christie m s c c 131109
TRANSCRIPT
Gail Eva

What are the consequences of disability for patients with spinal cord compression?
What strategies do patients use to manage disability?
How do health care staff understand / respond to patients’ disability?
What support is offered to patients in managing disability? Is it useful?
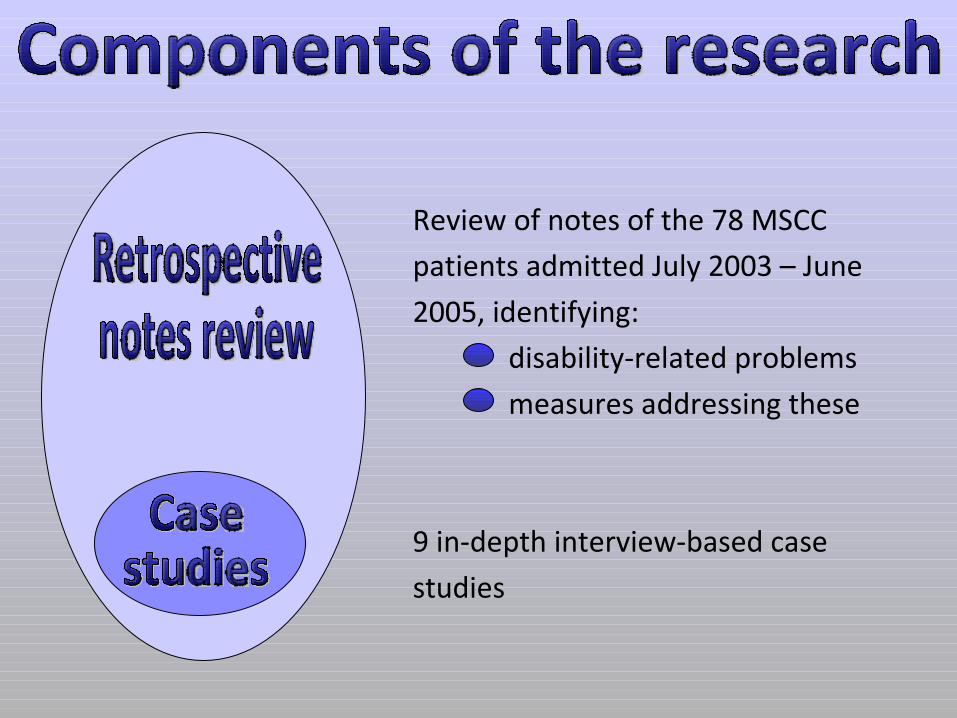
Review of notes of the 78 MSCC
patients admitted July 2003 – June
2005, identifying:
disability-related problems
measures addressing these
9 in-depth interview-based case
studies
Each case made up of interviews with a patient, their carer(s), and a range of health care professionals – total of 58 interviews.

Alf, late 70sCa ProstateRetired technician
Ben, early 40sCa ThymusAcademic
Celia, mid 50sMyelomaCleaner and carer
Derek, early 70sCa ProstateRetired salesman
Eddie, early 80sEddie, early 80sCa ProstateCa ProstateRetired sailorRetired sailor
Frank, mid 50sCa BladderRetired accountant
Gill, mid 40sCa BreastProject manager
Hugh, early 80s Ca ProstateRetired academic
Ian, early 60sIan, early 60sCa Kidney Ca Kidney EngineerEngineer
The way that rehabilitation is placed on patients’ agenda.
The way that information passes from senior medical staff to rehabilitation staff.
A focus on discharge as the end-point of rehabilitation.
