chapter 5 bodily dysfunction: eating and sleeping problems and psychophysiological disorders
TRANSCRIPT

Chapter 5
BODILY DYSFUNCTION: EATING AND SLEEPING
PROBLEMS AND PSYCHOPHYSIOLOGICAL
DISORDERS

Psychological, Social and Bodily Interaction
The Psychosomatic Hypothesis Current research focuses on bodily reaction to
emotion-arousing stimuli or stressors. The Biopsychosocial Model
Psychological factors intersect with biological vulnerabilities.
Behavioral medicine and health psychology are concerned with reducing and preventing the stress of illness
Stress and Illness Stress can play a role in illness. Stress-coping skills can decrease stress and risk of
illness.
HEALTH IN THE U.S.
About one-fourth of the adult population are 20 percent or more above desirable weight.
About one-half of adults experience at least a moderate amount of stress in as 2-week period.
Only 28 percent of the population is physically active.
About 30 per cent of persons over 18 years of age smoke cigarettes.
Half of mothers 18 to 24 years of age who are not high school graduates smoked in the year preceding the birth of their last child.
EATING DISORDERS
Anorexia nervosa Obsessed with thinness Great deal of weight loss
Bulimia nervosa Excessive eating followed by purging
Binge eating Excessive eating without purging
ANOREXIA NERVOSA
Prevalence One in 100 girls 16-18 years of age Five to 7 percent of patients die within 10
years of onset Causes
Personality factors Family factors Cultural factors
Treatment Medication Cognitive behavioral therapy Nutritional rehabilitation

