chapter- iii - shodhgangashodhganga.inflibnet.ac.in/bitstream/10603/5373/6/06_chapter 3.pdf ·...
TRANSCRIPT
69
CHAPTER- III
AVAILABILITY OF HEALTHCARE SERVICES WITH SPECIAL REFERENCE TO REPRODUCTIVE HEALTH IN MIZORAM
3.1. Introductory Statement
No issue is more central to global well-being than reproductive health. Every
individual, every family and every community at some point is intimately involved with
pregnancy and the success of child birth. Yet every day a large number of mothers are
suffering from pregnancy as well as postpartum complications. In order to mitigate
reproductive health problems and complications, improving healthcare facilities and
availability of services- both physical and social- are imperative. It is important to
understand that maternal and new born services as a key component of the overall
healthcare system will enhance effort to achieve greater integration of services and long-
term financial sustainability in the country.
It was observed that in Mizoram major chunk of reproductive health problems
occurred due to poor service provision, as well as due to lack of access to and use of
these services. Although effective interventions of government to prevent morbidity and
mortality are known, for many women and new born, appropriate care remains partially
available, unused, inaccessible or of poor quality. In Mizoram reproductive healthcare is
often combined with other services such as immunization, malaria and other health
problems.
Healthcare covers a broad spectrum of personal health services ranging from
health education and information through prevention of disease, early diagnosis and
treatment and rehabilitation. The term health services imply organisation, delivery,
staffing, regulatory and quality control (Thangdailova, 2003). Reproductive health
services comprise a range of women’s health interventions, often provided under the
fabric of maternal and child healthcare which, itself, can be substantially integrated into
primary healthcare. These interventions include family planning information, education
and communication; contraceptive counselling and provision of contraceptives; basic
70
screening of sexually transmitted infections; prenatal or newborn care; and breastfeeding
support (Guttamacher Institute, 2005). Dispensaries and Primary Health Centres in
Mizoram started as early as in 1890s when the British came to Mizoram and over the last
two centuries it has undergone several changes to meet the increasing demand for
healthcare services. After attaining statehood the emphasis was on the expansion of the
healthcare establishment. However, it was realised that mere expansion of healthcare
services across the state did not provide adequate facility. It required also sound
geographical distribution of healthcare facilities, ideal location and population coverage
of health centre and quality rather than quantity especially on reproductive healthcare
services. This chapter evaluates availability of healthcare services pertaining to
reproductive healthcare in Mizoram. It highlights the growth and developments of formal
healthcare facilities as well as maternity services in the state and types of healthcare
facilities available from to Sub-centre to hospital level.
3.2. Healthcare under Christian Missionaries
A brief reflection of growth of formal healthcare facilities is imperative to
understand the pace of growth as well as spatial coverage of health centres. There were
two pioneering agencies that started and carried on the charity services for providing
healthcare among the Mizos; one under the Christian missionaries and another under the
government. Both these agencies had been working side by side. The contributions of
early Christian missionaries were commendable for the growth and development of
modern healthcare system in Mizoram. The pioneer missionaries, who first settled
Mizoram, J.H.Lorraine and F.W Savidge during their time (1894-1897) had distributed
medicines as evidence by common saying of those days which goes like, “I went to where
the missionaries’ live, good medicines are what they give”. The missionaries visited
interior places of Mizoram and explored the horrible conditions of the people’s health,
which can be expressed in the statement of a missionary: “Malaria was of course
prevalent everywhere. There was also dropsy, internal parasites, hookworm, dysentery,
tuberculosis and other dread diseases. Parents had large families but more than 50
71
percent of the children died before reaching adolescence. Many mothers died at
childbirth due to lack of care and superstitious diseases” i
Two Christian missionaries-Rev. D.E Jones and Rev. E Rowland, immediately
after their arrival ventured to acquaint the Mizos with modern medicines. But as their
knowledge of medicines was limited, they simply helped in curing simple diseases. The
steps taken by Rev. D.E. Jones and Rev. E Rowland were, however, the first in this kind
of Mizos’ acquaintance with the medicines and use of medicines for cure of diseases. The
Mizos never knew what medicine was and its use before this (J.M Lloyd, 1991).
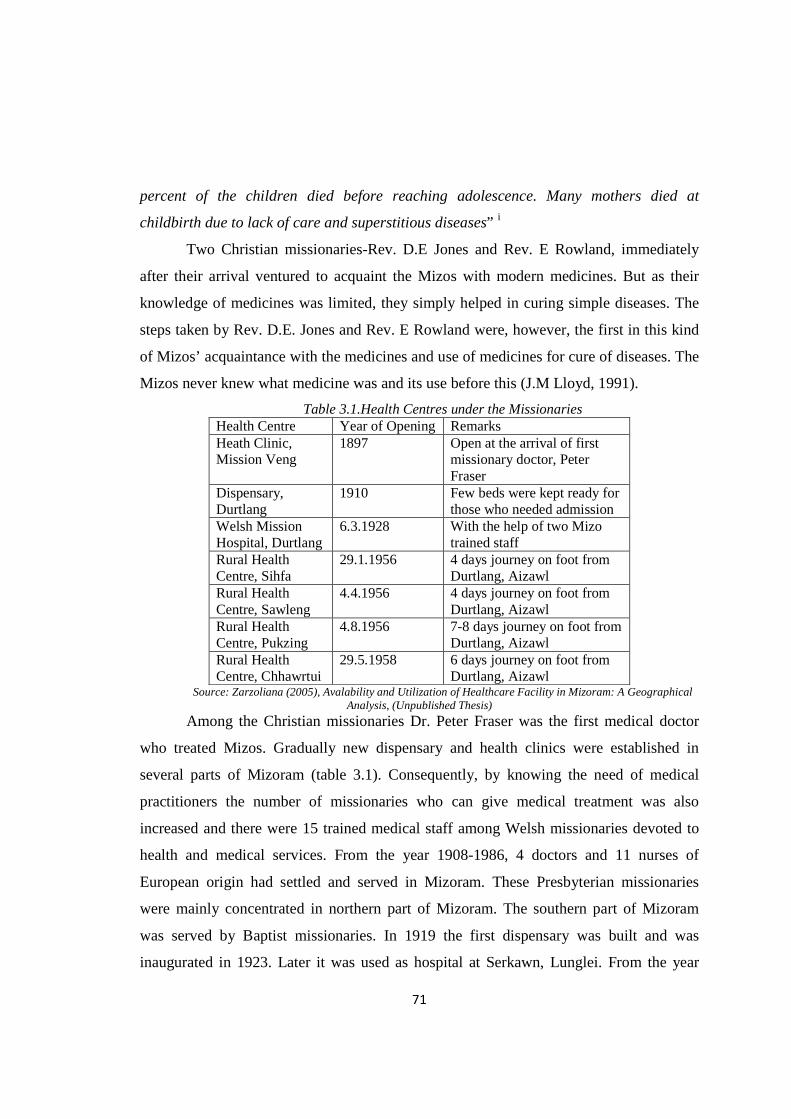
Table 3.1.Health Centres under the Missionaries Health Centre Year of Opening Remarks Heath Clinic, Mission Veng
1897 Open at the arrival of first missionary doctor, Peter Fraser
Dispensary, Durtlang
1910 Few beds were kept ready for those who needed admission
Welsh Mission Hospital, Durtlang
6.3.1928 With the help of two Mizo trained staff
Rural Health Centre, Sihfa
29.1.1956 4 days journey on foot from Durtlang, Aizawl
Rural Health Centre, Sawleng
4.4.1956 4 days journey on foot from Durtlang, Aizawl
Rural Health Centre, Pukzing
4.8.1956 7-8 days journey on foot from Durtlang, Aizawl
Rural Health Centre, Chhawrtui
29.5.1958 6 days journey on foot from Durtlang, Aizawl
Source: Zarzoliana (2005), Avalability and Utilization of Healthcare Facility in Mizoram: A Geographical Analysis, (Unpublished Thesis)
Among the Christian missionaries Dr. Peter Fraser was the first medical doctor
who treated Mizos. Gradually new dispensary and health clinics were established in
several parts of Mizoram (table 3.1). Consequently, by knowing the need of medical
practitioners the number of missionaries who can give medical treatment was also
increased and there were 15 trained medical staff among Welsh missionaries devoted to
health and medical services. From the year 1908-1986, 4 doctors and 11 nurses of
European origin had settled and served in Mizoram. These Presbyterian missionaries
were mainly concentrated in northern part of Mizoram. The southern part of Mizoram
was served by Baptist missionaries. In 1919 the first dispensary was built and was
inaugurated in 1923. Later it was used as hospital at Serkawn, Lunglei. From the year
72
1919-1977 there were 9 nurses and one doctor of European origin who settled and served
in Mizoram under the Baptist Mission Society (BMS). Nursing training school was
started at Serkawn in 1952 with a coursed in Auxiliary Nursing and Midwifery. These
institutions continue to play important role in providing training and healthcare to many
people.
3.2.1. Reproductive Healthcare under Christian Missionary
It is critical that formal healthcare system and reproductive healthcare are
inseparably intertwined. However, maternal healthcare requires special treatment for its
importance in ensuring better health management of the mother and the child. By Mizo
tradition, pregnancy related complications were in no sense an ailment that needed
special care. Pregnant mothers having problems are considered normal and they are not
expected to rest or to be free from usual work. The mothers, especially those expecting
their first child, are young and active and cannot be excused. As a result, a young mother
might give birth to her baby on the side of the path or on the rice-field itself. In olden
days only half the number of such babies was born alive. Early Christian Missionaries
took note of this and made strenuous efforts in bringing awareness for special maternal
care among the Mizos.
During those days the Lushai (Mizo) practiced a sort of infanticide, if a woman
died soon after giving birth. The little one used to be smothered and buried along with his
mother. Mrs. Savidge and Mrs. Lorrain (wives of the first Christian missionaries) took
steps to stop this practice by taking care of the motherless babies. In 1914 they wrote to
the headquarters of Baptist Missionary Society (BMS) in the following words: “We hope
that the committee at home are keeping in mind the earnest appeal of our Indian
Secretary in 1913 for a fully qualified missionary-nurse to work among the women and
young children of South Lushai” (Annual Report of BMS, 1901-1938)
Since 1926, motherly missionary had taken an increasing interest in the Welfare
Clinic, which had been started and Katie Hughes taught the rudiment of child care once a
week in Dr. Fraser’s old building (dismantled in 1930). For the local mother it provided
an hour’s relaxation and a chance to discuss their areas of interest. This became a popular
73
event and in Mizo they christened the little room as ‘Nau Buk In’ (the House for
Weighing Babies). No doubt some competitive spirit and modest excitement was
engendered by comparing each baby’s weight week by week and the prejudice against
washing babies gradually died away (Lloyd, 1991). Women Evangelist or Bible women,
an organization introduced primarily to spread Christianity among the Mizo women
started during this time and side-by-side, it guided the womenfolk in cleanliness. The
organizers threw light on sanitation, maternity care and the like. Child welfare
Organization was established by the Presbyterian Mission at Aizawl, which aimed to give
instructions to mothers on child care and rudiments of sanitation. In southern part of the
state, the Baptist Mission opened one orphanage, which not only looked after the
motherless but also trained a number of Mizo mothers (Zarzoliana, 2005). Besides,
Mother’s School was also opened once a week for the women living on the compound of
Serkawn hospital during 1922 to spread Christianity, education and healthcare among the
women. Significantly, the Christian missionaries regularly conducted Baby Shows in
order to encourage womenfolk to keep the baby healthy. In 1932, Miss Oliver reported
that “Our Baby Show in October was quite a success; there were 50 babies, many of them
clean, healthy and well developed in this direction, though, of course, there is plenty yet
to be done” (The Annual Report of BMS, 1901-1938).
The Missionaries thus made a commendable effort in providing a sound
foundation to maternal and child care in Mizo Hills which had its impacts in years to
follow.
3.3. Healthcare Facility under the Government
Growth and development of modern healthcare system under government cannot
be underestimated though the contributions of early Christian missionaries were
commendable on this regard. During that period Mizoram was under the state of Assam
and in 1952 it attained the status of a District Council and in 1972 it got the status of a
Union Territory. In 1986 Mizoram attained the status of statehood. Growth of healthcare
74
during these periods was quite slow. This section briefly highlights the growth and
development of healthcare facilities under the government initiative.
3.3.1. Healthcare Facility before Independence
In 1894, a tent was erected at Aizawl to provide healthcare to labourers which
was converted to a dispensary in 1896 with some emergency beds (Thangdailova, 2003).
Subsequently, in 1896 Aizawl hospital was made functional with 20 beds. Only in 1920,
another nominal hospital was established in Lunglei (Table 3.2). Even though dispensary
was started way back in 1896, the rate of growth was slow. In 1920 there were 7
dispensaries that were established in various parts of the state such as Champhai, Kolasib,
Sairang, N.Vanlaiphai, Sialsuk, Tlabung and Tuipang with 5-6 emergency beds each.
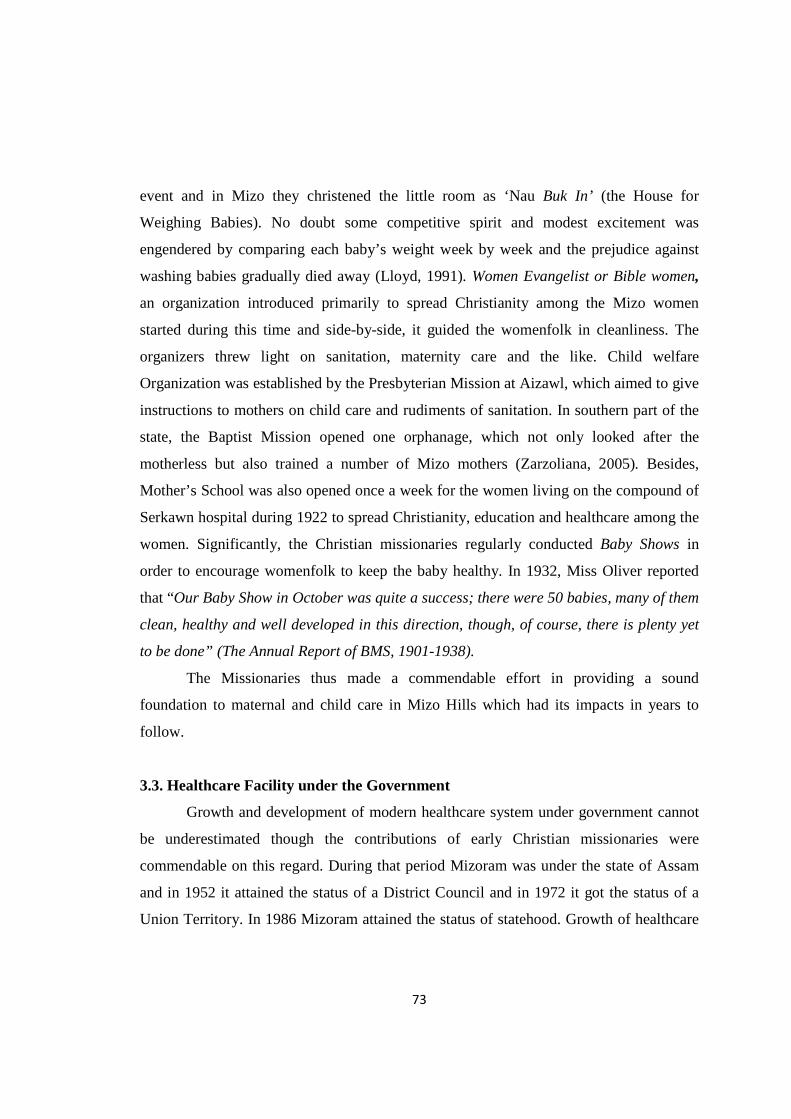
Table 3.2.Mizoram: Growth of Healthcare Facilities under Government Events Year Hospital Dispensary **PHC/CHC Sub-centre Pre-Independence
1896 1 1 - - 1920 2 7 - -
Post- Independence up to Union Territory
1947 2 7 - - 1966 3 21 3 - 1972 3 55 4 -
Under statehood till date
1986 7 - 51 314 2001 7 - 64 336 2010 8 - 64 336
2010* 20 - 64 366 *Include 11 non-government hospitals; ** PHC=Primary Health Centre, CHC=Community Health Centre
Source: Zarzoliana (2005) Availability and Utilization of Healthcare Facility in Mizoram: A Geographical Analysis. (Unpublished Thesis) & Primary Survey, 2010
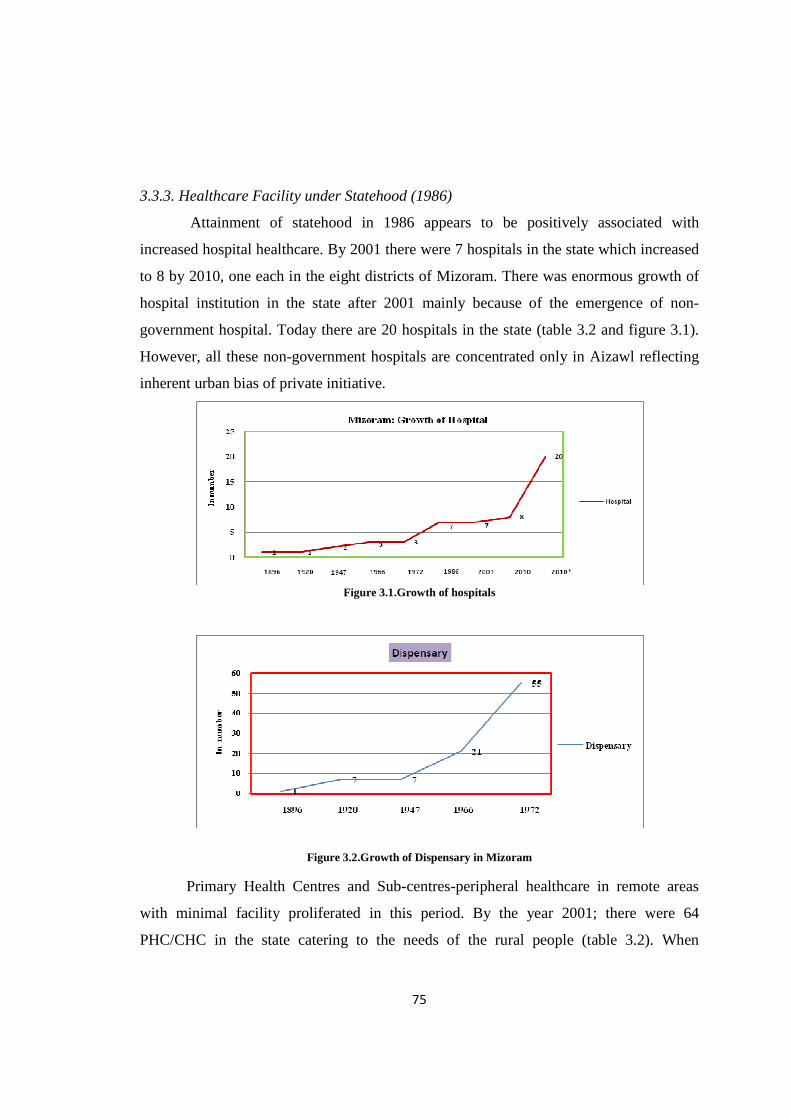
3.3.2. Healthcare Facility between Independence and Union Territory (1947-1972)
Even after Independence there was not much progress pertaining to healthcare
facilities and only after a gap of 46 years from the establishment of first hospital, another
hospital was set up at the time when insurgency broke out in Mizoram in 1966. Even
though growth of hospitals was abnormally slow, there was substantial growth of
dispensaries which increased from 7 in 1947 to 21 in 1966 and increased to 55 when
Mizoram attained the status of a Union territory in 1972. During this period, Primary
Health Centres (PHC) were started to provide healthcare in less urbanised and/or rural
areas. By 1966, there were 3 PHCs in Mizoram and the number increased to 4 in 1972.
75
3.3.3. Healthcare Facility under Statehood (1986)
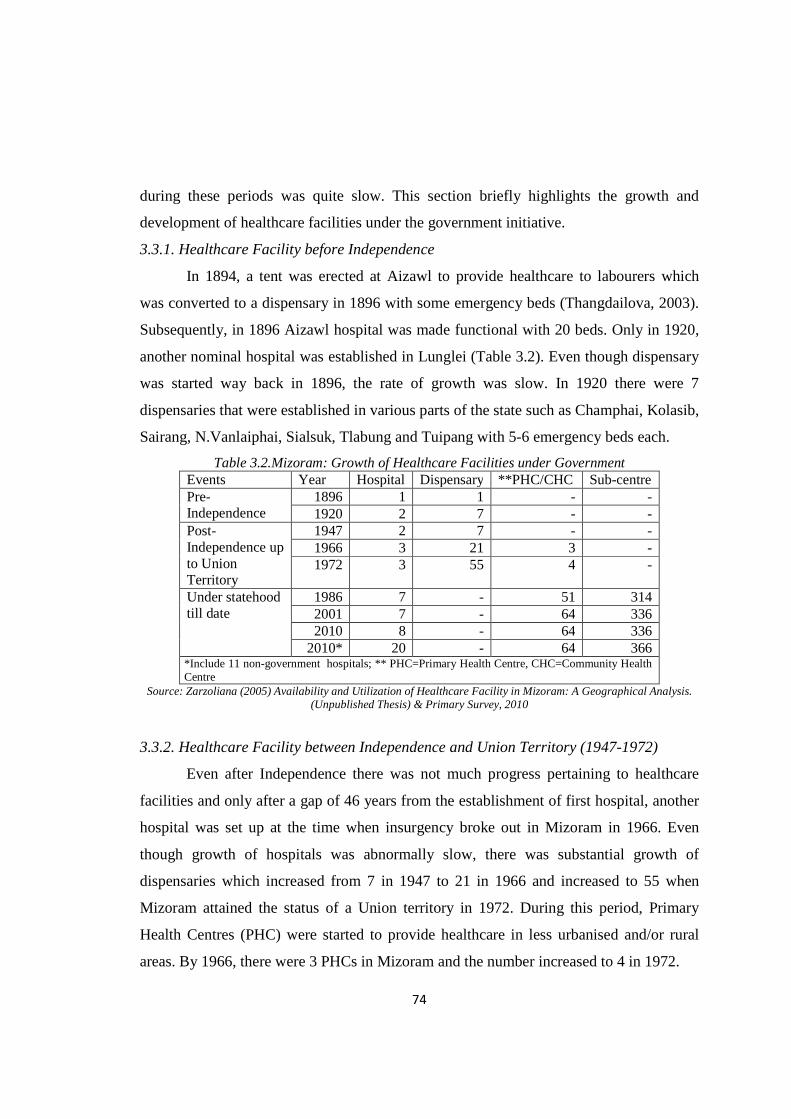
Attainment of statehood in 1986 appears to be positively associated with
increased hospital healthcare. By 2001 there were 7 hospitals in the state which increased
to 8 by 2010, one each in the eight districts of Mizoram. There was enormous growth of
hospital institution in the state after 2001 mainly because of the emergence of non-
government hospital. Today there are 20 hospitals in the state (table 3.2 and figure 3.1).
However, all these non-government hospitals are concentrated only in Aizawl reflecting
inherent urban bias of private initiative.
Figure 3.1.Growth of hospitals
Figure 3.2.Growth of Dispensary in Mizoram
Primary Health Centres and Sub-centres-peripheral healthcare in remote areas
with minimal facility proliferated in this period. By the year 2001; there were 64
PHC/CHC in the state catering to the needs of the rural people (table 3.2). When

