chemotherapy pharmacology
TRANSCRIPT

Chemotherapy
Review
Present by Napannop Boonthanom, Pharmacist in Oncology Unit, Rajavithi Hospital
Slide by Suthan Chanthawong, Residency Pharmacist Faculty of Pharmaceutical Sciences, Khon Kaen University

Cell Cycle Phase
Synthesis of cellular Components required
for mitosis
Synthesis DNA precursors, proteins, etc.
Resting state (cell is not dividing)

Overview of Cell Cycle
teachline.ls.huji.ac.il/.../substance_x/q2a.html
Vinca,paclitaxel,docetaxel
Antimetabolite
Cell cycle (phase) Nonspecific agent
Alkylating agents
Anthracycline
Antitumor antibiotics
Asparaginase
Topo II Inh. :Bleomycin,Etoposide
Topo I Inh. : Irrinotecan, Topotevan

Biochemical classification
1. Alkylating agents 2. Antimetabolites 3. Antitumor antibiotics 4. Enzyme Inhibitors 5. Antimicrotubules 6. Miscellaneous

Cell cycle specific agents
M Vincristine, Vinorelbine, Vinblastin, Paclitaxel, Docetaxel
G0 Carmustine, Lomustine
G1 Asparagenase
S Cladribine, Cytarabine, Floxuridine (FUDR), Fludarabine, 5FU, Hydroxyurea, 6MP, MTX, Pentostatin, 6TG
G2 Bleomycin, Etoposide, Teniposide

Cell cycle non-specific agents
Busulfan Carboplatin Carmustine Chlorambucil Cisplatin Cyclophosphamide Decarbazine Dactinomycin
Daunorubicin Doxorubicin Idarubicin Ifosfamide Lomustine Mechlorethamine Melphalan Mitomycin C

Alkylating agents A. Nitrogen mustards
Chlorambucil Cyclophosphamide Ifosfamide Melphalan Mechlorethamine
B. Ethylenimines Thiotepa
C. Nitrosoureas Carmustine Lomustine Semustine Streptozocin
D. Alkyl sulfonates
Busulfan
E. Triazenes
Dacarbazine Temozolomide
F. Platinum analogues
Cisplatin Carboplatin Oxaliplatin

Alkylating agents
Mechanism of action (MOA):
Form covalent bonds Cross-linking between double DNA strands or
between bases in the same strand of DNA inhibit DNA replication
Cell-cycle non specific Damage DNA in any phase of the cell cycleGreatest effect seen in rapidly dividing cell

Alkylating agents

Nitrogen mustards

CTX and IFEX
MOA: Broadest spectrum of nitrogen mustards Prodrug: must be activated in the liver to active
metabolites Also form inactive metabolite Acrolein
IFEX metabolism occurs more slowly than CTX Require higher dose Higher risk of hemorrhagic cystitis
Prevention of Hemorrhagic Cystitis
by MESNA
Mercapto ethane sulfonate sodium Indication Hemorhagic cystitis 2nd to “Acrolein”
Hydration with frequently voiding May be sufficient with conventional dose of CTX Not with IFEX

MESNA
MOA: Sulhydryl group binds with acrolein Form a stable nontoxic product excreted in the urine Prevent bladder mucosa damage
Give before & at 4 and 8 hrs following IFEX dose Dose = 60% of IFEX dose Oral dose = 120% of IFEX dose due to bioavailability

CTX and IFEX
CTX Indication
NHL, HD, CLL, CML, ALL, AML, myeloma
Neuroblastoma, Breast, Ovarian, Retinoblastoma, NSCLC, SCLC, bladder, Sarcoma, Endometrial, BMT, SLE
IFEX Indication
NHL
Testicular, NSCLC, SCLC, Sarcoma

Cisplatin and Carboplatin
MOA: Alkylating-like agents which form a reactive
electrophile that covalently binds to DNA Indication:
Effective for the treatment of lung, testicular, bladder, breast, ovarian, colorectal, head and neck and gastric carcinomas

