chapter 62 –brain attacks overview –brain attack (obj....
TRANSCRIPT
1
Chapter 62 – Brain Attacks Overview – Brain Attack (Obj. 10)
• Brain attack = CVA= CerebroVascular
Accident=Stroke
• Reason for new term
• 3rd leading cause of death in U.S.
• 700,000 peeps have one every year
• 2/3 are new, 1/3 are repeats
• 4,800,000 survivors around
• Estimated direct and indirect cost (2004) was 53
Billion dollars
Risk Factors and Prevention (Obj. 11) Non-Modifiable Risk Factors
1. AGE: 55 and older – incidence doubles
every decade
2. GENDER: Men
3. RACE: African Americans 2X more likely
than Caucasians
Modifiable Risk Factors
• Chart 62-1, p.2210
• Hypertension – major risk factor
• A-Fib
• Hyperlipidemia
• Diabetes
• Smoking
• Carotid Stenosis, valvular heart disease
• Obesity
• ETOH – excessive consumption
• Periodontal Disease
Prevention
• Modify the modifiable risk factors
• Educate the public – risk screenings, etc.
2
Types Of Brain Attacks, Causes,
Manifestations, and Tx (Obj. 12)
Ischemic Brain Attack
• Sudden loss of function resulting from disruption of the blood supply to the brain
• Accounts for 80% of Brain Attacks
• Needs to be treated early to have fewer stroke symptoms, less loss of function, less permanent loss, etc.
• Causes – 1. atherosclerotic plaques in the large blood vessels of the brain result in thrombus formation and occlusion at site, and result in ischemia and infarction
Large Artery Thrombotic Attack
Ischemic Brain Attack – Causes
(cont)
• 2. several small vessels affected, but they
are ones that penetrate deeper into the
brain (small penetrating artery thrombotic
attack)
• 3. heart can throw clots (a-fib, etc.)
• 4. other causes: some are just unknown,
illicit drug use, coagulopathies,
spontaneous dissection of the carotid
artery

3
Small Penetrating Artery
Thrombotic Attack
Pathophysiology
• Disruption of cerebral blood flow because
of an obstruction of a blood vessel
• This starts a series of events known as the
Ischemic Cascade
The Ischemic Cascade1. Blood flow decreases to a point where neurons
are no longer able to maintain aerobic respiration
2. So the mitochondria in the cells switch to anaerobic respirations (less efficient)
3. Anaerobic respirations causes a large amount of lactic acid to be produced
4. A. The large amount of lactic acid causes a change in the pH level (acidosis)
B. Anaerobic respirations cause less ATP to be produced (because it is less efficient system), and depolarization of the cells is inhibited
