childhood obesity
TRANSCRIPT

Supervised by Dr. Najlaa Jassas
Done by Dr. Rahma ShahBahai

OUTLINE:
• Definition
• Epidemiology
• Etiology& Pathophysiology
• Approach to obese child
• Complication
• Treatment& prevention

• English formula for BMI:
703 x Weight in pounds ÷ (Height in inches)2
• Metric formula for BMI:
Weight in Kilograms ÷ (Height in meters)2

DEFINITIONfor children between 2 and 20 years of age:
●Underweigh – BMI <5th percentile for age and sex
●Normal weight – BMI between the 5th and 85th percentile
●Overweight – BMI between the 85th and 95th
●Obese – BMI ≥95th percentile
●Severe obesity – BMI ≥120 percent of the 95th percentile values, ora BMI ≥35 kg/m2 (whichever is lower)

For children <2 Y.O:
Standard weight for length curves

Currently, almost one third of children and adolescents in the United States are either overweight or obese.
●Overweight or obese (body mass index [BMI] ≥85th percentile)
22.8 percent of preschool children (2 to 5 years)34.2 percent of school-aged children (6 to 11 years)34.5 percent of adolescents (12 to 19 years)
●Obese (BMI ≥95th percentile)
8.4 percent of preschool children17.7 percent of school-aged children20.5 percent of adolescents
●Severe obesity (BMI that is either ≥120 percent of the 95th percentile or ≥35 kg/m2)
1.7 percent of school children 6.8 percent of school-aged children7.7 percent of adolescent girls and 6.8 percent of adolescent boys
National Center for Health Statistics, Centers for Disease Control and Prevention, 2012.

• 19 317 healthy children and adolescents
• 5 to 18 years of age
• The overall prevalence of:
• Overweight 23.1%
• obesity 9.3%
• severe obesity 2% Over weight obesity severe obesity

• Environmental factors
• Genetic factors
• Endocrinal diseases

Environmental factors:
• Sugar
• Sweetened beverage
• Television
• Video games
• Sleep
• Medications
• psychoactive drugs
(particularly olanzapine and
risperidone)
• antiepileptic drugs
• Glucocorticoids
• Virus: Adenovirus 36
• Gut microbes
• Toxins: BPA(bisphenol A), DDT

Genatic factors:
• Down syndrome>>>most common
• Prader-Willi syndrome
• Bardet-Biedl syndrome
• Cohen syndrome
• Turner syndrome

Endocrine diseases:
• Growth hormone deficiency
• Growth hormone resistance
• Hypothyroidism
• Leptin deficiency or resistance to leptin action
• Glucocorticoid excess (Cushing syndrome)
• Precocious puberty
• Polycystic ovary syndrome (PCOS)

PATHOPHYSIOLOGY
1. Genetic & environmental component.
caloric intake= caloric expenditure

2.THE (THRIFTY) GENE HYPOTHESIS.
• (thrifty) phenotype gene:
• Storage calories in adipose tissues ^
• Protect energy store during starvation
• More intense food-seeking behavior.
• (wasteful) phenotype gene:
• Store less calories as adipose tissues
• Less intense food-seeking behavior.

3.WEIGHT SET POINT& REGULATION OF ENERGY HOMEOSTASIS
• Weight set point is maintained by adjustment to metabolic rate in response to changes in body mass.
Dec. caloric intake=dec. leptin

