childhood malaria in a region of unstable transmission and high human immunodeficiency virus...
TRANSCRIPT

Childhood malaria in a region of unstable transmission and high human immunodeficiency virus prevalence: An EBM Review
Sonia Seng, M.D.MSSM Global Health Center

HIV and Malaria Co-infection Why is this interaction important in global
health? How does co-infection affect the disease
process? What is the current evidence in different
populations?• Adult population• Pregnant Women• Children
EBM review PIDJ 2003 How does this apply to my patients?

Scope of the disease
HIV: 38.6 million people worldwide living with HIV at the end of 2005. In sub-Saharan Africa, 6.5 million people die of AIDS and 9,500 contract HIV on a daily basis. In 2003, 600 K children were newly infected.
Malaria: 1 million people die of malaria yearly. >90% deaths take place in tropical Africa. Malaria is the leading cause of mortality in children < 5 years old. In 2002, malaria accounted for 10% child deaths in Sub-Saharan Africa. Malaria costs Africa 12 billion USD in lost production yearly
UNAIDS 2006 Report Global AIDS Epidemic

Distribution of Malaria and HIV
Together, they are responsible for 4 million deaths annually.
The burden of co-infection occurs in sub-Saharan Africa, South- East Asia, and Latin America. Prevalence vary widely in these geographical locals.
HIV and Malaria Interactions and Implications: Conclusions of a Technical Consultation Convened by WHO, 23-25 June 2004

HIV and Malaria Co-infection Most severely affected areas
Mozambique, Zambia, Zimbabwe, Malawi, Central African Republic. Here, 90% population is exposed to malaria and 10% are HIV +
South Africa has the highest prevalence of HIV and a lower burden of malaria but increased risk of dual infection with frequent malaria epidemics. South Africa and Namibia have HIV prevalence 20%. Rates > 35% Botswana and Swaziland
Epidemics Kwazulu-Natal
Korenromp et al., Malaria attributable to the HIV epidemic, sub-Saharan Africa. Emerg. Infect Dis. 2005 Sep 11 (9): 1410-9
HIV and Malaria Interaction
T cells limit parasite maturation in liver Increased incidence and density of rbc stage
of parasites in HIV+ patients with malaria HIV may decrease acquired immunity to
malaria Increased incidence and severity of malaria P falciparum may activate T cells Increased rates of clinical treatment failure

Limitations of Earlier Studies:
Malaria = fever No CD4 counts reported Population studied:
– stable vs unstable malaria transmission – Adults, pregnant women, and children
Hewitt et al., Interactions between HIV and malaria in non-pregnant adults: Evidence and Implications. AIDS 2006,
20: 1993-2004.

Pregnant Women
– 25 million pregnant women exposed to malaria yearly – HIV prevalence among pregnant women is 9% , 500 K will
have malaria during pregnancy – HIV alters time course so women are more susceptible to
malaria during their entire pregnancy – Increased risk of anemia, pre-term birth and IUGR in HIV+
pregnant women with malaria– Children born to these women more likely to be VLBW and
are more likely to die during infancy – Poorer response to malaria prophylaxis and treatment in HIV
+ women – Increased adverse drug reactions if fansidar and
cotrimoxazole are taken together (sulfas)

Adult Men and Non-pregnant Women: HIV and malaria co-infection
– Increases infection rate– Increases parasite density– Causes severe/complicated malaria– Decreases response to treatment
In sub-Saharan Africa, with an HIV prevalence of 8%, Adult malaria secondary to HIV is 4% parasitemia and 5% clinical malaria. In Southern Africa, where the HIV prevalence is 30%, these rates increase to 20% and 30%.
Whitworth J et al, Lancet 2000