BULIMIA NERVOSA
Prevalence Four to 9 percent of high school and college
students Ten to 15 percent of cases are males
Causes Genetic Low self-esteem Personality factors Family factors Negative mood states
Treatment Antidepressant medication Cognitive behavioral therapy
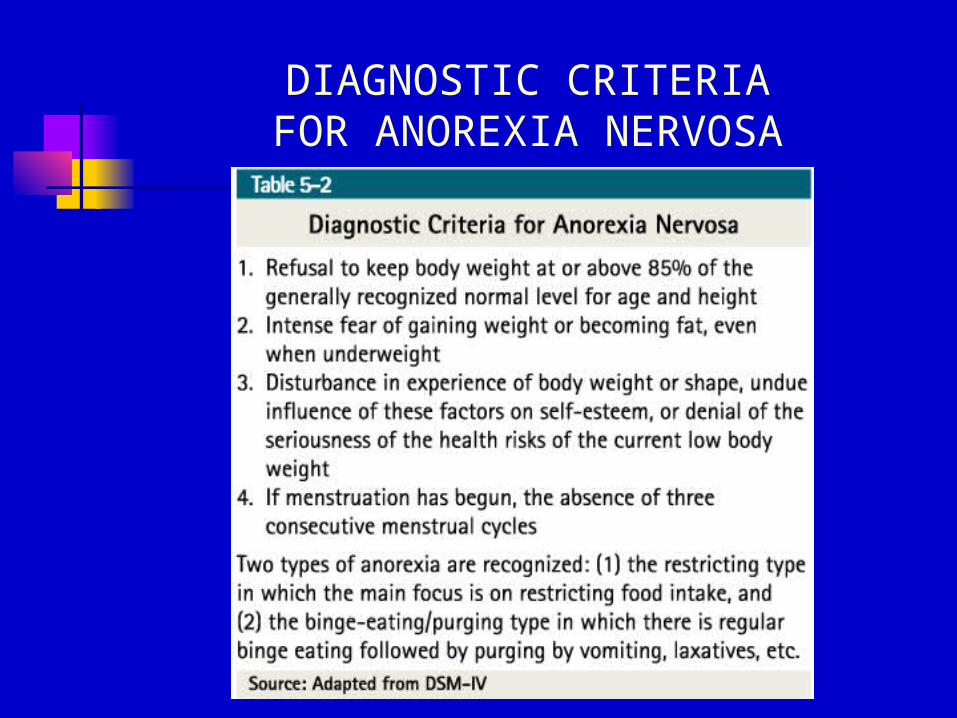
DIAGNOSTIC CRITERIAFOR ANOREXIA NERVOSA
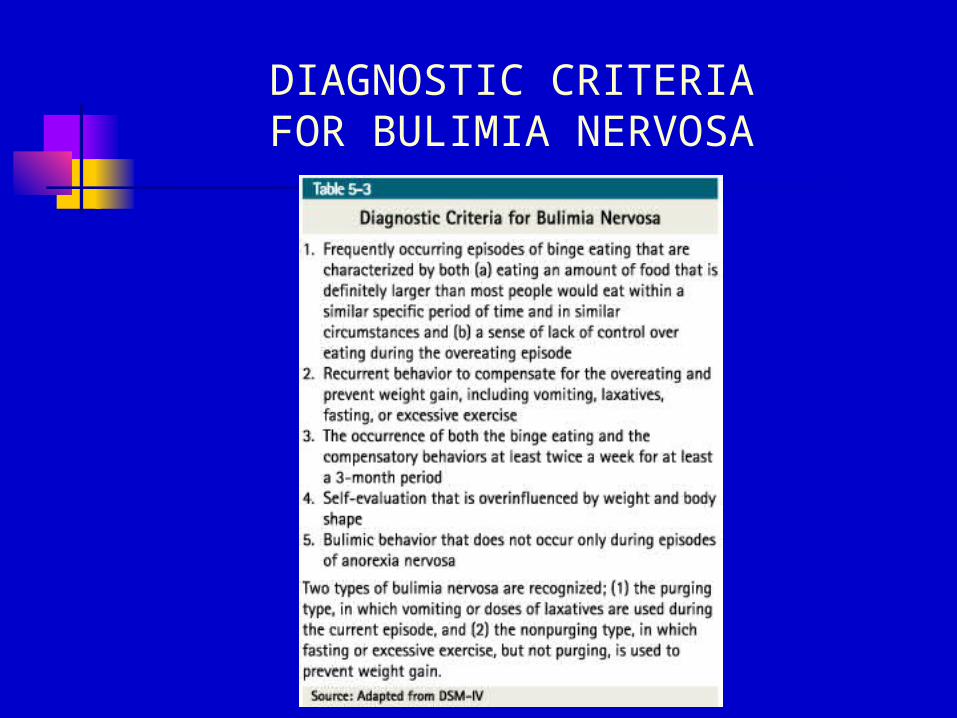
DIAGNOSTIC CRITERIAFOR BULIMIA NERVOSA

COGNITIVE AND BEHAVIORAL FEATURES OF ANOREXIA NERVOSA AND BULIMIA
NERVOSA
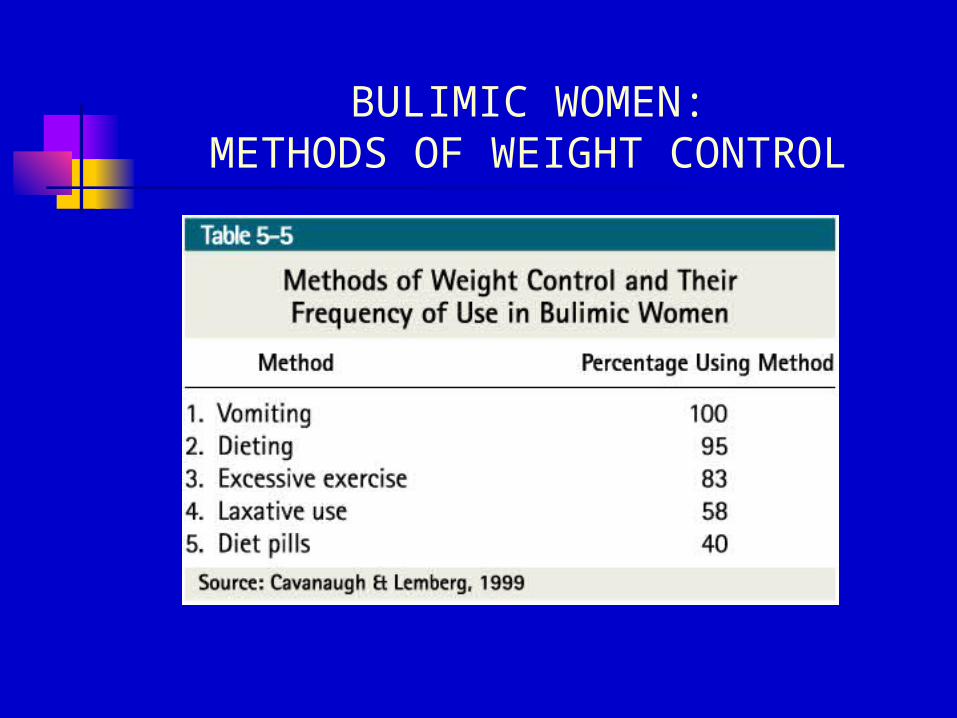
BULIMIC WOMEN:METHODS OF WEIGHT CONTROL
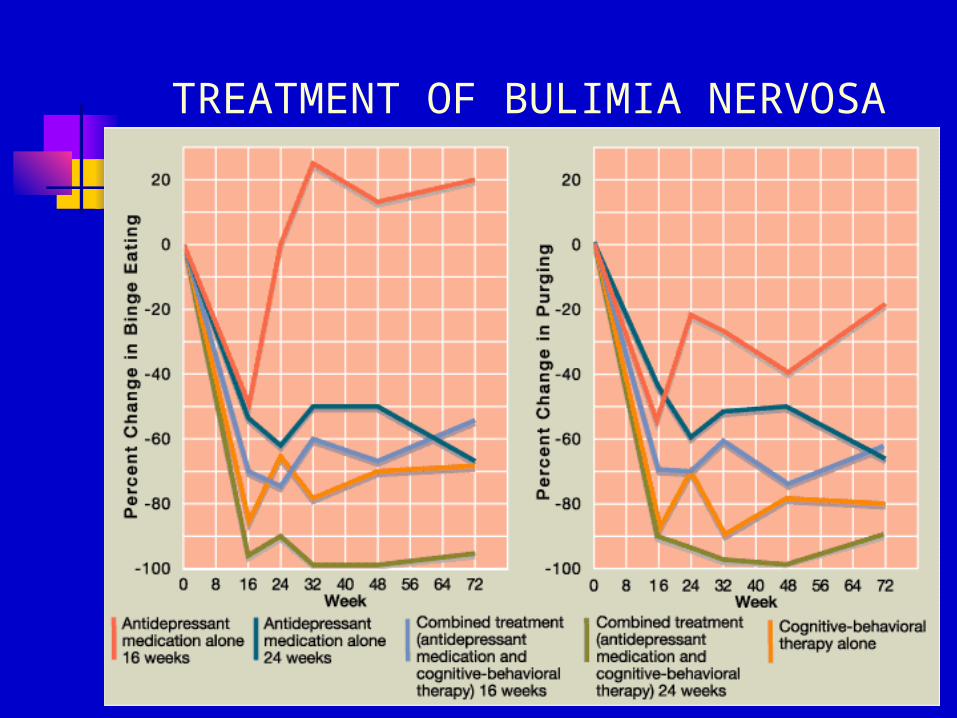
TREATMENT OF BULIMIA NERVOSA
TRIGGERS OF BINGE EATING
Particular stressful situations Particular upsetting thoughts Feeling guilty Feeling socially isolated Worries about responsibilities,
