chapter 37 inflammatory and structural heart disorders valvular heart disease
TRANSCRIPT
Chapter 37
Inflammatory and Structural Heart Disorders
Valvular Heart Disease
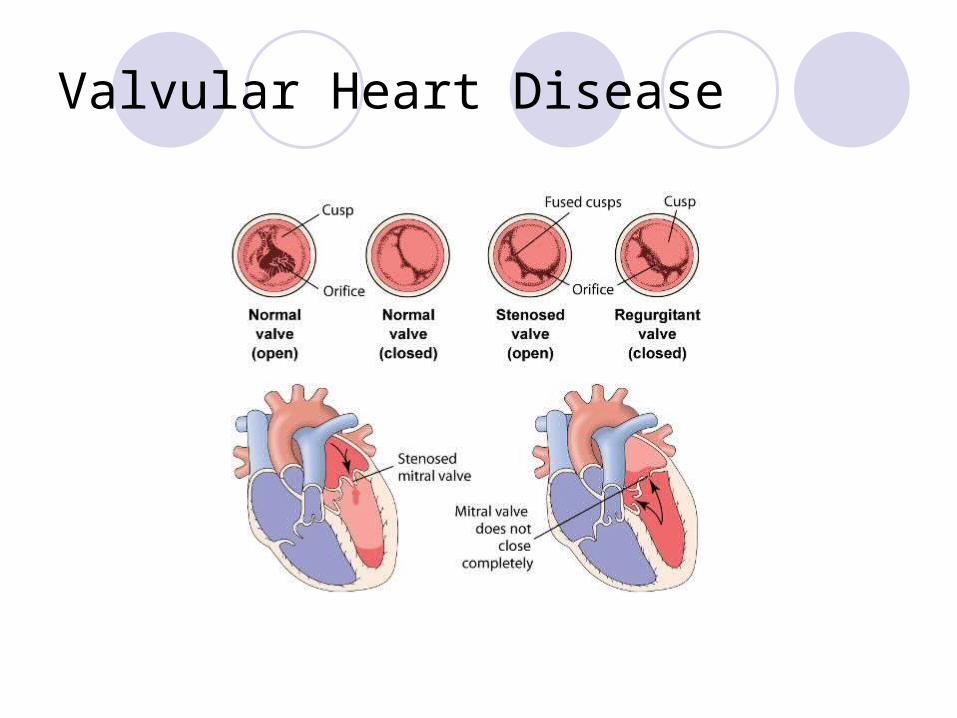
Valvular Heart Disease
Stenosis Valve orifice is restricted Impending forward blood flow Creates a pressure gradient across open valve Degree of stenosis reflected in pressure
gradient differences

Regurgitation Incomplete closure of valve leaflets Results in backward flow of blood

Mitral Stenosis
Most adult cases result from rhematic heart disease Other causes
Mitral valve becomes scarred and narrowed Left atrial overload eventually leads to right
ventricular failure
Mitral Stenosis
Manifestations include fatigue, palpitations, dysrhythmias, low pitched diastolic murmur
Mitral Regurgitation
Mitral valve fails to close properly Usually chronic Blood flows back into left ventricle, elading to
LA and LV dilation
Manifestations include symptoms of LV failure, holosystolic murmur

Mitral Valve Prolapse
One or more of the mitral valve leaflets prolapses back into the left atrium during systole
Usually congenitalUsually benign, but can be problematic if it
progresses to mitral regurgitationMost people asymptomatic, but
manifestations may include CP, dyspnea and palpitations

Aortic Stenosis
Narrowing of the aortic valve causes obstruction of blood flow form the LV to the aorta during systole
Common causes include congenital, rheumatic heart disease and senile or degenerative stenosis
Manifestations: classic triad; systolic ejection murmur

Aortic Regurgitation
Aortic valve fails to close properly Blood flow back from the aorta into the LV during
diastole-->volume overload of LV
Cause may be acute or chronic (rheumatic disease, bicuspid AV, autommune conditions)
Manifestations include signs and symptoms of LV failure (late), waterhammer pulse, high pitched diastolic murmur

Tricuspid and Pulmonic disease
Uncommon
Will manifest as RV failure
Diagnosis of valvular heart disease
History and physicalCXRECGEchocardiogramCardiac catheterization
Collaborative Care
Prophylactic antibiotic therapy Rheumatic fever, infective endocarditis
Management of associated heart failure Vasodilators (except aortic stenosis) Inotropes (digoxin) Diuretics Beta blockers
Anticoagulant therapy as indicated
Surgical Treatment
Percutaneous transluminal balloon valvuloplasty For stenotic disease
Valve repair Eg, valvuloplasty, annuloplasty
Valve replacement (prosthetic valves) Mechanical valves
Biological valves
Choice of valve depends on variety of factors
Surgical Treatment
Valve replacement Teaching
Prophylaxis
Anticoagulation


Nursing Diagnoses and Interventions
Activity intolerance
Excess fluid volume
Decreased cardiac output
Deficient knowledge
Chapter 37
Cardiomyopathies

Cardiomyopathy
Constitutes a group of diseases that directly affect the structural or functional ability of the myocardium
Three major types
Dilated Cardiomyopathy
Characterized by diffuse inflammation and rapid degeneration of the myocardium that results in ventricular and atrial dilation and impaired systolic function
May develop acutely or insidiously Manifest as heart failure, often biventricular Causes (table 37-18)

Dilated CardiomyopathyInterventions focused on improving heart
failure Enhance contractility, decrease afterload Drugs
Nitrates, diuretics, ACE inhibitors, beta blockers, aldosterone antagonists, anticoagulation
Treat underlying disease process (as able) Cardiac resychronization therapy May require VAD or transplant

Hypertrophic Cardiomyopathy
Asymmetical left ventricular hypertrophy without ventricular dilation Primary defect is diastolic dysfunction May be idiopathic, often genetic Usually seen in young adults High risk of SCD
Manifestations include dyspnea, fatigue, angina, syncope

Hypertrophic Cardiomyopathy Collaborative management
Reduce contractility and relieve outflow obstruction Drugs
Beta blockers, calcium channel blockers Nitrates, digoxin contraindicated Avoid diuretics
ICD placement Surgical treatment Teaching
Avoid strenous activity Avoid dehydration Symptoms - elevate feet

Restrictive Cardiomyopathy
Impaired ventricular fillingManifestations include signs and
symptoms of heart failureTreat to maintain cardiac output and
manage symptoms

Patient and Family Teaching for Cardiomyopathy Meds as prescribed Low sodium diet Hydration Avoid ETOH, tobacco and stimulants Balace activity and rest Avoid heavy lifting, discuss exercise with health
care provider Stress reduction Report signs/symptoms of heart failure promptly May require IE prophylaxis