Cisplatin and Carboplatin
Dosage and Administration: Cisplatin:
Vigorous hydration with adequate urine flow rate Prehydration
1 L of NSS + 20 mEq KCl & 8mEq MgSO4 over 1-2 hrs to obtain a urine flow rate of > 100ml/hour
Posthydration consists of the same IV fluids
Carboplatin: Using the Calvert method: Dose(mg) = Target AUC x (CrCl + 25) Target AUC is 4-8
Oxaliplatin Cumulative peripheral neuropathy Acute (within the first two days), reversible (resolves
within 14 days), primarily peripheral symptoms that are often exacerbated by cold
Persistent (>14 days) that often interferes with daily activities such as writing, buttoning and swallowing symptoms may improve upon treatment
discontinuation
Minimal nephrotoxicity and ototoxicity Delayed hypersensitivity (800 mg/m2)


Cisplatin-induced N/V
Vomiting Center
Effector organs
Vestibular Cortex CTZ GI tract
AC
Histamine ??
5-HT3,D2, NK1 5-HT3,
NK1,
SP
Treatment/Prevention• Acute: Steroids + 5HT3 + Apprepitant
• Delayed: Steroids + Metoclopramide + Apprepitant • Anticipatory: Lorazepam
Risk Factors ?

Cisplatin-induced nephrotoxicities
Proximal tubules GFR decrease Risk factors High single doses cumulative doses Dehydration Preexisting renal impairment Concurrent renal toxic drugs
Prevention Aggressive hydration

Toxicities Common to most
Alkylating Agents
Nausea and vomiting Myelosuppression Alopecia Sterility/Infertility 2nd Malignancies

Toxicities unique to Specific
Alkylating Agents Hemorrhagic cystitis Cyclophosphamide,
Ifosfamide
Neurotoxicities Ifosfamide, Cisplatin
SIADH Cyclophosphamide, Ifosfamide
Nephrotoxicities, Ototoxicities
Cisplatin, Carboplatin
Antimetabolites
A. Folate antagonists
Methotrexate
Pemetrexed
B. Purine analogues
Cladribine Fludarabine Mercaptopurine Pentostatin
Thioguanine
C. Pyrimidine analogues Cytarabine Gemcitabine Fluorouracil Capecitabine

Antimetabolites
Structural analogues of natural compound MOA:
Replacing metabolites in key DNA/RNA replication molecules
Inhibit DNA/RNA function or synthesis Active on most rapidly proliferating cells

Folate antagonists
Methotrexate MOA: Inhibits the conversion of folic acid to tetrahydrofolate
by competitively inhibiting dihydrofolate reductase This results in inhibition of DNA synthesis via
blockage of thymidine and purine synthesis Effect on both cancer and normal cells Rescue by giving reduced folate (folinic acid) or
“leucovorin” Bypass the metabolic block induced by MTX


Methotrexate
Indication ALL,CNS Lymphoma, NHL, Bladder, Breast, Gastric,
Head and neck, Osteosarcoma, BMT
Drugs which are highly protein bound may displace MTX form albumin and increase toxicity sulfonamides, salicylates, phenytoin and tetracycline
NSAIDS compete for renal excretion of MTX and increase levels
Vitamin C will acidify the urine and may increase MTX levels

Pemetrexed
MOA: inhibit five major folate-dependent enzymes.
Thymidylate synthase Dihydrofolate reducatase Glycinamide ribonucleotide formyltransferase
Approved in February 2004 for malignant plural mesothelioma

Pemetrexed
Hanauske AR, et al. Oncologist 2001;6;363-373

Pemetrexed
Start vitamin supplements 1 weeks before initial dose of pemetrexed prevent BM supression Folic acid 350-1000 ug/day orally
(continuing for 21 days after last dose of pemetrexed) Vitamin B12 1000 ug IM q 9 weeks
Dexamethasone 4 mg twice daily start a day before andcontinue the day of and the day after to minimize cutaneous reactions
Purine analogue
Thioguanine (6-TG), Mercaptopurine (6-MP) MOA:
Converted to ribonucleotides inhibit purine biosynthesis
May be incorporated into DNA as false purines More so 6-TG
Administration: Oral form only
(variable bioavailability, reduced absorption by food)
6-TG and 6-MP
6-MP inactivated by xanthine oxidase Decrease dose 50% with allopurinol
Indication ALL, AML, CLL,Hairy cell leukemia
Toxicities Dose limiting leukopenia and thrombocytopenia Additional toxicities include:
Liver toxicity and jaundice (higher with 6-MP), stomatitis, mucositis, rash, N/V