problems, or the future Boredom

SLEEP DISORDERS
Stages of Sleep Stage 1 – Light sleep Stage 2 – Brain waves become slower, eye
movements stop Stage 3 – Delta waves appear Stage 4 – Almost exclusively delta waves Rapid eye movement (REM) sleep
Breathing becomes rapid and irregular Jerky eye movements Blood pressure rises Dream Occurs about every 70 to 90 minutes
during a night’s sleep
SLEEP DISORDERS
Narcolepsy Hypnogogic hallucinations Breathing related sleep disorders
Sleep apnea Primary sleep disorders
Dyssomnias Hypersomnia Insomnia
Parasomnias Nightmare disorder Sleep terror disorder Sleepwalking disorder
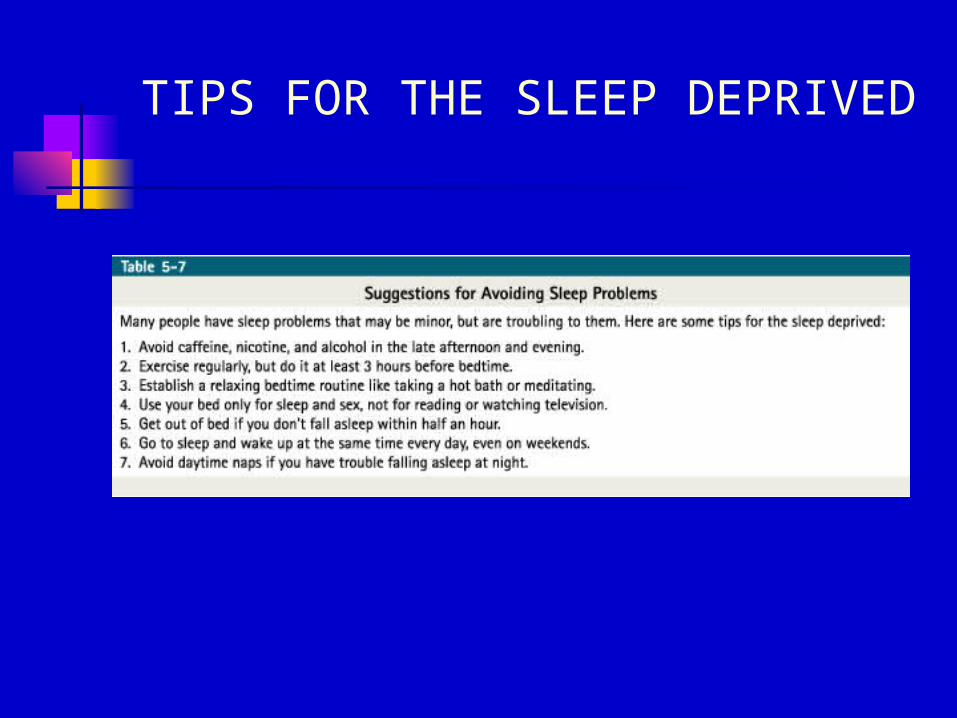
TIPS FOR THE SLEEP DEPRIVED

PSYCHOPHYSIOLGOICAL DISORDERS
