childhood obesity gds...
TRANSCRIPT

Childhood ObesityChildhood ObesityGDS K49
Subdiv. of Nutrition and Metabolic DiseaseDept. of Child Health
Medical Faculty, Univ. of Sumatera Utaray,

PROBLEM NUTRISI IN INDONESIA
Overweight:
PROBLEM NUTRISI IN INDONESIA
Adult BMI (> 27 kg/m²) 11,1%
( Survey BMI in 1997)
Children < 5 years BW/Age (>+2SD) 2 46%Children < 5 years BW/Age (>+2SD) 2,46%
( Susenas in 2003)
Gizi Dalam Angka sampai dengan Tahun 2003, Ditjen Binakesmas , Depkes RI, Jakarta, 2005

DefinitionsDefinitions
• Obesity• Obesity– Excessive deposition of adipose tissue
• Overweight– Weight in excess of the average for
heightg– ↑ lean body mass or adipose tissue or
bothboth

Prevention ( WHO 1998 )
• PrimerS d• Secunder
managementmanagement obesityobesity
• Tertier

Clinical ManifestationsClinical Manifestations
• Round face double chin• Round face, double chin• Increased truncal fat deposition • Gynecomastia• Pendulous abdomen and white/purple striaep p• Buried penis• Tall for age & Early menarche• Tall for age & Early menarche• Genu valgum

Clinical manifestations

Clinical manifestations

Contributing Factors• Genetic FactorsGenetic Factors• Energy intake
h i l i i• Physical activity• Sedentary behaviory
Crombie C, Appetite and Body Weight Regulation: Sugar, Fat and M t i t S b tit t B R t FL CRC P 1994 125Macronutrient Substitutes. Boca Raton, FL: CRC Press 1994;125–136. (2.)Eaton DK, Youth Risk Behavior Surveillance — United States, 2005. Surveillance Summary 2006; SS-5 (55).
Anthropometric MeasurementAnthropometric Measurement
• BMI ≥ 95th percentile • % Ideal Body Weight (IBW) ≥ 120%% Ideal Body Weight (IBW) ≥ 120%• Triceps Skinfold ≥ 85th percentile
F t di t ib ti tt ( i t hi• Fat distribution patterns (waist-hip-ratio)– < 0.8 gynecoid type (feminine type)– > 0.8 android type (masculine type)


CausesCauses
• Positive energy • Medical causesPositive energy balance (± 95%)– Excessive caloric
• Medical causes(<5%)
End crin lExcessive caloric intake
– Decreased
– Endocrinology• Cushing syndr.
G th h physical activity– Decreased
resting metabolic
• Growth hormone deficiency, etc
G n ti sresting metabolic rate
– Genetics• Prader Willi, etc

Karakteristik obesitas idiopatik danKarakteristik obesitas idiopatik dan endogen
Obesitas Idiopatik Obesitas endogen• >90 % kasus < 10 % kasus>90 % kasus < 10 % kasus• Perawakan tinggi Pendek
Ob i k l ( ) ( )• Obesitas kel ( + ) ( - )• Fungsi mental normal Retardasi• Usia tulang N Terlambat ( delayed)• Pem fisis Normal StigmataPem fisis Normal Stigmata

Complicationsp• Endocrine : Insulin resistance, NIDDM
– Impaired glucose tolerance, acanthosis nigricansp g g• Cardiovascular: dyslipidemia (LDL >160mg/dl.
HDL <35 mg/dl),hypertension– Altered lipid profiles
• Respiratory : obstructive sleep apnea, Pickwickian syndrome
– Snoring and restless sleep, abnormal lung function teststests
• Orthopedic : Blount disease, slipped capital femoral epiphysis goutfemoral epiphysis, gout

Complicationsp
• Gastrointestinal : Cholelithiasis NASHGastrointestinal : Cholelithiasis, NASH– Hepatomegaly, altered serum transaminases
• Sexual development & growth : abnormal growth acceleration early onset of menarche growth acceleration, early onset of menarche, pubertal gynecomastia
• Psychiatric : psychosocial dysfunction


