checkpoint inhibitors in sclc - oncologypro.esmo.org · • neuroendocrine origin •
TRANSCRIPT

Luis Paz-Ares
Hospital Universitario Doce de Octubre,Madrid, Spain
Checkpoint Inhibitorsin SCLC

• Neuroendocrine origin
• <15% of all lung cancers, mostly diagnosed in smokers
• Early spread (stage IV at diagnosis 70%) and short doubling time
• High chemosensitivity but rapid emergence of resistance
• Autoinmunity – paraneoplastic syndromes
• 5 yr survival rate 6%;
• LS-SCLC median OS -15-20 months
• ES-SCLC median OS – 8-13 months
First line Treatment Options1. Platinum + etoposide/irinotecan2. Clinical trial
Second line Treatment Options1. Topoisomerase 1 inhibitor2. Clinical trial 3. Palliative care
Clinical Characteristics of SCLC

0%
20%
40%
60%
80%
100%
0 5 10 15Years After Enrollment
IAIBIIAIIBIIIAIIIBIV
Deaths / N17 / 2514 / 198 / 15
84 / 101332 / 384424 / 481
1400 / 1439
Medianin Months
3135681713128
SCLC - TNM stage
ES Small Cell Lung Cancer: Evolution of Therapy
Alkylating Based
Chemotherapy
(CMV)
Anthracycline Based
Chemotherapy
(CAV)
1970s 1980s
Platinum Based
Chemotherapy
(EP/IP)
1990s
Targeted Therapy
and Sequencing
2000s
Immunotherapy
and ADCs?
2010s
L Horn, WLCC 2016
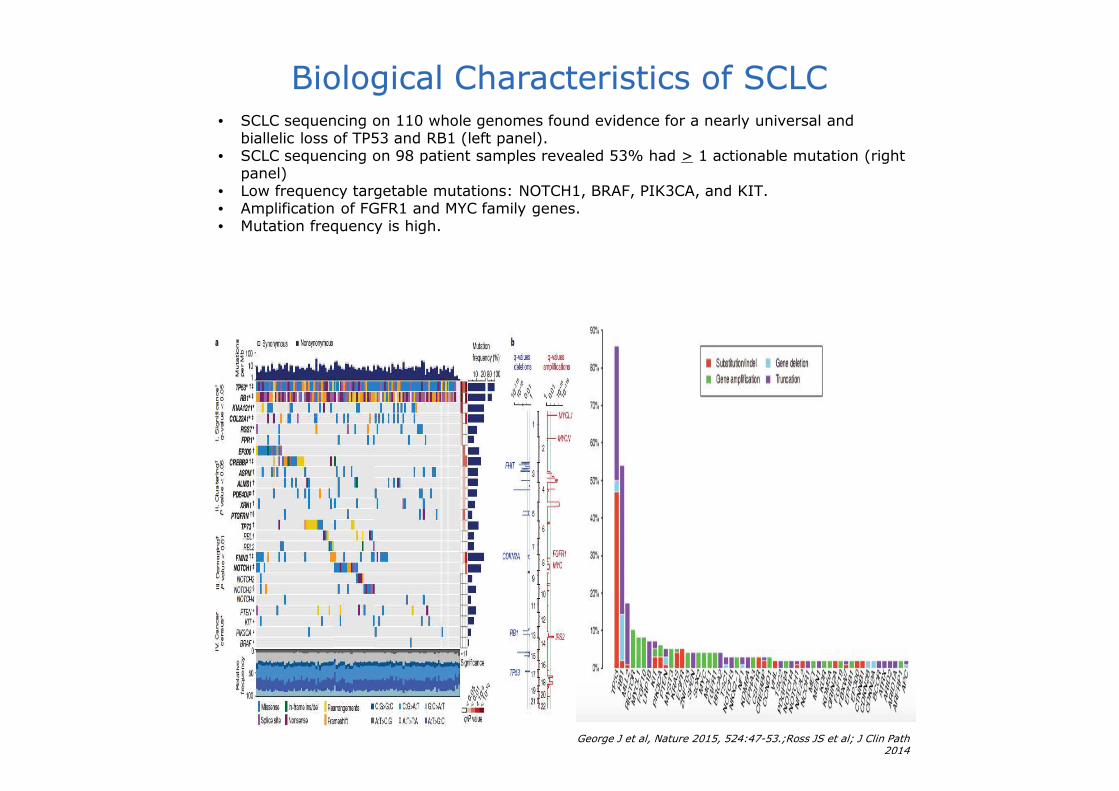
George J et al, Nature 2015, 524:47-53.;Ross JS et al; J Clin Path 2014
Biological Characteristics of SCLC• SCLC sequencing on 110 whole genomes found evidence for a nearly universal and
biallelic loss of TP53 and RB1 (left panel).• SCLC sequencing on 98 patient samples revealed 53% had > 1 actionable mutation (right
panel)• Low frequency targetable mutations: NOTCH1, BRAF, PIK3CA, and KIT. • Amplification of FGFR1 and MYC family genes.• Mutation frequency is high.

• Non-synonymous mutation rate 5.5-7.4/Mb (melanoma 6-6.5)• 180-240 mutations per tumor
Mutation Load and SCLC
Alexandrov LB, Nature 2013
Mutational catalogues of 7,042 primary cancers (507 from whole genome and 6,535 from exome sequences)
Alexandrov LB, Nature 2013

7J. Gorge et al..Nature.2015 524(7563): 47–53
Genomic Landscape
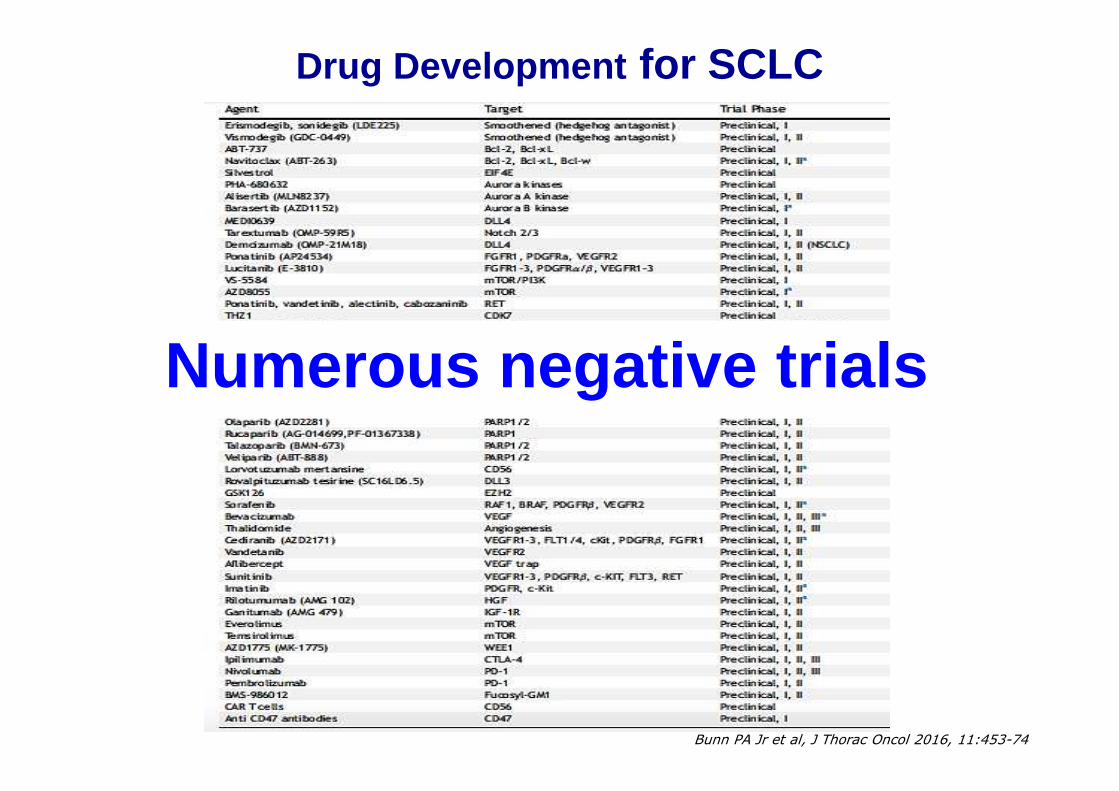
Drug Development for SCLC
Bunn PA Jr et al, J Thorac Oncol 2016, 11:453-74
Numerous negative trials

Mutation burden, smoking signature in predicting response in
NSCLC patients
Naiyer A. Rizvi et al. Science 2015;348:124-128

Clinical trials of cancer vaccines for lung cancer
Li Yang et al. Am J Clin Exp Immunol 2016;5(1):1-20

Checkpoint Inhibitors
• Anti-CTLA-4
• Anti-PD-1
• Anti-PD-L1
11

CTLA-4 Inhibitors in SCLC

CA184-041: Phase II Ipilimumab + Chemotherapy for 1L ED -SCLC*
N=130Concurrent
Ipilimumab (10 mg/kg) +
Paclitaxel (175 mg/m2)/carboplatin (AUC 6)
Q3W
(n=43)Key Inclusion Criteria
≥18 years of age
ED-SCLC*
ECOG PS ≤1
No prior systemic therapy for lung cancer
No symptomatic CNS metastases or autoimmune disease
R
ControlPlacebo + paclitaxel (175 mg/m2)/carboplatin
(AUC 6)
(n=45)
• Primary outcome measure: irPFS• Key secondary outcome measures: OS,
PFS, BORR, safety
Phased †
Ipilimumab (10 mg/kg) +
Paclitaxel (175 mg/m2)/carboplatin (AUC 6)
Q3W
(n=42)
MTNIpi‡
MTNIpi‡
MTNplacebo
* This trial also included 204 NSCLC patients.† 2 doses of paclitaxel/carboplatin prior to start of ipilimumab.‡ 10 mg/kg intravenous.

