charcot joint / neuropathic joint
TRANSCRIPT
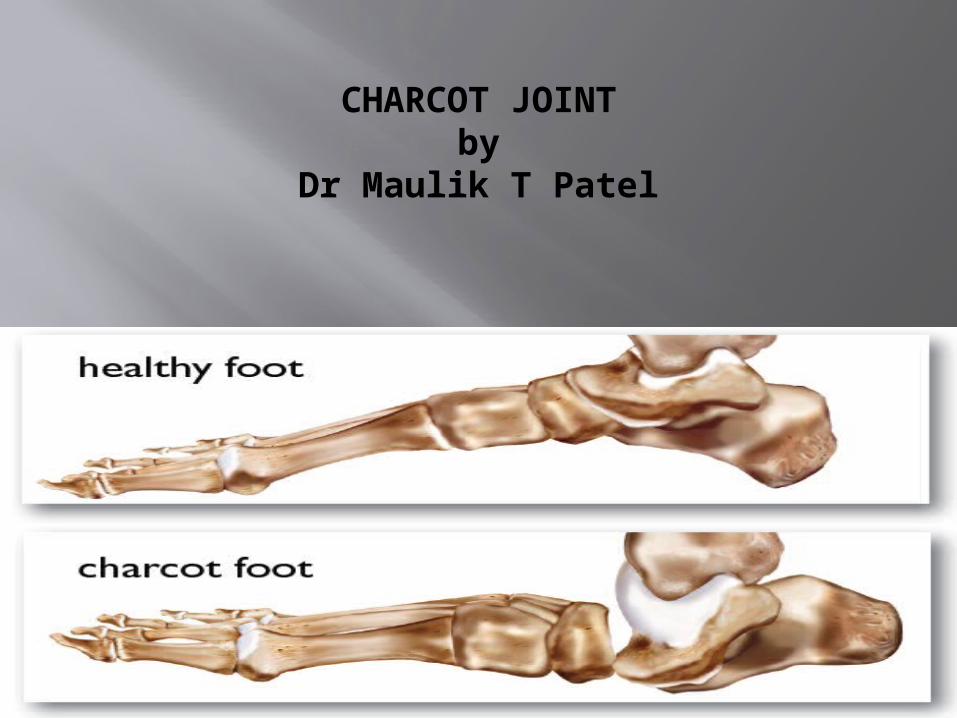
CHARCOT JOINTby
Dr Maulik T Patel
In 1868, Jean-Martin Charcot gave the first detailed description of the neuropathic aspect of this disease; hence, the condition is named after him.
Progressive destructive disease of joint.
Painless arthropathy with dislocation, fracture, debilited deformities.
Frequently misdiagnosed.

Most commonly involve joints of lower limb.
Any condition that causes sensory or autonomic neuropathy can lead to a Charcot joint
Diabetes is considered to be the most common cause of Charcot arthropathy.
Prevalence is 0.5%.
Bilateral disease in < 10%

Pathophysiology
NEUROTRAUMATIC THEORY; An unperceived trauma or injury to an
insensate joint.
NEUROVASCULAR THEORY: autonomic neuropathy increase
vascularity mismatch in destruction & synthesis
Genetics molecular biology RANK/RANKL/OPG triad pathway is thought to be
involved

Associated conditions shoulder syringomyelia
most common etiology of neuropathic arthropathy of the upper extremity
25% of these patients develop a neuropathic joint Mono articular (shoulder > elbow)
Hansen's disease (leprosy) second most common cause of upper extremity
neuropathic arthropathy