76
Mizoram got the status of statehood there were as many as 314 Sub-centres spread in
rural areas and the number increased to 366 in 2001.
It is clear that the efforts of Christian missionaries in providing a foundation to
good healthcare in the pre-independence phase had its echo on the Government policies
which made strenuous efforts to provide healthcare to people even in remote areas. It is
also evident that attainment of statehood in 1986 provided the much needed incentive to
the state government to push forward healthcare facility at a pace unprecedented in the
history of the state. The policy changes were obvious. Earlier emphasis on Dispensaries
disappeared to give rise to the concept of Primary and Community health centres
providing access to people living in remote rural areas to modern healthcare system. Sub-
centres filled the gap in this process of access to modern healthcare system in most
difficult areas unserved by PHCs. Ironically however; there emerged disparities of
various kinds with growth of healthcare facilities. Better and efficient forms of healthcare
got concentrated in the urban as well as more developed areas while the rural and
difficult locations were served by Sub-centres or primary health centres with minimal
healthcare facility.
3.4. Spatial Variation in Healthcare Facility: Inter-District Variation
Health System at the district level is fundamental in implementing various health
policies and delivery of healthcare, management of health services for defined geographic
areas. Every district is expected to have a district hospital linked with the public
hospitals/health centres such as Sub-district/Sub-divisional hospitals, Community Health
Centres, Primary Health Centers and Sub-centres. The district hospitals cater to the
people living in urban (district headquarters town and adjoining areas) and the rural
people in the district.
3.4.1. Availability
Spatial distribution of healthcare facilities plays an important role in serving the
population of a region. According to 2001 census, Mizoram comprised eight districts. In
term of geographical area, Lunglei district is the largest, followed by Aizawl and
77
Champhai districts while Kolasib is the smallest district. With respect to population size,
Aizawl district is the most populous district (325676) with 36.65 percent of the state’s
population concentrated in the district followed by Lunglei district (137223) with 15.44
percent of the state’s population and Champhai district (108392) supporting 12.19
percent population. The population in other districts ranges from as low as 53861 in
Serchhip district to 73620 in Lawngtlai district.
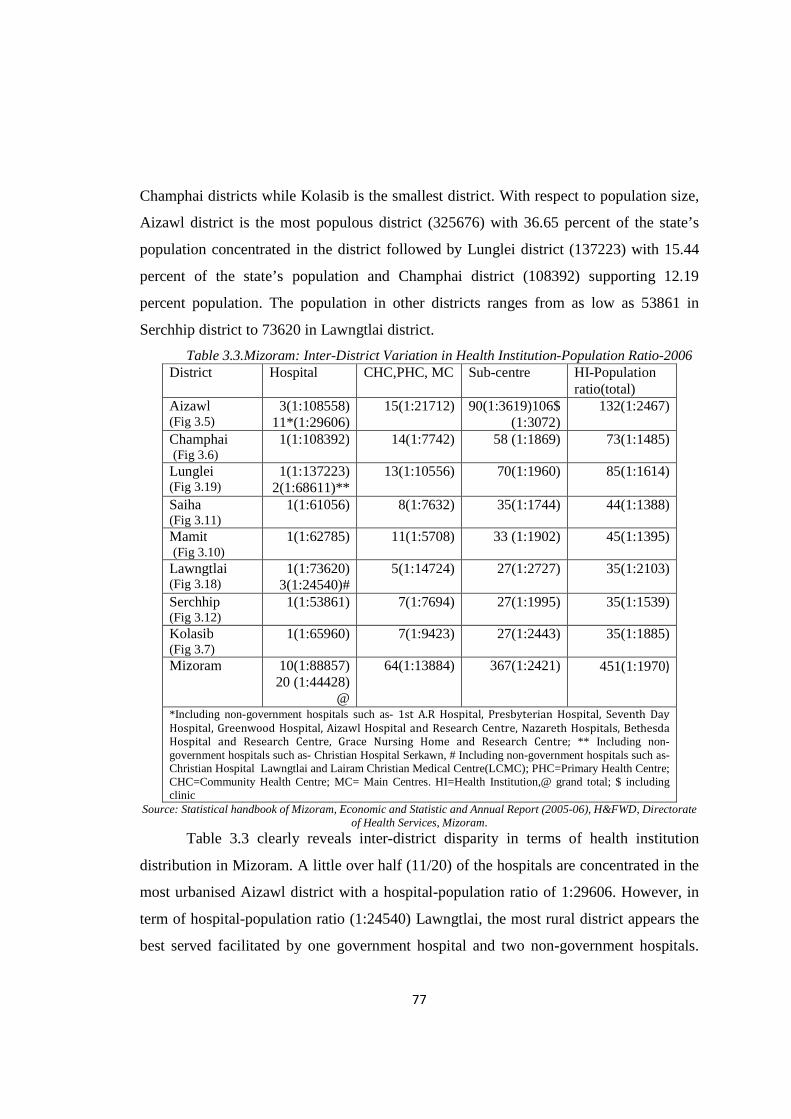
Table 3.3.Mizoram: Inter-District Variation in Health Institution-Population Ratio-2006 District Hospital CHC,PHC, MC Sub-centre HI-Population
ratio(total) Aizawl (Fig 3.5)
3(1:108558) 11*(1:29606)
15(1:21712) 90(1:3619)106$ (1:3072)
132(1:2467)
Champhai (Fig 3.6)
1(1:108392) 14(1:7742) 58 (1:1869) 73(1:1485)
Lunglei (Fig 3.19)
1(1:137223) 2(1:68611)**
13(1:10556) 70(1:1960) 85(1:1614)
Saiha (Fig 3.11)
1(1:61056) 8(1:7632) 35(1:1744) 44(1:1388)
Mamit (Fig 3.10)
1(1:62785) 11(1:5708) 33 (1:1902) 45(1:1395)
Lawngtlai (Fig 3.18)
1(1:73620) 3(1:24540)#
5(1:14724) 27(1:2727) 35(1:2103)
Serchhip (Fig 3.12)
1(1:53861) 7(1:7694) 27(1:1995) 35(1:1539)
Kolasib (Fig 3.7)
1(1:65960) 7(1:9423) 27(1:2443) 35(1:1885)
Mizoram 10(1:88857) 20 (1:44428)
@
64(1:13884) 367(1:2421) 451(1:1970)
*Including non-government hospitals such as- 1st A.R Hospital, Presbyterian Hospital, Seventh Day
Hospital, Greenwood Hospital, Aizawl Hospital and Research Centre, Nazareth Hospitals, Bethesda
Hospital and Research Centre, Grace Nursing Home and Research Centre; ** Including non-government hospitals such as- Christian Hospital Serkawn, # Including non-government hospitals such as- Christian Hospital Lawngtlai and Lairam Christian Medical Centre(LCMC); PHC=Primary Health Centre; CHC=Community Health Centre; MC= Main Centres. HI=Health Institution,@ grand total; $ including clinic
Source: Statistical handbook of Mizoram, Economic and Statistic and Annual Report (2005-06), H&FWD, Directorate of Health Services, Mizoram.
Table 3.3 clearly reveals inter-district disparity in terms of health institution
distribution in Mizoram. A little over half (11/20) of the hospitals are concentrated in the
most urbanised Aizawl district with a hospital-population ratio of 1:29606. However, in
term of hospital-population ratio (1:24540) Lawngtlai, the most rural district appears the
best served facilitated by one government hospital and two non-government hospitals.
78
Champhai district is the least served with a ratio of 108392 people dependent on only one
hospital. This unequal distribution of hospital facility is a serious matter as far as
maternity care is concerned. Generally maternity cares are available in the tertiary and
secondary level healthcare system like hospitals compared with lower level of health
institutions. Aizawl, Lunglei and Lawngtlai are the only districts have the advantage of
both government as well as non-government hospitals. If one considers only government
hospitals in the districts Serchhip is the best served while Aizawl is the least served. This
is mainly due to unequal distribution of population distribution in the state. Only 6
percent of the population is concentrated in Serchhip district.
In the state as a whole one hospital is available to 44428 people. Going by this
average hospital-population ratio, only the most urbanised district of Aizawl (1:29606)
and the most rural district of Lawngtlai (1:24540) are the best served districts. In the
remaining districts the ratio is much higher than the state average. Aizawl district has
eight hospitals under private sector which provide maternal healthcare facility along with
general healthcare. Lunglei district was also having one church run hospital in Serkawn,
besides a public hospital. More than half (20/11) of all hospitals are concentrated in
Aizawl district that too in Aizawl city alone which distinguished Aizawl from the
remaining districts as far as hospital facility is concerned.
The main function of Main Centre (MC) is to receive information and report from
Sub-centre under one health supervisor and above it is the Primary Health Centre (PHC)
equipped with 10 beds and again above it is the Community Health Centre (CHC) with
30 beds, which are finally linked with the district hospital. PHCs and CHCs are expected
to provide various services in the area of maternal and child healthcare and family
planning. These three healthcare systems are treated together in the present analysis
though their functions and available facilities are different.
As shown in table 3.3, there were 64 of MC/PHC/CHC in Mizoram. As far as
MC/PHC/CHC-population ratio is concerned Mizoram can be divided into two broad
regions i.e better served districts and poorly served districts. Districts such as Mamit
(1:5708), Serchhip (1:7694), Champhai (1:7742), Serchhip, Kolasib (1:9423) and Saiha
79
(1:7632) fall under the category of better served districts. The remaining three districts
such as Aizawl (1:21712), Lawngtlai (1:14724) and Lunglei (1:10556) fall under the
category of poorly served districts.
However, there is glaring intra-district disparities in Mizoram with regard to the
distribution of PHCs. Sub-centres (SCs) are the most peripheral health institutions
catering to the healthcare needs of the rural population. It is the critical contact point
between the Primary Healthcare system and the community. It is manned by one
multipurpose male and a female worker. Sub-centres provide preventive care like
immunization and vaccination etc. Even though the Sub-centre wise population norm at
the national level has been met by Mizoram, it was unevenly distributed across Mizoram.
In terms of Sub-centre-population ratio, the most urbanized district of Aizawl and the
least urbanised district of Lawngtlai shared common weaknesses being the least served
districts with ratios of 1:3072 and 1:2727 respectively. In the remaining districts the ratio
varied between 1: 1744 in Saiha and 1:1995 in Serchhip district.
It is ironical that Aizawl district with a large concentration of health institutions
appears to be the worst served when health institution-population ratio is taken into
consideration. Nearly one-third (132/451) of all health institutions are concentrated in the
district. However, poor institution population ratio in the district is largely due to
excessive population concentration in the district. Moreover, the district has more tertiary
health institutions which are large enough but their numbers are less. Thus the low
institution population ratio does not necessarily reflect poor health infrastructure in the
district. But the same cannot be said about Lawngtlai district.
3.4.2. Doctor–Population Ratio
Mere availability of health institutions may not guarantee quality of healthcare.
Availability of beds and doctors is extremely important.
Out of a total of 311 doctors serving in the state, 209 (67.20 percent) are
concentrated only in hospitals located in Aizawl district and 35(11.25 percent) in
hospitals located in Lunglei district. On the other hand only 7(2.25 percent) and 8 (2.27
percent) doctors are available in Mamit and Lawngtlai hospitals respectively. In the
80
remaining districts the number of available doctors varies from 11(3.54 percent) in
Champhai and Serchhip to 14 (4.50 percent) doctors in Saiha district.
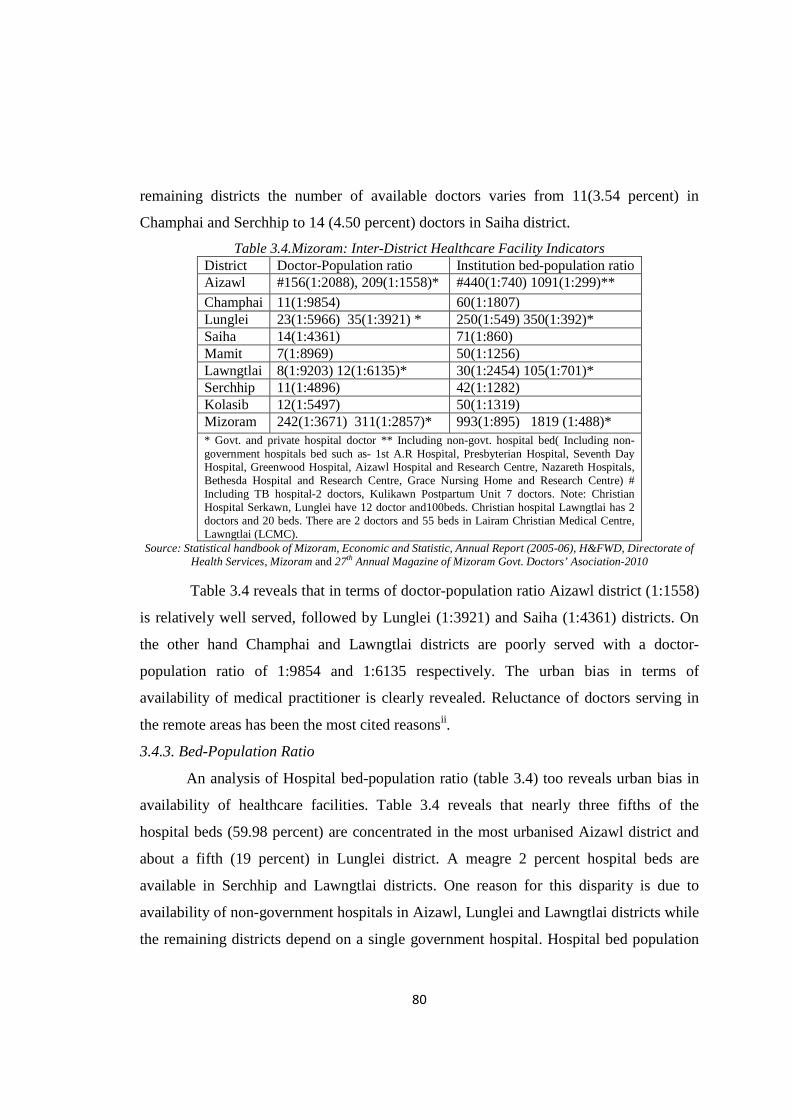
Table 3.4.Mizoram: Inter-District Healthcare Facility Indicators District Doctor-Population ratio Institution bed-population ratio Aizawl #156(1:2088), 209(1:1558)* #440(1:740) 1091(1:299)**
Champhai 11(1:9854) 60(1:1807) Lunglei 23(1:5966) 35(1:3921) * 250(1:549) 350(1:392)* Saiha 14(1:4361) 71(1:860) Mamit 7(1:8969) 50(1:1256) Lawngtlai 8(1:9203) 12(1:6135)* 30(1:2454) 105(1:701)* Serchhip 11(1:4896) 42(1:1282) Kolasib 12(1:5497) 50(1:1319) Mizoram 242(1:3671) 311(1:2857)* 993(1:895) 1819 (1:488)* * Govt. and private hospital doctor ** Including non-govt. hospital bed( Including non-government hospitals bed such as- 1st A.R Hospital, Presbyterian Hospital, Seventh Day Hospital, Greenwood Hospital, Aizawl Hospital and Research Centre, Nazareth Hospitals, Bethesda Hospital and Research Centre, Grace Nursing Home and Research Centre) # Including TB hospital-2 doctors, Kulikawn Postpartum Unit 7 doctors. Note: Christian Hospital Serkawn, Lunglei have 12 doctor and100beds. Christian hospital Lawngtlai has 2 doctors and 20 beds. There are 2 doctors and 55 beds in Lairam Christian Medical Centre, Lawngtlai (LCMC).
Source: Statistical handbook of Mizoram, Economic and Statistic, Annual Report (2005-06), H&FWD, Directorate of Health Services, Mizoram and 27th Annual Magazine of Mizoram Govt. Doctors’ Asociation-2010
Table 3.4 reveals that in terms of doctor-population ratio Aizawl district (1:1558)
is relatively well served, followed by Lunglei (1:3921) and Saiha (1:4361) districts. On
the other hand Champhai and Lawngtlai districts are poorly served with a doctor-
population ratio of 1:9854 and 1:6135 respectively. The urban bias in terms of
availability of medical practitioner is clearly revealed. Reluctance of doctors serving in
the remote areas has been the most cited reasonsii.
3.4.3. Bed-Population Ratio
An analysis of Hospital bed-population ratio (table 3.4) too reveals urban bias in
availability of healthcare facilities. Table 3.4 reveals that nearly three fifths of the
hospital beds (59.98 percent) are concentrated in the most urbanised Aizawl district and
about a fifth (19 percent) in Lunglei district. A meagre 2 percent hospital beds are
available in Serchhip and Lawngtlai districts. One reason for this disparity is due to
availability of non-government hospitals in Aizawl, Lunglei and Lawngtlai districts while
the remaining districts depend on a single government hospital. Hospital bed population
81
ratio is higher in the three districts of Aizawl (1:299), Lunglei (1:392) and Lawngtlai
(1:701) (table3.4).
The analysis of district level healthcare availability reveals some contradiction. In
terms of availability of health institutions the most urbanised districts of Aizawl is best
served in terms of hospital institution. However, in terms of hospital-population ratio
Lawngtlai, the most rural district appears better served facilitated by one government
hospital and two non-government hospitals. The contradiction is explained by disparity in
population concentration as around 36 percent of the state population is concentrated in
Aizawl district compared to only 8 percent in Lawngtlai. Unequal distribution of
population among the districts as well as disparity in the availability of non-government
healthcare facilities across the districts play critical role in terms of health infrastructure.
In other words, urbanisation and participation of private sector in healthcare, particularly
hospital, are significant influence on availability of health facilities in the state.
3.5. Availability of Healthcare Facilities: Inter Block Variation
Analysis of healthcare availability and its disparities at lower level of spatial
aggregation is expected to reveal the extent of disparity within the state as far as health
infrastructure is concerned. There are 22 rural development blocks in Mizoram. The
analysis is confined to availability of healthcare facility at Community Health Centre
(CHC)/ Primary Health Centre (PHC)/Main Centre (MC) and Sub-centre level. As per
the Ministry of health and family welfare norms, Primary Health Centre (PHC) is
expected to serve 20,000 persons in the hilly tribal areas and 30,000 persons in the plain
areas. The Community Health Centre (CHC) is expected to serve for 80,000 persons in
the hilly tribal areas and 1, 20,000 persons in the plain areas (MHFW, 2006).
3.5.1. Availability of Health Infrastructure
Generally block headquarters in Mizoram are facilitated with PHC or CHC health
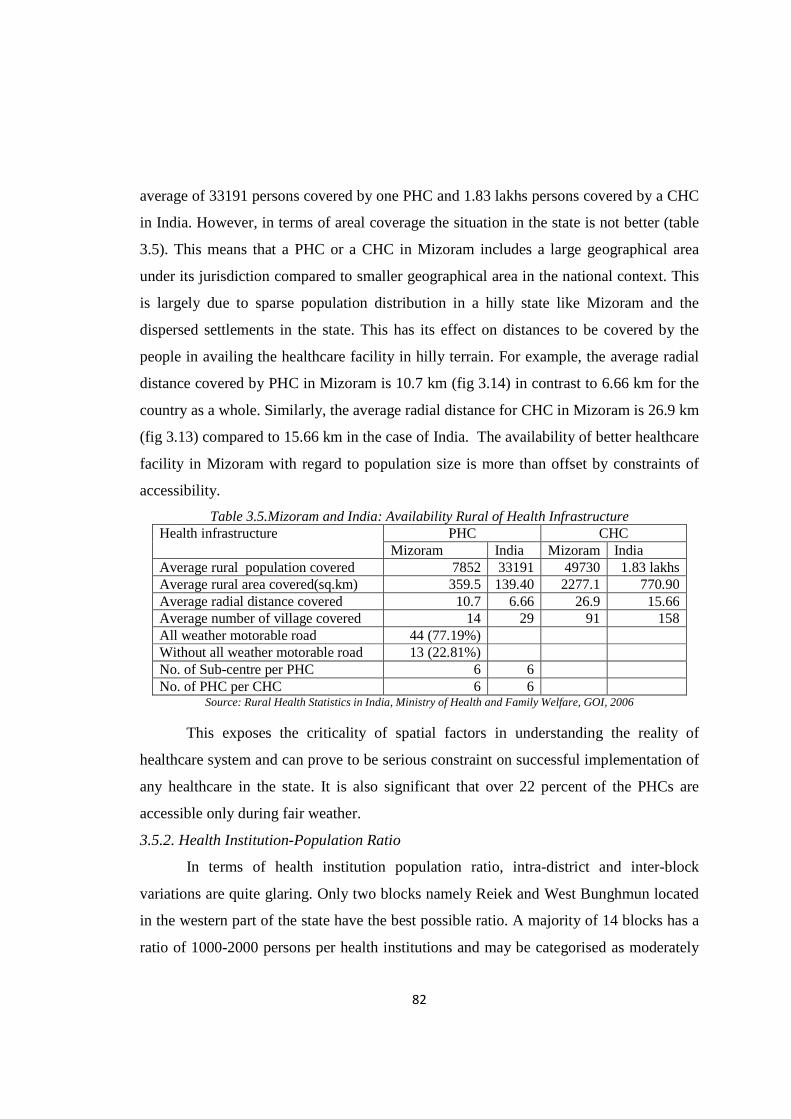
institution. Table 3.5 reveals that the population coverage of PHC and CHC in Mizoram
is better than national norm. Average population covered by a PHC in Mizoram is around
7852 persons while 49730 persons are covered by a CHC. This is far below the national
82
average of 33191 persons covered by one PHC and 1.83 lakhs persons covered by a CHC
in India. However, in terms of areal coverage the situation in the state is not better (table
3.5). This means that a PHC or a CHC in Mizoram includes a large geographical area
under its jurisdiction compared to smaller geographical area in the national context. This
is largely due to sparse population distribution in a hilly state like Mizoram and the
dispersed settlements in the state. This has its effect on distances to be covered by the
people in availing the healthcare facility in hilly terrain. For example, the average radial
distance covered by PHC in Mizoram is 10.7 km (fig 3.14) in contrast to 6.66 km for the
country as a whole. Similarly, the average radial distance for CHC in Mizoram is 26.9 km
(fig 3.13) compared to 15.66 km in the case of India. The availability of better healthcare
facility in Mizoram with regard to population size is more than offset by constraints of
accessibility.
Table 3.5.Mizoram and India: Availability Rural of Health Infrastructure Health infrastructure PHC CHC
Mizoram India Mizoram India Average rural population covered 7852 33191 49730 1.83 lakhs Average rural area covered(sq.km) 359.5 139.40 2277.1 770.90 Average radial distance covered 10.7 6.66 26.9 15.66 Average number of village covered 14 29 91 158 All weather motorable road 44 (77.19%) Without all weather motorable road 13 (22.81%) No. of Sub-centre per PHC 6 6
No. of PHC per CHC 6 6 Source: Rural Health Statistics in India, Ministry of Health and Family Welfare, GOI, 2006
This exposes the criticality of spatial factors in understanding the reality of
healthcare system and can prove to be serious constraint on successful implementation of
any healthcare in the state. It is also significant that over 22 percent of the PHCs are
accessible only during fair weather.
3.5.2. Health Institution-Population Ratio
In terms of health institution population ratio, intra-district and inter-block
variations are quite glaring. Only two blocks namely Reiek and West Bunghmun located
in the western part of the state have the best possible ratio. A majority of 14 blocks has a
ratio of 1000-2000 persons per health institutions and may be categorised as moderately