PFS and BORR in the ED -SCLC Population: CA184-041
ResponseControl
Pbo + chemo(n=45)
ConcurrentIpi + chemo
(n=43)
Phased *
Ipi + chemo(n=42)
irPFSMedian (mo)
5.3 5.7(HR=0.75, P=0.11)
6.4(HR=0.64, P=0.03†)
mWHO-PFSMedian (mo)
5.2 3.9(HR=0.93, P=0.38)
5.2(HR=0.93, P=0.37)
irBORR 53% 49% 71%
irWHO-BORR 49% 33% 57%* Phased regimen: 2 doses of paclitaxel (175 mg/m2)/carboplatin (AUC=6) prior to start of ipilimumab.† P-values are based on an unstratified log-rank test with a one-sided α of 0.1.
See slide notes for references and abbreviations.

OS in ED-SCLC: CA184 -041
OS of Phased vs Control
Months
Control Phased *
Median
HRP
9.9 mo----
12.9 mo0.750.13
ControlConcurren
t
Median
HRP
9.9 mo----
9.1 mo0.950.41
0 3 6 9 12 15 18 21
1.0
0.8
0.6
0.4
0.2
0.0
OS
(p
rob
ab
ilit
y)
0 3 6 9 12 15 18 21 24
1.0
0.8
0.6
0.4
0.2
0.0
OS
(p
rob
ab
ilit
y)
* Phased regimen: 2 doses of paclitaxel (175 mg/m2)/carboplatin (AUC=6) prior to start of ipilimumab.
OS of Concurrent vs Control
Months
See slide notes for references and abbreviations. Reck et al, Ann Oncol, 2013.

Safety: Treatment-Related AEs in ≥15% Patients - CA184 -041
ConcurrentIpilimumab
(n=42)
Grade 1/2, % Grade 3/4, %
PhasedIpilimumab
(n=42)
Grade 1/2, % Grade 3/4, %
Control
(n=44)
Grade 1/2, % Grade 3/4, %/%
Total treatment-related AEs
41 43 45 50 61 23/7
Anemia† 87 5 81 10 84 7/0
Thrombocytopenia† 44 3 50 7 61 2/0
Alopecia 57 n/a 67 n/a 59 n/a/n/a
Neutropenia† 41 8 40 10 40 2/0
Arthralgia 24 0 36 10 32 0/0
Peripheral sensory neuropathy*
24 0 33 0 32 0/0
Fatigue 24 7 17 12 20 5/0
Nausea 24 0 29 0 20 2/0
Diarrhea 21 4 24 10 11 5/0
Peripheral neuropathy 14 0 24 0 11 0/0
Pruritis 24 0 17 2 5 0/0
ALT† 36 18 36 4 21 0/0
AST† 39 13 33 7 33 0/0
* As reported by investigators. † Based on laboratory results.
Adverse events listed were those (any grade) reported in at least 5% of treated patients in any arm. Patients could have more than one adverse event. One death
in the concurrent ipilimumab arm was attributed to treatment-related hepatotoxicity.
Adapted from Reck et al, Ann Oncol, 20131

CA184-156: Phase III Ipilimumab + Chemotherapy for 1L ED -SCLC
N=1414
Ipilimumab +
Pt/Etoposide
Key Inclusion Criteria
� ≥18 years of age
� ED-SCLC
� ECOG PS ≤1
� No prior systemic therapy for lung cancer
� No symptomatic CNS metastases or autoimmune disease
R
Placebo +
Pt/Etoposide
• Primary outcome measure: OS• Secondary outcome measure: PFS
Start Date: December 2011Estimated Study Completion Date: March 2017Estimated Primary Completion Date: March 2015Status: Ongoing, but not recruitingStudy Director: Bristol-Myers Squibb

PE ± Ipilimumab
Reck M et al, JCO 2016 [Epub ahead of print]
• N = 1132• Documented ED-SCLC• ECOG PS 0-1• No brain mets requiring tx• No autoimmune disease• No systemic immunosuppression
PE + Ipilimumab
10/mg/kg IV Q3Wn = 478
PE + Placebo Q3Wn = 476
R1:1 N = 954

Why was this study negative?• Drug delivery
• 15% randomly assigned pts did not receive study drug.
• Only 13% of ipilimumab pts lived long enough to receive this drug
for maintenance
• Correct neoantigens not expressed sufficiently to drive
immunogenicity.
• Anti-CTLA-4 agent may not be the best drug to use after
chemotherapy (cytotoxic T cell effect occurs during priming phase).
• Trial populaton not enriched enough for patient population that
benefit from immunotherapy.
• Exclude rapid disease progressors
• Need for biomarker.
• Combined anti-CTLA-4 and anti-PD-1/PD-L1 may be more effective.
19

20LOCAL APPROVAL MAY BE REQUIRED BEFORE EXTERNAL USE. REFER TO LOCAL GUIDELINES.
.
NCT01331525 / ICE: Phase II Ipilimumab + Chemotherapy for 1L ED -SCLC
* 3-monthly maintenance ipilimumab planned.† Assessed by investigators. ‡ Fatal event presented like anti-Hu syndrome; both events occurred in patients with positive baseline anti-neuronal antibodies. §At 1 year.
1L ED-SCLC[1,2]
Chemo-immunotherapy with ICE was feasible, but with appreciable immune-related AEs [1]
− 61% of patients experienced >Grade 3 AEs, 42% possibly ipi-related †
− 6% (2 pts) had ipi-related neurological events ‡ (1 case was fatal)
Immuno-Oncology for SCLCImmuno-Oncology for SCLC
Ipilimumab(Cycles 3–6, in
responding patients*)
EC
N=42
• Primary outcome measure: PFS§
• Secondary outcome measures: tumor response and toxicity
Start Date: June 2011
Estimated Study Completion Date: June 2015Estimated Primary Completion Date: June 2015Status: CompletedStudy Director: University Hospital Southampton NHS
Foundation Trust collaboration with Bristol-Myers Squibb and
others
See slide notes for references and abbreviations.

NCT02046733 / STIMULI: Phase II Ipilimumab with nivolumab vs Observation for 1L L D-
SCLC
* ≤ 1 for enrollment, ≤ 2 for randomization.† Except fatigue, appetite, esophagitis, and renal impairment (≤ Grade 2 allowed) and alopecia (any grade allowed).
N=260
• Primary outcome measure: OS, PFS• Secondary outcome measures: OR,
TTF, AEs
Start Date: July 2014
Estimated Study Completion Date: January 2022Estimated Primary Completion Date: October 2019Status: Active, recruitingStudy Director: European Thoracic Oncology Platform
collaboration with Bristol-Myers Squibb and others
Ipilimumab +
nivolumab
R
Observation
Key Inclusion Criteria
� ≥18 years of age
� Untreated LD-SCLC
� ECOG PS ≤1 or 2*
� Non PD after completion of CRT, PCI
� Adequate hematological, renal, and liver function
� Recovery of all AEs to Grade ≤1†
CRT + PCI

PD-1/PD-L1 Inhibitors in SCLC
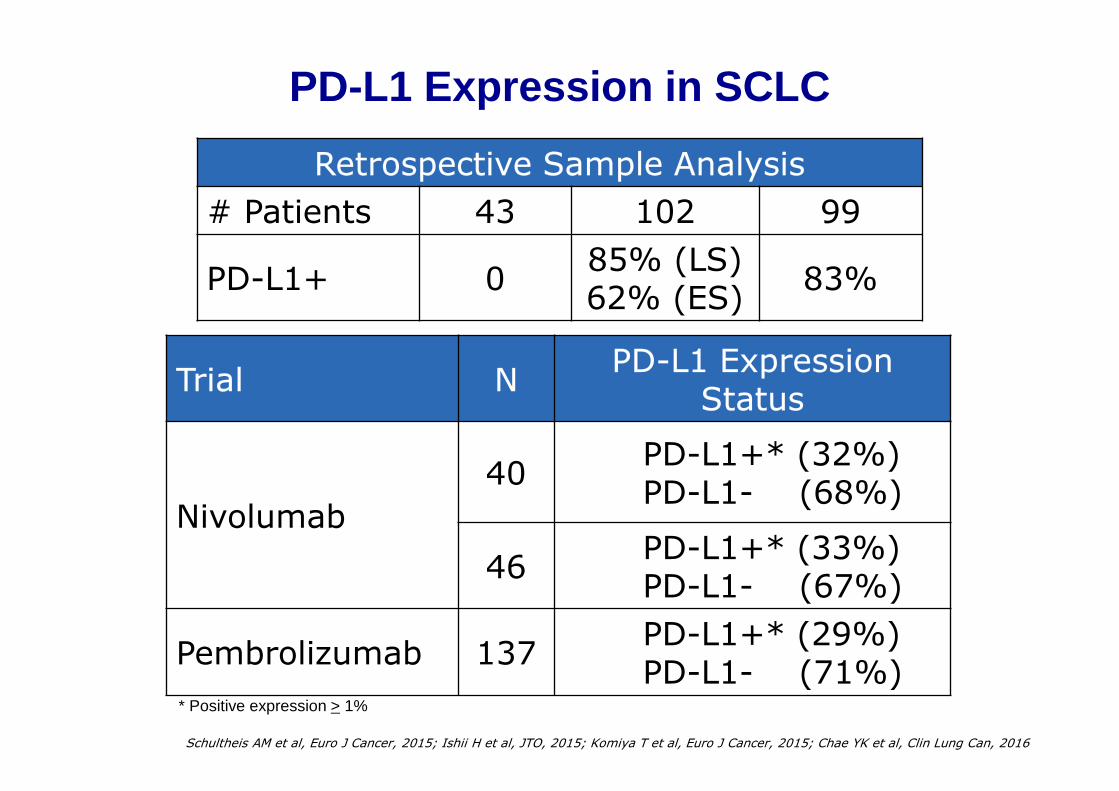
PD-L1 Expression in SCLC
Retrospective Sample Analysis
# Patients 43 102 99
PD-L1+ 085% (LS)62% (ES)
83%
Schultheis AM et al, Euro J Cancer, 2015; Ishii H et al, JTO, 2015; Komiya T et al, Euro J Cancer, 2015; Chae YK et al, Clin Lung Can, 2016
Trial NPD-L1 Expression
Status
Nivolumab
40PD-L1+* (32%)PD-L1- (68%)
46PD-L1+* (33%)PD-L1- (67%)
Pembrolizumab 137PD-L1+* (29%)PD-L1- (71%)
* Positive expression > 1%