syphilis usually affects the knee can be poly articular
diabetes most common cause of foot and ankle neuropathic
joints
Arnold- Chiari malformation cervical spondylosis adhesive arachnoiditis and TB arachnoiditis posttraumatic syringomyelia alcoholism
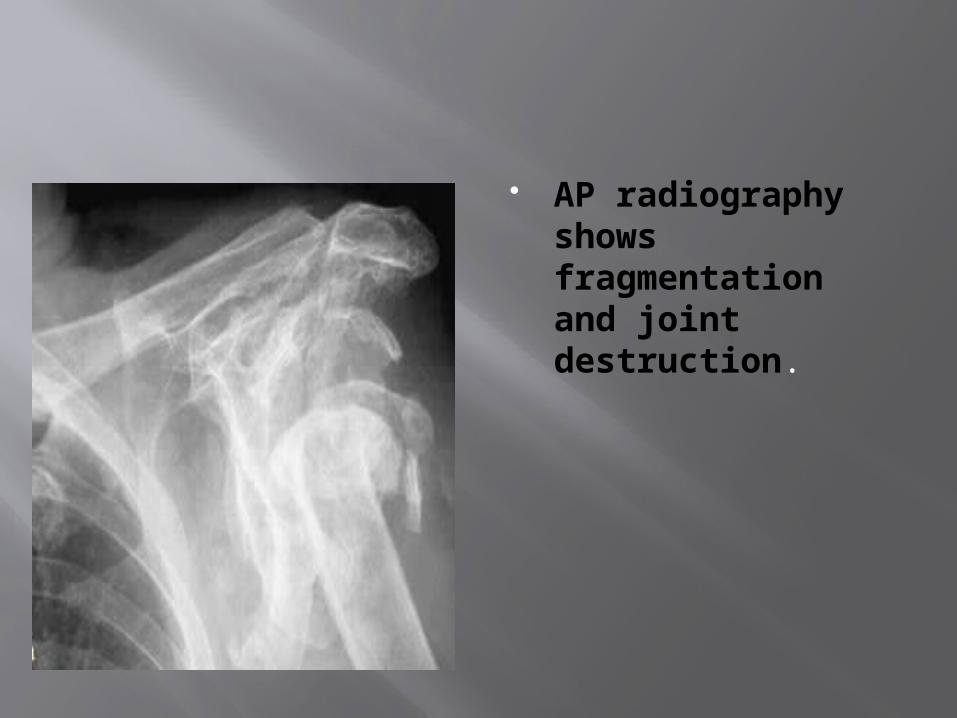
AP radiography shows fragmentation and joint destruction.

AP radiograph shows joint destruction and dislocation.

Elbow
syringomyelia syphilis congenital insensitivity to pain diabetes Charcot-Marie-Tooth

AP radiograph shows joint destruction and heterotrophic ossificans.

X rays showing joint destruction and dislocation

X rays shows joint destruction and new bone formation

Classification Eichenholtz Classification
Stage 0 • Joint edema • Radiographs are negative • Bone scan may be positive in all stages
Stage 1 • Joint edema • Radiographs show osseous fragmentation with joint dislocation
Stage 2 • Decreased local edema • Radiographs show coalescence of fragments and absorption of fine bone debris
Stage 3 • No local edema • Radiographs show consolidation and remodeling of fracture fragments
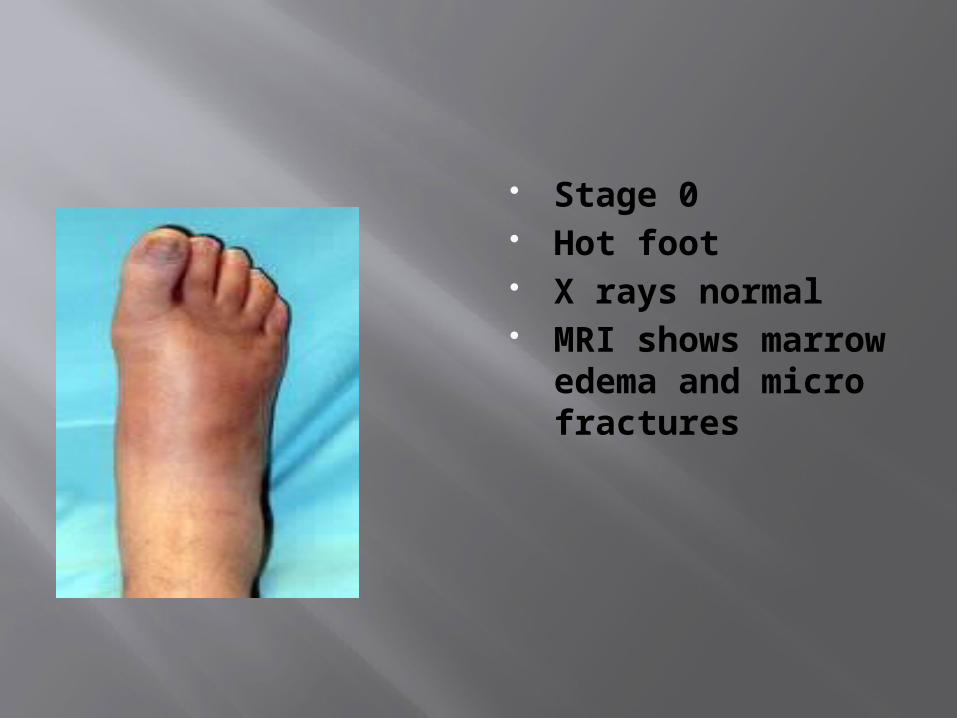
Stage 0 Hot foot X rays normal MRI shows
marrow edema and micro fractures