Adult Men and Non-pregnant Women
Increased frequency of clinical malaria in patients with HIV:– Uganda: 1347 HIV + : Malaria fever rates inversely related to
CD4 counts and parasite density increased with decreasing CD4 counts.
– Malawi: 660 HIV + Adults: Clinical malaria rates of 391 and 230 / 1000 pyo for CD4 <200 and > 500 p <0.03.
– A retrospective RCT in Uganda of >2000 patients presenting with fever and positive thick blood smears found a > 6 fold increased risk for new falciparum infections in HIV + patients
Hewitt et al., AIDS 2006
Kemya et al., JID 2006

Adult Men and Non-pregnant Women
HIV/AIDS augments malarial illness – A prospective cohort study of 613 patients in
South Africa in 2000 demonstrated increased risk of severe malaria and death in HIV + population with OR 1.8 (CI, 1.2-2.8) and 5.3 (CI, 2.5-11.4) respectively.

Adult Men and Non-pregnant Women
Patients with severe immunosuppression are at increased risk of treatment failure with anti-malarial therapies. – Uganda: In a retrospective RCT performed in 7 sites in Uganda
with 1965 patients randomized to receive 1 of 3 treatment regimens (chloroquine, SP, amodiaquine, artesunate) HIV + individuals (n =95) had increased treatment failure with a HR (6.35 CI, 1.64-24.5) p< 0.007 for new uncomplicated infections.
– A retrospective case note review study of 142 HIV + patients and 58 HIV – pts tx with chloroquine or SP in Uganda from 1987-89 found no significant difference response to malaria therapy as defined by disappearance or decreased parasitemia by 90% after initial standard treatment.

Molecular genotyping demonstrated that there was no difference in treatment failure for recrudescent infections.
Adult Men and Non-pregnant Women
Prophylaxis with anti-malarial therapy and ART is cumulative in HIV + adults
– A recent study in Uganda found that the use of co-trimaxole prophylaxis, ART, and insect treated bed nets was cumulative in HIV + adults with reduction of febrile parasitemia 76% (95% CI, 62-85), 92% (CI, 83-96%), and 95% (CI, 92-97) Lancet, 2006
Adult Men and Non-pregnant Women
Acute malaria may increase HIV VL– A prospective cohort study evaluating VL before, during, and after
malarial fever in HIV + adults in Malawi found a mean increase in VL of 0.25 log copies/ml (CI 0.1-0.4) with return of VL to baseline levels 8 weeks after treatment. 13 patients with CD4 >300 with fever and high parasite density had a mean increase of 0.82 log copies /ml.
– Evidence does not support that malaria infection affects HIV
disease progression
Children
WHO review on mortality data from surveillance sites in rural Africa highlights the potential of HIV and malarial co-infection as a major global health burden in children <5 :– Mortality generally decreased 1980-90’s– Malaria attributable mortality in this age group increased– Proportion of deaths from malaria in children < 5 increased
from 18- 37%– In 1999, HIV infection caused 7.7% of deaths in children
Data gathered on the implications of HIV and malaria co-infection are largely inconclusive
The definition of HIV in young children likely contributes to these results

Children
Severe malaria is associated with anemia and increased need for blood transfusions . In children this poses an increased risk for transmission of HIV.
Fogerty International Center NIH August 2003

Children
Uganda 1997: HIV + children had no increase in incidence of malaria (p= 0.001) or differences in parasite densities (p< 0.02) compared to HIV – controls.
Kinshasa Zaire 1990: Increased rates of clinical malaria (p=0.003) and higher parasite densities (p = 0.04) in children with advanced immunosuppression.
Kalyesbula et al., Ped Infect Dis. J 1997
Colebunders et al., Journal of Infection 1990

EBM Review
Childhood malaria in a region of unstable transmission and high human immunodeficiency virus prevalence
Grimwade et al., Pediatric Infect Dis J, 2003;22:1057-63
Was there a representative and well-defined sample of
patients in a similar point in the course of their disease?
All patients <14 years old with an acute febrile illness and symptoms typical of malaria (acute onset of fever, headache, diarrhea, confusion, seizure, respiratory difficulty, jaundice, impaired level of consciousness) presenting to one of four community based clinics + Hlabisa district hospital from Jan to May 2000

