crisis develops to assist health care work-ers and the client’s significant others in facilitating theclient’s wishes. A living will and healthcare proxy canavoid legal expenses, delays in obtaining guardianship, ordecisions made by an ethics committee or court whenthere are no advance directives. Therefore, nurses shouldinform all clients about their right to self-determination,encourage them to compose advance directives, and sup-port the decisions they make
Code Status
A client’s code status refers to the manner in whichnurses and other healthcare personnel are required tomanage the care of the client at the time of cardiac or res-piratory arrest. Without a written order from the physi-cian to the contrary, the client is designated as a full code.A full code means that all measures to resuscitate theclient are used.
After a discussion with the physician, some clients mayindicate that they do not want any resuscitative efforts,that is, “no code” or “do not resuscitate (DNR)”, or theymay select a combination of interventions that constituteless than a full code. Some clients specify using just chem-icals (drugs) to facilitate resuscitation, but refuse cardiacdefibrillation or endotracheal intubation for mechanicalventilation. For anything less than a full code, the physi-cian must write an order to that effect in the client’s med-ical record.
Allocation of Scarce Resources
Allocation of scarce resources is the process of decid-ing how to distribute limited life-saving equipment orprocedures among several who could benefit. Such deci-sions are very difficult to make. In effect, those whoreceive the resources will have a greater potential to live,and those who do not will most likely die prematurely.One decision-making strategy is to take a “first come, firstserved” approach. Another approach is to project whatwould produce the most good for the most people, eventhough forecasting the future is humanly impossible.
Whistle-Blowing
Whistle-blowing (reporting incompetent or unethicalpractices), as the name implies, calls attention to an unsafeor potentially harmful situation. In most circumstances, itoccurs in the institution where the reporting person isemployed. For instance, a nurse may report another nurseor physician who cares for clients while under the influ-ence of alcohol or a controlled substance.
Whenever a problem is identified, the first step is toreport the situation to an immediate supervisor. If thesupervisor takes no action, the nurse faces an ethicaldilemma about what further steps to take. It may become
42 UNIT 2 ● Integrating Basic Concepts
The nurse teaches the following points:■ An advance directive is not required, but it is
encouraged.■ A lawyer is not needed to create an advance
directive; printed forms are available from healthcare agencies, organizations such as the Ameri-can Association of Retired Persons, and variousInternet sites such as http://www.ama-assn.org/publicbooklets/ livgwill.htm.
■ When filling out the form, indicate specific wishesfor the initiation or withdrawal of life-sustainingmedical treatments such as cardiopulmonary resus-citation, kidney dialysis, mechanical ventilation,use of a tube for administering food and water,obtaining comfort measures such as pain medica-tion, and donation of organs.
■ Write additional instructions if something is notaddressed in the form; for example, your instruc-tions may be different if you are pregnant.
■ Obtain the signatures of two witnesses, other thanyour physician or spouse.
■ Give a copy to your physician for your medical file.■ Tell family members or your lawyer that you have
an advance directive and its location.■ Keep the original advance directive in a place
where it can be found easily.■ Bring a copy of your advance directive whenever
you are hospitalized or admitted to a health carefacility (e.g., nursing home, extended care facility).
■ Change your advance directive by revoking oradding instructions at any time; share the re-vised copy with those who will carry out yourinstructions.
■ A separate or different advance directive is notneeded for each state; they are generally recog-nized universally within the United States.
3-1 Client and Family TeachingAdvance Directives
necessary to go beyond the administrative hierarchy andmake public revelations.
The decision to “blow the whistle” involves personalrisks and may result in grave consequences such as char-acter assassination, retribution in the form of crimesagainst one’s person or property, negative evaluations,demotions, or shunning. Nevertheless, the ethical priorityis protecting clients in general and the community at large.
Critical Thinking Exercises
1. What actions might protect a nurse from being sued when aclient assigned to his or her care falls out of bed?
2. Two people need a liver transplant; only one liver is available.If a teleologist and a deontologist were members of an ethicscommittee, what information might they use to determinewhich person should receive the organ?