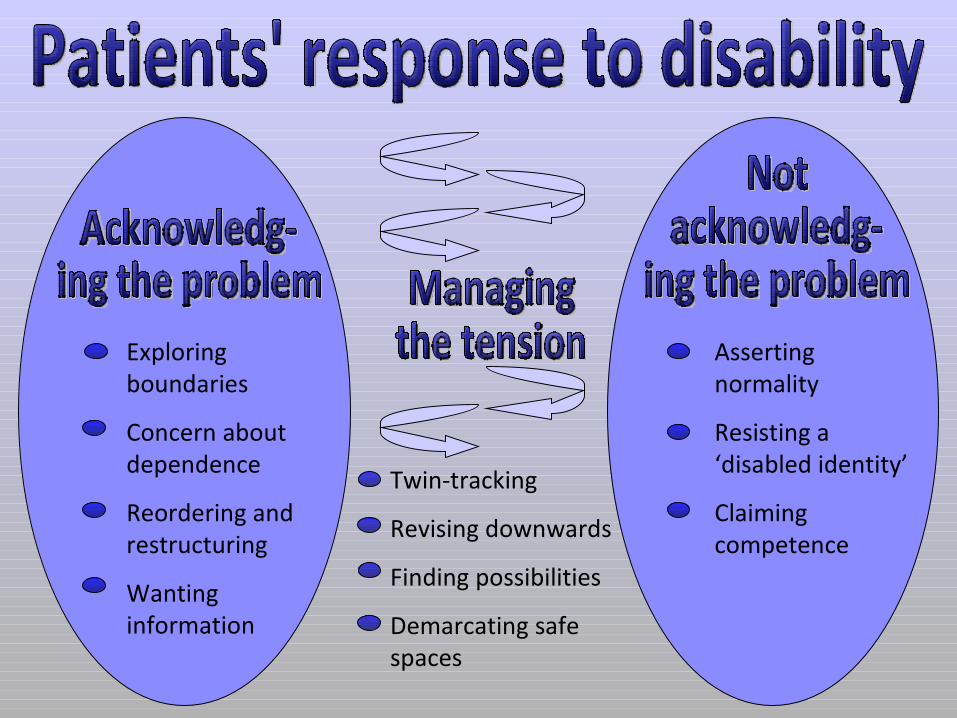
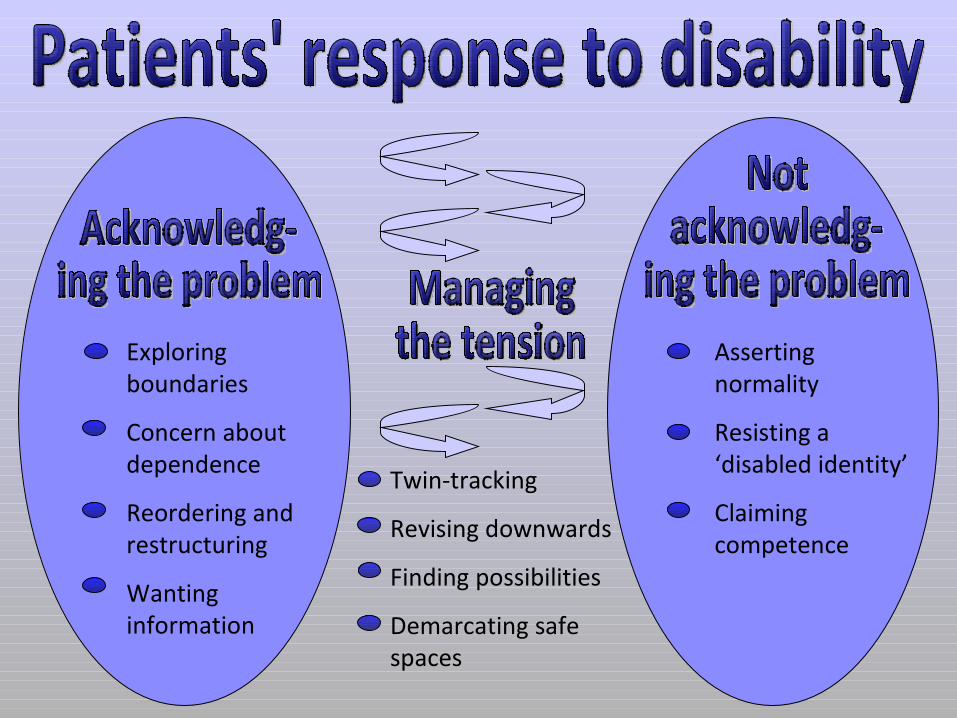
Patients’ response to disability.
Patients’ presentation of themselves and their circumstances, and staff’s responses to this.