83
served. These blocks are quite widespread across the state (Table-3.6 see fig 3.15). The
remaining 6 blocks are least served and are found in two pockets, one in the north and the
other in the south (fig 3.15). Out of these, Chawngte and Lawngtlai, located in the
southern part belong to the rural district of Lawngtlai. Paradoxically, Tlangnuam and
Thingsulthliah located in the central part of the state belong to the most urbanised Aizawl
district.
Table 3.6.Mizoram: Government Health Institution –Population Ratio Category No. of
Block Name of the Blocks
Best Served Blocks (< 1:1000 )
2 Reiek, W. Bunghmun
Moderately Served Block (1:1000-2000)
14 Zawlnuam, Darlawn, Phullen, E. Lungdar, Ngopa, Hnahthial, Sangau, Aibawk, Serchhip, Tuipang, Lunglei, W.Phaileng, Khawbung, Khawzawl,
Least Served Blocks (1:2000 and above)
6 Lawngtlai, Tlangnuam, Thingsulthliah, N. Thingdawl, Chawngte, Lungsen
Source: Annual Report 2005-06, Health & Family Welfare Dept. Govt. of Mizoram
It is clear that mere numerical strength of healthcare centre is not a sufficient
indicator of the region being well served. For example, West Bunghmun block is the
worst served block in terms of total number of health institutions. However, it is the best
served block (1:747) when it comes to healthcare centre-population ratio (table 3.6). This
is due largely to unequal distribution of population across the blocks (Appendix-I).
3.5.3. Doctor-Population Ratio
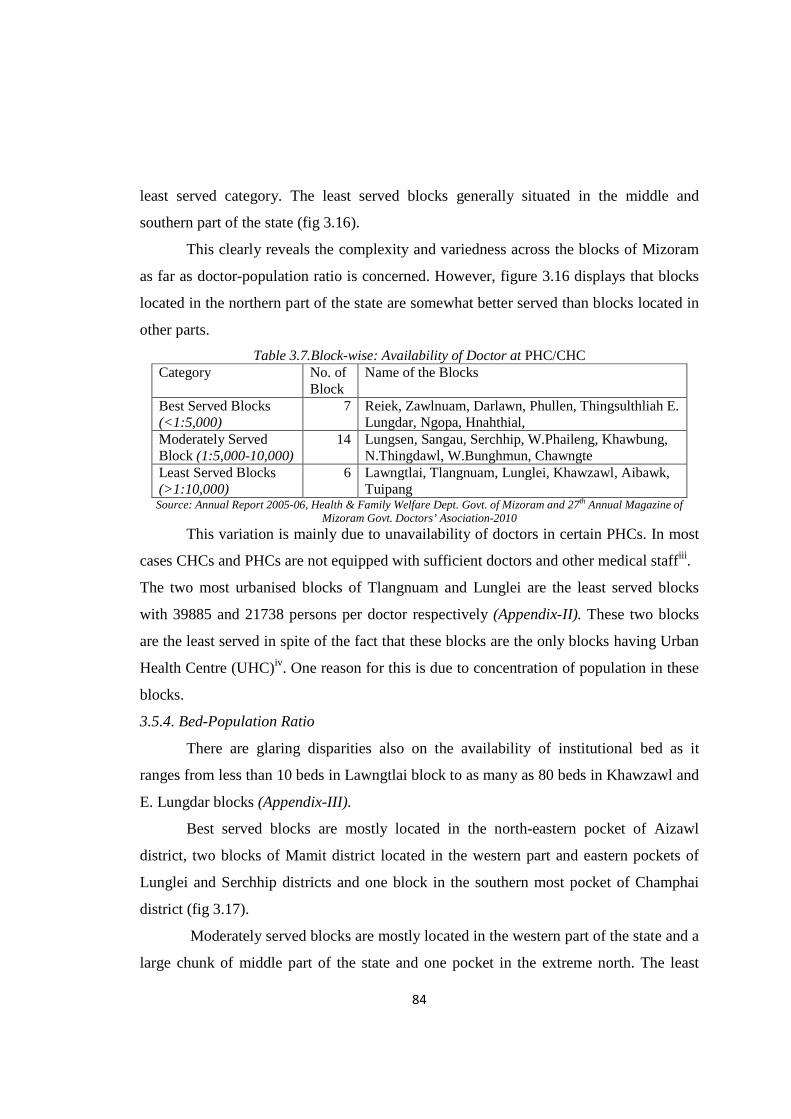
Table 3.7 reveals that there are significant inter-block variations in the availability
of doctor at health centres (appendix 3.2). Only one-third of the blocks are in the best
served category. The best served blocks are located in three pockets such as north-eastern
part of Aizawl district, two blocks in Mamit district and small pocket in the eastern part
of Lunglei and Serchhip districts. Majority of the blocks (14 blocks) are in the category
of moderately served block spread across the state. Most of the western part bordering
Bangladesh and Tripura are in the moderately served blocks. Other blocks belonging to
moderately served category are dotted in various part of the state. For example: Serchhip
block located in the central part of the state, N.Thingdawl block in the northern part of
the state and Sangau block in the south (fig3.16). The remaining six blocks are under
84
least served category. The least served blocks generally situated in the middle and
southern part of the state (fig 3.16).
This clearly reveals the complexity and variedness across the blocks of Mizoram
as far as doctor-population ratio is concerned. However, figure 3.16 displays that blocks
located in the northern part of the state are somewhat better served than blocks located in
other parts.
Table 3.7.Block-wise: Availability of Doctor at PHC/CHC Category No. of
Block Name of the Blocks
Best Served Blocks (<1:5,000)
7 Reiek, Zawlnuam, Darlawn, Phullen, Thingsulthliah E. Lungdar, Ngopa, Hnahthial,
Moderately Served Block (1:5,000-10,000)
14 Lungsen, Sangau, Serchhip, W.Phaileng, Khawbung, N.Thingdawl, W.Bunghmun, Chawngte
Least Served Blocks (>1:10,000)
6 Lawngtlai, Tlangnuam, Lunglei, Khawzawl, Aibawk, Tuipang
Source: Annual Report 2005-06, Health & Family Welfare Dept. Govt. of Mizoram and 27th Annual Magazine of Mizoram Govt. Doctors’ Asociation-2010
This variation is mainly due to unavailability of doctors in certain PHCs. In most
cases CHCs and PHCs are not equipped with sufficient doctors and other medical staffiii .
The two most urbanised blocks of Tlangnuam and Lunglei are the least served blocks
with 39885 and 21738 persons per doctor respectively (Appendix-II). These two blocks
are the least served in spite of the fact that these blocks are the only blocks having Urban
Health Centre (UHC)iv. One reason for this is due to concentration of population in these
blocks.
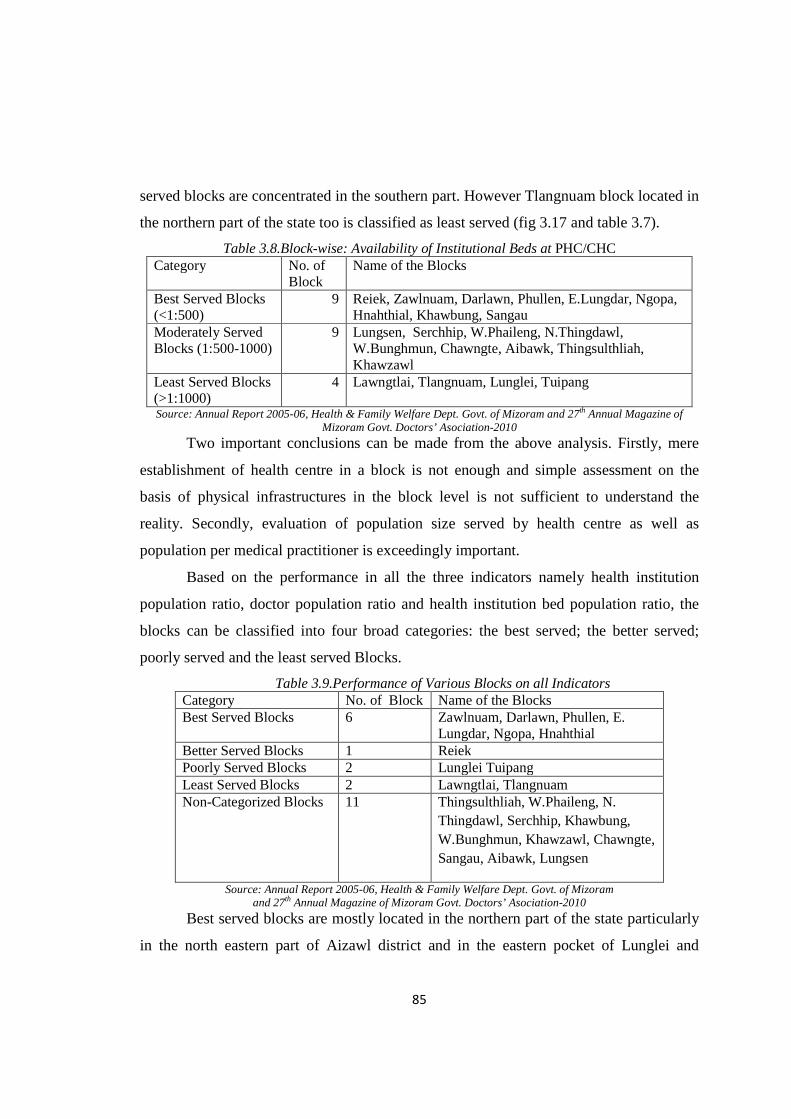
3.5.4. Bed-Population Ratio
There are glaring disparities also on the availability of institutional bed as it
ranges from less than 10 beds in Lawngtlai block to as many as 80 beds in Khawzawl and
E. Lungdar blocks (Appendix-III).
Best served blocks are mostly located in the north-eastern pocket of Aizawl
district, two blocks of Mamit district located in the western part and eastern pockets of
Lunglei and Serchhip districts and one block in the southern most pocket of Champhai
district (fig 3.17).
Moderately served blocks are mostly located in the western part of the state and a
large chunk of middle part of the state and one pocket in the extreme north. The least
85
served blocks are concentrated in the southern part. However Tlangnuam block located in
the northern part of the state too is classified as least served (fig 3.17 and table 3.7).
Table 3.8.Block-wise: Availability of Institutional Beds at PHC/CHC Category No. of
Block Name of the Blocks
Best Served Blocks (<1:500)
9 Reiek, Zawlnuam, Darlawn, Phullen, E.Lungdar, Ngopa, Hnahthial, Khawbung, Sangau
Moderately Served Blocks (1:500-1000)
9 Lungsen, Serchhip, W.Phaileng, N.Thingdawl, W.Bunghmun, Chawngte, Aibawk, Thingsulthliah, Khawzawl
Least Served Blocks (>1:1000)
4 Lawngtlai, Tlangnuam, Lunglei, Tuipang
Source: Annual Report 2005-06, Health & Family Welfare Dept. Govt. of Mizoram and 27th Annual Magazine of Mizoram Govt. Doctors’ Asociation-2010
Two important conclusions can be made from the above analysis. Firstly, mere
establishment of health centre in a block is not enough and simple assessment on the
basis of physical infrastructures in the block level is not sufficient to understand the
reality. Secondly, evaluation of population size served by health centre as well as
population per medical practitioner is exceedingly important.
Based on the performance in all the three indicators namely health institution
population ratio, doctor population ratio and health institution bed population ratio, the
blocks can be classified into four broad categories: the best served; the better served;
poorly served and the least served Blocks.
Table 3.9.Performance of Various Blocks on all Indicators Category No. of Block Name of the Blocks Best Served Blocks 6 Zawlnuam, Darlawn, Phullen, E.
Lungdar, Ngopa, Hnahthial Better Served Blocks 1 Reiek Poorly Served Blocks 2 Lunglei Tuipang Least Served Blocks 2 Lawngtlai, Tlangnuam Non-Categorized Blocks 11 Thingsulthliah, W.Phaileng, N.
Thingdawl, Serchhip, Khawbung, W.Bunghmun, Khawzawl, Chawngte, Sangau, Aibawk, Lungsen
Source: Annual Report 2005-06, Health & Family Welfare Dept. Govt. of Mizoram and 27th Annual Magazine of Mizoram Govt. Doctors’ Asociation-2010
Best served blocks are mostly located in the northern part of the state particularly
in the north eastern part of Aizawl district and in the eastern pocket of Lunglei and

86
Serchhip district. Reiek block (table 3.9) located in the western part of the state qualifies
to be better served block going by all the three indicators. There are two poorly served
blocks i.e Lunglei and Tuipang, both located in the southern part of the state. It is quite
perplexing that the most rural block of Lawngtlai, located in the southern part of the state
and the most urbanised block Tlangnuam, located in the northern part of the state fall
under least served category. The remaining 11 blocks cannot be categorised as their
position varied significantly in all the three indicators.
It is clear from the above analysis that blocks located in northern part of the state
are generally better off than blocks located in southern part of the state except in the case
Tlangnuam block.
3.6. Availability of Healthcare Facilities: Village Level Analysis
In the public sector, a sub-health Centre (Sub-centre) is the most peripheral and
the first contact point between the primary healthcare system and the community. As per
the population norms, one sub-centre is established for every 5000 persons in plain areas
and for every 3000 persons in hilly/tribal/desert areas. It is the lowest rank in a three-tier
set up consisting of the Sub-centre established for every 3000-5000 population with
referral linkage to the Primary Health Centre (PHC) and the Community Health Centre
(CHC). A Sub-centre provides an interface with the community at the grass-root level,
providing all the primary healthcare services. Of particular importance are the packages
of services such as immunization, antenatal, natal and postnatal care, prevention of
malnutrition and common childhood diseases, family planning services and counselling.
They also provide elementary drugs for minor ailments such as ARI, diarrhea, fever,
worm infestation etc. and carryout community needs assessment (Indian Public Health
Standards, Guidelines for Sub-centres, MHFW-2006).
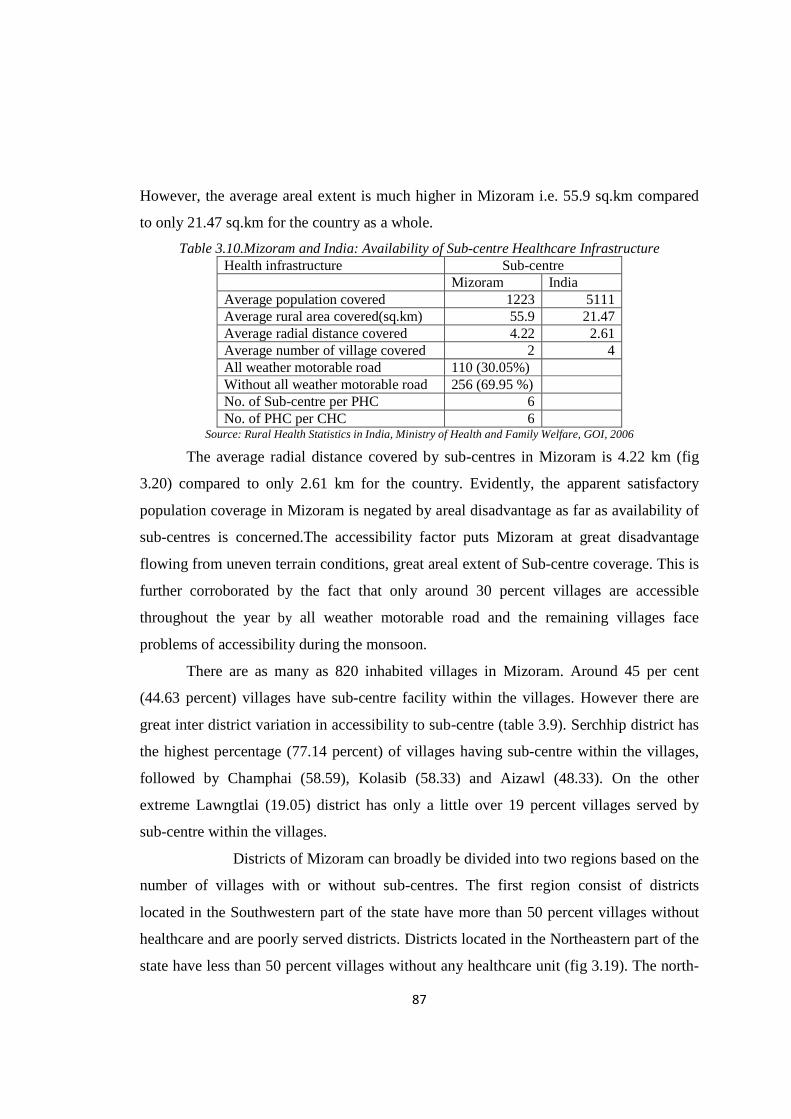
3.6.1. Availability of Healthcare Infrastructure
Table 3.10 shows that average population (1222) covered by a sub-centre in
Mizoram is less than the national average (5111). Likewise two villages are under the
jurisdiction of one sub-centre in Mizoram as against four villages in the national context.
87
However, the average areal extent is much higher in Mizoram i.e. 55.9 sq.km compared
to only 21.47 sq.km for the country as a whole.
Table 3.10.Mizoram and India: Availability of Sub-centre Healthcare Infrastructure Health infrastructure Sub-centre Mizoram India Average population covered 1223 5111 Average rural area covered(sq.km) 55.9 21.47 Average radial distance covered 4.22 2.61 Average number of village covered 2 4 All weather motorable road 110 (30.05%) Without all weather motorable road 256 (69.95 %) No. of Sub-centre per PHC 6 No. of PHC per CHC 6
Source: Rural Health Statistics in India, Ministry of Health and Family Welfare, GOI, 2006
The average radial distance covered by sub-centres in Mizoram is 4.22 km (fig
3.20) compared to only 2.61 km for the country. Evidently, the apparent satisfactory
population coverage in Mizoram is negated by areal disadvantage as far as availability of
sub-centres is concerned.The accessibility factor puts Mizoram at great disadvantage
flowing from uneven terrain conditions, great areal extent of Sub-centre coverage. This is
further corroborated by the fact that only around 30 percent villages are accessible
throughout the year by all weather motorable road and the remaining villages face
problems of accessibility during the monsoon.
There are as many as 820 inhabited villages in Mizoram. Around 45 per cent
(44.63 percent) villages have sub-centre facility within the villages. However there are
great inter district variation in accessibility to sub-centre (table 3.9). Serchhip district has
the highest percentage (77.14 percent) of villages having sub-centre within the villages,
followed by Champhai (58.59), Kolasib (58.33) and Aizawl (48.33). On the other
extreme Lawngtlai (19.05) district has only a little over 19 percent villages served by
sub-centre within the villages.
Districts of Mizoram can broadly be divided into two regions based on the
number of villages with or without sub-centres. The first region consist of districts
located in the Southwestern part of the state have more than 50 percent villages without
healthcare and are poorly served districts. Districts located in the Northeastern part of the
state have less than 50 percent villages without any healthcare unit (fig 3.19). The north-
88
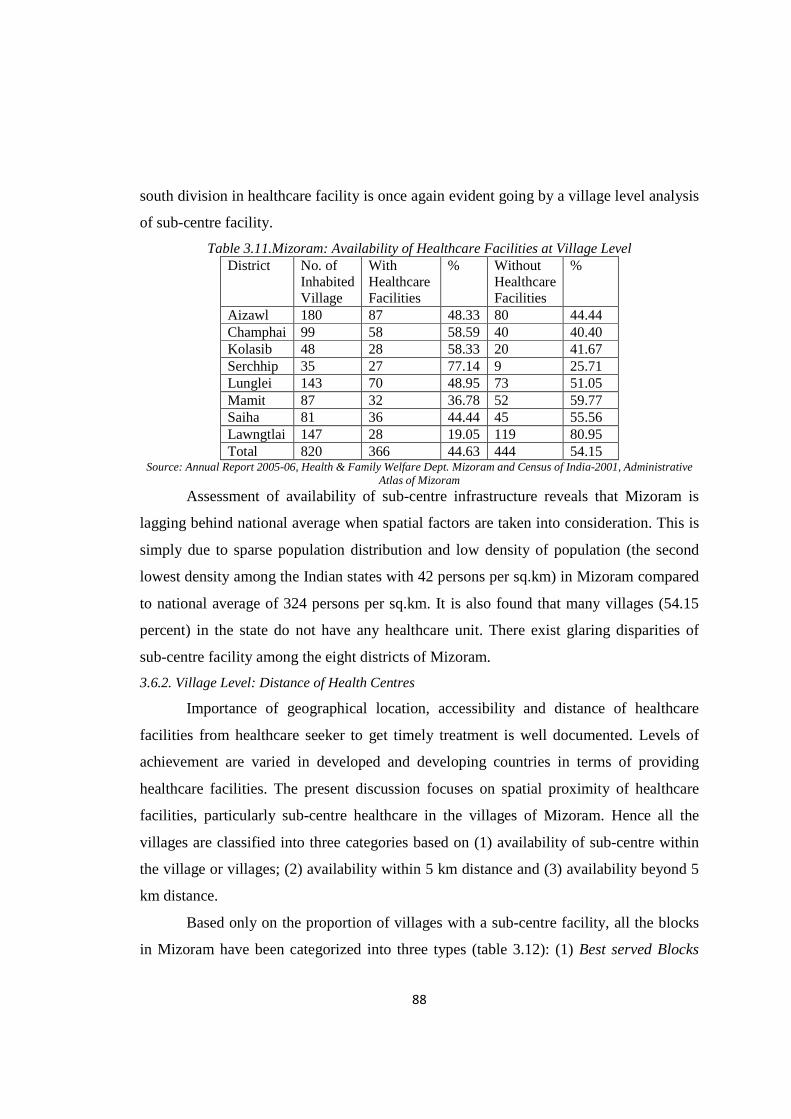
south division in healthcare facility is once again evident going by a village level analysis
of sub-centre facility.
Table 3.11.Mizoram: Availability of Healthcare Facilities at Village Level District No. of
Inhabited Village
With Healthcare Facilities
% Without Healthcare Facilities
%
Aizawl 180 87 48.33 80 44.44 Champhai 99 58 58.59 40 40.40 Kolasib 48 28 58.33 20 41.67 Serchhip 35 27 77.14 9 25.71 Lunglei 143 70 48.95 73 51.05 Mamit 87 32 36.78 52 59.77 Saiha 81 36 44.44 45 55.56 Lawngtlai 147 28 19.05 119 80.95 Total 820 366 44.63 444 54.15
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
Assessment of availability of sub-centre infrastructure reveals that Mizoram is
lagging behind national average when spatial factors are taken into consideration. This is
simply due to sparse population distribution and low density of population (the second
lowest density among the Indian states with 42 persons per sq.km) in Mizoram compared
to national average of 324 persons per sq.km. It is also found that many villages (54.15
percent) in the state do not have any healthcare unit. There exist glaring disparities of
sub-centre facility among the eight districts of Mizoram.
3.6.2. Village Level: Distance of Health Centres
Importance of geographical location, accessibility and distance of healthcare
facilities from healthcare seeker to get timely treatment is well documented. Levels of
achievement are varied in developed and developing countries in terms of providing
healthcare facilities. The present discussion focuses on spatial proximity of healthcare
facilities, particularly sub-centre healthcare in the villages of Mizoram. Hence all the
villages are classified into three categories based on (1) availability of sub-centre within
the village or villages; (2) availability within 5 km distance and (3) availability beyond 5
km distance.
Based only on the proportion of villages with a sub-centre facility, all the blocks
in Mizoram have been categorized into three types (table 3.12): (1) Best served Blocks