Coronary Heart Disease (CHD) Angina pectoris Myocardial infarction
Risk factors for CHD Stress Type A personalities Hypertension
Cancer Chronic Fatigue Syndrome (CFS) Headaches
Tension headaches Migraine headaches Cluster headaches
Irritable Bowel Syndrome

CORONARY HEART DISEASE (CHD) RISK FACTORS
Risk Factors Bodily
Health habitsCommunity life-style
and cultural factors
Personality
Examples Age, hypertension,
cholesterol, obesity, heredity
Smoking, alcohol use Socioeconomic status,
education Anxiety, hostility, life
goals

Coronary Heart Disease (CHD)Among Type A and Type B Men
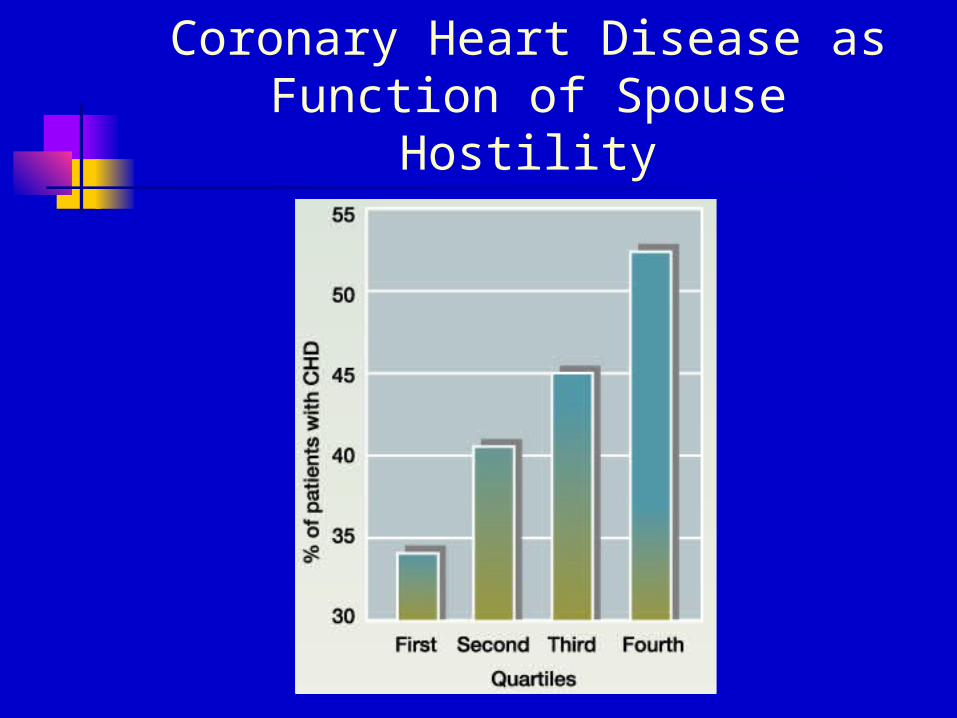
Coronary Heart Disease as Function of Spouse Hostility
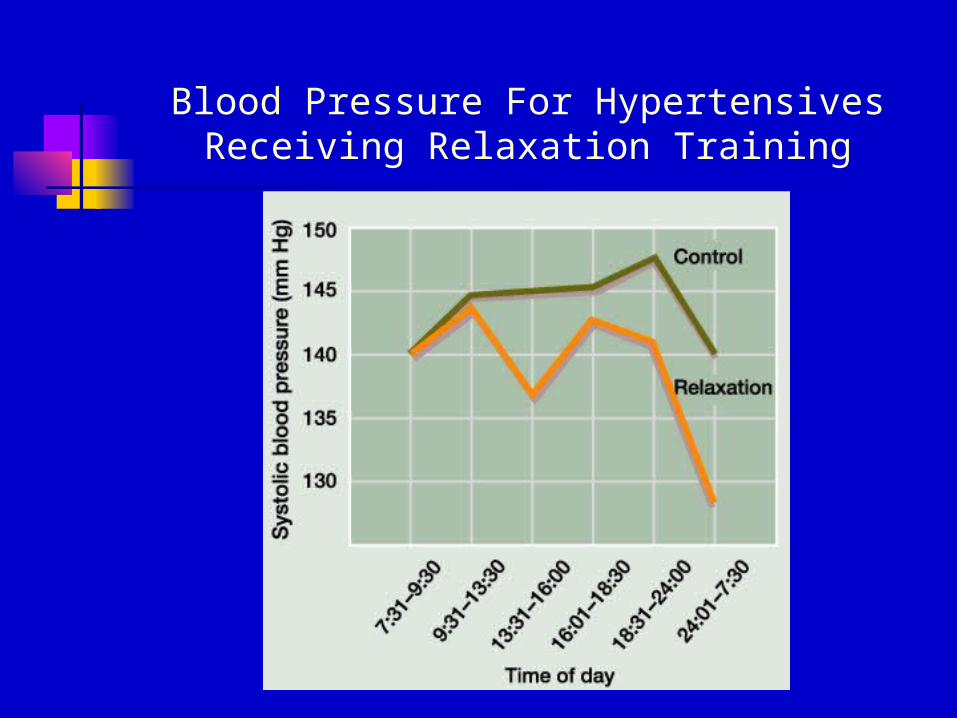
Blood Pressure For Hypertensives Receiving Relaxation Training