christie eheman, phd, mshp cancer surveillance branch...
TRANSCRIPT

Christie Eheman, PhD, MSHP Cancer Surveillance Branch
Division of Cancer Prevention and ControlNational Center for Chronic Disease Prevention and Health Promotion

1992 Cancer Registry Amendment Act, Public Law 102-515, authorized CDC to establish NPCR
◦ Provided funds to CDC for funding states and territories to enhance or plan/implement registries
◦ Work with states to develop model legislation and regulations
◦ Provide training on Central Registry operations
◦ Standardize a minimum set of data items
◦ Set national standards for completeness, timeliness and quality


48 funded programs ◦ 45 states, DC, Puerto Rico, Pacific Islands JurisdictionNPCR U.S. population coverage - 96% percent◦ In collaboration with NCI – 100% population coverageNPCR Cancer Surveillance System ◦ Approximately 1.2 million new invasive cancer
cases are submitted to CDC electronically each year◦ Data base includes approximately 17.4 million
invasive cancer cases from 1995–2007◦ CDC does not receive identifiers (name, address,
SSN)

◦ Membership organization – central cancer registries in U.S. and Canada◦ Supported by CDC, NCI, and other sponsoring
organizations as well as membership fees, etc.◦ Sets standards for data items and electronic data
record structure Work group structure used to establish standards and include representatives from registries and other partners including CDC

State Central Cancer Registry
•Cleaning•Editing
•Analyzing
•Hospitals
•Outpatient
centers
•Laboratories
•Radiation
therapy centers
•Medical oncology
facilities
•Physicians
Electronic
Hard copy
Final data

Record Identification◦ Registry
identification◦ Patient ID
numberDemographic◦ Race◦ Age◦ Sex◦ State◦ County◦ Zip code◦ Census tract
Cancer Identification1
◦ Date of diagnosis◦ Primary site◦ HistologyReporting SourceStage/Prognostic Factors◦ Summary
stage◦ Biomarkers
(HER2, PR, ER)
Follow-up/Death◦ Date of last
contact/death◦ Vital status◦ Cause of deathConfidential◦ Patient name◦ Patient
address
1ICD-O codes – conversion in data set to manage changes over time
Individual NPCR central cancer registries (CCRs) may collect more than is required for their own purposes including researchVital Status◦ Collected from local vital statistics◦ Linkage with National Death Index
Encouraged and financially supported by CDCNot all registries have linkedNot all registries that have linked have updated their data bases
Significant manual review of partial matches

Less complete reporting from◦ Physician offices◦ Treatment facilities◦ Out-patient clinics◦ Entire data set (1995 - forward) is resubmitted
each year and completeness improves over timeLocal funding for CCRs has been decreasing◦ Furloughs◦ Hiring freezesData access for research
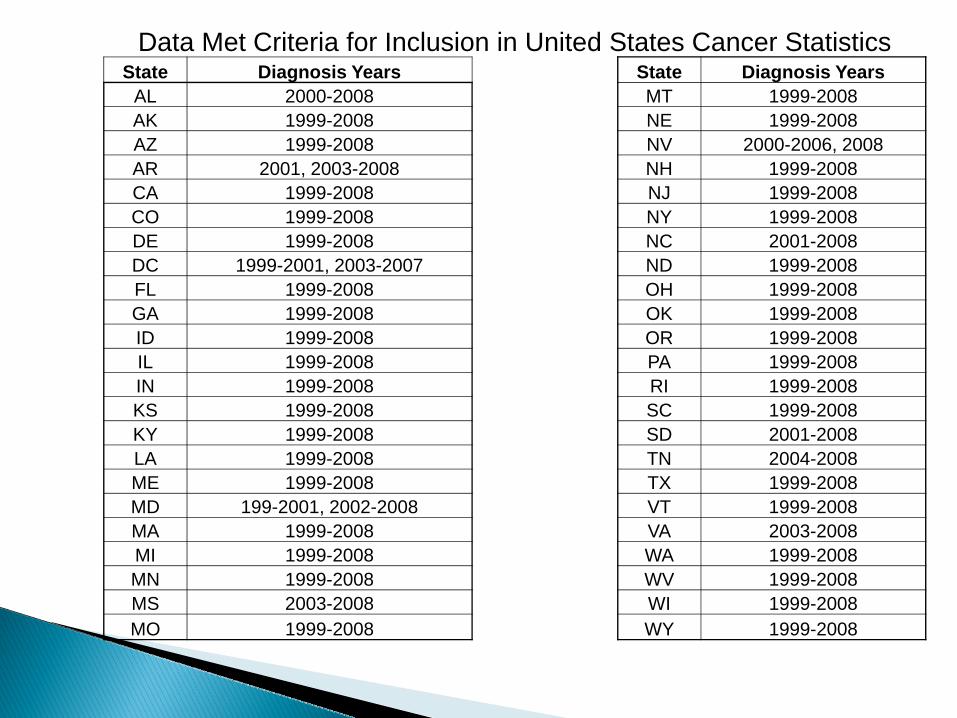
Data Met Criteria for Inclusion in United States Cancer StatisticsState Diagnosis Years State Diagnosis Years
AL 2000-2008 MT 1999-2008AK 1999-2008 NE 1999-2008AZ 1999-2008 NV 2000-2006, 2008AR 2001, 2003-2008 NH 1999-2008CA 1999-2008 NJ 1999-2008CO 1999-2008 NY 1999-2008DE 1999-2008 NC 2001-2008DC 1999-2001, 2003-2007 ND 1999-2008FL 1999-2008 OH 1999-2008GA 1999-2008 OK 1999-2008ID 1999-2008 OR 1999-2008IL 1999-2008 PA 1999-2008IN 1999-2008 RI 1999-2008KS 1999-2008 SC 1999-2008KY 1999-2008 SD 2001-2008LA 1999-2008 TN 2004-2008ME 1999-2008 TX 1999-2008MD 199-2001, 2002-2008 VT 1999-2008MA 1999-2008 VA 2003-2008MI 1999-2008 WA 1999-2008MN 1999-2008 WV 1999-2008MS 2003-2008 WI 1999-2008MO 1999-2008 WY 1999-2008