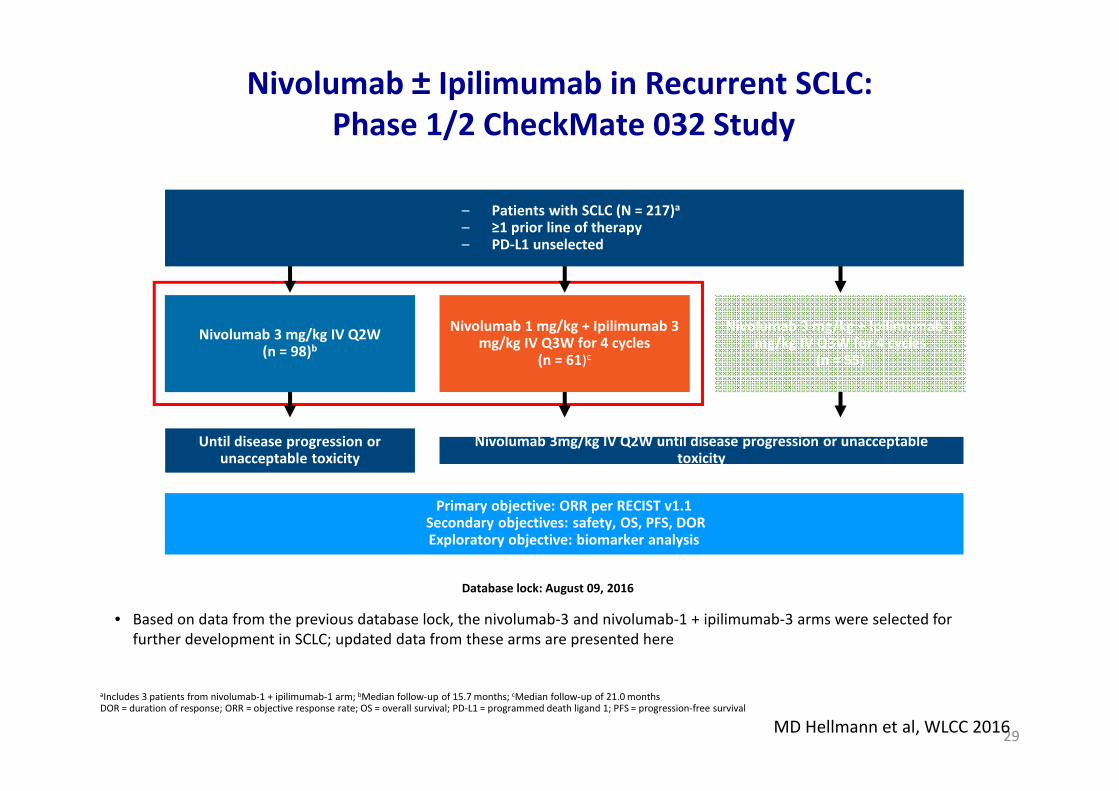
Nivolumab ± Ipilimumab in Recurrent SCLC:
Phase 1/2 CheckMate 032 Study
• Based on data from the previous database lock, the nivolumab-3 and nivolumab-1 + ipilimumab-3 arms were selected for
further development in SCLC; updated data from these arms are presented here
24
aIncludes 3 patients from nivolumab-1 + ipilimumab-1 arm; bMedian follow-up of 15.7 months; cMedian follow-up of 21.0 monthsDOR = duration of response; ORR = objective response rate; OS = overall survival; PD-L1 = programmed death ligand 1; PFS = progression-free survival
– Patients with SCLC (N = 217)a
– ≥1 prior line of therapy– PD-L1 unselected
Until disease progression or unacceptable toxicity
Primary objective: ORR per RECIST v1.1Secondary objectives: safety, OS, PFS, DORExploratory objective: biomarker analysis
Database lock: August 09, 2016
Nivolumab 3 mg/kg IV Q2W(n = 98)b
Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg IV Q3W for 4 cycles
(n = 61)c
Nivolumab 3 mg/kg + Ipilimumab 1 mg/kg IV Q3W for 4 cycles
(n = 55)
Nivolumab 3mg/kg IV Q2W until disease progression or unacceptable toxicity
S Antonia et al., Lancet Oncol 2016

* Three patients in the nivolumab 3 mg/kg group, two patients in the nivolumab 1 mg/kg plus ipilimumab 3 mg/kg group, and four patients in the nivolumab 3
mg/kg plus ipilimumab 1 mg/kg group did not receive first-line platinum therapy and did not meet eligibility criteria, although they were treated and included
in the analysis. †Defined as a patient who relapsed <90 days after chemotherapy.
Baseline Patient Characteristics:
CheckMate 032 SCLC Cohort
Nivolumab3 mg/kg(n = 98)
Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg
(n = 61)
Nivolumab 3 mg/kg + Ipilimumab 1 mg/kg
(n = 54)
Median age, years(range)
Age ≥75 years63 (57–68)
9 (9%)66 (58–71)
7 (11%)61 (56–65)
0
Male, % 62 57 59
Race, %WhiteBlack/African AmericanOther Not reported
93340
98200
96022
Number of prior treatment regimens, %12–3>3
41563
523810
43526
First-line platinum-treated patients*, %Platinum-sensitivePlatinum-resistant†
Unknown
563110
413818
393915
See slide notes for references and abbreviations. PERMISSION NOT OBTAINED Antonia et al, ASCO 20161
S Antonia et al., Lancet Oncol 2016

*Percentage of PD-L1 evaluable patients; may exceed 100% due to rounding.
Nivolumab3 mg/kg(n = 98)
Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg
(n = 61)
Nivolumab 3 mg/kg + Ipilimumab 1 mg/kg
(n = 54)
Smoking Status, %Current/former smokerNever smokedUnknown
9730
9370
8992
PD-L1 expression level*≥ 1%< 1%≥ 5%< 5%Indeterminate, not evaluable, or missing
14866
9430
24765
9539
13883
9826
Baseline Patient Characteristics:
CheckMate 032 SCLC Cohort
S Antonia et al., Lancet Oncol 2016

Nivolumab 3
(n = 98)
Nivolumab 1 + Ipilimumab 3
(n = 61)
Nivolumab 3 + Ipilimumab 1
(n = 54)
ORR, % 10 23 19
Platinum-sensitivea 11 28 19
Platinum-resistanta 10 17 10
Complete response 0 2 0
Partial response 10 21 19
Stable disease 22 21 17
Progressive disease 53 38 54
Unable to determine 12 13 11
Not evaluableb 2 5 0
Time to objective response, months 2.0 (1.3–2.8) 2.1 (1.4–2.8) 1.4 (1.3–2.7)
aPlatinum sensitivity was unknown for 29 patients as follows: nivolumab-3, n=10; nivolumab-1/ipilimumab-3, n=11; nivolumab-3/ipilimumab-1, n=8. 3
patients in the nivolumab-3 arm, 2 patients in the nivolumab-1/ipilimumab-3 arm and 4 patients in the nivolumab-3/ipilimumab-1 arm did not receive
first-line platinum therapy and did not meet eligibility criteria, although they were treated and included in the analysis.bNo tumor assessment follow-up.
Summary of Clinical Activity: CheckMate 032 SCLC Cohort
S Antonia et al., Lancet Oncol 2016