5. This messes up the cells so much that electrolyte functions begin to fail, and the cells cease to function and die.
Ischemic Cascade and Penumbra
-Penumbra – an area of low cerebral blood flow around the site of the infarction
It is an area of ischemic brain tissue that can be saved with timely intervention
-If the Ischemic Cascade continues, it threatens the area of the penumbra also, causing cell death in that area and enlarging the infarction
-If this happens , it is called “extending the stroke”
PenumbraClinical Manifestations
• Symptoms depend upon the location and size of the affected area
• Numbness or weakness of face, arm, or leg, especially on one side - Hemiplegia, Hemiparesis, Aphagia, Drooping of 1 side of mouth
• Confusion or change in mental status
• Trouble speaking or understanding speech – Dysarthria, Aphasia (expressive vs. receptive)
• Difficulty in walking, dizziness, or loss of balance or coordination, Apraxia
• Sudden, severe headache
• Perceptual disturbances – Hemianopsia, Agnosia
4
LEFT SIDE RIGHT SIDE• Paralysis/weakness on
right side
• Right visual field deficit
• Aphasia
• Altered intellectual ability
• Slow, cautious, behavior
• Paralysis/weakness on
left side
• Left visual field deficit
• Spatial-perceptual deficits
• Increased distractibility
• Impulsive behavior or
poor judgment
• Lack of awareness of
deficits
TIA’s –Transient Ishemic Attack
• Temporary neurological deficit resulting
from a temporary impairment of blood
flow
• “Warning of an impending stroke”
• Diagnostic work-up is required to treat
and prevent irreversible deficit
Medical Management
• ABC’s, stabilizing the pt., and preventing
complications
• Mainly focusing on preventing extending
the attack, and secondary prevention
• t-PA Tx
• Carotid Stents
• Carotid Endarterectomy
• Medications
Medical Mgt. - Medications
• Warfarin (Coumadin) – esp. useful for a-
fib, or cardioembolitic attacks – the target
INR= 2.5
• If warfarin is contradicted –ASA
• Clopidogrel (Plavix)
• Ticlopidine (Ticlid)
• Statins – Zocor, Crestor, Lipitor
• Antihypertensives
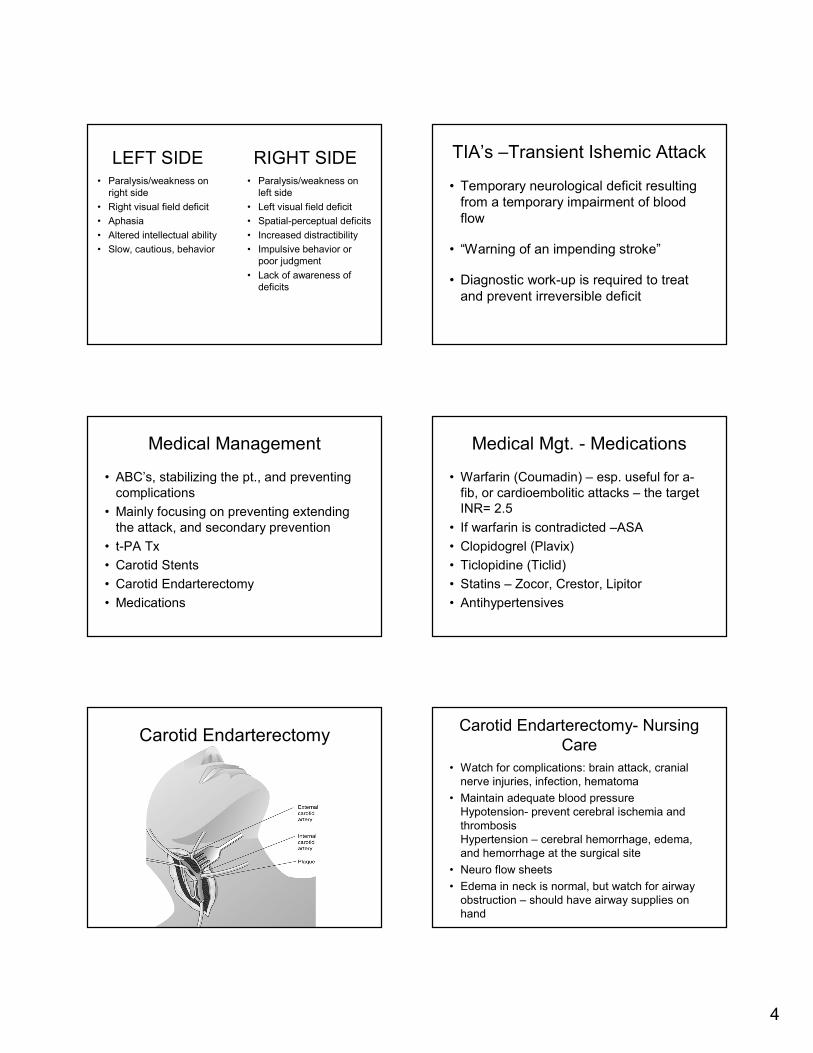
Carotid Endarterectomy Carotid Endarterectomy- Nursing
Care
• Watch for complications: brain attack, cranial
nerve injuries, infection, hematoma
• Maintain adequate blood pressure
Hypotension- prevent cerebral ischemia and
thrombosis
Hypertension – cerebral hemorrhage, edema,
and hemorrhage at the surgical site
• Neuro flow sheets
• Edema in neck is normal, but watch for airway
obstruction – should have airway supplies on
hand

5
Nursing Management – Acute
Phase
• Acute phase
– Ongoing/frequent monitoring of all systems including
vital signs and neurologic assessment: LOC and
motor, speech, and eye symptoms
– Monitor for potential complications including
musculoskeletal problems, swallowing difficulties,