89
(more than 60 percent of villages having Sub-centre within the village); (2) Moderately
Served Blocks (30-60 percent of villages having Sub-centre within the village itself); and
(3) Low Served Blocks (less than 30 percent of villages having Sub-centre within the
villages itself).
Table 3.12.Block level: Availability of Sub-centre from Distance of the Nearest Village Category No. of
Block Name of the Blocks
Best Served Blocks (<60 percent)
5 Phullen, E.Lungdar, Ngopa, Khawzawl, Serchhip
Moderately Served Blocks (30-60percent)
12 N.Thingdawl, W.Bunghmun, Aibawk, Thingsulthliah, Reiek, Sangau, Khawbung, Hnahthial, Darlawn, Lunglei, Tuipang, Tlangnuam
Least Served Blocks(> 30 percent)
5 Lawngtlai, Zawlnuam, W.Phaileng, Chawngte, Lungsen
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
All the best served blocks are located in the north-eastern part of the state
(fig.3.21). Majority of the blocks (12 out of 22) however fall under the moderately served
category and are scattered in various parts of the state. As many as five blocks located in
the south-western part of the state are poorly served (fig 3.21). A detail account of each
of the blocks is given below.
3.6.2 (a). Best Served Blocks (<60 percent)
Serchhip Block
The best among the best served blocks lies in the central part of Mizoram,
extended over 798 sq.km of area.
Table 3.13. Serchhip Block: Distribution of Villages by Distance from the Nearest Sub-centre, 2001
Distance (Broad Range) No. of Villages % of Villages Total geographical area(in sq.km) 798 Number of towns 2 Distance from district headquarters 0 Sub-centre within the village 14 82.35 Sub-centre within 5 km 2 11.76 Sub-centre beyond 5km 1 5.88 Total 17 100.00
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram

90
The block is characterised by great altitudinal variation ranging from 600m to
over 1200m. As many as 14 (82.35 percent) villages contain a sub-centre within these
villages. Only 2 villages have no sub-centre within the village but can avail the facility at
a distance of 5 km or less while a single village is located beyond 5 km distance from the
nearest sub-centre (table 3.13 and fig 3.22).
Khawzawl Block
Khawzawl is the largest block in the state spread over 1802.06 sq.km area.
Altitudinal variation in this block is less pronounced as much of the land falls within
1000m to 1500m above the mean sea level. Towns like- Khawzawl, Khawhai and district
capital Champhai are located in this block. Table 3.14 shows that out of 44 villages in the
block, 32(72.73 percent) villages house a sub-centre within the villages while a little over
13 percent of the village are located within a distance of 5 km from the nearest sub-
centre. Another 13 percent villages are located at a distance over 5 km from the nearest
sub-centre (fig.3.23). Settlements are mixtures of both sparse and linear in character
(fig.3.23).
Table 3.14.Khawzawl Block: Distribution of Villages by Distance from Nearest Sub-centre, 2001 Distance (Broad Range) No. of Villages % of Villages Total geographical area (in sq.km.) 1802.06 Total number of towns 3 Distance from district headquarters 24 km Sub-centre within the village 32 72.73 Sub-centre within 5 km 6 13.64 Sub-centre beyond 5km 6 13.64 Total 44 100
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
East Lungdar Block
Situated in a fairly high altitudinal zone, 900m to above 1800m from mean sea-
level and at 70 km away from the district headquarter of Serchhip. East Lungdar block
embraces about 1328 sq.km geographical land area.
More than 72 percent of villages have sub-centres whereas little over 11 percent
villages are without health centre but are located in the proximity of 5 km distance from
the nearest village with a sub-centre.
91
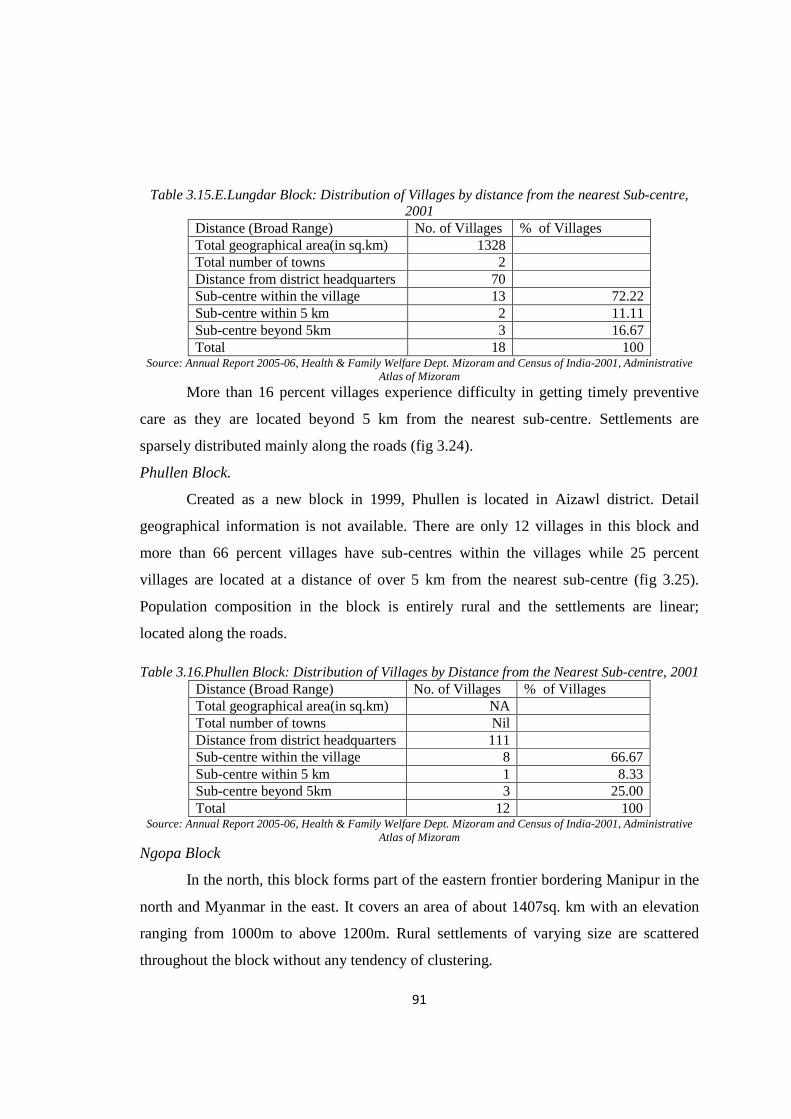
Table 3.15.E.Lungdar Block: Distribution of Villages by distance from the nearest Sub-centre, 2001
Distance (Broad Range) No. of Villages % of Villages Total geographical area(in sq.km) 1328 Total number of towns 2 Distance from district headquarters 70 Sub-centre within the village 13 72.22 Sub-centre within 5 km 2 11.11 Sub-centre beyond 5km 3 16.67 Total 18 100
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
More than 16 percent villages experience difficulty in getting timely preventive
care as they are located beyond 5 km from the nearest sub-centre. Settlements are
sparsely distributed mainly along the roads (fig 3.24).
Phullen Block.
Created as a new block in 1999, Phullen is located in Aizawl district. Detail
geographical information is not available. There are only 12 villages in this block and
more than 66 percent villages have sub-centres within the villages while 25 percent
villages are located at a distance of over 5 km from the nearest sub-centre (fig 3.25).
Population composition in the block is entirely rural and the settlements are linear;
located along the roads.
Table 3.16.Phullen Block: Distribution of Villages by Distance from the Nearest Sub-centre, 2001 Distance (Broad Range) No. of Villages % of Villages Total geographical area(in sq.km) NA Total number of towns Nil Distance from district headquarters 111 Sub-centre within the village 8 66.67 Sub-centre within 5 km 1 8.33 Sub-centre beyond 5km 3 25.00 Total 12 100
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
Ngopa Block
In the north, this block forms part of the eastern frontier bordering Manipur in the
north and Myanmar in the east. It covers an area of about 1407sq. km with an elevation
ranging from 1000m to above 1200m. Rural settlements of varying size are scattered
throughout the block without any tendency of clustering.

92
Table 3.17.Ngopa Block: Distribution of Villages by Distance from the Nearest Sub-centre, 2001 Distance (Broad Range) No. of Villages % of Villages Total geographical area(in sq.km) 1407 Total number of towns Nil Distance from district headquarters 108 Sub-centre within the village 11 64.71 Sub-centre within 5 km 3 17.65 Sub-centre beyond 5km 3 17.65 Total 17 100.00
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
Nearly 65 percent villages are equipped with a sub-centre facility (table 3.17). On
the other hand more than 17 percent villages are located at a distance of over 5 km from
the nearest sub-centre (fig 3.26).
3.6.2 (b). Moderately Served Blocks (30-60percent)
Sangau Block
Sangau block lies in the southern loftiest part of the mountainous region of the
state with the elevation ranging from 1200m to 2000m above the mean sea level. It
covers an area of 565.91 sq.km. It is the second smallest block in the state.
Table 3.18.Sangau Block: Distribution of Villages by Distance from the Nearest Sub-centre, 2001 Distance (Broad Range) No. of Villages % of Villages Total geographical area(in sq.km) 565.91 Total number of towns Nil Distance from district headquarters 80 Sub-centre within the village 11 57.89 Sub-centre within 5 km 1 5.26 Sub-centre beyond 5km 7 36.84 Total 19 19.00
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
Table 3.18 reveals that almost 58 percent of the villages are facilitated with a sub-
centre while over 36 percent villages are located at a distance beyond 5 km from the
nearest sub-centre. Settlements are sparsely distributed all over the block (fig 3.27).
North Thingdawl Block
North Thingdawl block is the second largest block of the state located in the
northern most part of the state bordering Cachar district of Assam in the north. It covers
an area of 1472.12 sq.km. The general elevation progressively increases from north to
93
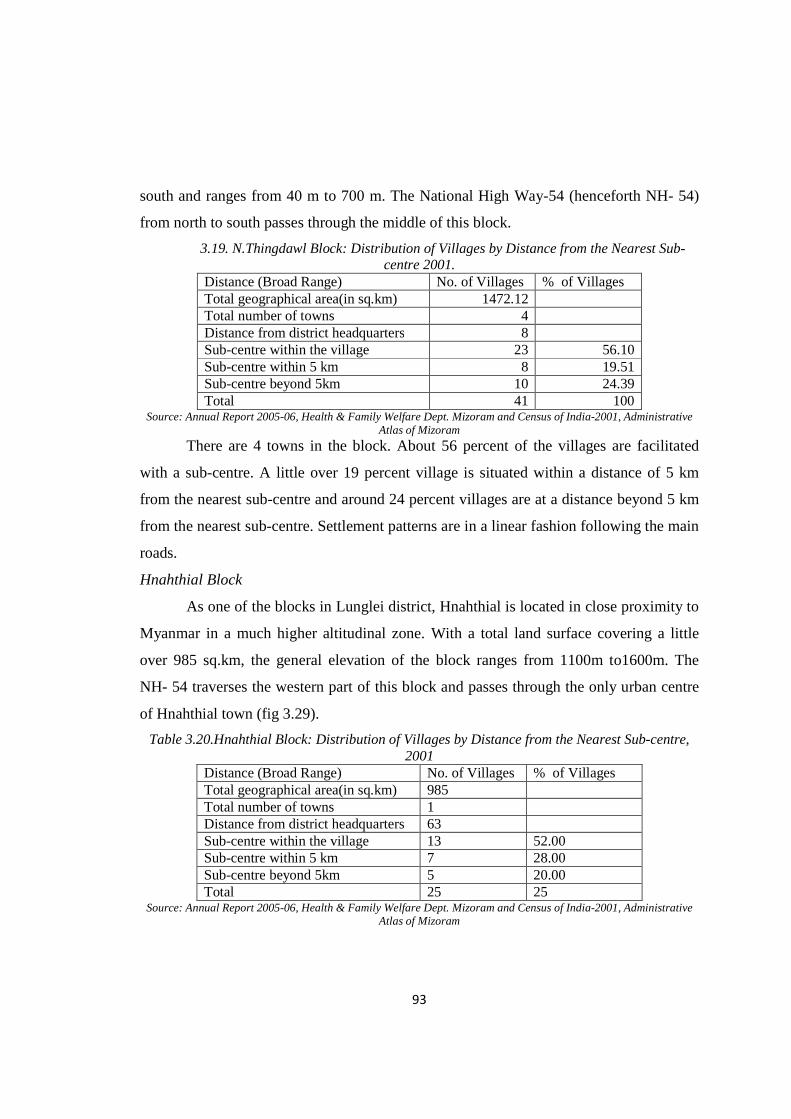
south and ranges from 40 m to 700 m. The National High Way-54 (henceforth NH- 54)
from north to south passes through the middle of this block.
3.19. N.Thingdawl Block: Distribution of Villages by Distance from the Nearest Sub-centre 2001.
Distance (Broad Range) No. of Villages % of Villages Total geographical area(in sq.km) 1472.12 Total number of towns 4 Distance from district headquarters 8 Sub-centre within the village 23 56.10 Sub-centre within 5 km 8 19.51 Sub-centre beyond 5km 10 24.39 Total 41 100
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
There are 4 towns in the block. About 56 percent of the villages are facilitated
with a sub-centre. A little over 19 percent village is situated within a distance of 5 km
from the nearest sub-centre and around 24 percent villages are at a distance beyond 5 km
from the nearest sub-centre. Settlement patterns are in a linear fashion following the main
roads.
Hnahthial Block
As one of the blocks in Lunglei district, Hnahthial is located in close proximity to
Myanmar in a much higher altitudinal zone. With a total land surface covering a little
over 985 sq.km, the general elevation of the block ranges from 1100m to1600m. The
NH- 54 traverses the western part of this block and passes through the only urban centre
of Hnahthial town (fig 3.29).
Table 3.20.Hnahthial Block: Distribution of Villages by Distance from the Nearest Sub-centre, 2001
Distance (Broad Range) No. of Villages % of Villages Total geographical area(in sq.km) 985 Total number of towns 1 Distance from district headquarters 63 Sub-centre within the village 13 52.00 Sub-centre within 5 km 7 28.00 Sub-centre beyond 5km 5 20.00 Total 25 25
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
94
Out of a total of 25 villages in the block, 13 (52 percent) of them have a sub-
centre located within the village, 28 are located within 5 km from the nearest sub-centre
and 20 percent are located beyond 5 km from the nearest sub-centre ( table 3.20).
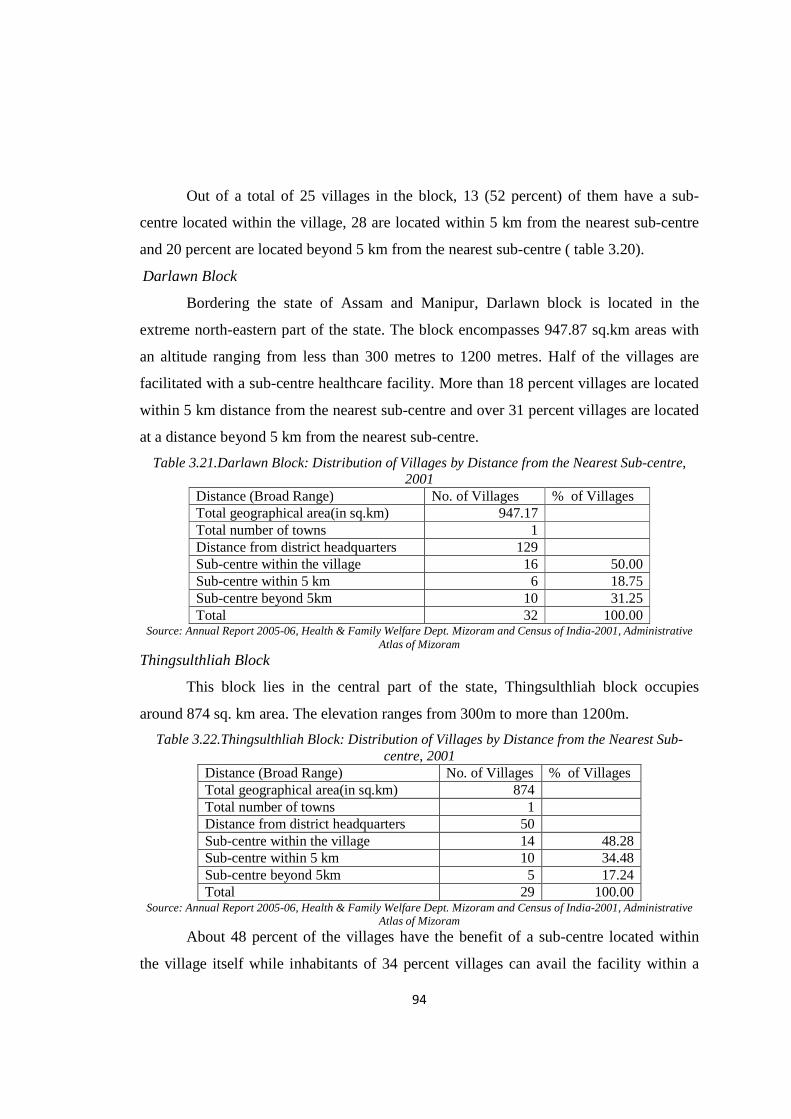
Darlawn Block
Bordering the state of Assam and Manipur, Darlawn block is located in the
extreme north-eastern part of the state. The block encompasses 947.87 sq.km areas with
an altitude ranging from less than 300 metres to 1200 metres. Half of the villages are
facilitated with a sub-centre healthcare facility. More than 18 percent villages are located
within 5 km distance from the nearest sub-centre and over 31 percent villages are located
at a distance beyond 5 km from the nearest sub-centre.
Table 3.21.Darlawn Block: Distribution of Villages by Distance from the Nearest Sub-centre, 2001
Distance (Broad Range) No. of Villages % of Villages Total geographical area(in sq.km) 947.17 Total number of towns 1 Distance from district headquarters 129 Sub-centre within the village 16 50.00 Sub-centre within 5 km 6 18.75 Sub-centre beyond 5km 10 31.25 Total 32 100.00
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
Thingsulthliah Block
This block lies in the central part of the state, Thingsulthliah block occupies
around 874 sq. km area. The elevation ranges from 300m to more than 1200m.
Table 3.22.Thingsulthliah Block: Distribution of Villages by Distance from the Nearest Sub-centre, 2001
Distance (Broad Range) No. of Villages % of Villages Total geographical area(in sq.km) 874 Total number of towns 1 Distance from district headquarters 50 Sub-centre within the village 14 48.28 Sub-centre within 5 km 10 34.48 Sub-centre beyond 5km 5 17.24 Total 29 100.00
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
About 48 percent of the villages have the benefit of a sub-centre located within
the village itself while inhabitants of 34 percent villages can avail the facility within a

95
distance of 5kms. Around 17 percent villages are located more than 5 kms from the
nearest sub-centre (table 3.22 and fig 3.31).
Lunglei Block
Located in the southern part of the state, Lunglei covers 1117 sq.km area with an
altitude ranging from 300m to 1200m. This is the second most urbanised block in the
state containing one town i.e Lunglei.
Nearly 47 percent villages are equipped with sub-centre; but around 26
percent villages avail the facility at a distance of 5 kms or less (table 3.23). A little over
27 percent of the villages have to travel more than 5 kms to avail such a facility.
Settlements are generally scattered across the block. (fig3.32)
Table 3.23.Lunglei Block: Distribution of Villages by Distance from the Nearest Sub-centre, 2001
Distance (Broad Range) No. of Villages % of Villages Total geographical area(in sq.km) 1117 Total number of towns 1 Distance from district headquarters 0 Sub-centre within the village 22 46.81 Sub-centre within 5 km 12 25.53 Sub-centre beyond 5km 13 27.66 Total 47 100.00
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
Tlangnuam Block
The most urbanised Tlangnuam block has the capital city of Aizawl located
within and contains a very high proportion of health centres of various types but also has
an excessive concentration of population. The block forms part of the central ridge with
an elevation ranging from 600m-1220 m.
Table 3.24 reveals that there are 20 villages in the block , of which 9 (45
percent) are facilitated with a sub-centre, 7 villages are in a close proximity of 5 km or
less from the nearest sub-centre and the remaining 4 villages at a distance of over 5 km
from the nearest sub-centre (fig 3.33).