Safety: Treatment-Related AEs in ≥10% Patients
• Treatment-related deaths
• Two patients in the nivolumab 1 mg/kg plus ipilimumab 3 mg/kg group (myasthenia gravis and worsening of renal failure, respectively)
• One patient in the nivolumab 3 mg/kg plus ipilimumab 1 mg/kg cohort died from pneumonitis, regarded as treatment-relatedAnalysis included all patients enrolled at least 90 days prior to database lock. Patients with AEs after crossover from nivolumab 3 mg/kg to combination treatment excluded. Some
patients had more than one AE.
Nivolumab 3 mg/kg(n=98)
Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg (n=61)
Nivolumab 3 mg/kg + Ipilimumab 1 mg/kg (n=54)
Grade 1–2
Grade 3 Grade 4Grade 1–
2Grade 3 Grade 4
Grade 1–2
Grade 3 Grade 4
Total treatment-related AEs, n (%)
39 (40%) 9 (9%) 4 (4%) 30 (49%) 14 (23%) 4 (7%) 30 (56%) 8 (15%) 2 (4%)
Fatigue 10 (10%) 1 (1%) 0 16 (26%) 0 0 12 (22%) 0 0
Pruritus 11 (11%) 0 0 11 (18%) 1 (2%) 0 5 (9%) 0 0
Diarrhea 7 (7%) 0 0 10 (16%) 3 (5%) 0 8 (15%) 1 (2%) 0
Nausea 7 (7%) 0 0 6 (10%) 1 (2%) 0 4 (7%) 0 0
Decreased appetite 6 (6%) 0 0 4 (7%) 0 0 6 (11%) 0 0
Hypothyroidism 3 (3%) 0 0 9 (15%) 1 (2%) 0 4 (7%) 0 0
Hyperthyroidism 2 (2%) 0 0 7 (11%) 0 0 3 (6%) 0 0
Rash 2 (2%) 0 0 10 (16%) 2 (3%) 0 4 (7%) 0 0
Rash, maculopapular 1 (1%) 0 0 6 (10%) 2 (3%) 0 2 (4%) 0 0
Treatment-related AEs leading to
discontinuations6 (6%) 7 (11%) 4 (7%)
See slide notes for references and abbreviations. S Antonia et al., Lancet Oncol 2016
Nivolumab ± Ipilimumab in Recurrent SCLC:
Phase 1/2 CheckMate 032 Study
• Based on data from the previous database lock, the nivolumab-3 and nivolumab-1 + ipilimumab-3 arms were selected for
further development in SCLC; updated data from these arms are presented here
29
aIncludes 3 patients from nivolumab-1 + ipilimumab-1 arm; bMedian follow-up of 15.7 months; cMedian follow-up of 21.0 monthsDOR = duration of response; ORR = objective response rate; OS = overall survival; PD-L1 = programmed death ligand 1; PFS = progression-free survival
– Patients with SCLC (N = 217)a
– ≥1 prior line of therapy– PD-L1 unselected
Until disease progression or unacceptable toxicity
Primary objective: ORR per RECIST v1.1Secondary objectives: safety, OS, PFS, DORExploratory objective: biomarker analysis
Database lock: August 09, 2016
Nivolumab 3 mg/kg IV Q2W(n = 98)b
Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg IV Q3W for 4 cycles
(n = 61)c
Nivolumab 3 mg/kg + Ipilimumab 1 mg/kg IV Q3W for 4 cycles
(n = 55)
Nivolumab 3mg/kg IV Q2W until disease progression or unacceptable toxicity
MD Hellmann et al, WLCC 2016
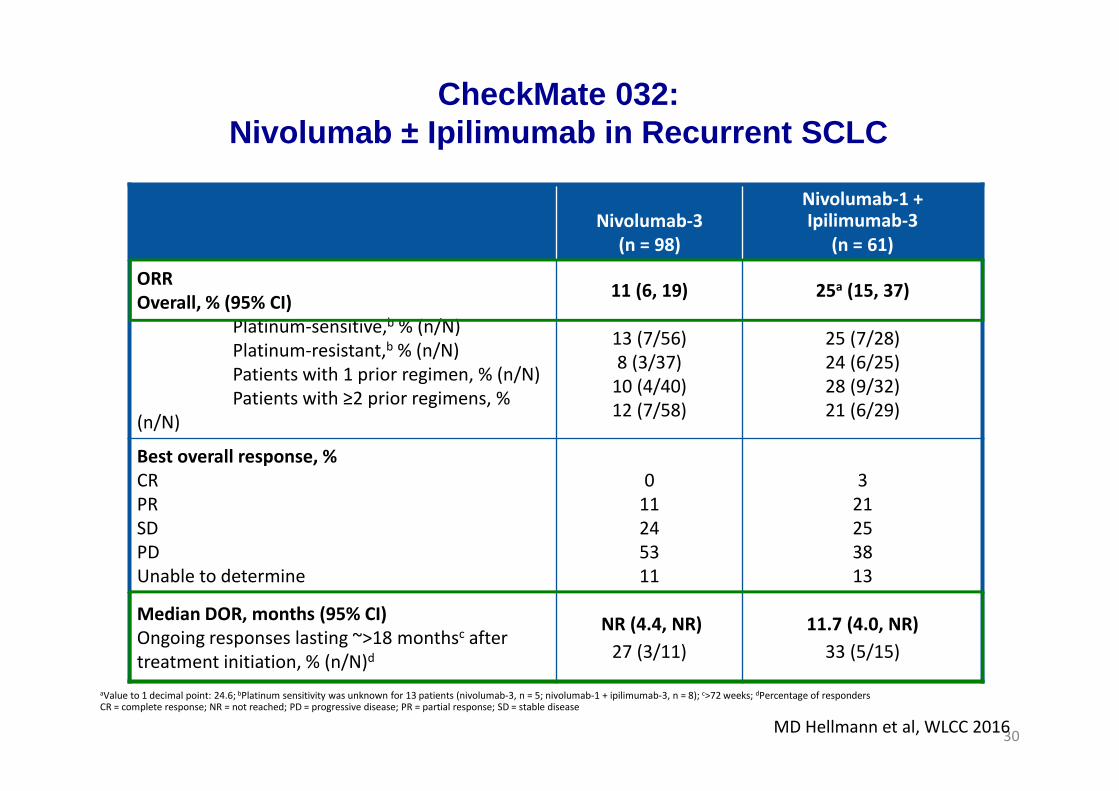
CheckMate 032: Nivolumab ± Ipilimumab in Recurrent SCLC
Summary of Efficacy
30
Nivolumab-3
(n = 98)
Nivolumab-1 + Ipilimumab-3
(n = 61)
ORR
Overall, % (95% CI)
Platinum-sensitive,b % (n/N)
Platinum-resistant,b % (n/N)
Patients with 1 prior regimen, % (n/N)
Patients with ≥2 prior regimens, %
(n/N)
11 (6, 19)
13 (7/56)
8 (3/37)
10 (4/40)
12 (7/58)
25a (15, 37)
25 (7/28)
24 (6/25)
28 (9/32)
21 (6/29)
Best overall response, %
CR
PR
SD
PD
Unable to determine
0
11
24
53
11
3
21
25
38
13
Median DOR, months (95% CI)
Ongoing responses lasting ~>18 monthsc after
treatment initiation, % (n/N)d
NR (4.4, NR)
27 (3/11)
11.7 (4.0, NR)
33 (5/15)
aValue to 1 decimal point: 24.6; bPlatinum sensitivity was unknown for 13 patients (nivolumab-3, n = 5; nivolumab-1 + ipilimumab-3, n = 8); c>72 weeks; dPercentage of respondersCR = complete response; NR = not reached; PD = progressive disease; PR = partial response; SD = stable disease
CheckMate 032: Nivolumab ± Ipilimumab in Recurrent SCLC
MD Hellmann et al, WLCC 2016