Pyrimidine analogue: 5FU
MOA: Acts as a “false” pyrimidine inhibiting the formation
of the DNA base thymidine The main mechanism inhibit the enzyme
thymidylate synthase (TS), the rate limiting step in thymidine formation
Prodrug: must be metabolized to its active metabolite; fluorodeoxyuridine (F-dUMP)
Additionally, metabolites of 5-FU may incorporate into RNA inhibiting its synthesis

Fluorouracil (5-FU)
Administration Continuous infusion inhibit TS Intermitten bolus incorporate into RNA
Leucovorin co-administration Increase stability of FdUMP and TS complex Increase cytotoxicity to tumor cells
Indication: Colorectal, breast, gastric, pancreas, esophageal,
head and neck, cervical

Fluorouracil (5-FU)
Toxicities: Dose limiting leukopenia, thrombocytopenia and
anemia (with bolus administration) Dose limiting hand-foot and diarrhea (continuous
infusions) Additional toxicities include:
Skin discoloration Nail changes Photosensitivity Neurologic toxicity
Capecitabine
MOA:
Orally active prodrug of 5-FU
3-step conversion to 5-FU, the last step being
phosphorylation by thymidine phosphorylase (TP)
TP levels are reported to be higher in tumor cells then
normal tissues, therefore the systemic exposure of active
drug is minimized
Toxicities:
Dose-Limiting: Hand-foot syndrome, diarrhea
Additional toxicity: Nausea, vomiting, fatigue, rash


Cytarabine and Gemcitabine
MOA: Structural analogues of cytosine
Penetrated tumor cell : phosphorylated Ara-CTP
Inhibits DNA polymerase (strand elongation) : Acts as a chain terminate

Cytarabine and Gemcitabine
Indication: Cytarabine: ALL, AML, CML, CNS leukemia, NHL Gemcitabine: pancreatic, lung, breast, ovarian cancer
Toxicities: Dose limiting leukopenia and thrombocytopenia Additional toxicities: Nausea and vomiting, mucositis,
diarrhea, flu-like syndrome, rash High dose ara-C therapy (1-2 g/m2) excessive bone
marrow depression, CNS toxicity and conjunctivitis

Cytarabine and Gemcitabine
Additional issues: High doses of ara-C often given with
Allopurinol to prevent tumor lysis syndrome Dexamethasone eye drops 0.1% q 4-6 hrs for 7 days to prevent conjunctivitis
Gemcitabine should be administered within 30 mins
Prevent time dependent myelosuppression

Toxicities Common to most
Antimetabolites
Myelosuppression Mucositis Mild N/V Except high-dose cytarabine and high-dose
MTX may cause moderate to severe emetics complications

Toxicities Unique to
Specitic Antimetabolites Neurotoxicities High-dose cytarabine
(cerebella)
Nephrotoxicities High-dose MTX
Hepatotoxicities Chronic MTX administration
Rash and skin changes Cytarabine (Ara-C), Clardribine
Gastrointestinal Toxicities Fluorouracil (5-FU)

Oral mucositis
Occurs 5-7 days after CMT Supportive measures
Oral hygiene Stomatitis cocktail Pain control
Prevention Sucralfate suspension at
beginning of or prior to CMT Cryotherapy

Enzyme inhibitors TOPOISOMERSE II INHIBITORS
A. Anthracyclines Daunorubicin hydrochloride Doxorubicin hydrochloride Idarubicin Epirubicin Mitoxantrone
B. Epipodophyllotoxins Etoposide Teniposide
TOPOISOMERSE I INHIBITORS
C. Camptothecins Irinotecan Topotecan
Antitumor Antibiotic Anthracyclines
Daunorubicin hydrochloride Doxorubicin hydrochloride Idarubicin Epirubicin
Mitoxanthrone Antibiotics
Bleomycin Mitomycin Dactinomycin plicamycin
Doxorubicin hydrochloride

Anthracyclines
MOA: Inhibit Topoisomerase II Bind covalently to double strand DNA Insert between base pairs of DNA (intercalation) Free radical formation
Form hydroxy radical cleave DNA Require iron or copper