Was there a representative and well-defined sample of patients in a similar point in the course of their disease?
Was there a representative and well-defined sample of patients in a similar point in the course of their disease?
All were assessed for P falciparum malaria rapid horseradish peroxidase ag malaria test
Children <14 with + test and consent were enrolled HIV testing anonymously with blood spot on filter
paper results linked to clinical data Thick blood smear was taken on a subset of patient
Was follow up sufficiently long and complete? Children were treated according to national
guidelines and by severity of illness Well + ambulatory (no vomiting) = outpatient +
sulfadoxinepyrimethamine (Fansidar) Less well + did not respond to oral therapy =
Hospitalized Severe disease or complicated disease or vomiting =
inpatient + iv quinine There was no mention of follow up or length of
treatment, especially those treated as outpatients.

Were objective and unbiased
outcome criteria used? Primary outcome measures: presence of severe
complicated disease and death from malaria HIV testing performed at outside lab was blind to
clinical data Blood spots tested for HIV with commercial kit
Wellcozyme GAC-ELISA Indeterminate results were repeated and excluded if
these results persisted Slides were read in duplicate by experienced
microscopists
Were objective and unbiased outcome criteria used?
During the early phase, thick film prep was poor. Parasite density was measured semi-quantitatively.
Parasites were counted against 200 wbc and scored + for 1-20, ++ for 21-250, +++ for 251-500, ++++ for >501
Gametocytes were counted to 200 wbc and scored + for 1-10, ++ for 11-30, +++ for 31-100, ++++ for >100

Was there adjustment for important prognostic factors? HIV Ab + status and < 1 year old = HIV likely Sickle Cell Disease and Trait CD4 count, Viral Load Age – why >14 large range within this group as
severe malaria tends to present in those < 5 years old

How large was the likelihood of the outcome of the events? 729 enrolled + malaria
Ag + appropriate clinical history
66 had incomplete clinical history or laboratory data
663 children were included in analysis

HIV Prevalence
<1 (n= 59) >1 (n=604)
HIV likely +
HIV - HIV Ab + HIV -
8 (14) 51 (86) 60 (10) 544 (90)
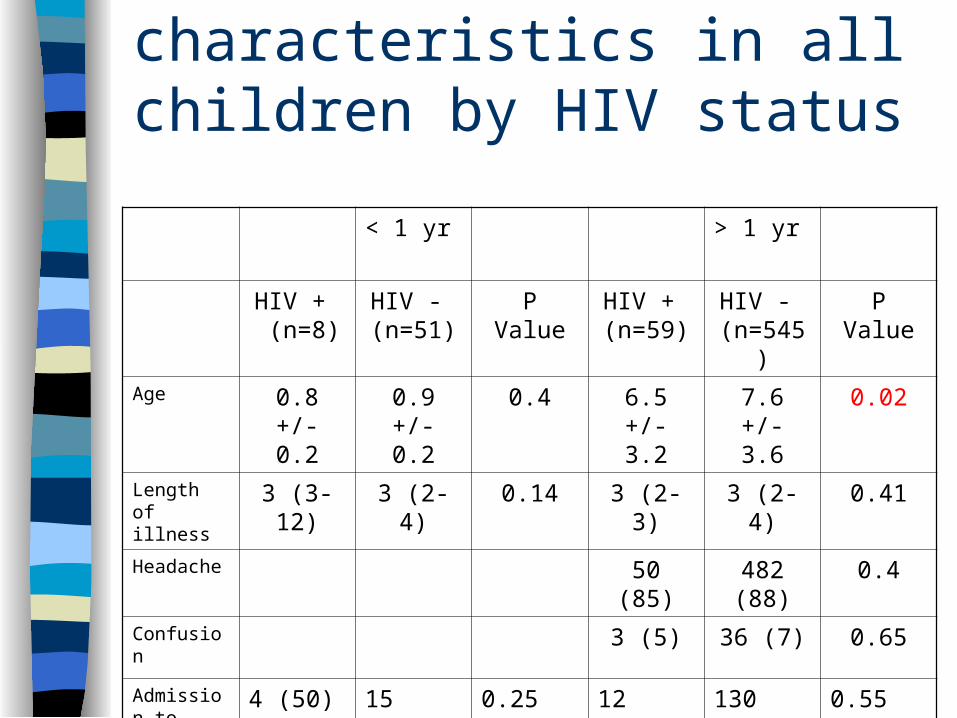
Presentation characteristics in all children by HIV status
< 1 yr > 1 yr
HIV + (n=8)
HIV - (n=51)
P Value HIV + (n=59)
HIV - (n=545)
P Value
Age 0.8 +/- 0.2
0.9 +/- 0.2
0.4 6.5 +/- 3.2
7.6 +/- 3.6
0.02
Length of illness
3 (3-12) 3 (2-4) 0.14 3 (2-3) 3 (2-4) 0.41
Headache 50 (85) 482 (88) 0.4
Confusion 3 (5) 36 (7) 0.65
Admission to Hosp.
4 (50) 15 (29) 0.25 12 (21) 130 (24) 0.55