Goals of treatment program
• Appropriate for the child’s age and pp p gdevelopmental status
• Result in significant weight reduction to within 20% of the IBW
• Long-term appropriate eating and physical activity that result in weight physical activity that result in weight maintenance but do not hinder growth & development& development

Principles of treatmentPrinciples of treatment
• Dietary managementPh si l ti it ( x is )• Physical activity (exercise)
• Behaviour modification• Family involvement
l h• Alternative therapy

Dietary management• Hypocaloric balance diet
– Reduces caloric intake 200-500 kcal/day of Reduces caloric intake 200 500 kcal/day of usual intake
– 50% carbohydrate, 30% fat, and 20% proteiny p
• Protein Sparing Modified Fast Diet(4-12 weeks)– 600-800 kcal/day
1 5 2 t i /k id l b d i ht/d– 1.5-2 g protein/kg ideal body weight/day– No carbohydrate. Low starch vegetables
W t l i f fl id t l st 2 L/d– Water or calorie-free fluid at least 2 L/day– Daily supplements : multivitamins & mineral
Principle of exercise• Frequency 3-5 x/week• Intensity 50-60% maximal ability• Duration 15 min initially, building to 30-40 min• Mode : use large muscles walking, jogging,
s immin linswimming, cycling• Interest : patient dependent tennis, dancing,
martial arts skatingmartial arts, skating• Enjoyment : important factor• Incorporation into functional activities Incorporation into functional activities
walking to school, taking stairs vs elevator, bicycles vs cars
h • Reducing passive activities TV watching, videogames

Behaviour modification• Diet and activity self monitoring• Set weekly goal• Set weekly goal• Stimulus control
– Eat meals and snacks at scheduled times etc– Eat meals and snacks at scheduled times, etc• Cue elimination
– Store all food out of sight leave the table Store all food out of sight, leave the table immediately after eating, etc
• Behaviour substitution– Substitute exercise for snacking, etc
• Parental support

Alternative (aggressive) therapy(f bid b it )(for morbid obesity)
• BMI ≥ 95th percentile– Very Low Caloric Diet (PSMF)
• Pharmacotherapypy– at this time no drugs approved for
use in children• BMI ≥ 97th percentile (rarely used)
– Bariatric surgery (reduced caloric & g y (nutrient absorption)• jejunoileal bypass
• Roux-en-Y gastric bypass
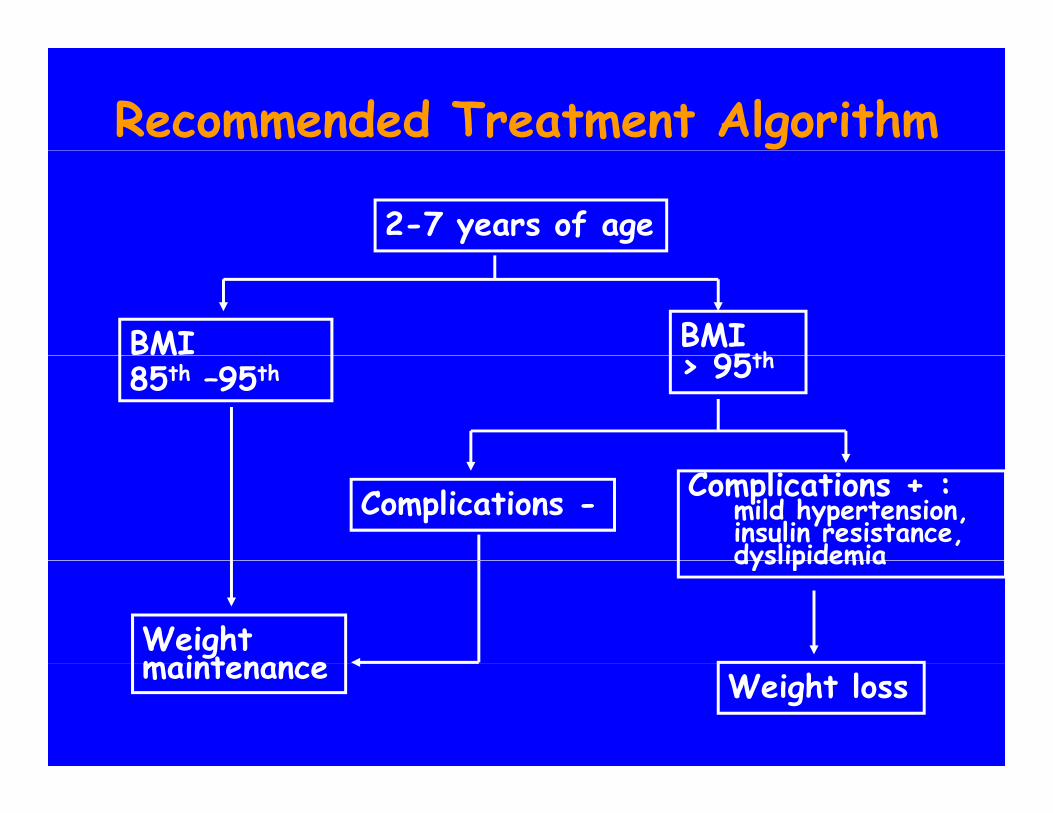
Recommended Treatment Algorithm
2-7 years of age
BMI BMI 95thM
85th –95th > 95th
Complications - Complications + :mild hypertension,insulin resistance,dyslipidemia
Weightmaintenance
dyslipidemia
maintenance Weight loss