96
Table 3.24.Tlangnuam Block: Distribution of Villages by Distance from the Nearest Sub-centre, 2001
Distance (Broad Range) No. of Villages % of Villages Total geographical area(in sq.km) 532.27 Total number of towns 2 Distance from district headquarters 0 Sub-centre within the village 9 45.00 Sub-centre within 5 km 7 35.00 Sub-centre beyond 5km 4 20.00 Total 20 100.00
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
Tuipang Block
Situated in the high altitudinal zone, Tuipang block lies in the south-eastern
corner of the state within Saiha district bordering Myanmar. It occupies 1399.90 sq.km
geographical areas with an altitude that ranges from 800m to 2000m above mean sea
level indicating extreme variation in altitude.
Table 3.25.Tuipang Block: Distribution of Villages by Distance from the Nearest Sun-Centre, 2001
Distance (Broad Range) No. of Villages % of Villages Total geographical area(in sq.km) 1399.9 Total population 47034 Distance from district headquarters 75 Sub-centre within the village 25 44.64 Sub-centre within 5 km 21 37.50 Sub-centre beyond 5km 10 17.86 Total 56 100
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
It is evident that 44.64 percent of the villages have sub-centres located within the
villages; about 35 percent located at a distance of less than 5 km from the nearest sub-
centre and more than 17 percent at a distance farther than 5 km from the nearest sub-
centre (table 3.25 and fig 3.34).Settlements are dotted sparsely across the block.
Khawbung Block
Khawbung block is situated in the eastern high mountainous range of Champhai
district bordering Myanmar. Because of its late creation in 1999, detail geographical
variables are not yet properly drawn as a block (table 3.26).

97
Table 3.26.Khawbung Block: Distribution of Villages by Distance from the Nearest Sub-centre, 2001
Distance (Broad Range) No. of Villages % of Villages Total geographical area(in sq.km) NA Total number of towns Nil Distance from district headquarters 56 Sub-centre within the village 10 37.04 Sub-centre within 5 km 7 25.93 Sub-centre beyond 5km 10 37.04 Total 27 100
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
Settlements are sparsely distributed all over the block. There are 27 villages but
only a little over 37 percent have sub-centre facility located within the villages. Almost
26 percent villages are situated within 5 km distance from the nearest sub-centre and
more than 37 percent are located far from health sub-centre (fig 3.35).
Aibawk Block
Aibawk block in Aizawl district is located in the interior part of the state covering
a geographical area of 616.88 sq. km. The elevation ranges from 600m–900m. Rural
settlements are usually in a linear fashion along the roads (fig 3.36).
Table 3.27.Aibawk Block: Distribution of Villages by Distance from the Nearest Sub-centre 2001 Distance (Broad Range) No. of Villages % of Villages Total geographical area (in sq.km) 616.18 Total number of towns Nil Distance from district headquarters 30 Sub-centre within the village 9 36.00 Sub-centre within 5 km 7 28.00 Sub-centre beyond 5km 9 36.00 Total 25 100
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
Even though located within the most urbanised district of Aizawl, only 36 percent
villages are facilitated with sub-centre facility and an equal proportion is situated farther
than 5 km from the nearest health centre (table 3.27).
Reiek Block
Reiek Block in the district of Mamit bordering Aizawl district in the east is covers
937.42 sq.km land area. This block is characterised by great altitudinal variation ranging
between 600m to 1465 metres.
98
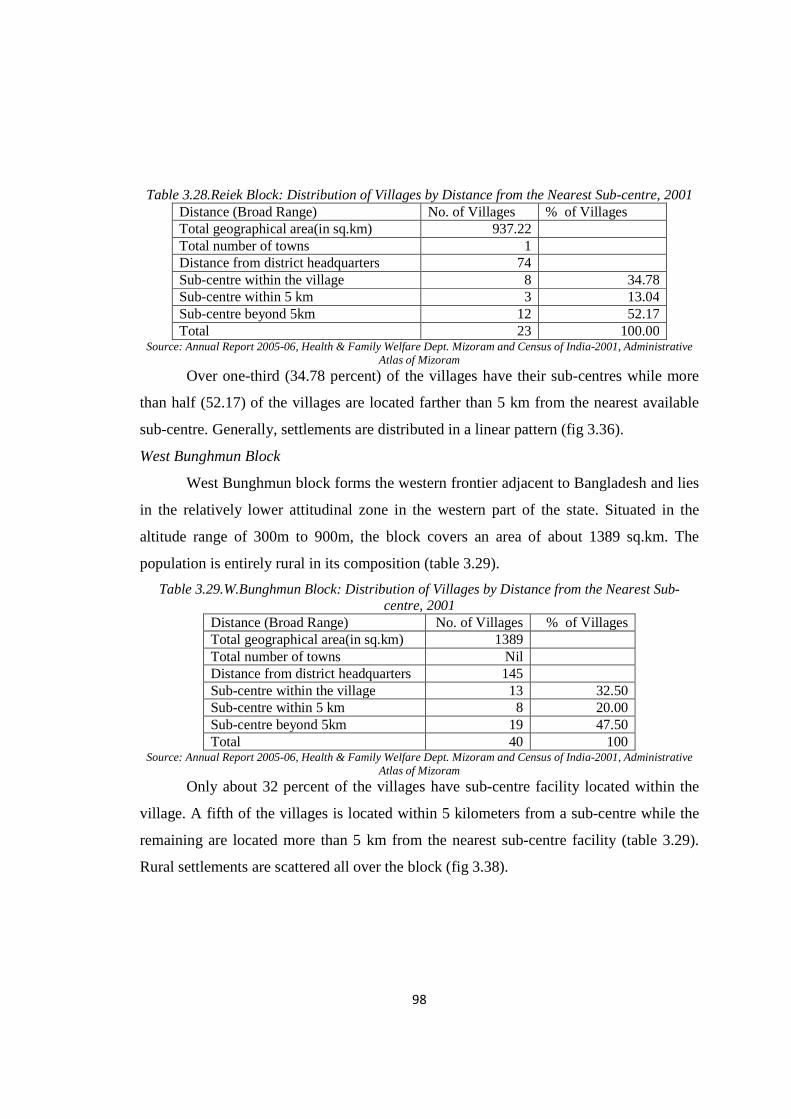
Table 3.28.Reiek Block: Distribution of Villages by Distance from the Nearest Sub-centre, 2001 Distance (Broad Range) No. of Villages % of Villages Total geographical area(in sq.km) 937.22 Total number of towns 1 Distance from district headquarters 74 Sub-centre within the village 8 34.78 Sub-centre within 5 km 3 13.04 Sub-centre beyond 5km 12 52.17 Total 23 100.00
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
Over one-third (34.78 percent) of the villages have their sub-centres while more
than half (52.17) of the villages are located farther than 5 km from the nearest available
sub-centre. Generally, settlements are distributed in a linear pattern (fig 3.36).
West Bunghmun Block
West Bunghmun block forms the western frontier adjacent to Bangladesh and lies
in the relatively lower attitudinal zone in the western part of the state. Situated in the
altitude range of 300m to 900m, the block covers an area of about 1389 sq.km. The
population is entirely rural in its composition (table 3.29).
Table 3.29.W.Bunghmun Block: Distribution of Villages by Distance from the Nearest Sub-centre, 2001
Distance (Broad Range) No. of Villages % of Villages Total geographical area(in sq.km) 1389 Total number of towns Nil Distance from district headquarters 145 Sub-centre within the village 13 32.50 Sub-centre within 5 km 8 20.00 Sub-centre beyond 5km 19 47.50 Total 40 100
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
Only about 32 percent of the villages have sub-centre facility located within the
village. A fifth of the villages is located within 5 kilometers from a sub-centre while the
remaining are located more than 5 km from the nearest sub-centre facility (table 3.29).
Rural settlements are scattered all over the block (fig 3.38).

99
3.6.2 (c). Least Served Blocks (> 30 percent)
Zawlnuam Block
The block is situated in the north-western part of the state bordering
Tripura in the west and Assam in the north. Characterised generally by low relief (300m
to 600m) the block covers a geographical area of 1071.15 sq.km. There are 57 villages in
the block (fig 3.38). Only a quarter (26.32 percent) of the villages has sub-centres located
in them. A very large number of the villages (54.39 percent) lack easy access to minimal
healthcare as provided by the sub-centres. Rural settlements are sparse and scattered in
this block (fig 3.39).
Table 3.30.Zawlnuam Block: Distribution of Villages by Distance from the Nearest Sub-centre 2001
Distance (Broad Range) No. of Villages % of Villages Total geographical area(in sq.km) 1071.15 Total number of towns 2 Distance from district headquarters 67 Sub-centre within the village 15 26.32 Sub-centre within 5 km 11 19.30 Sub-centre beyond 5km 31 54.39 Total 57 100
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
Lawngtlai Block
Lawngtlai block lies in the southern extreme of the state being sandwiched by the
most deprived block Chawngte in the west and Tuipang block in the east. Covering an
area of 1304.84 sq.km in a relatively low relief zone (400m-900m), the block supports a
population entirely rural in population composition (table 3.31).
Table 3.31.Lawngtlai Block: Distribution of Villages by Distance from the Nearest Sub-centre 2001
Distance (Broad Range) No. of Villages % of Villages Total geographical area (in sq.km) 1304.84 Total number of towns Nil Distance from district headquarters 0 Sub-centre within the village 14 21.54 Sub-centre within 5 km 26 40.00 Sub-centre beyond 5km 25 38.46 Total 65 100
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
100
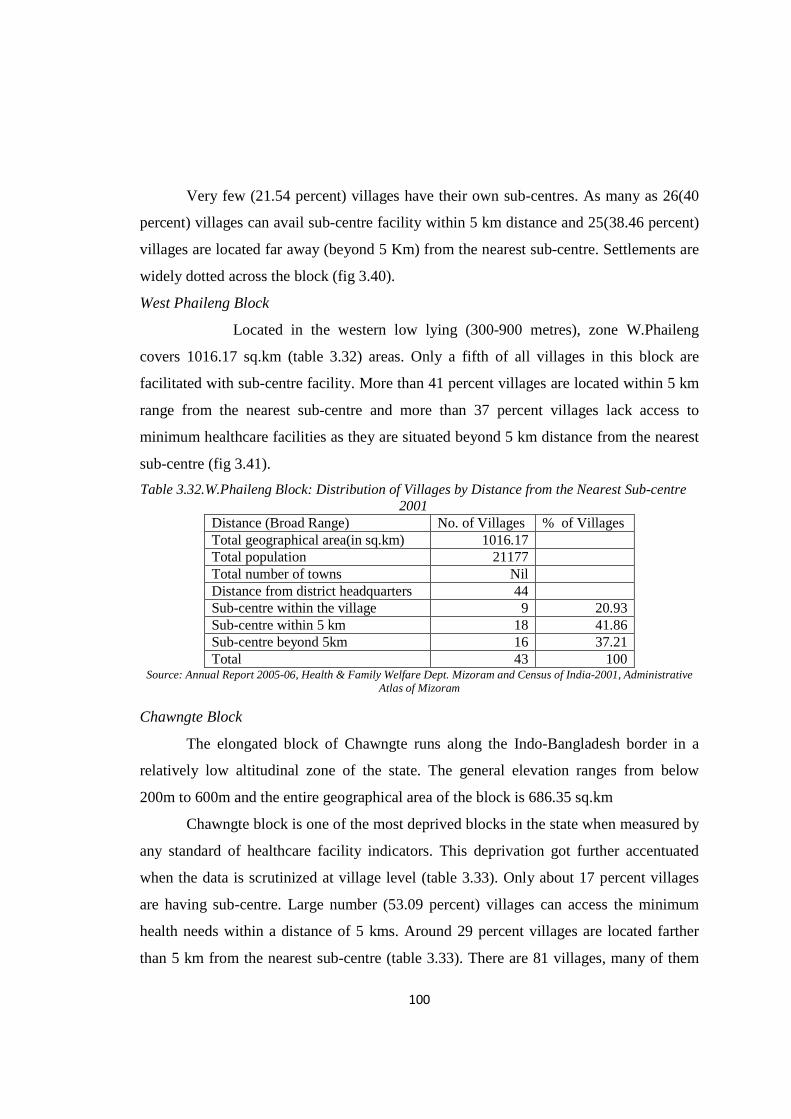
Very few (21.54 percent) villages have their own sub-centres. As many as 26(40
percent) villages can avail sub-centre facility within 5 km distance and 25(38.46 percent)
villages are located far away (beyond 5 Km) from the nearest sub-centre. Settlements are
widely dotted across the block (fig 3.40).
West Phaileng Block
Located in the western low lying (300-900 metres), zone W.Phaileng
covers 1016.17 sq.km (table 3.32) areas. Only a fifth of all villages in this block are
facilitated with sub-centre facility. More than 41 percent villages are located within 5 km
range from the nearest sub-centre and more than 37 percent villages lack access to
minimum healthcare facilities as they are situated beyond 5 km distance from the nearest
sub-centre (fig 3.41).
Table 3.32.W.Phaileng Block: Distribution of Villages by Distance from the Nearest Sub-centre 2001
Distance (Broad Range) No. of Villages % of Villages Total geographical area(in sq.km) 1016.17 Total population 21177 Total number of towns Nil Distance from district headquarters 44 Sub-centre within the village 9 20.93 Sub-centre within 5 km 18 41.86 Sub-centre beyond 5km 16 37.21 Total 43 100
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
Chawngte Block
The elongated block of Chawngte runs along the Indo-Bangladesh border in a
relatively low altitudinal zone of the state. The general elevation ranges from below
200m to 600m and the entire geographical area of the block is 686.35 sq.km
Chawngte block is one of the most deprived blocks in the state when measured by
any standard of healthcare facility indicators. This deprivation got further accentuated
when the data is scrutinized at village level (table 3.33). Only about 17 percent villages
are having sub-centre. Large number (53.09 percent) villages can access the minimum
health needs within a distance of 5 kms. Around 29 percent villages are located farther
than 5 km from the nearest sub-centre (table 3.33). There are 81 villages, many of them
101
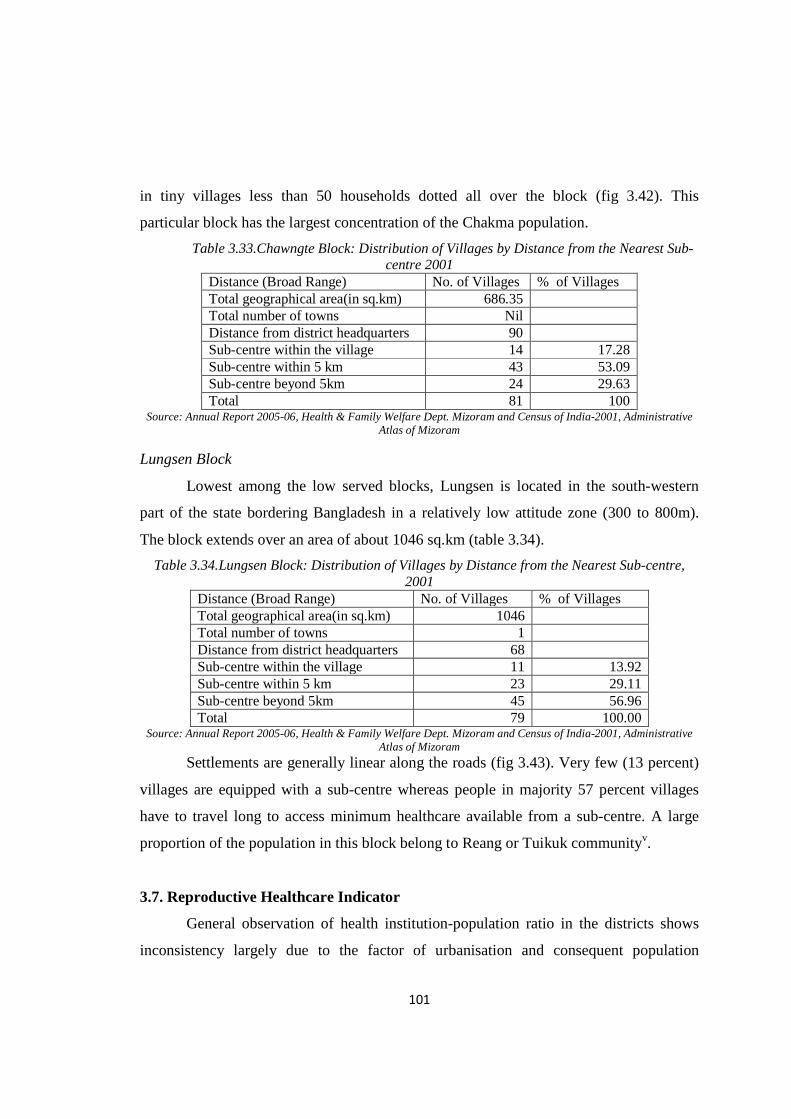
in tiny villages less than 50 households dotted all over the block (fig 3.42). This
particular block has the largest concentration of the Chakma population.
Table 3.33.Chawngte Block: Distribution of Villages by Distance from the Nearest Sub-centre 2001
Distance (Broad Range) No. of Villages % of Villages Total geographical area(in sq.km) 686.35 Total number of towns Nil Distance from district headquarters 90 Sub-centre within the village 14 17.28 Sub-centre within 5 km 43 53.09 Sub-centre beyond 5km 24 29.63 Total 81 100
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
Lungsen Block
Lowest among the low served blocks, Lungsen is located in the south-western
part of the state bordering Bangladesh in a relatively low attitude zone (300 to 800m).
The block extends over an area of about 1046 sq.km (table 3.34).
Table 3.34.Lungsen Block: Distribution of Villages by Distance from the Nearest Sub-centre, 2001
Distance (Broad Range) No. of Villages % of Villages Total geographical area(in sq.km) 1046 Total number of towns 1 Distance from district headquarters 68 Sub-centre within the village 11 13.92 Sub-centre within 5 km 23 29.11 Sub-centre beyond 5km 45 56.96 Total 79 100.00
Source: Annual Report 2005-06, Health & Family Welfare Dept. Mizoram and Census of India-2001, Administrative Atlas of Mizoram
Settlements are generally linear along the roads (fig 3.43). Very few (13 percent)
villages are equipped with a sub-centre whereas people in majority 57 percent villages
have to travel long to access minimum healthcare available from a sub-centre. A large
proportion of the population in this block belong to Reang or Tuikuk communityv.
3.7. Reproductive Healthcare Indicator
General observation of health institution-population ratio in the districts shows
inconsistency largely due to the factor of urbanisation and consequent population
102
concentration. Analysis on the availability of maternity services in the districts of
Mizoram has been made in this section by considering maternal bed-eligible couple
(mother aged 15-49) ratio as an indicator. In order to ensure better health of the mother,
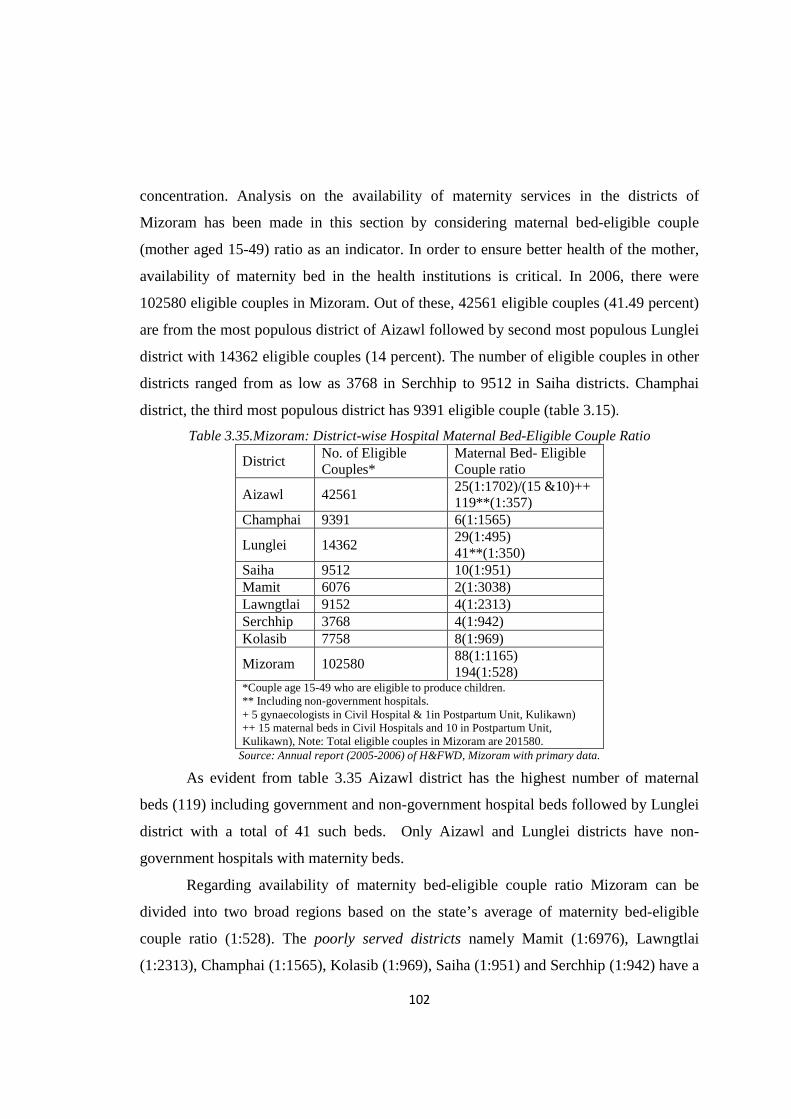
availability of maternity bed in the health institutions is critical. In 2006, there were
102580 eligible couples in Mizoram. Out of these, 42561 eligible couples (41.49 percent)
are from the most populous district of Aizawl followed by second most populous Lunglei
district with 14362 eligible couples (14 percent). The number of eligible couples in other
districts ranged from as low as 3768 in Serchhip to 9512 in Saiha districts. Champhai
district, the third most populous district has 9391 eligible couple (table 3.15).
Table 3.35.Mizoram: District-wise Hospital Maternal Bed-Eligible Couple Ratio
District No. of Eligible Couples*
Maternal Bed- Eligible Couple ratio
Aizawl 42561 25(1:1702)/(15 &10)++ 119**(1:357)
Champhai 9391 6(1:1565)
Lunglei 14362 29(1:495) 41**(1:350)
Saiha 9512 10(1:951) Mamit 6076 2(1:3038) Lawngtlai 9152 4(1:2313) Serchhip 3768 4(1:942) Kolasib 7758 8(1:969)
Mizoram 102580 88(1:1165) 194(1:528)
*Couple age 15-49 who are eligible to produce children. ** Including non-government hospitals. + 5 gynaecologists in Civil Hospital & 1in Postpartum Unit, Kulikawn) ++ 15 maternal beds in Civil Hospitals and 10 in Postpartum Unit, Kulikawn), Note: Total eligible couples in Mizoram are 201580.
Source: Annual report (2005-2006) of H&FWD, Mizoram with primary data.
As evident from table 3.35 Aizawl district has the highest number of maternal
beds (119) including government and non-government hospital beds followed by Lunglei
district with a total of 41 such beds. Only Aizawl and Lunglei districts have non-
government hospitals with maternity beds.
Regarding availability of maternity bed-eligible couple ratio Mizoram can be
divided into two broad regions based on the state’s average of maternity bed-eligible
couple ratio (1:528). The poorly served districts namely Mamit (1:6976), Lawngtlai
(1:2313), Champhai (1:1565), Kolasib (1:969), Saiha (1:951) and Serchhip (1:942) have a
103
ratio more than the state average (1:528). The Well served districts consist of two most
urbanised Aizawl and Lunglei districts with 357 and 350 maternity beds per eligible
couple respectively (fig.3.16).
In hospitals of Mamit district only 2 out of 50 beds are maternity beds while
hospitals in Lawngtlai (30 beds) and Serchhip (50 beds) districts have 4 maternity beds
each. It is important to note that Champhai district hospital facilitated by 70 beds has only
6 maternity beds while Kolasib district hospital with 50 beds has 8 maternity beds. Only
88 maternity beds are available in government hospitals and 106 in non-government
hospitals in Mizoram.
There exists a positive relationship between urbanisation and availability of
maternity beds in Mizoram. Wide disparity in maternity bed- eligible couple ratio across
the districts of Mizoram is a serious concern. As far as availability of maternity bed in the
government hospital is concerned Lunglei is the best served district largely due to
establishment of non-government hospitals. The two urbanised districts have
comparatively longer history as far as healthcare service is concerned.
3.7.1. Gynaecologist- Eligible Couple Ratio
Maternal and infant deaths can be prevented by ensuring high quality maternal
and newborn healthcare facility and that maternal health complications are recognized,
referred, and treated by a skilled healthcare worker (PHR plus, 2003). It is also necessary
to ensure that sufficient number of reproductive healthcare professionals is available in
all institutions.
In 2006, six districts had at least one gynaecologist in the hospitals. Not a single
gynaecologist is available in the southern Lawngtlai district hospital and Saiha has only
one gynaecologist. Except Aizawl and Lunglei, the remaining four districts like Serchhip,
Champhai, Mamit and Kolasib have just one gynaecologist each. The situation for
Aizawl and Lunglei were also unsatisfactory in view of large concentration of eligible
couples in these two districts. This is in spite of the fact that non-government hospitals
contribute gynaecologists to treat reproductive complications. Because of non-
government health institutions, specialist- eligible couple ratio is best served in Aizawl