How large was the likelihood of the outcome of the events? Children w HIV were significantly younger. When
data was grouped by HIV status including both age groups, p value was 0.01 Authors suggest that is representative of the natural progression of HIV in this setting.
There was no significant assoc between HIV and clinical symptoms reported including fever, vomiting, headache, confusion, rigors, malaise.
The duration of illness and rate of admission were similar to both groups.

Parasite Density and HIV status:
TK films done in 90% -- poor quality Parasite densities available in 42% cases Neither semi-quantitative asexual trophozoite
nor gametocyte densities varied according to HIV status
When identification was possible –all were p. falciparum
Higher parasite burden was associated with severe disease p<0.08
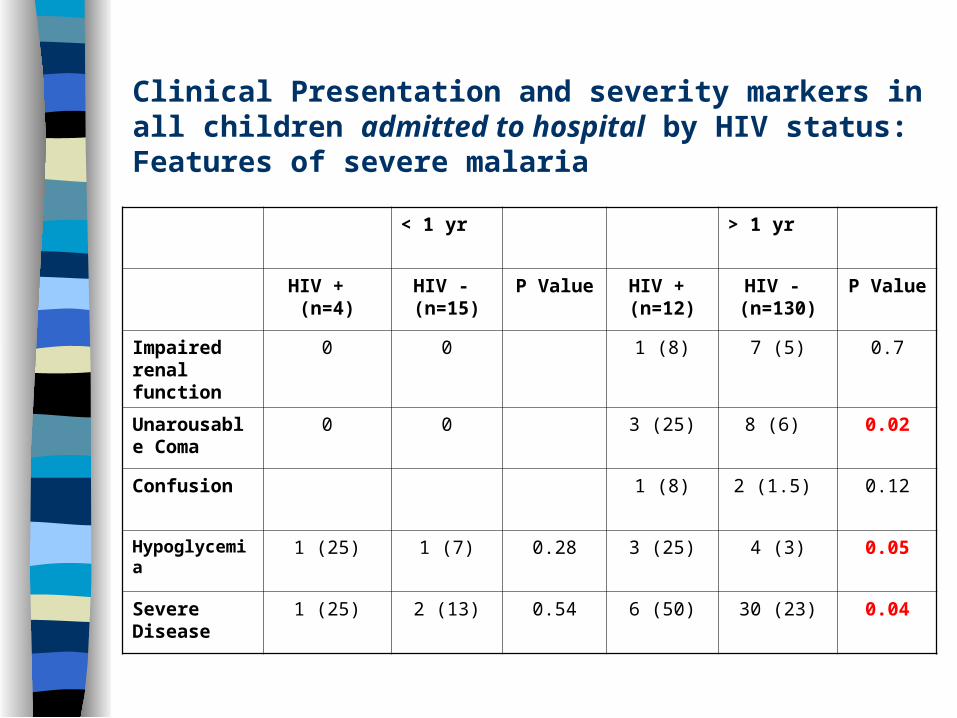
Clinical Presentation and severity markers in all children admitted to hospital by HIV status: Features of severe malaria
< 1 yr > 1 yr
HIV + (n=4) HIV - (n=15)
P Value HIV + (n=12)
HIV - (n=130)
P Value
Impaired renal function
0 0 1 (8) 7 (5) 0.7
Unarousable Coma
0 0 3 (25) 8 (6) 0.02
Confusion 1 (8) 2 (1.5) 0.12
Hypoglycemia 1 (25) 1 (7) 0.28 3 (25) 4 (3) 0.05
Severe Disease
1 (25) 2 (13) 0.54 6 (50) 30 (23) 0.04