respiratory problems, and signs and symptoms of
increased ICP
Hemorrhagic Brain Attack
• 15-20% of attacks
• Mortality rate up to 43%
• Usually have more severe deficits, and a
longer recovery time
• Caused by bleeding into brain tissue, the
ventricles, or subarachnoid space
Subarachnoid Hemorrhage Hemorrhagic Brain Attack -Causes
• May be due to spontaneous rupture of small
vessels primarily related to hypertension;
subarachnoid hemorrhage due to a ruptured
aneurysm; or intracerebral hemorrhage related
to amyloid angiopathy, arterial venous
malformations (AVMs), intracranial aneurysms,
or medications such as anticoagulants
Pathophysiology
• Brain metabolism is disrupted by exposure to
blood
• ICP increases due to blood in the
subarachnoid space
• Compression or secondary ischemia from
reduced perfusion and vasoconstriction injures
brain tissue and cranial nerves
Intracranial Aneurysm
6
Hemorrhagic Attack -
Manifestations
• Similar to ischemic stroke
• Severe headache
• Early and sudden changes in LOC
• Vomiting
Management – Medical
• Goal – allow the brain to recover, prevent
rebleeding, prevent and Tx complications
• Usually not treated surgically unless
hematoma is at least 3 cm
• Surgical evacuation of hematoma, or
isolate the aneurysm
• Bed rest with sedation
Nursing Management
• Goals may include:
– Improved cerebral tissue perfusion
– Relief of sensory and perceptual deprivation
– Relief of anxiety
– Absence of complications
• Complications – Vasospasms –occurs 4-14 days after the event
• Narrowing of the blood vessels –leads to vascular resistance-impedes blood flow-ischemia and infarction (calcium channel blockers)
Nursing Management -
Complications
• ICP
• Hypertension
• Seizures
• Rebleeding
• Hyponatremia – IV Tx of
• Hydrocephalus (CSF cannot drain) - shunt
Care Of The Patient – Acute Brain
Attack (Obj. 13)
Nursing Care – Acute Phase -
Summary
• Include:
– Improved cerebral tissue perfusion
– ABC’s
– Relief of anxiety
– Elevate HOB
– Monitor V/S and document neurological status
– Absence of complications
– Teaching and preparing for tests and procedures

7
Acute Phase – Procedures (t-
PA)
• Dissolves the blot clot - Works by binding fibrin, and converts plasminogen to plasmin, which stimulates fibrinolysis of the clot
• Must be given within 3 hrs of the onset of the attack
• Revascularization of necrotic tissue (>3 hrs) increases the risk for cerebral edema and hemorrhage
• Leads to a decrease in the size of the attack and an overall improvement in outcome
t- PA Criteria (chart 62-2)
• 3 hr. time window – importance of
education, 911, EMS, and communicating
to E.R., who needs to get the staff
together
• Must be Dx by CT scan
• Other: 18, B/P parameters, no seizure, no
coumadin, labs, Hx, etc.
t-PA (cont)
• Dosage is based on weight -10% is given
as a bolus, other 90% over 1 hr.
