chest x rays
TRANSCRIPT

In the Name of Allah, The Most Merciful, The Most Beneficent

CHEST X-RAYSAND THEIR
INTERPRETATION
PRESENTED BY
SAAD SALEEM
By This Presentation We Will Learn• Objectives of a chest x-ray
• Views of chest x-rays• Interpretation of chest x-rays• Specific diseases which can be identified in
chest x-rays
Objectives Of A Chest X-ray
• To identify normal cardiothoracic anatomical structures demonstratable on x-rays
• To recognize radiographic signs of lung pathologies
Views Of Chest X-rays• There are basically two types of views which can
be taken in chest radiographs• 1: STANDARD VIEWS A) Posterioanterior (PA)B) Lateral C) Anterioposterior (AP)• 2: SPECIAL VIEWSA) Lordotic viewB) Inspiration and expiration viewsC) Reverse Lordotic viewD) ObliqueE) Supine CXRF) Lateral decubitus film

Interpretation Of Chest X-rays
The key to successfully interpretate any radiograph is to be systematic
Identification: Correct patient, date, time, MR # (if applicable), and examination
Side marker: Where is the side marker located
Technique: Concentrate on technical factors such as:
• Is examination complete• Requested views present or not• Is the entire anatomical area included on
the films (projection, position, penetration, rotation, and inspiration)

Systemic AnalysisSystemic Analysis• Soft tissues, chest wall.• Bones; shoulder girdle, spine rib cage.• Diaphragm shape, position, sub-diaphragmatic
abnormalities.• Review abdomen for bowel gas, organ size, abnormal
calcifications, and free air.• Plastic; OETT, lines, and tubes.• Pacemaker.• Review mediastinum: size and shape; trachea
(position, carina, trachea should be central); margins (ascending aorta, right atrium, left subclavian artery, aortic arch, main pulmonary artery, left ventricle).
• Heart size and shape: width of heart should not be greater than 50% of the width of the rib cage.
• Review hila: normal relationships of hila should be in mind, size.
• Parenchyma: now the lungs; divide entire chest into three parts, upper, middle, and lower thirds, then methodically compare the right and left sides of each lung section looking for asymmetry. Compare lung sizes, aeration, vascular distinctness, and abnormal opacities.
• Pleura: costophrenic and cardiophrenic angles, thickening fissures (if seen).

Normal Chest X-ray

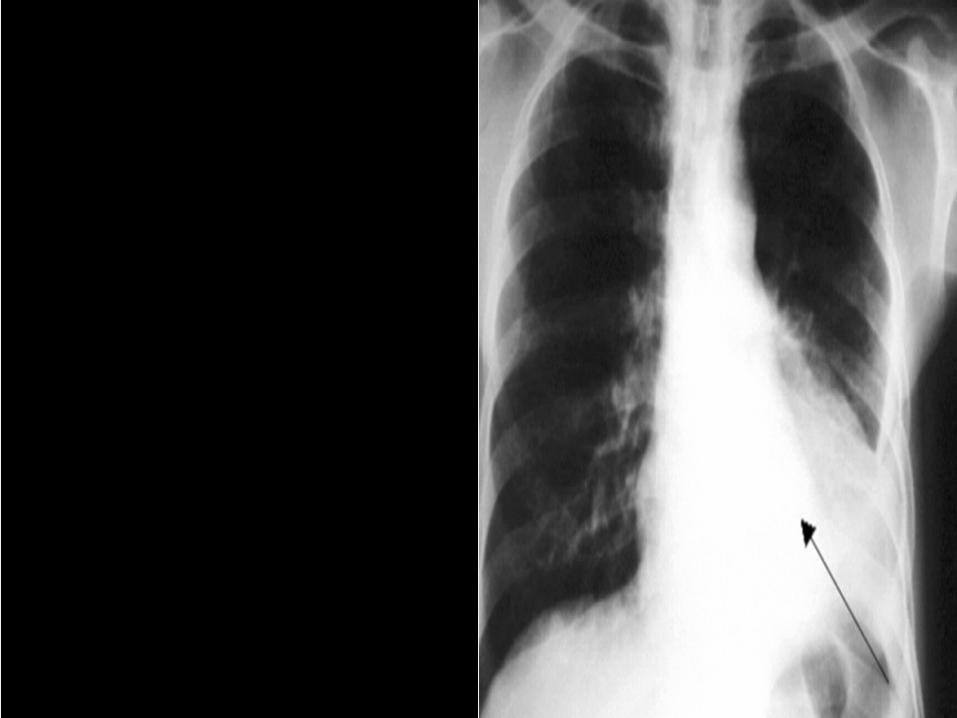
COLLAPSE (ATLECTASIS)Volume loss due to alveolar collapse or failure to expand
causing increased opacification of radiographTypes• Obstructive • Compressive• Cicatrization• Adhesive• PassiveFeatures of lobar collapse• Shift of fissures• Area of increased opacity• Crowding of vessels• Tracheal displacement towards the side of collapse• Hilar shift• Mediastinal shift towards the side of collapse• Elevation of hemi-diaphragm• Herniation of the opposite lung across midline