104
district with 2027 couples depending on one gynaecologist followed by Serchhip district
with 3768 couples per gynaecologist. The eligible couple-specialist ratio in the remaining
districts ranges from 4787 in Lunglei district to 9391 in Champhai district.
Table 3.36.Mizoram: District-wise Gynaecologist-Eligible Couple Ratio, 2006
Name of District No. of Eligible Couples
Gynaecologist-Eligible Couple* ratio
Aizawl 42561 10(1:4256) /(9 & 1)+ 21**(1:2027)
Champhai 9391 1(1:9391)
Lunglei 14362 2(1:7181) 3**(1:4787)
Saiha 9512 0(1:9512) Mamit 6076 1(1:6076) Lawngtlai 9152 0(0:9252) Serchhip 3768 1(1:3768) Kolasib 7758 1(1:7758)
Mizoram 102580 12(1:8548) 24**(1:4274)
*Couple age 15-49 who are eligible to produce children. ** Including non-government hospitals. + 5 gynaecologists in Civil Hospital & 1in Postpartum Unit, Kulikawn) ++ 15 maternal beds in Civil Hospitals and 10 in Postpartum Unit, Kulikawn) Note: Total eligible couples in Mizoram are 201580.
Source: Annual Report (2005-2006) of H&FWD, Mizoram with primary data.
3.8. Concluding Statement
The analysis of availability of healthcare facility across the state at each level of
healthcare establishments can be summarised as follows:
Firstly, the growth of healthcare facilities in the state is extremely slow.
Dispensaries, which started earlier, gradually disappeared in the later years as Primary
health centre and Community health centre took its place. People living in remote rural
areas were provided with simple modern healthcare system like Sub-centre only after
Mizoram attained statehood in 1986. The pattern in the growth of healthcare facilities
reveals a strong urban bias particularly in Aizawl city.
Secondly, growth in reproductive healthcare clearly reflects remarkable
contribution made by early Christian missionaries which germinated with the passage of
time. The present health consciousness and maternity care among the people of the state,
105
particularly mothers owe much to the relentless efforts of the missionaries followed by
the Government.
The functioning of the most district hospitals in the public sector leaves much to
be desired especially in relation to availability, accessibility and quality. The staff
strength, beds strength, equipment supply and service availability and population
coverage are not uniform among all the district hospitals in the Mizoram. Even Aizawl
district which stood first in terms of available health institutions is the worse served when
health institution-population ratio is taken into consideration. This is mainly due to
enormous concentration of population in Aizawl district compared with the remaining
districts.
The analysis at district level yields a different story depending on the parameters.
It is thus difficult to draw a comprehensive and firm conclusion. However, unequal
distribution of population among the districts as well as disparity in the availability of
non-government healthcare facilities across the districts play critical role in this regard. In
other words, urbanisation and efforts made by non-governmental sector in providing
health services, particularly hospitals, is significant in the context of Mizoram.
Two important conclusions can be made from the above analysis on the
availability of health personnel as well as health institutional bed in rural development
blocks. Firstly, mere establishment of health institution is not enough. Availability of
healthcare providers and in-patient bed is extremely important for healthcare seekers.
Secondly, evaluation of population size served by health centre as well as population per
medical practitioner is exceedingly important in the context of Mizoram to realise level
of sufficiency of healthcare facilities.
Assessment of availability of sub-centre infrastructure reveals that Mizoram is
lagging behind the national average wherever spatial factors are taken into consideration
such as average geographical areas covered by sub-centres and average radial distance
covered by sub-centres. The condition of Mizoram is better off than national performance
in terms of population coverage by a sub-centre. This is simply due to sparse population
distribution and low density of population in Mizoram.
106
It is also found that many villages (54.15 percent) in the state are not having any
healthcare unit. There exists glaring disparities in the distribution of sub-centre facility
among the eight districts of Mizoram. The condition in Lawngtlai district displays the
most unfortunate situation as more than 80 percent of the villages are bereft of minimum
healthcare facility.
Discussion on location of villages from the nearest health centre reveals there are
extreme variations across the districts of Mizoram. Nearly 19 percent (18.29 percent)
villages in the state are not having any healthcare unit, located far beyond 5 km from the
nearest health centre and as many as 35.73 percent villages have health centre within 5
km radius from the village. It is interesting to note that there exist regional differences
regarding availability of health centre at the village level. Districts located in the
Northeastern part of the state are generally well served compared to districts located in
the Southwestern part of the state. This Northeast-Southwest divide appears to be
important for further studies as many developmental factors can be involved.
Analysis reveals that there exists glaring disparities in the availability of
reproductive healthcare facilities across the districts in Mizoram. This may in turn have
negative effect among the reproductive age groups in the state. There is a wide disparity
in maternity bed- eligible couple ratio as well as gynaecologist eligible couple ratio
across the districts of Mizoram. The two southernmost districts of Lawngtlai and Saiha
are in extreme danger as far as gynaecologist-eligible couple ratio is concerned while the
two most urbanised districts of Aizawl and Lunglei are better off than the remaining
district in this regard. Increase of maternity services in Aizawl and Lunglei districts, is
largely due to establishment of non-government hospitals in these two most urbanised
districts.

107
Notes i J.M Lloyd, “On every High Hills” p.41 quoted in C.R Nag’s(1993) The Mizo Society in Transition,Vikas Publishing House, New Delhi, ..155 ii Field survey and personal interviews reveals that some doctors are very reluctance to reside in rural areas and with the supports of relatives and politician they can stay in urban areas, particularly in Aizawl city. It was also known from some doctors that certain villages, especially in the PHC level, villagers are not co-operative and makes unnecessary complaints to the higher authority, which compels some doctors to leave the village. iii According to national norms Primary Health Centre(PHC) should be facilitated with one each of the following healthcare providers such as-Medical Officer, Pharmacist, Nurse Mid-wife (Staff Nurse), Health Worker (Female)/ANM ,Health , Health Assistant Male), Health Assistant (Female)/LHV, Upper Division Clerk, Lower Division Clerk, Laboratory Technician, Driver (Subject to availability of Vehicle)and four Class IV. Community Health Centre (CHC) should have the following staffs, such as- four Medical Officer (Either qualified or specially trained to work as Surgeon, Obstetrician, Physician and Pediatrician. One of the existing Medical Officers similarly should be either qualified or specially trained in Public Health),7 Nurse Mid– Wife(staff Nurse) 1 Dresser , 1 Pharmacist/Compounder , 1 Laboratory Technician,1 Radiographer, 2 Ward Boys,1 Dhobi,3 Sweepers, 1 Mali,1 Chowkidar, Aya and 1Peon. iv Urban Health Centre (UHC) is mainly maternity cares equipped with 2-3 beds, one doctor and other staffs usually located in a distance far from other hospitals within urban areas. For example there are 4 UHC in Aizawl city such as-ITI, Hlimen, Chawlhhmun and Ramhlun mostly located far from the main centre of the city where hospital facilities are available. Likewise, there is one UHC in Hrangchal under the jurisdiction of Lunglei town, which is also far from main centre of the city where hospital facilities are located. v Reang, locally called as ‘Tuikuk’ community are not belong to Mizoram but settled sometimes back in this part of the state. Majority of this community settled in Tripura. Now they claim that to be settled in Mizoram and talks has been going on between state government and leaders of Tuikuk community till date.
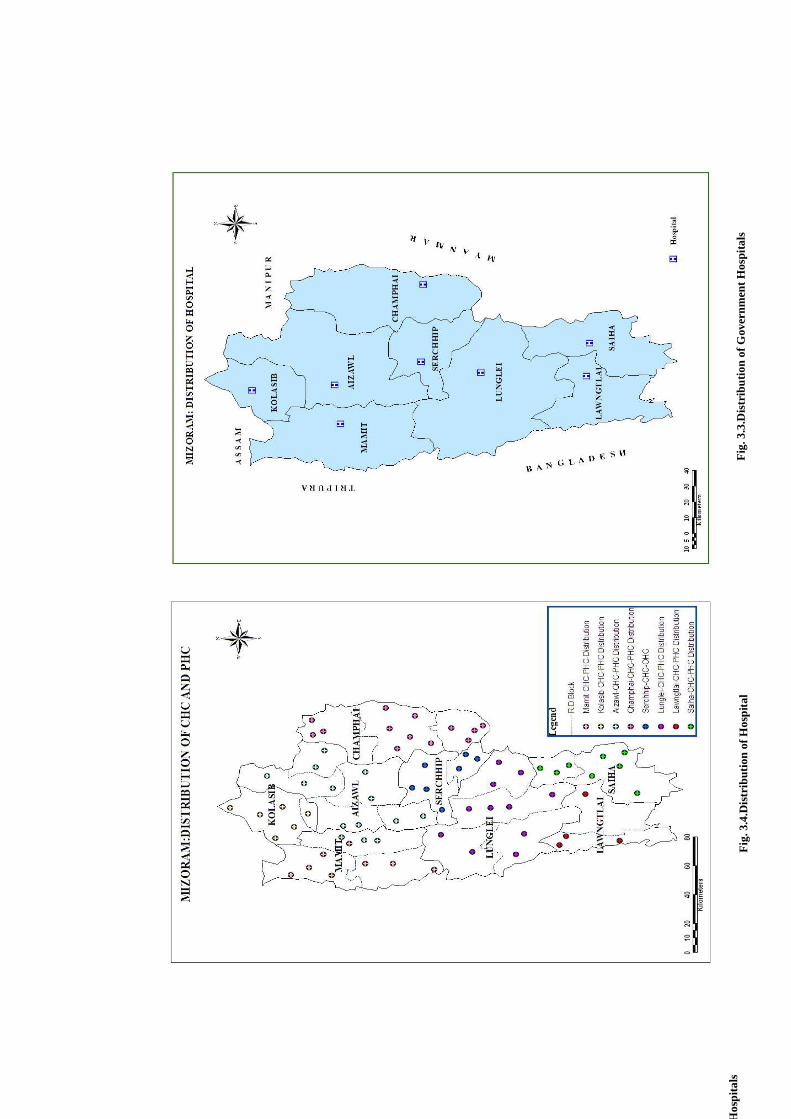
Fig
. 3.4
.Dis
trib
utio
n of
Hos
pita
l
Fig
. 3.4
Dis
trib
utio
ns o
f PH
C/C
HC
Fig
. 3.3
.Dis
trib
utio
n of
Gov
ernm
ent H
ospi
tals
D
istr
ibut
ion
of G
over
nmen
t Hos
pita
ls
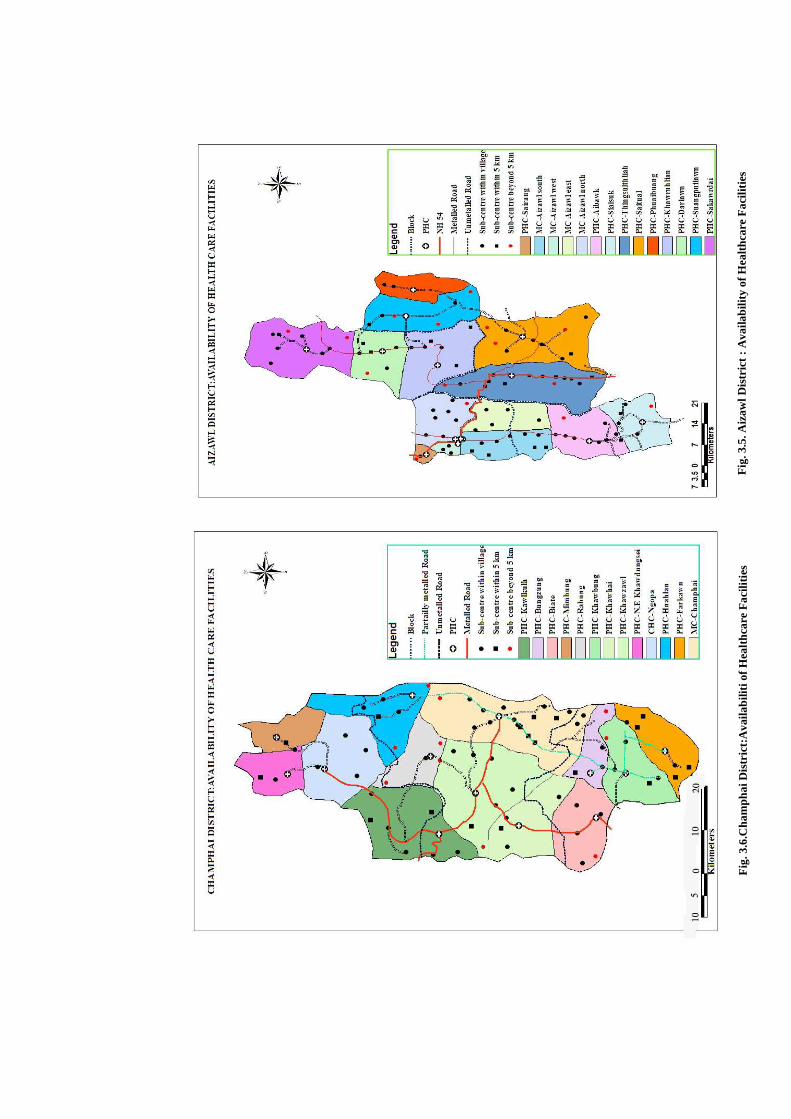
Fig
. 3.5
. Aiz
awl D
istr
ict
: A
vaila
bilit
y of
Hea
lthc
are
Fac
iliti
es
Fig
. 3.6
.Cha
mph
ai D
istr
ict:
Ava
ilabi
liti o
f Hea
lthc
are
Fac
iliti
es
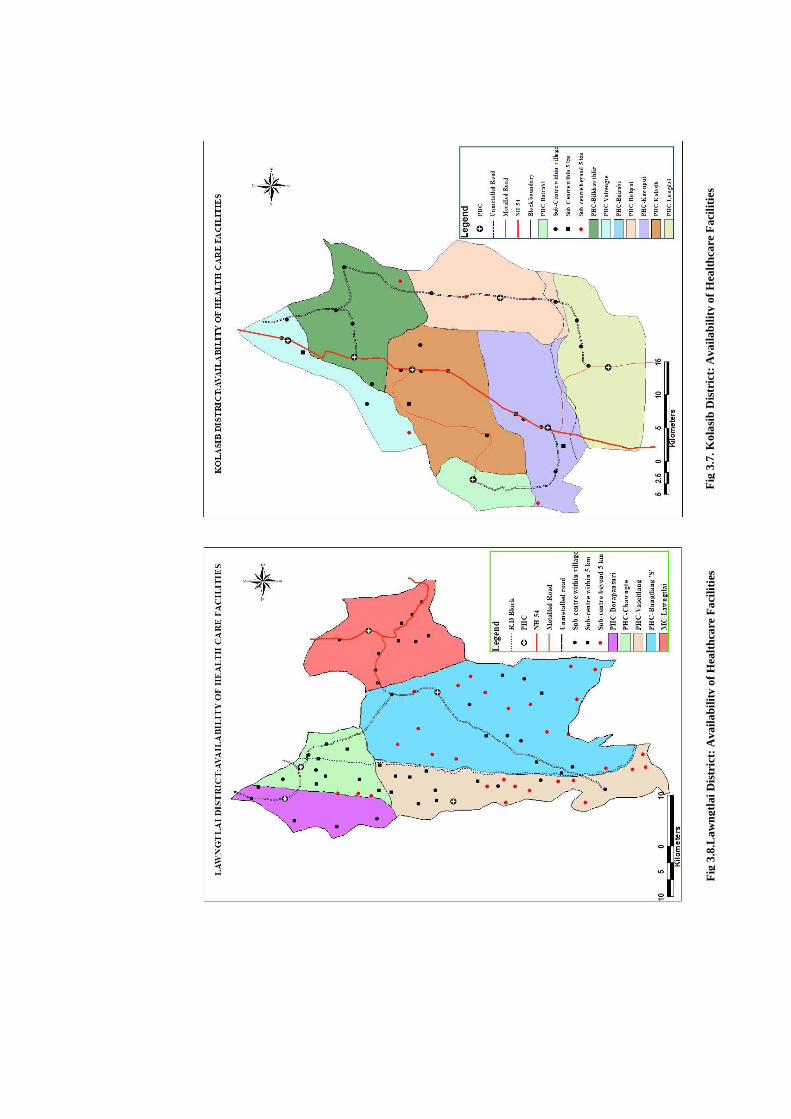
Fig
3.7
. Kol
asib
Dis
tric
t: A
vaila
bilit
y of
Hea
lthc
are
Fac
iliti
es
Fig
3.8
.Law
ngtl
ai D
istr
ict:
Ava
ilabi
lity
of H
ealt
hcar
e F
acili
ties
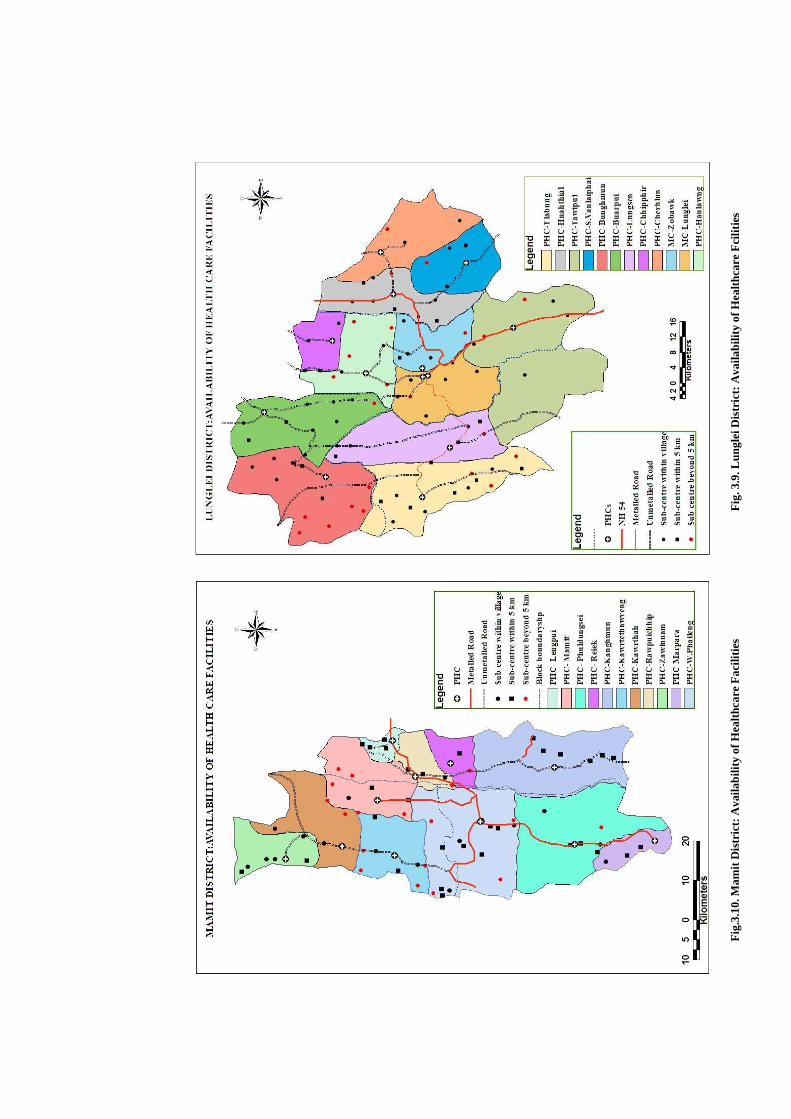
Fig
. 3.1
2.Se
rchh
ip D
istr
ict:
Ava
ilabi
lity
of H
ealt
hcar
e F
acili
ties
Fig
.3.1
0. M
amit
Dis
tric
t: A
vaila
bilit
y of
Hea
lthc
are
Fac
iliti
es
Fig
. 3.9
. Lun
glei
Dis
tric
t: A
vaila
bilit
y of
Hea
lthc
are
Fci
litie
s
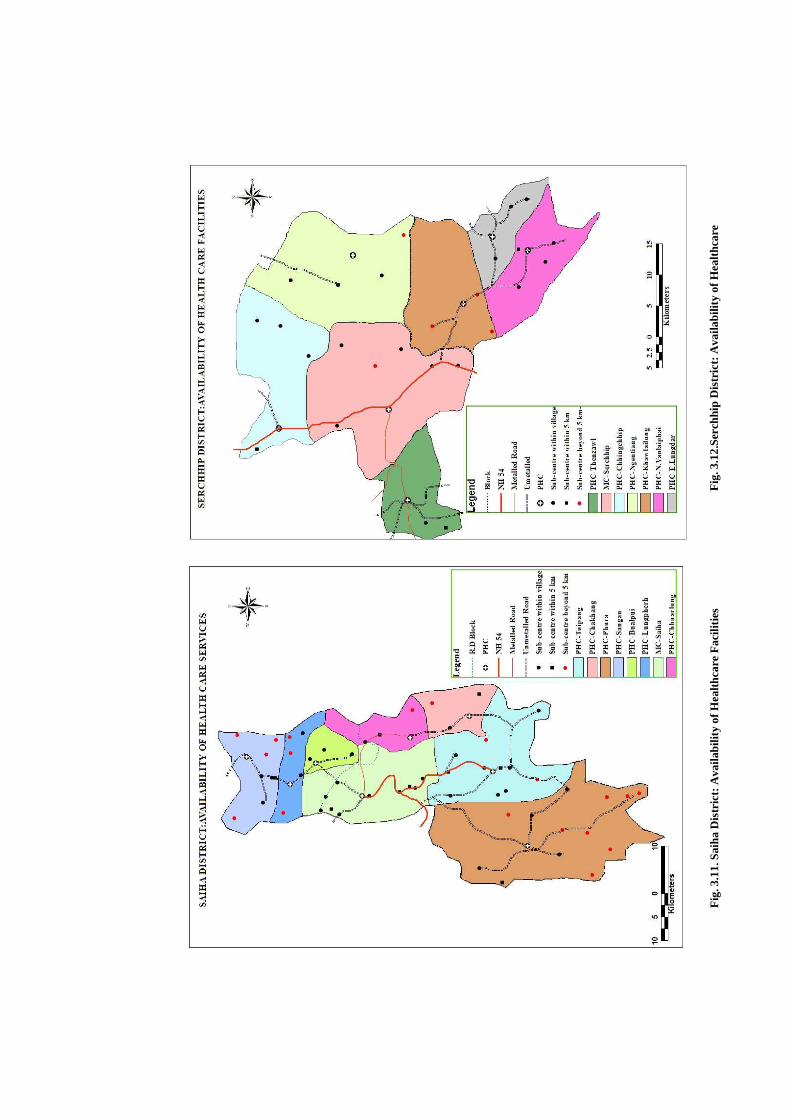
Fig
. 3.1
1. S
aiha
Dis
tric
t: A
vaila
bilit
y of
Hea
lthc
are
Fac
iliti
es
Fig
. 3.1
2.Se
rchh
ip D
istr
ict:
Ava
ilabi
lity
of H
ealt
hcar
e F
acili
ties
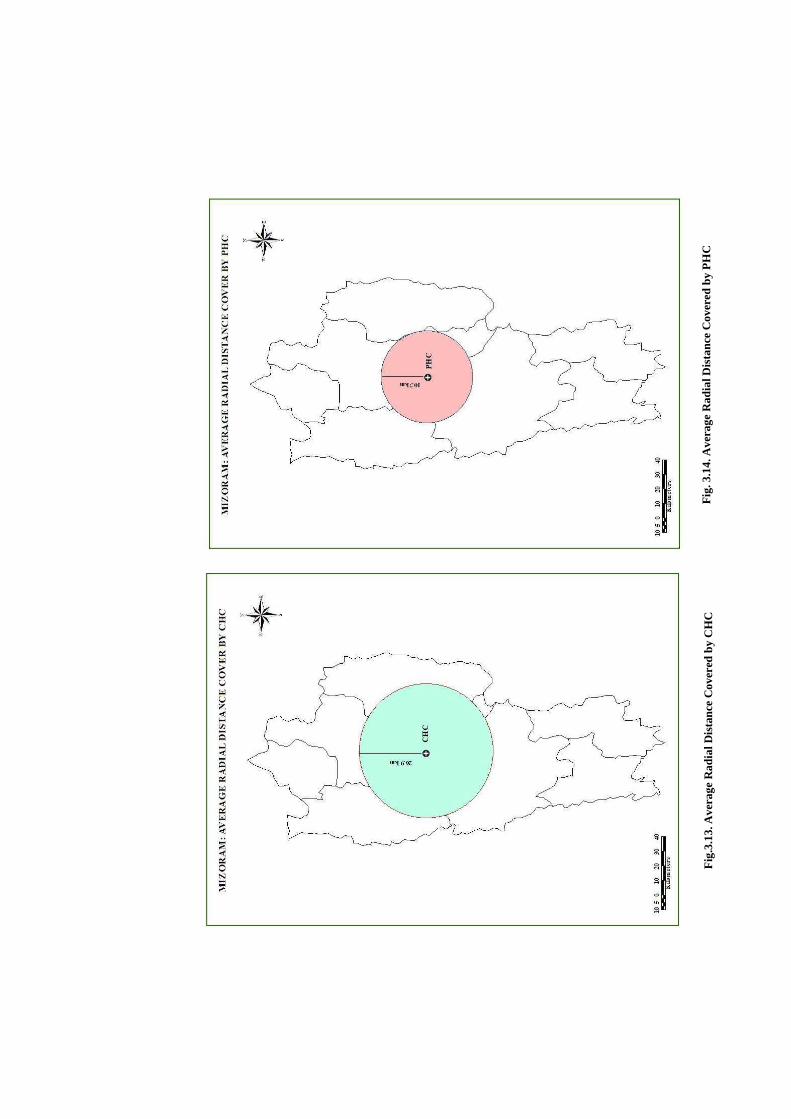
Fig
.3.1
3. A
vera
ge R
adia
l Dis
tanc
e C
over
ed b
y C
HC
F
ig. 3
.14.
Ave
rage
Rad
ial D
ista
nce
Cov
ered
by
PH
C
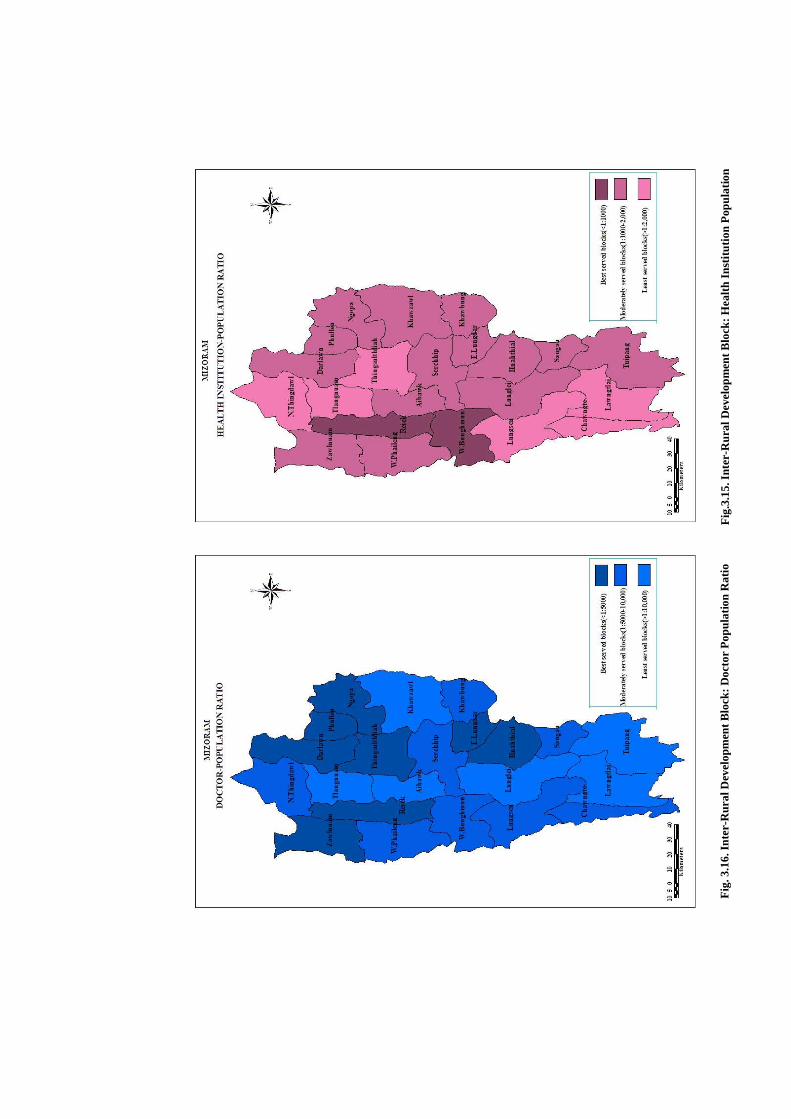
Fig
.3.1
5. I
nter
-Rur
al D
evel
opm
ent B
lock
: Hea
lth
Inst
itut
ion
Pop
ulat
ion
Fig
. 3.1
6. I
nter
-Rur
al D
evel
opm
ent B
lock
: Doc
tor
Pop
ulat
ion
Rat
io