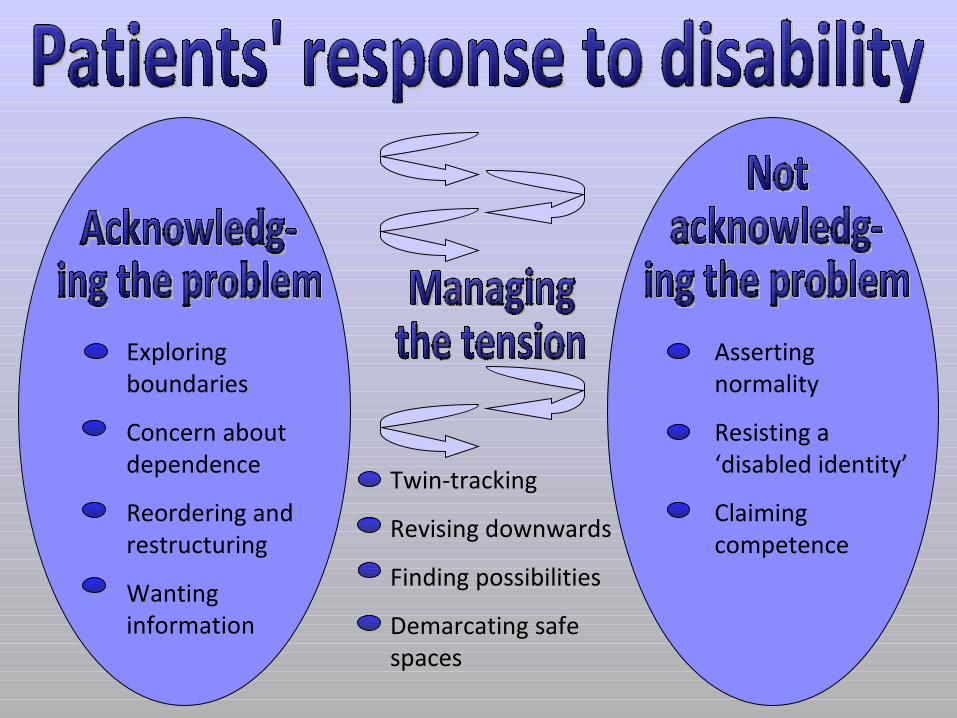
Exploring boundaries
Concern about dependence
Reordering and restructuring
Wanting information
Asserting normality
Resisting a ‘disabled identity’
Claiming competence
Twin-tracking
Revising downwards
Finding possibilities
Demarcating safe spaces

Exploring boundaries
Concern about dependence
Reordering and restructuring
Wanting information
I’m working out the boundaries:
seeing what I can and can’t do. I
tried to walk up to the doctors
the other day, and I couldn’t
make it.
I sit in the house and I feel fine,
and I think yes, I can do it. But
when I go out, after a hundred
meters I feel very weak.
That’s an awful thing to have to
surrender yourself to. You can’t
get around any more.
Asserting normality
Resisting a ‘disabled identity’
Claiming competence
Exploring boundaries
Concern about dependence
Reordering and restructuring
Wanting information
Asserting normality
Resisting a ‘disabled identity’
Claiming competence
Twin-tracking
Revising downwards
Finding possibilities
Demarcating safe spaces
I’ve had to give up my allotment,
which is sad – that was a good
break for me, winter digging,
that’s hard work. But now I can’t
stand and move without a frame. I
mean, I could hold on to a fork to
steady myself, but then I couldn’t
dig. But I have a few ambitions
that I will achieve. And the first
one – the essence of being
independent – is to go and hit a
golf ball. Proper swing, unaided,
followed by a hole.
Interview 1While I can still walk, it’s alright. I mean, if I had to be in a wheelchair, it would just be terrible.
Interview 1While I can still walk, it’s alright. I mean, if I had to be in a wheelchair, it would just be terrible.
Interview 2 (five months later)If we’d discussed this last November I would have been in tears. But now I can honestly say it’s an absolute joy to go out in the wheelchair. The wheelchair thing, it’s almost crept on me, and it turns out it’s not a big issue.
Interview 1While I can still walk, it’s alright. I mean, if I had to be in a wheelchair, it would just be terrible.
Interview 2 (five months later)If we’d discussed this last November I would have been in tears. But now I can honestly say it’s an absolute joy to go out in the wheelchair. The wheelchair thing, it’s almost crept on me, and it turns out it’s not a big issue.
…
I can still walk a bit and get into the chair. If I couldn’t get up stairs at all, or couldn’t get out of the seat… I can’t imagine what that might be like.
Exploring boundaries
Concern about dependence
Reordering and restructuring
Wanting information
Asserting normality
Resisting a ‘disabled identity’
Claiming competence
Twin-tracking
Revising downwards
Finding possibilities
Demarcating safe spaces
The way that rehabilitation is placed on patients’ agenda.
The way that information passes from senior medical staff to rehabilitation staff.
A focus on discharge as the end-point of rehabilitation.
Patients’ response to disability.
Patients’ presentation of themselves and their circumstances, and staff’s responses to this.
Everything has been arranged,
from A to Z. I had the funeral
directors around, chose my coffin. I
love my husband very much, but I
love my Mum and Dad as well. And
it worried me – if I get buried here,
it’s too far for my parents to come
if they want to grieve and vice
versa, Graham. So I’ve spoken to
the vicar, and although I didn’t
want to get cremated, I’m going to
be cremated so there are two
caskets. One will be buried back
home and one will be buried here…
… I’ve got it all paid for. I’ve chosen
the hymns and the music I want
played. The vicar e-mailed me the
service and all the missing bits I
needed to fill in. And it’s all done,
it’s all done.
So if, God forbid, I take a turn for
the worse, today or tomorrow, the
i’s are dotted the t’s are crossed on
the service and what I want.