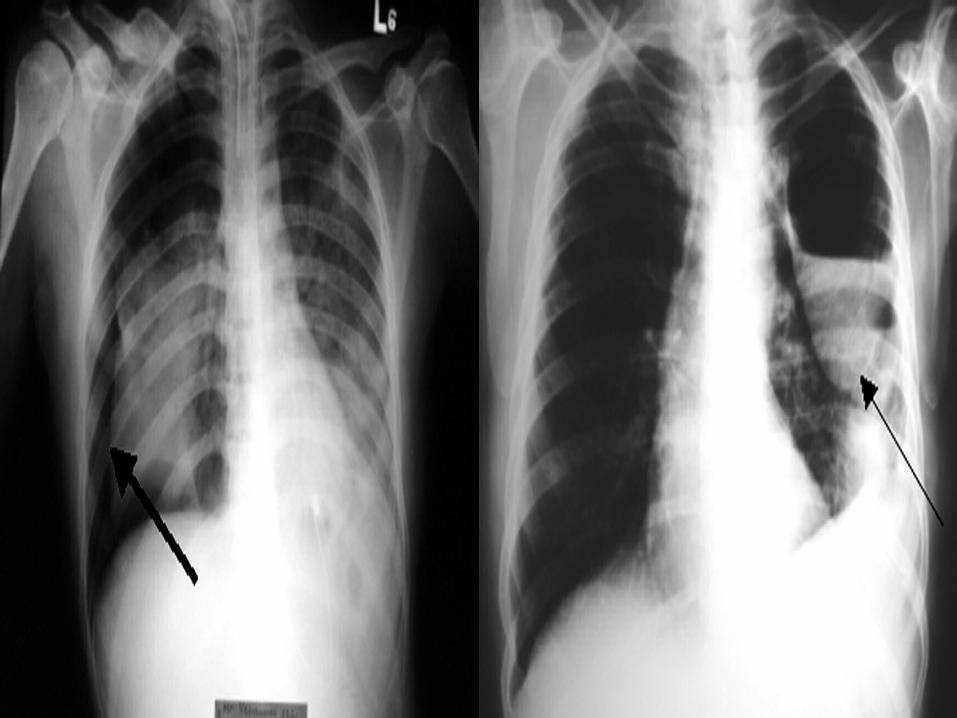
PLEURAL EFFUSION
• Defined as fluid in pleural space.• Fluid can be transudative or exudative
in nature.• Various types of effusions include:1. Hydrothorax; transudative effusion i.e.
CHF, hypoalbuminemia2. Pyothorax; pus in pleural space i.e.
empyema from pneumonia3. Hemothorax; blood4. Chylothorax; chyle
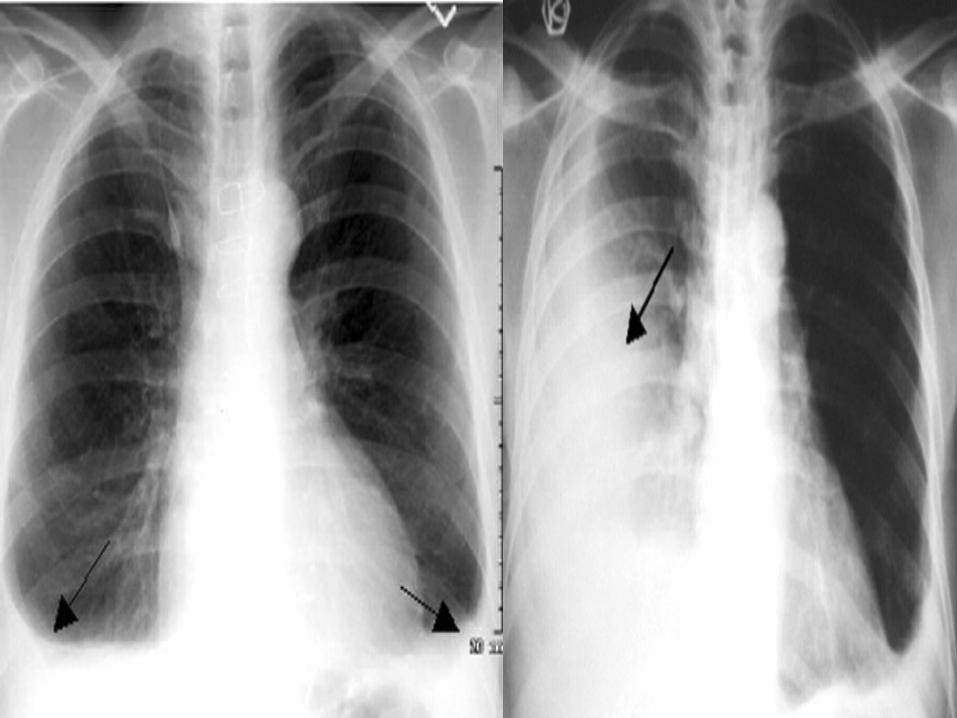