Anthracyclines
Doxorubicin ALL, AML, NHL, HD, Wilm’s tumor,
bladder, gastric, ovarian, thyroid, neuroblastoma, SCLC, osteosarcoma, sarcoma, KS, NSCLC, myeloma, endometrial
Daunorubicin AML, ALL, KS
Idarubicin AML
Epirubucin Breast

Anthracyclines
Dosage and Administration: Dose reductions required with hepatic impairment
dose by 50% if bilirubin levels 1.2-3.0 mg/dL dose by 75% for bilirubin levels > 3.0 mg/dL
All agents are potent vesicants and require immediate medical attention if extravasation occurs
Apply cold ice pack and evaluate for antidote use (99% DMSO 1-2% ml applied to site q 6 hours for 7-14 days)
Doxorubicin red discoloration of the urine and tear

Mitoxanthrone
Anthracycenedione (synthetic agent) MOA: similar to anthracyclines but
Lacks ability to produce free radicals
Indication: AML, prostate, NHL, HD, breast Toxicities: Dose limiting leukopenia. Additional toxicities include:
Nausea and vomiting alopecia cardiac toxicity
Patients’ urine may turn blue for 24-48 hrs after infusion

Mitomycin C
Fermentation product form streptomyces MOA: similar to alkylating agents may also produce
super oxide free radicals Indication:
Gastric, Pancreas, Bladder, Breast, Colorectal, Esophagus NSCLC

Toxicities common to most
Antitumor ATB
Myelosuppression (except bleomycin) Mucositis Nausea & Vomiting (except bleomycin) Alopecia Vesicant (except bleomycin & mitoxanthrone)

Extravasation of cytotoxic
Common Vinca alkaloids Anthracyclines
Management Withdraw CMT Antidote Supportive care
Cold/Warm compress Symptom management
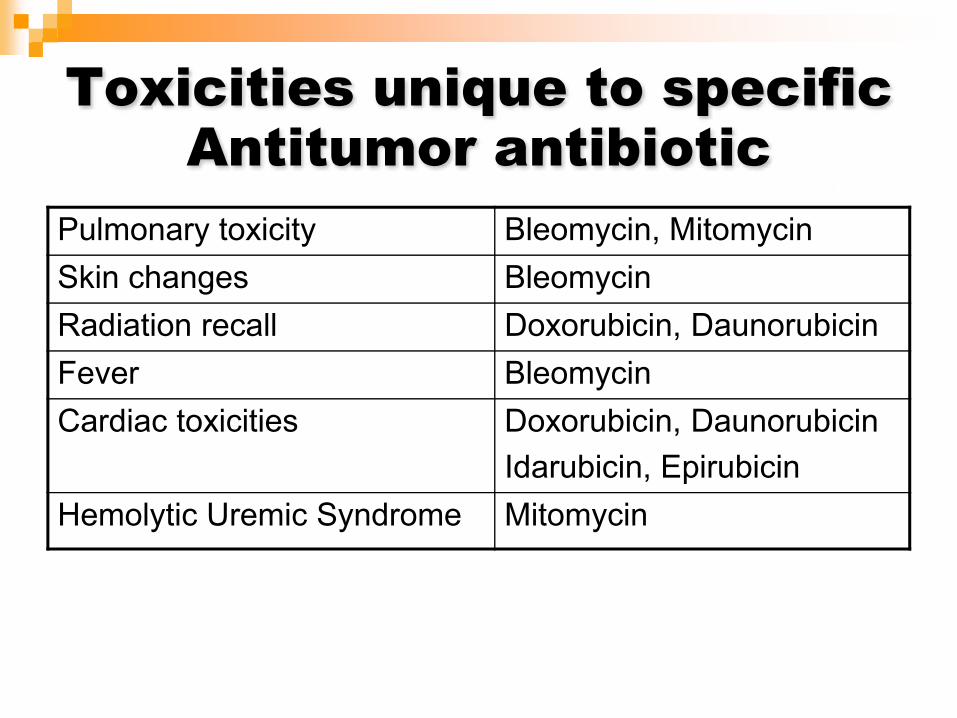
Toxicities unique to specific
Antitumor antibiotic Pulmonary toxicity Bleomycin, Mitomycin
Skin changes Bleomycin
Radiation recall Doxorubicin, Daunorubicin
Fever Bleomycin
Cardiac toxicities Doxorubicin, Daunorubicin Idarubicin, Epirubicin
Hemolytic Uremic Syndrome Mitomycin

Anthracyclines
Rhythm disturbance
Cardiomyopathy Cumulative dose
doxorubicin < 450-550mg/m2
daunorubicin < 450-550mg/m2
Idarubicin < 150 mg/m2
Epirubicin < 900mg/m2
Shan K et al. Ann Intern Med. 1996;125(1):47-58.