StateRegistry Ref Yr NPCR Ref Yr State
Registry Ref Yr NPCR Ref Yr
AL 1996 1996 MT 1979 1994AK 1996 1996 NE 1987 1994AZ 1981 1994 NV 1979 1994AR 1996 1996 NH 1987 1994CA 1988 1994 NJ 1979 1994CO 1979 1994 NY 1979 1995DE 1979 1997 NC 1985 1994DC 1979 1995 ND 1997 1994FL 1981 1994 OH 1992 1994GA 1995 1995 OK 1995 1995ID 1979 1994 OR 1996 1996IL 1985 1994 PA 1982 1994IN 1987 1994 RI 1987 1994KS 1995 1995 SC 1994 1994KY 1991 1994 SD 2001 2001LA 1983 1994 TN 1983 1997ME 1983 1994 TX 1979 1994MD 1992 1995 VT 1994 1994MA 1982 1994 VA 1979 1995MI 1985 1994 WA 1992 1994MN 1988 1994 WV 1993 1994MS 1996 1996 WI 1979 1994MO 1979 1994 WY 1979 1995
Percent case completeness estimated based on mortality data Electronic data edits◦ Single field edits for valid code◦ Inter-field edits for consistency
Sex, primary siteDate of last contact/death, vital status
◦ Inter-record edits for consistency among multiple primary sites
Verify date of birth same on all records for a patientVerify vital status same on all records for a patient

Technical assistance provided by certified tumor registrars from CDCTraining Registry software from CDCData sharing agreements◦ Case sharing across states - strong relationships
between states where cancer patients regularly move across states (Florida, New York)
Data Audits ◦ Central registries◦ CDC

Compare data from medical records with central registry data file Also look for missed casesOver last 5 year time period, all registries audited onceCentral registry self-audits required – a small number of cases each year
Investigating the Risk of Cancer in 1990–1991 US Gulf War Veterans With the Use of State Cancer Registry Data◦ Ann Epidemiol. 2010 Apr;20(4):265-272.e1. Epub 2010 Jan 29A combined healthy lifestyle score and risk of pancreatic cancer in a large cohort study. ◦ Arch Intern Med . 2009;169:764-70Lung Cancer Risk Among Smokers of Menthol Cigarettes◦ J Natl Cancer Inst. 2011;103:1–7 Methodological Issues in United States Retrospective Cancer Incidence Studies◦ Am J Epidemiol . 2009;170:112–119

State-Level Mammography Utilization from 2000-2006 with Corresponding Breast Cancer Incidence Rates◦ AJR Am J Roentgenol. 2009;192:352-60Utilization of screening mammography in New Hampshire: a population-based assessment◦ Cancer. 2005;104:1726–1732Characteristics of adult osteosarcoma patients: Results from an ongoing postmarketing drug safety surveillance study◦ Journal of Clinical Oncology, 2010 ASCO Annual Meeting
Proceedings (Post-Meeting Edition).Vol 28, No 15_suppl (May 20 Supplement), 2010: 1608
Authorizing law requires that CCRs maintain a balance between releasing data for the purposes of cancer control and protecting the patients’ right of privacy.