● NCLEX-STYLE REVIEW QUESTIONS
1. If a nurse suspects that a colleague is stealing narcoticsand recording their administration to assigned clients,the first action the nurse should take is to:
1. Refer the nurse to the ethics committee.2. Notify the local police department.3. Share concerns with nursing peers.4. Report suspicions to a supervisor.
2. During a preadmission assessment before surgery, it ismost appropriate for the nurse to ask a client for a copyof his or her:
1. Birth certificate2. Social security number3. Advance directive4. Proof of insurance
3. After checking the condition of a client who has fallenout of bed, the nurse’s next action should be to:
1. Institute fall precautions.2. Complete an incident report.3. Call the nursing supervisor.4. Notify the client’s family.
References and Suggested Readings
Ahern, K., & McDonald, S. (2002). The beliefs of nurses whowere involved in a whistleblowing event. Journal of AdvancedNursing, 38(3), 303–309.
Aveyard, H. (2002). Implied consent prior to nursing care pro-cedures. Journal of Advanced Nursing, 39(2), 201–207.
Booth, S. (2002). A philosophical analysis of informed consent.Nursing Standard, 16(39), 43–46.
Douglas, R., & Brown, H. N. (2002). Patients’ attitudes towardadvance directives. Image: Journal of Nursing Scholarship,34(1), 61–65.
Elger, B. S., & Harding, T. W. (2002). Terminally ill patientsand Jehovah’s Witnesses: Teaching acceptance of patients’refusals of vital treatments. Medical Education, 36(5),479–488.
Fremgen, B. F. (2002). Medical law and ethics. Upper SaddleRiver, NJ: Prentice Hall.
Johnstone, M. (2002). The changing focus of health care ethics:Implications for health care professionals. ContemporaryNurse, 12(3), 213–224.
Kyba, F. C. (2002). Legal and ethical issues in end-of-life care.Critical Care Nursing Clinics of North America, 14(2),141–155.
Marquis, B. L., & Huston, C. J. (2003). Leadership roles andmanagement functions in nursing (4th ed.). Philadelphia:Lippincott Williams & Wilkins.
McDermott, A. (2002). Involving patients in discussions of do-not-resuscitate orders. Professional Nurse, 17(8), 465–468.
McDonald, S., & Ahern, K. (2002). Physical and emotionaleffects of whistleblowing. Journal of Psychosocial Nursingand Mental Health Services, 40(1), 14–27, 54–55.
Michael, J. E. (2002). Legal checkpoints. DNR orders: Proceedwith caution. Nursing Management, 33(6), 22–23, 56.
Mohr, W. K. (2002). Op-ed. Let no harm be done. Nursing Out-look, 50(2), 45–46.
O’Keefe, M. E., & Crawford, K. (2002). End-of-life care: Legaland ethical considerations. Seminars in Oncology Nursing,18(2), 143–148.
Parsons, L. C. (2002). Protecting patient rights: A nursing re-sponsibility. Policy, Politics, & Nursing Practice, 3(3), 274–278.
Russell, B. J. (2002). Health-care rationing: Critical features,ordinary language, and meaning. Journal of Law, Medicine &Ethics, 30(1), 69–72.
Shaw, S. (2002). Legal issues surrounding consent and with-drawing and withholding treatment: A case study. Nursingin Critical Care, 7(2), 94–98.
Smith, K. V., & Godfrey, N. S. (2002). Being a good nurse anddoing the right thing: A qualitative study. Nursing Ethics:An International Journal for Health Care Professionals, 9(3),269–278.
Weijer, C. (2002). I need a placebo like I need a hole in thehead. Journal of Law, Medicine & Ethics, 30(1), 69–72.
Zimring, S. D. (2002). Multi-cultural issues in advance direc-tives. Journal of the American Medical Directors Association,3(2), S88–S93.
Visit the Connection site at http://connection.lww.com/go/timbyFundamentals for links to chapter-related resources on the Internet.
CHAPTER 3 ● Laws and Ethics 43