CheckMate 032: Nivolumab ± Ipilimumab in Recurrent SCLC 2-Year Overall Survival
Additional follow-up since ASCO 2016: 4.6 months
31
Events/number
at risk
Median OS, Months (95%
CI)
Medianfollow-up
time,a months
Nivolumab-3 71/98 4.1 (3.0, 9.1) 15.7
Nivolumab-1 + ipilimumab-3
40/61 7.9 (3.6, 14.2) 21.0
Months
OS
(%
)100
90
80
70
60
50
40
30
10
0
20
330 30272421181512963
0144810102435385498Nivolumab-3
Number of patients at risk
0013512192428334361Nivolumab-1 + ipilimumab-3
1-yr OS = 30%
2-yr OS = 17%c
2-yr OS = 30%b
1-yr OS = 42%
MD Hellmann et al, WLCC 2016
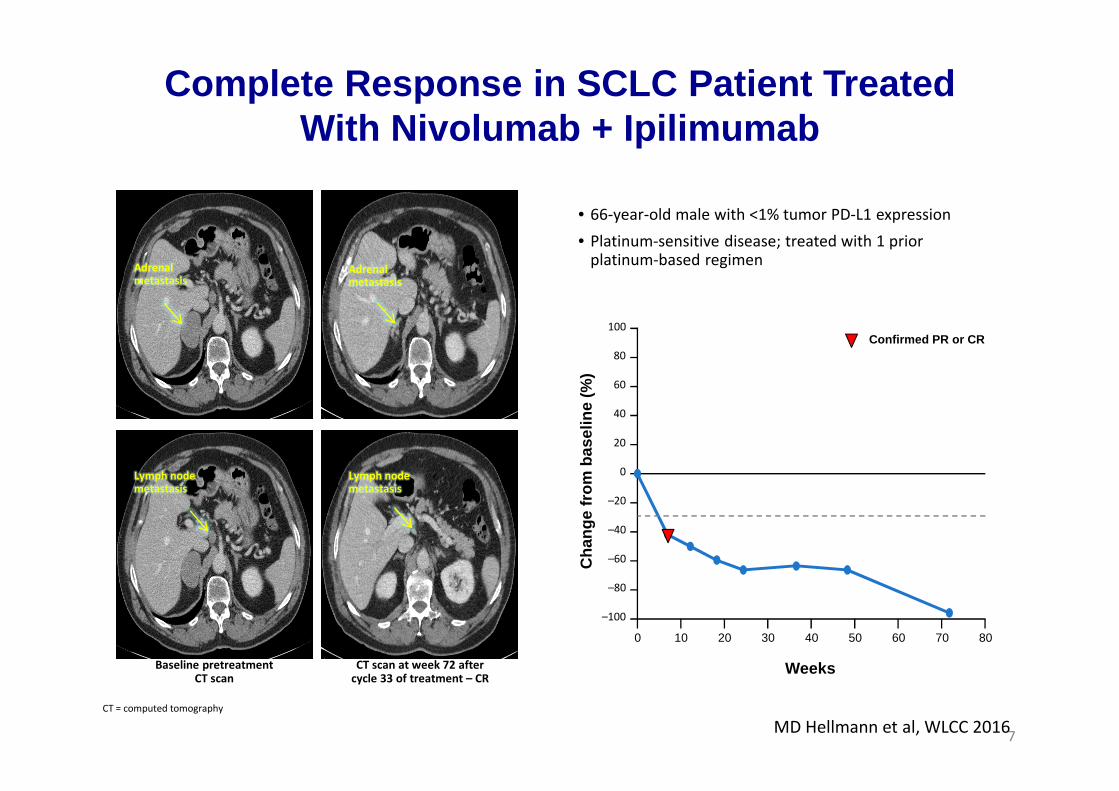
7
• 66-year-old male with <1% tumor PD-L1 expression
• Platinum-sensitive disease; treated with 1 prior platinum-based regimen
CT scan at week 72 after cycle 33 of treatment – CR
Baseline pretreatment CT scan
Adrenalmetastasis
Adrenalmetastasis
Lymph nodemetastasis
Lymph nodemetastasis
CT = computed tomography
0 10 20 30 40 50 60 70 80
Weeks
Cha
nge
from
bas
elin
e (%
)
–100
–80
–60
–40
–20
20
40
60
80
100
0
Confirmed PR or CR
Complete Response in SCLC Patient Treated With Nivolumab + Ipilimumab
MD Hellmann et al, WLCC 2016

Across cohorts, 73% evaluable for PD-L1 expression at baseline; 17% (of PD-L1 evaluable samples) with ≥1% tumor PD-L1 expression
33
Nivolumab-3
Nivolumab-1 + Ipilimumab-3
aKaplan–Meier estimates, with error bars indicating 95% CIs
0
10
20
30
40
50
60
70
80
30
98n
All patients
OS
rat
e (%
)
Overall PD-L1 expression
42
61
32
65
<1%
44
31
30
10
≥1%
50
10
26
23
Unknown
35
20
Nivolumab ± Ipilimumab in Recurrent SCLC 1-Year OS Rates a by PD-L1 Expression
MD Hellmann et al, WLCC 2016

No additional treatment-related deaths were reported; at prior disclosure, 2 treatment-related deaths occurred with nivolumab-1 + ipilimumab-3: one due to myasthenia gravis and one due to worsening of renal failure
Grade 3–4 treatment-related limbic encephalitis occurred in 1 patient in the nivolumab-3 arm
Treatment-related pneumonitis occurred in 4 patients in the nivolumab-3 arm (2 grade 3–4 events) and 2 patients in the nivolumab-1 + ipilimumab-3 arm (1 grade 3–4 event)
34
Grade 1−2
Grade 3−4
Pat
ient
s w
ith a
n ev
ent,
%
Nivolumab-3
(n = 98)
Nivolumab-1 + Ipilimumab-3
(n = 61)
13
DC = discontinuation
CheckMate 032: Nivolumab ± Ipilimumab in Recurrent SCLC
Treatment-Related AEs in ≥10% of Patients
MD Hellmann et al, WLCC 2016
Presentation Number: Presentation Title – Presenting Author
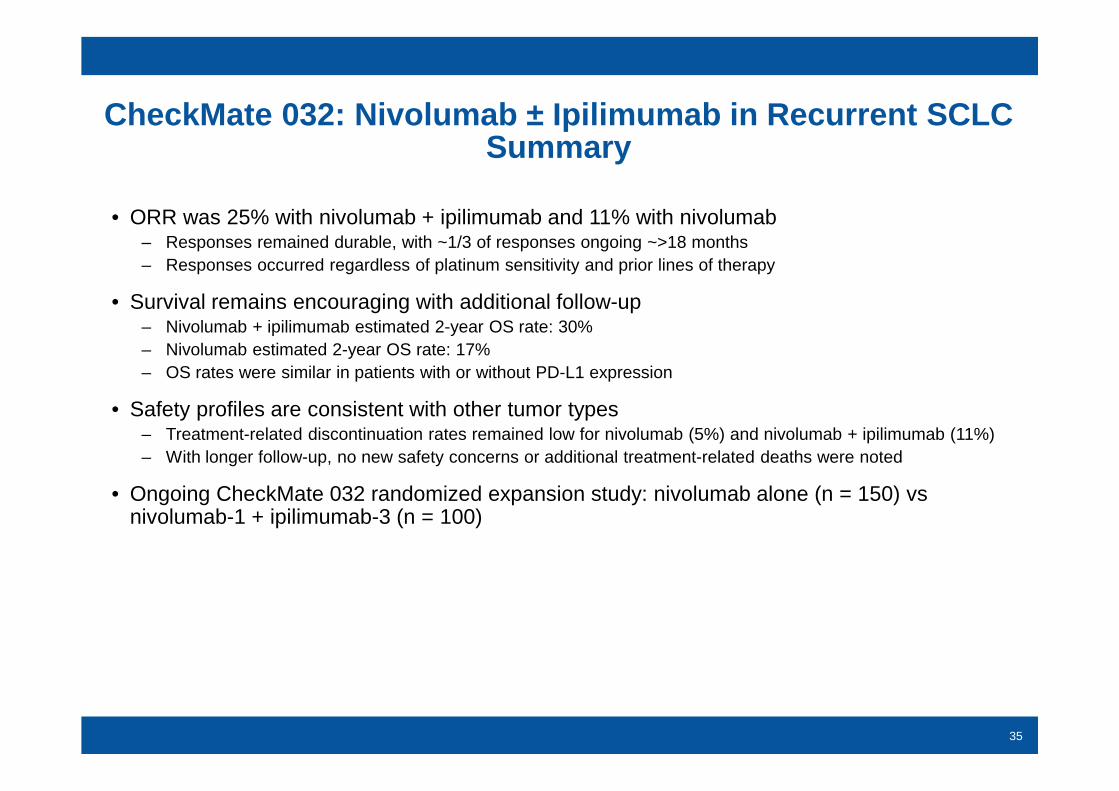
CheckMate 032: Nivolumab ± Ipilimumab in Recurrent SCL C Summary
• ORR was 25% with nivolumab + ipilimumab and 11% with nivolumab– Responses remained durable, with ~1/3 of responses ongoing ~>18 months– Responses occurred regardless of platinum sensitivity and prior lines of therapy
• Survival remains encouraging with additional follow-up– Nivolumab + ipilimumab estimated 2-year OS rate: 30%– Nivolumab estimated 2-year OS rate: 17% – OS rates were similar in patients with or without PD-L1 expression
• Safety profiles are consistent with other tumor types– Treatment-related discontinuation rates remained low for nivolumab (5%) and nivolumab + ipilimumab (11%)– With longer follow-up, no new safety concerns or additional treatment-related deaths were noted
• Ongoing CheckMate 032 randomized expansion study: nivolumab alone (n = 150) vs nivolumab-1 + ipilimumab-3 (n = 100)
35

CHECKMATE 451
Ready. ASCO 2016 Abstract TPS 8579.
CheckMate 451

Nivolumab and SCLC
Trial population Intervention
CHECKMATE 331
Relapse/refractory SCLC
[NCT02481830]
Randomised phase 3 study.
2nd line
Nivolumab vs Topotecan
STIMULI
LD-SCLC
[NCT02046733]
Randomised phase 2 study. LD-SCLC.
Nivolumab +Ipilimumab v no Tx following CRT
Relapse/refractory SCLC
[NCT02247349]
BMS-986012 anti- fucosyl GM1, alone and in
combination with nivolumab
Relapse/refractory SCLC
[NCT02472977]
Advanced solid tumours incl SCLC. Phase 1 study
of Ulocuplumab (anti-CXCR4 mab) alone or in
combination with Nivolumab
Nivolumab in SCLC