Fig
. 3.1
7. I
nter
-RD
Blo
ck: H
ealt
h In
stit
utio
n B
ed-P
opul
atio
n R
atio
Fig
.3.1
8. R
D B
lock
s: A
vaila
bilit
y of
Hea
lthc
are
Fac
iliti
es
b
ased
on
the
perf
orm
ance
of a
ll th
ree
Indi
cato
rs
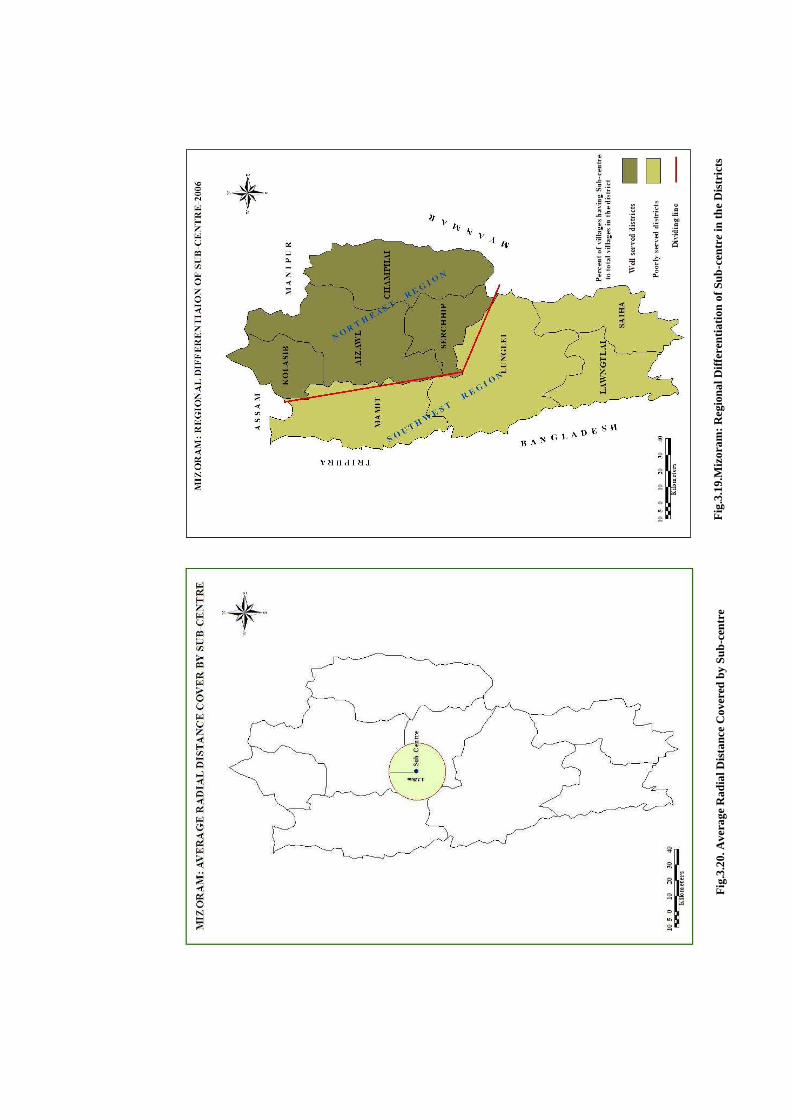
Fig
.3.1
9.M
izor
am: R
egio
nal D
iffe
rent
iati
on o
f Sub
-cen
tre
in th
e D
istr
icts
Fig
.3.2
0. A
vera
ge R
adia
l Dis
tanc
e C
over
ed b
y Su
b-ce
ntre

Fig. 3.21.Availability of Sub-centre in the Villages
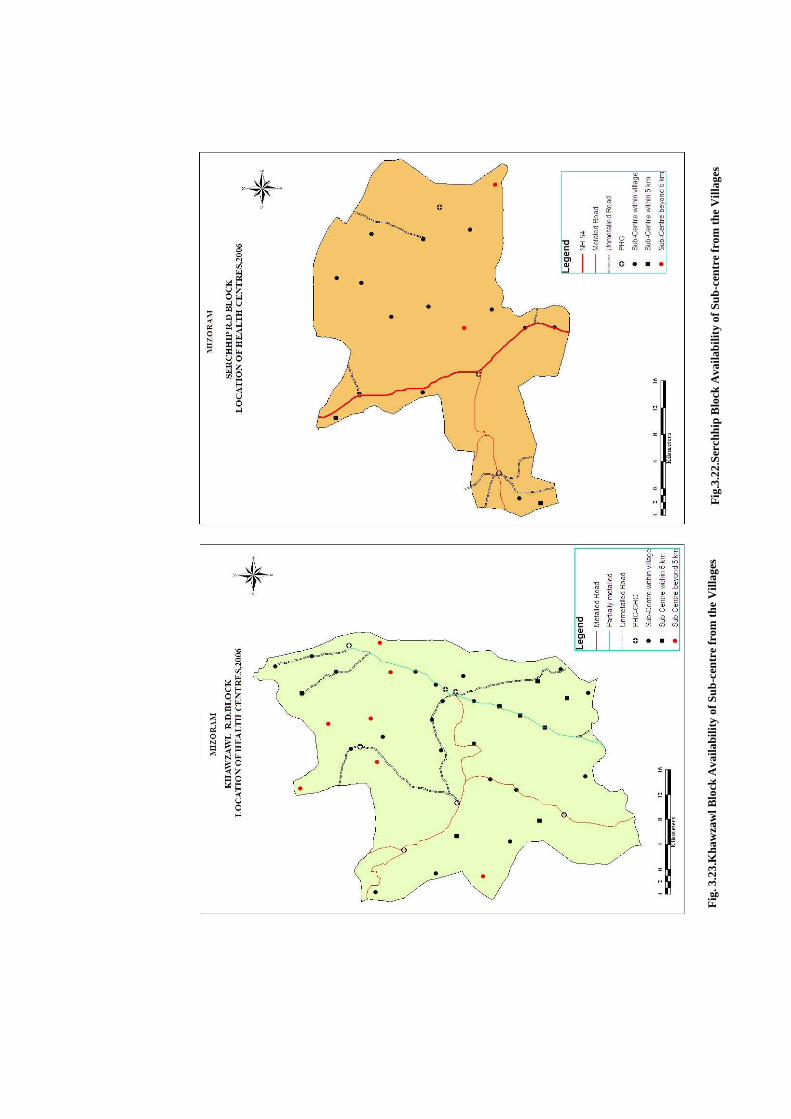
Fig
.3.2
2.Se
rchh
ip B
lock
Ava
ilabi
lity
of S
ub-c
entr
e fr
om th
e V
illag
es
Fig
. 3.2
3.K
haw
zaw
l Blo
ck A
vaila
bilit
y of
Sub
-cen
tre
from
the
Vill
ages
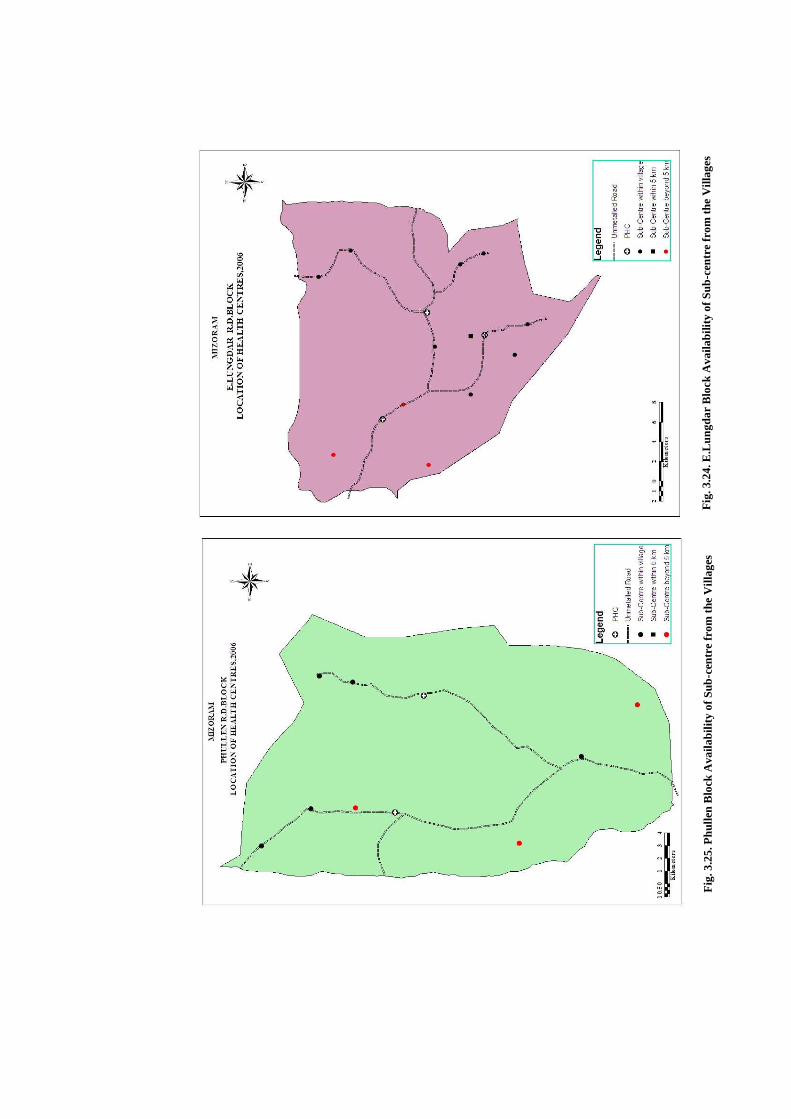
Fig
. 3.2
4. E
.Lun
gdar
Blo
ck A
vaila
bilit
y of
Sub
-cen
tre
from
the
Vill
ages
F
ig. 3
.25.
Phu
llen
Blo
ck A
vaila
bilit
y of
Sub
-cen
tre
from
the
Vill
ages