Stage 1 (Hydrarthrosis)
Fragmentation Bone resorption Fracture dislocation

Stage 2 ( Atrophy)
Coalescence Sclerosis Fracture healing Debris resorption
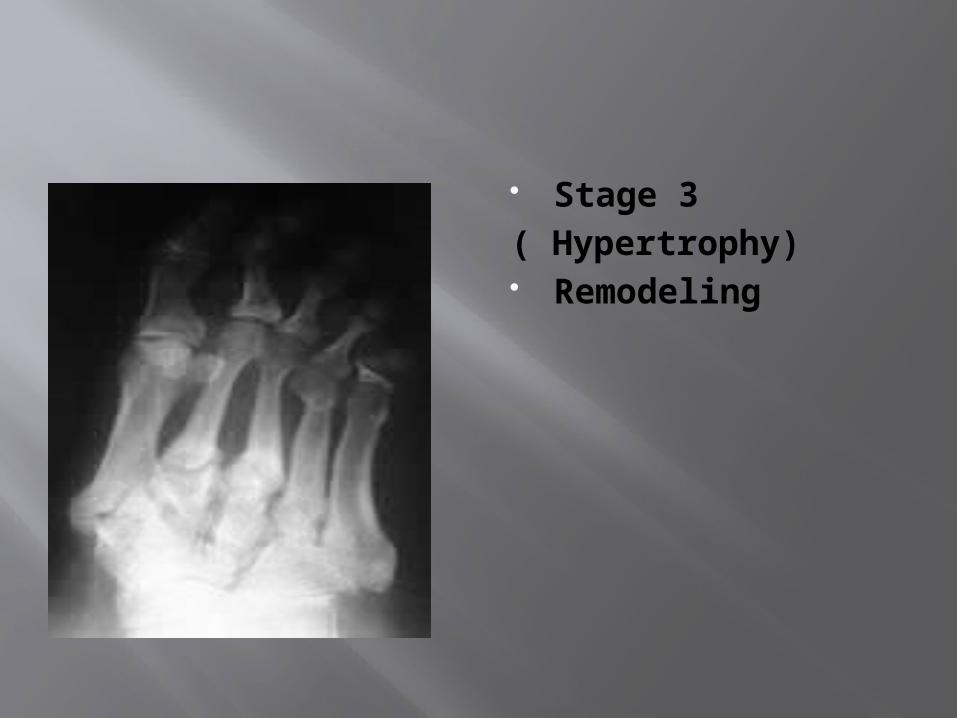
Stage 3( Hypertrophy) Remodeling
Presentation Symptoms swollen shoulder or elbow 50% have pain, 50% are painless loss of function
Physical exam inspection
swollen, warm, erythematous joint mimics infection
motion joint may be mechanically unstable loss of active motion, but passive motion is maintained
neurovascular a neurologic evaluation is essential

Imaging Radiographs recommended views
standard views of affected joint AP and scapula Y of the shoulder AP and lateral of the elbow AP and lateral of foot and ankle
findings early changes
degenerative changes may mimic osteoarthritis late changes
obliteration of joint space fragmentation of both articular surfaces of a joint leading
to subluxation or dislocation scattered "chunks" of bone in fibrous tissue joint distention by fluid surrounding soft tissue edema heterotopic ossification fracture

MRI indications
MRI of cervical spine to rule out syrinx when neuropathic shoulder arthropathy is present
Bone scan technetium bone scan
findings may be positive (hot) for neuropathic joints and
osteomyelitis indium WBC scan
findings will be negative (cold) for neuropathic joints and positive
(hot) for osteomyelitis useful to differentiate from osteomyelitis

Studies Labs
ESR and WBC can be elevated making it difficult to differentiate from osteomyelitis
Histology synovial hypertrophy detritic synovitis (cartilage and bone distributed in
synovium)
Differential diagnosis :
Osteomyelitis/septic joint difficult to distinguish from osteomyelitis based on
radiographs and physical exam common findings in both conditions
swelling, warmth elevated WBC and ESR technetium bone scan is "hot"
unique to Charcot joint disease indium leukocyte scan will be "cold" (negative)
will be "hot" (positive) for osteomyelitis
Treatment Non operative
rest, elevation, protected immobilization with a sling, and restriction of activity indications
neuropathic shoulder joint functional bracing
indications neuropathic elbow joint
technique should allow flexion-extension, but neutralizes varus-
valgus stresses

Operative
Arthrodesis do not attempt during acute inflammatory stage
(Eichenholtz 0-2) because of continued bone erosion only perform during quiescent stage (Eichenholtz 3)
requires long periods of immobilization
Total joint replacement indications
Charcot joint is a contraindication to total joint replacement due to poor bone stock, prosthetic loosening, instability,
and soft-tissue compromise
An ounce of prevention is worth a pound of cure.”
– Benjamin Franklin