6198 – PA Ott
KEYNOTE-028 (NCT02054806): Phase 1b Multicohort Stud y of Pembrolizumab for PD -L1–Positive Advanced Solid Tumors
aIf clinically stable, patients are to remain on pembrolizumab until progressive disease is confirmed on a second scan performed ≥4 weeks later.
aResponse assessment : Every 8 weeks for the first 6 months; every 12 weeks thereafter
Primary end points: ORR per RECIST v1.1 (investigator assessed) and safety
Secondary end points: PFS, OS, duration of response
Pembrolizumab 10 mg/kg IV
Q2W
Complete or partial response or stable disease
Treat for 24 months or until progression a
or intolerable toxicity
Confirmed progressive disease a
or unacceptable toxicity
Discontinue pembrolizumab
ResponseAssessment a
Patients•Small cell lung cancer•Failure of or inability to receive standard therapy•ECOG PS 0 or 1•≥1 measurable lesion•PD-L1 positivity•No autoimmune disease or interstitial lung disease
PA Ott et al., WLCC 2016

6198 – PA Ott
Analysis of PD -L1 Expression
• Samples: archival or newly obtained core or excisional biopsy of a nonirradiated lesion
• Immunohistochemistry: performed at a central laboratory using a prototype assay and the 22C3 antibody clone (Merck & Co., Inc., Kenilworth, NJ, USA)
• Positivity: membranous PD-L1 expression in ≥1% of tumor and associated inflammatory cells or positive staining in stroma
• SCLC cohort: of 147 evaluable samples, 42 PD-L1 positive (28.6%)
Examples of PD-L1 Staining in SCLC Specimens From K EYNOTE-028
PD-L1 Negative PD-L1 Positive
PA Ott et al., WLCC 2016

6198 – PA Ott
Patient and Disease Characteristics
Characteristic, n (%) N = 24
Age, median (range), years
60.5 (41-80)
Male 14 (58.3)
RaceWhiteAsianNot specified
13 (54.2)3 (12.5)8 (33.3)
ECOG performance status01
7 (29.2)17 (70.8)
Stable brain metastases 5 (20.8)
HistologySmall cellNeuroendocrine
23 (95.8)1 (4.2)
Characteristic, n (%) N = 24
Type of prior therapya
ChemotherapyRadiotherapyInvestigational TKIOther investigational therapy
24 (100)
1 (4.2)1 (4.2)1 (4.2)
Specific prior therapiesa,b
Cisplatin/carboplatin + etoposideIrinotecan or topotecanTaxane
24 (100)
11 (45.8)
7 (29.2)
Previous lines of therapyc
12
3 (12.5)
12
aPatients could have received ≥1 type of prior therapy. bNot all prior
therapies are listed. cIncludes adjuvant and neoadjuvant therapies.
Data cutoff date: June 20, 2016.
6198 – PA Ott
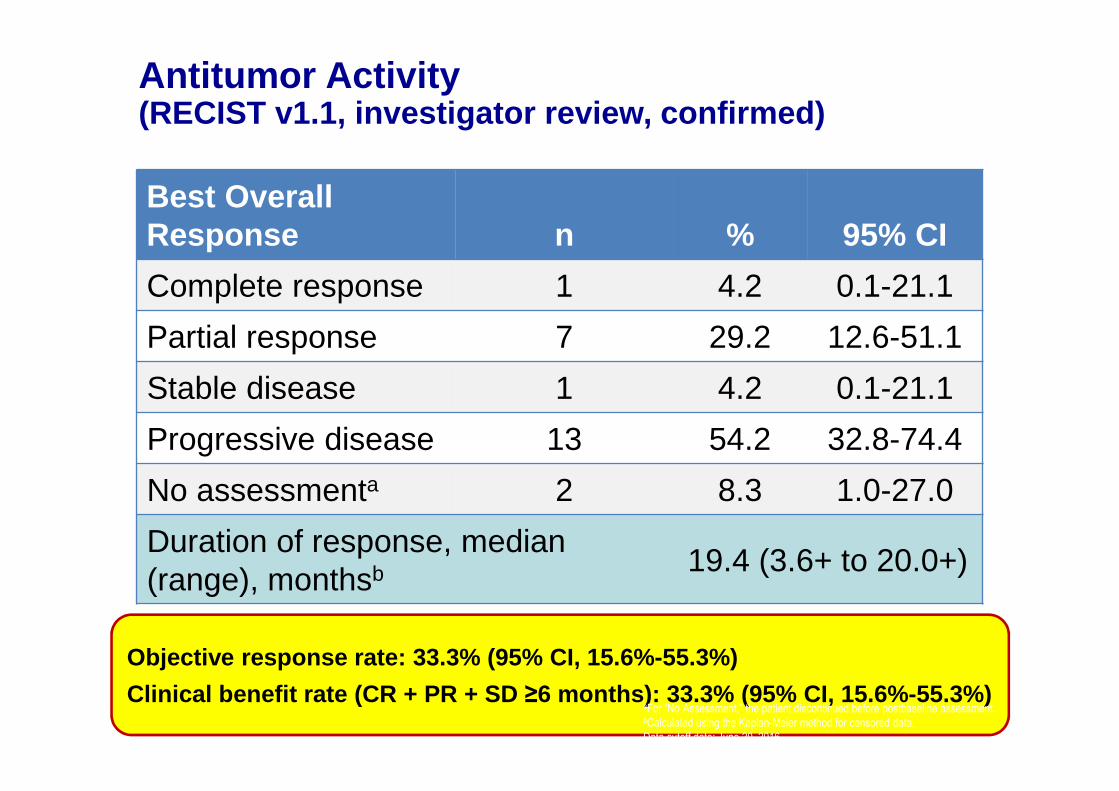
Antitumor Activity (RECIST v1.1, investigator review, confirmed)
Best Overall Response n % 95% CI
Complete response 1 4.2 0.1-21.1
Partial response 7 29.2 12.6-51.1
Stable disease 1 4.2 0.1-21.1
Progressive disease 13 54.2 32.8-74.4
No assessmenta 2 8.3 1.0-27.0
Duration of response, median (range), monthsb 19.4 (3.6+ to 20.0+)
Objective response rate: 33.3% (95% CI, 15.6%-55.3% )
Clinical benefit rate (CR + PR + SD ≥6 months): 33.3% (95% CI, 15.6%-55.3%)aFor “No Assessment,” the patient discontinued before postbaseline assessment.bCalculated using the Kaplan-Meier method for censored data.
Data cutoff date: June 20, 2016.

Change From Baseline in Tumor Size (RECIST v1.1, investigator review)
Bar lengths are best target lesion changes, bar colors are best overall responses.
Data cutoff date: June 20, 2016.PA Ott et al., WLCC 2016

6198 – PA Ott
Treatment Duration and Duration of Response (RECIST v1.1, investigator review)
0 20 40 60 80 100
Duration of Treatment, Weeks
Treatment discontinuation
Progressive disease
Stable disease
Partial response
Complete response
Treatment ongoing
The length of each bar corresponds to the duration of treatment.
Response symbols represent time to first report and not best overall.
Data cutoff date: June 20, 2016.
PA Ott et al., WLCC 2016

6198 – PA Ott
Progression-Free Survival(investigator review)
PFS N = 24
Events, n (%) 20 (83.3)
PFS, median (95% CI), months
1.9 (1.7–5.9)
28.6%23.8%
PA Ott et al., WLCC 2016
6198 – PA Ott
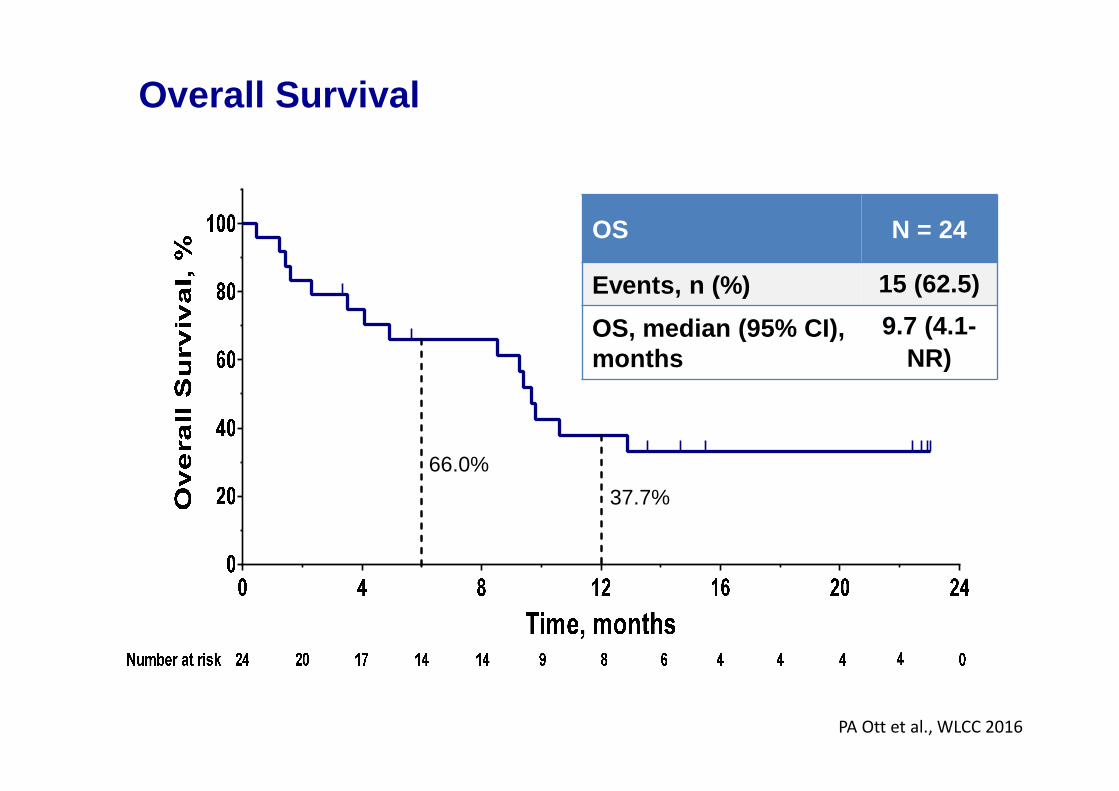
Overall Survival
OS N = 24
Events, n (%) 15 (62.5)
OS, median (95% CI), months
9.7 (4.1-NR)
66.0%
37.7%
PA Ott et al., WLCC 2016