Anthracyclines related
cardiac-toxicity
Risk factors Previous cardiac irradiation Elderly Very young Females Preexisting HTN or cardiac disease Peak concentration
Idarubicin less cardiotoxicity

Prevention of anthracyclines
cardiotoxicity
Dexrazoxane (Zinecard) Chelation of divalent ions e.g. ferric iron Prevent free radical formation FDA approved or breast cancer with cumulative
dose 300 mg/m2 with benefit from doxorubicin
Liposomal doxorubicin and daunorubicin Liposomes are not taken up as freely as free drug into the cardiac tissue

Relative cardiotoxicity of
anthracyclines
Drug Relative cardiotoxicity
Cumulative (mg/m2)
Doxorubicin
bolus weekly 24 hr infusion
1.000.700.64
400550550
Daunorubicin 0.75 800
Idarubicin 0.53 150
Epirubucin 0.66 900
Mitoxanthrone 0.50 160

Epipodophyllotoxins
Etoposide and Teniposide MOA:
Form complexes with topoisomerase II and DNA Inhibit strand breakage and rejoining for replication Cell cycle specific in S and early G2 phase
More effective in divided doses
Teniposide more potent at stimulating DNA cleavage

Etoposide and Teniposide
Indication Etoposide: testicular, SCLC, AML, HD, NHL,
NSCLC, gastric, BMT, KS Teniposide: ALL, neuroblastoma, NHL
Etoposide IV infusion should be infused over 30-60 minutes to
avoid hypotension IV solution should be diluted to a concentration
< 0.4 mg/ml Oral dose is 2x greater than the IV

Etoposide and Teniposide
ADRSMyelosuppression N/V (mild and more with oral form) Alopecia Mucositis Hypersensitivity Hypotension prevent with slow infusion 2nd leukemias
AML in 1-3 years

Topoisomerase I Inhibitor (camptothecin)
Irinotecan and Topotecan Semisynthetic derivatives of camtothecin Plant derivative MOA
Inhibit topoisomerase I Stabilize DNA single strand breaks and inhibit religation
Indication Irinothecan: colorectal, NSCLC, cervical Topotecan: ovarian, SCLC

Irinotecan and Topotecan
ADRMyelosuppression: neutrophil and platelets Diarrhea: irrinothecan, acute or delayed N/V – severe with irinotecan, mild with topotecan Alopecia Rash Low-grade fever Malaise mucositis

Antimicrotubules
A. Vinca alkaloids Vinblastine Vincristine Vinorelbine
B. Taxanes Paclitaxel Docetaxel

Vincristine, Vinblastine and Vinorelbine
Products derived form periwinkle (Vinca) plant
MOA: Act as mitotic inhibitor or “spindle poison” bind to tubulin Disrupt the normal balance between polymerization and
depolymerization of microtubules M phase arrest
Dosage and Administration Biliary excretion, require adjustments for hepatic impairment.
50% dose reduction for blilrubin > 1.5 mg/dL, 75% reduction for bilirubin > 3.0 mg/dL

Vincristine
ALL, HD, NHL, myeloma, SCLC, brain, breast, KS, sarcoma, osteosarcoma, neuroblastoma, wilm’s tumor
Do not give IT (IV max 2 mg) ADRs
Neurotoxicities Peripheral Autonomic Decrease deep tendon reflex (DTRs)
Extravasation warm compress + hyaluronidase Constipation SIADH (Syndrome of Inappropriate Anti-diuretic Hormone) Alopecia
Vinblastine
HD, NHL, testicular, KS, breast, NSCLC, bladder, prostate, renal cell
Do not give IT ADRs
Myelosuppression Extravasation warm compress + hyaluronidase Less neurotoxicities Constipation Alopecia

