cholesterol and bile acid metabolism medical biochemistry lecture #52
TRANSCRIPT

Cholesterol and Bile Acid Metabolism
Medical Biochemistry
Lecture #52

CHOLESTEROL SYNTHESIS, TRANSPORT, AND EXCRETION
• Cholesterol is present in tissues and in plasma lipoproteins either as free cholesterol or, combined with a long-chain free fatty acid, as cholesteryl ester.
• It is synthesized in many tissues from acetyl-çoA and is eliminated from the body in the bile as cholesterol or bile salts.
• Cholesterol is the precursor of all other steroids, such as sex hormones, bile acids, and vitamin D.
• It occurs in foods of animal origin such as egg yolk, meat, liver, and brain.

CHOLESTEROL SYNTHESIS, TRANSPORT, AND EXCRETION
(cont)• A little more than half the cholesterol of
the body arises by synthesis (about 700 mg/d), and the remainder is provided by the average diet. The liver accounts for 10% of total synthesis in humans, the intestine for about another 10%.
• Microsomal (endoplasmic reticulum) and cytosol fraction of the cell is responsible for cholesterol synthesis.
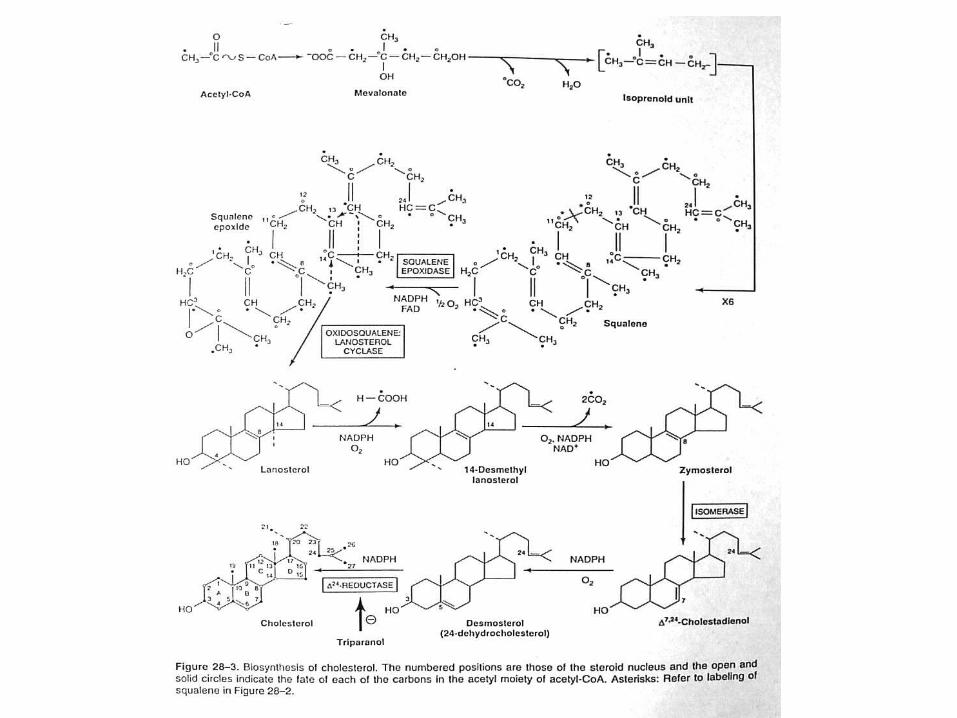
Acety-CoA is the source of all carbon atoms in cholesterol:
It can be divided into five steps:
• Step 1. Acetyl-CoA forms HMG-CoA and mevalonate.
• Step 2. Mevalonate forms active isoprenoid units.
• Step 3. Six isoprenoid units form squalene. • Step 4. Squalene is converted to lanosterol. • Step 5. Lanosterol is converted to cholesterol.




Cholesteryl ester transfer protein facilitates transfer of cholesteryl
ester from HDL to other lipoproteins:
• This protein is present in the plasma of humans but not the rat, is associated with HDL.
• It facilitates transfer of cholesteryl ester from HDL to VLDL, IDL, and LDL and allows triacylglycerol to transfer in the opposite direction.



Bile acids are formed from cholesterol:
• About 1 gram of cholesterol is eliminated from the body per day. Approximately half is excreted in the feces after conversion to bile acids. The remainder is excreted as cholesterol.
• The primary bile acids are synthesized in the liver from cholesterol. These are cholic acid and chenodeoxycholic acid.


CLINICAL ASPECTS: • Serum cholesterol is correlated with the incidence of
atherosclerosis and coronary heart disease. • Changes in diet play an important role in reducing
serum cholesterol: Substitution in the diet of polyunsaturated and monosaturated fatty acids for some of the saturated fatty acids is most beneficial. Sunflower, cottonseed, corn, olive, and soybean oil contain high concentration of monounsaturated fatty acids. On the other hand, butterfat, beef fat, and palm oil contain a high proportion of saturated fatty acids.
• Lifestyle affects the serum cholesterol level:

When diet changes fail, hypolipidemic drugs will reduce serum cholesterol
and triacylglycerol: • Cholestyramine resins: Block reabsorption of bile acids. • Sitosterols: acts by blocking the absorption of
cholesterol from the gastrointestinal tract. • Mevocore or lovastatin: inhibitors of HMG-CoA
reductase • Clofibrate or gemfibrozil: exert their effect by diverting
esterification to oxidation of free fatty acids. • Probucol: increase LDL catabolism via receptor
independent pathway, prevents oxidation of LDL • Nicotinic acid: reduces the flux of FFA by inhibiting
adipose tissue lipolysis, thereby inhibiting VLDL production by the liver.