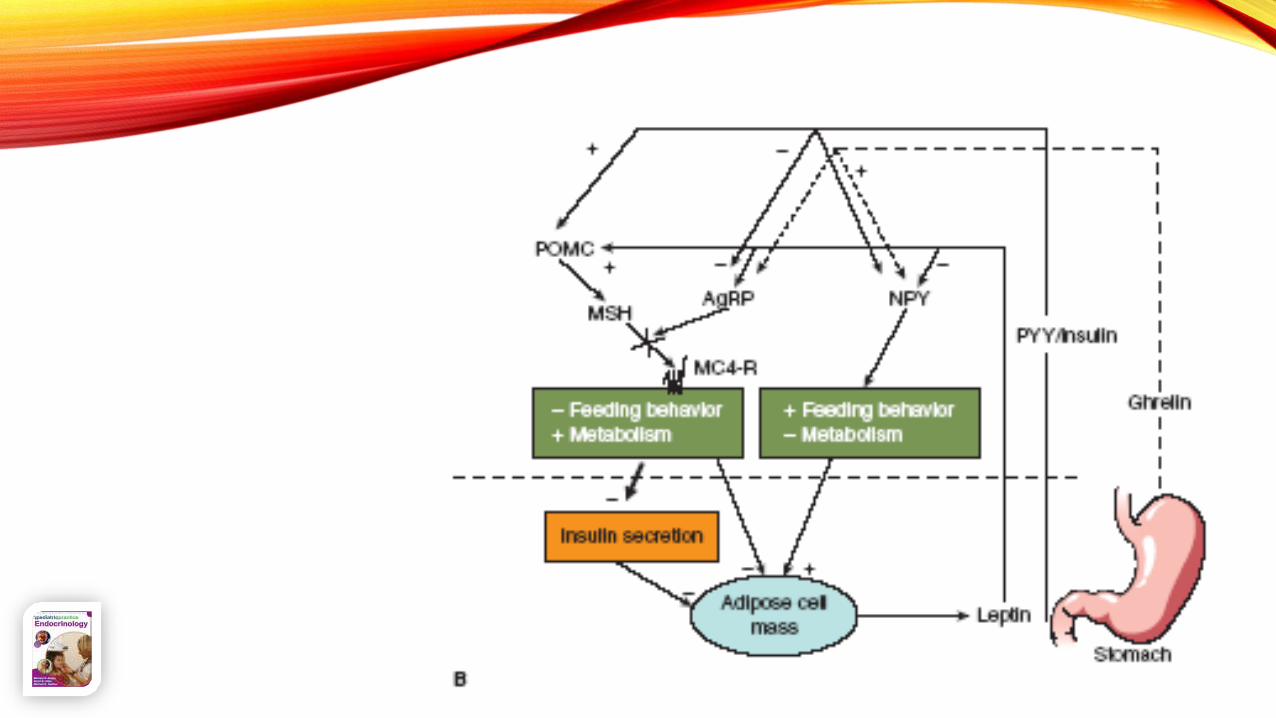
4.THE NEUROENDOCRINOLOGY
OF WEIGHT REGULATION

4 HORMONES:
• Leptin:
• Inhibit NPY/AgRP
• Appetite
• Metabolic rate
• Stimulate POMC
• Inhibit appetite
• Metabolic rate
• Secreted from >>>>
• insuline:
• Post prandial
• May act to feed intake
• Secreted from >>>>
• Ghrelin:
• in fasting
• Stim. NPY/AgRP
• Appetite
• Metabolic rate
• Secreted from >>>>
• Peptide yy:
• With feeding
• NPY/AgRP
• stimulate POMC
• Secreted from >>>>



HISTORY

EXAMINATION

INVESTIGATION
?
?



TREATMENT

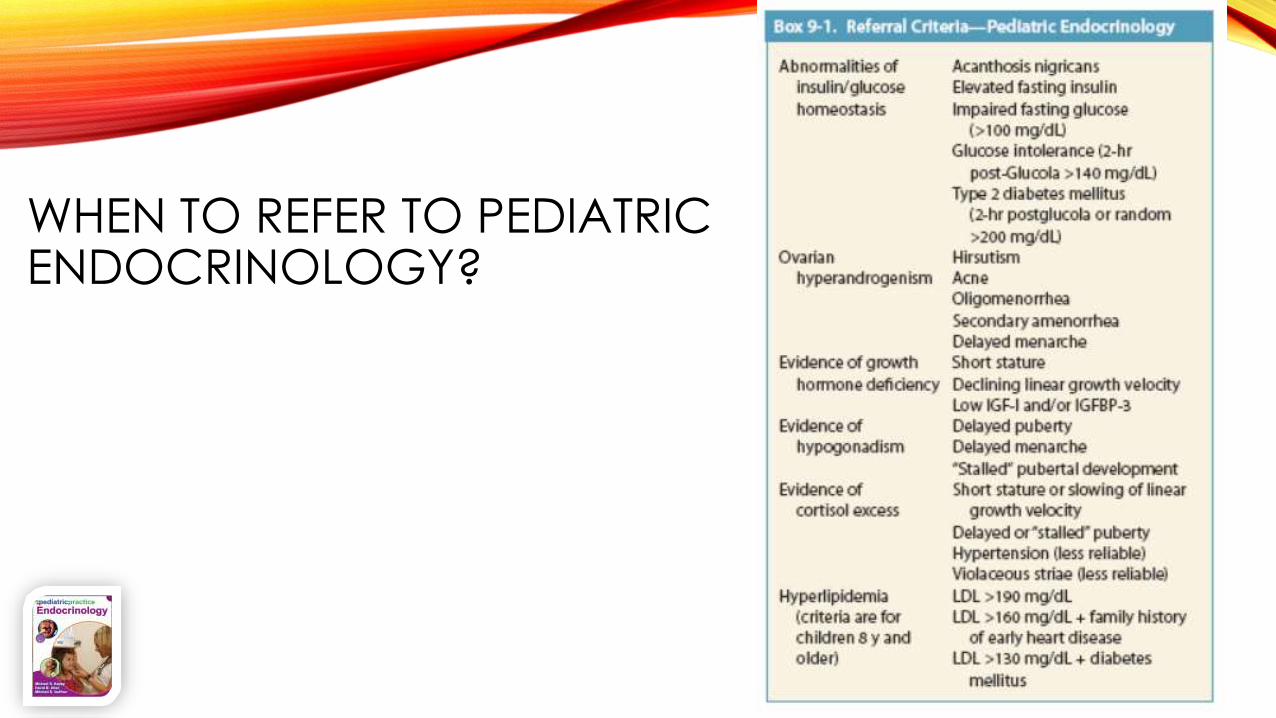
WHEN TO REFER TO PEDIATRIC ENDOCRINOLOGY?

PREVENTION

REFERENCES