Clinical Presentation and severity markers in all children admitted to hospital by HIV status: Outcome
< 1 yr old > 1 yr old
HIV + (n=4)
HIV - (n=15)
P Value HIV + (n=12)
HIV - (n=130)
P Value
Received iv quinine
2 (50) 5 (33) 0.54 6 (50) 42 (32) 0.22
Parental Abx
3 (75) 6 (40) 0.3 4 (27) 25 (19) 0.27
Length of stay
7 (4-14) 6 (4-9) 0.92 8 (6-12) 6 (4-7) 0.04
Died 1 (25) 1 (7) 0.39 1 (8) 4 (3) 0.35
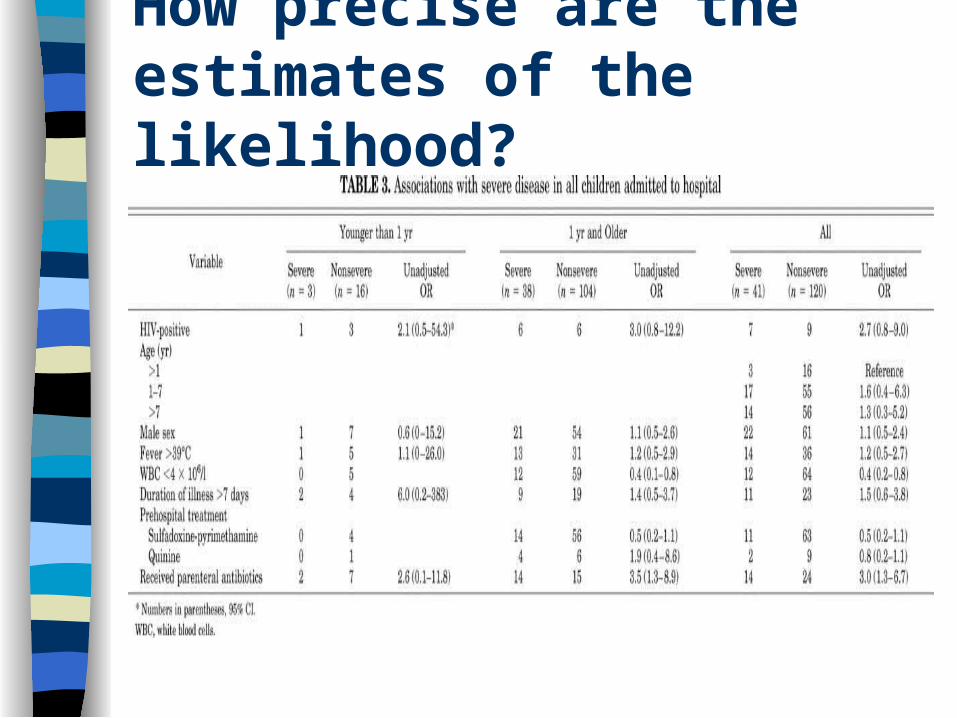
How precise are the estimates of the likelihood?
How precise are the estimates of the likelihood?
Logistic regression analysis comparing multiple factors and presence of severe disease:
– IV Abx use assoc w severe disease adjusted OR 3.0 (95% CI, 1.2-7.7)– Wbc < 4000/ mm3 assoc with non severe disease adjusted OR 0.27 (95%
CI, 0.1- 0.7)
Logistic regression analysis comparing multiple factors and hospital survival:
– Coma adjusted OR 50.5 (95% CI, 1.3 to 1851)– Low wbc 142 (95% CI, 3.1 – 6577)– Age < 1 0.06 (95% CI, 0.01 – 0.98) independent predictors of poor outcome – HIV in children > 1 yr of age 10.2 (95% CI, 0.8 – 138.5)
Conclusion
In the preliminary analysis, children > 1 yr old that were HIV + were more likely to present with severe disease, specifically unarousable coma and hypoglycemia. In the logistic regression analysis, HIV status did not emerge as a significant factor associated with severe disease or mortality in both age groups.
HIV was not a major risk factor for death and few children died HIV + and HIV – patients presented with similar symptoms In general HIV + patients were younger Parasite density was not altered by HIV status
Will the results help me in caring for my patients? The clinical course of malaria for HIV infected
children may be different than that for adults and pregnant women.
There is no difference in the presentation, clinical course, or mortality of HIV infected children between 1-14 years old with acute malaria.
While results for those <1 year old demonstrated no significant difference between HIV negative and “HIV likely” with acute malaria, it is difficult to draw any conclusions given inadequate follow up as to their HIV Ab status.