Vinorelbine
Semisynthetic NSCLC, breast, ovarian, HD, prostate Do not give IT ADRs
Myelosuppression Neurotoxicities
Intermediate Paresthesia Loss of deep tendon reflex (DTRs)
Extravasation warm compress + hyaluronidase Constipation N/V Alopecia

Taxanes: Paclitaxel and Docetaxel
Paclitaxel from bark of Pacific Yew tree Docetaxel in semisynthetic MOA:
Bind to tubulin but not interfere with tubulin assembly Promote microtubule assembly Interfere with microtubule disassemble by inducing tubulin polymerization

Paclitaxel and Docetaxel
MOA: Form stable but not functional microtubules Also act by promoting apoptosis
Docetaxel more active taken up (3X greater) Retained intracellularly for longer period of time
(5-6 hrs) Therefore, considered 2-4X more potent than paclitaxel

Paclitaxel and Docetaxel
ADRsMyelosuppression
Paclitaxel: related to duration of infusion, higher doses, combination CMT and q 3 weeks VS weekly regimen
Hypersensitivity More with paclitaxel due to 50% cremophor Premedication and infuse over 24 hrs
Bradycardia and hypotension

Paclitaxel and Docetaxel
Patients must receive premedication prior to receiving paclitaxel to decrease hypersensitivity reactions Dexamethasone 20 mg PO or IV prior to treatment
Before 12, 6 and 0 (15-30 min) hr
Diphenhydramine 50 mg and an H2 blocker (ranitidine 50 mg) IV 30 minutes prior tx
Patients receive both pre and postmedication with docetaxel to prevent fluid retention associated with use Dexamethasone 8 mg PO BID starting 1 day prior to
treatment and continuing for 2 additional days

Paclitaxel and Docetaxel
ADRs Peripheral neuropathy
> 175 mg/m2 (paclitaxel)
Longer infusion, History of Ethanol, DM Mucositis, N/V (mild) Alopecia Fluid retention
docetaxel (Wt gain, edema, pleural effusions) Rash: docetaxel (PPE, maculopapular) Nail changes: docetaxel

Antimicrotubules drug
http://www.cancerquest.emory.edu/images/mitosis-cycai.gif
Taxanes
Vinca alkaloids

Miscellaneous agent A. Asparaginase B. Hydroxyuria
L-asparagenase
Enzyme produced by bacteria Responsible for the degradation of asparagenase
L-asparagenase Nonessential amino acid Synthesized by most cells except certain human
malignant cells
Conjugation with polyethylene glycol (PEG) Prolong T1/2 Allow for lower doses Less frequent administration

L-asparagenase
Indication: ALL
ADRs: Anaphylaxis (PEG form is less immunogenic) Fever/chills Decrease clotting factors Decrease insulin Pancreastitis Somnolence or confusion Myelosuppression Nausea
L-asparagenase
Test dose 0.1 ml of dilute 20 unit/ml solutions (~2 units) prior to
initial administration and observe 1 hr for a wheal or erythema
http://ethnomed.org/clin_topics/tb/firland/screening/latent_tb_faqs/latent_tb_faqs_clip_image023.gif

Hydroxyurea
Antimetabolite but not a nucleoside analogue MOA:
Inhibit ribonucleotide reductase, enzyme required to convert ribonucleotided to the deoxy form for the DNA synthesis and repair
Stop DNA synthesis without interfering with formation of RNA or protein
Cell accumulate in the S phase, only short DNA strand are produced

Hydroxyurea
Indication CML, melanoma, ovarian, head and neck
ADRs: Myelosuppression N/V Anorexia Mucositis Skin-hyperpigmentation and radiation recall Erythema of hands and face
Hormonal agents
A. Antiestrogens Tamoxifen citrate Megestrol acetate
B. Aromatase inhibitors Aminoglutethimide Anastrozole Letrozole Exemestane
C. LH-RH analogues Goserelin Leuprolide
D. Antiandrogens Bicalutamide Flutamide Nilutamide
E. Miscellaneous hormonal agents Estramustine

Targeted therapies A. Monoclonal antibodies
Gemtuzumab Alemtuzumab Rituximab Ibritumomab Tositumomab Trastuzumab Cetuximab
B. Tyrosine kinase inhibitors Erlotinib Gefitinib Imatinib mesylate Sunitinib malate


Thank you for your attention
and any questions???