OT: Gill was remaining incredibly positive considering what was happening to her. My perception was that she was holding it together because that’s her personality. She’s a professional lady and she’s always taken a bright outlook on things as far as she can.
OT: Gill was remaining incredibly positive considering what was happening to her. My perception was that she was holding it together because that’s her personality. She’s a professional lady and she’s always taken a bright outlook on things as far as she can.
--ooOOoo--
Social Worker: She’s a very competent person, and she has overcome a lot of the problems herself, like finding somebody to provide the care that she wants. She’s very resourceful, she will not sit there feeling sorry for herself. She will work on ways of achieving what she wants.
OT: Gill was remaining incredibly positive considering what was happening to her. My perception was that she was holding it together because that’s her personality. She’s a professional lady and she’s always taken a bright outlook on things as far as she can.
--ooOOoo--
Social Worker: She’s a very competent person, and she has overcome a lot of the problems herself, like finding somebody to provide the care that she wants. She’s very resourceful, she will not sit there feeling sorry for herself. She will work on ways of achieving what she wants.
--ooOOoo--
Nurse: Gill’s a great initiator. She knows how to take things forward and she’s very clear about you don’t wait around for people to do stuff for you, you get on and do it yourself.

OT:
Gill went home adamant that she wanted to be
upstairs, which we completely went with because
that was her wish. The bath was highly important to
her and there was no way of having a bath
downstairs, and she felt that was a better option.
Three am, I’m wide awake and
thinking about going home and
what I’m going to do… how will I
get my rice pudding from the
kitchen to my table? Now, see, I’ve
got the problem solved. I’ve got a
tea trolley I made years ago. I’ll take
the back two casters off, add some
handles, there’s plenty of timber
down the shed. I’ll walk with my tea
trolley: push, stop, push, stop, like
so. I’m looking forward to going
home. It’ll be an adventure!
I had a happy childhood – we ran wild. I
would watch the blacksmith pump his
bellows when I was seven. I learned so
much then, that when I got a job at the
factory at fourteen I knew more than the
other young starters so I did really well.
Fortunately, everything is just fortunately, I
met a good gang of kids, they didn’t drink,
they were really good lads. The chaps at
work, I always met the best ones, I don’t
know why, but everything seemed to work
out right for me. My friend knew someone
in the Merchant Navy, helped me to get a
job there. I’ve been to almost every country
in the world. The blokes on the ship were
really good fellows, they took care of me.
OT:
When I first met him he was relatively realistic, saying he didn’t think that he
would cope at home as he was. I agreed that he needed to be independent with
his mobility before he could go home. But he didn’t really improve with
radiotherapy and he was getting more and more frustrated, maybe feeling like
we were handling him with kid gloves a little bit, saying you’re not ready to go
home. The more conversations I had with him, the less he seemed to understand
what we were getting at and that he wouldn’t be able to go back to how he was
originally. …
Eventually, we said you’ve got options: either go home as you are but agree not
to undertake any kitchen activities, or if you want to be independent, you’ll need
adaptations to the kitchen to allow you more space to manoeuvre. He said he just
needed a rail on the work surface, things that we thought weren’t so appropriate
because work surfaces aren’t meant for such weight bearing activities.
We had to be quite assertive with him to make
him understand where we were coming from and
why we were saying what we were saying and
that it wasn’t to take away his independence,
even though it was in the short term, we were
trying to do it so that long term he would maybe
have some rehabilitation at home as such.

We had to be quite assertive with him to make him understand
where we were coming from and why we were saying what we
were saying and that it wasn’t to take away his independence,
even though it was in the short term, we were trying to do it so
that long term he would maybe have some rehabilitation at home
as such.
Gill went home adamant that she wanted to be upstairs, which we
completely went with because that was her wish.
I asked him whether he wanted me to make a referral
to the [community services] for ongoing rehab at
home because I knew independence was really
important to him. He declined, which was a shame
really. I tried to explain that they could carry on the
work that we were doing in hospital but he still didn’t
want it. I was surprised actually, I really thought that
he’d be very keen on that.
The first time I used it, it was
the wrong move really,
because we went to Tesco and
Tesco was busy, and there I
was down, you know, in this
wheelchair and all of these
people, I just felt all these
people coming towards me.
And it was like – oh, I had no
control. It was terrifying,
absolutely terrifying and I just
wanted to get out.
Prioritising
Pacing
Planning
• What needs to be done in your day or week?
• What do you want to do?
• (What do others expect you to do?)
• How important is this activity to you?
• How much energy do these different activities use up?
• What can you eliminate or stop doing?
• What can you ask others to do for you?
Three Ps
Looking out for, and supporting, the ways in which patients are acknowledging and adapting to disability.
Identifying short-term, achievable goals and focussing on these.
Encouraging realism without contradicting patients’ preferred sense of self.