Currently, laws and regulations regarding CCRs and the release of CCR data aremostly promulgated at the state level
- impose additional requirements for review of research and informed consent when human subjects are involved
- State statutes often overlap with the federal rules in conducting of human subjects research, but the scope, definitions, and standards of protection vary.

Result: One set of procedures for data useand confidentiality cannot be mandated for all locations.
Consequence: Accessing CCR data for research, particularfor multi-state CCR data is complicated and challenging.
Purposes: • Gain understanding of comprehensive requirements and
barriers of cancer registry data access for research.
• Identify optimal state/registry rules and policies.
• Investigate methods for streamlining the IRB processes and pilot test the best methods.
• Assist researchers in managing the process.
Time line: Sept 21, 2010 – Sept 20, 2013
Finished compilation on - federal and state level policies/regulations/rules for CCR data collection and
access- state level IRB application requirements and contacts for access CCR data- state-specific step by step data access application instruction
In the process of analysis and loading information into an interactive website. This website has two sites to serve the following purposes:
• Public site - Provide laws and regulation on cancer registry data collection and access to public and guide researchers step by step to apply and access state-specific CCR data
• Individual site - Assist researchers to manage multi-state CCR data access and IRB • application process

Basic required documents from 48 states:
• Cancer registry data use application• Study proposal/protocol• List of data items needed• Cancer Registry data use/confidentiality agreement
In addition to basic requirements, special requirements for data access vary substantially among states

State‐specific Requirements Summary
1. Initial cancer registry contactrequired prior to applicationsubmission
• 45 states (including DC, US Pacific Islandsand Puerto Rico)
2. Allowance of releasing state residents’ identifiable data to researchers
• 48 states allowed after patient’s consent • 1 state only allows to release it to their own
state health department researchers after patient’s consent
3. Requirement of sponsorship from local researcher
• 3 states required local sponsorship• 2 states indicated local sponsorship
will make application easier• 1 state required to be co‐author for
publications
4. Requirement of Cancer registry specific Human Subject Protection training
• 16 states required some type of Human Subject Protection training

State‐specific Requirements Summary
5. IRB approval from requested state and/or researcher’s affiliated institution
• 16 states required only IRB approval from researcher’s affiliated institution
• 7 states required only IRB approval from registry affiliated institution
• 23 states required IRB approvals from both researcher’s and registry affiliated institution
• 4 state required IRB approvals from registry affiliated institution but information was not available if IRB approval required from researcheraffiliated institution
6. Pediatric research special requirements
15 states have special requirements:• 4 states required parental and/or physician’s consent• 1 state required special section in application• 1 state required cases by case review• 1 state does not provide parents contact info• 7 states indicated more difficult approval process
required• 1 states never handled pediatric study requests

State‐specific Requirements Summary
7. Patient contact and consent required for releasing of confidential data
Required consent:• 26 states ‐required patient consents• 21 states ‐ required both physician and patients
consents• 3 state ‐ had no standards• Consents can be passive or active
Who (including DC, US Pacific Islands and Puerto Rico) contacts patients:• 16 states - the researcher does the contacting and
consenting • 15 states - the cancer registry does the contacting
and consenting • 12 states - the cancer registry does initial contact
and researcher consents • 4 states - have options on contact and consent

State‐specific Requirements Summary
8. Level of detail and number ofsteps in the approval process
One level:• 2 states only required Registry approval• 2 states only required IRB approval• 1 state only required Cancer Advisory group approval
Two levels• 14 states required Registry + IRB(s) approval• 6 states required Registry + Cancer Advisory group(s )
approval• 1 state required Cancer Advisory groups + IRB approval• 2 states required State level officer(s) + IRB approval• 2 states required Registry + State level officer(s)
approval
≥Three levels• 13 states required Registry + Cancer Advisory groups +
IRB approval• 5 states required Registry + state level officer(s) +IRB approval

State‐specific Requirements Summary
9. Frequency of IRB and other regulatory committee meetings
• Weekly: 2 states• Monthly: 5 states• Quarterly : 5 states • Part‐time: 1 state
10. Charge of a fee/Structure of the fee (IRB fee, data process fee, data linkage fee, etc.)
• 33 states will charge fees
11. Timeframe for the approval process
• <2 months: 25 states• 3‐6 months: 16 states• >6 months: 4 states• Varied: 5 states (depends
on available staff time, seasons, and complexity of case)

The findings and conclusions in this presentation are those of the presenter, and do not necessarily represent the official position of the Centers for Disease Control and Prevention
Christie [email protected]