6198 – PA Ott
Treatment-Related Adverse Events
aOccurred in the same patient.
Data cutoff date: June 20, 2016.
Any Grade, Occurring in ≥3 Patients
N = 24n (%)
Any 16 (66.7)
Arthralgia 4 (16.7)
Asthenia 4 (16.7)
Rash 4 (16.7)
Diarrhea 3 (12.5)
Fatigue 3 (12.5)
Grade 3-5, Occurring in ≥1 Patient
N = 24
n (%)
Any 2 (8.3)
Astheniaa 1 (4.2)
Blood bilirubin increased 1 (4.2)
Colitisa 1 (4.2)
Intestinal ischemiaa 1 (4.2)
AEs of Interest Based on Immune Etiology Occurring in ≥1 Patient
N = 24
n (%)
Any3
(12.5)
Autoimmune thyroiditis 1 (4.2)
Infusion site reaction 1 (4.2)
Cytokine release syndromea 1 (4.2)
Colitisa 1 (4.2)
• Median follow-up duration• 9.8 months (range, 0.5-24 months)
• No cases of pneumonitis
PA Ott et al., WLCC 2016

Pembrolizumab and SCLC
Trial population Intervention
Refractory SCLC
[NCT 02551432]
Pembrolizumab + Paclitaxel (single arm phase 2)
Second line SCLC
[NCT 02963090]
Pembrolizumab vs Topotecan [phase 2]
REACTION; First line ED-SCLC
[NCT 02580994]
platinum-etoposide chemotherapy +/- pembro [phase 2]
LD-SCLC
[NCT 02402920]
Pembrolizumab & Platinum-Etoposide, plus concurrent
radiotherapy [phase 1]
ED-SCLC
[NCT 023312251]
Pembrolizumab & chemotherapy in advanced solid tumours, incl
SCLC – Irinotecan & Pembrolizumab
ED-SCLC
[NCT 02661100]
Pembrolizumab in advanced solid tumours, incl SCLC. Treated with
CDX-1401 (tumour specific antigen) & Poly-ICLC (Toll-like receptor
agonist) & Pembrolizumab
KEYNOTE 158
[NCT 02628067]
Pembrolizumab in advanced solid tumours, incl SCLC.
Pembrolizumab in SCLC

Atezolizumab and SCLC
Trial population Intervention
IMpower133
First line ED-SCLC
[NCT02763579]
Carboplatin-etoposide +/- Atezolizumab or Placebo
(phase 3)
Untreated ED-SCLC
[NCT 02748889]
Carboplatin-etoposide +/- Atezolizumab
(phase 1 / 2)
Atezolizumab in SCLC

Durvalumab and SCLC
Trial population Intervention
Relapse SCLC
[NCT 02701400]
Durvalumab & Tremelimumab +/- Radiotherapy
Platinum-refractory
ED-SCLC
[NCT 02937818]
Durvalumab & novel combination therapies (e.g. XXX)
First line treatment in
solid tumours, incl
SCLC
[NCT 02658214]
Durvalumab & Tremelimumab
Advanced solid
tumours, incl SCLC
[NCT 02734004]
Durvalumab & Olaparib
No trials registered with Avelumab in Small cell lung cancer
Durvaluumab in SCLC

• Combination with first line platinum based chemotherapy or as maintenance therapy following induction therapy (pembrolizumab, atezolizumab and nivolumab)
• Compared to second line chemotherapy (nivolumab and pembrolizumab)
• Combined with paclitaxel as second line therapy (pembrolizumab)
• Following concurrent chemo-radiation therapy (nivolumab and pembrolizumab)
• Ipi+Nivo or Treme+Durva combos (+/- Chemo) in the first line setting
Ongoing Trials with PD -1/PD-L1 Inhibitors
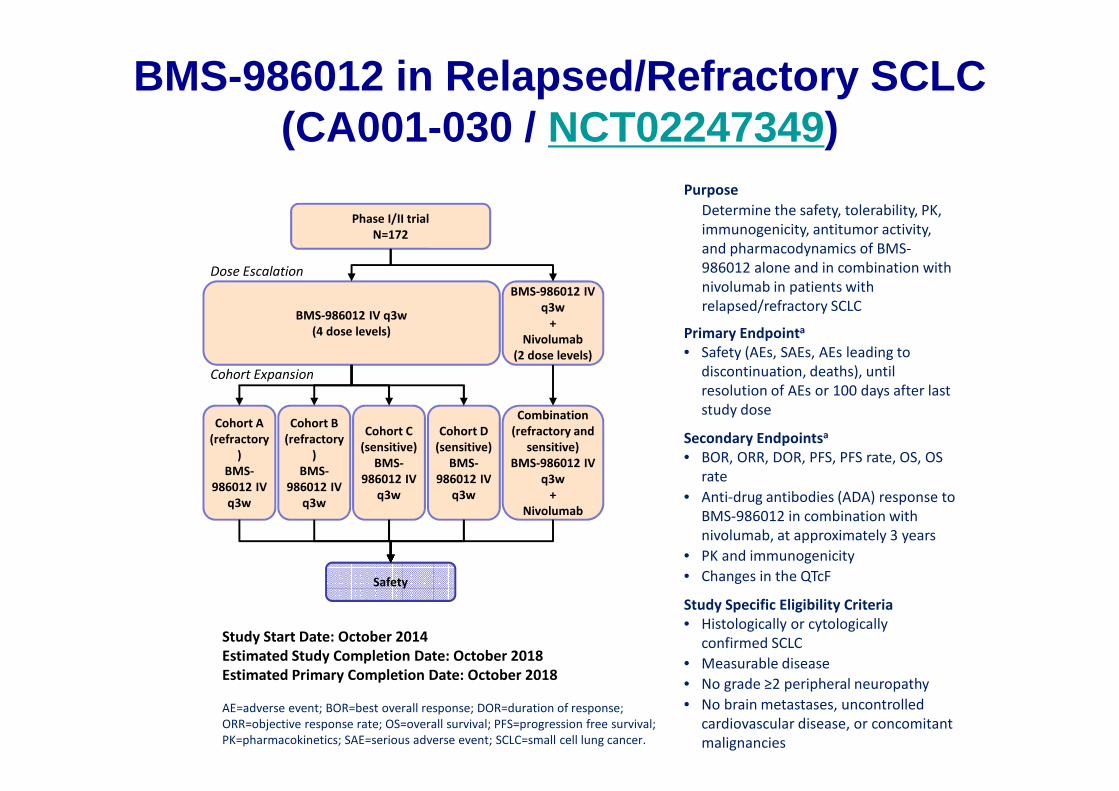
BMS-986012 in Relapsed/Refractory SCLC (CA001-030 / NCT02247349)
Purpose
Determine the safety, tolerability, PK,
immunogenicity, antitumor activity,
and pharmacodynamics of BMS-
986012 alone and in combination with
nivolumab in patients with
relapsed/refractory SCLC
Primary Endpointa
• Safety (AEs, SAEs, AEs leading to
discontinuation, deaths), until
resolution of AEs or 100 days after last
study dose
Secondary Endpointsa
• BOR, ORR, DOR, PFS, PFS rate, OS, OS
rate
• Anti-drug antibodies (ADA) response to
BMS-986012 in combination with
nivolumab, at approximately 3 years
• PK and immunogenicity
• Changes in the QTcF
Study Specific Eligibility Criteria
• Histologically or cytologically
confirmed SCLC
• Measurable disease
• No grade ≥2 peripheral neuropathy
• No brain metastases, uncontrolled
cardiovascular disease, or concomitant
malignancies
AE=adverse event; BOR=best overall response; DOR=duration of response;
ORR=objective response rate; OS=overall survival; PFS=progression free survival;
PK=pharmacokinetics; SAE=serious adverse event; SCLC=small cell lung cancer.
Study Start Date: October 2014
Estimated Study Completion Date: October 2018
Estimated Primary Completion Date: October 2018
Phase I/II trial
N=172
Safety
BMS-986012 IV q3w
(4 dose levels)
Cohort A
(refractory
)
BMS-
986012 IV
q3w
Cohort C
(sensitive)
BMS-
986012 IV
q3w
Cohort B
(refractory
)
BMS-
986012 IV
q3w
Cohort D
(sensitive)
BMS-
986012 IV
q3w
BMS-986012 IV
q3w
+
Nivolumab
(2 dose levels)
Combination
(refractory and
sensitive)
BMS-986012 IV
q3w
+
Nivolumab
Dose Escalation
Cohort Expansion