• Side effect : Bleeding is the most common,
6.4% have intracranial bleeding
• Nursing: watch IV site for bleeding, no NG
tubes or foleys should be started, neuro
checks
Acute Phase – Complications –
ICP (Obj. 15)• ICP = Increased Intracranial Pressure
• Causes a decrease in cerebral perfusion, stimulates further swelling, and can cause death by shifting brain tissue through openings in dura, or by causing so much loss in cerebral blood flow
• Can occur with ischemic attack, but almost always with a hemorrhagic attack
• Occurs during acute phase, but may also develop in the recovery phase
• Also occurs tumors, head injuries, etc.
Example of a Head Injury ICP
• Your cranial vault contains brain tissue, blood, and CSF
• They exist in state of equilibrium, if one of them increases – ICP
• Brain tissue has limited space to expand-so either CSF or blood has to decrease to compensate, if it does not compensate-ICP
• It is a true medical emergency, can result in death!

8
ICP – Clinical Manifestations -Early
• Early – The earliest sign of increasing ICP is a
change in LOC.
• Other early indicators are slowing of speech,
and delay in verbal response. Pupillary changes
and impaired ocular movements
• Weakness in one extremity or one side
• Headache: constant, increasing in intensity, or
aggravated by movement or straining
ICP- Clinical Manifestations - Late
• Respiratory and vasomotor changes
• VS: increase in systolic blood pressure,
widening of pulse pressure, and slowing of the
heart rate; pulse may fluctuate rapidly from
tachycardia to bradycardia and temperature
increase
– Cushing’s triad: bradycardia, hypertension, and
bradypnea
• Projectile vomiting
ICP – Manifestations (late- cont.)
• Further deterioration of LOC; stupor to coma
• Hemiplegia, decortication, decerebration, or
flaccidity
• Respiratory pattern alterations including
Cheyne-Stokes breathing and arrest
• Loss of brain stem reflexes: pupil, gag,
corneal, and swallowing
Decortication and Decerebration
ICP – Interventions (Obj. 15) ICP - Early Interventions
• Early detection is the best intervention
• Administer diuretics as prescribed
• HOB elevated 30 degrees
• Maintain alignment of the head
• Prevent Valsalva maneuver – teach, stool
softeners, control coughing

9
Long Term Nursing Mgt./Rehab
(Obj. 16)A Few Nursing DX
• Impaired physical mobility
• Acute pain
• Self-care deficits
• Disturbed sensory perception
• Impaired swallowing
• Urinary incontinence
• Disturbed thought processes
• Impaired verbal communication
• Risk for impaired skin integrity
• Interrupted family processes
• Sexual dysfunction
Goals/Outcomes
• Major goals include:
– Improved mobility
– Avoidance of shoulder pain
– Achievement of self-care
– Relief of sensory and
perceptual deprivation
– Prevention of aspiration
– Continence of bowel and
bladder
– Improved thought
processes
– Achievement of a form of
communication
– Maintenance of skin
integrity
– Restoration of family
functioning
– Improved sexual function
– Absence of complications
General Interventions
• Focus on the whole person
• Provide interventions to prevent
complications and to promote
rehabilitation
• Provide support and encouragement
• Listen to the patient
Improving Mobility and Preventing
Joint Deformities
• Turn and position the patient in correct alignment every 2
hours
• Lateral position – pillow between legs BEFORE the
patient is turned. Do not flex the thigh very much –
promotes venous return and prevents edema
• Prone position – 15 to 30 minutes several times a day –
small pillow (folded blanket) under the pelvis (umbilicus
to upper third of thigh) –prevents hyperextension of the
hip joints, drain bronchial secretions, and prevents
contractures of the shoulder and knees
Prone Position to Prevent Hip
Flexion

10
Mobility/Joint Deformities (cont)
• Position hands and fingers – barely flexed
–may have to use a rolled up washcloth or
consult O.T. for device -if
pt. is spastic, do not use a hand roll, as it
stimulates the grasping reflex -
palms facing up, elevate
• Use splints at HS
Improving Mobility (cont.)