Were study patients similar to my own?
Important to note that the sites were specifically targeted to be most inclusive of a population with high HIV burden in an area with unstable malaria transmission.
This study represents first infection when children have not developed immunity to P. falciparum during acute malaria. The study does not represent larger burden of malaria in endemic areas.

Will the results lead to directly selecting or avoiding therapy?
Yes, this study demonstrates that unlike adults and pregnant women, children with HIV are not more susceptible to a more severe course of malaria than HIV negative counterparts. Given the burden of severe disease in this age group, WHO recommends insecticide treated nets.
Copyright WHO Pierre Virot
Are the results useful for reassuring or
counseling patients?
May reinforce WHO emphasis of insecticide treated nets to populations vulnerable to malaria.
Results are not applicable to patients < 1 yr old who need further follow-up to discern HIV Ab + status and course.

Bibliography
UNAIDS 2006 Report Global AIDS Epidemic HIV and Malaria Interactions and Implications: Conclusions of a Technical Consultation
Convened by WHO, 23-25 June 2004 Brentlinger et al. , Challenges in the concurrent management of malaria and HIV in
pregnancy in sub-Saharan Africa. Lancet Infect Dis. 2006; 6: 100-11 Colebunders et al., Incidence of malaria and efficacy of oral quinine in patients recently
infected with human immunodeficiency virus in Kinshasa, Zaire Journal of Infection, Volume 21, Issue 2, September 1990, Pages 167-173
Kemya et al.,Effect of HIV-1 Infection on Antimalarial Treatment Outcomes in Uganda: A Population Based Study. JID 2006;193;9-15.
Korenromp et al., Malaria attributable to the HIV epidemic, sub-Saharan Africa. Emerg. Infect Dis. 2005 Sep 11 (9): 1410-9.
Kublin HIV Infection and Malaria- Understanding the Interactions; JID 2006:193: 1-3. Hewitt et al., Interactions between HIV and malaria in non-pregnant adults: Evidence and
Implications. AIDS 2006, 20: 1993-2004. Grimwade et al., Childhood malaria in a region of unstable transmission and high human
immunodeficiency virus prevalence Pediatric Infect Dis J, 2003;22:1057-63.