Recommended Treatment Algorithm
7 years of age / older
BMI h h
BMI85th – 95th 95th
Complications - Complications +
Weight maintenance Weight loss

Preventing Obesity: Tips f P ntsTips for Parents
Respect your child's appetite: children do not need to finish every bottle or meal. Avoid pre-prepared and sugared foods when possible. Limit the amount of high-calorie foods kept in the home.g pProvide a healthy diet, with 30 percent or fewer calories derived from fat. Provide ample fiber in the child's diet. Skim milk may safely replace whole milk at 2 years of ageSkim milk may safely replace whole milk at 2 years of age.Do not provide food for comfort or as a reward. Do not offer sweets in exchange for a finished meal. Li it t f t l i i i iLimit amount of television viewing.Encourage active play. Establish regular family activities such as walks, ball games and other
d i i ioutdoor activities.

Components of a Successful Weight Loss PlanWeight Loss Plan
Component CommentReasonable eight Initiall 5 to 10 lb or a rate of 1 to 4 lb per monthReasonable weight-loss goal
Initially, 5 to 10 lb, or a rate of 1 to 4 lb per month.
Dietary management Provide dietary prescription specifying total numberof calories per day and recommended percentage ofof calories per day and recommended percentage ofcalories from fat, protein and carbohydrates.
Physical activity Begin according to child's fitness level, withultimate goal of 20 to 30 minutes per day (inultimate goal of 20 to 30 minutes per day (inaddition to any school activity).
Behaviormodification
Self-monitoring, nutritional education, stimuluscontrol modification of eating habits physicalmodification control, modification of eating habits, physicalactivity, attitude change, reinforcements andrewards.
Family involvement Review family activity and television viewingFamily involvement Review family activity and television viewingpatterns; involve parents in nutrition counseling.

The Pickwickian syndromew y m
• Severe cardiorespiratory distress & Severe cardiorespiratory distress & alveolar hypoventilation
• Decreased pulmonary tidal & expiratory reserve volume
• Clinical manifestation : polycytaemia, h i i di hypoxemia, cyanosis, cardiac enlargement, congestive cardiac failure somnolencefailure, somnolence