• Perform passive or active ROM 4 to 5 times day -Pt. is usually flaccid post attack, but if tightness develops, increase frequency -Repetition forms new pathways in the CNS
• Encourage patient to exercise unaffected side -good leg under the bad leg
• RN positioning, light, eyesight
• Establish regular exercise routine -written –give it pt. (supervise and support) -improvement can only be made thru daily exercise
Mobility (cont.) • Assist patient out of bed as soon as
possible: assess and help patient
achieve balance and move slowly
-gotta be able to sit before you can walk
• Implement ambulation training -chair or wheelchair nearby -lock them brakes , assistive devices
• P.T/O.T.
• Term - apraxia
Shoulder Pain
• 70% of patients – can prevent them from
learning new skills –balance, transfers,
and ADL’s
• Flaccid shoulder should never be used in
lifting, nor pull on affected arm
• If arm is paralyzed after attack -
subluxation occurs by overstretching of
joint capsule, or even by gravity – painful!
Positioning to Prevent Shoulder
Adduction
Shoulder Pain (cont)
• Shoulder-hand syndrome – painful shoulder and generalized swelling of the hand, can cause a frozen shoulder – pain and atrophy of subcutaneous tissue –Elevate hand
• Proper positioning- important -sitting – place arm on table/pillow -ambulation – sling -ROM exercises
• OK to give pain meds!

11
Self Care
• Enhance self-care
– Set realistic goals with the patient
– Encourage personal hygiene
– Ensure that patient does not neglect the affected side
– Use assistive devices and modification of clothing
– Be aware that not all pt.’s are going to get there
Sensory – Perceptual
Difficulties• Approach pt. on side with good vision
• Clock, glasses, dentures, TV, calendar, etc. should be placed on “good” side
• Teach and encourage pt. to turn head in direction of affected side to compensate
• After pt. knows you are there, then you can stand on other side to encourage pt. to turn head
• If hemianopsia – pt. tends to forget about and neglect that side- encourage and remind pt. about other side of body, maintain alignment, if possible, place extremities where pt. can see them
Intake and Output
• Nutrition
– Consult with speech therapist or nutritionist
– Have patient sit upright to eat, preferably OOB
– Use chin tuck or swallowing method
– Feed thickened liquids, pureed diet , other
• Bowel and bladder control
– Assess and schedule voiding
– Implement measures to prevent constipation: fiber,
fluid, and toileting schedule
– Provide bowel and bladder retraining
Improving Thought Process
• May be temporary
• Support and encourage
• Speech Tx, Recreation Tx
• Reality orientation
• Term - agnosia
Improving Communication
• Aphasia – more common for Left Side attacks. Not uncommon for peeps who have R-sided paralysis, to also have aphasia (Broca’s area is very close to the left motor area of the brain)
• Speech Tx
• Patient – depressed, angry, frustrated
• Provide support and understanding
• Do not finish sentences for pt.
• Use a communication board
• Get their attention, speak slowly, one instruction at a time, use gestures, talk to pt. during ADL’s
Skin Integrity
• Pressure ulcer prevention

12
Family Coping
• Encourage participation in counseling
• Encourage to use support systems
• Keep them informed -
about outcomes -
about certain conditions (emotional lability)
, may improve with time
• Keep them from preventing loved one’s
independence
• They are a part of the patient’s Tx
Sex
• Medical reasons
• Medicines
• Depression, lower self esteem
• Encourage dialog
• Provide literature and referrals
Home and Community – Based
Care
• Nutrition: diet, swallowing
techniques, and tube
feeding administration
• Elimination: bowel and
bladder programs and
catheter use
• Exercise and activities:recreation and diversion
• Socialization, support
groups, and community
resources
• Prevention of subsequent strokes, health promotion, and implementation of follow-up care
• Prevention of and signs and symptoms of complications
• Medication teaching
• Safety measures
• Adaptive strategies and use of assistive devices for ADLs