Fig
. 3.2
6. N
gopa
Blo
ck A
vaila
bilit
y of
Sub
-cen
tre
from
the
Vill
ages
Fig
ure
3.27
. San
gau
Blo
ck A
vaila
bilit
y of
Sub
-cen
tre
from
the
Vill
ages
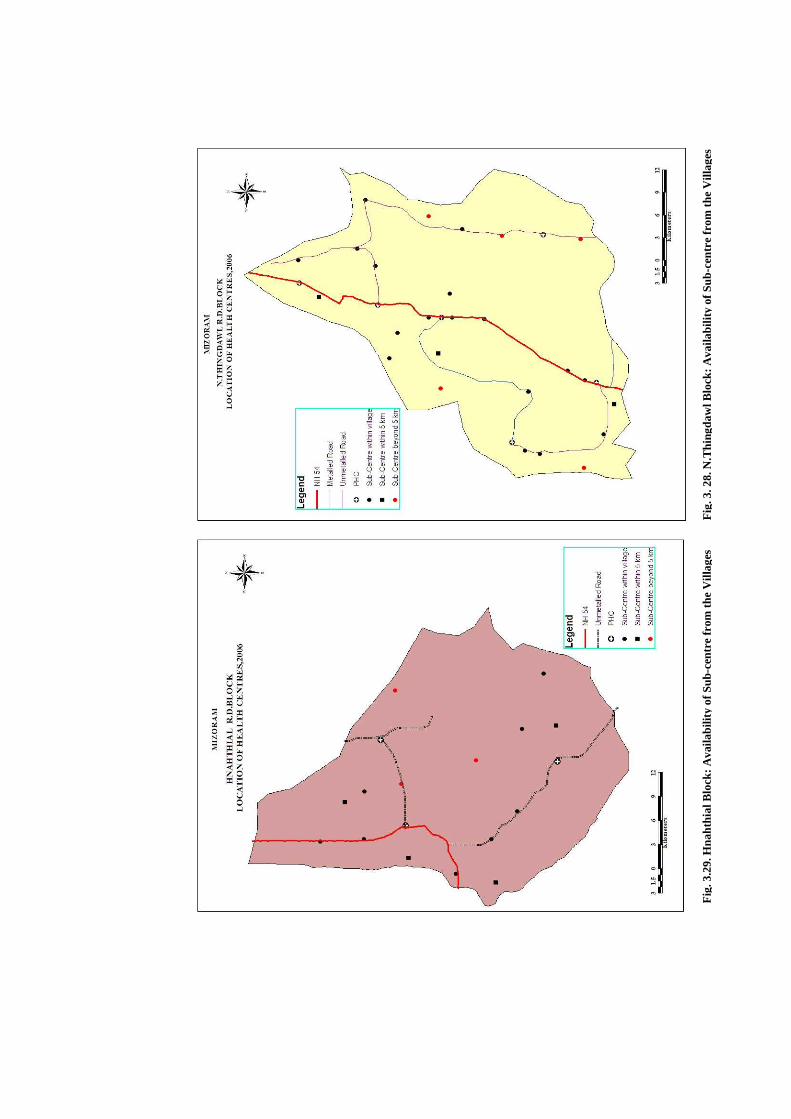
Fig
. 3. 2
8. N
.Thi
ngda
wl B
lock
: Ava
ilabi
lity
of S
ub-c
entr
e fr
om t
he V
illag
es
Fig
. 3.2
9. H
naht
hial
Blo
ck: A
vaila
bilit
y of
Sub
-cen
tre
from
the
Vill
ages
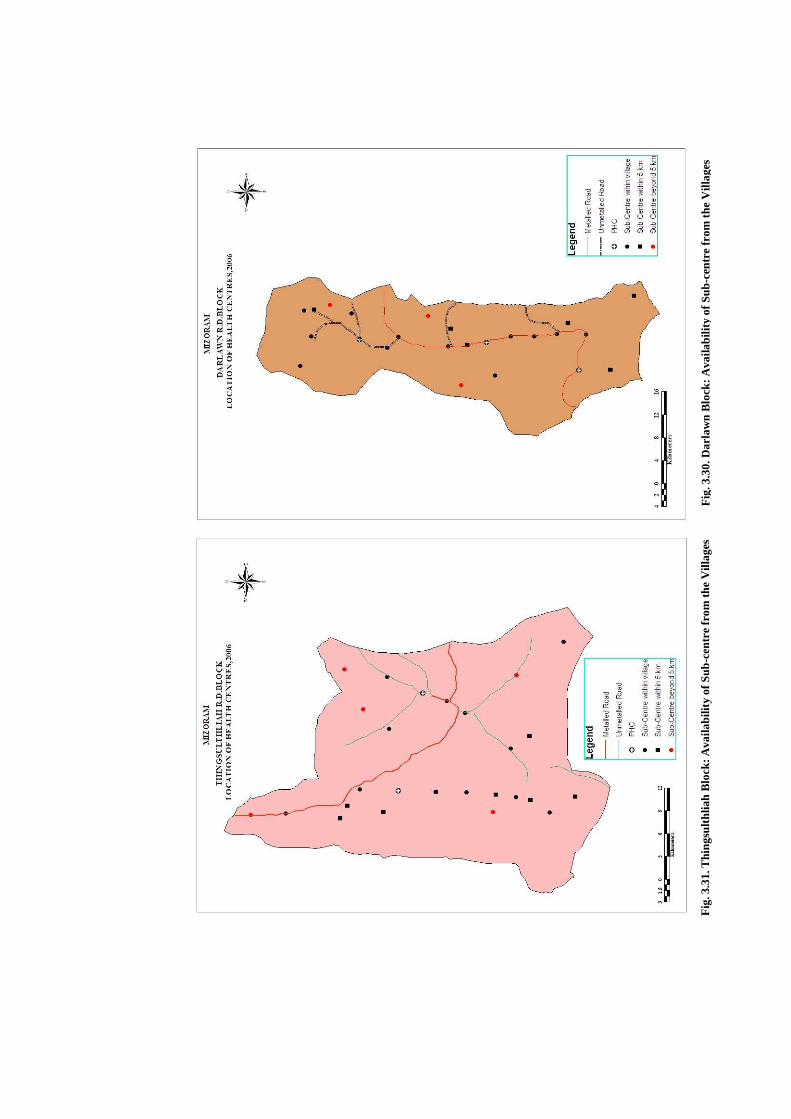
Fig
. 3.3
0. D
arla
wn
Blo
ck: A
vaila
bilit
y of
Sub
-cen
tre
from
the
Vill
ages
F
ig. 3
.31.
Thi
ngsu
lthl
iah
Blo
ck: A
vaila
bilit
y of
Sub
-cen
tre
from
the
Vill
ages
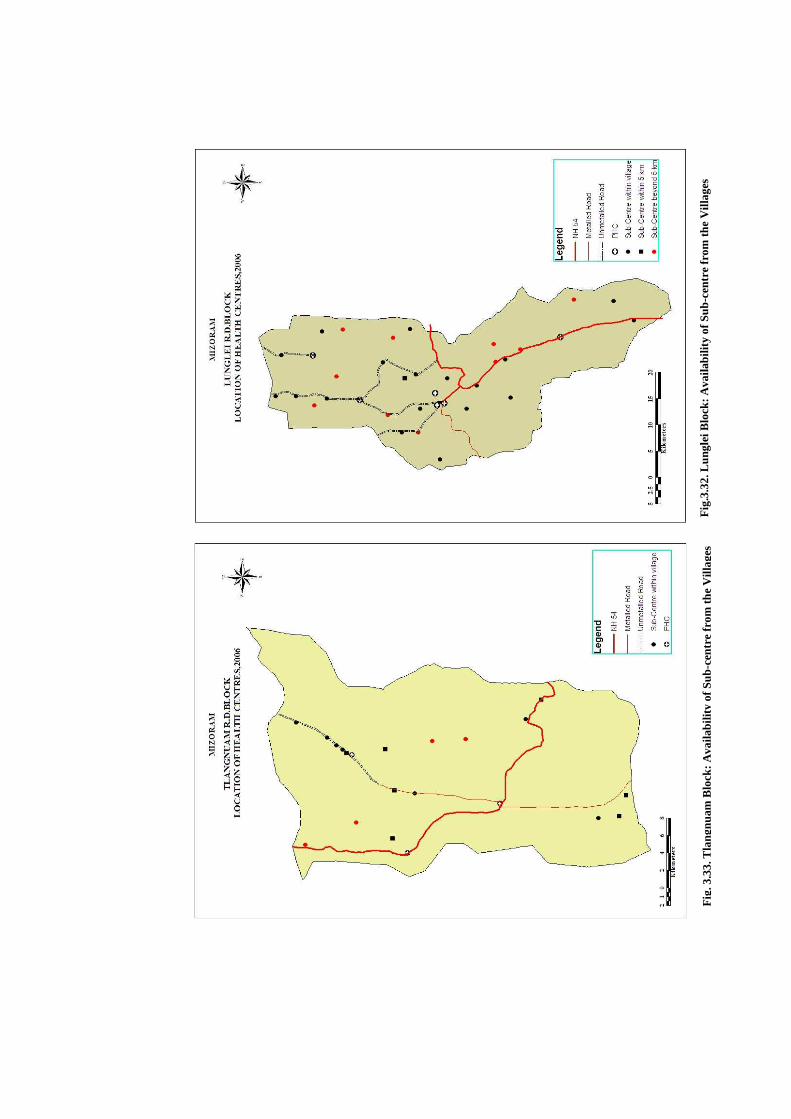
Fig
.3.3
2. L
ungl
ei B
lock
: Ava
ilabi
lity
of S
ub-c
entr
e fr
om th
e V
illag
es
Fig
. 3.3
3. T
lang
nuam
Blo
ck: A
vaila
bilit
y of
Sub
-cen
tre
from
the
Vill
ages
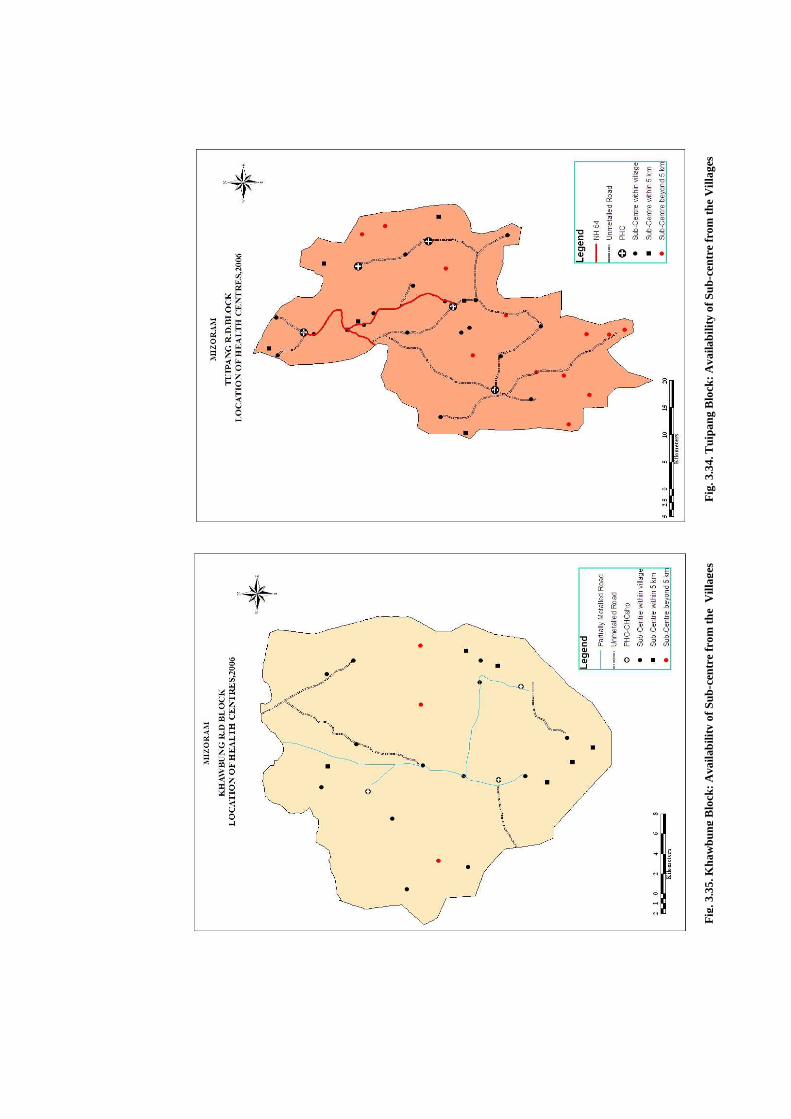
Fig
. 3.3
4. T
uipa
ng B
lock
: Ava
ilabi
lity
of S
ub-c
entr
e fr
om th
e V
illag
es
Flo
ck: A
vaila
bilit
y of
Sub
-cen
tre
from
the
Vill
ages
Fig
. 3.3
5. K
haw
bung
Blo
ck: A
vaila
bilit
y of
Sub
-cen
tre
from
the
Vill
ages
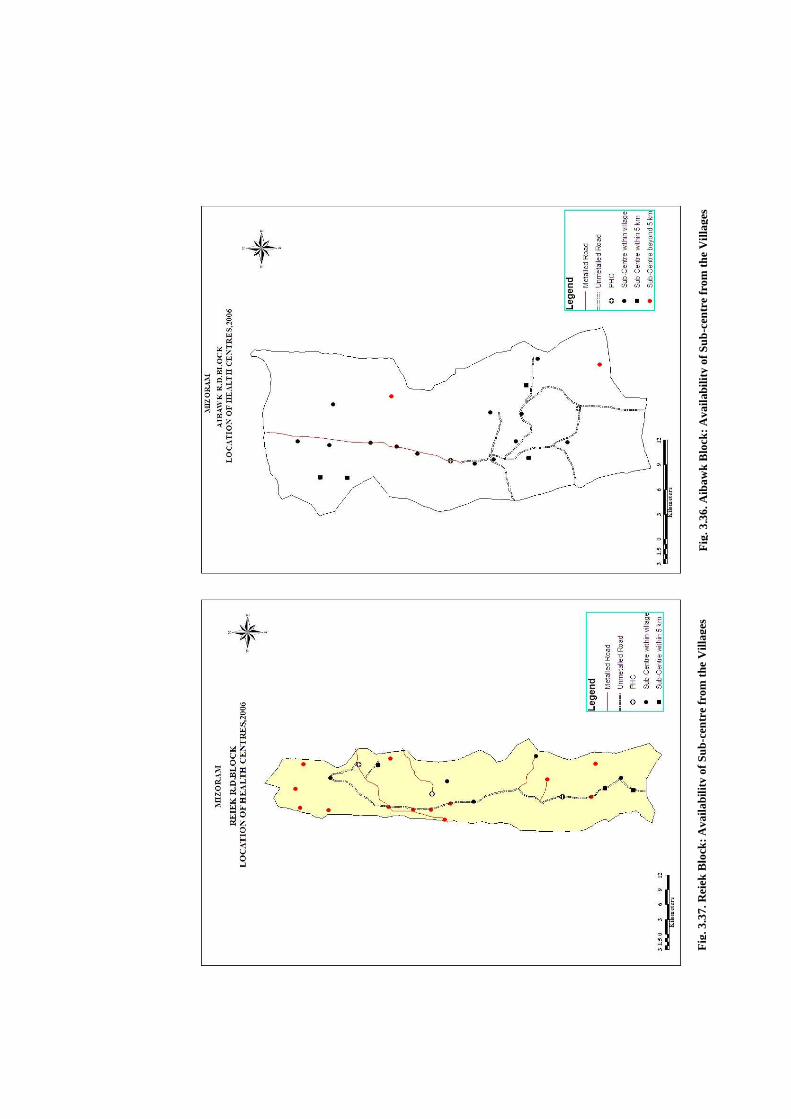
Fig
. 3.3
7. R
eiek
Blo
ck: A
vaila
bilit
y of
Sub
-cen
tre
from
the
Vill
ages
F
ig. 3
.36.
Aib
awk
Blo
ck: A
vaila
bilit
y of
Sub
-cen
tre
from
the
Vill
ages
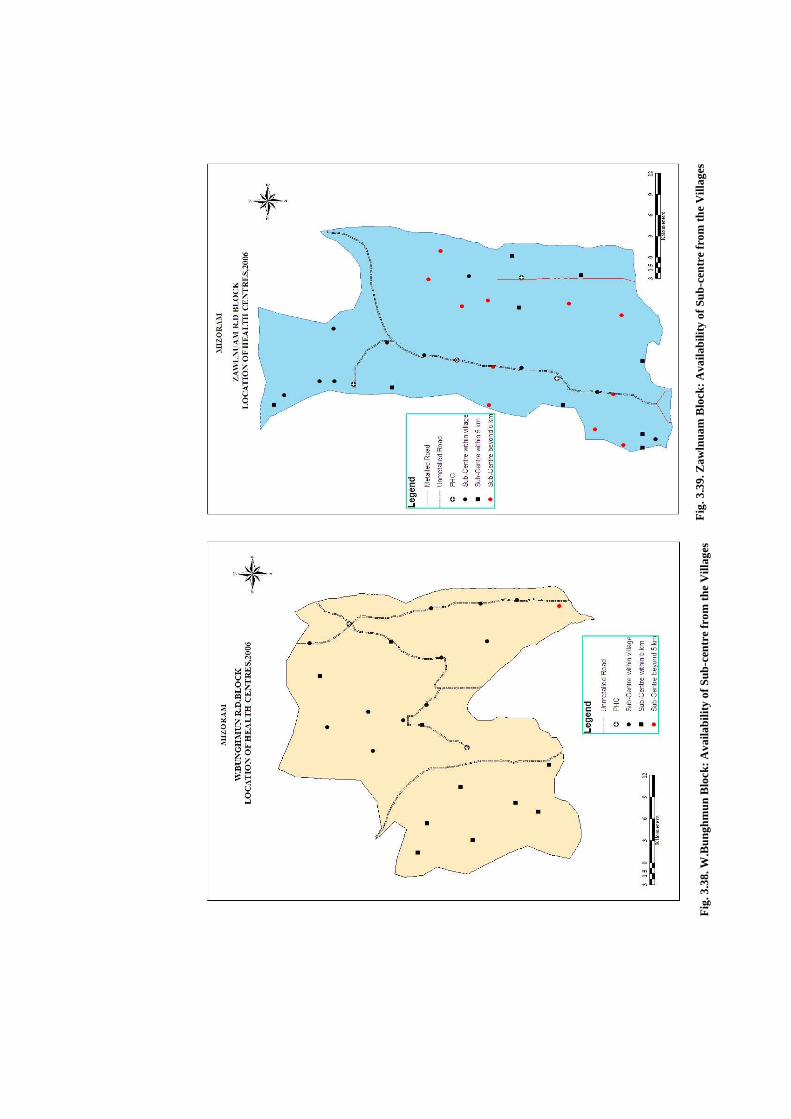
Fig
. 3.3
9. Z
awln
uam
Blo
ck: A
vaila
bilit
y of
Sub
-cen
tre
from
the
Vill
ages
Fig
. 3.3
8. W
.Bun
ghm
un B
lock
: Ava
ilabi
lity
of S
ub-c
entr
e fr
om th
e V
illag
es

Fig
. 3.4
0. L
awng
tlai
Blo
ck: A
vaila
bilit
y of
Sub
-cen
tre
from
the
Vill
ages
F
ig. 3
.41.
W.P
haile
ng B
lock
: Ava
ilabi
lity
of S
ub-c
entr
e fr
om th
e V
illag
es
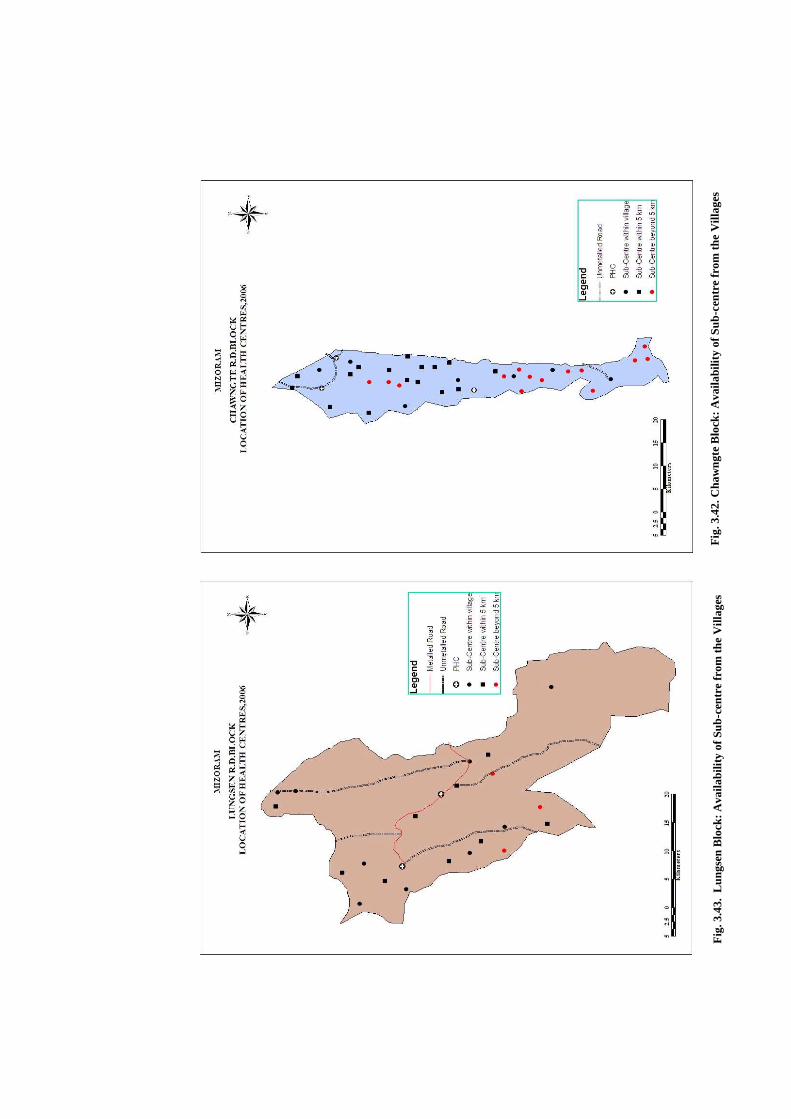
Fig
. 3.4
3. L
ungs
en B
lock
: Ava
ilabi
lity
of S
ub-c
entr
e fr
om th
e V
illag
es
Fig
. 3.4
2. C
haw
ngte
Blo
ck: A
vaila
bilit
y of
Sub
-cen
tre
from
the
Vill
ages
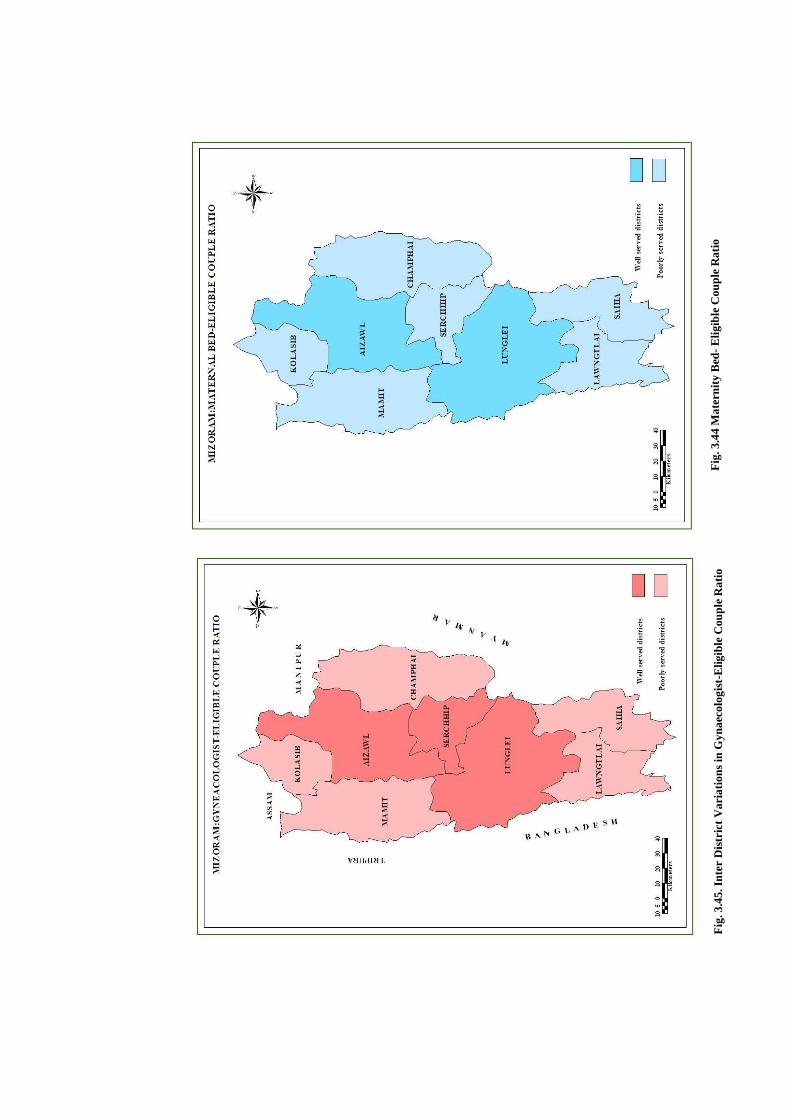
Fig
. 3.4
5. I
nter
Dis
tric
t V
aria
tion
s in
Gyn
aeco
logi
st-E
ligib
le C
oupl
e R
atio
F
ig. 3
.44
Mat
erni
ty B
ed- E
ligib
le C
oupl
e R
atio