Trial of BMS -986012 in Combination With Platinum and Etoposide (CA001-044 /
NCT02815592)
Phase I/II trial
N=120
Safety and tolerability,
PFS
ARM 1
BMS-
986012
+
Cisplatin
+
Etoposide
ARM 2
BMS-
986012
+
Carboplati
n
+
Etoposide
ARM 3A
BMS-
986012
+
Platinum
+
Etoposide
ARM 3B
Platinum
+
Etoposide
Purpose
To administer BMS-986012 in combination with
platinum and etoposide as first-line therapy in
extensive-stage SCLC
Primary Endpointsa
• Number of patients with AEs
• Number of patients with SAEs
• Number of patients discontinuing due to AEs
• Number of AE-related deaths
• Number of patients with laboratory toxicity
grade shift from baseline
• PFS up to 2 years
Secondary Endpointsb
• Pharmacokinetic parameters
• Immunogenicity
Study Specific Eligibility Criteria
• Histologically or cytologically documented
SCLC
• Extensive-stage disease (stage IV)
• No prior systemic therapy for lung cancer
• No symptomatic brain metastases
• No grade 2 peripheral neuropathy
Study Start Date: September 2016
Estimated Study Completion Date: July 2019
Estimated Primary Completion Date: July 2019

Safety and Efficacy Study of Ulocuplumab and Nivolumab in Patients With Solid Tumors (CXCR4
inhibitor, NCT02472977)
Purpose
To determine whether the combination of
ulocuplumab and nivolumab is safe and
effective in the treatment of pancreatic
cancer and SCLC
Primary Endpointsa
DLT
ORR
OS
Secondary Endpointsa
Safety and tolerability
PFS
Study Specific Eligibility Criteria
Advanced, metastatic SCLC or pancreatic cancer
At least one prior chemotherapy
ECOG PS ≤1
No brain metastases
No prior treatment with checkpoint inhibitors
Phase I/II trial
N=195
SCLC Arm
Nivolumab
+
Ulocuplumab
DLT, ORR, and OS
Pancreatic Arm
Nivolumab
+
Ulocuplumab
Study Start Date: July 2015
Estimated Study Completion Date: February 2018
Estimated Primary Completion Date: February 2018

Study of BMS-986158 in Patients With Select Advanced
Solid Tumors (CA011-001 / NCT02419417)
Purpose
Determine the safety, tolerability, pharmacokinetics,
and pharmacodynamics of BMS-986158 in patients
with select advanced solid tumors
Primary Endpoint
• Safety (rate of AEs and SAEs), 30 days from last dose
or until AEs are grade ≤1 or have returned to baseline
Secondary Endpoints
• BOR, ORR, DOR, PFS, PFS rate, every 8 weeks until last
dose, expected average of 4 months
• PK, at c1 d1 to c8 d8 of dosing for dose escalation
phase and c1 d1 to c2 d8 for dose expansion phase
• BET expression, at c1 d1 through c2 d15 of dosing
• Changes in QTcF, at c1 d1 to c8 d8 of dosing for dose
escalation phase and c1 d1 to c2 d8 for dose
expansion phase
Study Specific Eligibility Criteria
• TNBC, ovarian (serous histology for expansion phase),
SCLC, or other solid tumors
• Life expectancy ≥3 months
• ≥1 measurable lesion by RECIST v1.1
• No uncontrolled medical conditions, second
malignancy, or uncontrolled cardiovascular disease
Study Start Date: June 2015
Estimated Study Completion Date: December 2018
Estimated Primary Completion Date: December 2018
Phase I/II trial
N=150
Safety
Arm A
BMS-986158
Dose Escalation Phase
Dose Expansion Phase
Arm B
BMS-986158
Arm C
BMS-986158
Arm A
BMS-986158
Arm B
BMS-986158
Arm C
BMS-986158

KEYNOTE 078 (AIO Thoraxoncology) - M. ReckPembrolizumab Maintenance Following First-Line
Platinum Based Chemotherapy Metastatic Squamous -
NSCLC
Primary endpoint Progression-free survival (RECIST 1.1)
Secondary endpoints Overall response rate
Overall survival
PD-L1 expression in tumor samples
Tolerability and safety
Quality of life (FACT-L, LCSS)
Metastatic
Squamous
NSCLC (n = 130)
First line
metastatic
Measurable
disease
ECOG PS 0-1
Any PD-L1
status
EML4/ALK (-)
EGFR wild type
Pembrolizumab
200 mg Q3W x 2 yrs
Placebo
Q3W 2 yrs
Carbo/Cis
platin
Combination
Min 2-6
cycles
C
R
o
r
P
R
R
1:1

Primary endpoint
Progression-free survival @ 6 months
Secondary endpoints
Overall response rate (ORR)
Progression Free Survival (PFS)
Immune-Related Disease Control Rate (iDCR)
Overall survival
Tolerability and safety
KEYNOTE 068 (REACTION - EORTC 1416) - B. BesseA phase II study of etoposide and cis/carboplatin with or
without pembrolizumab in untreated extensive SCLC
Metastatic SCLC
(n = 152)
First line metastatic
Measurable
disease
ECOG PS 0-1
PD-L1 status
Pembrolizumab200 mg Q3WPD/Death*
Carbo/
Cis
Etopos
ide
(2
cycles)
C
R
o
r
P
R
Carbo/Cis EtoposidePembrolizumanb(4 cycles)
Carbo/Cis
Etoposide
(4 cycles)
R
1:1
PD
End
Study
PD
* Patients receiving pembrolizumab are allowed to stop after one year. Should they progress more than 3
months after stopping therapy, retreatment will be allow provided they are meeting all inclusion criteria.

CCTG Protocol Number: IND.227A phase II randomized study of pembrolizumab in
patients with advanced malignant pleural
mesothelioma
Cisplatin/Pemetrexed
Pembrolizumab
R
1:
1
Malignant pleural mesothelioma(n = 126)
No prior therapy
Unresectable
disease
ECOG PS 0-1
PD-L1 status
End
Study
Primary Endpoint:Progression Free Survival
Secondary Endpoints: Overall Survival, QOL, Safety
Cisplatin/Pemetrexed/Pembrolizumab + Pembrolizumab maintenance PD
Stratifications:Epitheloid vs other subtypes


6198 – PA Ott
Summary and Conclusions
• Pembrolizumab demonstrated meaningful antitumor activity in previously treated patients with PD-L1–positive SCLC
– 33.3% ORR (1 CR, 7 PR) and 37.7% 12-month OS
– Responses were durable, with a median duration of response of 19.4 months
• Safety profile was consistent with previous experience for pembrolizumab in other tumor types
– Safety profile did not change with longer follow-up
• Ongoing trials of pembrolizumab for extensive-stage SCLC– NCT02359019: phase 2 study of pembrolizumab maintenance therapy following
combination chemotherapy
– NCT02580994: phase 2 study of etoposide and cis/carboplatin with or without pembrolizumab in untreated extensive-stage SCLC

Immunotherapy TrialsDrug Trial
Pembrolizumab
Phase I trial of MK-3475 and concurrent chemo/radiation for the elimination of small cell lung cancer
Study of pembrolizumab and chemotherapy with or without radiation in small cell lung cancer (SCLC)
Pembrolizumab plus chemotherapy in untreated extensive SCLC
Pembrolizumab and paclitaxel in refractory small cell lung cancer
Pembrolizumab in treating patients with extensive stage small cell lung cancer after completion of combination chemotherapy
Nivolumab
Small cell lung carcinoma trial with nivolumab and ipilimumab in limited doses
Effectiveness study of nivolumab compared to chemotherapy in patients with relapsed small-cell lung cancer ChekMate 331
A study of nivolumab, or nivolumab in combination with ipilimumab, or placebo in patients with ED-SCLC after completion of platinum-based chemotherapy CheckMate 451
AtezolizumabA study of carboplatin plus etoposide with or without atezolizumab in participants with untreated extensive-stage small cell lung cancer
DurvalumabDurvalumab and Tremelimumab with or without radiation in relapsed SCLC
Take Home Messages
ED 14: Small Cell Lung Cancer and Neuroendocrine Tu mors: Immunotherapy of Lung Cancer: Nevin Murray MD Canada
• Rovalpituzumab tserine demonstratates encouraging single agent
activity in relapsed SCLC (DLL3 first SCLC biomarker for Rx).
• Chemotherapy with phased Ipilimumab not more effective than
chemotherapy alone first line.
• Anti-PD-1 (nivolumab and pembrolizumab) active in previously treated
SCLC.
• Combined nivolumab and ipilumimab more toxic but possibly more
effective.
• No first-line data for immunotherapy without chemotherapy (can we
wait for response??).
• Approval of new agents expected (2nd line Rx SCLC “soft target”).

More and better targeting is needed!!
Conclussion

T cell mediated immune rejection of tumours
Therapeutic intervention
Presentation of
tumour-specific/associated Ag
Activation of
Tumour-specific
T cells
Co-stimulatory
T cell
Signals
Negative
Regulatory signals
(immune check-points)
Other
immunosuppressive
factors environment
CD137
CD28
IL-2
IL-15CTLA-4
PD1
B7-1
Agonists Antagonists
T regulatory cellsMyeloid supp cellsIL-10, TGFbeta
Tumour vaccine
e.g. MAGE
or intrinsic (unknown)