PNEUMOTHORAX
• Air enters pleural space• Two types1. Spontaneous pneumothoraces2. Traumatic pneumothoraces
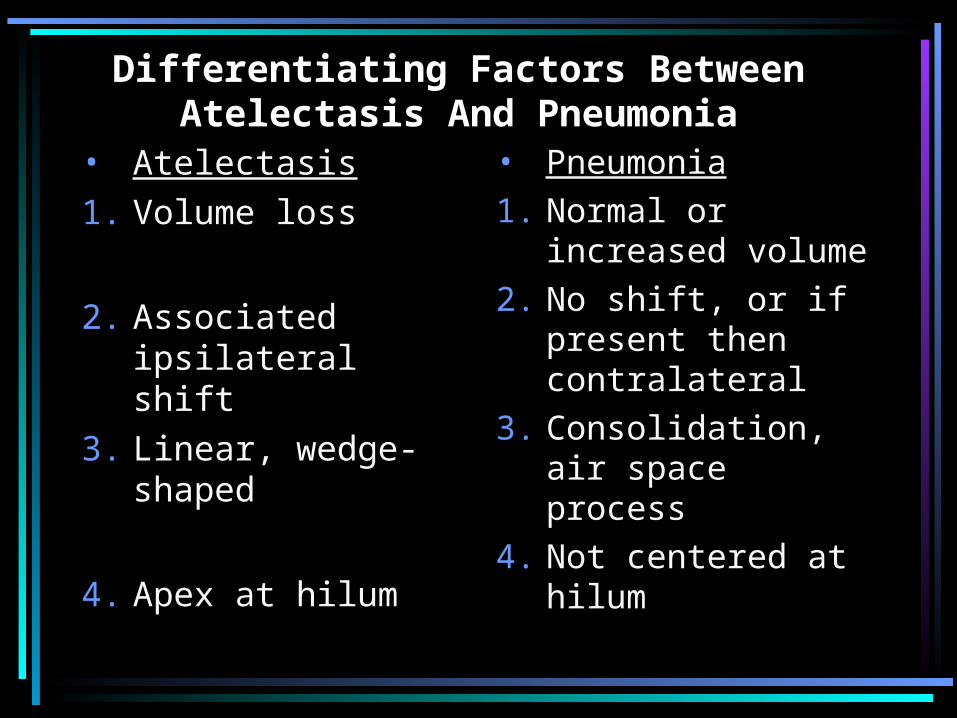
Differentiating Factors Between Atelectasis And Pneumonia
• Atelectasis1. Volume loss
2. Associated ipsilateral shift
3. Linear, wedge-shaped
4. Apex at hilum
• Pneumonia1. Normal or
increased volume2. No shift, or if
present then contralateral
3. Consolidation, air space process
4. Not centered at hilum

Pneumonia Left lung collapse

Left Upper Lobe Collapse Pleural Effusion Pulmonary Edema

ARDS
